
Cardiorenal syndrome: therapeutic · Cardiorenal syndrome: therapeutic approaches-Ultrafiltration...
42
Cardiorenal syndrome: therapeutic approaches-Ultrafiltration Dr Pascaline ALIX Université Claude Bernard Lyon 1 Néphrologie-Hôpital E. Herriot Lyon, FRANCE
Transcript of Cardiorenal syndrome: therapeutic · Cardiorenal syndrome: therapeutic approaches-Ultrafiltration...

Cardiorenal syndrome: therapeutic
approaches-Ultrafiltration
Dr Pascaline ALIX Université Claude Bernard Lyon 1
Néphrologie-Hôpital E. Herriot Lyon, FRANCE
Heart failure
• Despite modern heart failure therapy, the prognosis of patients with heart failure remains poor
• Prevalence of chronic kidney disease : 32% • Worsening renal function and mortality
Damman et al, 2013 Mahon et al, 2002
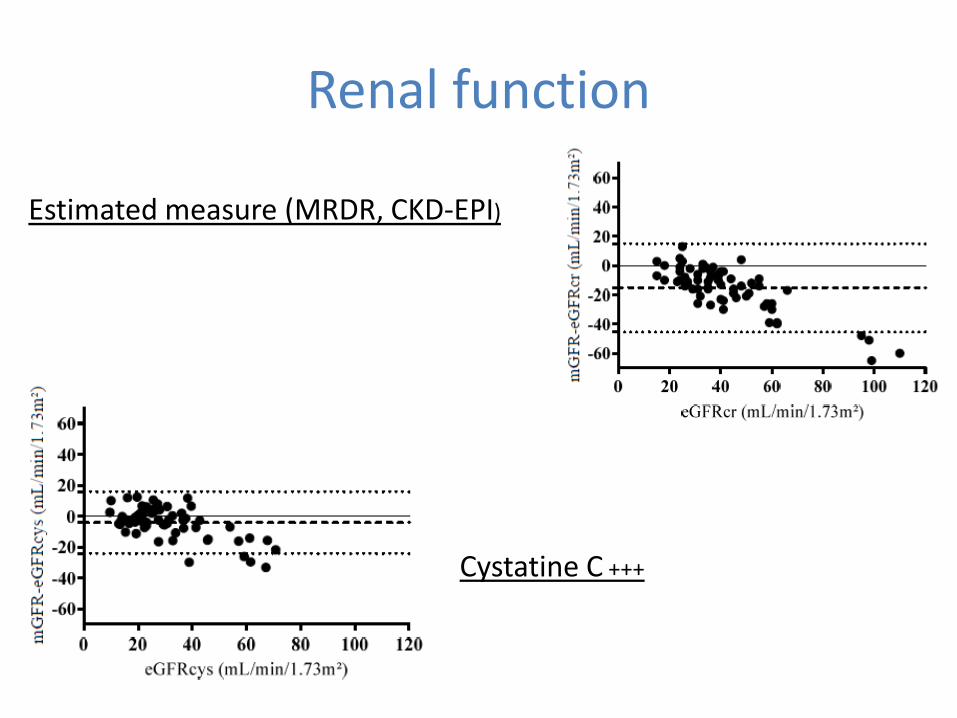
Renal function
Estimated measure (MRDR, CKD-EPI)
Cystatine C +++
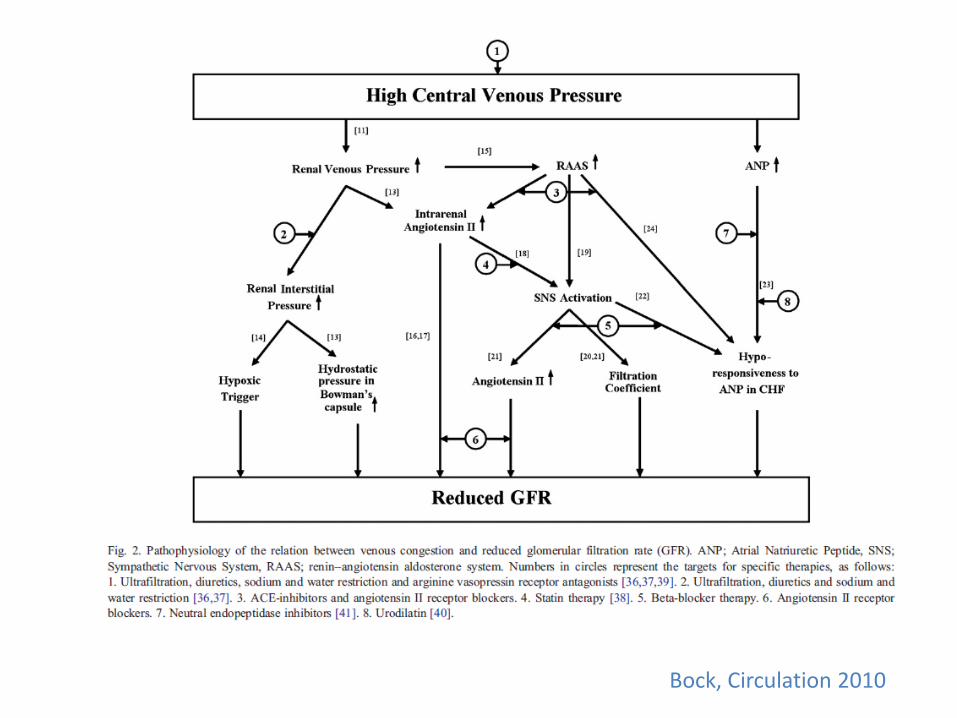
Bock, Circulation 2010
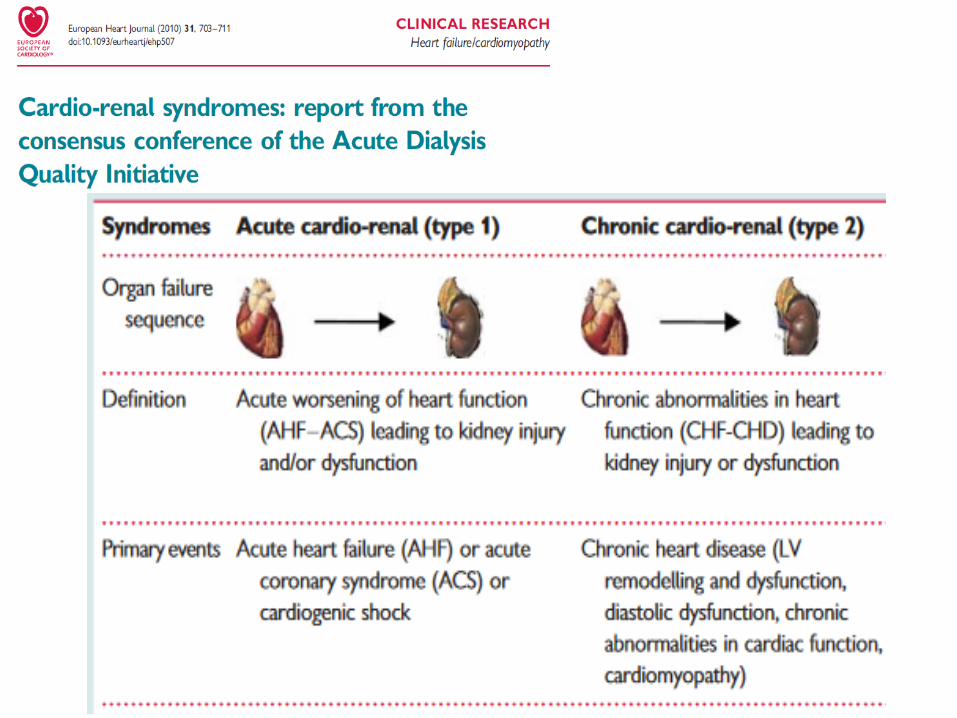
Ultrafiltration Type 1 cardiorenal syndrome
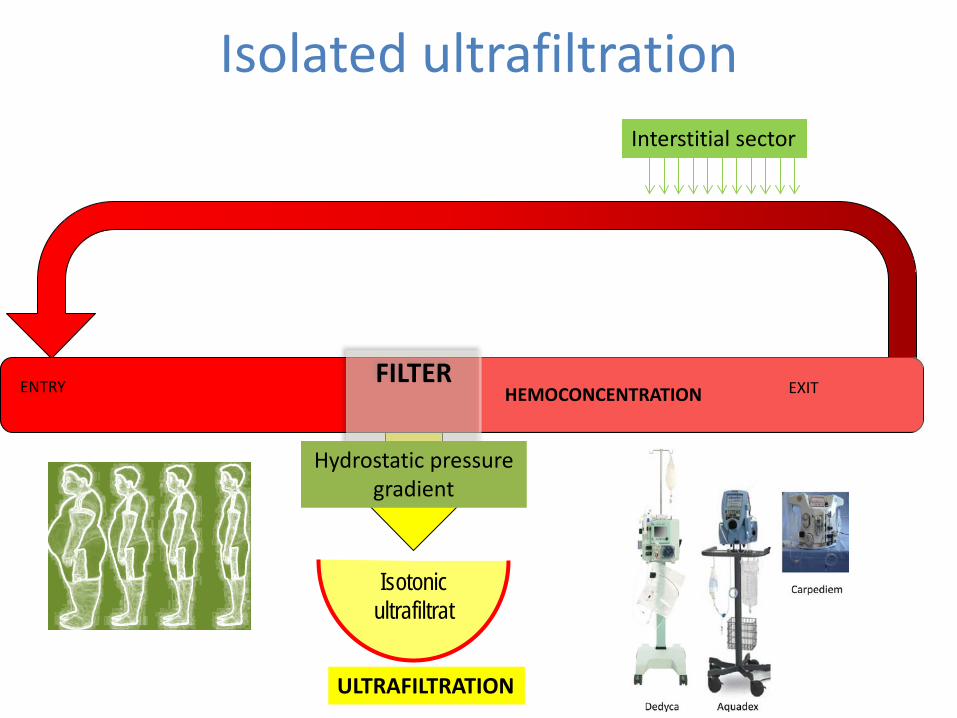
Isolated ultrafiltration
Isotonic ultrafiltrat
HEMOCONCENTRATION
ULTRAFILTRATION
ENTRY
EXIT
FILTER
Hydrostatic pressure gradient
Interstitial sector
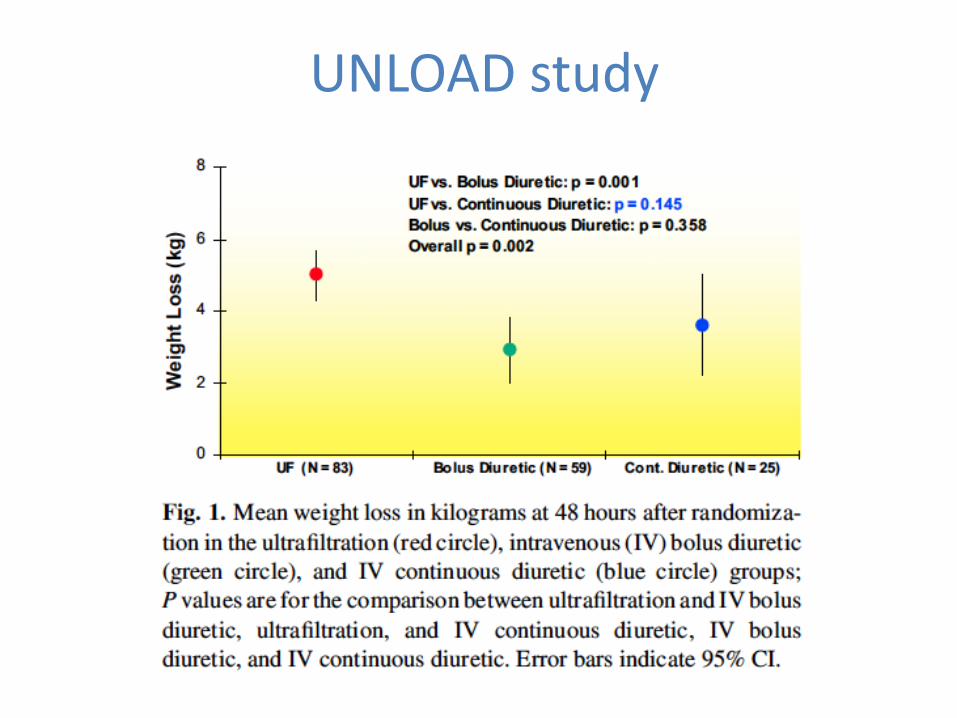
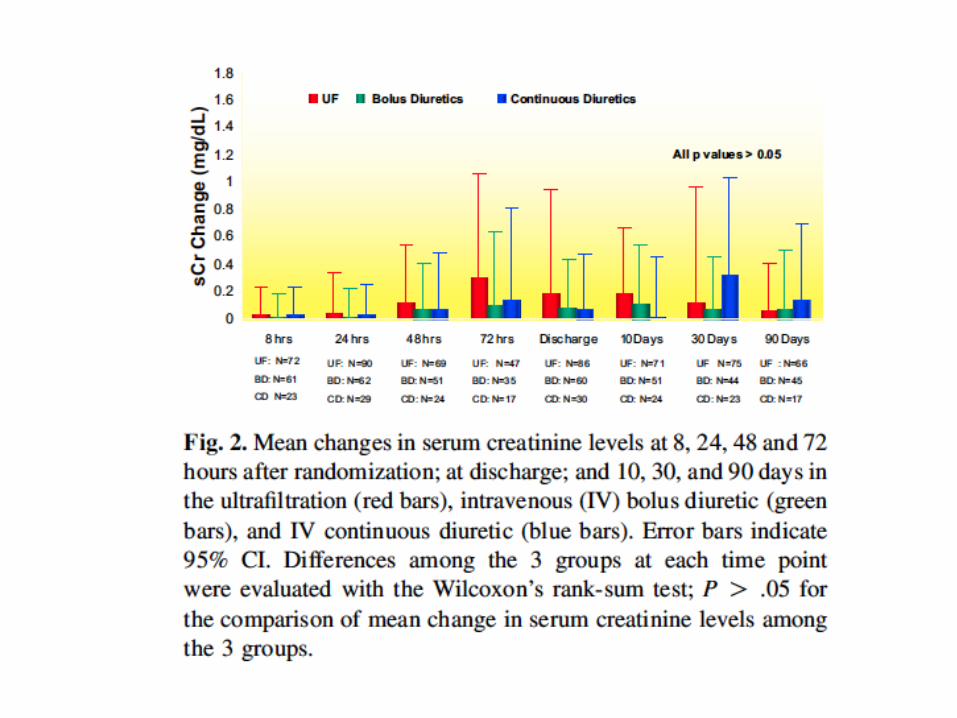
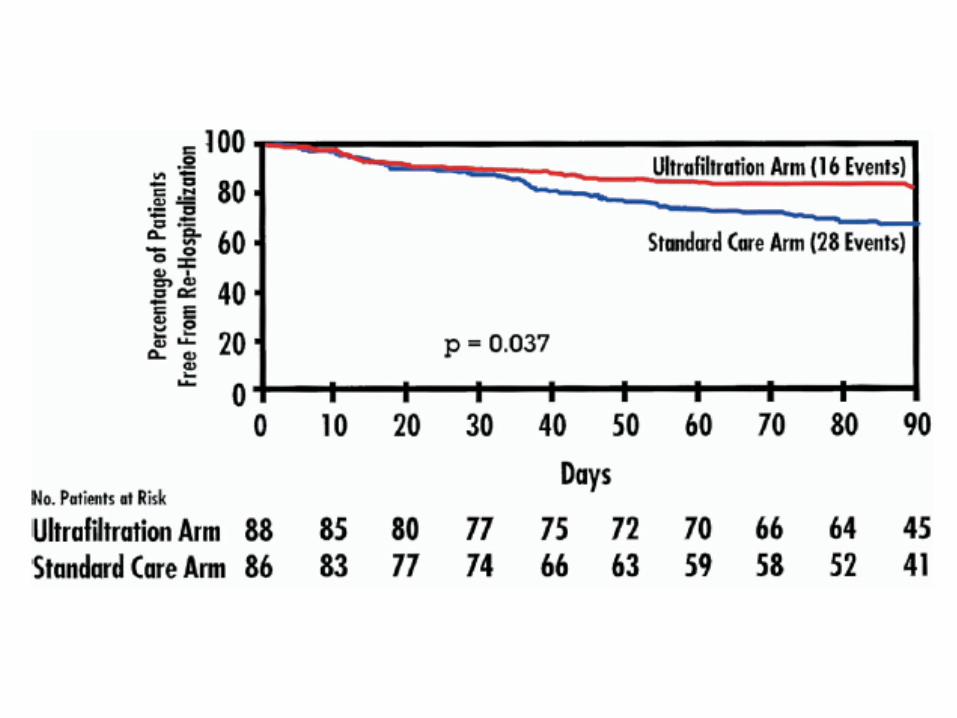
UNLOAD study
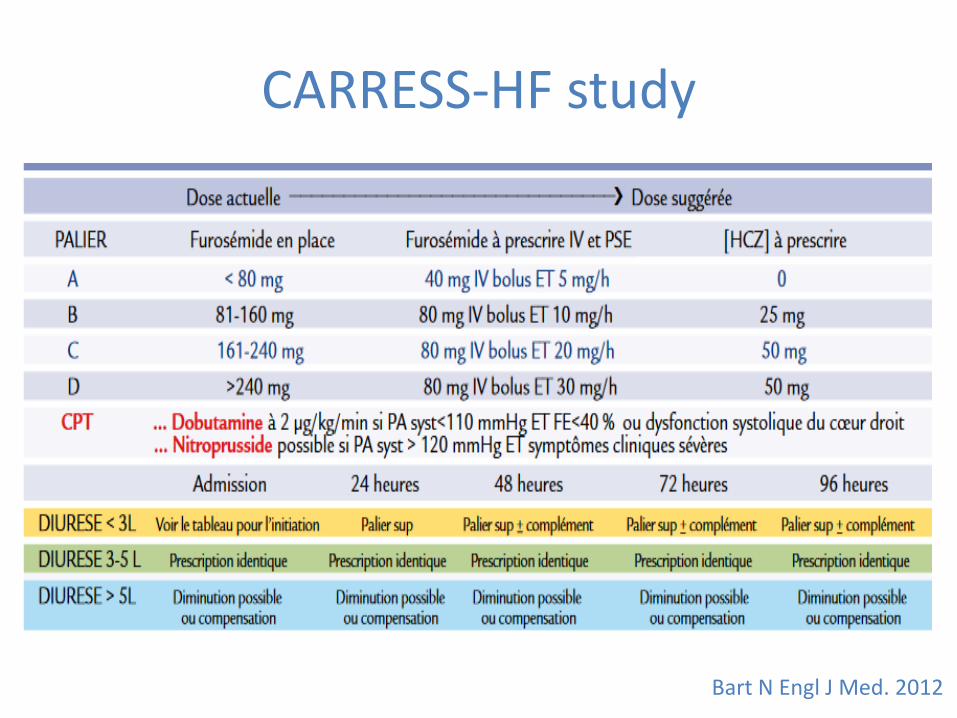
CARRESS-HF study
Bart N Engl J Med. 2012
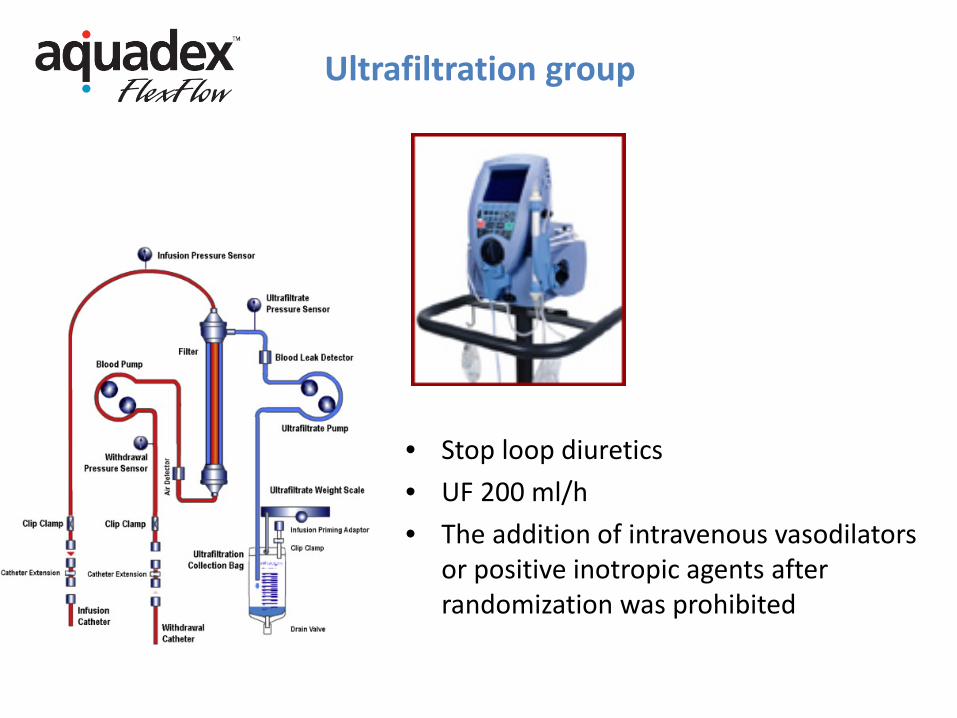
Ultrafiltration group
• Stop loop diuretics • UF 200 ml/h • The addition of intravenous vasodilators
or positive inotropic agents after randomization was prohibited
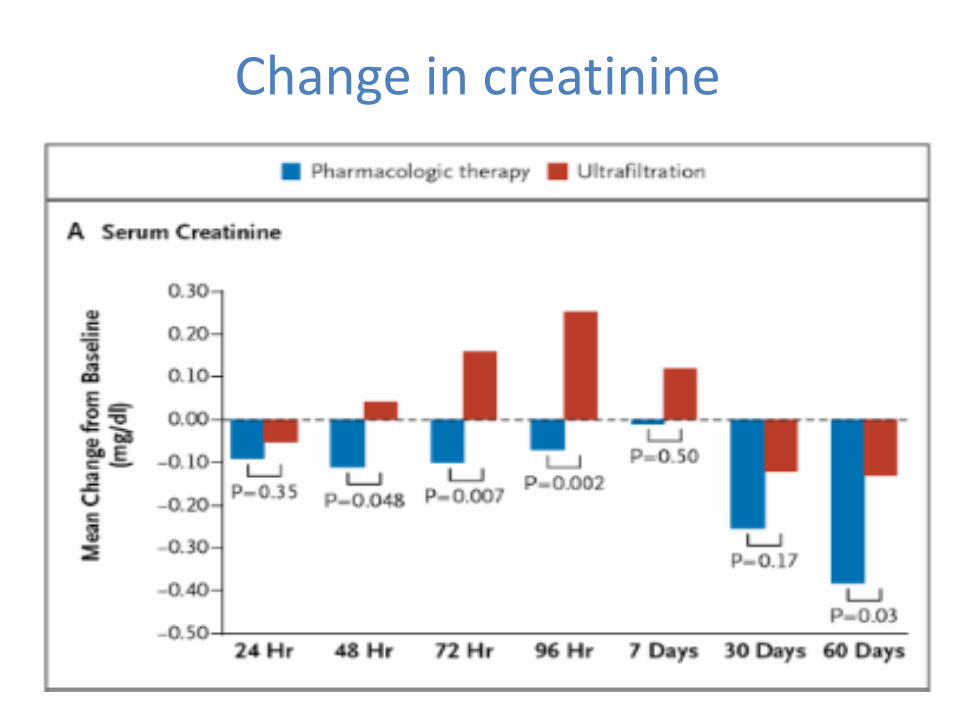
Change in creatinine
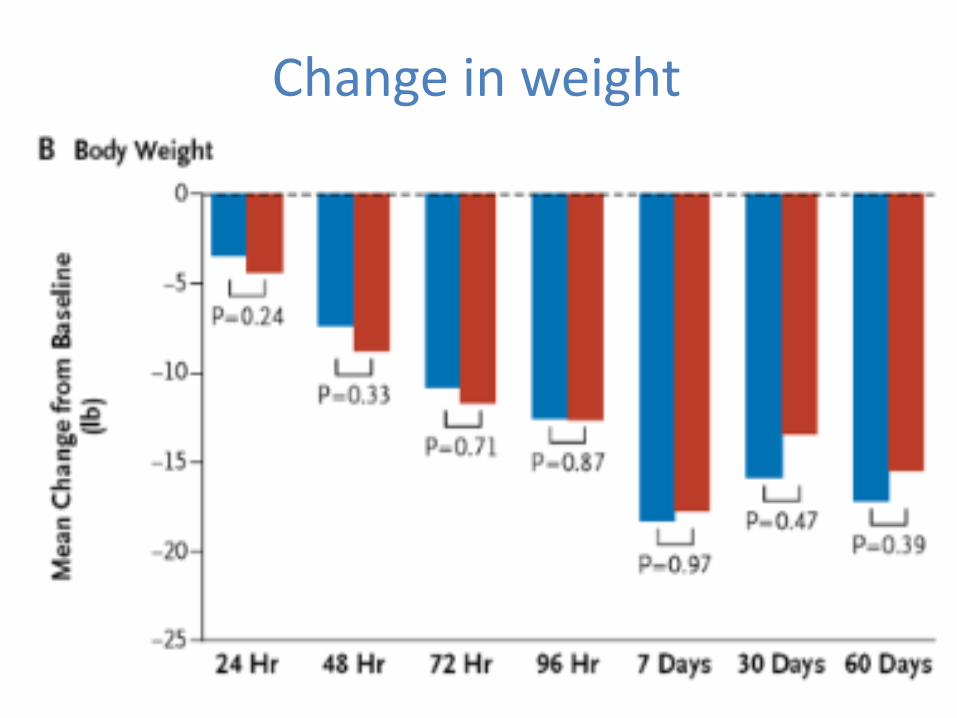
Change in weight
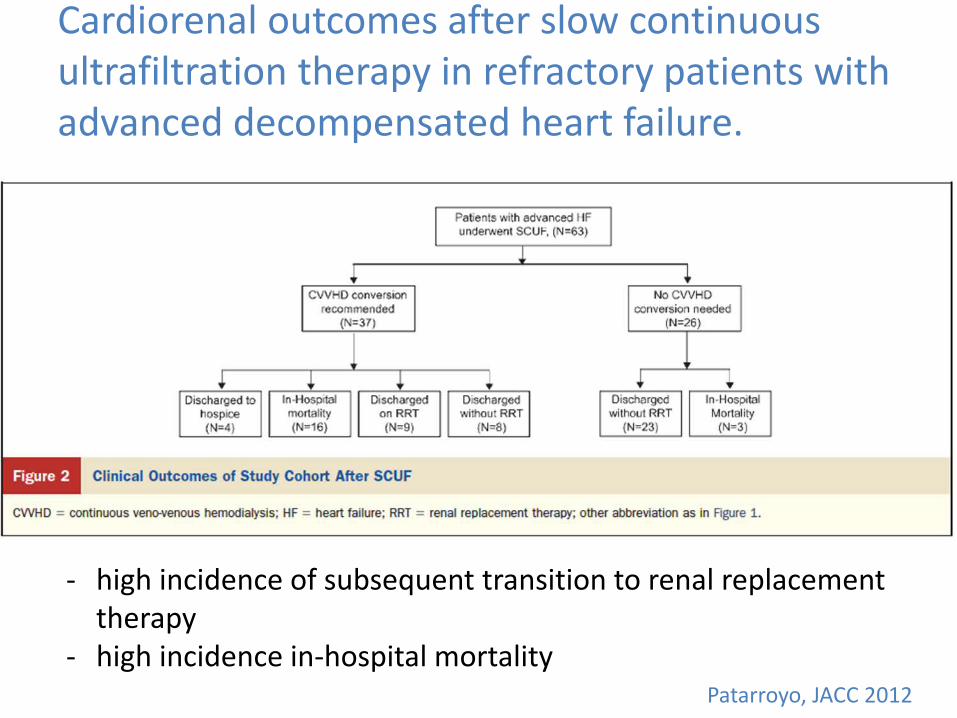
Cardiorenal outcomes after slow continuous ultrafiltration therapy in refractory patients with advanced decompensated heart failure.
- high incidence of subsequent transition to renal replacement therapy
- high incidence in-hospital mortality Patarroyo, JACC 2012
Continuous Ultrafiltration for Congestive
Heart Failure
Patients with congestive HF randomized to receive standard medical therapy or ultrafiltration - a lower incidence of rehospitalizations in the ultrafiltration
group - more stable renal function, unchanged furosemide dose,
and lower B-type natriuretic peptide levels - At 1 year, 7 deaths (30%) occurred in the ultrafiltration
group and 11 (44%) in the control group
Marenzi et al, JCF, 2014
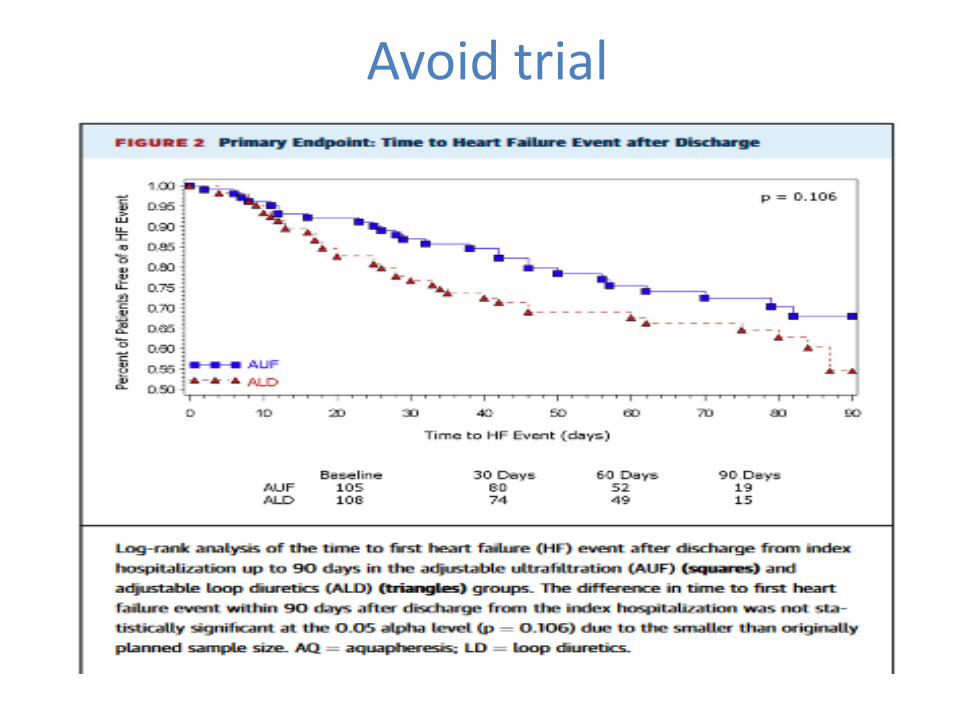
Avoid trial
Chronic cardiorenal syndrom and Ultrafiltration
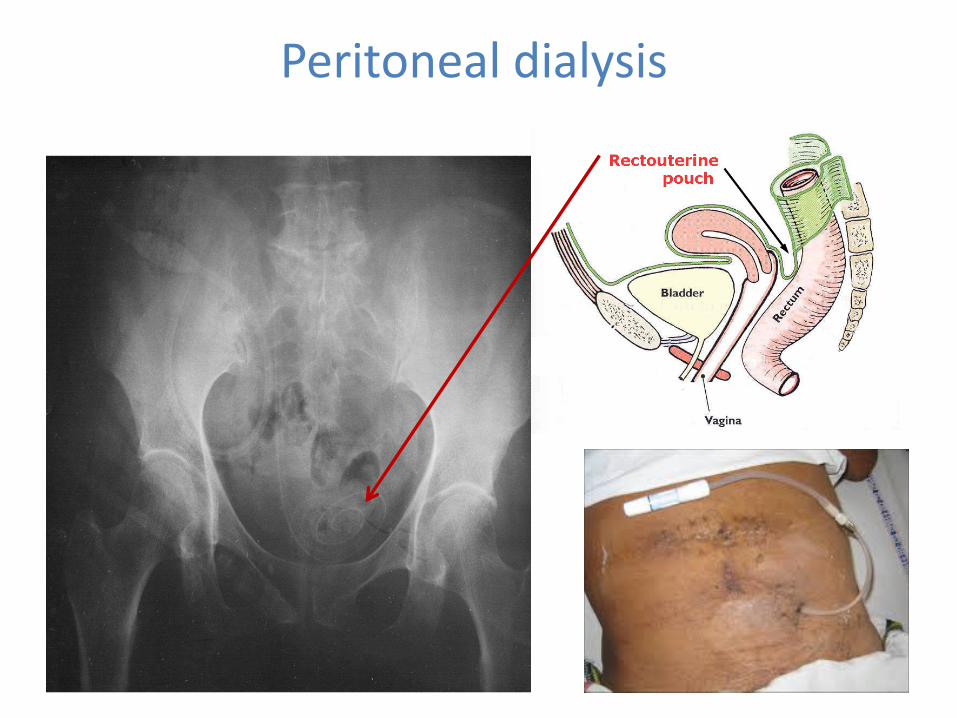
Peritoneal dialysis
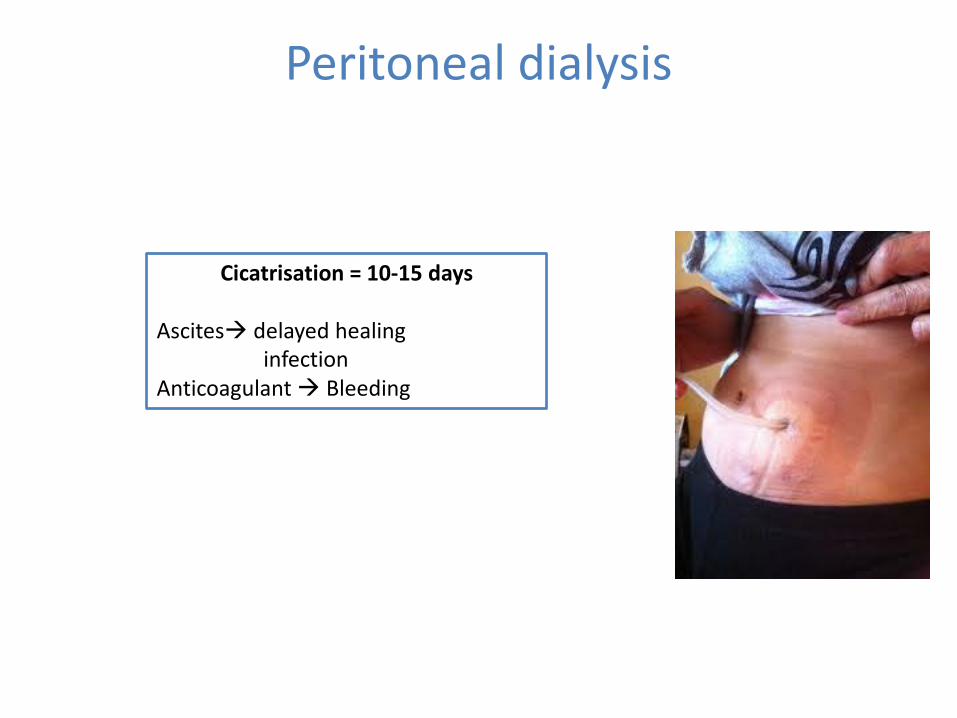
Cicatrisation = 10-15 days Ascites delayed healing infection Anticoagulant Bleeding
Peritoneal dialysis
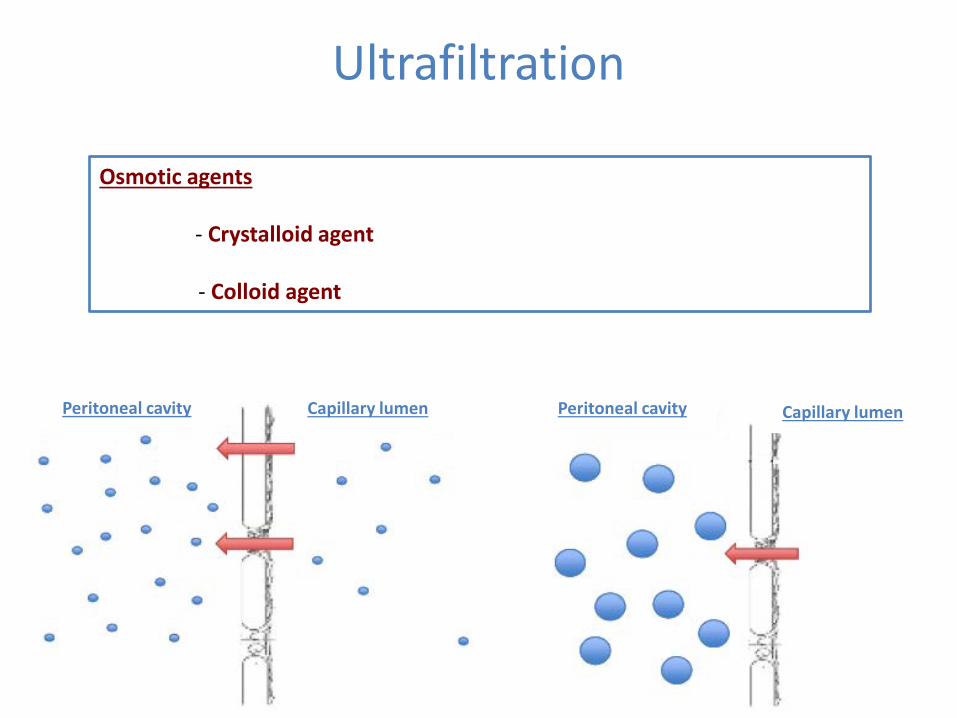
Ultrafiltration
Osmotic agents - Crystalloid agent - Colloid agent
Peritoneal cavity Capillary lumen Capillary lumen Peritoneal cavity
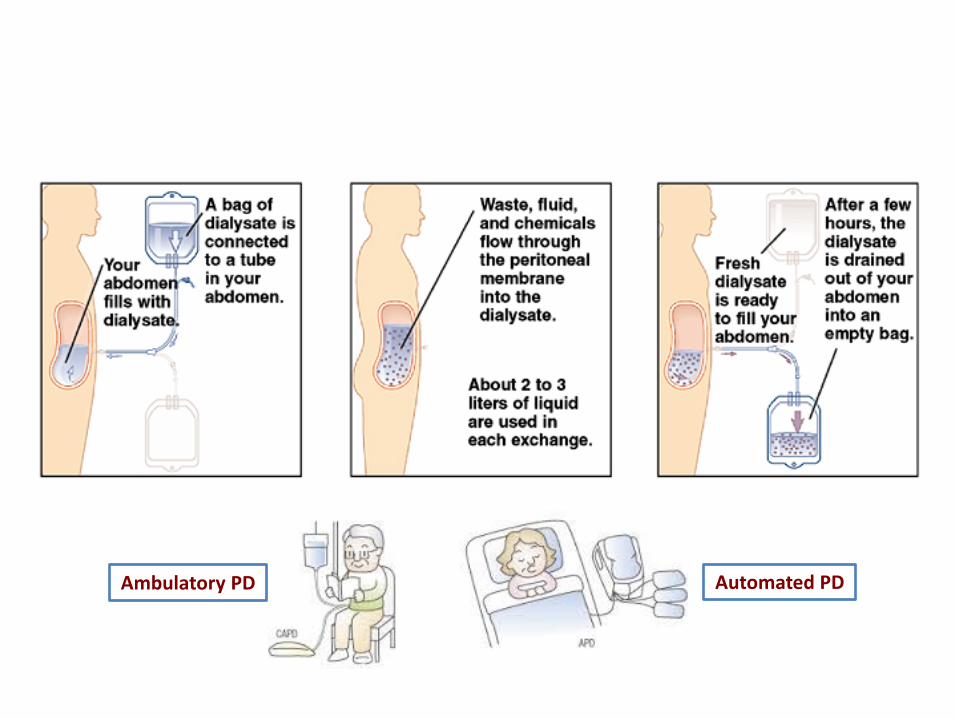
Ambulatory PD Automated PD
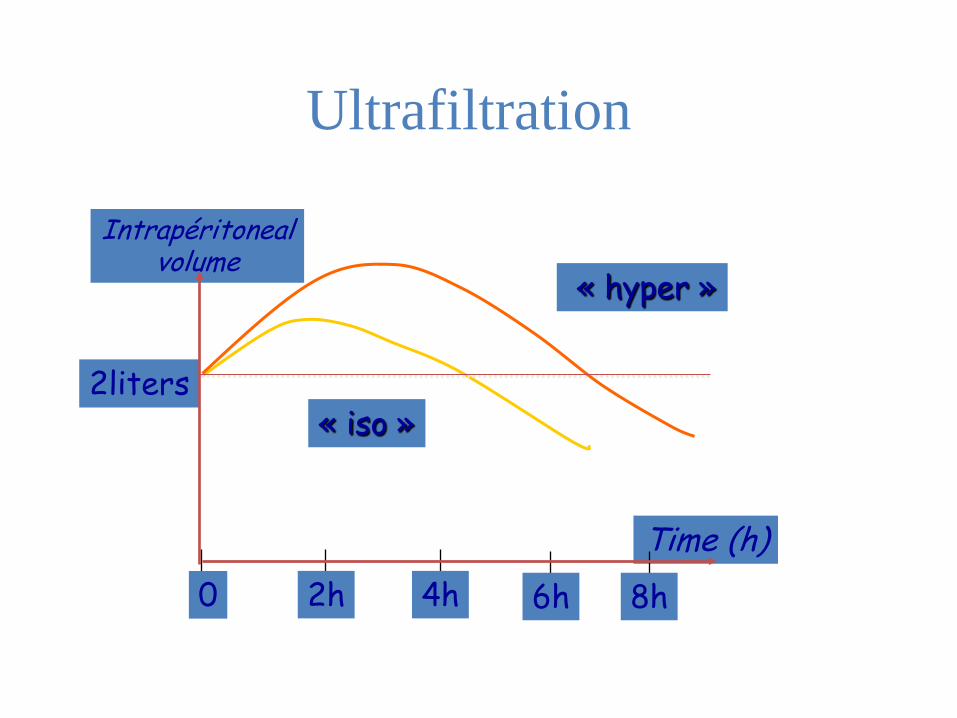
Ultrafiltration
Intrapéritoneal volume
Time (h) 0 2h 4h
« iso » 2liters
6h 8h
« hyper »
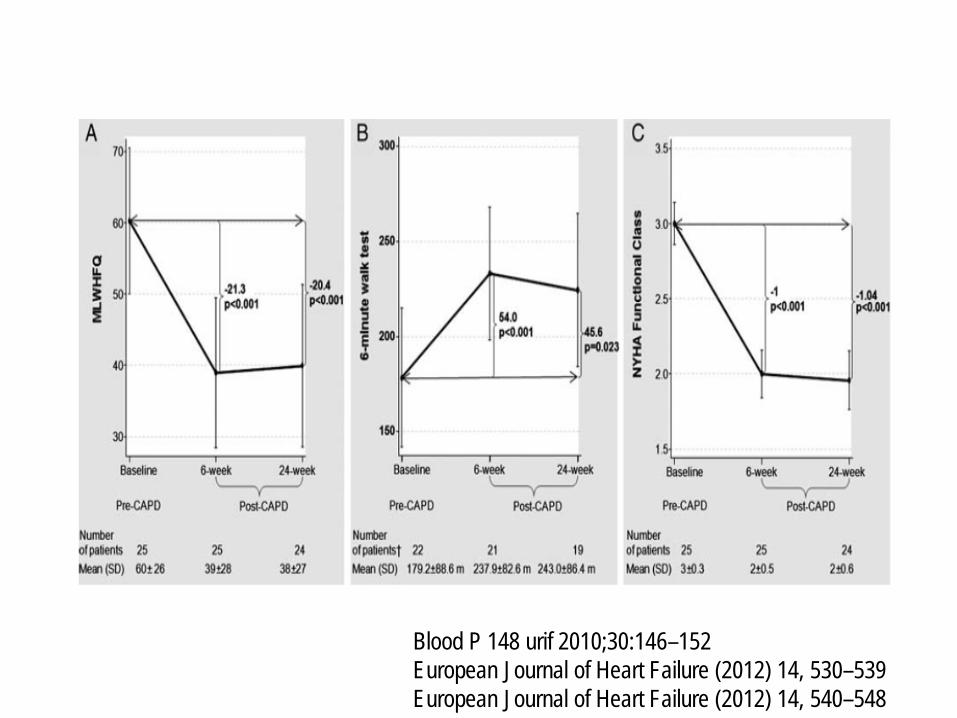
Blood P 148 urif 2010;30:146–152 European Journal of Heart Failure (2012) 14, 530–539 European Journal of Heart Failure (2012) 14, 540–548
• Hospitalizations Before: 3,3 ±2,6 days/patient/month After: 0,3 ±0,5 days/patient/month
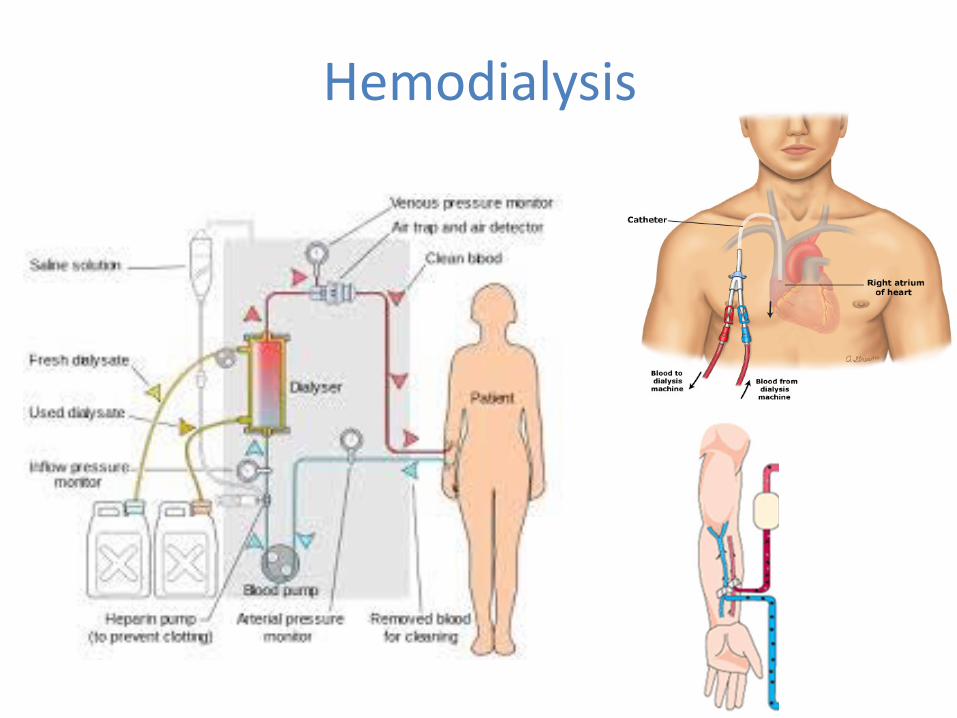
Hemodialysis
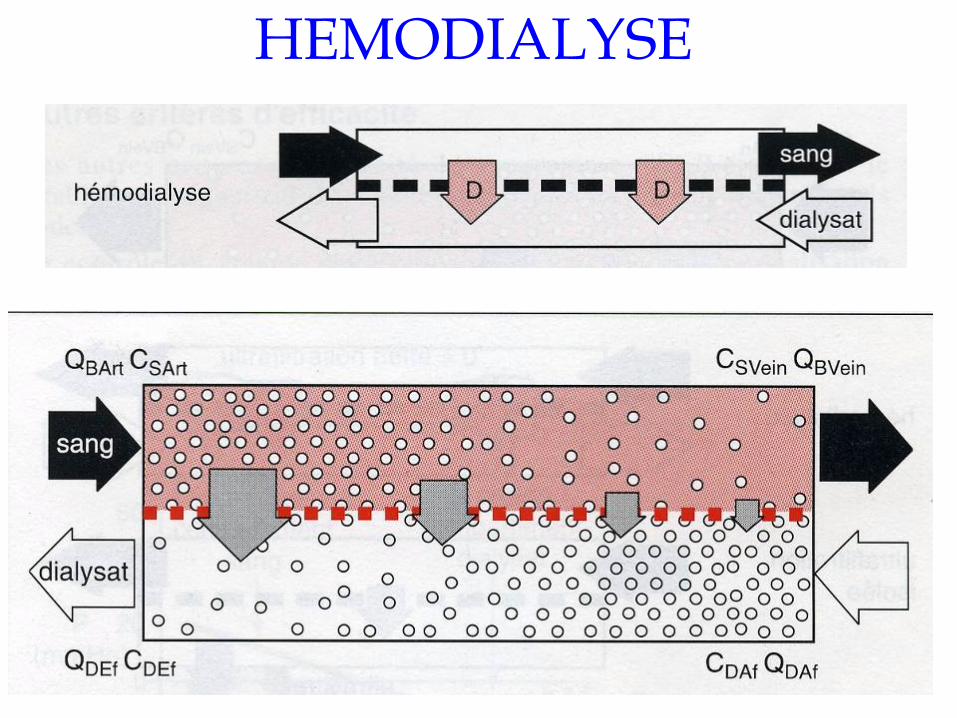
HEMODIALYSE
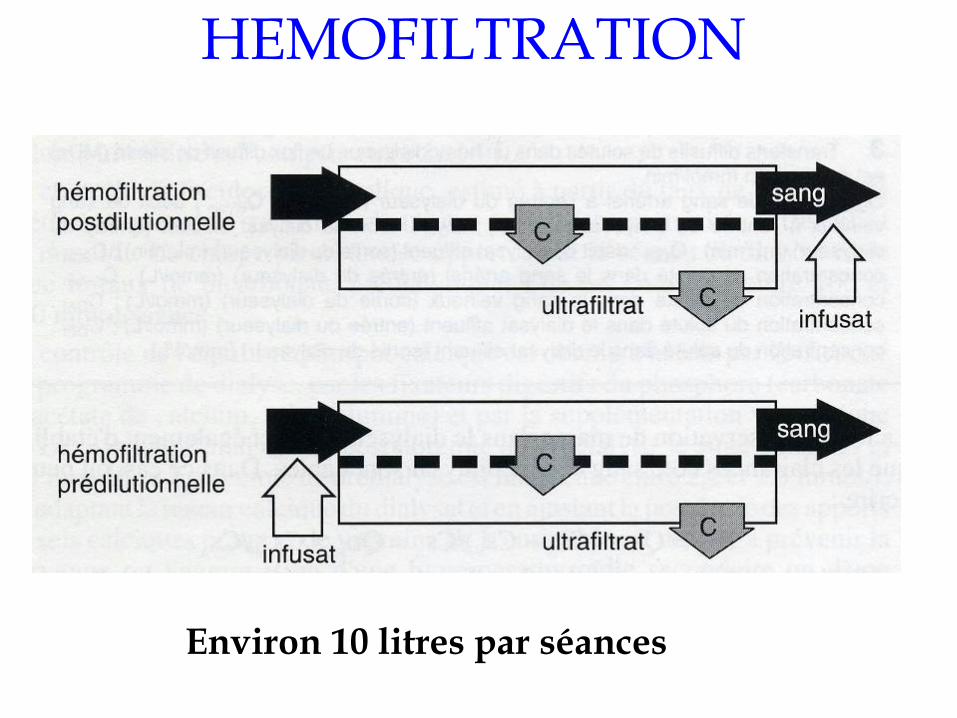
HEMOFILTRATION
Environ 10 litres par séances
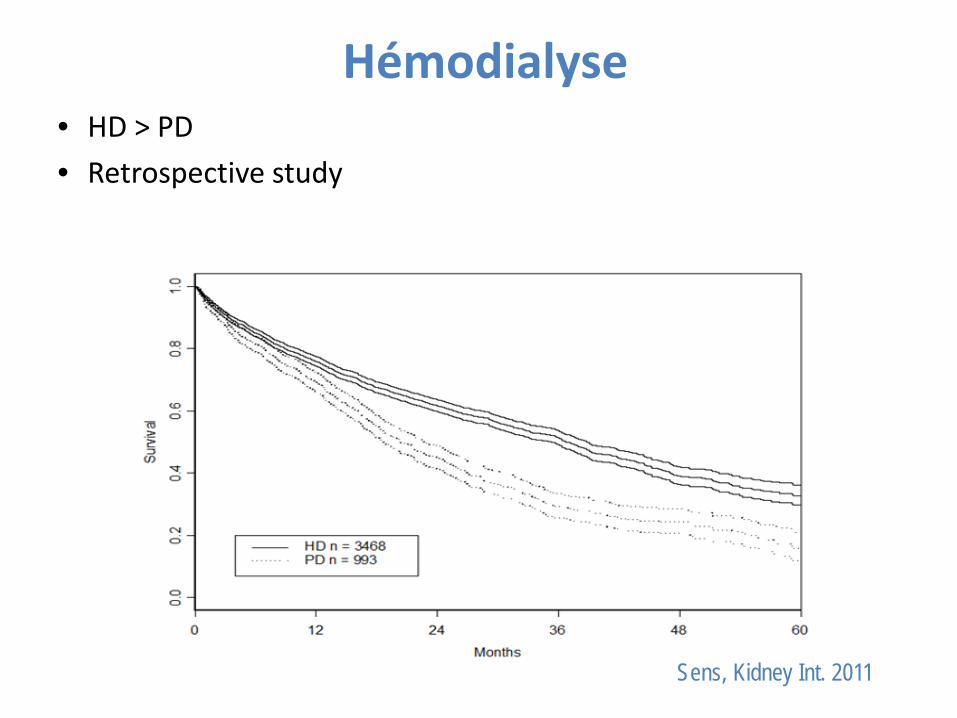
Hémodialyse • HD > PD • Retrospective study
Sens, Kidney Int. 2011

Experience in LYON
Cohorte Lyon-CARE
Nephrologists and cardiologists
Standardized evaluation
Information: prognosis, therapeutics and levels of evidence
Shared medical decision
Longitudinal follow-up
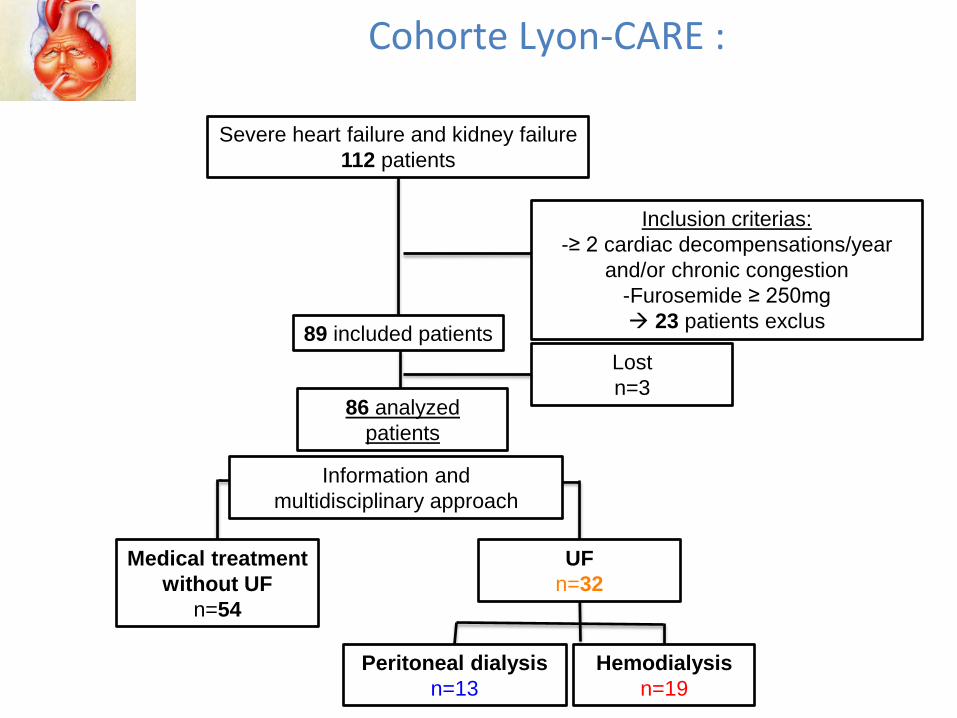
Lost n=3
Severe heart failure and kidney failure 112 patients
Inclusion criterias: -≥ 2 cardiac decompensations/year
and/or chronic congestion -Furosemide ≥ 250mg 23 patients exclus 89 included patients
86 analyzed patients
Medical treatment without UF
n=54
Information and multidisciplinary approach
UF n=32
Hemodialysis n=19
Peritoneal dialysis n=13
Cohorte Lyon-CARE :
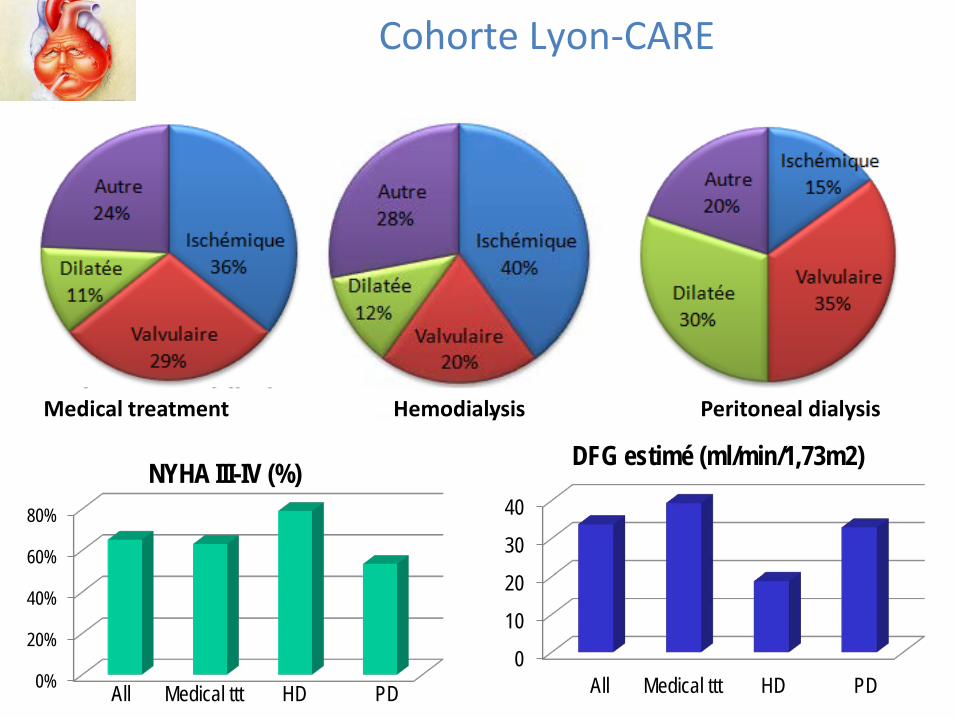
0%
20%
40%
60%
80%
NYHA III-IV (%)
All Medical ttt HD PD 0
10
20
30
40
DFG estimé (ml/min/1,73m2)
All Medical ttt HD PD
Cohorte Lyon-CARE
Medical treatment Hemodialysis Peritoneal dialysis
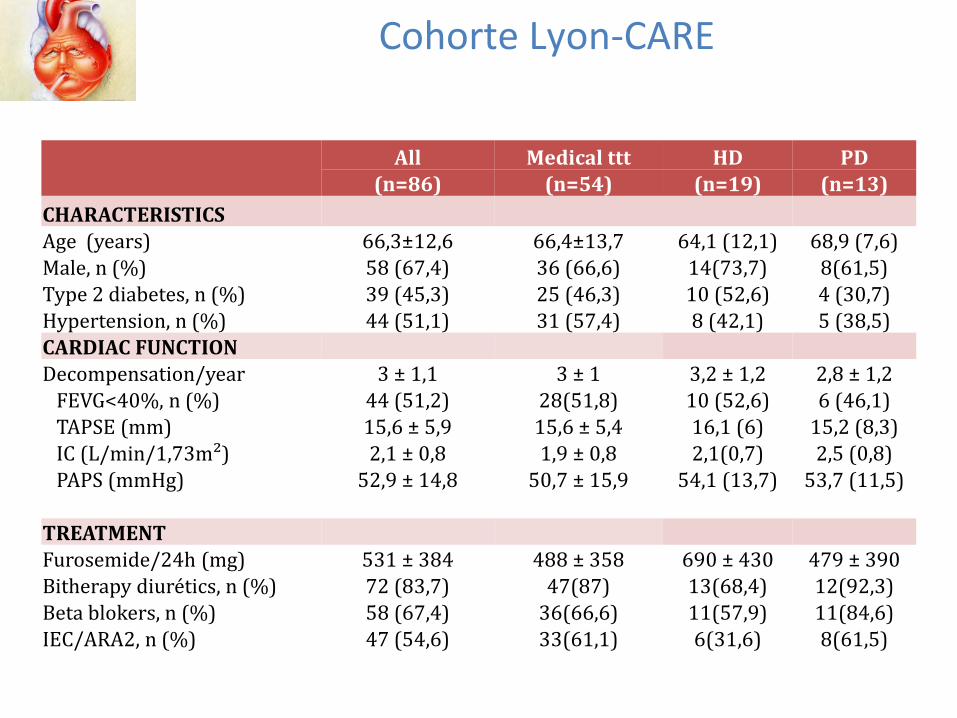
Cohorte Lyon-CARE
All Medical ttt HD PD (n=86) (n=54) (n=19) (n=13)
CHARACTERISTICS Age (years) 66,3±12,6 66,4±13,7 64,1 (12,1) 68,9 (7,6) Male, n (%) 58 (67,4) 36 (66,6) 14(73,7) 8(61,5) Type 2 diabetes, n (%) 39 (45,3) 25 (46,3) 10 (52,6) 4 (30,7) Hypertension, n (%) 44 (51,1) 31 (57,4) 8 (42,1) 5 (38,5) CARDIAC FUNCTION Decompensation/year 3 ± 1,1 3 ± 1 3,2 ± 1,2 2,8 ± 1,2 FEVG<40%, n (%) 44 (51,2) 28(51,8) 10 (52,6) 6 (46,1) TAPSE (mm) 15,6 ± 5,9 15,6 ± 5,4 16,1 (6) 15,2 (8,3) IC (L/min/1,73m²) 2,1 ± 0,8 1,9 ± 0,8 2,1(0,7) 2,5 (0,8) PAPS (mmHg) 52,9 ± 14,8 50,7 ± 15,9 54,1 (13,7) 53,7 (11,5)
TREATMENT Furosemide/24h (mg) 531 ± 384 488 ± 358 690 ± 430 479 ± 390 Bitherapy diurétics, n (%) 72 (83,7) 47(87) 13(68,4) 12(92,3) Beta blokers, n (%) 58 (67,4) 36(66,6) 11(57,9) 11(84,6) IEC/ARA2, n (%) 47 (54,6) 33(61,1) 6(31,6) 8(61,5)
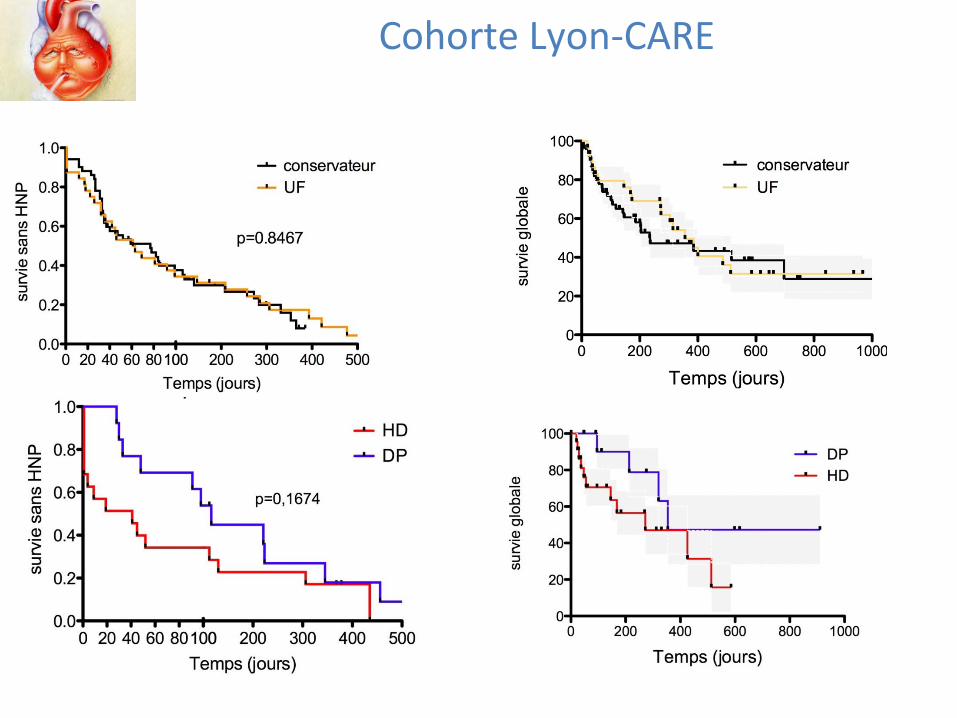
Cohorte Lyon-CARE
Ultrafiltration versus medical therapies in the
management of cardiorenal syndrome • Prospective, controlled, open, randomized,
multicentric trial • Primary outcome measure: death and/or
unscheduled hospitalizations • Secondary outcomes measures:
– Survival – Hospitalizations for acute decompensated heart
failure – Evolution to end stage renal disease – Cardiac parameters – Safety – Quality of life
UF-CARE
• Ultrafiltration – Peritoneal dialysis – Hemodialysis – Isolated ultrafiltration
• Enhanced medical treatment
UF-CARE • Inclusion criterias
– Severe heart failure with recurring congestive symptoms and at least one the following criteria :
• At least 2 hospitalizations during the 12 months before the inclusion, whose the latest one was in the 6 months before the inclusion
• Persistent congestive symptoms throughout 30 days before the randomization: dyspnea (class III or IV NYHA), lower limbs edema and/or ascites.
– Diuretic treatment with at least 250mg furosemide per day (or 6mg bumetamide per day)
– Cardiac medical treatment enhanced by the European cardiology society guidance (except intolerance, and/or contraindication)
– Non end stage kidney disease or kidney failure : estimated DFG (CKD-Epi formula) between 20 and 60 mL/min/1.73m² (or DFG estimated between 60 and 90 mL/min/1.73m² with proteinuria and/or hematuria) and urea rate under 50 mmol/L
Acknowledgments
• Dr Florence SENS • Dr Eric POULIQUEN • Pr Laurent JUILLARD • Pr Eric BONNEFOY


















