Cardiomyopathy.pptx2!5!13 3 Year Mbbs
155
DR ABDUL GHANI WASEEM
-
Upload
mannat-zaidi -
Category
Documents
-
view
218 -
download
0
Transcript of Cardiomyopathy.pptx2!5!13 3 Year Mbbs

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 1/155
DR ABDUL GHANI WASEEM

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 2/155
TYPES IDIOPATHIC DILATED CARDIOMYOPATHY

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 3/155

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 4/155
ETIOLOGIES OF DILATED CARDIOMYOPATHY
0
5
10
15
20
25
30
35
40
45
50
Disorder
IDCM
Myocarditis
Ischmic CM
InfiltrativediseasePeripartum CM
Hypertension
HIV
CTD
Substanceabuse
7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 5/155
IDIOPATHIC DILATED CARDIOMYOPATHY
PATHOLOGY
Four chamber dilatation
Mild to moderate ventricular hypertrophy
Varying degrees of interstitial fibrosis and
myocyte hypertrophy
“Functional” atrioventricular regurgitation is
common

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 6/155
IDIOPATHIC DILATED CARDIOMYOPATHYPATHOLOGIC FINDINGS

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 7/155
IDIOPATHIC DILATED CARDIOMYOPATHY
PATHOGENESIS Familial/genetic factors
Viral myocarditis and cytotoxic insults
Immunologic abnormalities Beta-receptor auto-antibodies
Abnormal T-cell function
Metabolic, energetic, and contractile
abnormalities Ca2+-ATPase
Myofibrillar ATPase
Creatine Kinase
7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 8/155
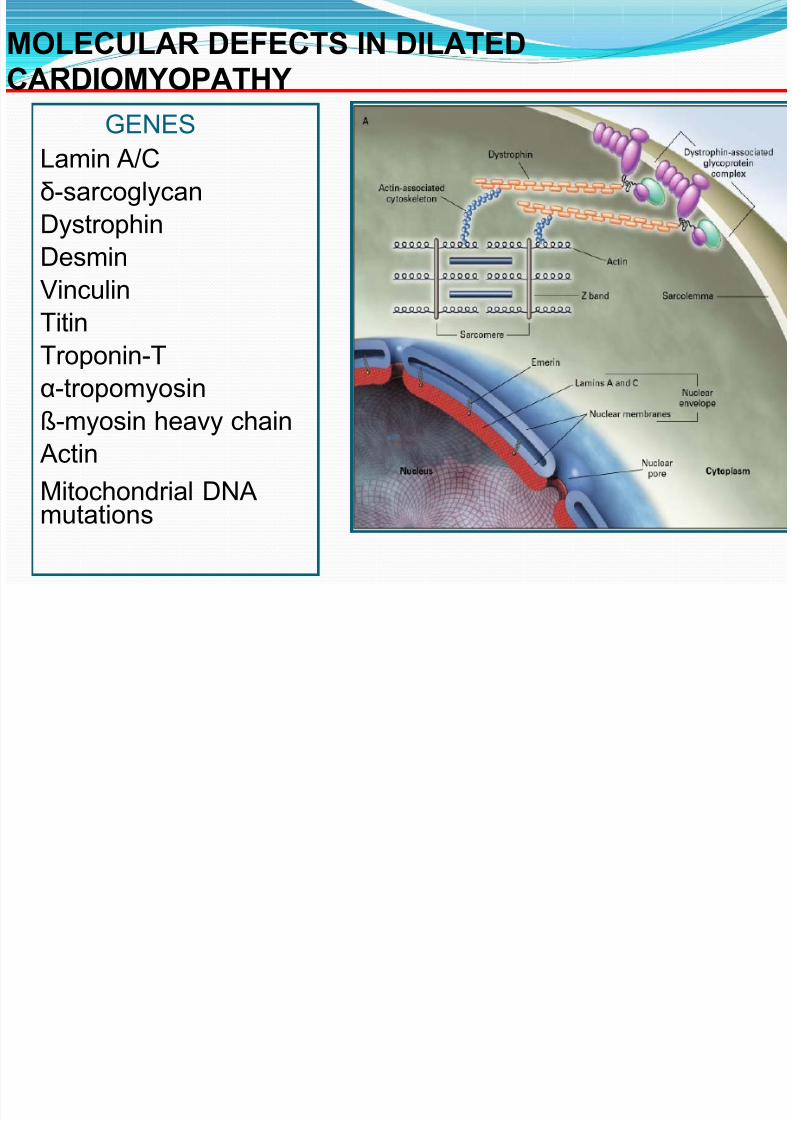
MOLECULAR DEFECTS IN DILATEDCARDIOMYOPATHY
GENESLamin A/C
δ-sarcoglycan
Dystrophin
Desmin
Vinculin
Titin
Troponin-T
α-tropomyosin
ß-myosin heavy chain
Actin
Mitochondrial DNAmutations

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 9/155
FAMILIAL DILATED CARDIOMYOPATHYCOMMON ASSOCIATED ABNORMALITIES
Conduction system disease
Skeletal muscle myopathy or muscular dystrophy
X-linked and autosomal dominant inheritancepatterns are most common
Extracardiac manifestations:
Sensorineural hearing loss Neutropenia

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 10/155
NON-INVASIVE EVALUATION OF MYOCARDITIS MRI IMAGING
Unenhanced Enhanced

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 11/155
IDIOPATHIC DILATED CARDIOMYPATHY
EPIDEMIOLOGY
ANNUAL INCIDENCE 5-8/100,000
PREVELANCE 36/ 100,000
INCREASED RISK ASSOCIATED WITH: MALE GENDER
BLACK RACE
HYPERTENSION
CHRONIC BETA-AGONIST USE

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 12/155
IDIOPATHIC DILATED CARDIOMYPATHY
CLINICAL PRESENTATIONS
Heart failure symptoms 75%-85%
Anginal chest pain 8%-20%
Emboli (systemic or pulmonary) 1%-4%
Syncope <1%
Sudden cardiac death <1%

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 13/155
SPONTANEOUS IMPROVEMENT IN ACUTE
DILATED CARDIOMYOPATHY
PATIENT POPULATION
49 patients with heart failure symptoms of lessthan 6 months duration were compared to a
cohort of 248 chronic dilated cardiomyopathypatients
Improvement was prospectively defined as a rise
in LVEF > 0.15 to a final value of > 0.30
-Steimle AE et al. JACC 1994;23:553-9
ACUTE DILATED CARDIOMYOPATHY

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 14/155
ACUTE DILATED CARDIOMYOPATHYOUTCOME
49 Patients with Recent Onset Cardiomyopathy
12 Died/10 Tx 16 Alive & Unimproved 11 Improved
18 Died/13 Tx 5 Alive & Unimproved 13 Improved
11±15 mos 27 ± 22 mos 43 ± 29 mos
12 months
Steimle et al JACC 1994;23:553-9
2 9 5
9

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 15/155
SPONTANEOUS IMPROVEMENT IN ACUTE
DILATED CARDIOMYOPATHY
UNIVARIATE PREDICTORS OF IMPROVEMENTshort duration of symptomshigher cardiac outputlower NYHA functional classificationsmaller LV end-diastolic dimensionlower filling pressures
higher serum sodium concentration
STEPWISE REGRESSION MODELshort duration of symptomshigher serum sodium concentrationlower right atrial pressure
lower pulmonary capillary wedge pressure
IDCM PROGNOSTIC FEATURES

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 16/155
IDCM:PROGNOSTIC FEATURES
VENTRICULOGRAPHIC FINDINGS
Degree of impairment in LVEF Extent of left ventricular enlargement
Coexistent right ventricular dysfunction
Ventricular mass/volume ratio
Global wall motion abnormalities
Left ventricular sphericity
CLINICAL FINDINGS
Favorable prognosis: NYHA < IV, younger age, femalesex
Poor prognosis: Syncope, persistent S3 gallop, right-sided heart failure, AV or bundle branch block,hyponatremia, troponin elevation, increased BNP,maximum oxygen uptake < 12 mg/kg/min

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 17/155
ACC/AHA HEART FAILURE EVALUATION GUIDELINES
CLASS I & II RECOMMENDATIONS
Laboratory Studies
Blood count, urinalysis, electrolytes, renal function,glucose, LFTs (class I; level C)
Thyroid stimulating hormone (class I; level C)
Fe/TIBC, ferritin (class IIa, level C)
Urinary screening for hemochromatosis (class IIa; level C) Measurement of ANA, rheumatoid factor, urinary VMA and
metanepherines in selected patients (class IIa; level C)
HIV testing (class IIb; level C)
Electrocardiogram (class I; level C)
Chest x-ray (class I; level C)

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 18/155
DILATED CARDIOMYOPATHYELECTROCARDIOGRAPHIC FINDINGS
Disease Etiology Pathologic Q-waves
Ischemic cardiomyopathy 10/12 (83%)*
(n=15)
Idiopathic cardiomyopathy 2/21 (10%)+ #
(n=21)
*LBBB (n=2); paced rhythm (n=1)
+ LVH (n=10);
IVCD (n=3)# P < 0.003

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 19/155
SEGMENTAL WALL MOTION ABNORMALITIES INDILATED CARDIOMYOPATHY
Regional wall motion abnormalities observed in at least50% of patients with non-ischemic causes of dilatedcardiomyopathy
Most frequent wall motion abnormalities: anterior wall & apex
Posterior and lateral walls most likely to be preserved
Type of abnormality: hypokinesis (83%) akinesis (11%)
dyskinesis (6%)
Heterogeneity in regional oxidative metabolism using C-11acetate clearance has been demonstrated in DCM

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 20/155
NONINVASIVE ASSESSMENT OF CORONARY ARTERY
DISEASE IN NEW ONSET DILATED CARDIOMYOPATHY
Retrospective studies have shown up to 94% of patientswith idiopathic dilated cardiomyopathy will havemyocardial perfusion defects Reversible defect(s): 60%
Fixed defect(s): 15%
Reversible+ fixed defect(s): 25%
Global myocardial blood flow reserve (dipyridamole-induced) is diminished in DCM patients compared tocontrols using PET imaging
Low myocardial blood flow reserve correlates with highleft ventricular wall stress and anaerobic metabolism
Ann Inter Med 1992;152:679-72; JACC 2000;35:19-28.

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 21/155
INDICATIONS FOR CORONARY ANGIOGRAPHY IN NEW
ONSET CARDIOMYOPATHYACC/AHA CONSENSUS GUIDELINES (2001)
Patients with Known Coronary Artery Disease/Angina Pectoris
Revascularization recommended in vast majority of such individuals
with multivessel disease. Little role for non-invasive testing.
Coronary angiography considered Class I Recommendation (Level of
evidence: B)
Patients with Known Coronary Artery Disease Who Lack Angina
No controlled trials have examined whether coronary revascularization
can improve outcomes in this population
Many centers first evaluate patient for myocardial hibernation
Coronary angiography considered Class IIa Recommendation (Level of
Evidence:C)
Patients with or without Chest Pain in Whom Coronary Artery
Disease has Not Been Evaluated
Approximately 35% of patients with IDCM will report angina-like pain
Coronary angiography should be considered Class IIa recommendation
(Level of Evidence: C)
Hunt SA,et al. Circulation 2001;104:2996
ENDOMYOCARDIAL BIOPSY IN DILATED CARDIOMYOPATHY

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 22/155
RIGHT
VENTRICULAR
BIOPSY
TECHNIQUE
ENDOMYOCARDIAL BIOPSY IN DILATED CARDIOMYOPATHY
7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 23/155
INDICATIONS FOR ENDOMYOCARDIALBIOPSY
Acute dilated cardiomyopathy with refractory heart failuresymptoms
Rapidly progressive ventricular dysfunction in an unexplainedcardiomyopathy of recent onset
New onset cardiomyopathy with recurrent ventricular tachycardia or high grade heart block
Heart failure in the setting of fever, rash, and peripheraleosinophilia
Dilated cardiomyopathy in setting of systemic diseases
known to affect the myocardium (systemic lupus erythematosus,polymyositis, sarcoidosis)
Wu LA, et al. Mayo Clin Proc 2001;76:1030-8

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 24/155
SURVIVAL BY HISTOPATHOLOGICAL TYPE OFMYOCARDITIS
CP977755-6
0.0
0.2
0.4
0.6
0.8
1.0
0 1 2 3 4 5
Survival (yr)
P
r o p o r t i o n s
u r v i v i n g
GCM group
LM group
Cooper, et al NEJM 1997

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 25/155
DILATED CARDIOMYOPATHY PROVEN THERAPEUTIC OPTIONS
TREATMENT INDICATIONS
ACE Inhibitors Symptomatic heart failure andasymptomatic LV dysfunction
ARBs ACE intolerance
Hydralazine- nitrates ACE intolerance
Diuretics Volume overloadPotassium/Magnesium Diuretic-induced depletion
Beta-blockers Symptomatic heart failure in addition to ACE inhibitor
Digoxin Persistent heart failure despitediuretics, ACE inhibitor
Warfarin Chronic or paroxysmal atrial fibrillation
LV thrombus or prior embolic event
ICD Cardiac arrest; uncontrolled VT

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 26/155
STATIN THERAPY IMPROVES VENTRICULAR
FUNCTION IN DILATED CARDIOMYOPATHY
Node K, et al. Circulation 2003;108:839-43

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 27/155
CONTROLLED TRIAL OF IMMUNE GLOBULIN IN
RECENT ONSET DILATED CARDIOMYOPATHY
Purpose: To determine whether intravenous immunoglobulin G
(IVIG) improves ejection fraction in adults with recent onset
idiopathic dilated cardiomyopathy or myocarditis
Methods: 62 patients with symptomatic DCM < 6 months and
LVEF < 40% were randomized to receive IVIG 2 g/kg or placebo
Study Population:
Age (mean) 43 ± 12 yrs
LVEF 25 ± 8%
Symptom duration 2.0 ± 1.5 months
Myocarditis 16%
McNamara et al. Circulation 2001;103:2254-9

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 28/155
IMMUNOGLOBULIN THERAPY FOR ACUTE DILATEDCARDIOMYOPATHY:IMAC TRIAL RESULTS
McNamara et al. Circulation 2001;103:2254-9
IMMUNOADSORPTION THERAPY FOR DILATED

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 29/155
IMMUNOADSORPTION THERAPY FOR DILATED
CARDIOMYOPATHY
12 MONTH AUTOANTIBODY LEVELS BY TREATMENT
GROUP
Muller J et al. Circulation 2000;101: 385 - 391
IMMUNOADSORPTION THERAPY FOR DILATED

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 30/155
IMMUNOADSORPTION THERAPY FOR DILATEDCARDIOMYOPATHY12 MONTH CHANGE IN EJECTION FRACTION BY TREATMENT
GROUP
Muller J et al. Circulation 2000;101: 385 - 391

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 31/155
EFFECT OF REMOVAL OF ANTIBODIES BYIMMUNOADSORPTION IN DILATED CARDIOMYOPATHY
Felix SB, et al. JACC 2002;39:646-52
n=12
Effect of
column
effluent on
adult rat
cardiocyte
contractility
CONTROLLED TRIAL OF IMMUNOADSORPTION AND

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 32/155
CONTROLLED TRIAL OF IMMUNOADSORPTION AND
IMMUNOGLOBULIN SUBSTITUTION IN DILATEDCARDIOMYOPATHY
Hypothesis: Immunomodulatory therapy may decreasemyocardial inflammation and improve ventricular systolicfunction
Methods: 25 patients with DCM were randomized toimmunoabsorption (IA) followed by IgG (0.5 gm/kg)
replacement for 3 consecutive months (n=12) or conventional therapy (n=13):
Age: 50 ± 11 years
LVEF: 20% ± 6%
Symptom Duration: 4.0 yearsFibrosis: 8.7%
Primary End-points: Change in LVEF (3 month)
Change in CD3+, CD4+ & CD8+ cells
Staudt A et al. Circulation 2001;103:2681-8

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 33/155
IMMUNOABSORPTION AND REPLACEMENT
TREATMENT FOR DILATED CARDIOMYOPATHYCHANGES IN CELLULAR INFILTRATION (3 mon ths )
Staudt A et al. Circulation 2001;103:2681-8
IA/IgG treatment
resulted in a
significant declinein all subtypes of
infiltrating
lymphocytes
** p < 0.05 vs baseline
++ p < 0.05 vs controls
7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 34/155
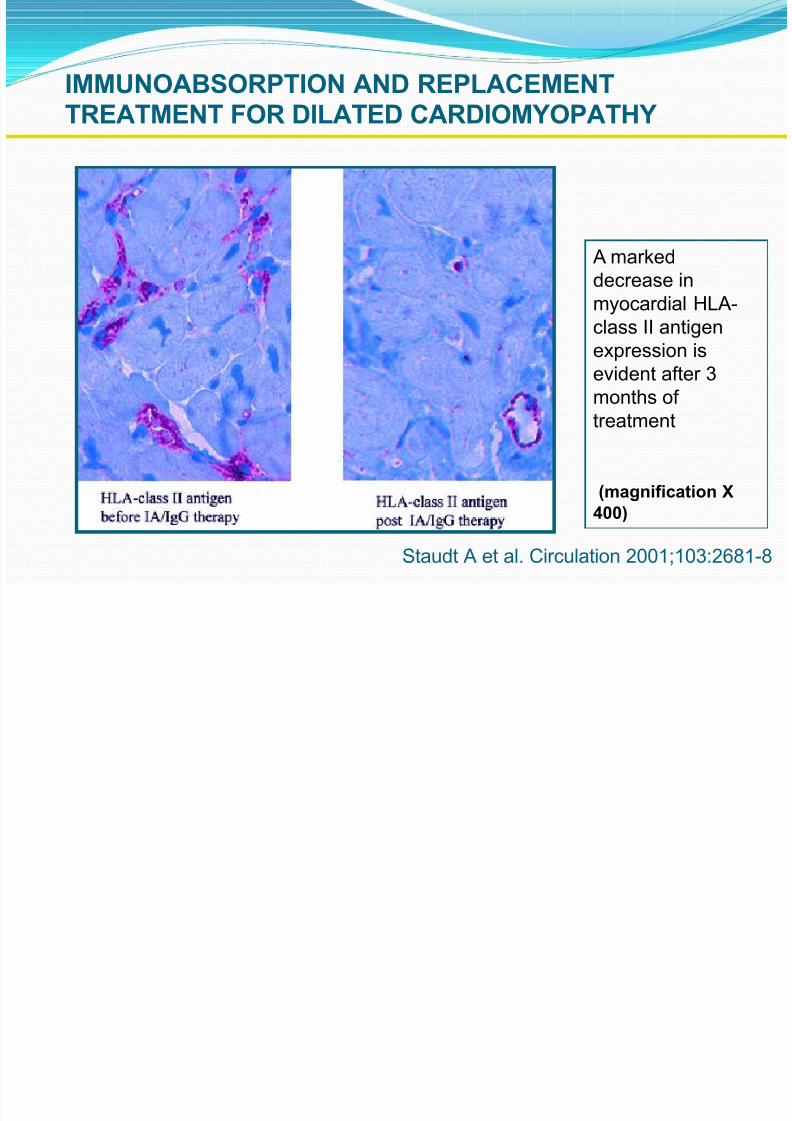
IMMUNOABSORPTION AND REPLACEMENTTREATMENT FOR DILATED CARDIOMYOPATHY
Staudt A et al. Circulation 2001;103:2681-8
A marked
decrease inmyocardial HLA-
class II antigen
expression is
evident after 3
months of
treatment
(magnification X
400)

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 35/155
CONTROLLED TRIAL OF IMMUNOADSORPTION AND
IMMUNOGLOBULIN SUBSTITUTION IN DILATED CARDIOMYOPATHY
CHANGE IN LEFT VENTRICULAR FUNCTION (3 Months)
**p <0.05 vs baseline
++p < 0.01vs controls
Staudt A et al. Circulation 2001;103:2681-8

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 36/155
IMMUNOSUPPRESSIVE THERAPY FORINFLAMMATORY DILATED CARDIOMYOPATHY
Purpose: To assess the efficacy of immunosuppressive therapy in patients
with dilated cardiomyopathy and HLA up-regulation on biopsy.
Study Population: 84 (of 202 DCM) patients had HLA class I or II
expression on myocytes, endothelium or interstitial cells and were
randomized to 24 months of conventional therapy [ digoxin, furosemide,spironolactone, ACE inhibitor, beta-blocker, nitrates, and amiodarone]
alone or with concomitant immunosuppression [ prednisone 1mg/kg/day
taper to 0.2 mg/kg/day for 90 days + azathioprine 1 mg/kg/day for 100
days].
Primary Endpoint: Death, transplantation or hospital readmission
Secondary Endpoints: LVEF, LVEDD, LVESD, NYHA class
Wojnicz R, et al. Circulation 2001;104:39-45
IMMUNOSUPPRESSIVE THERAPY FOR DILATED

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 37/155
IMMUNOSUPPRESSIVE THERAPY FOR DILATED
CARDIOMYOPATHYCHANGE IN VENTRICULAR FUNCTION
0%
5%10%
15%
20%
25%
30%
35%
40%
45%
Baseline 3 Month 6 Month 12 Month 24 Month
Placebo
Immuno
Left Ventricular Ejection Fraction
Wojnicz R, et al. Circulation 2001;104:39-45
7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 38/155
ALIAN UNCONTROLLED IMMUNOSUPPRESSIVE TRIAL
R MYOCARDITIS
112 patients had biopsy-proven lymphocytic myocarditis41 patients had progressive symptoms for > 3 months
duration and were treated with 6 months with
prednisone (1 mg/kg/day x 4 wks; 0.33 mg/kg/day x 5 months)
and azathioprine (2 mg/kg/day x 6 months)
Efficacy of therapy was evaluated at 6 & 12 months
Responders demonstrated:Decrease in NYHA class
Increase in LVEF > 10 Units
Frustaci A, et al. Circulation 2003;107:857-63

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 39/155
ITALIAN UNCONTROLLED TRIAL OF IMMUNOSUPPRESSIVE
THERAPY FOR MYOCARDITIS
0.00%
10.00%
20.00%
30.00%
40.00%
50.00%
LVEF
1 2 3
Frustaci A, et al. Circulation 2003;107:857-63
BASELINE 6 MO 12 MO
RRR

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 40/155
IMMUNOSUPPRESSIVE THERAPY FOR MYOCARDITIS
STUDY DESIGN
RESPONDERS NON-RESPONDERS(N=21) (N=20)
Frustaci A, et al. Circulation 2003;107:857-63
Viral Genome 3 (14%) * 17 (85%) +
Cardiac Antibodies 19 (90%)# 0 (0%)
* P < 0.001; # p < 0.001
+ Enterovirus 5; EB virus 5; adenovirus 4; influenza
1; parvovirus 1

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 41/155
TREATMENT FOR IDIOPATHIC DILATED
CARDIOMYOPATHY
2004 AND BEYOND
Conventional neurohormonal antagonists
? Anticoagulation (WATCH; WARCEF)
? ICD implantation (DEFINITE & SCD-HeFT)
? Immunosuppression vs immunomodulation
Gene therapy (SERCA2a, phospholamban)
Cellular transplantation
Fetal cardiomyocytes Skeletal myoblasts
Adult (tissue) stem cells
Embryonic stem cells
IMAC TRIAL RESULT:APOPTOSIS AND

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 42/155
668N =
Fas gene expression
HighModerateLow
50.0
40.0
30.0
20.0
10.0
0.0
-10.0
-20.0
668N =
Fas gene expression
HighModerateLow
40.0
30.0
20.0
10.0
0.0
-10.0
Fas Expression and LV Recovery
p=0.002 p=0.006
Six months Twelve months
Sheppard, AHA 2003
IMAC TRIAL RESULT:APOPTOSIS AND
RECOVERY OF VENTRICULAR FUNCTION

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 43/155

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 44/155
Hypertrophic Cardiomyopathy

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 45/155
Definition WHO
Left and/or Right ventricular hypertrophy, usually asymmetric and involves the interventricular septum.

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 46/155
Differential Diagnosis:
HCM
Can be asymmetric
Wall thickness: > 15 mm
LA: > 40 mm
LVEDD : < 45 mm
Diastolic function: always
abnormal
Athletic heart
Concentric & regresses
< 15 mm
< 40 mm
> 45 mm
Normal

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 47/155
Stimulus Unknown
Disorder of intracellular calcium metabolism
Neural crest disorder
Papillary muscle malpositioned and misoriented

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 48/155
Genetic abnormality Autosomal dominant.
Mutations in genes for cardiac sarcomeric proteins.
Polymorphism of ACE gene.
ß-myosin heavy chain gene on chromosome 14.

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 49/155
Variants of HCM
Most common location: subaortic , septal, and ant. wall.
Asymmetric hypertrophy (septum and ant. wall): 70 %.
Basal septal hypertrophy: 15- 20 %.
Concentric LVH: 8-10 %.
Apical or lateral wall: < 2 % (25 % in Japan/Asia):characteristic giant T-wave inversion laterally & spade-like left ventricular cavity: more benign.

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 50/155

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 51/155
Hypertensive hypertrophic Cardiomyopathy
Elderly women
Simulates HCM
Prognosis better than non-hypertensive HCM

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 52/155
Pathophysiology of HCM Dynamic LV outflow tract obstruction
Diastolic dysfunction
Myocardial ischemia Mitral regurgitation
Arrhythmias

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 53/155
Left ventricular outflow tract gradient
↑ with decreased preload, decreased afterload, orincreased contractility.
Venturi effect: anterior mitral valve leaflets & chordaesucked into outflow tract→
↑ obstruction, eccentric jet of MR in mid-late systole.

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 54/155
Maneuvers that ↓ end-diastolic volume
(↓ venous return & afterload, ↑ contractility)
Vasodilators
Inotropes
Dehydration
Valsalva
Amyl nitrite Exercise
→ ↑HCM murmur

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 55/155

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 56/155
Arrhythmias:
Sustained V-Tach and V-Fib: most likely mechanism of syncope/ sudden death.
Dependant on atrial kick: CO ↓ by 40 % if A. Fibpresent.

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 57/155
Histology: Myocardial fiber disarray, endocardial plaques.
Abnormal relaxation and diversely orientedmyocardial fibers.
Intimal hyperplasia of intramural coronary arteries,endothelial dysfunction, myocardial perfusion defects.

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 58/155
Clinical presentation: Any age
Leading cause of sudden death in competitive athletes
Triad: DOE, angina, presyncope/syncope.

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 59/155

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 60/155

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 61/155
Physical exam: Apex localized, sustained
Palpable S4
Tripple ripple
Prominent “a” wave
Rapid upstroke carotid pulse, “jerky” bifid (spike-and-dome pulse)
Harsh systolic ejection murmur across entireprecordium→ apex & heart base
MR: separate murmur: severity of MR related todegree of outf low obstruction

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 62/155
EKG:

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 63/155
Echocardiography:
2D-echo:
Asymmetric septal hypertrophy
Diffuse concentric or localized to apex/anterior wall
Systolic anterior motion of MV (SAM)
7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 64/155
Doppler Echocardiocraphy:
Typical appearance: late-peaking signal “dagger-shaped”
Bernoulli for peak systolic gradient(+ maneuvers)
Obstructive or non-obstructive
Distinguish MR and intra-cavitary obstruction(looking for the aortic closure signal)

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 65/155

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 66/155

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 67/155
Cardiac cath:
Not necessary

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 68/155
Brockenbrough response ↑ LV systolic pressure
↓ Ao systolic pressure
↑ gradient between LV & Ao
Post PVC

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 69/155
Brockenbrough response

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 70/155

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 71/155
Imitator of HCM Amyloidosis:
Thickened walls & low voltage on EKG.

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 72/155
Natural history of HCM Mortality: 3 %/year (6-8 % with NSVTach)
Poor prognosis:
- Younger age- Male sex
- + family hx. of sudden death
- Hx. of syncope- Genetic markers (mutations of arginine gene)
- Exercise-induced hypotension (worst)

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 73/155

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 74/155
Genetic defect and prognosis

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 75/155
Management All first degree relatives: screening…
echocardiography/genetic counseling
Avoid competitive athletics
Prophylactic antibiotics before medical & dentalprocedures
Holter x 48 hours

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 76/155
β- Blockers: Propranolol 200-400 mg/d
(large doses)/ Selective β- B lose selectivity at highdoses:
Slow HR → longer diastolic filling time → ↓ myocardial O2 consumption →
↓ myocardial ischemia & LVOT obstruction
CaCh- Blockers: Verapamil 240-320 mg/d(with caution for hemodynamic deterioration)
Combination of both

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 77/155
Disopyramide: class I antiarrhythmic + strong –iveinotropic effect
Non-responders to Medical therapy

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 78/155
p py
???
1- Surgery (Myotomy/Myectomy) +/- MVR
2- ICD
3- DDD pacemaker
4- NSRT (alcohol septal ablation)

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 79/155
1- Surgery:Septal myotomy/myectomy:
Patients < 40 years: mortality < 1 %
Patients > 65 years: mortality 10-15 %
Survival better than medically treated patients Should be considered in: resting gradient > 50 mmHg, or
refractory to medical Rx.
Young patients, particularly those with severe disease
Additional structural abnormalities affecting the mitral valve or coronary arteries.
Complication (rare): Aortic incompetence

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 80/155
Myotomy/Myectomy
7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 81/155
2- ICD: Previous sudden death
High risk of sudden death
EPS use ?

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 82/155
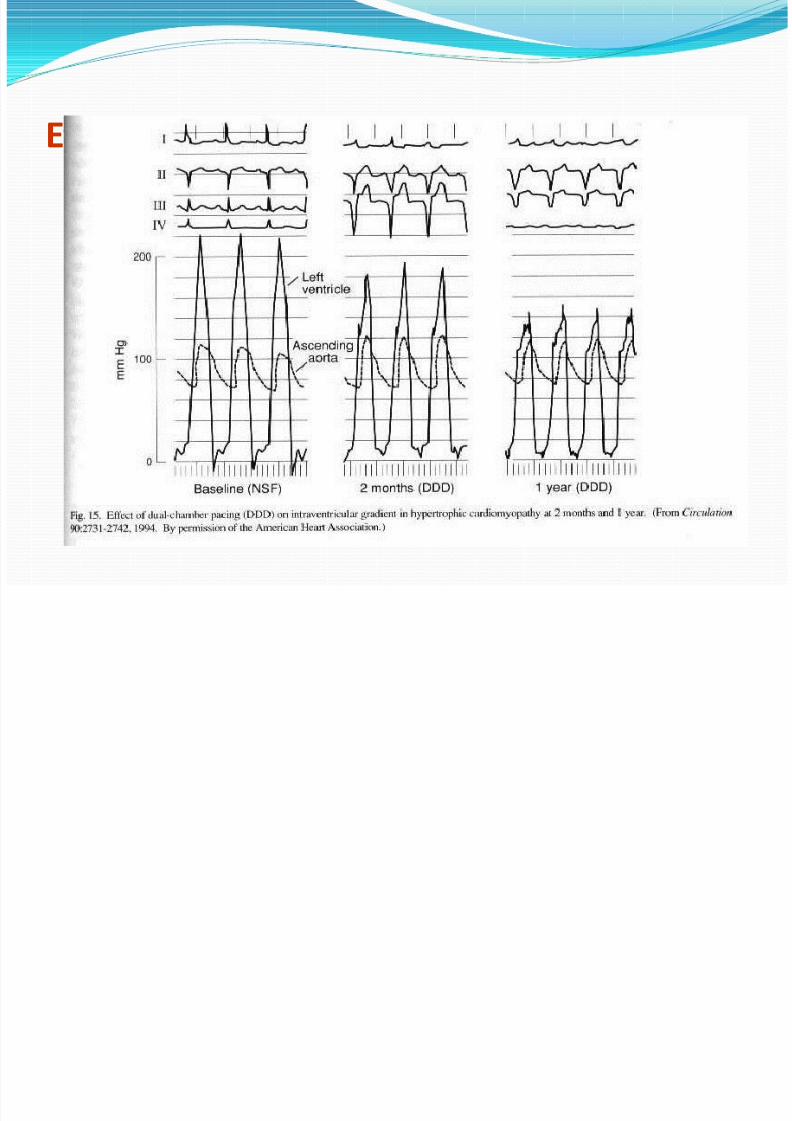
3- DDD pacemakerSubstantial ↓ gradient(~ 50 %)
7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 83/155
Effect of DDD pacemaker in HCM

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 84/155
P t ti l M h i f b fit f P i i HCM

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 85/155
Potential Mechanisms of benefit of Pacing in HCM:
RV apical pacing & maintenance of AV synchrony → abnormal pattern of septal contraction → ↓ early systolic bulging of hypertrophic subaortic septum in
LVOT &↓ Venturi forces that produce SAM.
↑ LVOT width during systole
↓ systolic hypercontractility: ↑ end-systolic volume→
↓ intraventricular pressure gradients & myocardial work

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 86/155
↓ MR
May favorably alter diastolic function
LVH regression

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 87/155
Candidates for DDD
7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 88/155
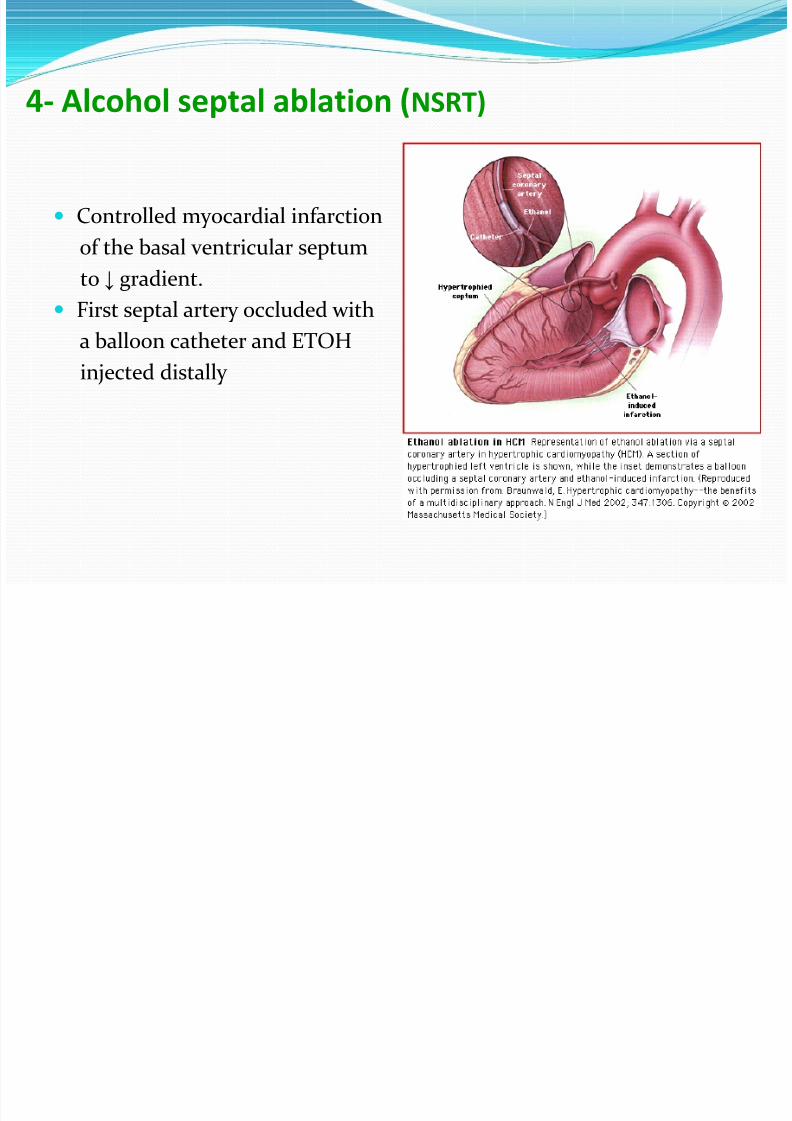
4- Alcohol septal ablation (NSRT)
Controlled myocardial infarction
of the basal ventricular septum
to ↓ gradient. First septal artery occluded with
a balloon catheter and ETOH
injected distally

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 89/155
NSRT (Non Surgical Septal Reduction Therapy)The most appropriate candidates for NSRT should meet all of thefollowing criteria :
- HCM with severe symptoms of heart failure (NYHA class III to IV)
despite adequate tolerated drug therapy
- An LVOT gradient 50 mmHg at rest or after exercise or >30 mmHg atrest or 60 mmHg under stress
- Basal septal thickness 18 mm
- NYHA class II heart failure with a resting LVOTgradient >50 mmHg or>30 mmHg at rest and 100 mmHg with stress .
- Elderly or comorbidities that may increase the risk of surgical
correction.

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 90/155

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 91/155
H hi C di h

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 92/155
Hypertrophic Cardiomyopathy

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 93/155
Definition:
WHO: left and/or right ventricular
hypertrophy, usually asymmetric and
involves the interventricular septum.

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 94/155
Differential Diagnosis:
HCM
Can be asymmetric
Wall thickness: > 15 mm
LA: > 40 mm
LVEDD : < 45 mm
Diastolic function: always
abnormal
Athletic heart
Concentric & regresses
< 15 mm
< 40 mm
> 45 mm
Normal

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 95/155
Stimulus:
Unknown
Disorder of intracellular calcium metabolism
Neural crest disorder
Papillary muscle malpositioned and misoriented

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 96/155
Genetic abnormality: Autosomal dominant.
Mutations in genes for cardiac sarcomeric proteins.
Polymorphism of ACE gene.
ß-myosin heavy chain gene on chromosome 14.
7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 97/155
Variants of HCM:Most common location: subaortic , septal, and ant. wall.
Asymmetric hypertrophy (septum and ant. wall): 70 %.
Basal septal hypertrophy: 15- 20 %.
Concentric LVH: 8-10 %.
Apical or lateral wall: < 2 % (25 % in Japan/Asia):characteristic giant T-wave inversion laterally & spade-like left ventricular cavity: more benign.

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 98/155

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 99/155
Hypertensive hypertrophic Cardiomyopathy
Elderly women
Simulates HCM
Prognosis better than non-hypertensive HCM

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 100/155
Pathophysiology of HCM Dynamic LV outflow tract obstruction
Diastolic dysfunction
Myocardial ischemia
Mitral regurgitation
Arrhythmias

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 101/155
Left ventricular outflow tract gradient
↑ with decreased preload, decreased afterload, orincreased contractility.
Venturi effect: anterior mitral valve leaflets & chordaesucked into outflow tract→
↑ obstruction, eccentric jet of MR in mid-late systole.

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 102/155
Maneuvers that ↓ end-diastolic volume
(↓ venous return & afterload, ↑ contractility)
Vasodilators
Inotropes
Dehydration
Valsalva
Amyl nitrite Exercise
→ ↑HCM murmur

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 103/155

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 104/155
Arrhythmias:
Sustained V-Tach and V-Fib: most likely mechanism of syncope/ sudden death.
Dependant on atrial kick: CO ↓ by 40 % if A. Fibpresent.

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 105/155
Histology: Myocardial fiber disarray, endocardial plaques.
Abnormal relaxation and diversely orientedmyocardial fibers.
Intimal hyperplasia of intramural coronary arteries,endothelial dysfunction, myocardial perfusion defects.

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 106/155
Clinical presentation:
Any age
Leading cause of sudden death in competitive athletes
Triad: DOE, angina, presyncope/syncope.

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 107/155

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 108/155

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 109/155
Physical exam:
Apex localized, sustained
Palpable S4
Tripple ripple
Prominent “a” wave Rapid upstroke carotid pulse, “jerky” bifid (spike-
and-dome pulse)
Harsh systolic ejection murmur across entireprecordium→ apex & heart base
MR: separate murmur: severity of MR related todegree of outf low obstruction

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 110/155
EKG:

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 111/155
Echocardiography:
2D-echo:
Asymmetric septal hypertrophy
Diffuse concentric or localized to apex/anterior wall
Systolic anterior motion of MV (SAM)

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 112/155
Doppler Echocardiocraphy:
Typical appearance: late-peaking signal “dagger-shaped”
Bernoulli for peak systolic gradient(+ maneuvers)
Obstructive or non-obstructive
Distinguish MR and intra-cavitary obstruction
(looking for the aortic closure signal)

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 113/155

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 114/155

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 115/155
Cardiac cath:
Not necessary

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 116/155
Brockenbrough response
↑ LV systolic pressure
↓ Ao systolic pressure
↑ gradient between LV & Ao
Post PVC

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 117/155
Brockenbrough response

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 118/155

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 119/155
Imitator of HCM
Amyloidosis:
Thickened walls & low voltage on EKG.

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 120/155
Natural history of HCM
Mortality: 3 %/year (6-8 % with NSVTach)
Poor prognosis:
- Younger age
- Male sex
- + family hx. of sudden death
- Hx. of syncope
- Genetic markers (mutations of arginine gene)
- Exercise-induced hypotension (worst)

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 121/155

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 122/155
Genetic defect and prognosis

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 123/155
Management
All first degree relatives: screening…
echocardiography/genetic counseling
Avoid competitive athletics
Prophylactic antibiotics before medical & dentalprocedures
Holter x 48 hours

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 124/155
β- Blockers: Propranolol 200-400 mg/d(large doses)/ Selective β- B lose selectivity at highdoses:
Slow HR → longer diastolic filling time → ↓ myocardial O2 consumption →
↓ myocardial ischemia & LVOT obstruction
CaCh- Blockers: Verapamil 240-320 mg/d
(with caution for hemodynamic deterioration)
Combination of both

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 125/155
Disopyramide: class I antiarrhythmic + strong –iveinotropic effect
Non-responders to Medical therapy
???

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 126/155
???
1- Surgery (Myotomy/Myectomy) +/- MVR
2- ICD
3- DDD pacemaker
4- NSRT (alcohol septal ablation)

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 127/155
1- Surgery:
Septal myotomy/myectomy:
Patients < 40 years: mortality < 1 %
Patients > 65 years: mortality 10-15 %
Survival better than medically treated patients Should be considered in: resting gradient > 50 mmHg, or
refractory to medical Rx.
Young patients, particularly those with severe disease
Additional structural abnormalities affecting the mitral valve or coronary arteries.
Complication (rare): Aortic incompetence

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 128/155
Myotomy/Myectomy

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 129/155
2- ICD:
Previous sudden death
High risk of sudden death
EPS use ?

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 130/155
3- DDD pacemakerSubstantial ↓ gradient(~ 50 %)

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 131/155
Effect of DDD pacemaker in HCM

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 132/155
Potential Mechanisms of benefit of Pacing in HCM:

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 133/155
RV apical pacing & maintenance of AV synchrony → abnormal pattern of septal contraction → ↓ early systolic bulging of hypertrophic subaortic septum inLVOT &
↓ Venturi forces that produce SAM.
↑ LVOT width during systole
↓ systolic hypercontractility: ↑ end-systolic volume→ ↓ intraventricular pressure gradients & myocardial work

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 134/155

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 135/155
Candidates for DDD
4 Alcohol septal ablation (NSRT)

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 136/155
4- Alcohol septal ablation (NSRT)
Controlled myocardial infarction
of the basal ventricular septum
to ↓ gradient.
First septal artery occluded with
a balloon catheter and ETOH
injected distally

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 137/155
NSRT (Non Surgical Septal Reduction Therapy)The most appropriate candidates for NSRT should meet all of thefollowing criteria :
- HCM with severe symptoms of heart failure (NYHA class III to IV)despite adequate tolerated drug therapy
- An LVOT gradient 50 mmHg at rest or after exercise or >30 mmHg atrest or 60 mmHg under stress
- Basal septal thickness 18 mm
- NYHA class II heart failure with a resting LVOTgradient >50 mmHg or>30 mmHg at rest and 100 mmHg with stress .
- Elderly or comorbidities that may increase the risk of surgicalcorrection.

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 138/155

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 139/155
DEFINITION

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 140/155
WHO• RCM as a myocardial disease characterized by
restrictive filling and reduced diastolic volume of either or both ventricles with normal or near-normal
systolic function and wall thickness.
• The hallmark of the restrictive cardiomyopathies is
abnormal diastolic function; the ventricular walls areexcessively rigid and impede ventricular filling.

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 141/155
Types – based on etiology

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 142/155
yp gy
Primary or Idiopathic
Familial
Secondary Amyloidosis (commonest)
Sarcoidosis
Endomyocardial fibrosis
Symptoms• Gradually worsening shortness of breath, progressive

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 143/155
exercise intolerance, and fatigue. This exertional dyspnea
reflects the left heart failure.
• Fatigue and weakness are results of the decreased stroke volume.
• Patients may have distention of the abdomen andbilateral swollen feet (right heart failure).
• Angina like chest pains are observed only in patients withamyloidosis.
Symptoms• Patients may complain of palpitations (atrial fibrillation),
7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 144/155
which are common in idiopathic RCM.
• As many as one third of patients with idiopathic RCMmay present with thromboembolic complications.
• Patients may have a history of syncopal attacks.
• Conduction disturbances particularly are common ininfiltrative RCM.
• Depending on the etiology, patients may have a priorhistory of radiation therapy, heart transplantation,chemotherapy, or a systemic disease.

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 145/155
SignsGPE
Px may be more comfortable sitting
Px may have minimal to moderate ascites and pitting
pedal edema
CVS Exam The pulse is low volume, consistent with decreased
stroke volume.

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 146/155
Signs• High JVP with diastolic collapse (Friedreich's sign).
• JVP with rapid X and Y descents, but the mostprominent wave is the Y descent (atrium emptyinginto the “stiff” ventricle)
• Elevation of JVP with inspiration (Kussmaul's sign).
• S4 in early disease (forceful atrial contraction against astiff ventricle).
• S3 in advanced disease.• Murmurs due to mitral and tricuspid valveregurgitation may be present.

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 147/155
SignsResp. Exam.
Reduced breath sounds because of pleural effusion
Crepitations due to left heart failure
Abd. Exam.
In advanced cases, liver may be palpable and pulsatile.

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 148/155
The goal of treatment in RCM is to reduce symptomsby lowering elevated filling pressures withoutsignificantly reducing the cardiac output.
i i

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 149/155
Investigations• CXR
– Pulmonary venous congestion .The cardiac silhouettecan be normal (familial) or show cardiomegaly and/oratrial enlargement.
• ECG – usually has low-voltage and ST segment and T wave
abnormalities.
• Echocardiogram – symmetrical myocardial thickening and often a normal
systolic ejection fraction, but impaired ventricularfilling.

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 150/155
Cardiac catheterization and haemodynamic studieshelp distinction from constrictive pericarditis.
Endomyocardial biopsy in contrast with othercardiomyopathies is often useful in this condition andmay permit a specific diagnosis such as amyloidosis to
be made.
DIFFERENTIAL DIAGNOSIS

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 151/155
DIFFERENTIAL DIAGNOSISConstrictive Pericarditis
Pericardial calcification on x-ray, which occurs inconstrictive pericarditis, is absent.
Right ventricular transvenous endomyocardial biopsy (by revealing myocardial infiltration or fibrosis inrestrictive cardiomyopathy)
CT scan or MRI (by demonstrating a thickened
pericardium in constrictive pericarditis).
pericarditis and restrictivecardiomyopathy

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 152/155
y p y
Clinical Features Constrictive Pericarditis RestrictiveCardiomyopathy
History Prior history of pericarditisor condition that causes
pericardial disease
History of systemic disease(eg, amyloidosis,
hemochromatosis)
General examination Peripheral stigmata of systemic disease
Systemic examination -Heart sounds
Pericardial knock, high-frequency sound
Presence of loud diastolicfilling sound S3, Low-
frequency soundMurmurs No murmurs Murmurs of mitral and
tricuspid insufficiency
Prior chest x-ray Pericardial calcification Normal results of priorchest x-ray
TREATMENT & PROGNOSIS
7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 153/155
TREATMENT & PROGNOSIS There is no specific treatment.
Cardiac failure and embolic manifestations should be
treated.
Cardiac transplantation should be considered in somesevere cases, especially the idiopathic variety.
In primary amyloidosis, combination therapy withmelphalan plus prednisolone with or without
colchicine may improve survival

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 154/155
However, patients with cardiac amyloidosis have a worse prognosis than those with other forms of thedisease, and the disease often recurs after
transplantation.
Liver transplantation may be effective in familial
amyloidosis (due to production of mutantprealbumin) and may lead to reversal of the cardiacabnormalities.

7/29/2019 Cardiomyopathy.pptx2!5!13 3 Year Mbbs
http://slidepdf.com/reader/full/cardiomyopathypptx2513-3-year-mbbs 155/155