Cardiology - Update on CardioVascular Disease

of 36
-
Upload
m-dicky-hidayatullah -
Category
Documents
-
view
228 -
download
0
Transcript of Cardiology - Update on CardioVascular Disease
-
8/12/2019 Cardiology - Update on CardioVascular Disease
1/36
-
8/12/2019 Cardiology - Update on CardioVascular Disease
2/36
Learning ObjectivesAmerican Family Physician monographs are designed to provide family physi-cians with high-quality continuing medical education that reflects the spectrumof family practice. After reading this monograph, physicians should be able to:1. Understand the actions of the various pharmacologic agents used in the
treatment of acute and chronic heart failure.2. Differentiate heart failure due to diastolic versus systolic dysfunction and
discuss the drugs most suitable for each.3. Describe the therapeutic stages in the management of acute myocardial
infarction (MI).4. State current recommendations for the management of patients following
acute MI, as well as recommendations for reducing coronary artery diseaserisk.
5. Review the treatment approaches to the arrhythmias most often seen in
clinical practice.6. Describe the three main steps involved in managing the patient with atrialfibrillation.
This American Family Physician monograph is made possible by an education-al grant from the following companies: Bristol-Myers Squibb Company,Hoechst Marion Roussel, Novartis Pharmaceutical Corporation, Knoll Phar-maceutical Company and Wyeth-Ayerst Laboratories. The information pre-sented and opinions expressed herein are those of the authors and do notnecessarily represent the views of the sponsors, American Family Physician orits publisher, the American Academy of Family Physicians. Any recommen-dation made by the authors must be weighed against the physicians own
-
8/12/2019 Cardiology - Update on CardioVascular Disease
3/36
KEN GRAUER , M.D., is professor and assistant director of the Family Practice Residen-cy Program, Department of Community Health and Family Medicine, School of Med-
icine, University of Florida, Gainesville. After receiving his medical degree from theState University of New York at Syracuse, he completed residency training in familypractice at St. Margaret Memorial Hospital, Pittsburgh, Pennsylvania.
DANIEL S. CLARK , M.D., is assistant clinical professor of medicine (cardiology) atUCLA School of Medicine, Los Angeles, and director of the Critical Care Unit, Ven-tura County Medical Center, Ventura, California. He received his medical degreefrom Tufts University School of Medicine, Boston, Massachusetts, and completed aninternship/residency in medicine at Greenwich Hospital, Greenwich, Connecticut,
and a clinical fellowship in cardiology at the University of Miami School of Medi-i Mi i Fl id
Cardiovascular Disease:Update on Management of Heart Failure,
Acute Myocardial Infarction, andCardiac ArrhythmiasAn American Family Physician Monograph
Prepared by Health Science Communications, Inc.,
in consultation with:
KEN GRAUER, M.D.University of Florida School of MedicineGainesville, Florida
DANIEL S. CLARK, M.D.UCLA School of MedicineLos Angeles, California
GARY E. RUOFF, M.D.Michigan State University College of MedicineKalamazoo, Michigan
-
8/12/2019 Cardiology - Update on CardioVascular Disease
4/36
Contents3 Introduction3 Heart Failure
12 Acute Myocardial Infarction
22 Cardiac Arrhythmias
28 References
30 Monograph Quiz
6 Table 1. Etiology of Heart Failure (HF)
8 Table 2. Effects of ACE Inhibitors in Heart Disease
9 Table 3. Pharmacokinetics and Dosing of ACE Inhibitors in Heart Failure
13 Table 4. Differential Diagnosis of Chest Pain
16 Table 5. Contraindications to Thrombolytic Therapy
17 Table 6. Comparison of Selected Thrombolytic Agents
20 Table 7. Recommendations for Reducing Coronary Risk Factors in Patients After Acute MI
23 Table 8. Underlying or Precipitating Causes of Atrial Fibrillation
27 Table 9. Extracardiac Factors and Exacerbating Causes of Ventricular Arrhythmias
3 Figure 1. Schematic illustration of selected types of hypertrophic responses.
19 Figure 2. Algorithm for a suggested approach to cost-effective risk stratification acuteand after management myocardial infarction.
21 Figure 3. Algorithm for office staff response to patients with symptoms of acute MI.
Ray Jarris, M.D. Medical Editor
Leigh McKinneySpecial ProjectsDepartment Manager
Michele WebbSpecial Projects Editor
Brian TorreySpecial Projects Editor
Dana GuthrieEditorial Assistant
Joetta MeltonPublisher and ProjectCoordinator
Robert L. EdsallEditorial Director
Kathy MayfieldProduction Manager
Julia NothnagelAssistant Production
Manager
John AllisonArt Director
Stacey HerrmannGraphic Associate
Clayton Raker HasserGroup Publisher andVice President forPublications andCommunications
Robert Graham, M.D.Executive Vice President
Cover illustration by
-
8/12/2019 Cardiology - Update on CardioVascular Disease
5/36
THE FAMILY PHYSICIAN IS OFTEN CALLED UPON TO
diagnose and manage major causes of cardio-vascular morbidity and mortality, whichinclude heart failure (HF), acute myocardial
infarction (MI), and cardiac arrhythmias. This
monograph provides an overview of theseconditions and addresses their causes andmanagement.
Introduction
Epidemiology HEART FAILURE , DEFINED AS AN IMPAIRMENT THATprevents the heart from adequately perfusing body tissues to meet metabolic demands, 1 is amajor health problem that affects between 2and 3 million Americans. 2 With 400,000 newcases of HF diagnosed annually, the cost to theU.S. health care system is considerable, sinceHF is the primary reason for an estimated 1
million hospitalizations per year. In 1990, HFwas responsible for approximately $10 billionin direct (e.g., hospitalization) and indirect(e.g., prolonged nursing home stays) costs. 2
HF has a poor prognosis. After theonset of symptoms, the five-year mortalityrate in patients with HFbased on data fromthe Framingham Heart Studyis 62 percentin men and 42 percent in women, 3 with
200,000 deaths attributable to HF each year inthe United States alone.
PathophysiologyTraditionally, HF has been thought to be aresult of an impairment of systolic (inotropic)function, which is a reflection of decreasedcontractility of myocardial cells, most commonin the left ventricle. More recently, impaired
left ventricular (LV) filling or diastolic dys-
easily recognized on echocardiography as abig, baggy heart.In HF due to diastolic dysfunction, cardiac
contractility is preserved or even increased(Figure 1C). The thickened and stiffened ven-tricle limits the amount of blood that can enterthe heart, resulting in decreased ventricularfilling during diastole. Ventricular dysfunction
Heart Failure
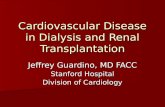
Figure 1
Schematic illustration of selected types of hypertrophic responses. In A, theleft ventricular dimensions are normal. With end-stage systolic dysfunction(B), cardiac chamber wall thickness remains the same or decreases in associa-tion with generalized dilatation of several cardiac chambers. Contractileactivity is globally reduced. In lesser degrees of systolic dysfunction, contrac-tility is reduced, but cardiac chambers do not necessarily demonstratemarked dilatation. In pure diastolic dysfunction (C), symmetric thickening of the IVS and LVFW occurs at the expense of left ventricular cavitary volume.Cardiac contractility is typically preserved, if not increased, resulting in cor-responding preservation (or increase) in ejection fraction. However, overallcardiac output is reduced because the ventricle never completely fills.
IVS = interventricular septum;LA = left atrium; LV = left ventricle;LVFW = left ventricular free wall;RA = right atrium; RV = rightventricle.
LA
RA
LV
FW
LV
A
-
8/12/2019 Cardiology - Update on CardioVascular Disease
6/36
is often mixed, however, and has elements of both systolic and diastolic dysfunction.
Unfortunately, the physical examinationwill usually not allow the physician to reliably
distinguish between systolic and diastolicdysfunction. Sometimes, a laterally displaced,dilated point of maximum impulse (PMI)may suggest that HF has a component of sys-tolic dysfunction. On the other hand, in purediastolic dysfunction, the PMI is not typicallydisplaced or dilated, albeit the impulse may be abnormally sustained in duration.
It is important to recognize that diastolic
and systolic dysfunction often overlap andmay occur in the same patient. As an exam-ple, hypertensive patients commonly devel-op concentric hypertrophy with diastolicdysfunction as a result of the increase in after-load associated with persistent hypertension.If the hypertension is not controlled, LV func-tion eventually deteriorates, and systolic dys-function becomes superimposed on the
initially hypertrophied left ventricle. Eventu-ally, the left ventricle dilates and the diastolicdysfunction present in the early HF of hyper-tension evolves to dilated cardiomyopathy, sothat the component of diastolic dysfunctionmay no longer be recognized.
Myocardial function is controlled bypreload (Frank-Starling curve), afterload,ventricular contractility, heart rate, and heart
rhythm. In HF, impaired heart functionresults in hemodynamic stress in the form of falling cardiac output. This stress unleashes aseries of interdependent acute and chroniccompensatory events, all of which are intend-ed to maintain perfusion to vital organs.
Myocardial cell hypertrophy andincreased LV wall thickness resulting fromHF are accompanied by decreased ventricu-
lar compliance (increased ventricular stiff
system, increases release of atrial natriureticpeptide (ANP), may increase the secretion of antidiuretic hormone (ADH) and renalprostaglandins, and has long-term pathologic
consequences.6
Early in the course of HF, neurohormon-al responses to hypovolemia lead to plasmaexpansion and selective vasoconstriction. Thecardiovascular system compensates for thefunctional decrease in circulatory volume byshunting blood away from nonvital organ sys-tems (e.g., kidneys, gastrointestinal tract), and by increasing cardiac contractility. Long-term
neurohormonal adaptation to decreased per-fusion results in desensitization of the heart tosympathetic stimulation, increased impedenceto LV outflow, dysfunctional vascularendothelium, impaired glycolysis in fast-twitch muscles, physical deconditioning, andmuscle deterioration.
In HF, norepinephrine is chronically ele-vated due to an increase in release and
spillover from the adrenal gland, decreasedplasma clearance, and decreased neuronal andnon-neuronal reuptake. Norepinephrineincreases afterload, causes cardiac arrhythmias,and has a direct toxic effect on the myocardi-um. There is a direct correlation between nor-epinephrine levels and both the hemodynamicseverity and the poor prognosis of HF. 6
Decreased cardiac output, characteristic
of HF, results in constriction of the kidneysefferent arterioles, which maintain the glomeru-lar filtration rate (GFR). As HF progresses, apoint is reached at which further constrictionis impossible, and the GFR becomes flow-dependent and decreases in tandem withadditional decreases in cardiac output.
When the GFR falls, sodium is reab-sorbed by the renal tubules, which activates
the RAA system The RAA system plays a key
-
8/12/2019 Cardiology - Update on CardioVascular Disease
7/36
ADH is produced in the posterior pitu-itary and promotes renal tubular reabsorp-tion of water by the kidneys in response todecreased plasma volume, as occurs in HF.
Although ADH is often increased in HF, itscontribution to the vascular dynamics of HFis unclear.
ANP is produced in atrial tissue of theheart in response to atrial stretch fromincreased blood volume. This causes natriuresisand vasodilation, and counteracts the water-retaining effect of the adrenergic and RAA sys-tems. In early-stage HF, the vasodilatory
response of peripheral arteries to ANP is pre-served, but it becomes blunted as the HF entersa decompensation phase, an effect attributed tothe down-regulation of ANP receptors. 6
One of the compensatory responses tothe chronic overstimulation of the sympathet-ic nervous system (SNS) and the RAA systemis an increased release of prostaglandins,resulting in peripheral vasodilation.
Clinical FindingsIt is essential to keep in mind that mild HF isnot necessarily the same as early-stage HF.Mild HF suggests that the patients ability tofunction is only mildly affected. Early-stage HF, on the other hand, refers to theduration of pathogenic events that occur inthe compensated phase of HF.
It is also important to emphasize thatLV dysfunction does not always progress in apredictable fashion, nor is the degree of LVdysfunction necessarily paralleled by theclinical severity of symptoms. Some patientsmay present with significant symptoms of HF, yet only have minimal alteration of LVfunction. Other patients with only mildsymptoms may come to medical attention in
later stages of HF which reflects the efficacy
cardiac index and oxygen saturation, and lac-tic acidosis. Low-output HF may be for-ward, in which oxygenated blood does notreach peripheral tissues, or backward, in
which blood backs up in the lungs.The symptoms of low-output forwardHF include weakness, fatigue, lethargy, light-headedness, and confusion. In decompensatedHF, cardiac cachexia, which is characterized by generalized exhaustion and loss of leanmuscle mass, ensues. The symptoms of low-output backward, or congestive, HF reflectpulmonary edema, in which fluids accumulate
in the lungs and result in dyspnea, initiallyonly on exertion. Decompensated low-output backward failure is characterized by orthop-nea and paroxysmal nocturnal dyspnea.
The clinical findings in HF includeperipheral edema, rales, S3 gallop, sinustachycardia, hypotension, increased jugularvenous pressure, and hepatojugular reflux.Despite the presence of one or more of these
signs, HF may be misdiagnosed in up to 40percent of patients. 7 The severity of HF canalso be evaluated with chest radiography.Chest films may demonstrate cardiacenlargement, interstitial and alveolar edema,and pulmonary vascular redistribution in HF.However, HF may also be misdiagnosedusing x-ray studies. Therefore, all patientssuspected of having HF should be evaluated
by two-dimensional echocardiography andDoppler studies to determine LV contractili-ty, ventricular compliance, hypertrophy, andthe presence or absence of other underlyingconditions, such as valve pathology.
Management StrategiesHF is a syndrome that consists of a constella-tion of symptoms evoked by a wide range of
conditions and precipitating factors ( Table 1) Its
-
8/12/2019 Cardiology - Update on CardioVascular Disease
8/36
cal ventilation to optimize oxygenation andgas exchange. An intravenous (IV) diureticshould be administered to reduce preload,relieve pulmonary congestion, and improve
oxygenation. Furosemide (Lasix) is usuallygiven in doses of 20 to 40 mg IV, with the dosedoubled, as needed, every 30 minutes until amaximum of 160 mg is reached. The initialdose depends on the severity of pulmonarycongestion, duration of HF symptoms (time toallow compensatory fluid retention), renaldysfunction, and known responsiveness tofurosemide.
Morphine sulfate remains an extremelyeffective treatment for pulmonary edema andadministration should be titrated in smallaliquots (2 to 5 mg IV) to reduce preload andimprove cardiac performance by reducingafterload. Morphine also alleviates the sensa-tion of air hunger, thereby indirectly reducingthe level of circulating catecholaminesreleased due to anxiety. Overadministration of
morphine is unusual in patients with pul-monary edema; if respiratory depression doesoccur, it can be easily reversed with IV nalox-one hydrochloride (Narcan).
Nitroglycerin acts by reducing both pre-load and afterload, thereby improving cardiacperformance. Sublingual (0.4 mg), cutaneous,or IV nitroglycerin may be used, dependingon the patients clinical condition. IV nitroglyc-
erin has a greater effect on afterload, whereasthe sublingual and cutaneous forms reducepreload to a greater extent. Nitroglycerin isalso indicated if angina accompanies HF.
Inotropic therapy with digoxin is gener-ally not indicated in the treatment of acutepulmonary edema. Digoxin may be useful,however, as an antiarrhythmic agent to slowrapid atrial fibrillation or atrial flutter if these
conditions accompany the HF Central moni
Table 1
Cardiac causes of HF
CardiomyopathyDilated (congestive) cardiomyopathyInfectious (e.g., viral, parasitic)Toxic (e.g., alcohol abuse, doxorubicin hydrochloride
[Adriamycin], cyclophosphamide [Cytoxan, Neosar])Nutritional (e.g., l-carnitine, selenium, thiamine, or protein deficiency)Connective tissue disease
Hypertrophic cardiomyopathy (concentric left ventricularhypertrophy)
Infiltrative cardiomyopathyAmyloidHemochromatosisSarcoidosis
Hypertensive heart diseaseMyocardial ischemia or infarction accompanied by left ventricular
dysfunctionValvular heart diseaseCardiac arrhythmias (e.g., persistent tachycardia, atrial fibrillation)
Noncardiac causes of HF
Albrights disease (polyostotic fibrous dysplasia)AnemiaCarcinoid syndromeArteriovenous fistulas (e.g., trauma, Pagets disease of bone,
hemangiomatosis, glomerulonephritis, hemodialysis)Hepatic disease (e.g., alcohol-related thiamine deficiency)Decreased peripheral arterial resistanceHyperkinetic heart syndromePolycythemia veraThyrotoxicosis
Factors that may precipitate HFAlcoholCor pulmonaleDrug-related (e.g., inappropriate medications, noncompliance)Excess fluid or sodium intakeFeverHypothyroidismHypoxiaInfectionObesity
Etiology of Heart Failure (HF)
-
8/12/2019 Cardiology - Update on CardioVascular Disease
9/36
valvular disease, long-term therapy for HFshould be initiated, including both nonphar-macologic supportive measures and pharma-cologic therapy. Nonpharmacologic measures
include salt restriction (aiming for less than 2 gsodium per day), smoking cessation, elimina-tion of alcohol intake, aerobic exercise as tol-erated, and fluid restriction in patients withimpaired renal function, refractory HF, orpsychogenic polydipsia. Patients who areprone to developing congestive symptomsshould monitor their weight daily and reportany rapid weight gain in excess of 3 to 5 lb.
The pharmacologic management of HFmay require the use of multiple agents, includ-ing diuretics, angiotensin-converting enzyme(ACE) inhibitors, digoxin, nitrates, calcium-channel blockers (CCBs), and beta-adrenergic blockers. Treatment should be tailored to theunderlying systolic or diastolic dysfunction.
Diuretics
Diuretics are a mainstay in the acute manage-ment of HF, and are usually the first drugsadministered to the patient with congestivesymptoms. They reduce the preload (venousreturn volume and ventricular filling pressure)and, by decreasing the effective circulating vol-ume, relieve the symptoms of pulmonary con-gestion and peripheral edema. Although highlyeffective in the management of acute conges-
tion, diuretics do not prevent disease progres-sion and their long-term effect on mortality isunknown. Moreover, the use of diuretics may be associated with adverse effects on hemody-namics, renal function, and serum electrolytes.For example, they may result in reflex tachy-cardia, activation of the SNS and RAA system,increased blood urea nitrogen (BUN) andcreatinine levels (from volume depletion), and
decreased potassium and magnesium levels
clearance 20 mL per minute). These diureticsare ineffective with more severe degrees of renal impairment.
In moderate to severe HF, low doses of
loop diuretics, such as furosemide, may beeffective. Other loop diuretics include bumetanide (Bumex), which has a morerapid onset but a shorter duration of action;ethacrynic acid (Edecrin), the most ototoxic of the loop diuretics; and torsemide (Demadex),the newest of these agents, which is as effec-tive as furosemide but has a longer durationof action, allowing for less frequent dosing.
In patients with HF that is refractory toattempts at diuresis with moderate to highdoses of a loop diuretic, the addition of 2.5 to5.0 mg of metolazone (Mykrox, Zaroxolyn) 30to 60 minutes before giving the loop diureticmay restore an effective diuretic response.
Potassium-sparing diuretics effect milddiuresis but have the advantage of conserv-ing both potassium and magnesium, which
may be more effective in maintaining elec-trolyte balance than cation supplementation.Potassium-sparing diuretics include amiloride(Midamor), triamterene (Dyrenium), a combi-nation of hydrochlorothiazide and triamterene(Dyazide, Maxzide), and spironolactone(Aldactone). Careful monitoring of potassiumis required when these agents are added to aregimen that contains either ACE inhibitors or
angiotensin II receptor antagonists (ARAs)due to an increased risk for hyperkalemia.Because of their weak diuretic action, potassi-um-sparing diuretics are mainly used asadjuncts to other, more potent diuretics.
Diuretics must be used carefully inpatients with diastolic dysfunction, becausethey are highly volume-dependent. Excessivevolume depletion could exacerbate the prob-
lem with ventricular filling
-
8/12/2019 Cardiology - Update on CardioVascular Disease
10/36
hemodynamics and electrical stability, as wellas reduced SNS activity and reduced LV mass.The vasculoprotective benefits includeimproved endothelial function, vascular com-
pliance and tone, as well as direct antiprolifer-ative and antiplatelet effects. 8 ACE inhibitorsalso stimulate prostaglandin synthesis, reducethe size of myocardial infarcts, reduce reperfu-sion injury and complex ventricular arrhyth-mias, and have antiatherogenic activity incholesterol-, mechanical- and immune-mediat-ed experimental models of atherosclerosis.
ACE inhibitors have emerged as the
treatment of choice in HF with systolic dys-function because of their neurohormonaleffects and their ability to reduce both preloadand afterload. The ACE inhibitor-inducedreduction of angiotensin II results in reducedrelease of aldosterone, which in turn reducessodium and water retention, and, by exten-sion, decreases preload. ACE inhibitorsimprove the hemodynamics of HF by reduc-
ing right atrial pressure, pulmonary capillarywedge pressure, arterial blood pressure, andpulmonary and systemic vascular resistance.These agents also increase both the cardiacand stroke indices and reduce the right ven-tricular end-diastolic volume, thereby result-ing in increased cardiac output, reducedcardiac load, and decreased myocardial oxy-gen consumption. They also down-regulate
the SNS, which, as discussed earlier, is inti-mately linked to the pathogenesis of HF.The net effects of the reversal of the
pathophysiologic cascade of HF by ACEinhibitors include improvement in symp-toms, functional status, exercise tolerance,and quality of life plus prolonged survival.
After initial patient stabilization, ACEinhibitor therapy may be started with a short-acting agent (e.g, captopril [Capoten]) beforeswitching to a long-acting drug ( Table 3). Ini-
tial use of short-acting ACE inhibitors mini-mizes the frequency and duration of ACEinhibitor-related hypotensive episodes, as itpermits more rapid withdrawal of therapy.Such treatment is often not needed in morestable patients. Although there are differencesamong the ACE inhibitors in pharmacokinet-ics and other properties, these differences areof relatively little clinical significance. Long-
acting ACE inhibitors are generally preferredfor long-term therapy because of theirdecreased frequency of administration, whichtranslates into improved patient compliance.
ACE inhibitors are indicated for use invirtually all patients with HF due to systolicdysfunction, unless there are specific con-traindications to their use, such as hyper-kalemia, pregnancy, clinically significant
renal insufficiency, symptomatic hypoten-sion, or a history of adverse reactions or intol-erance. Potential adverse effects of ACEinhibitors include hypotension, renal impair-ment, hyperkalemia, cough, and angioneu-rotic edema. In addition, idiopathic adverseeffects, such as skin eruptions, disturbancesin taste, and bone marrow suppression, have been noted.
In patients who cannot tolerate ACEinhibitors because of cough or angioedema,two alternative therapeutic regimens can beused: either combination therapy withhydralazine (Apresoline) and a nitrate, ortreatment with an ARA, such as losartan(Cozaar), valsartan (Diovan) or irbesartan(Avapro). Despite the ability of hydralazineand isosorbide dinitrate (Isordil, Sorbitrate) to
effectively reduce preload and afterload thisTable 2
-
8/12/2019 Cardiology - Update on CardioVascular Disease
11/36
on the RAA system, angiotensin II is alsoformed by enzymes other than angiotensin-converting enzymes. Thus, since ARAs bind at
a site more distal to angiotensin II receptors,they more completely antagonize angiotensinII effects, including vasoconstriction, SNS acti-vation, and aldosterone release. Unlike ACEinhibitors, ARAs do not interfere with bradykinin and prostaglandin metabolism,which has been suggested to be responsible forthe cough and angioedema of ACE inhibitors.
In the ELITE study, patients with New
York Heart Association (NYHA) class II-IVheart failure were randomized to receive eithercaptopril or losartan. Preliminary data fromthat study suggest that survival in patientsreceiving losartan may be comparable to thatin patients receiving captopril, although fur-ther study is warranted before general recom-mendations can be made. 9 In general, sideeffects from ARA drugs are minimal.
fraction (LVEF). However, digoxin has not been shown to improve survival in patientsreceiving diuretics and ACE inhibitors. 10,11
Digoxins efficacy in treating HF hingeson its positive inotropic effects, whichinclude increases in the force and velocity of myocardial contraction, ejection fraction, andexercise tolerance. In addition to improvingthe hearts mechanical functions, digoxinslows cardiac conduction and affects neuro-hormonal activity.
Digoxin prolongs the refractory period
of the atrioventricular (AV) node, resulting ina slowed ventricular response to supraven-tricular tachyarrhythmias, especially atrialfibrillation, for which digoxin remains anagent of choice, especially when the fibrilla-tion accompanies acute myocardial infarctionor LV failure. Digoxin also ameliorates theautonomic dysfunction typical of HF byattenuating SNS activity.
Digoxin is of limited use in the treat
Table 3
Ligand Bioavailability Half-life Recommended
classification (%) (hr) Excretion Initial dose Target dose maximal doseSulfhydrylCaptopril (Capoten) 70 2 Renal 12.5 mg TID 25 - 50 mg TID 50 mg TID
CarboxylEnalapril (Vasotec) 60 11 Renal 2.5 mg BID 10 mg BID 20 mg BIDLisinopril (Prinivil, 25 12 Renal 5 mg QD 20 mg QD 40 mg QD
Zestril)Quinapril (Accupril) 75 - 80 2 - 3 Renal 5 mg BID 20 mg BID 20 mg BID
PhosphinylFosinopril (Monopril) 36 14 Renal/ 10 mg QD 20 - 40 mg QD 40 mg QD
compensatoryhepatic
Pharmacokinetics and Dosing of ACE Inhibitors in Heart Failure
-
8/12/2019 Cardiology - Update on CardioVascular Disease
12/36
weeks if no loading dose is given. Results of the PROVED and RADIANCE trials indicatethat in a significant percentage of patientswith HF due to systolic dysfunction, their
condition worsened when digoxin was dis-continued. 12,13 Therefore, maintaining suchpatients indefinitely on digoxin, providedthey have no adverse reactions, seems war-ranted. That said, the more recently complet-ed Digoxin Trial failed to show reducedmortality with long-term use of this drug. 14
Because of digoxins narrow therapeuticindex, dosing must be titrated carefully. Con-
ditions contributing to digoxin toxicityinclude renal insufficiency (with concomitantdiuretic), ACE inhibitor use, and concomitantadministration of potassium-depleting corti-costeroids and diuretics. Symptoms of digox-in toxicity include loss of appetite, nausea andvomiting; defects in color vision, in particularfor reds and greens, or seeing halos aroundlight bulbs; symptoms that suggest psychosis;
weakness, fatigue, or dizziness; cardiacarrhythmias, including frequent or multiformpremature ventricular contractions (PVCs),ventricular tachycardia, atrial tachycardiawith block, accelerated junctional rhythms,rhythms with Wenckebach conduction, andatrial fibrillation with slowed or regular ven-tricular responses; and hyperkalemia.
Digoxin toxicity is managed by discon-
tinuing the drug; monitoring arrhythmias;correcting acid-base, electrolyte, and volumeabnormalities; and treating hypoxia,ischemia, and arrhythmias. Arrhythmias area common manifestation of digoxin toxicityand often respond to lidocaine (Xylocaine) orphenytoin (Dilantin), or both. In extremeemergencies, digoxin antibody fragments,which bind the active portion of the digoxin
molecule may be needed to reduce the
may be used in diastolic dysfunction. How-ever, because these agents produce vasodila-tion, they must be used with caution so as notto excessively reduce blood pressure and
exacerbate the problem with filling.Positive inotropic agents, such as digox-in, are contraindicated in pure diastolic dys-function because they further increase cardiaccontractility. However, negative inotropicagents (lusotropic agents), such as beta-block-ers or the CCBs diltiazem (Cardizem) andverapamil (Calan, Isoptin), are treatments of choice in pure diastolic dysfunction, because
they allow ventricular relaxation and improvefilling.
Beta-blockersAs indicated above, beta-blockers are a thera-py of choice in patients with diastolic dys-function in which contractility is preserved.These agents reduce the heart rate and con-tractility, resulting in increased diastolic fill-
ing and cardiac output. Recent data suggestthat long-term therapy with beta-blockersmay also be useful in systolic dysfunction. 16In patients with severe HF from end-stagecongestive cardiomyopathy, beta-blockerswere shown to significantly improve LVfunction and increase survival. 16
The mechanisms by which beta-blockersact to improve contractility in patients with
systolic dysfunction are not completely clear,although it is thought that the effects are mul-tifactorial and primarily the result of opposi-tion to oversecretion of catecholamines.Chronic SNS overstimulation is one of theprincipal pathogenic mechanisms of HF.Effects are both structural (e.g., myocardialfibrosis and myocyte hypertrophy) and func-tional (e.g., tachycardia, constriction of coro-
nary arteries reduced ventricular filling time
-
8/12/2019 Cardiology - Update on CardioVascular Disease
13/36
on the RAA system, angiotensin II is alsoformed by enzymes other than angiotensin-converting enzymes. Thus, since ARAs bind at
a site more distal to angiotensin II receptors,they more completely antagonize angiotensinII effects, including vasoconstriction, SNS acti-vation, and aldosterone release. Unlike ACEinhibitors, ARAs do not interfere with bradykinin and prostaglandin metabolism,which has been suggested to be responsible forthe cough and angioedema of ACE inhibitors.
In the ELITE study, patients with New
York Heart Association (NYHA) class II-IVheart failure were randomized to receive eithercaptopril or losartan. Preliminary data fromthat study suggest that survival in patientsreceiving losartan may be comparable to thatin patients receiving captopril, although fur-ther study is warranted before general recom-mendations can be made. 9 In general, sideeffects from ARA drugs are minimal.
fraction (LVEF). However, digoxin has not been shown to improve survival in patientsreceiving diuretics and ACE inhibitors. 10,11
Digoxins efficacy in treating HF hingeson its positive inotropic effects, whichinclude increases in the force and velocity of myocardial contraction, ejection fraction, andexercise tolerance. In addition to improvingthe hearts mechanical functions, digoxinslows cardiac conduction and affects neuro-hormonal activity.
Digoxin prolongs the refractory period
of the atrioventricular (AV) node, resulting ina slowed ventricular response to supraven-tricular tachyarrhythmias, especially atrialfibrillation, for which digoxin remains anagent of choice, especially when the fibrilla-tion accompanies acute myocardial infarctionor LV failure. Digoxin also ameliorates theautonomic dysfunction typical of HF byattenuating SNS activity.
Dig i i f li it d i th t t
Table 3
Ligand Bioavailability Half-life Recommended
classification (%) (hr) Excretion Initial dose Target dose maximal doseSulfhydrylCaptopril (Capoten) 70 2 Renal 12.5 mg TID 25 - 50 mg TID 50 mg TID
CarboxylEnalapril (Vasotec) 60 11 Renal 2.5 mg BID 10 mg BID 20 mg BIDLisinopril (Prinivil, 25 12 Renal 5 mg QD 20 mg QD 40 mg QD
Zestril)Quinapril (Accupril) 75 - 80 2 - 3 Renal 5 mg BID 20 mg BID 20 mg BID
PhosphinylFosinopril (Monopril) 36 14 Renal/ 10 mg QD 20 - 40 mg QD 40 mg QD
compensatoryhepatic
Pharmacokinetics and Dosing of ACE Inhibitors in Heart Failure
-
8/12/2019 Cardiology - Update on CardioVascular Disease
14/36
ever so slowly over a period of months. Somepatients may develop worsening congestionthat may need to be treated with increaseddosages of diuretics. With time and carefulupward titration of beta-blocker doses, LVfunction ultimately improves in most patients.
Calcium Channel BlockersThe role of CCBs in the treatment of patientswith heart failure from systolic dysfunctionremains unclear. As discussed previously,negatively inotropic CCBs (i.e., verapamiland diltiazem) are drugs of choice for the
treatment of HF with diastolic dysfunction.They should not be used in HF with systolicdysfunction. Dihydropyridine CCBs tend notto be negatively inotropic in vivo. However, because of the potent vasodilation they pro-duce, they are prone to evoke neurohumoralresponses in the form of SNS stimulation andreflex tachycardia, both of which are deleteri-ous in patients with HF.
The recently completed ProspectiveRandomized Amlodipine Survival Evaluation(PRAISE) I Trial suggested that the dihy-dropyridine agent amlodipine (Norvasc) mayhave a different clinical effect than other dihy-dropyridines, and survival was increased inpatients treated with this drug who had non-ischemic cardiomyopathy. 17 Survival was notincreased, however, in patients so treated
who had ischemic cardiomyopathy, suggest-ing that the true effect of amlodipine inpatients with HF from systolic dysfunctionmay not yet be known. Results from thePRAISE II Trial that is currently in progresswill hopefully help answer this question.
A recently approved CCB, mibefradil(Posicor), warrants specific comment. Unlikeall other CCBs, which block the L- and T-type
(l g ti g) l i h l f d th
arrhythmias and ischemia. Ventriculararrhythmias are often present in patients withHF. Despite their ubiquity, treatment should be limited to potassium and magnesium sup-plementation for asymptomatic prematureventricular contractions (PVCs), even if fre-quent, or for short periods of nonsustainedventricular tachycardia. In those patients who become symptomatic due to sustained ven-tricular tachycardia, medical therapy withagents such as amiodarone (Cordarone) may be indicated, or, in the more refractory cases,consideration may be given to implantation of
a cardioverter-defibrillator.19
Among otherancillary therapies for managing HF arenitrates or anticoagulants. Both are discussedat greater length under management of acutemyocardial infarction (MI).
Practically speaking, the best chance forlong-term survival in the patient with HF fromsystolic dysfunction lies with identifying apotentially reversible underlying or precipitat-
ing cause of the heart failure and then attempt-ing to correct it. Potential surgical interventionsinclude valve repair or replacement; coronaryrevascularization (bypass surgery, angioplasty,or stenting); or heart transplantation.
The patient with a significant heart mur-mur who develops HF should be evaluatedfor the possibility of valve replacement. Inselected circumstances, surgical correction of
the valvular abnormality will resolve the HF.Admittedly, it will not be often that HF is thesole result of reversible ischemic heart disease.However, when the possibility exists thatischemia is causative, cardiac catheterization isindicated to define the anatomy. In occasionalpatients, revascularization may significantlyimprove ventricular function.
Finally, for the patient with end-stage
HF h i th i h lth d t ld l
-
8/12/2019 Cardiology - Update on CardioVascular Disease
15/36
Acute Myocardial InfarctionEpidemiology EACH YEAR IN THE UNITED STATES , AN ESTIMATED1.5 million individuals experience acute MI.Approximately one-fourth of all U.S. deathsare due to acute MI, and more than 60 per-cent of the deaths related to acute MI occurwithin one hour of the event. Most of theseare attributable to arrhythmias, in particular,ventricular fibrillation. Because early reperfu-sion treatment improves LV systolic function
and survival, efforts to minimize prehospitaldelay should be a priority. Such effortsinclude patient education about acute MIsymptoms and the appropriate action to take,in addition to prompt initial care by the com-munity emergency medical system.
The economic burden of MIs is consid-erable. As much as one-half of the $100 bil-lion annual price tag of coronary artery
disease is directly linked to acute MIs; theaverage five-year medical expenses of anacute MI survivor was $50,000 in 1990.22
EtiologyThe most common cause of acute MI, occur-ring in 90 to 95 percent of cases, is total occlu-sion of a major coronary artery. Thismechanism is similar to that which occurs in
unstable angina, except that in unstable angi-na, occlusion of the coronary artery is notcomplete. It is now known that acute MI mostoften develops in a vessel with a lesser gradeocclusion.23 This surprising finding is linkedto the instability of the lipid-laden, thinlycapped atherosclerotic plaque, which is moresusceptible to rupture and subsequent forma-tion of an occluding thrombus. A plaque with
l li id d t i i t t
usually not transmural, and, therefore,incomplete. As a result, non-Q-waveinfarctions tend to be smaller and associatedwith a better prognosis initially. With time,however, the long-term prognosis for bothnon-Q-wave and Q-wave infarctions becomessimilar, because of the tendency of non-Q-wave infarctions to complete in the weeks tomonths after the initial event. Therefore, con-sideration of early revascularization is a criti-
cal component of managing patients withnon-Q-wave infarction. Many (if not most) of these patients should be catheterized prior tohospital discharge in the hope of identifyingthose with high-risk lesions who are likely to benefit from revascularization. At the least,careful risk stratification is mandatory.
Acute MI is generally followed withinhours by the process of remodeling, which
continues for weeks to months after the acuteevent. In remodeling, the left ventricle tendsto enlarge and become more spherical, result-ing in a thinning of the ventricular wall. Theremodeled ventricle has a greater propensityfor developing arrhythmias and heart failure,as it continues to stretch in an attempt toincrease contractility.
Diagnosis of Acute MIAlthough acute MI is the most commoncause of acute chest pain in older adults,other conditions must be excluded from diag-nostic consideration ( Table 4). In practice, thediagnosis of acute MI is based on history,physical examination (to exclude other possi- ble causes of chest pain), an electrocardio-gram (ECG), and laboratory testing for the
f k f t i f
-
8/12/2019 Cardiology - Update on CardioVascular Disease
16/36
radiate to the chest. The pain may be accom-panied by nausea and vomiting, especially ininferior infarction. Other symptoms that may be seen in acute MI include shortness of breath , gast ro in test inal di scomfort , andchanges in mental status.
The characteristic clinical picturenotwithstanding, the diagnosis is often moredifficult in practice. Each year in the UnitedStates, an estimated 1.7 million patients areadmitted to the hospital for suspected acuteMI, which is then confirmed in only aboutone third of the cases. 24 The remaining two-thirds represent either cardiac ischemicepisodes or noncardiac pain.
The presentation of acute MI is oftenatypical. According to a long-term follow-upof the Framingham study, as many as one-third of first infarctions in men and 50 percentin women were clinically unrecognized. 25There are two types of clinically silent MIs:those in which there are no manifestations at
all (and MI is only diagnosed retrospectively by subsequent development of Q waves onECG), and those in which chest pain is absent but other symptoms occur, such as shortnessof breath, gastrointestinal symptoms, flu-like illness, or mental status changes.
The patients history of chest pain mayprovide clues to the duration of the infarc-tion. However, it is important to keep in
mind that the duration of the pain does notalways correlate with the age of the infarc-tion. For example, a patient who has hadchest pain for 10 hours could have had unsta- ble angina (i.e., subtotal occlusion) for eightof those hours, and therefore still be a candi-date for reperfusion therapy despite the pro-longed history of chest pain. That this is thecase would be suggested by ECG findings of
i ifi t ST t l ti d l k f
is still having chest pain, the ECG should berepeated. Even if the patient is pain-free, arepeat ECG two hours after presentation mayyield important evidence of an acute MI.
The presence of ST-segment elevationindicates injury (viable myocardium). In gen-eral, to reduce the chance that the ECGchanges might be due to some other cause, atleast 1 mm of ST-segment elevation in two ormore contiguous leads should be document-ed before thrombolytic therapy is adminis-tered. Patients with extensive evidence of ST-segment elevation, indicating a larger areaof injury, may benefit more from thrombo-lytic therapy. ST-segment depression or T-wave inversion is not a criterion forinstituting thrombolytic therapy unless theST-segment depressions are reciprocal to ST-segment elevations. The absence of Q wavesor the presence of only small q waves alsosuggests potentially more benefit fromthrombolytic therapy.
Table 4
Permission to reproduceTable 4 on CD-ROM wasnot granted in time for
d i Pl f
-
8/12/2019 Cardiology - Update on CardioVascular Disease
17/36
Patients whose initial ECG is normal orshows only minimal nonspecific changestend to have a better prognosis, even if theygo on to have an acute infarction. If suchpatients are hemodynamically stable and freeof chest pain they can often be managed safe-ly on a monitored ward in the hospital. Incontrast, patients with acute ECG changes aremuch more prone to develop complicationsand should generally be admitted to an inten-sive care unit (ICU).
Laboratory TestsThe decision to admit a patient with chestpain is best made on the basis of the historyand initial ECG results. Once the decision ismade to admit the patient, use of acute serummarkers may be invaluable for definitivedetermination of whether an infarct occurred,for estimation of the relative size of infarc-tion, and determination for suitability forthrombolytic therapy.
While the accuracy of a single serummarker is clearly not infallible, serial testing orcombining two or more markers may improvediagnostic accuracy. CK, its MB isoenzyme(CK-MB), and a troponin marker are pre-ferred. CK is released early into the circula-tion when the sarcolemma is damaged butnot necessarily destroyed, so its release mayalso indicate HF, cardiomyopathy, or angina.
As already noted, CK measurement is usefulin conjunction with ST-segment elevation todetermine the onset of infarction when chestpain has lasted for many hours. For example,if the ST-segment is still elevated but CK isnot greatly increased, the onset of infarctionis likely to be recent, even if the patient hashad chest pain for more than six hours.
CK-MB isoenzymes are released into
h i l i i hi h f i f i
plex that binds to various components of con-tracting myocardial cells and regulates the cal-cium-dependent interactions between myosinand actin. Of the three markers, troponin I isfound only in cardiac muscle and appears to be the most specific for true cardiac injury. 27Troponin T may be somewhat less reliable because it is also found in skeletal muscle, butit is more rapidly assayed than troponin I. Tro-ponin I and T serum levels rise within three tofour hours of symptom onset, peak at 12 to 24hours, and are cleared over five to 15 days. Asa result, these markers are excellent indicatorsof recent infarction in the patient with symp-toms of several days duration. Whereas onepositive troponin value can be used to diag-nose acute MI, troponin alone cannot be usedto diagnose reinfarction or infarct extension because levels remain elevated for up to 15days. Although the ultimate role that thesemarkers will play in the diagnosis of acute MIis still being worked out, 28 troponin I measure-
ment may soon become a gold standard forevaluating patients with suspected acute MI.Myoglobin, another marker, rises early,
usually within two to four hours of an acuteMI, even before CK-MB becomes elevated.However, myoglobin is present in skeletal aswell as cardiac muscle, and therefore risesrapidly with muscle injury. In addition, it hasa very narrow window of release; myoglobin
may be cleared by the time serum levels areordered. As a result, it is far from being anoptimal marker of acute infarction.
Management of Acute MIManagement of acute MI involves multipleoverlapping therapeutic stages that beginwhen the patient is first seen by emergencymedical services, continue with long-term
h h d i l d
-
8/12/2019 Cardiology - Update on CardioVascular Disease
18/36
the data, and making a decision about appro-priate treatment interventions. For optimal benefit, initial therapy for acute MI should bein progress within 30 minutes of arrival at theemergency department. Most patients who diedo so because they delay calling: The averagedelay in seeking medical attention for acute MIis still between two and six hours. 29 Once thepatient is in the emergency department, IVaccess is established, supplemental oxygenprovided, and pain and anxiety are addressed.
Pain ManagementCentral to the early management of acute MIis controlling the pain associated with theischemic process. Angiographic studies havedemonstrated that relief of pain often accom-panies reperfusion of an occluded coronaryartery. Thus, failure to relieve the pain sug-gests that there is still potentially viablemyocardial tissue at risk of necrosis. Persis-tence of chest pain is deleterious because itsets up a vicious circle of physiologic changes,including increased oxygen demand and com-promised blood flow, that result in more pain.Anxiety aggravates these effects even further.
Four types of medications may be usefulin treating the ischemic pain of acute infarc-tion and addressing its underlying cause:analgesics, anti-ischemic agents, thrombolyticagents, and anxiolytic agents. Combining two
or more of these agents may produce a syner-gistic effect. Of the various analgesics thathave been used to manage the pain of acuteMI, morphine continues to be preferred. Mor-phine relieves anxiety, reduces preload andafterload, and lowers heart rate and respirato-ry rate. It may be given in 2 to 5 mg incre-ments IV every five to 30 minutes as needed,in conjunction with other treatments such as
b bl k d i l i M hi
arteries and decreasing myocardial oxygendemand by reducing the preload and theafterload. Because nitroglycerin causesvenous dilation, it should not be used inpatients with hypovolemia or hypotension,and with caution in patients with right ven-tricular infarction. IV nitroglycerin exerts asignificant afterload-reducing effect, resultingin a reduction in blood pressure, whereasother forms of nitroglycerin work mainly onpreload reduction.
While nitroglycerin is widely used, datafrom the GISSI-3 and ISIS-4 studies, whichinvolved over 50,000 patients, failed to showa beneficial effect on mortality resulting fromthe early administration of nitroglycerin inacute MI.30,31 Unfortunately, use of sublingualnitroglycerin before entry into these studieswas not always controlled, calling the resultsinto question. Many patients with an acuteMI have already taken one or more sublin-gual nitroglycerin tablets before being admit-ted to the hospital.
Nonetheless, in patients with new-onsetchest pain, sublingual nitroglycerin should beadministered, if not by the patient then by theemergency medical service team on arrival atthe scene. Patients who present with an acuteischemic syndrome, especially if they arehypertensive or in heart failure, shouldreceive nitroglycerin intravenously. The infu-
sion should be started at a rate of 10 g perminute and increased up to a range of 30 to100 g per minute as needed. Patients inwhom the suspicion of acute MI is low andwho have easily controlled pain are oftenadequately treated with the paste form of nitroglycerin. However, if acute ischemicchest pain is not easily controllable by initialmeasures, admission to the ICU and initia-
i f i l i i f i h ld b
-
8/12/2019 Cardiology - Update on CardioVascular Disease
19/36
In the large (more than 17,000 patients),placebo-controlled ISIS-2 Trial, early use of aspirin reduced mortality at a rate comparableto that of thrombolytic therapy. 32 When givenin combination, aspirin and streptokinase(Kabikinase, Streptase) had a synergistic effect,with a 42-percent reduction in mortality.
Ticlopidine (Ticlid), another antiplateletagent, is used in patients with a history of allergy to aspirin or anaphylaxis. Ticlopidinehas been shown to be effective in reducingcardiovascular mortality and acute MI inpatients with unstable angina. 19 However, ithas a delayed onset of action compared withaspirin (24 to 48 hours), which makes it aclear second choice for platelet inhibition.Long-term use of ticlopidine may result inthe development of neutropenia; therefore,patients receiving this antiplatelet agentshould be monitored with frequent bloodcounts.
Thrombolytic Therapy.Patients with acuteMI, ST-segment elevation, and presumednew-onset left bundle-branch block should beevaluated as possible candidates for throm- bolytic therapy, assuming there are no con-traindications ( Table 5). Experience to datesuggests that thrombolytic therapy is used in40 to 50 percent of patients younger than 75
years and in less than 20 percent of patientsolder than 65 years. 19 Whereas some increasein use rates can be achieved, contraindicationsto thrombolytic therapy prohibit its use in asignificant portion of patients.
The decision to administer thrombolytictherapy should be based on patient parame-ters and assessment of the clinical situation athand. Among the most common reasons fornot administering a thrombolytic agent istime delay. However, six hours should nolonger be viewed as the absolute cut-off forsuch treatment, particularly if chest pain andST-segment elevation are still present and CKenzymes are normal or only slightly elevated.Studies have confirmed that the treatment benefit for thrombolytic therapy may extendup to 12 hours in patients in whom the risk- benefit ratio is favorable. 19,33 In addition, ageshould no longer be viewed as a contraindi-cation for beginning treatment. In the past,patients older than 75 years were routinelyexcluded from consideration for thrombolytictherapy. However, the potential for saving 20to 30 patients per 1,000 offsets the increasedrisk of one to two additional cases of centralnervous system (CNS) bleeding per 1,000patients treated.
Thrombolytic agents include strepto-kinase; APSAC, a streptokinase derivative;tissue plasminogen activator (tPA; alteplase);
and reteplase (Retavase), a recombinant pro-tein derivative of tPA. While streptokinase isfar less expensive than tPA, the latter mayoffer a slight increase in initial opening ratesof the infarcted artery. However, unlikestreptokinase and APSAC, tPA and reteplasemust be immediately followed by infusion of heparin. Practically speaking, the choice of which agent to use is probably far less impor-
h h d i i i i i h
Table 5
Absolute contraindicationsPrevious hemorrhagic stroke at any time; other strokes or
cerebrovascular events within one yearKnown intracranial neoplasmActive internal bleeding (except menses)Suspected aortic dissection
Contraindications to Thrombolytic Therapy
-
8/12/2019 Cardiology - Update on CardioVascular Disease
20/36
administration of tPA was tested to determineif the infusion time could be further shortened.However, this regimen was associated withhigher mortality and a higher rate of intracra-nial hemorrhage than that associated with a90-minute infusion. 36 Therefore, infusion of tPA over a period of 90 minutes remains thepreferred regimen. Reteplase can be adminis-tered in two bolus doses given 30 minutesapart, but it has not demonstrated an addition-al survival benefit over tPA. 37 Unlike tPA,reteplase does not require dosage adjustmentaccording to weight.
IV heparin has become one of the stand-ard therapies in acute MI used for the first 24to 48 hours following tPA and reteplaseadministration to maintain patency of theinfarct-related coronary artery. IV heparin isa standard therapy for unstable angina,which may be difficult to differentiate fromacute MI with normal ECG and enzymes.This agent is probably not needed with strep-tokinase or APSAC because of their longerduration of action. 19 In fact, the use of IVheparin in conjunction with APSAC mayincrease the risk of serious intracranial hem-orrhage. 38 To reduce this risk during throm- bolyti c therapy, the American College of Cardiology/American Heart Association(ACC/AHA) Task Force has recently recom-mended that partial thromboplastin time(PTT) be lowered to between 50 and 75 sec-onds (1.5 to 2.0 times control) from the previ-ous target of 60 to 85 seconds.
In acute MI patients without complica-tions, IV heparin has not been shown todecrease mortality over that with aspirin. 19Patients with the following characteristics whodo not receive thrombolytic therapy should begiven IV heparin, followed by oral warfarin(Coumadin) for at least three months:
History of systemic or pulmonaryembolism.
Echocardiographic evidence of muralthrombosis.
Large acute anterior MI. Severe LV dysfunction, cardiomyopa-
thy, or HF. Chronic atrial fibrillation.
Primary Percutaneous Transluminal Coro-nary Angioplasty (PTCA). Andreas Grntzigperformed the first balloon angioplasty at theUniversity of Zrich in 1977, which was thefirst time that coronary artery disease wastreated without major cardiovascular surgery.Since then, marked advances in the procedurehave occurred. If performed promptly inappropriate patients, PTCA may yield superi-or results to those of thrombolysis. The proce-dure is particularly beneficial in patients inwhom thrombolysis is contraindicated,patients in cardiogenic shock, and patientswho are hemodynamically unstable. 39
According to ACC/AHA guidelines foracute MI, concern that a routine policy of pri-mary PTCA will result in unacceptable delaysin achieving reperfusion in a significant num- ber of patients, and less than optimal out-
Table 6
Expected
Eli i i f i H i All i A i i
Comparison of Selected Thrombolytic Agents
-
8/12/2019 Cardiology - Update on CardioVascular Disease
21/36
comes if performed by less experienced opera-tors, has led to the recommendation of strictperformance criteria. 19 The current guidelinesstate that as an alternative to thrombolytictherapy, balloon dilation should be achievedwithin 60 to 90 minutes of diagnosis of MI, theoperator should perform 75 PTCAs per year,and the treatment center should perform atleast 200 procedures per year. In addition, car-diologists and cardiac centers must have docu-mented clinical success rates in achievingperfusion and preventing emergency coronaryartery bypass graft (CABG), stroke, and death.Thus, since only about 20 percent of hospitalsin the United States have the capacity to per-form PTCA under the appropriate conditions,the focus of treatment for most patients mustremain thrombolytic therapy. However, morethan 70 percent of patients are within 30 min-utes of a catheterization laboratory. The role of coronary stent placement with PTCA in acuteMI awaits further trials. 19,40
Beta-blockersBeta-adrenergic blockers are still underutilizedin acute MI. 41 They are administered intra-venously in fewer than 15 percent of patientsduring the acute phase of acute MI and orallyin less than 40 percent of patients to preventreinfarction. Beta-blockers have many benefi-cial effects, including reduction in the follow-ing: myocardial oxygen demand, SNS blockade, anti-ischemic effects, anti-arrhyth-mic effects, acute infarct size, and associatedcomplications and reinfarction in patients alsoreceiving thrombolytic therapy. When contin-ued orally after infarction, these drugs signifi-cantly reduce the incidence of sudden death.
Beta-blockers appear to be most effec-tive for myocardial preservation when
d d h h f h f
to a maximum of 0.1 mg per kg IV. Initiationof an oral beta-blocker within 30 to 60 min-utes after completion of the IV infusionshould be strongly considered as a secondarypreventive measure. 19
ACE InhibitorsRelatively recent additions to the treatment of acute MI are ACE inhibitors. Their major bene-fit in the treatment of acute MI relates to theirability to limit the degree of ventricular remod-eling after a large infarction, which may ulti-mately reduce the risk of developingmalignant ventricular arrhythmias or HF. Theymay also retard the atherosclerotic process andprotect against future ischemic events. 8
ACE inhibitors are indicated in patientswith acute MI, and patients who present withanterior wall injury, acute clinical HF, asymp-tomatic LV dysfunction (ejection fraction
-
8/12/2019 Cardiology - Update on CardioVascular Disease
22/36
The use of CCBs in patients with anacute MI should be restricted to cases inwhich a beta-blocker cannot be used and yetangina or rapid atrial fibrillation or flutterrequires therapy. The agent of choice in thiscase would be verapamil or diltiazem.Nifedipine (Adalat, Procardia) and otherdihydropyridine CCBs are best avoided because of their adverse effect on mortality inacute MI patients.
Magnesium. The usefulness of magne-
sium administration in patients with acuteMI is uncertain. Magnesium evokes systemicand coronary arterial vasodilation, inhibitsplatelets, stabilizes myocardial cell mem- branes, and may reduce the incidence of arrhythmias. In the placebo-controlledLIMIT-2 Trial, which evaluated 2,000patients, there was a 28-percent reduction inmortality in patients with acute MI whoreceived magnesium infusion. 44 The subse-quent ISIS-4 Trial, which had a much larger
Figure 2
Algorithm for a suggested approach tocost-effective, risk-stratification and man-agement after acute myocardial infarction(MI). This approach entails risk stratifica-tion and initiation of preventive therapyin all patients before discharge, includingthose without symptoms. Patients withpersistent or recurrent symptoms of car-diac failure, ischemia, or ventricular
arrhythmias (unstable condition) shouldundergo direct coronary angiography,followed by myocardial revascularization(percutaneous transluminal coronaryangioplasty [PTCA] or coronary artery bypass graf t surgery [CABG] whenappropriate). Patients who appear clini-cally stable after an acute MI may or maynot have evidence of left ventricular (LV)dysfunction. Patients with no evidence of LV dysfunction should undergo submax-imal treadmill exercise testing (ET).Patients with evidence of LV dysfunctionshould undergo echocardiography toassess LV function. If ejection fraction is40 percent, ET should be performed todetect myocardial ischemia. If the ejectionis
-
8/12/2019 Cardiology - Update on CardioVascular Disease
23/36
patient base, found no benefit on acute MImortality resulting from the administrationof magnesium. 31 Unfortunately, study para-meters were different in these two trials, inthat most patients in ISIS-4 received throm- bolytic therapy, but were not started on mag-nesium for up to 10 hours. In contrast,patients in LIMIT-2 generally did not receivethrombolytic therapy and were given IVmagnesium much soonerat an average of three hours after the onset of symptoms. It istherefore difficult to know how best to inter-pret these conflicting results. What can besaid is that magnesium is indicated in treat-ment of patients with acute MI whose serumlevels of this cation are low. Magnesium mayalso be given to patients who are suspected of having low body stores of this cationevenif their serum level is normal. This includespatients with other electrolyte abnormalities,patients taking digoxin or diuretics, andthose with a history of alcohol abuse.Although dosing of magnesium is empiric, itshould be kept in mind that a total of 18 g of IV magnesium were administered in theLIMIT-2 trial over a period of 24 hours inacute MI with only minimal adverse effects.In patients deficient in magnesium, onemight therefore safely infuse several gramsover a period of hours (if patients do nothave renal insufficiency).
Post-MI Risk Stratification andManagement
The survivor of an acute MI is, virtually bydefinition, a patient at high risk for subse-quent coronary events. Each year, almost 1million Americans suffer an acute MI; oneyear later, mortality may be more than 10percent. Recent advances in pharmacologicand interventional therapy have resulted in awide array of modalities that can reduce mor- bidity and increase long-term survival inacute MI survivors.
Whereas approximately 20 percent of patients with acute MI fall into a higher-risk group (recurrent angina, HF, malignant ven-tricular arrhythmias) and are likely to requiretimely interventional therapy, the remainingpatients must also be evaluated for their risk of subsequent coronary events. Three risk factors have been recognized as primarydeterminants of posthospital mortality: LVfunction, residual myocardial ischemia, andcardiac arrhythmias. Of these, LV function isprobably the most important.
Recently published guidelines for man-aging patients following acute MI suggestassessment of LV function in such patients(Figure 2).45 Echocardiography is a convenient,noninvasive modality for accomplishing suchevaluation, but radionuclide ventriculographycan also be used. One-year mortality followinginfarction is as low as 3 percent with a normalresting LVEF of greater than 50 percent. Mor-tality increases to more than 40 percent if LVEF is less than 30 percent. Long-term thera-py with an ACE inhibitor is recommended forall patients with significant LV dysfunction(LVEF < 40 percent).46-48
Modification of coronary risk factors isessential for effective secondary prevention,and the positive effects of risk-reduction
Table 7
Cigarette smoking should be stopped. Strategies include direct and strongadvice from the physician and advising participation in a formal smokingcessation program. Oral or transcutaneous nicotine replacement therapymay be useful as a temporary adjunct but should not be given in the early
Recommendations for Reducing Coronary Risk Factorsin Patients After Acute MI
-
8/12/2019 Cardiology - Update on CardioVascular Disease
24/36
Figure 3
Early medical therapy can reduce the rates of morbidity and mortality associated with acute myocardialinfarction (MI). Providers must educate patients about the symptoms that they might have during a coro-nary occlusion, what steps to take if symptoms occur, and the importance of contacting emergency med-
ical services immediately. All staff members of the health care office should understand the actions thatshould be taken when a patient who has symptoms telephones or walks into the office and seeks advice.An algorithm for triage may help staff members identify which patients need emergency referral.
Nitroglycerin oraspirin previously
prescribed?
Symptomsstill present?
Call emergency
Patient reports chest pain or other symptomsof acute myocardial infarction (ask how long
symptoms have been present).
History of myocardialinfarction, coronary heart disease, or
cerebrovascular or peripheralvascular disease?
Advise patient to:Take one dose of nitroglycerin and waitfive minutes. Repeat twice, if needed,five minutes apart.
Chew an adult (325 mg) uncoatedaspirin tablet.
(Meanwhile, place patient on hold andpage physician. If contact with patientis lost, call emergency medical
Yes
Yes
Yes
No
No
No
-
8/12/2019 Cardiology - Update on CardioVascular Disease
25/36
Cardiac Arrhythmias
(2.49 mmol per L); high-density lipoprotein(HDL) cholesterol, greater than or equal to 35mg per dL (0.91 mmol per L); and triglyc-erides, less than 140 mg per dL (1.58 mmol perL). Evaluation of lipid levels should be per-formed at the time of hospital admission, because values become altered during acuteMI. Lowering LDL levels as much as possible(ideally to below 100 mg per dL) followinginfarction is believed to stabilize the athero-sclerotic plaque and make it less likely to sub-sequently rupture. As a result, strongconsideration should be given to treating allacute MI survivors with an abnormal lipidprofile using a statin type drug.
Hypertension can increase one-year post-acute MI mortality by 50 percent; control of hypertension favorably affects prognosis.Appropriate nondrug and pharmacologic ther-apy can be combined to achieve a blood pres-sure goal of 140/90 mm Hg. Sodium restriction,weight reduction, limiting of alcohol intake toless than two drinks per day, and exercise areinitial recommendations, followed by treatmentwith a beta-blocker, ACE inhibitor, and/orother suitable agents as needed.
Carefully monitored and graduatedaerobic exercise increases functional capacityand reduces myocardial oxygen demand at agiven workload, thereby helping to avert
myocardial ischemia and angina. In addition,exercise promotes weight loss, blood pres-sure reduction, decreases in triglyceride andLDL cholesterol levels, and increases in HDLcholesterol level. In stable patients, exercise isusually recommended at an intensity of 60 to75 percent of predicted maximal heart ratefor 20 to 40 minutes, three to five times perweek. Referral to a formal cardiac rehabilita-tion program is recommended when feasibleto optimize safety in the conditioningprocess. Adherence to therapeutic regimensis clearly improved in these programs because of the expertise of the staff and thesupportive environment offered. Meta-analy-sis of rehabilitation programs shows a reduc-tion of 20 to 25 percent in cardiovascular andall-cause mortality in patients who participat-ed and kept with the program. 50
Patients at increased risk for subsequentMI must be educated on the actions theyshould take if symptoms of acute MI occur.In addition, all office staff members should be given clear instructions on the actions totake when a patient with symptoms sugges-tive of an acute MI calls or walks into theoffice to seek advice. An office telephonetriage algorithm for such situations has beendeveloped by the National Heart Attack Alert Program ( Figure 3).29
Epidemiology and Scope of ProblemCARDIAC ARRHYTHMIAS ARE EXCEEDINGLY COM-mon, regardless of the individuals state of health. The following discussion addressesthe arrhythmias that are most often seen inclinical practice: atrial fibrillation (AF), parox-
The foremost consideration whenevaluating a patient with new-onset AF ishemodynamic stability. Patients who arehemodynamically unstable require immedi-ate synchronized cardioversion, at an initialenergy of 200 J. However, the majority of
-
8/12/2019 Cardiology - Update on CardioVascular Disease
26/36
Work-up
Evaluation of AF is aimed at identifying theunderlying cause and should include a care-ful history (with particular attention to cluesto alcohol or drug abuse); laboratory testing,including thyroid function studies, a com-plete blood count (CBC) and chemical profile;a chest x-ray to assess the presence of pul-monary disease and HF, a 12-lead ECG, andan echocardiogram. Despite its expense, anechocardiogram provides invaluable infor-mation for determining the precipitatingcauses of AF. In addition, determination of the left atrial size by M-mode echocardiogra-phy helps gauge the likelihood that AF can be converted and a sinus rhythm maintained(which is less likely if the left atrial diameteris greater than 45 mm). Finally, left atrial sizeand LV function provide insight into the like-lihood of thromboembolism, with this com-plication being more likely if the left atrium isenlarged and LV function impaired.
The images provided by transesophagealechocardiography (TEE) are clearly superior tothose obtained with two-dimensional or M-mode echocardiography for detecting atrialthrombi. However, since TEE is invasive, sig-nificantly more expensive and not infallible fordetecting patients at risk for stroke, 53 routineprecardioversion TEE is not recommended.
Slowing the RateDigoxin. Once it is established that the patientwith AF is hemodynamically stable and eval-uation is initiated, management is directedtoward slowing the ventricular response.Although digoxin has been the most com-monly used drug in the past for treating new-onset AF, its choice may be less than optimal.Digoxin does not facilitate conversion of AFto sinus rhythm in patients without HF. 54
and IV form in slowing the ventricularresponse to rapid AF. Of the two, diltiazemhas a lesser hypotensive and negativeinotropic effect, and, when given by IV infu-sion, the dose can be carefully titrated.
Beta-blockers.IV or oral beta-blockers arealso highly effective in slowing the ventricu-lar response to rapid atrial fibrillation or flut-ter. The ultra-short acting agent esmolol(Brevibloc) has the advantage of rapid onsetof action and short half-life in case the drugneeds to be stopped. Alternatively, other beta-blockers (such as metoprolol or propran-olol) may also be used. An important point toemphasize is that IV infusion of a beta-block-er should not be attempted following IV infu-sion of verapamil or diltiazem, because thesynergistic action of these drugs may pro-duce asystole. As a result, most physiciansselect either a beta-blocker or verapamil ordiltiazem as their rate-slowing agent of choice.
Table 8
Permission to reproduceTable 8 on CD-ROM wasnot granted in time forproduction. Please referto original print version.
-
8/12/2019 Cardiology - Update on CardioVascular Disease
27/36
rhythm will occur within 12 to 24 hours, evenif no underlying cause can be found. There-fore, in hemodynamically stable patients,antiarrhythmic therapy aimed at convertingthe AF might best be delayed for at least 24hours. If the AF persists beyond 24 hours andthe patient is a suitable candidate, medicalconversion should be attempted. Poor candi-dates for conversion include patients withlong-standing AF (more than six to 12 months)or a markedly dilated left atrium. Suchpatients are unlikely to maintain a sinusrhythm, even if initial conversion is successful.
In general, class IA antiarrhythmicagents, such as disopyramide (Norpace), pro-cainamide (Pronestyl), and quinidine, are usedfirst for medical conversion of AF, with the lat-ter being the agent that has been most com-monly selected. Although these medicationsare effective in converting AF to sinus rhythminitially, long-term therapy is not benign andhas been associated with a threefold increasein mortality within two years. Quinidine isalso associated with diarrhea and gastroin-testinal intolerance, which can sometimes belessened by using the gluconate form of thedrug. On average, quinidine results in a dou- bling of serum digoxin levels, although manypatients have either a much lower or higherserum level when given this drug. In practice,many physicians halve the dose of digoxin before beginning quinidine therapy. Others donot alter the daily digoxin dose, but insteadfollow the patient closely. Either approach isacceptable. Procainamide offers severaladvantages over quinidine since it can beadministered intravenously and it is often welltolerated. Unfortunately, a lupus-like syn-drome may develop in patients treated chroni-cally with procainamide.
Other antiarrhythmics, either class IC
utes. In about half of these patients, conver-sion is accomplished within the initial 10-minute infusion. If needed, the dose may berepeated. In approximately 5 percent of patients, there is a risk of torsades de pointes.
If attempts at medical conversion of AFto sinus rhythm fail, electrical cardioversionshould be considered. Electrical cardiover-sion is not an innocuous procedure, and isassociated with a 1-percent risk of stroke,even in patients who are being adequatelytreated with anticoagulants. It has been rec-ommended that cardioversion not be per-formed on an outpatient basis.
Prevention of ThromboembolismThe final step in managing a patient with AFis the prevention of thromboembolism, towhich patients with AF are particularly sus-ceptible. Without long-term anticoagulation,the risk of embolic stroke in patients with AFis about 5 percent a year, with a lifetime risk of about 35 percent. If the patient has AF for 48hours or more, anticoagulation should bestarted before conversion (either medically orelectrically) is considered. A therapeutic inter-national normalized ratio (INR) (between 2-3)should be maintained for three weeks prior toattempted conversion. If conversion fails andAF persists, chronic rate control with digoxin,a CCB, or a beta-blocker is indicated, alongwith chronic anticoagulant therapy. All stud-ies in which this issue has been examined haveconcluded that long-term anticoagulation of patients with AF results in a significant overallreduction (68 percent) in the risk of stroke. 56
Anticoagulation with warfarin is clearlyindicated for high-risk patients with AF, whoare defined as those older than 65 years of ageor with underlying heart disease. Otherhigher-risk groups include those with hyper-
-
8/12/2019 Cardiology - Update on CardioVascular Disease
28/36
heart disease or hypertension. Such patientscan probably be treated with aspirin, 325 mg,instead of warfarin because of their low risk of embolization. 56 Although aspirin is not aseffective as warfarin in preventing stroke, theincreased risk of bleeding associated with war-farin use cancels out its benefit in these patientsin whom the risk of stroke is low.
Atrial FlutterThe initial clinical approach to atrial fibrilla-tion and atrial flutter is similar in many ways.Assuming the patient is hemodynamically sta- ble, similar medications may be tried in anattempt to slow the ventricular response toatrial flutter and convert the arrhythmia tosinus rhythm. The new antiarrhythmic agentibutelide is the most effective medical treat-ment for converting atrial flutter to sinusrhythm, being successful in up to two-thirdsof cases. If the rhythm fails to respond to oneor two doses of ibutelide, synchronized car-dioversion has an extremely high success rate,often at relatively low energy levels. Atrialactivity in atrial flutter is organized, and therisk of thromboembolism is therefore muchless than in AF; however, the same decision-making process is recommended for bothrhythms with regard to long-term anticoagula-tion to reduce the incidence of stroke. Selectedpatients with classic atrial flutter who do notrespond to the above treatment measures may be successfully treated with catheter ablation.
Paroxysmal SupraventricularTachycardia (PSVT)PSVT is a common arrhythmia that occursamong all age groups in both ambulatory andinpatient settings. Although most patients withPSVT are symptomatic in some way from thisarrhythmia (with lightheadedness, awareness
lacking on the surface ECG. Terminology of the various forms of PSVT may be confusing, because there are a number of di fferentmechanisms that may produce a similar elec-trocardiographic picture. Most commonly thephenomenon of reentry exists, in which theelectrical impulse continually circulates overa well defined reentrant pathway. In a prima-ry care setting, the overwhelming majority of adults who present with the ECG picture of PSVT (regular narrow complex tachycardiaat a rate of between 140-240 beats per minutewithout evidence of normal atrial activity)will have a reentrant tachycardia in which atleast a portion of the reentry circuit involvesthe AV node. Surprisingly, up to one-third of these patients have an accessory pathwayinvolved in reentry circuit that is concealed(not manifested by delta waves on the surfaceECG), reflecting the fact that conduction onlyoccurs over the accessory pathway in retro-grade fashion. 57 This reentrant form of PSVTis said to manifest orthodromic conduction, because the electrical impulse travels firstdown the normal AV nodal pathway andthen back up the accessory pathway. As aresult of this sequence of activation, the usualECG hallmarks of an accessory pathway(short PR interval, delta wave, QRS widen-ing) are not seen.
Clinically, initial management of patients with PSVT from a concealed accesso-ry pathway (i.e., with orthodromic conduc-tion first through the AV node, and then back up the accessory pathway in retrograde fash-ion) is similar to management of the morecommon form of PSVT in which the entirereentry circuit is contained within the AVnode (atrioventricular nodal reentrant tachy-cardia, or AVNRT). In both cases, thearrhythmia behaves as an AV nodal depen-
-
8/12/2019 Cardiology - Update on CardioVascular Disease
29/36
tion of action. If this occurs, either adenosinemay be repeated, or use of a longer actingagent (verapamil or diltiazem) may be tried.Alternatively, use of digoxin or a beta-blockercould be considered. The addition of an anxio-lytic agent may be a helpful adjunct for treat-ment of PSVT because it reduces the anxietythat often accompanies this arrhythmia, aswell as the physiologic effect it may have inattenuating sympathetic tone and thereforealtering conduction properties in one or botharms of the reentrant pathway.
Long-term management of the patientwith PSVT includes elimination of all stimu-lants (including caffeine), alcohol, tobacco,and other substances of possible abuse, sym-pathomimetic agents, and diet pills. Selectedpatients can be taught the Valsalva maneu-ver, to be performed when necessary.
Consideration may sometimes be givento administration of drugs on an episodic basisfor patients with infrequent attacks, or dailyfor more frequent occurrence. Intermittenttherapy may be appropriate for selected indi-viduals whose PSVT only occurs at infrequentintervals, in which the treating physician pre-scribes the use of verapamil, diltiazem, or a beta-blocker that may be taken by the patientat home at the time of the episode. Such thera-py should not be used unless the mechanismof the arrhythmia has been clearly defined.However, when appropriate, use of intermit-tent therapy for treatment of PSVT is wellreceived by patients because it restores a mea-sure of control over their condition and avoidsthe need to take a medication daily when theirarrhythmia only occurs at infrequent intervals.The addition of a benzodiazepine to the rate-slowing regimen may be beneficial because itreduces the anxiety that accompanies PSVTduring the time that it takes the oral regimen
the potential to suddenly develop antegrade(forward) conduction down the accessorypathway in association with tachycardia. Inparticular, development of atrial fibrillationin such a patient with antidromic conductionover an accessory pathway may lead toexcessively rapid ventricular rates (of 250 beats per minute, or more) with associatedlife-threatening hemodynamic compromise.Electrophysiologic study of these patientsallows identification of the culprit accessorypathway in most cases, which may then beablated with cure of the arrhythmia.
Finally, it should be appreciated that asmall percentage of patients who present withthe ECG picture of PSVT in reality have anAV nodal independent mechanism respon-sible for their arrhythmia. This group of tachy-arrhythmias include entities such as sinusnode reentry, intra-atrial reentry, and ectopic(automatic) atrial tachycardia, as may occurwith digitalis toxicity. The importance of beingaware of these much less commonly occurringarrhythmias is that the usual measures usedfor treatment of AV nodal dependent PSVTrhythms may not be effective if the AV node isnot involved in the genesis and/or mainte-nance of the arrhythmia. For example, with-holding digoxin may be all that is needed forresolution of atrial tachycardia with block thatarises as a manifestation of digoxin toxicity.Clinically, sinus node reentrant tachycardiaand intra-atrial reentrant tachycardia are bothoften resistant to treatment with standardantiarrhythmic agents. Early referral for elec-trophysiologic study should be strongly con-sidered for such patients.
Ventricular ArrhythmiasVentricular arrhythmias are a broad categoryof conditions that include premature ventric-
-
8/12/2019 Cardiology - Update on CardioVascular Disease
30/36
cance. PVCs themselves are not a cause of mor-tality, unless they lead to sustained VT or VF.Clinically, one should look first for disordersassociated with increased catecholamine levels,hypoxia, electrolyte abnormalities, drug toxici-ty, HF, and ischemia. These conditions should be corrected if they exist. If PVCs persist,Holter monitoring could be considered in anattempt to determine if more malignant formsare present. In the absence of underlying heartdisease, PVCs, even if frequent, are generally benign and need not be treated. If the patient issymptomatic from such PVCs, a beta-blocker isthe antiarrhythmic agent of choice.
In contrast, if PVCs occur in a patientwho does not have underlying heart disease,cardiovascular risk is increased. The problem isthat with rare exceptions, antiarrhythmic thera-py has not been shown to increase survival insuch patients. If treatment is deemed neces-sary, a beta-blocker is again the agent of choice.It should be kept in mind that antiarrhythmicdrugs are not benign and, in 5 to 10 percent of cases, may be associated with a proarrhythmiceffect, in which they paradoxically exacerbatethe arrhythmia. This is a major reason for thereluctance to treat PVCs in recent years.
Ventricular tachycardia. When shortepisodes of VT occur in a normal heart, theyare usually benign. However, once VT isfound, intensive cardiac evaluation is usuallyindicated to assess the patient for underlyingheart disease. If heart disease is not present,no therapy may be needed.
On the other hand, when VT occurswith organic heart disease, the risk of VF ishigher and, therefore, the risk of sudden car-diac death increases. Full evaluation withechocardiography, cardiac catheterization,and/or electrophysiologic studies should bestrongly considered. Treatment options
of an ICD appeared to benefit a select group of patients with nonsustained VT and impairedleft ventricular function following myocardialinfarction. 58 Although additional data are need-ed to confirm these results, it would seem thatpatients with sustained VT and underlyingheart disease should be referred for extensivecardiac evaluation including electrophysiologicstudy. Management decisions are less clear atthis time for patients with asymptomaticepisodes of nonsustained ventricular tachycar-dia (NSVT) who have underlying heart disease.At the least, control of potentially exacerbatingcauses of ventricular arrhythmias (wheneverpossible) is essential in such patients, includingcorrection of electrolyte abnormalities andtreatment of ischemia, heart failure and/orhypoxia (Table 9). Preference should be given touse of ACE inhibitors and beta-blockers whenappropriate for treatment of these underlyingconditions. Whether or not patients with
Table 9
Permission to reproduceTable 9 on CD-ROM wasnot granted in time forproduction. Please referto original print version.
-
8/12/2019 Cardiology - Update on CardioVascular Disease
31/36
1. Shipley JB, Hess ML. Inotropic therapy for thefailing myocardium. Clin Cardiol 1995;18:615-9.
2. Konstam M, Dracup K, et al. Heart failure: man-agement of patients with left ventricular systolicdysfunction. Quick Reference Guide for Clini-cians No. 11. AHCPR Publication no. 94-0613.Rockville, Md.: Agency for Health Care Policyand Research, Public Health Service, U.S. Depart-ment of Health and Human Services, June 1994.
3. McKee PA, Castelli WP, McNamara PM, KannelWB. The natural history of congestive heart fail-ure: the Framingham Study. N Engl J Med1971;285:1441-6.
4. Aronow WS. Management of congestive heartfailure in the elderly patient. Compr Ther1995;21:329-38.
5. Deedwania PC. Clinical profile of fosinopril, anovel phosphinic acid ACE inhibitor for thetreatment of heart failure. Heart Failure1995;June/July:125-36.
6. Demopoulos L, LeJemtel TH. Peripheral factorsin the management of congestive heart failure.Cardiovasc Drugs Ther 1994;8:75-82.
7. Eagle KA, Quertermous T, Singer DE, et al. Left
ventricular ejection fraction. Physician estimatescompared with gated blood pool scan measure-ments. Arch Intern Med 1988;148:882-5.
8. Lonn EM, Yusuf S, Jha P, et al. Emerging role of angiotensin-converting enzyme inhibitors incardiac and vascular protection. Circulation1994;90:2056-69.
9. Pitt B, Segal R, Martinez FA, et al. Randomizedtrial of losartan versus captopril in patients over65 with heart failure (Evaluation of Losartan inthe Elderly Study, ELITE). Lancet 1997;349:747-52.
10. The Digitalis Investigation Group. The effect of digoxin on mortality and morbidity in patientswith heart failure. N Engl J Med 1997;336:525-33.
11. Slatton ML, Irani WN, Hall SA, et al. Does digox-in provide additional hemodynamic and auto-nomic benefit at higher doses in patients withmild to moderate heart failure and normal sinusrhythm? J Am Coll Cardiol 1997;29:1206-13.
12. Uretsky BF, Young JB, Shahidi FE, Yellen LG,Harrison MC, Jolly MK. PROVED InvestigativeGroup. Randomized study assessing the effect
patients with chronic heart failure. N Engl J Med1996;334:1349-55.
17. Packer M, OConnor CM, Ghali JK, et al.Prospective Randomized Amlodipine SurvivalEvaluation Study Group. Effect of amlodipineon morbidity and mortality in severe chronicheart failure. N Engl J Med 1996;335:1107-14.
18. Mulder P, Richard V, Compagnon P, et al.Increased survival after long-term treatmentwith mibefradil, a selective T-channel calciumantagonist, in heart failure. J Am Coll Cardiol1997;29:416-21.
19. Ryan TJ, Anderson JL, Antman EM, et al. ACC/AHA guidelines for the management of patientswith acute myocardial infarction. a report of theAmerican College of Cardiology/American HeartAssociation Task Force on Practice Guidelines(Committee on Management of Acute MyocardialInfarction). J Am Coll Cardiol 1996;28:1328428.
20. The registry of the International Society forHeart and Lung Transplantation: ninth officialreport-1992.