Cardiology & Oncology Drug Development & Regulation
6
March 2009 Vol 9 No 3 www.drugdeliverytech.com IN THIS ISSUE Combination Devices 18 Abhijit Gokhale, PhD Excipient Sourcing 22 Alen Guy, PhD Solid Dose Injection 24 Charles Potter, PhD Nanomedicine Market 32 Bill Martineau, MBA Analytical Testing Labs 62 Cardiology & Oncology 68 Stuart L. Cantor, PhD The science & business of drug development in specialty pharma, biotechnology, and drug delivery FEATURING Xiaochun Yu, PhD A New Approach to Threshold Evaluation & Quantitation of Unknown Extractables & Leachables Using HPLC/CAD Ms. Cindy H. Dubin Proteins & Peptides: Dependent On Advances in Drug Delivery? Mr. Mike Mesa From Battlefield to Backpack: Evolution of the Auto-Injector INTERVIEW WITH DEPOMED’S PRESIDENT & CEO CARL A. PELZEL
description
Discusses CMC issues regarding Drug-eluting coronary stents (DES) & Oncology drugs.
Transcript of Cardiology & Oncology Drug Development & Regulation

March 2009 Vol 9 No 3 www.drugdeliverytech.com
IN THISISSUE
CombinationDevices 18Abhijit Gokhale, PhD
ExcipientSourcing 22Alen Guy, PhD
Solid DoseInjection 24Charles Potter, PhD
NanomedicineMarket 32Bill Martineau, MBA
AnalyticalTesting Labs 62
Cardiology &Oncology 68Stuart L. Cantor, PhD
The science & business of drug development in specialty pharma, biotechnology, and drug delivery
FEATURING
Xiaochun Yu,PhDANewApproach toThreshold Evaluation&Quantitation ofUnknownExtractables& LeachablesUsingHPLC/CAD
Ms. Cindy H.DubinProteins & Peptides:Dependent OnAdvances in DrugDelivery?
Mr. MikeMesaFrom Battlefield toBackpack: Evolutionof the Auto-Injector
INTERVIEW WITHDEPOMED’S
PRESIDENT & CEO
CARL A. PELZEL
* DDT March 2009 Covers:DDT Cover/Back April 2006.qx 2/26/09 11:31 AM Page 2

68
TherapeuticFocus
Cardiology & Oncology Drug Development& Regulation
SPEC
IALT
YPH
ARM
AM
ARCH
2009
Vol9
No3
IntroductionHeart disease and cancer are still the
two leading causes of mortality in the
world. Recent data show that in the US,
the total direct and indirect costs
associated with treating cardiovascular
diseases and stroke are estimated to be
$449 billion, by comparison, the
estimated costs for all types of cancer
was $219 billion.1 Sales of drugs treating
cardiovascular disorders, hypertension,
and cancer accounted for roughly 31% of
the $287 billion prescription
pharmaceutical market in 2007; these
drugs continue to be the largest therapy
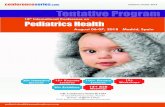
classes in the US (Figure 1).2 In the
cardiology sector, Pfizer’s Lipitor®
amassed sales revenues of $12.7 billion
in 2007, making it the best selling drug
in pharmaceutical history. Not to be
outdone, the biotech industry has
likewise developed a number of
successful blockbuster cancer therapies
as intravenous solutions or vaccines,
including Herceptin® and Avastin®,
monoclonal antibody-based therapies to
treat breast and colon cancer,
respectively, and Gardasil®, a vaccine
against cervical cancer.3 Sales of cancer
drugs are projected to double and could
reach $80 billion by 2012, according to
IMS Health.
There are several reasons for this
increased sales growth, which include
extended lifespan, increases in obesity
and hypertension in the US population,
an increasing number of patients on
chemotherapy in major markets, longer
treatment periods for a growing number
of patients, and the
greater availability
of more expensive
and modern
targeted therapies
to treat these
diseases. However,
hotly debated
issues have risen
over the long-term
safety of coronary
drug-eluting stents
(DES), efficacy of
beta-blockers in
treating
hypertension, and
the long-term
safety of statins. In
the oncology
sector, there has
been an increase in
the development of highly potent,
hydrophobic compounds, and difficulty
in ensuring their solubility as well as
specificity to target the tumor site.
Because oncology drugs are cytotoxic,
maintaining containment facilities during
the developmental phase for these actives
can become expensive. Furthermore,
with both of these drug classes,
Figure 1.
By: Stuart L. Cantor, PhD, Senior Scientist, and Kadriye Ciftci, PhD, Senior Director Drug Delivery,ICON Development Solutions
68-73-DDT MAr 2009 -SP-Therapeutic Focus:Layout 1 2/26/09 11:48 AM Page 68

69
SPEC
IALT
YPH
ARM
AM
ARCH
2009
Vol9
No3
difficulties proving efficacy or
unexpected safety concerns, particularly
during later-stage development amid
Phase III trials, can be particularly
challenging.
The increased number of
blockbuster drugs that are scheduled to
lose patent protection in the coming
years (Figure 2), coupled with the FDA’s
Amendments Act of 2007 granting
sweeping new powers to the agency for
such tasks as requiring drug makers to
do post-marketing clinical trials, are
making the regulatory climate more
expensive and time-consuming for the
pharmaceutical industry. Furthermore,
because drug safety issues are
paramount due to highly publicized
cases like Vioxx®, the FDA is closely
scrutinizing safety data while improving
its management of safety signals.
Drug DevelopmentOncology drugs in development are
generally highly potent as well as
cytotoxic; some may even have narrow
therapeutic windows. It is important to
assess the safety of these compounds
early on to determine that they are
effective in treating the disease process
while not damaging healthy tissue.
According to the M3 Guidance for
Industry, single-dose acute toxicity
studies are required to be performed for
pharmaceuticals and should be
evaluated in two small mammalian
model species before the first human
exposure.4
The ratio of time for animal to
human testing is 1:1, meaning that the
FDA will allow a company to conduct
human clinical trials for only the same
time period in which animal data has
been supplied. Sometimes, the agency
can also request that safety and/or
toxicity data in a non-human primate
also be supplied before an
Investigational New Drug (IND) can be
approved. A contract research
organization
(CRO) can assist a
company with
developing a
game plan for the
extent of both
preclinical animal
testing and future
clinical trials;
such services can
be outsourced by
start-up or virtual
companies with
limited in-house
drug development
resources. The
CRO can also
help the company
in its
correspondence
with the FDA and
offer guidance
during the critical pre-IND meeting.
Under current regulations, a sponsor is
permitted to start their clinical trials 30
days after filing its IND with the FDA
unless notified earlier that there are
issues with the application.
Recent reports from the
Pharmaceutical Research and
Manufacturers of America (PhRMA)
noted that 750 new medicines are being
tested in the fight against cancer, and
256 new medicines are in development
to treat cardiovascular diseases.5,6 While
there have been a number of successful
anti-neoplastic small molecules
launched over the years, such as 5-
fluorouracil, paclitaxel, and
doxorubicin, the focus has shifted away
from broad-acting cytotoxic drugs
toward the development of new
therapies directed against specific
molecular targets. Although biologics
and vaccines derived from larger protein
molecules offer promise in these
therapeutic areas due to their high
disease specificity and activity at
relatively low concentrations as
compared with small molecules,
physicochemical stability and potential
immunologic issues need to be closely
monitored and controlled to ensure a
drug product’s beneficial effects.
“In contrast to most drugs that are
chemically synthesized and with a
known structure, most biologics are
complex mixtures that are not easily
identified or characterized. Biological
products, including those manufactured
by biotechnology, tend to be heat
sensitive and susceptible to microbial
contamination,” says Paul Richards,
FDA Spokesperson at CBER.
“Therefore, it is necessary to use aseptic
principles from initial manufacturing
steps in order to ensure sterility of the
finished products, which is also in
contrast to most conventional drugs.”
Furthermore, vaccine clinical
development follows the same general
pathway as for drugs and other
biologics. However, due to the complex
nature of many vaccines, each lot must
be thoroughly tested for safety, sterility,
and potency by the manufacturer. These
tests, as well as many others that
manufacturers must perform, are
Table 2.
68-73-DDT MAr 2009 -SP-Therapeutic Focus:Layout 1 2/26/09 11:48 AM Page 69

70
SPEC
IALT
YPH
ARM
AM
ARCH
2009
Vol9
No3
specified in their biologic license
applications (BLAs). If the product is
subject to official release by the FDA’s
Center for Biologics Evaluation and
Research (CBER), the manufacturer
must submit samples of each production
lot to the Agency together with a release
protocol showing a summary of the lot
manufacturing history and the results of
all the manufacturer’s tests performed on
that lot, says Mr. Richards.
“The most challenging aspects to
developing these biologic drugs is the
design of efficient and robust
fermentation and purification processes
and the production of a stable
formulation,” says Peter Ihnat, PhD, Sr.
Principal Scientist, Protein Therapeutics,
Bristol-Myers Squibb.
Protein formulations can be
developed using either lyophilized
powders or liquid parenterals; however,
freeze-drying is not as popular an option
nowadays due to the increased cost and
longer development time required to
produce a successful formulation.
“Typically, the target level for
protein impurities for liquid formulations
is < 5%, and these are usually due to
oligomers or aggregates; however, due to
the immunogenic potential of these
compounds, impurity levels are
evaluated on a case-by-case basis.
Moreover, long-term protein stability is
monitored using at least two to three
orthogonal methods in addition to an in
vitro bioassay to assess biological
activity,” says Mr. Ihnat.
RegulatorySubmissions
The CTD or Common Technical
Document was developed to be used for
regulatory submissions and finalized as
the M4 Guidance for Industry in 2004.7,8
This table of contents format is highly
recommended for INDs, New Drug
Applications (NDAs), and Abbreviated
NDAs (ANDAs) from the US and
required for European and Japanese
submissions. Canadian INDs must also
be in CTD format; however, these are
referred to as CTAs or Clinical Trial
Applications for Phases I-III. The CTD
contains several modules with Modules 2
and 3 containing critical Chemistry,
Manufacturing, and Control (CMC)
information.
While Module 2 deals with both
non-clinical and clinical overviews and
summaries, the quality section or
Module 3 deals only with CMC issues
and provides information on the
physicochemical properties and control
of the drug substance as well as the
development, manufacture, and control
of the finished drug product. Modules 4
and 5 address non-clinical and clinical
study reports, respectively. Updates to
the IND data following Phase I-II trials
can be provided in information
amendments and annual reports;
however, the emphasis should be on
reporting significant changes that can
have a safety-related impact. CMC
development will continue in parallel
with the clinical development during
Phase III studies.9,10
If the CMC section will be written
for an already approved drug but a new
dosage form, the Drug Master File
(DMF) number, if available, can be
referenced for some of the pertinent
manufacturing information for the drug
substance. For all scientific data, the
FDA is particularly concerned that the
experimental study design and statistical
analysis be sound and free from flaws,
and requires a rationale and justification
used for final specifications selected as
well as the use of novel excipients and
any unusual tests performed.
Two other regulatory submission
pathways available are the 505(b)(2) and
combination product options. The
505(b)(2) route offers companies the
advantage of not having to supply the
safety and efficacy data on an already
approved drug product, and such filings
can be used to support new and
innovative drug delivery forms. Data
from published studies can even be
submitted to the FDA. However, the
company would need to provide
additional clinical data necessary to
demonstrate any safety and efficacy
differences between the original drug
and the 505(b)(2) drug. Some of the
different types of applications covered by
the section 505(b)(2) are:
• change in an active ingredient (ie,
different salt, ester, complex,
chelate, clathrate, racemate, or
enantiomer) for a listed drug
containing the same active
moiety;
• change in dosage form, strength,
formulation, dosing regimen, or
route of administration; and/or
• change from a prescription
indication to an over-the-counter
indication.
The important benefits of using the
505(b)(2) filing route are a faster
pathway toward regulatory approval
without giving the sponsor the burden of
supplying duplicate safety and efficacy
data on an already existing compound.
However, the FDA does still require that
a sponsor provide additional clinical
data, termed bridging studies, which are
necessary to support any changes or
modifications from the listed drug(s) to
the 505(b)(2) drug(s), and these studies
will allow extrapolation of the efficacy
and safety data. Furthermore, a
505(b)(2) applicant may qualify for 3 or
5 years of Hatch-Waxman marketing
exclusivity.11
The other non-traditional route for
regulatory approval deals with
combination products, such as coronary
DES, which are considered a drug-
device combination product under the
68-73-DDT MAr 2009 -SP-Therapeutic Focus:Layout 1 2/26/09 11:48 AM Page 70

71
SPEC
IALT
YPH
ARM
AM
ARCH
2009
Vol9
No3
Code of Federal Regulations (CFR) 21
CFR 3.2(e)(1). The Office of
Combination Products (OCP) at the FDA
assigns such products to a lead agency
center, based upon the product’s primary
mode of action. OCP ensures timely,
consistent pre-market review and
appropriate post-market regulation of
combination products by facilitating the
review process involving more than one
agency center. In this case, the
investigational device exemption (IDE)
application would be sent to the FDA’s
Center for Devices and Radiological
Health (CDRH) with significant
consultation by the Office of New Drug
Quality Assessment (ONDQA)/Division
of Cardiovascular and Renal Products.
Many scientific and regulatory issues
will arise due to the complex nature of a
coronary DES. Some important concerns
that would need to be evaluated and
discussed in a submission include acute
and chronic stent biocompatibility,
polymeric coating characterization (ie,
thickness, uniformity, integrity, adhesion
to stent), and drug release profile. The
predominant percentage composition of a
combination product does not dictate the
Agency center(s) where it is regulated,
rather, it is the primary mode of action or
the “most important therapeutic action of
a combination product” that determines
where a combination product will be
regulated. For example, DES submissions
are assigned to CDRH because the
device’s role in physically maintaining
vessel lumen patency provides the most
important therapeutic action of the
combination product. The drug plays only
a secondary role in reducing restenosis or
re-narrowing of the coronary arteries, a
phenomenon which is caused by the
body’s formation of scar tissue in
response to stent implantation.12
While the agency currently does not
require the use of Process Analytical
Technologies (PAT) for their submissions,
the use of PAT for CMC documentation
is looked upon favorably. PAT uses tools,
such as near-infrared (NIR) or Raman
spectroscopy, to provide real-time process
data. PAT finds wide applicability in the
pharmaceutical industry and can be used
to assess blend and content uniformity,
prediction of dissolution time, and can
determine the end-point of a coating or
drying operation. Not only can end-
product testing be reduced, which can
save a company money, but the FDA can
also provide some regulatory flexibility
for any process changes that could occur
in the future, provided that they are
accompanied by scientific justification.13
“The Agency considers PAT to be a
tool for designing, analyzing, and
controlling manufacturing through timely
measurements (ie, during processing) of
critical quality and performance attributes
of raw and in-process materials and
processes, with the goal of ensuring final
product quality. The goal of PAT is to
enhance understanding and control of the
manufacturing process and to facilitate
innovation in development,
manufacturing, and quality assurance by
focusing on process understanding. These
concepts are applicable to all
manufacturing situations,” says Jon E.
Clark, MS, Associate Director for the
Office of Pharmaceutical Science (OPS)
Policy Development at the FDA CDER.
Due to the serious nature of the
diseases they treat, both cardiology and
oncology drugs qualify under the fast-
track drug development program
classification. The three designations
given by the FDA are accelerated
approval, fast-track, and priority
review.14,15 In 1992, accelerated approval
for oncology drugs was codified into law
under Subpart H (21 CFR part 314.530)
and added to the new drug application
regulations. Accelerated approvals are
granted for the treatment of serious or
life-threatening conditions and a benefit
over available therapy exists.
This designation requires using a
surrogate endpoint for efficacy, ie, an
evaluation intended to substitute for a
clinical endpoint such as survival or
morbidity, and which is reasonably likely
to predict clinical benefit. Examples of
tumor assessment endpoints are response
rate to drug therapy or time to tumor
progression, measured using anatomic
imaging techniques. Once accelerated
approval has been granted, continued
marketing of the product will be
contingent on the sponsor’s providing
timely and conclusive evidence from
validation trials that establishes that the
experimental drug is safe and provides
tangible clinical benefit. The product
approval can be withdrawn if
confirmatory studies fail to show clinical
benefits, or if the drug sponsor fails to
conduct the confirmatory studies.
A fast-track status is granted by the
Agency for those drugs also developed to
treat life-threatening diseases and that
demonstrate the potential to address an
unmet medical need. In this instance, a
rolling NDA can be approved that allows
for completed sections of the NDA to be
submitted to the FDA on an ongoing
basis. The FDA strongly recommends
several meetings, including a pre-IND
consultation, meetings following Phases
I-II, and a pre-NDA meeting to expedite
the approval process. The other
designation, priority review, is for drugs
showing a significant therapeutic benefit
compared to the standard of care. In this
case, the FDA would review a NDA
within 6 months as opposed to the
standard review completion timeline of
10 months.
Outsourcing KeyCapabilities
In addition to hearing the term CRO
as a common buzzword these days, the
fact is that both small and large
pharmaceutical companies can benefit
from utilizing the added services and
expertise of a global CRO while focusing
on their core competencies. The CRO
68-73-DDT MAr 2009 -SP-Therapeutic Focus:Layout 1 2/26/09 11:48 AM Page 71

72
SPEC
IALT
YPH
ARM
AM
ARCH
2009
Vol9
No3
market size is currently estimated at about $15 billion in revenue per year and is
growing at a healthy annual rate of 14.8%. By 2010, the market is forecast to be in
the vicinity of $22.9 billion, according to Frost & Sullivan. A CRO should be chosen
carefully at the outset of a project after considering the budget, timelines, the range
of services provided, and the resources offered. A CRO can assist with the review and
editing of the regulatory submissions and can either represent the company as their
sole agent or accompany their client in meetings with the FDA. For smaller
companies with limited resources, limited regulatory expertise, and tight timelines,
meetings with the FDA early in the development process can alert the company if
they are going down the wrong pathway.
Meetings with the FDA can be arranged at both the pre-IND stage, where the
company can ask questions to see if they have done enough work to prove a drug’s
safety, and also before going through the time and expense for Phase III clinical trials
(an after Phase II meeting). These meetings are invaluable in identifying additional
safety, toxicity, or efficacy issues pertinent to cardiology and oncology IND/NDA
filings. More frequent interaction with the FDA would be recommended (ie, end of
Phase I meeting) if the drug would be marketed to a small patient population with a
rare disease or condition, ie, orphan drug classification for a disease affecting less
than 200,000 people in the US. Orphan drugs would also be granted accelerated
approval status, and NDAs are given a priority review timeline of 6 months.
A CRO can act as a regulatory resource for a company to guide them as to what
the minimum agency requirements are to prove safety and efficacy and which tests
would be superfluous. Another key advantage of using a CRO is that they have the
capability to offer their clients a strategic viewpoint on risk assessment and
management, and can additionally shoulder some of that risk in interactions with the
FDA. The Agency will take a global view of the scientific data to assess the risk-
benefit ratio, ie, the benefits of the drug substance and final drug product must far
outweigh any complications or potential risks to human health. The Agency also
examines what therapeutic advantages the new product has over therapies currently in
the market. Sometimes there is no information available on comparator products as
the regulatory submission is for a first-in-class therapy. In such instances, a CRO can
provide key information as it can draw from a wide knowledge base from past client
experiences with a variety of dosage forms. �
References1. Rosamond W, et al. Heart Disease and Stroke Statistics 2008 Update: A Report from the American Heart Association Statistics Committee and Stroke Statistics
Subcommittee. Circulation. [Available at: http://circ.ahajournals.org/cgi/content/full/117/4/e25 (DOI: 10.1161/circulationaha.107.187998); Accessed August 6, 2008].
2. Buono D. IMS study finds decline in prescription drug market growth. Drug Store News. (April 21, 2008) [Available at:
http://findarticles.com/p/articles/mi_m3374/is_5_30/ai_n25407255; Accessed July 30, 2008].
3. Lawrence S. Billion dollar babies-biotech drugs as blockbusters. Nature Biotechnol. 2007;25(4):380-382. [Available at: http://www.nature.com/naturebiotechnology ;
Accessed August 6, 2008].
4. FDA Guidance for Industry M3: Nonclinical Safety Studies for the Conduct of Human Clinical Trials for Pharmaceuticals. Center for Drug Evaluation and Research
(CDER) & Center for Biologics Evaluation and Research (CBER), (July 1997).
5. 2008 Report: Medicines in Development for Cancer. [Available at: http://www.phrma.org/files/meds_in_dev/Cancer2008.pdf; Accessed July 27, 2008].
6. 2007 Report: Medicines in Development for Heart Disease and Stroke. [Available at: http://www.phrma.org/files/Heart2007.pdf; Accessed July 27, 2008]
7. FDA Guidance for Industry M4: The CTD- Quality Questions and Answers/Location Issues. CDER & CBER, (June 2004).
8. FDA Guidance for Industry M4: The CTD- General Questions and Answers. CDER & CBER, (December 2004).
9. FDA Guidance for Industry: Content and Format of Investigational New Drug Applications (INDs) for Phase 1 Studies of Drugs, Including Well-Characterized,
Therapeutic, Biotechnology-derived Products. CDER & CBER, (November 1995).
10. FDA Guidance for Industry: INDs for Phase 2 and Phase 3 Studies. Chemistry, Manufacturing, and Controls Information. CDER, (May 2003).
11. FDA Guidance for Industry: Applications covered by Section 505(b)(2). CDER (October 1999).
12. FDA Guidance for Industry: Coronary Drug-eluting stents- Nonclinical and clinical studies. Center for Devices and Radiological Health (CDRH) and CDER (March
2008).
13. FDA Guidance for Industry: Q8 Pharmaceutical Development. CDER & CBER (May 2006).
14. FDA Guidance for Industry: Fast Track Development Programs- Designation, Development, and Application Review. CDER & CBER (January 2006).
15. Dagher R, Johnson J, Williams G, Keegan P, Pazdur R. Accelerated Approval of Oncology Products: A Decade of Experience. J Natl Cancer Inst. 2004;96(20):1500-
1509.
Stuart Cantor,PhD
Senior ScientistICON DevelopmentSolutions
Dr. Stuart Cantor graduated from the University of
Maryland Pharmacy School and is a Senior Scientist
for ICON. Dr. Cantor currently assists global clients
with their CMC sections of regulatory documents for
solid dosage forms and biologics, and also handles
clinical supply chain management issues. He has 7
pharmaceutical publications online/in-process, and
has published a book chapter on wet granulation.
He interned at Wyeth and Bristol Myers Squibb
(BMS) and studied different granulation processes
and their mechanical properties. His research
covered preformulation, formulation, analytical
method validation, blend segregation, and chemical
imaging. His expertise is in extrusion-
spheronization, wet granulation, and NIR
spectroscopy. Dr. Cantor previously developed the
sugarless fiber chews for diabetics launched by
BMS under the Choice® DM brand.
Dr. Kadriye Çiftci is Senior Director of Drug
Delivery/Formulations at ICON Development
Solutions. She has more than 15 years of
experience in academia and pharmaceutical R&D.
Dr. Ciftci completed her training at the University of
Illinois at Chicago and the University of Michigan
Medical School. She previously worked as a Tenure-
track Assistant Professor at Temple University and a
Research Fellow at the Schering Plough Research
Institute. Her special interests include cancer
research, gene therapy, and the development of
novel drug delivery systems, particularly biotech
products and vaccines.
Kadriye Ciftci,PhD
Senior Director DrugDeliveryICON DevelopmentSolutions
68-73-DDT MAr 2009 -SP-Therapeutic Focus:Layout 1 2/26/09 11:48 AM Page 72