Cardiac tamponade: contrast reflux as an indicator of cardiac
2
CASE REPORT Open Access Cardiac tamponade: contrast reflux as an indicator of cardiac chamber equalization Foeke Jacob Harmen Nauta, Wernard Aat Antoine Borstlap, Michael Stella and Zain Khalpey * Abstract Background: Traumatic hemopericardium remains a rare entity; it does however commonly cause cardiac tamponade which remains a major cause of death in traumatic blunt cardiac injury. Objectives: We present a case of blunt chest trauma complicated by cardiac tamponade causing cardiac chamber equalization revealed by reflux of contrast. Case report: A 29-year-old unidentified male suffered blunt chest trauma in a motor vehicle collision. Computed tomography (CT) demonstrated a periaortic hematoma and hemopericardium. Significant contrast reflux was seen in the inferior vena cava and hepatic veins suggesting a change in cardiac chamber pressures. After intensive treatment including cardiac massage this patient expired of cardiac arrest. Conclusion: Reflux of contrast on CT imaging can be an indicator of traumatic cardiac tamponade. Keywords: Cardiac tamponade, Hemopericardium, Blunt trauma, Contrast reflux, Cardiac hemodynamics Background Traumatic cardiac tamponade remains a deadly, but rare, reason for presentation to the emergency depart- ment [1]. Its main cause in trauma patients is penetrat- ing chest injury (80-90%) and it occurs in only 10% of blunt chest trauma injuries. Thoracic injuries account for approximately 25% of trauma related deaths and are a contributing factor in an additional 25% of deaths in the United States annually [1]. As it is typical for acute trauma, fast and accurate diagnostics are crucial. We present a case of blunt chest trauma including cardiac tamponade revealed by contrast reflux at CT. Case presentation A 29-years-old unidentified male suffered multiple blunt trauma in a severe motor vehicle collision. On suspicion of intracranial injury due to left sided globe rupture, FAST exam was skipped and the patient was rushed to CT. After intravenous administration of contrast, axial CT (Figure 1) demonstrated bilateral pneumothoraces, periaortic hematoma and pulmonary contusion. Coronal view (Figure 2) showed mild right sided deviation of the trachea, pseudoaneurysm of the descending aorta and hemopericardium. Remarkable contrast reflux was seen into the inferior vena cava (IVC) and hepatic veins. This phenomenon was presumably caused by equalization of cardiac chamber pressures typical of tamponade. Even though emergent thoracotomy following blunt trauma carries an overall survival rate of only 1-2% [2], after the loss of vital signs, emergent thoracotomy was per- formed and 2.5 liters of pericardial blood was found ori- ginating from a right atrial tear. This case shows that the use of contrast in CT can reveal changes in cardiac chamber pressures possibly indicating traumatic cardiac tamponade. Discussion Several studies have described the relationship between IVC contrast reflux and several morbidities (pulmonary hypertension, tricuspid regurgitation and right ventricu- lar systolic dysfunction) [3-5]. Dusaj et al. [6] demon- strated the hemodynamic potential of Coronary CT angiography (CTCA). Quantification of IVC and SVC contrast characteristics during CTCA provides a quick, feasible and accurate method of estimating right atrial and ventricular response. Their findings correlated with * Correspondence: [email protected] The University of Arizona Medical Center - University Campus, 1501 North Campbell Avenue Tucson, AZ 85724, USA © 2012 Nauta et al.; licensee BioMed Central Ltd. This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Nauta et al. Journal of Cardiothoracic Surgery 2012, 7:48 http://www.cardiothoracicsurgery.org/content/7/1/48
Transcript of Cardiac tamponade: contrast reflux as an indicator of cardiac

Nauta et al. Journal of Cardiothoracic Surgery 2012, 7:48http://www.cardiothoracicsurgery.org/content/7/1/48
CASE REPORT Open Access
Cardiac tamponade: contrast reflux as anindicator of cardiac chamber equalizationFoeke Jacob Harmen Nauta, Wernard Aat Antoine Borstlap, Michael Stella and Zain Khalpey*
Abstract
Background: Traumatic hemopericardium remains a rare entity; it does however commonly cause cardiactamponade which remains a major cause of death in traumatic blunt cardiac injury.
Objectives: We present a case of blunt chest trauma complicated by cardiac tamponade causing cardiac chamberequalization revealed by reflux of contrast.
Case report: A 29-year-old unidentified male suffered blunt chest trauma in a motor vehicle collision. Computedtomography (CT) demonstrated a periaortic hematoma and hemopericardium. Significant contrast reflux was seenin the inferior vena cava and hepatic veins suggesting a change in cardiac chamber pressures. After intensivetreatment including cardiac massage this patient expired of cardiac arrest.
Conclusion: Reflux of contrast on CT imaging can be an indicator of traumatic cardiac tamponade.
Keywords: Cardiac tamponade, Hemopericardium, Blunt trauma, Contrast reflux, Cardiac hemodynamics
BackgroundTraumatic cardiac tamponade remains a deadly, butrare, reason for presentation to the emergency depart-ment [1]. Its main cause in trauma patients is penetrat-ing chest injury (80-90%) and it occurs in only 10% ofblunt chest trauma injuries. Thoracic injuries accountfor approximately 25% of trauma related deaths and area contributing factor in an additional 25% of deaths inthe United States annually [1]. As it is typical for acutetrauma, fast and accurate diagnostics are crucial. Wepresent a case of blunt chest trauma including cardiactamponade revealed by contrast reflux at CT.
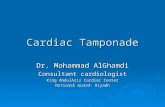
Case presentationA 29-years-old unidentified male suffered multiple blunttrauma in a severe motor vehicle collision. On suspicionof intracranial injury due to left sided globe rupture,FAST exam was skipped and the patient was rushed toCT. After intravenous administration of contrast, axialCT (Figure 1) demonstrated bilateral pneumothoraces,periaortic hematoma and pulmonary contusion. Coronal
* Correspondence: [email protected] University of Arizona Medical Center - University Campus, 1501 NorthCampbell Avenue Tucson, AZ 85724, USA
© 2012 Nauta et al.; licensee BioMed Central LCommons Attribution License (http://creativecreproduction in any medium, provided the or
view (Figure 2) showed mild right sided deviation of thetrachea, pseudoaneurysm of the descending aorta andhemopericardium. Remarkable contrast reflux was seeninto the inferior vena cava (IVC) and hepatic veins. Thisphenomenon was presumably caused by equalization ofcardiac chamber pressures typical of tamponade. Eventhough emergent thoracotomy following blunt traumacarries an overall survival rate of only 1-2% [2], afterthe loss of vital signs, emergent thoracotomy was per-formed and 2.5 liters of pericardial blood was found ori-ginating from a right atrial tear. This case shows thatthe use of contrast in CT can reveal changes in cardiacchamber pressures possibly indicating traumatic cardiactamponade.
DiscussionSeveral studies have described the relationship betweenIVC contrast reflux and several morbidities (pulmonaryhypertension, tricuspid regurgitation and right ventricu-lar systolic dysfunction) [3-5]. Dusaj et al. [6] demon-strated the hemodynamic potential of Coronary CTangiography (CTCA). Quantification of IVC and SVCcontrast characteristics during CTCA provides a quick,feasible and accurate method of estimating right atrialand ventricular response. Their findings correlated with
td. This is an Open Access article distributed under the terms of the Creativeommons.org/licenses/by/2.0), which permits unrestricted use, distribution, andiginal work is properly cited.

Axial contrast CT chest
Figure 1 Axial contrast CT chest showed bilateralpneumothoraces (1), periaortic hematoma (2) and pulmonarycontusion (3).
Nauta et al. Journal of Cardiothoracic Surgery 2012, 7:48 Page 2 of 2http://www.cardiothoracicsurgery.org/content/7/1/48
echocardiographic estimations of right atrial and rightventricular pressures. Similarly, we have found that con-trast reflux in the IVC, SVC and hepatic veins correlateswith acute hemodynamic changes associated with car-diac tamponade.
ConclusionThis case emphasizes the diagnostic potential of contrastenhanced CT of the chest to characterize acute cardio-vascular physiology, particularly in blunt chest trauma.
Coronal contrast CT chest Figure 2 Coronal contrast CT chest showed mild right sideddeviation of the trachea (1), pseudoaneurysm of thedescending aorta (2), hemopericardium (3) and contrast refluxinto the IVC and hepatic veins (4).
ConsentUnfortunately patient deceased and no medical consentwas obtained.
AbbreviationsCT: Computed tomography; FAST: Focused assessment with sonography fortrauma; IVC: Inferior vena cava; CTCA: Coronary CT angiography;SVC: Superior vena cava.
Competing interestThe author(s) declare that they have no competing interest.
AcknowledgementsNone.
Authors’ contributionsFN and WB reviewed the literature, FN wrote the manuscript. ZK, WB and MSedited the text. MS supplied and described the images. All authors read andapproved the final manuscript.
Author’s informationFN and WB are clinical research trainees. ZK is the supervising chief residentcardiac surgery and MS is a radiologist.
Received: 29 December 2011 Accepted: 31 May 2012Published: 31 May 2012
References1. Yamamoto L, Schroeder C, Morley D, Beliveau C: Thoracic trauma: the
deadly dozen. Crit Care Nurs Q 2005, 28(1):22–40.2. Hunt PA, Greaves I, Owens WA: Emergency thoracotomy in thoracic
trauma—a review. Injury 2006, 37(1):11–19.3. Groves AM, Win T, Charman SC, Wisbey C, Pepke-Zaba J, Coulden RA: Semi-
quantitative assessment of tricuspid regurgitation on contrast-enhancedmultidetector CT. Clin Radiol 2004, 59(8):715–719.
4. Yeh BM, Kurzman P, Foster E, Qayyum A, Joe B, Coakley F: Clinicalrelevance of retrograde inferior vena cava or hepatic vein opacificationduring contrast-enhanced CT. AJR Am J Roentgenol 2004,183(5):1227–1232.
5. Collins MA, Pidgeon JW, Fitzgerald R: Computed tomographymanifestations of tricuspid regurgitation. Br J Radiol 1995,68(814):1058–1060.
6. Dusaj RS, Michelis KC, Terek M, Sanai R, Mittal R, Lewis JF, Zeman RK, ChoiBG: Estimation of right atrial and ventricular hemodynamics by CTcoronary angiography. J Cardiovasc Comput Tomogr 2011, 5(1):44–49.
doi:10.1186/1749-8090-7-48Cite this article as: Nauta et al.: Cardiac tamponade: contrast reflux asan indicator of cardiac chamber equalization. Journal of CardiothoracicSurgery 2012 7:48.
Submit your next manuscript to BioMed Centraland take full advantage of:
• Convenient online submission
• Thorough peer review
• No space constraints or color figure charges
• Immediate publication on acceptance
• Inclusion in PubMed, CAS, Scopus and Google Scholar
• Research which is freely available for redistribution
Submit your manuscript at www.biomedcentral.com/submit








![Pericardiocentesis in cardiac tamponade: A case for “Less ... Journal … · cardiac tamponade may cause myocardial stunning leading to heart failure. It has been suggested [4]](https://static.fdocuments.in/doc/165x107/5ed0ca956d761e663b7d23c5/pericardiocentesis-in-cardiac-tamponade-a-case-for-aoeless-journal-cardiac.jpg)