
cardiac strategy 2010 - 2015 - Atrial Fibrillation Association (AFA)
158
Cardiac and Stroke Networks in Lancashire & Cumbria CARDIAC STRATEGY 2010 - 2015
Transcript of cardiac strategy 2010 - 2015 - Atrial Fibrillation Association (AFA)
Cardiac and Stroke Networks in Lancashire & Cumbria
CARDIAC STRATEGY 2010 - 2015
CONTENTS
Introduction 2 Epidemiology and Prevention of Cardio Vascular Diseases in Lancashire and Cumbria
4
Cardiac Imaging Diagnostics 20 Cardiac Arrhythmias and Devices 33 Revascularisation and Cardiac Surgery 46 Cardiac Rehabilitation 77 Heart Failure 85 Adult Congenital Heart Disease 98 Appendices 102 References 146
1

Cardiac and Stroke Networks in Lancashire & Cumbria
INTRODUCTION
The North West Specialised Commissioning Team and local Commissioners tasked the Cardiac and Stroke Networks in Lancashire and Cumbria (CSNLC) with the production of a five year Strategy for Cardiac services based on • Demographic need • Achieving national best practice standards and targets • Closing identified gaps in service • The development of cost effective, equitable, accessible high quality services The Cardiac Strategy is intended to support Network Primary Care Trust (PCT) organisations in developing world class commissioning1 of services that optimise health gains and reductions inequality for their local populations. It sets out the recommended key developments required over the next five years to ensure the commissioning of cardiac services that meet the health needs of the local population, which are delivered in the most personalised, practical and effective way possible, as envisaged by Lord Darzi in High Care Quality for All2. The strategy includes a summary of the North West Adult Congenital Heart Disease Strategic Plan but does not include Children’s Cardiac Services. The sections identify existing national commissioning drivers, evidence based medicine and relevant quality standards to inform commissioners in their decision making. Gap analysis, savings, and cost implications of the strategic recommendations have been included wherever possible. In the changing economic NHS climate it is recognised that it is unlikely the strategy can be implemented in totality within the next 5 years. It has been written therefore as a framework to allow commissioning decisions to be made around locally identified outcome focused strategic priorities. Recommendations in the strategy have been based on sound evidence, current needs assessment and future trends over the next five years. Involvement and Consultation CSNLC have used the following mechanisms to ensure stakeholder involvement throughout the development of the Strategy: • Cardiac Network Board • PCT Commissioners/ CVD Leads Group • Operational Steering Group • Cardiac Clinical Advisory Group • Healthcare Professionals Groups • Development of priority focused Task Advisory Groups (TAG) • Development of priority focused patient consultation groups • North West Ambulance Service Lead • North West Specialised Commissioning Lead
1 2
Stakeholders were asked to identify areas for inclusion in the Strategy. The following priorities were identified: 1. Prevention and Detection 2. Imaging and Diagnostics 3. Arrhythmias and Devices 4. Revascularisation & Surgery 5. Cardiac Rehabilitation 6. Heart Failure and End of Life Care 7. Adult Congenital Heart Disease Specific priority focused Task Advisory Groups (TAG) were established. Membership of the TAGs varied depending upon the priority but included clinical representation from each Acute Trust, PCT CVD Commissioning Leads and primary care representation. The first clinical priority identified for development was Revascularisation and the first TAG to assess Percutaneous Coronary Intervention (PCI) service provision was established in July 2008. This section of the strategy then expanded to incorporate Primary PCI and surgery and links to work undertaken by SG2 and Capgemini Consulting. Acknowledgements The production of this Strategy would not have been possible without the assistance and advice of a significant number of people both nationally and within Cumbria and Lancashire. Thanks are due therefore to all members of Task Advisory Groups, the Cardiac Clinical Advisory Group, PCT CVD Commissioning Leads, the Operational Steering Group and patients who have advised and contributed. Roger Boyle, David Hackett and Stephen Green are also thanked for their support and contribution.
2 3
EPIDEMIOLOGY AND PREVENTION OF CARDIO VASCULAR DISEASES IN LANCASHIRE AND CUMBRIA
Introduction This section aims to set out the demographic profile of Cumbria and Lancashire, describes the burden of coronary heart disease (CHD)i and its risk factors, and the opportunities for the prevention and early detection of CHD. Demography The current registered population of Lancashire and Cumbria is 1.987 million. The following table provides a population breakdown by Primary Care Trust.3
Primary Care Trust
Population
Blackburn with Darwen 165,000 Blackpool 150,000 Central Lancashire 460,000 Cumbria 500,000 East Lancashire 386,000 North Lancashire 324,300 Total 1,985,300
The average age of the general population across the Network area is above the national average with only Blackburn with Darwen and Preston reporting an average age below 39.5 years. The percentage of the population aged of 70 years is higher than the national average in Blackpool, Cumbria and North Lancashire. This should be considered as particularly significant as the cardiovascular risk increases with age, particularly over the age of 55, which also increases demand for cardiac services.4
Demographic changes are predicted within the two counties, particularly Cumbria which is projected to have a greater number of older people than the national average, which in itself predicts an aging population. Analysis shows that the older population will increase in number and in terms of the proportion of the total population they make up over the next 20 years. There will be fewer young people and people of working age. The population will also become increasingly diverse in terms of ethnicity.5
There is a gap in life expectancy of more than 14 years between the most affluent and the poorest neighbourhoods in Lancashire & Cumbria. i Please note that the term ‘coronary heart disease’ is used interchangeably with ischaemic heart disease that falls under the wider umbrella of diseases of the circulatory system (I00 – I99) in the International Classification of Diseases (ICD – 10).
1 4
Geography Cumbria and Lancashire is a diverse geographical area with an extremely varied mix of rural and urban communities all of which to a lesser or greater degree have some health issues which need to be tackled.
Lancashire & Cumbria
Greater Manchester
Cheshire &
Merse yside
Cumbria is England's second largest county and has the third highest levels of population sparsity. However, Cumbria is a county of contrasts. The popular national, and sometimes regional, perception of Cumbria as synonymous with the Lake District and idyllic rurality belies a much more complex mix of settlements, lifestyles and policy priorities, often masking significant levels of inequality. Parts of West Cumbria and Barrow, for instance, show a poorer than average performance across a range of health indices. Life expectancy is lower than the national average in all districts except South Lakeland and Eden. Barrow is the only district with life expectancy significantly lower than the national average and that of the north west. Lancashire County Council is the fourth largest local authority in England and Wales with a population of around 1.3 million people. There are significant variations in health and wellbeing across the whole county with some parts experiencing great deprivation in areas such East Lancashire (Burnley, Blackburn and surrounding small towns), parts of Preston and Blackpool.5
The counties of Cumbria and Lancashire have six and twelve district councils respectively. Six Primary Care Trusts (PCT) cover the two counties that contain four spearhead Local Authorities; one large PCT across Cumbria, three working within Lancashire and the two Unitary Authorities of Blackpool and Blackburn with Darwen. Acute cardiac services, cardiac diagnostics and outpatient services are provided locally across the network by five acute hospital trusts: Blackpool, Fylde & Wyre Hospitals NHS Trust; East Lancashire Hospitals NHS Trust, Lancashire Teaching Hospitals NHS Foundation Trust; University Hospitals of Morecambe Bay NHS Trust and North Cumbria University
Tertiary cardiac care for Lancashire and South Cumbria is provided by the Lancashire Cardiac Centre in Blackpool which is accessible via the M6 which is the main motorway network that runs through Lancashire and Cumbria. Tertiary cardiac care for the hospitals in Carlisle and Whitehaven is provided by The Freeman Hospital (Newcastle upon Tyne Hospitals NHS Foundation Trust) and James Cook University Hospital (South Tees Hospitals NHS Foundation Trust) respectively.
2 5

Although most of Lancashire benefits from easy access to the motorway network, travel across large rural areas of Lancashire and Cumbria can cause difficulties in relation to equitable access to services. Deprivation The following map shows the Index of Multiple Deprivation (IMD) by postcode sector for this Network. A plethora of evidence suggests that people living in deprived circumstances have poorer health than the rest of the population. This is strongly reflected in vascular diseases (coronary heart disease, stroke, kidney disease and diabetes) where people in lower socio-economic groups tend to suffer earlier and more severe disease.4,6,7,8 Therefore services need to focus on the significant pockets of deprivation to reduce health inequalities across this Network. Cardiac and Stroke Networks in Cumbria and Lancashire The index was calculated from the 2001 Census and is a continuous variable that takes into account factors such as age, health and employment. The value of IMD was split nationally into eight bands containing an equal number of postcodes. Band 1, mapped in blue, represents the most affluent areas, and Band 8, mapped in yellow, the most deprived areas. Some postcode sectors could not be allocated a value of IMD and they are shown in grey.
3 6

The following table demonstrates that Blackburn with Darwen and Blackpool PCTs are the most deprived areas covered by the Network.
Primary Care Trust *IMD IMD Rank
IMD Summary
Health Index
Health Rank
Health Summary
35.81 34 Moderately Deprived 1.10 19 Very
unhealthy 5CC Blackburn with Darwen
38.61 18 Very Deprived 1.23 6 Very
unhealthy 5HP Blackpool
5NE Cumbria 21.04 84 Average 0.22 77 Average
19.28 103 Slightly Affluent 0.32 67 Average 5NF North Lancashire
22.78 85 Average 0.59 53 Slightly unhealthy 5NG Central Lancashire
27.42 72 Average 0.70 42 Moderately unhealthy 5NH East Lancs
* The Index of Multiple Deprivation (IMD) is on an exponential scale (to accentuate small differences at the Deprived end of the spectrum), so it is appropriate to take the logarithm of the IMD score before calculating its average. This method has been used for the first time in the 2007 report.
Ethnicity
The burden of cardiovascular disease falls disproportionately on people living in deprived circumstances and also particular ethnic groups, such as South Asians. Across the whole of Lancashire there is a slightly higher percentage of people from a white ethnic background (91.9%) than is the average for England (88.7%) and the great bulk of these are "White British". Aside from these, the most significant ethnic group is "Asian or Asian British" who comprise 6% of the resident population, a proportion marginally above the national average. All other broad ethnic groups have a lesser representation in Lancashire that nationally. This is particularly marked in the case of "Black or Black British" who comprise just 0.5% of the population of Lancashire compared with 2.8% in England.9
Historically, there has been significant migration into East Lancashire (a few hundred per year) of dependants and spouses from India or Pakistan, moving to the UK. Since 2005/06 this has been overshadowed by a comparable, if not slightly larger, influx of working age adults and families from Eastern Europe, predominantly Poland and the implications of the health needs of this group should not be ignored when planning services.10
The population of Cumbria is predominately “White British”, with an overall proportion of 96% in 2007. This is much higher than the proportions for England and the North West. The BME population of Cumbria in 2007 was 4% which is significantly less than the North West average of 8%. Significantly the BME group had doubled since 2001 when the BME group only accounted for 2% of the population.11
Burden of Cardio Vascular Diseases National picture CVD is one of the leading contributors to the global disease burden. The single most common cardiovascular disease is ischaemic heart disease (IHD, also called coronary heart disease (CHD) or coronary artery disease (CAD)). IHD includes myocardial infarction (MI, heart attacks) and angina (chest pain on exertion due to inadequate blood flow to the heart muscle). The vast majority of CVD in England is caused by atherosclerosis (‘furring’ of the arteries). This is not only the case for IHD and for stroke, the two main diseases, but also for aortic aneurysm and peripheral vascular disease, with impaired blood flow to the limbs, as well as for diseases affecting the heart valves (which can also be congenital or caused by rheumatic fever) and abnormal heart rhythms.12
4 7
Although CVD death rates in England have been falling yet they remain a major cause of death, causing 184,000 deaths (up to 88,000 IHD and up to 50,000 stroke deaths) in England and Wales in 2005. CVD also caused 28% of premature deaths (deaths in people under 75) in 2005.13 The current government target is to reduce the CVD death rate from in people under 75 by at least 40% from the 1995-97 baseline to 2010 (to 83.8 deaths per 100,000 population).14 By 2003-05, it had fallen by 35.9%. Progress has also been made on reducing inequalities in mortality over that period, with a 26.4% absolute reduction in the difference between the higher mortality in spearhead PCTs and the average for England.15 The Coronary Heart Disease National Service Framework: Building for the Future - Progress Report for 200716 stated that the target to reduce mortality had been met five years earlier than anticipated, resulting in 22,000 fewer premature deaths from cardiovascular disease. This has in part been attributed to decreased waiting times for heart surgery, increased prescriptions for cholesterol-reducing statins, and the reduction in adult smoking prevalence. The percentage of heart attacks treated with thrombolysis within 60 minutes of a call for help has nearly trebled (from 24% in 2001 to 68% in 2007). In addition, the absolute gap between the England average and the fifth worst deprived areas has decreased by 32% (1995-97 baseline to 2007).16
However, in recent years, CHD death rates have been falling more slowly in younger age groups and fastest in those aged 55 and over. For example, between 1997 and 2006 there was a 46% fall in the CHD death rate for men aged 55 to 64 in the UK, compared to a 22% fall in men aged 35 to 44 years. In women there was a 53% fall in those aged 55 to 64 years and a 20% fall in those aged 35 to 44 years. There is some evidence that these rates are beginning to plateau in younger age groups.17
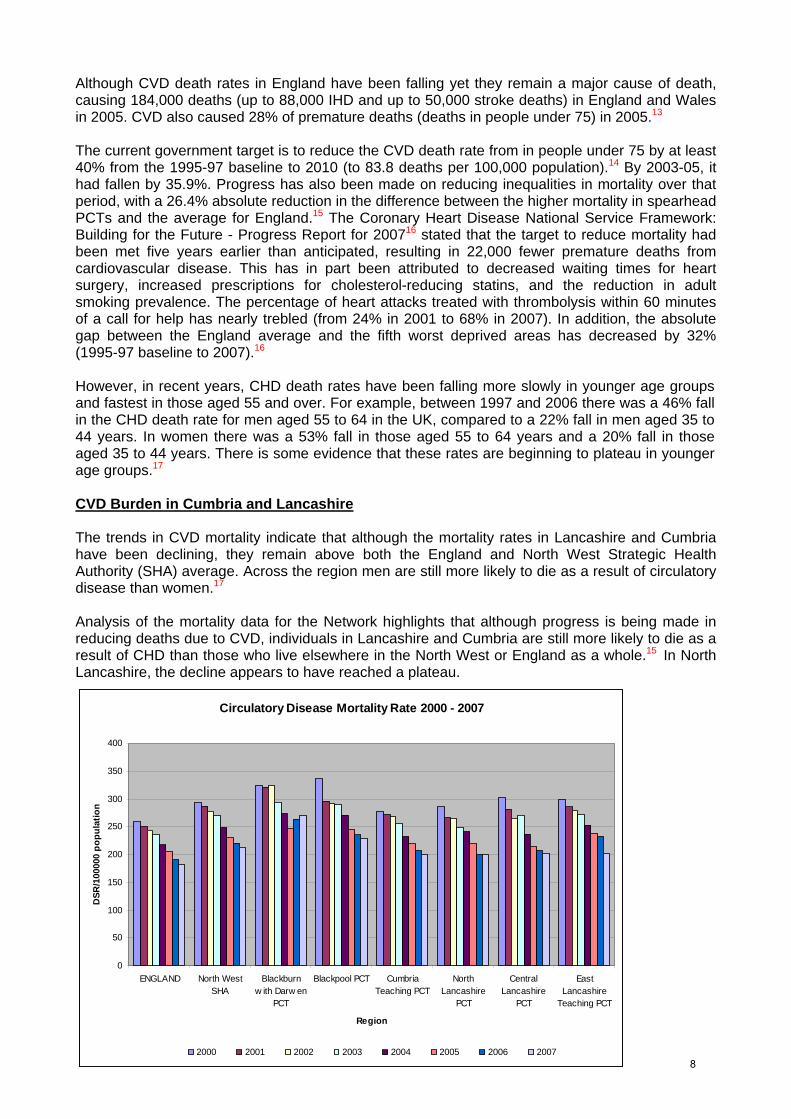
CVD Burden in Cumbria and Lancashire The trends in CVD mortality indicate that although the mortality rates in Lancashire and Cumbria have been declining, they remain above both the England and North West Strategic Health Authority (SHA) average. Across the region men are still more likely to die as a result of circulatory disease than women.17 Analysis of the mortality data for the Network highlights that although progress is being made in reducing deaths due to CVD, individuals in Lancashire and Cumbria are still more likely to die as a result of CHD than those who live elsewhere in the North West or England as a whole.15 In North Lancashire, the decline appears to have reached a plateau.
Circulatory Disease Mortality Rate 2000 - 2007
0
50
100
150
200
250
300
350
400
ENGLAND North WestSHA
Blackburnw ith Darw en
PCT
Blackpool PCT CumbriaTeaching PCT
NorthLancashire
PCT
CentralLancashire
PCT
EastLancashire
Teaching PCT
Region
DSR
/100
000
popu
latio
n
5 2000 2001 2002 2003 2004 2005 2006 2007
8
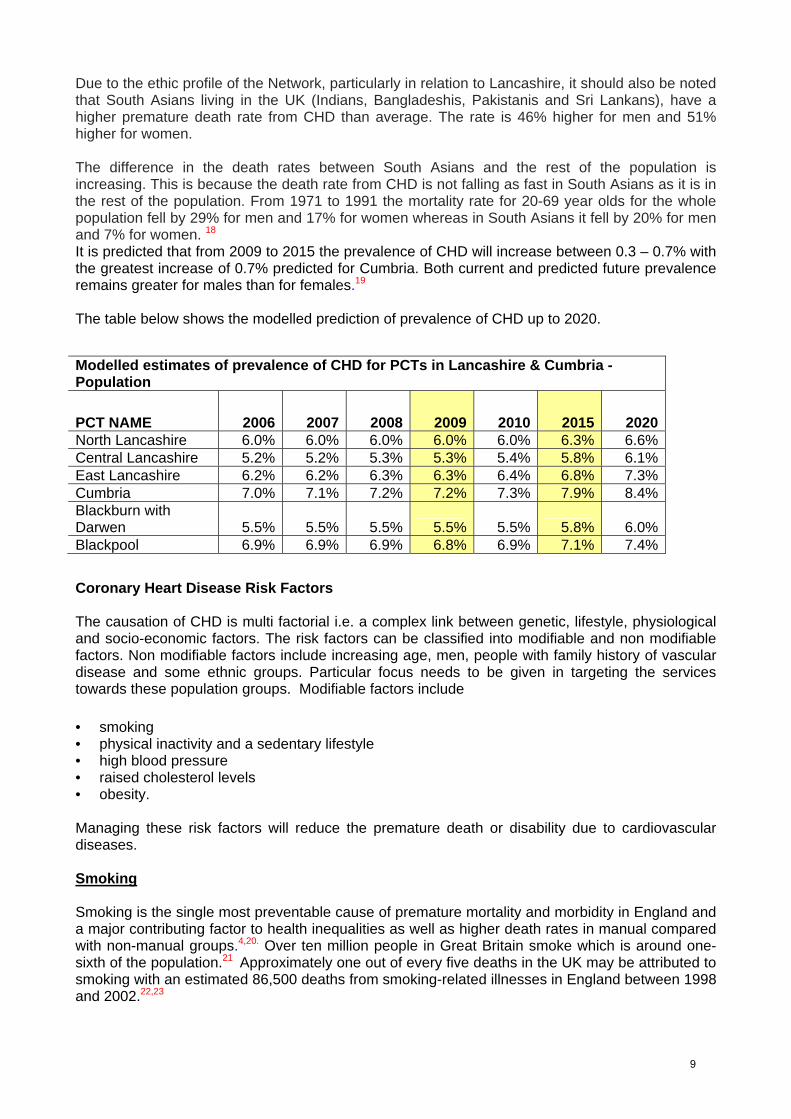
Due to the ethic profile of the Network, particularly in relation to Lancashire, it should also be noted that South Asians living in the UK (Indians, Bangladeshis, Pakistanis and Sri Lankans), have a higher premature death rate from CHD than average. The rate is 46% higher for men and 51% higher for women. The difference in the death rates between South Asians and the rest of the population is increasing. This is because the death rate from CHD is not falling as fast in South Asians as it is in the rest of the population. From 1971 to 1991 the mortality rate for 20-69 year olds for the whole population fell by 29% for men and 17% for women whereas in South Asians it fell by 20% for men and 7% for women. 18 It is predicted that from 2009 to 2015 the prevalence of CHD will increase between 0.3 – 0.7% with the greatest increase of 0.7% predicted for Cumbria. Both current and predicted future prevalence remains greater for males than for females.19 The table below shows the modelled prediction of prevalence of CHD up to 2020.
Modelled estimates of prevalence of CHD for PCTs in Lancashire & Cumbria - Population
2006 2007 2008 2009 2010 2015 2020 PCT NAME North Lancashire 6.0% 6.0% 6.0% 6.0% 6.0% 6.3% 6.6% Central Lancashire 5.2% 5.2% 5.3% 5.3% 5.4% 5.8% 6.1% East Lancashire 6.2% 6.2% 6.3% 6.3% 6.4% 6.8% 7.3% Cumbria 7.0% 7.1% 7.2% 7.2% 7.3% 7.9% 8.4% Blackburn with
Darwen 5.5% 5.5% 5.5% 5.5% 5.5% 5.8% 6.0% Blackpool 6.9% 6.9% 6.9% 6.8% 6.9% 7.1% 7.4%
Coronary Heart Disease Risk Factors The causation of CHD is multi factorial i.e. a complex link between genetic, lifestyle, physiological and socio-economic factors. The risk factors can be classified into modifiable and non modifiable factors. Non modifiable factors include increasing age, men, people with family history of vascular disease and some ethnic groups. Particular focus needs to be given in targeting the services towards these population groups. Modifiable factors include • smoking • physical inactivity and a sedentary lifestyle • high blood pressure • raised cholesterol levels • obesity. Managing these risk factors will reduce the premature death or disability due to cardiovascular diseases. Smoking Smoking is the single most preventable cause of premature mortality and morbidity in England and a major contributing factor to health inequalities as well as higher death rates in manual compared with non-manual groups.4,20. Over ten million people in Great Britain smoke which is around one-sixth of the population.21 Approximately one out of every five deaths in the UK may be attributed to smoking with an estimated 86,500 deaths from smoking-related illnesses in England between 1998 and 2002.22,23
6 9

Smoking is also related to a number of long-term conditions including respiratory disease (bronchitis, emphysema, asthma), hypertension, heart and circulatory disease, cancer of the bladder, throat and mouth24 with a cost to the NHS of approximately £1.5 billion per year. It is estimated that 34 million days are lost in England and Wales through sickness absence resulting from smoking-related illnesses.25 There are also longstanding issues surrounding second hand smoke, which has been found to exacerbate asthma and increase the risk of lung cancer, heart disease and stroke.25
The General Household Survey 2007 showed the prevalence of smoking in England to be 21%, a fall of one percentage point in a year. The North West region, along with the West Midlands, had the highest prevalence in England in 2007 (both 23%).4
The NWPHO report “Where Wealth Means Health”26 looked at the geographical variation in smoking prevalence based on synthetic estimates by quintile bands in the North West region. Higher smoking levels were found in East Lancashire as well as in diverse localities including Blackpool, Lancaster and Preston. These areas of Lancashire and Cumbria are also where significant pockets of deprivation are present. The findings from the Health Survey for England 200612 showed individuals in the lowest income quintile had the highest prevalence of smoking (36% of men and 30% of women). This is shown in the chart below. Percentage of adults who currently smoke, by Index of Multiple Deprivation 2007 quintile. There is a large body of evidence from prospective cohort studies regarding the beneficial effect of smoking cessation on coronary heart disease mortality.27 Government targets aim to reduce not only overall prevalence of smoking but also the proportions of people smoking who are in households that are headed by someone in manual employment.28 There is evidence of progress towards this target: in 2005 in England, 29% of people in manual occupations were smokers, compared with 33% in 1998.4
If national smoking cessation targets were achieved, it is estimated that there would be a cost benefit/saving of £524 million due to the reduction in the number of heart attacks and strokes.29
7 10

Physical Inactivity and Sedentary Lifestyle In developed countries a lack of physical activity is estimated to contribute to 22-33% of coronary heart disease, 15% of diabetes, 12-13% of stroke, 16-17% of colon cancer and 11% of breast cancer. Regular physical activity can help relieve stress and mild forms of depression and has a major impact on the prevalence of obesity.4
In the North West over one third of adults typically have a low level of physical activity. The percentage of adults that partake in a high level of physical activity decreases with increasing age, while low activity increases with age. Overall, men are 1.4 times more likely to partake in a high level of physical activity (46.1%) than women (32.4%).4
Significantly more men (14.5%) than women (8.9%) were sedentary for more than eight hours a day as well as for more than four but less than eight hours. Significantly more 25-64 year olds (25-34 years: 15.0%; 35-44 years: 14.0%; 45-54 years: 13.0%; 55-64 years: 10.7%) were sedentary for over eight hours a day compared with 16-24 year olds (7.7%), possibly reflecting higher levels of employment in these age groups, particularly in sedentary jobs.4 There was little variation in sedentary hours by deprivation score. The majority of adults living in both the most deprived (34.6%) and most affluent (33.0%) areas have between two and four sedentary hours in a typical day. Around 1.2 times more people in the most deprived areas (13.6%) had eight or more sedentary hours a day than those in the most affluent areas (11.2%) but this difference was not significant.4
In Lancashire and Cumbria, levels of physical activity in adults in Blackburn with Darwen PCT and Blackpool PCT are significantly worse than the England average.30
Hypertension
Hypertension, or high blood pressure, affects over 16 million people in the UK 4,31 and is a major cause of stroke, CHD and other illnesses including kidney disease, aortic aneurysm and heart failure.4,32. There are a number of lifestyle factors that can help to reduce high blood pressure: increasing intake of fresh fruit and vegetables; drinking alcohol in moderation; stopping smoking; increasing levels of activity; weight loss if overweight; and reducing salt intake, as this is a major contributor to high blood pressure.4
Hypertension is included in one of the key targets within the NHS National Standards, Local Action: Health and Social Care Standards and Planning Framework4,32 and The National Institute for Health and Clinical Excellence (NICE) has published the guidelines Hypertension: Management of hypertension in primary care.33 Effective management of hypertension may contribute towards the target to reduce the number of deaths from heart disease and stroke by 2010 as detailed in the National Service Framework for Coronary Heart Disease.16
The Health Survey for England (HSE) 200612 defined hypertension as “at least 140mmHg systolic and/or at least 90mmHg diastolic blood pressure or anyone receiving treatment for hypertension”. It also found the prevalence for hypertension was higher in men than women (31% and 28% respectively). North West figures were similar: 31% for men and 27% for women.34
The national QOF data for hypertension showed the unadjusted prevalence to be 12.5% in England and slightly higher in the North West at 12.8%. In Lancashire and Cumbria, NHS Cumbria had the highest unadjusted prevalence for hypertension (14.2%) and NHS Blackburn with Darwen had the lowest (11.7%).29 The unadjusted prevalence rates show these registers as a percentage of the total practice list size (all ages) and therefore only reflect those individuals already known to the GP. It does not reflect the true prevalence of hypertension in the overall population.
8 11

A crude epidemiologic hypertension model based on age and sex-specific prevalence was first developed in the UK by the Faculty of Public Health.36 Subsequently, English PCTs were required to set targets for hypertension case-finding in their 2007-8 Local Delivery Plans negotiated with strategic health authorities. To assist them a simple PCT-based prevalence model was developed rapidly by the Association of Public Health Observatories (APHO).37
Using this tool the comparisons of the expected hypertension prevalence for Lancashire & Cumbria are shown in the graph below. Prevalence of Hypertension Prevalence (persons 16+)
0.0%
5.0%
10.0%
15.0%
20.0%
25.0%
30.0%
35.0%
40.0%
Blackburn withDarwen
Blackpool North Lancashire Central Lancashire East Lancashire Cumbria ENGLAND
5CC 5HP 5NF 5NG 5NH 5NE
PCT
Perc
enta
ge
20092015
When comparing the modelled prevalence with the national QOF data it is clear that a substantial difference between the expected prevalence in the population and those known, and recorded, to have hypertension on GP registers. This highlights the need to develop robust systems to identify all individuals with hypertension across Lancashire and Cumbria. NICE 2006 Guidelines for Hypertension33 management recommend that drug treatment should be considered for individuals with blood pressures of 140/90mmHg or over, and that optimal blood pressure treatment targets are a systolic blood pressure of less than 140mmHg and a diastolic blood pressure of less than 85mmHg (and lower still, at 130/85mmHg, in people with diabetes). People with high normal blood pressures 130-139/85-89mmHg should be assessed yearly. The optimal blood pressure level is now classified as <120/<80mmHg. Both drug treatment and lifestyle changes - particularly weight loss, an increase in physical activity, and a reduction in salt and alcohol intake - can effectively lower blood pressure. Raised Cholesterol and Statins A raised level of blood cholesterol is a key modifiable risk factor for CHD. It is estimated that in high-income countries blood cholesterol levels in excess of 3.8 mmol/litre are responsible for more than 50% of CVD events.38,39.
HSE 200612 results for prevalence of total cholesterol of 4mmol/l or above by disease category show that the lowest prevalence occurred among those reporting existing CVD conditions.
9 12
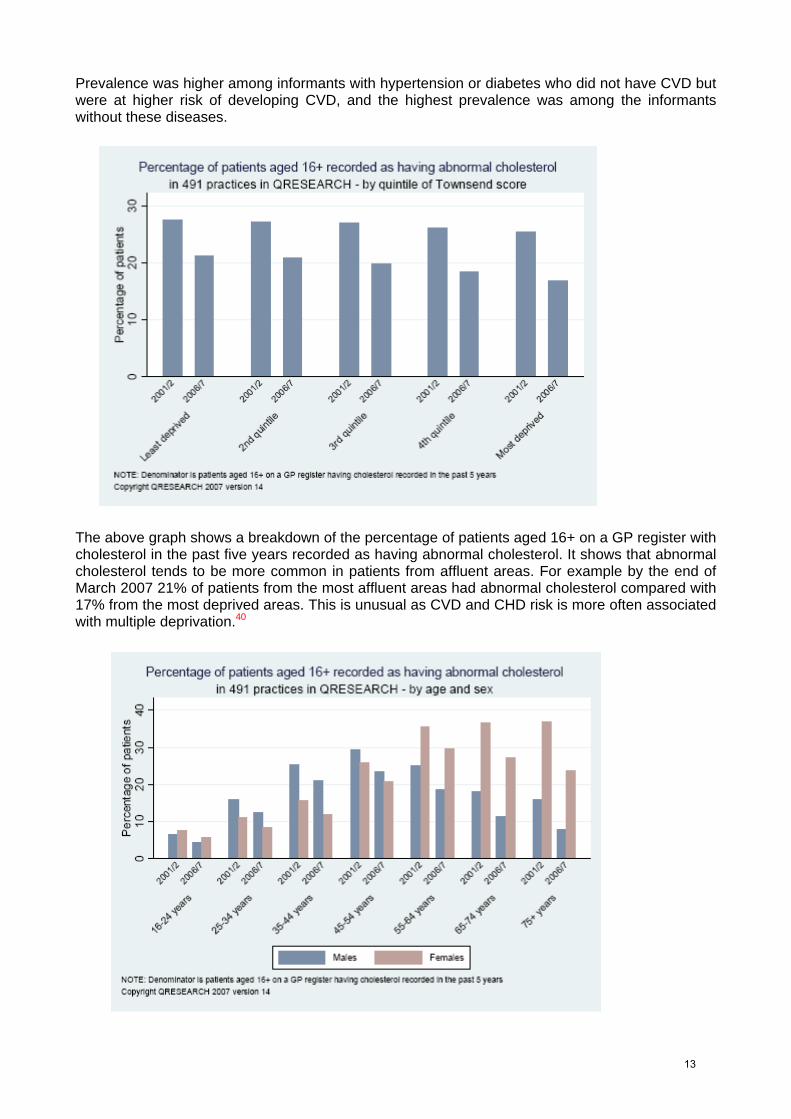
Prevalence was higher among informants with hypertension or diabetes who did not have CVD but were at higher risk of developing CVD, and the highest prevalence was among the informants without these diseases.
The above graph shows a breakdown of the percentage of patients aged 16+ on a GP register with cholesterol in the past five years recorded as having abnormal cholesterol. It shows that abnormal cholesterol tends to be more common in patients from affluent areas. For example by the end of March 2007 21% of patients from the most affluent areas had abnormal cholesterol compared with 17% from the most deprived areas. This is unusual as CVD and CHD risk is more often associated with multiple deprivation.40
10 13
The breakdown of the percentage of patients aged 16+ on a GP register with total cholesterol recorded in the past five years recorded as having abnormal cholesterol detailed in the above graph highlights that the percentage of patients with abnormal cholesterol increases with age. Abnormal cholesterol is more common in males than females between 25 and 54 years, and more common in females than males from age 55.40
Although the prevalence of raised cholesterol levels is falling, cholesterol levels remain higher than recommended among many with CVD, or those at a high risk. It should also be noted that the HSE findings show that since 2003, mean CRP levels have remained constant in men and women. The lack of change in this inflammatory marker during this timeframe may reflect the fact that overall risk is determined by a combination of factors, including smoking or obesity, as well as having hypertension or diabetes.12
Changes in diet and physical activity are central to cholesterol lowering strategies for the prevention of first and recurrent cardiovascular events. However those at highest risk, may in addition require medication with statins.41 The HSE12 indicates that there is already some targeting of those at risk of CVD with statins, as differences in the prevalence of raised levels and in mean values of cholesterol disappear when those taking lipid-lowering drugs are excluded. The use of statin therapy also appears to be effective in lowering cholesterol levels. High levels of cholesterol and specifically the low-density lipoproteins (LDL) in the blood are known to increase the risk of heart disease and stroke. Statins help to lower the harmful LDL cholesterol levels by slowing down the production of cholesterol in the liver and increasing the liver’s ability to remove the LDL cholesterol already in the blood. Consumption of plant sterols and stanols has been shown to lower cholesterol levels by 10-30%. These fats, which are found in fortified products such as margarines and yogurts substantially lower LDL cholesterol, and raise HDL cholesterol thereby significantly reducing the risk of CHD.39,42,43
Treatment with statins reduces the risk of recurrence and death in individuals with existing disease and in those with no apparent disease and SIGN97 guidance43 make clear that statin therapy is both effective and cost effective as secondary prevention in individuals with established disease, and as primary prevention. However, poor adherence may reduce cost effectiveness – some studies suggest that approximately half of all patients discontinue statins within two years.39
NICE has published comprehensive evidence-based guidance for use of lipid modifying drugs in a range of clinical situations.39 There are five statins currently approved for use within the UK for the treatment of high cholesterol: atorvastatin, fluvastatin, pravastatin, rosuvastatin and simvastatin. However these drugs vary markedly in price. There are non-proprietary versions of simvastatin and pravastatin, so by prescribing these two drugs generically clinicians can help keep prescribing costs down. Ezetimibe inhibits the intestinal absorption of cholesterol and is licensed as an add-on to statin and/or dietary therapy in hypercholesterolaemia. It is not licensed for primary or secondary prevention of cardiovascular disease.44
The number of prescriptions for statins is continuing to increase although there has been a significant change in the product mix of statins used over recent months. Current expenditure on statins is around £500 million a year. A 28-day course of a branded statin is on average about 6 times more costly than an appropriate generic statin. If PCTs with below 78% use of lower cost statins (achieved by the top quartile of trusts) increased this to 78%, over £19 m would be saved in a year (based on quarter 1, 2008/09).44
In April – March 2009, North West SHA spent £110.1m on lipid-regulating drugs (the highest section-level cost). This represents a 3.5% decrease in expenditure, in comparison to the 3.3% decrease in expenditure for the North of England, although the number of prescription items grew by 9.0%, compared with the same period in 2007/08.45
11 14

Prescribing levels of low cost statins for Blackburn with Darwen PCT indicate performance within the top 25% of PCTs in England. Both East Lancashire PCT and North Lancashire PCT are maintaining prescribing performance in line with the national average however, all other Lancashire and Cumbria PCTs are prescribing below the national average.40
The table below details current low cost statin prescribing trends detailing the national position of local PCTs.44
NOTE: if the Network Lipid Modification Guidelines are introduced to manage patients in the most
effective manner across Lancashire and Cumbria, there is an opportunity to save in the region of £3.8 million per annum.
12 15
Obesity Obesity is a growing health problem in both developed and developing countries.38 Prospective epidemiological studies have shown a relationship between overweight or obesity and cardiovascular morbidity, CVD mortality and total mortality. Obesity is strongly related to major cardiovascular risk factors, such as raised blood pressure, glucose intolerance, type 2 diabetes, and dyslipidaemia. 46-50
Obesity increases the risk of coronary heart disease by 2–3 times and, although BMI may not be a strong independent risk factor, other measures of obesity, such as waist:hip ratio, certainly are.51
Health Survey for England (HSE)12 data highlighted that over the period from 1993 to 2006, the prevalence of obesity in England rose from 13.2% to 24.9% in males, and from 16.4% to 25.2% in females2.The prevalence of morbid obesity rose seven fold in males from 0.2% to 1.4% and nearly doubled in females, from 1.4% to 2.7%.52
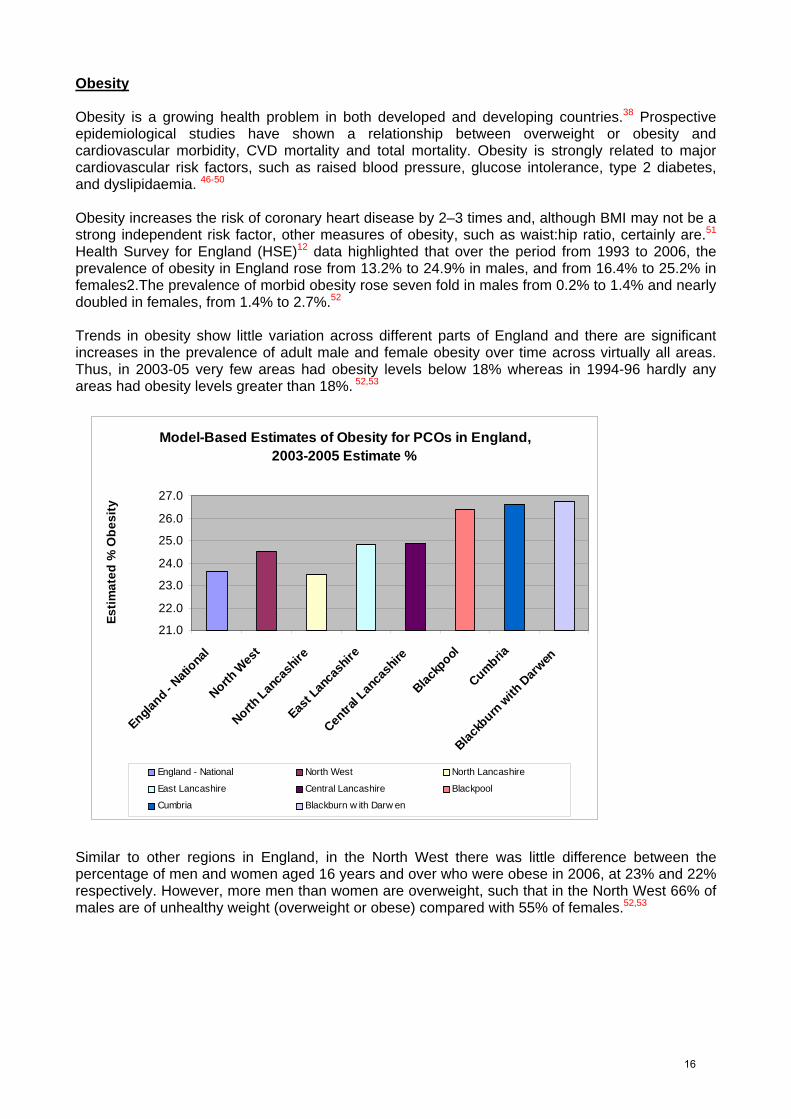
Trends in obesity show little variation across different parts of England and there are significant increases in the prevalence of adult male and female obesity over time across virtually all areas. Thus, in 2003-05 very few areas had obesity levels below 18% whereas in 1994-96 hardly any areas had obesity levels greater than 18%. 52,53
Model-Based Estimates of Obesity for PCOs in England, 2003-2005 Estimate %
21.0
22.0
23.0
24.0
25.0
26.0
27.0
England -
Nati
onal
North W
est
North Lan
cash
ire
East L
anca
shire
Centra
l Lan
cash
ire
Blackp
ool
Cumbria
Blackb
urn w
ith D
arwen
Estim
ated
% O
besi
ty
England - National North West North Lancashire
East Lancashire Central Lancashire Blackpool
Cumbria Blackburn w ith Darw en
Similar to other regions in England, in the North West there was little difference between the percentage of men and women aged 16 years and over who were obese in 2006, at 23% and 22% respectively. However, more men than women are overweight, such that in the North West 66% of males are of unhealthy weight (overweight or obese) compared with 55% of females.52,53
13 16

Modelled estimates of obesity prevalence in adults (aged 16+ years) for 2003-2005 in the North West region by local authority. 12,52
Estimates have been calculated to predict local patterns of adult obesity (at Middle Super Output Area), which enables organisations to target relevant local populations.12,52 See above. Information taken from the North West health profile highlighted six areas in Lancashire and Cumbria, Allerdale CD, Blackburn with Darwen UA, Blackpool UA, Carlisle CD, Fylde CD and Hyndburn, where obesity in the population is significantly worse than the England average.30
14 17

Significantly modelled estimates of adult obesity (2003-05) revealed that two of these local authorities, Allerdale and Eden in Cumbria, have the highest estimated prevalence in the North West where the prevalence of obesity in both areas is estimated at 28.3% of the population compared to a national measure of 23.6% 30,12,52 National Quality and Outcomes Framework (QOF) data which shows the unadjusted prevalencei of obesity in England and the North West,ii as 7.4% and 7.8% respectively, also indicates an area of concern for the Network with Blackpool PCT reporting the highest unadjusted prevalence of obesity (9.9%) in the North West. 54
With pockets of deprivation highlighted across Lancashire and Cumbria (see Epidemiology section) it is important to highlight that once again there is also a relationship between deprivation and obesity as seen in the table below. In the North West adults in the most deprived areas are 1.7 times more likely to be obese than adults in the least deprived areas. Even adults from the middle areas of deprivation are significantly more likely to be obese than adults from the least and second least deprived areas.16
Percentage of adults who are obese, by Index of Multiple Deprivation 2007 quintile.
I. Unadjusted prevalence rates show these registers as a percentage of the total practice list size (all ages).
II. Particular care may be taken when looking at the QOF obesity data. This indicator is based
upon BMI measurement, yet many people registered with a GP may not have had their BMI measured within the last 15 months. Therefore it may not provide an accurate picture of their actual obesity status, possibly underestimating the prevalence of obesity.
15 18
Recommendations 1. PCTs should implement the NHS Health Checks programme and develop local plans in line
with national guidance to ensure that CVD prevention and detection is ongoing (embedded in practice) across Lancashire and Cumbria. It will be useful to learn lessons from the experience of NHS Blackburn with Darwen as they were a test bed for NHS Health Checks and have got an established model to implement the programme.
2. PCTs should collaborate to develop and share effective strategies to capture those individuals
at greatest risk of CVD due to their socio economic status. CSNLC could be utilised to facilitate this.
3. PCTs should develop the wider use of social marketing approaches which target those groups
at highest risk of cardiovascular disease. 4. PCTs will continue to monitor CVD prevalence at practice level to ensure that GP Practices
patients at risk of CVD continue to be identified, managed and reviewed in line with best practice guidelines.
5. PCTs will collaborate in the development and implementation of an ongoing cardiovascular risk
educational/training programme 6. CSNLC should facilitate the collaborative commissioning of Lancashire and Cumbria wide CVD
prevention and detection services 7. All key stakeholders should collaborate to develop and share Network wide guidelines to
support optimal patient care based on gold standard, evidence based, cost effective prescribing practices, e.g. Network Lipid Modification Guidelines
8. PCTs should collaborate to develop and implement Network wide evaluation to measure the
effectiveness of CVD prevention and detection practices and inform future financial forecasting/planning.
16 19
CARDIAC IMAGING DIAGNOSTICS
Introduction This chapter of the Strategy outlines the developments and commissioning agreements for cardiac imaging diagnostic services within Lancashire and Cumbria. In order to diagnose and select patients for therapeutic interventions, clinicians rely on accurate diagnostic tools, particularly in the field of imaging. Two new imaging techniques have emerged in the last two decades: Cardiac Computed Tomography (CT) and Cardiac Magnetic Resonance Imaging (CMR), however all imaging diagnostics below will be addressed. Their use, requirements for the different modalities and the clinical benefits available, their appropriateness for disease and patient condition will be considered. Facility capability and capacity and workforce implications will also be considered as part of this Strategy. Standards for operational service developments and workforce requirements will be established and these will underpin service developments supported by the diagnostic pathways developed, aligned to the Map of Medicine. The following imaging diagnostics will be discussed. Echocardiography (Echo) Cardiac Angiography Cardiac Computed Tomography (CT) Cardiac Magnetic Resonance Imaging (CMR) Myocardial Perfusion Imaging (MPI)
Echocardiography Transthoracic Echocardiography is the backbone of cardiac imaging and is a non-invasive diagnostic used to assess myocardial structure and function, cardiac valvular function and cardiac structural abnormalities. There is an ever increasing demand on Echo services with increasing requests from both primary and secondary care, an increasing cohort of patients with heart failure, Atrial Fibrillation, implementation of Aortic Abdominal Aneurysm (AAA) screening and vascular checks and improvements in Adults with Congenital Heart Disease service provision will further increase demand for Echo in the future. Transoesophageal Echocardiography (TOE) is a semi-invasive technique used for the detailed assessment of patients where transthoracic images are inadequate, particularly with prosthetic valves, suspected endocarditis, and dissection and in ventilated patients including during cardiac surgery. It is also useful for assessment of detailed valvular function, pre-operative valvular assessment and TOE guided cardioversion. Stress Echocardiography is a specialised technique used to assess the myocardial response to pharmacological stress and is superior to exercise treadmill testing for the assessment of myocardial ischaemia, particularly in specific groups such as women, diabetics and hypertensive patients. It is also used to assess and identify viable myocardium that may guide treatment and interventions received. Cardiac Angiography Cardiac Angiography has been used to diagnose stenotic Coronary Artery Disease and allows assessment of the extent, severity and location of atherotic sclerosis. It has guided and informed the treatment of Percutaneous Coronary Intervention (PCI) for many years and is also utilised to assist in pacemaker and device implantation, electrophysiology and cardioversion procedures as well as assessing myocardial function structure and cardiac anatomy. Undertaken in conjunction with physiological measurements, e.g. Blood gas analysis, can assist in the diagnosis and treatment outcomes in those with ACHD, cardiac surgical procedures and cardiac transplantation.
20
It is currently the only method of coronary artery stenotic assessment and for this reason is explained within this section; however projection of future capacity and expected use is inextricably linked to and outlined within the revascularisation section.
Computed Tomography (CT) Cardiac Computed Tomography technology has rapidly advanced over the last few years with the development of ‘Multislice’ scanners with very high spatial and temporal resolution. It is useful for the non-invasive identification of coronary by-pass grafts, cardiac and thoracic structure abnormalities and has now increasingly been used in the investigation of coronary artery disease with clearer identification of the coronary tree. As Computed Tomography scanning is increasing in its sophistication, early work suggests that this imaging modality may replace a significant number of invasive cardiac angiographic studies. It could have a role also in the triage of patients with acute chest pain – particularly those with low to intermediate or intermediate probability of cardiac disease.
Cardiac Magnetic Resonance Imaging (CMR) Cardiac Magnetic Resonance Imaging provides high quality images of anatomy, function and viability of the myocardium. It also provides excellent information of cardiac haemodynamics in valvular diseases as well as in the presence of abnormal flow patterns and in shunt detection. The technique is capable of providing detailed information on complex congenital heart diseases, and in those with complex thoracic aortic disease. There is increased interest in the use of CMR in the detection of ischaemia and in the detection of myocardial scarring and myocardial viability. Access to CMR for the appropriate imaging of patients with Adult Congenital Heart Disease (ACHD), cardiomyopathies (including ischaemic), aortic diseases and valvular heart diseases would enhance the diagnostic ability in terms of quality, accuracy and quantity; thus allowing best therapeutic choices to be made including invasive and non-invasive interventions. In the management of patients with myocardial ischaemia it is important to have accurate and reliable evidence of clinically significant viable myocardium prior to embarking on high-risk revascularisation strategy. To attain that, advanced imaging techniques such as cardiac magnetic resonance imaging are valuable. The value of CMR has been recognised by specialist bodies such as the British Cardiovascular Society (BCVS) who advocate that there should be at least one full time expert in CMR in each tertiary centre.
Myocardial Perfusion Imaging (MPI) Myocardial Perfusion Imaging (MPI) is a well-established, non-invasive imaging technique. MPI is effective in the diagnosis and management of ischaemic heart disease and heart failure and has been shown reliably to be a more sensitive and specific measure of ischaemia than exercise tolerance ECG testing. MPI allows reliable risk stratification and guides the selection of patients for further interventions. This allows more appropriate utilisation of resources and greater cost-effectiveness. MPI is particularly important in investigating certain subgroups, including women, the elderly and those with diabetes.
21
However current provision locally, when compared to other parts of the country, is patchy. It is a requirement of NICE to increase the current rate of 1200 MPI per million population (pmp)/year to 4000 MPI pmp/year.55 In the short term, there are limitations with radioisotope supply and lack of available gamma camera capacity. For the test to have impact on the management of patients and to achieve the 18 week wait target, waiting times need to be less than six weeks. Multidisciplinary Team (MDT) Meetings All imaging modalities require specialist training and, following initial interpretation and reporting, these investigations should be correlated with the patients’ history symptoms and clinical signs, ideally in a multidisciplinary team environment. The value and benefits of MDT meetings has already been seen for surgical patients and it is recommended MDT environments be established considering the following: • Teleconferencing facilities, with viewing access to angiograms, cardiac CT, CMR and
Echocardiography at all sites • The assessment of existing and new consultant cardiologists’ and radiologists’ job plans need
to ensure MDT forms a part of weekly workload, embedding MDT into practice • Ensure attendance by multidisciplinary healthcare professionals is essential. National Drivers Significant advances have been made in access to diagnostics. The number of patients waiting for planned care diagnostics of all types has fallen from 127,000 in December 2006 to under 58,000 in February 2008.56 With the introduction and implementation of Referral to Treatment Targets (RRT) of 18 weeks, the demand on accessible and timely diagnostic services will increase. Advances in technology and the drive to support technology innovation and improvement2 impacts highly on the imaging diagnostics discussed both for technology advancement for equipment and facility capability but also where diagnostics are performed and the requirement to provide community based services. Finally NICE Guidance will be used to support and influence the development of this Strategy. These will be considered and include: • NICE Technology Appraisal Guidance 73 - Myocardial perfusion scintigraphy for the diagnosis
and management of angina and myocardial infarction which assesses the requirement for MPI in this patient group. Issue date: November 200355
• NICE Clinical Guideline 36 – Atrial Fibrillation: The Management of Atrial Fibrillation (AF) which outlines those patients with AF whom require Echocardiography. Issue date June 2006.57
Currently under consultation is the NICE guidance for the management of ACS patients, which should be considered once published as this may impact on the referral pathways that are developed. • Nice Guideline (Draft for Consultation) – Acute coronary syndromes: the management of
unstable angina and non-ST-segment-elevation myocardial infarction: Draft, July 200958
22
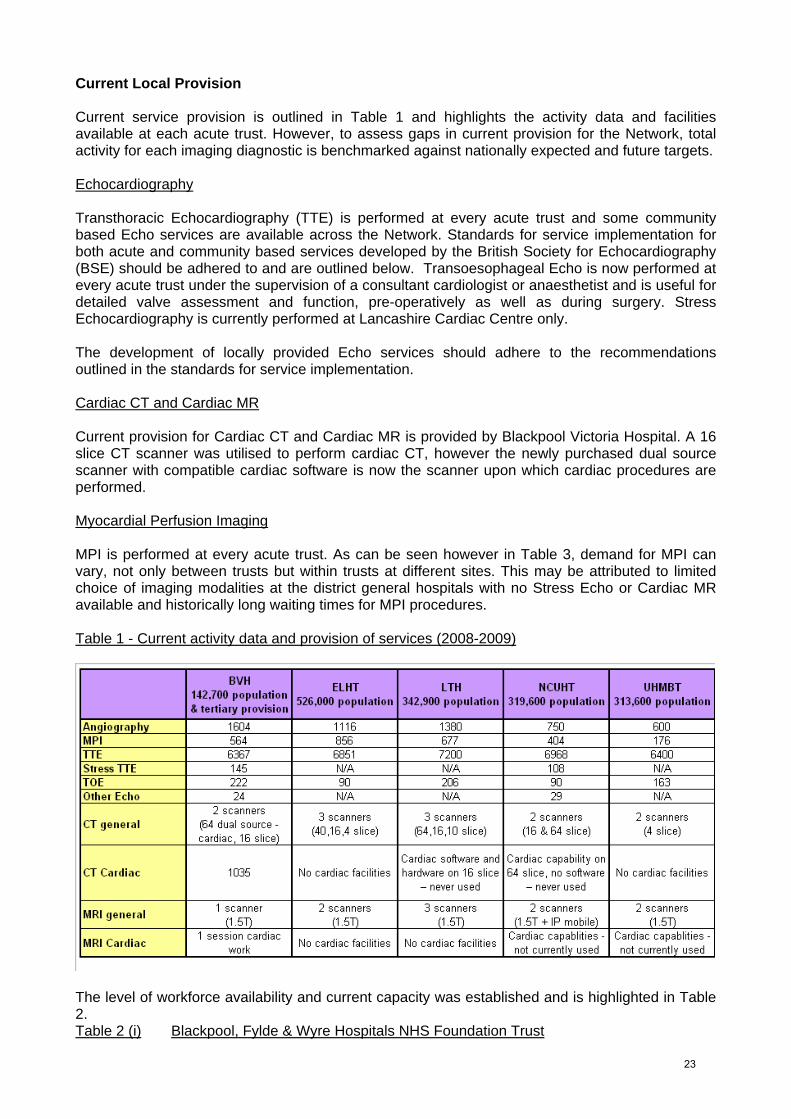
Current Local Provision Current service provision is outlined in Table 1 and highlights the activity data and facilities available at each acute trust. However, to assess gaps in current provision for the Network, total activity for each imaging diagnostic is benchmarked against nationally expected and future targets. Echocardiography Transthoracic Echocardiography (TTE) is performed at every acute trust and some community based Echo services are available across the Network. Standards for service implementation for both acute and community based services developed by the British Society for Echocardiography (BSE) should be adhered to and are outlined below. Transoesophageal Echo is now performed at every acute trust under the supervision of a consultant cardiologist or anaesthetist and is useful for detailed valve assessment and function, pre-operatively as well as during surgery. Stress Echocardiography is currently performed at Lancashire Cardiac Centre only. The development of locally provided Echo services should adhere to the recommendations outlined in the standards for service implementation. Cardiac CT and Cardiac MR Current provision for Cardiac CT and Cardiac MR is provided by Blackpool Victoria Hospital. A 16 slice CT scanner was utilised to perform cardiac CT, however the newly purchased dual source scanner with compatible cardiac software is now the scanner upon which cardiac procedures are performed. Myocardial Perfusion Imaging MPI is performed at every acute trust. As can be seen however in Table 3, demand for MPI can vary, not only between trusts but within trusts at different sites. This may be attributed to limited choice of imaging modalities at the district general hospitals with no Stress Echo or Cardiac MR available and historically long waiting times for MPI procedures. Table 1 - Current activity data and provision of services (2008-2009)
The level of workforce availability and current capacity was established and is highlighted in Table 2. Table 2 (i) Blackpool, Fylde & Wyre Hospitals NHS Foundation Trust
23
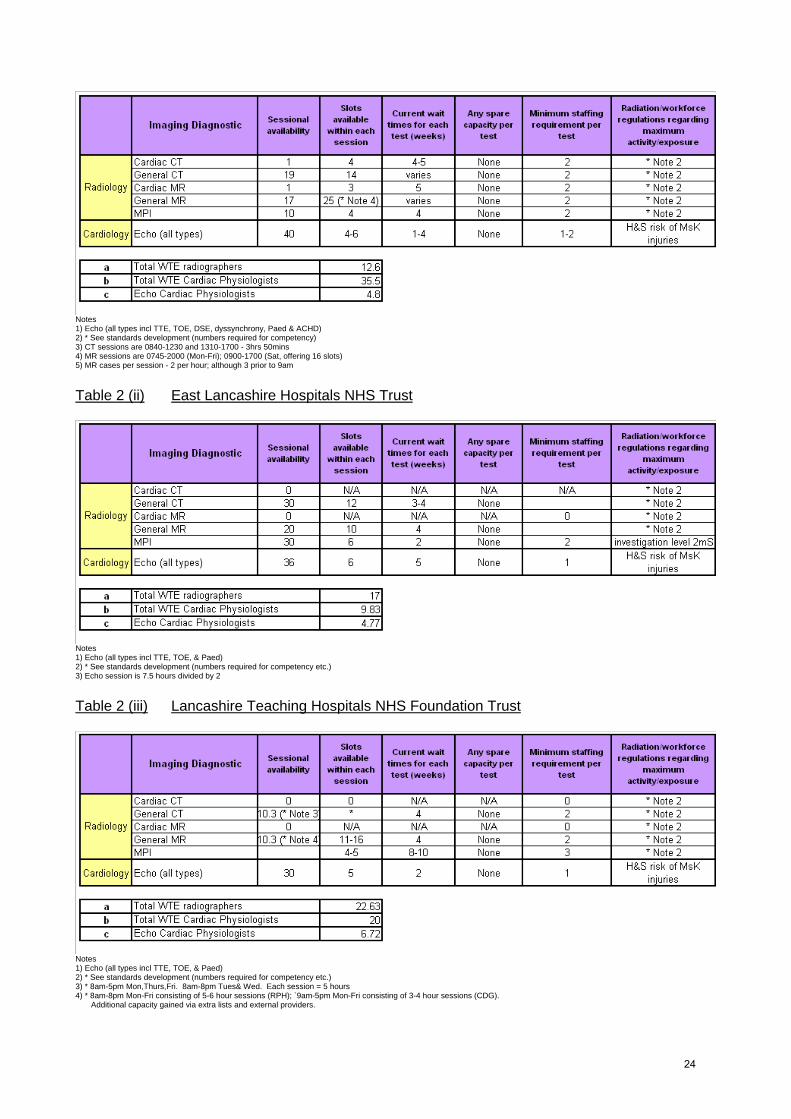
Notes 1) Echo (all types incl TTE, TOE, DSE, dyssynchrony, Paed & ACHD) 2) * See standards development (numbers required for competency) 3) CT sessions are 0840-1230 and 1310-1700 - 3hrs 50mins 4) MR sessions are 0745-2000 (Mon-Fri); 0900-1700 (Sat, offering 16 slots) 5) MR cases per session - 2 per hour; although 3 prior to 9am
Table 2 (ii) East Lancashire Hospitals NHS Trust
Notes 1) Echo (all types incl TTE, TOE, & Paed) 2) * See standards development (numbers required for competency etc.) 3) Echo session is 7.5 hours divided by 2
Table 2 (iii) Lancashire Teaching Hospitals NHS Foundation Trust
Notes 1) Echo (all types incl TTE, TOE, & Paed) 2) * See standards development (numbers required for competency etc.) 3) * 8am-5pm Mon,Thurs,Fri. 8am-8pm Tues& Wed. Each session = 5 hours 4) * 8am-8pm Mon-Fri consisting of 5-6 hour sessions (RPH); `9am-5pm Mon-Fri consisting of 3-4 hour sessions (CDG). Additional capacity gained via extra lists and external providers.
24
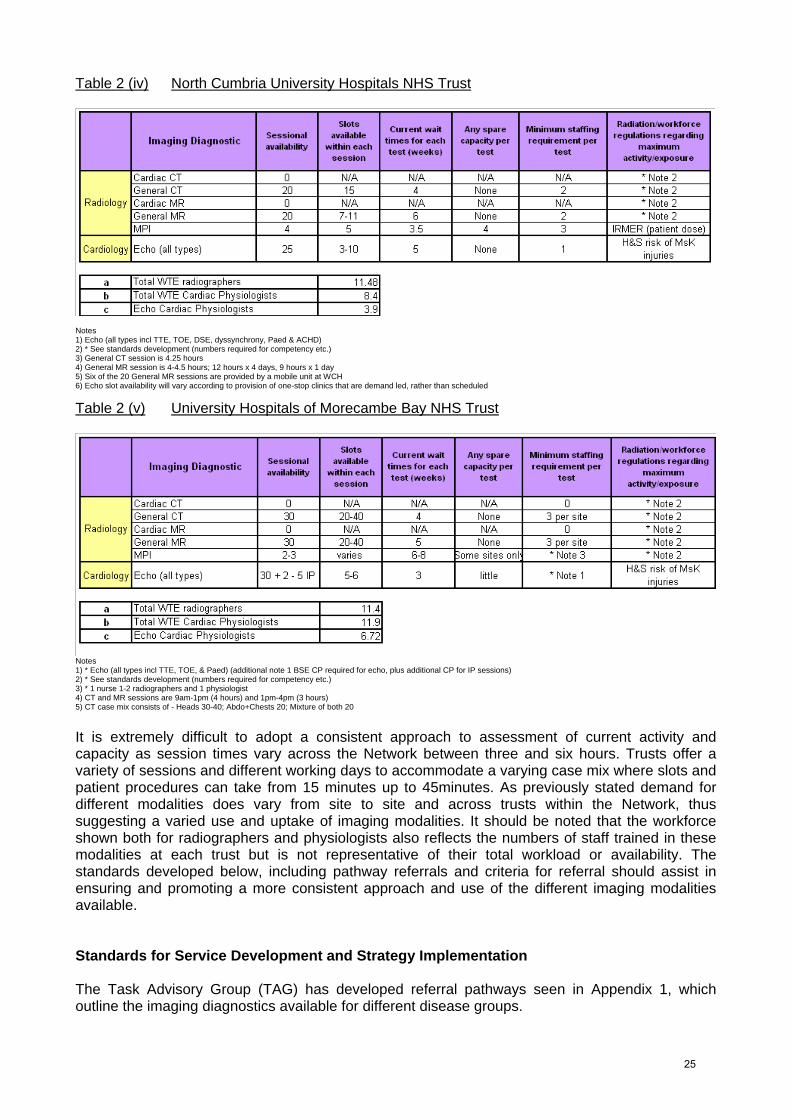
Table 2 (iv) North Cumbria University Hospitals NHS Trust
Notes 1) Echo (all types incl TTE, TOE, DSE, dyssynchrony, Paed & ACHD) 2) * See standards development (numbers required for competency etc.) 3) General CT session is 4.25 hours 4) General MR session is 4-4.5 hours; 12 hours x 4 days, 9 hours x 1 day 5) Six of the 20 General MR sessions are provided by a mobile unit at WCH 6) Echo slot availability will vary according to provision of one-stop clinics that are demand led, rather than scheduled
Table 2 (v) University Hospitals of Morecambe Bay NHS Trust
Notes 1) * Echo (all types incl TTE, TOE, & Paed) (additional note 1 BSE CP required for echo, plus additional CP for IP sessions) 2) * See standards development (numbers required for competency etc.) 3) * 1 nurse 1-2 radiographers and 1 physiologist 4) CT and MR sessions are 9am-1pm (4 hours) and 1pm-4pm (3 hours) 5) CT case mix consists of - Heads 30-40; Abdo+Chests 20; Mixture of both 20
It is extremely difficult to adopt a consistent approach to assessment of current activity and capacity as session times vary across the Network between three and six hours. Trusts offer a variety of sessions and different working days to accommodate a varying case mix where slots and patient procedures can take from 15 minutes up to 45minutes. As previously stated demand for different modalities does vary from site to site and across trusts within the Network, thus suggesting a varied use and uptake of imaging modalities. It should be noted that the workforce shown both for radiographers and physiologists also reflects the numbers of staff trained in these modalities at each trust but is not representative of their total workload or availability. The standards developed below, including pathway referrals and criteria for referral should assist in ensuring and promoting a more consistent approach and use of the different imaging modalities available. Standards for Service Development and Strategy Implementation The Task Advisory Group (TAG) has developed referral pathways seen in Appendix 1, which outline the imaging diagnostics available for different disease groups.
25
Where possible, these have been aligned to the Map of Medicine pathways to ensure a consistent approach to pathway development. These pathways are to be implemented along with the referral criteria for each imaging modality and act as a standard for implementation which should be adopted and attached to the Map of Medicine pathways where possible by each PCT locally. The referral criteria for each imaging modality are seen in Appendix 2. Echocardiography The British Society of Echocardiography (BSE) is the Society, affiliated to the British Cardiovascular Society, which regulates and sets the clinical and professional standards for individuals and departments to perform Echocardiography procedures. The full standards are outlined in Appendix 3, however BSE state that accreditation of individual echocardiographers alone cannot guarantee a high quality department and that it is also necessary to have adequate machines, management and organisation. Therefore the standards set by the Task Advisory Group promote and support the application for departmental BSE accreditation status by all Echocardiography departments. It is recommended that all newly commissioned services achieve departmental accreditation status and that any community based services achieve the standards outlined in the community echocardiography for heart failure consensus statement. Cardiac Computed Tomography and CMR Currently the British Institute of Radiology are working jointly with the British Cardiovascular Society (BCVS) and British Cardiovascular Intervention Society (BCIS) to develop standards associated with service development, accreditation and training for Cardiac CT and CMR. It is recommended that these standards once ratified should be adopted by all services providing Cardiac CT and CMR. Myocardial Perfusion Imaging The Royal College of Radiology (RCR) and the Royal College of Physicians (RCP) develop and support the joint curriculum for nuclear medicine radiology as a sub-speciality for radiologist training. Additionally, an Administration of Radioactive Substances Advisory Committee (ARSAC) licence is required to provide clinical governance for the administration of radioactive products within a trust providing an MPI service. This is generally given to a radiologist with sub-speciality training and as a requirement is given to a minimum of one radiologist within each trust. The following standards are recommended for implementation for MPI services: o Imaging should be carried out in a department staffed by specialist radiographers with
appropriate medical support o Imaging should be overseen by medically qualified personnel with appropriate ARSAC
certification o Stress examinations should be performed by medical, physiology, radiography or nursing staff
who have completed appropriate specialist training o Reporting should be carried out by medical staff (usually radiologists/nuclear medicine
physicians or cardiologists) who have completed subspecialist training, at least one of whom should have ARSAC certification.
Workforce, Education and Training There is currently no specific assessment of future workforce required for the individual diagnostic imaging modalities established nationally.
26

Dr David Hackett and the BCS working group on cardiology workforce requirements however carried out a workforce assessment of cardiologists needed to deliver services.59 It was estimated at 35 cardiologists required per million population, however this relates to all cardiology specialities, not imaging alone and does not include or assess the radiologist workforce. This report suggests a minimum of 3.1 WTE consultants providing diagnostic angiography services pmp, 12.6 WTE consultants providing basic Echo services pmp and tertiary/specialist imaging service provision requiring a further 8.3 WTE pmp (for specialist Echo, nuclear, CMR and CT). Non consultant cardiology workforce, including GPs with a Special Interest (GPwSI), cardiac nurses, cardiac physiologists and cardiac radiographers) was also assessed and suggests a minimum of 8.4 WTE pmp for diagnostic angiography and 34 WTE pmp for delivery of Echo services. Assessment of staff required for other imaging modalities was not included. For the purpose of this Strategy development, and to undertake a workforce gap analysis, minimum staff required to undertake all imaging modalities was assessed by each trust and this data is provided in Table 2. Diagnostic angiography requirements were based on four non-consultant staff of nurses, physiologists and radiographers. It is important to acknowledge that, whilst adhering to the standards outlined above, all service developments will develop an adequate workforce, supported by adequate robust education and training provision. In particular, the cardiac physiology workforce is still in short supply nationally and it is also difficult to recruit radiographers to cardiac catheter laboratories. Forward planning to ensure adequate availability of the healthcare professional workforce to support future expansion is essential. Assessment of workforce requirements to support the current and future workload for imaging diagnostics is calculated in the workforce gap analysis seen in Table 4. As specialist imaging modalities are becoming more widespread and technology advancement allows a greater depth of imaging, providing additional clinical information, a specialist workforce is required to support this. Many trusts employ cardiology and radiology consultants with cardiac imaging as a speciality and it is recommended that new and existing consultant job plans are assessed to allow and provide support for this growing speciality. This will also support and lead the development of MDT meetings that are required to underpin current and future services, education and training as well as provide clinical leadership and governance for all cardiac imaging modalities. It is a recommendation that each trust should appoint at least one cardiologist with a special interest in imaging either from the existing cardiologist workforce or as additional staffing and also that each trust identify or appoint a radiologist with a special interest in cardiovascular imaging in particular, Cardiac CT and Cardiac CT angiography. This would underpin the development of and provide continuing clinical support for stress echocardiography services and allow jointly developed cardiology and radiology CT Angiography services. Gap Analysis Current provision and gap analysis There is currently under provision in Stress Echocardiography, Cardiac CT and Cardiac MR. However, the clinical requirement for MPI can also be achieved utilising the imaging modalities CMR and Stress Echocardiography (SE) and until further national targets are established for each imaging modality separately, the assessment of provision of services for MPI will be merged with those for CMR and SE both for current and future projections and mapped against the targets set in NICE Technology Appraisal Guidance 73. 60
27

Table 3 – Current and Future Gap Analysis Based on Lancashire and Cumbria (population 1.96million)
(1) Angiography targets are based on NSF revascularisation activity targets of 1500 pmp61 currently, 1,900
pmp revascularisations by 2011 and 2,250 revascularisations by 2015. This is based on a 50% conversion rate from angiography to revascularisation. A further 15% reduction in this target has been attributed to cardiac CT as a percentage of patients that would be suitable for this procedure instead of diagnostic angiography.
(2) MPI, CMR and SE targets are based on a current target of 1,200 MPI procedures pmp and future targets of 4,000 MPI pmp which has been divided between all three modalities due to the interchangeable nature of these imaging diagnostics. As it can be seen, current targets for MPI activity are being achieved; however this target was set in 2003, was meant to be reviewed in 2006, and has not yet been done. It is expected that MPI activity will not continue to increase as SE and CMR modalities become more widely available, however the NICE clinical guidance currently under consultation: Assessment and investigation of recent onset chest pain or discomfort of suspected cardiac origin, may suggest Exercise Tolerance Testing is no longer the primary diagnostic chosen for myocardial ischaemia in people without known coronary artery disease (CAD). Other imaging modalities may well become the first choice for this patient group. At this time therefore, the targets for CMR, MPI and SE are interchangeable and future assessment should be undertaken as a joint target until further national targets are set for each modality.
(3) There is currently no national target set for Cardiac CT and future projections can only be assessed by benchmarking against other established services. Some assessment of the percentage of coronary angiography that may be replaced by cardiac CT was made by the Task Advisory Group. This was agreed at 15% and the gap analysis undertaken in Table 3 shows a reduction of 15% from the diagnostic angiography target as a rudimentary baseline target for cardiac CT. It is important to note that this would only represent a small proportion of the CT case mix and workload.
Table 4 – Workforce Gap Analysis Based on Lancashire and Cumbria (population 1.96million)
Notes: 1) The level of 80% workforce capacity was derived from deducting full Annual Leave and Bank Holiday quotas (33 + 8 days), 5 days allocated for study leave and 5 days for sickness and absence from the workforce availability. 2) Calculation based on 41.6 weeks per year
28

Projection of future activity Future activity for coronary angiography, MPI, CMR and Stress Echo can be assessed against future targets set out in Table 3. Clearly expansion and development of angiography in relation to future requirements for Percutaneous Coronary Intervention (PCI) and Primary PCI (PPCI), CMR and SE is required. Cardiac CT Assessment of the percentage of coronary angiography that may be replaced by cardiac CT was made by the Task Advisory Group. This was agreed at 15% and the gap analysis undertaken in Tables 3 and 4 shows a reduction of 15% from the diagnostic angiography target as a rudimentary baseline target for cardiac CT. It is important to note that this would only represent a small proportion of the CT case mix and work load and currently Cardiac CT and Cardiac MR are mostly undertaken for cardiac structural assessment not the diagnosis of coronary artery stenosis. The assessment of graft patency post surgery is performed occasionally but referral for this procedure is under-utilised. Therefore any projections for future activity should encompass the potential for future expansion of procedures performed as routine. Cost Analysis/Benefit Table 5 outlines the cost incurred for PCTs achieving targets established using HRG4 Tariffs. Assessment of cost for current activity gap and future activity gap is calculated. The lack of availability of Stress Echo and Cardiac MRI has historically driven clinical choice towards MPI and this may not be able to continue if radioisotope shortages persist. Clinical choice is currently restricted and availability of a wider range of diagnostic modalities across the Network should be available. The cost analysis has therefore followed the gap analysis undertaken and has calculated the cost of MPI, CMR and SE provision as an equal split (as in Table 3). However this is rudimentary and may not reflect future activity depending on which services are developed locally. Table 5 – Cost Analysis
Notes 1) Angiography - OPCS K633 - Angiocardiography of left side of heart NEC; HRG4 EA36Z - Catheter 19 years and over - Planned same day tariff £1342 2) Cardiac CT - HRG4 RA10Z - Computerised Tomography Scan, one area, pre and post contrast - Non-mandatory tariff £147 3) MPI - OPCS U106 - Myocardial perfusion scan; HRG4 RA39Z - Nuclear Medicine - category 5 - Planned same day tariff £712 4) Cardiac MR - HRG4 RA07Z - Magnetic Resonance Imaging Scan, requiring extensive patient repositioning and/or more than one contrast agent - Non-mandatory tariff £353 5) SE - OPCS U205 - Stress echocardiography; HRG4 EA45Z - Complex Echocardiogram (include Congenital, Transoesophageal and Fetal Echocardiography) - Planned same day tariff £413
(1) Both CMR and MPI are procedures taking on average 40 minutes scan time. Gamma cameras
operationally may cost less to operate than MRI scanners and cost effectiveness of scanner utilisation should be considered.
29
(2) Access to non-invasive imaging modalities, in particular Cardiac CT, will reduce the need for current and future invasive diagnostic angiography by an estimated 15%.
(3) Local unbundled tariffs as a recommendation to commissioners may support locally required service developments.
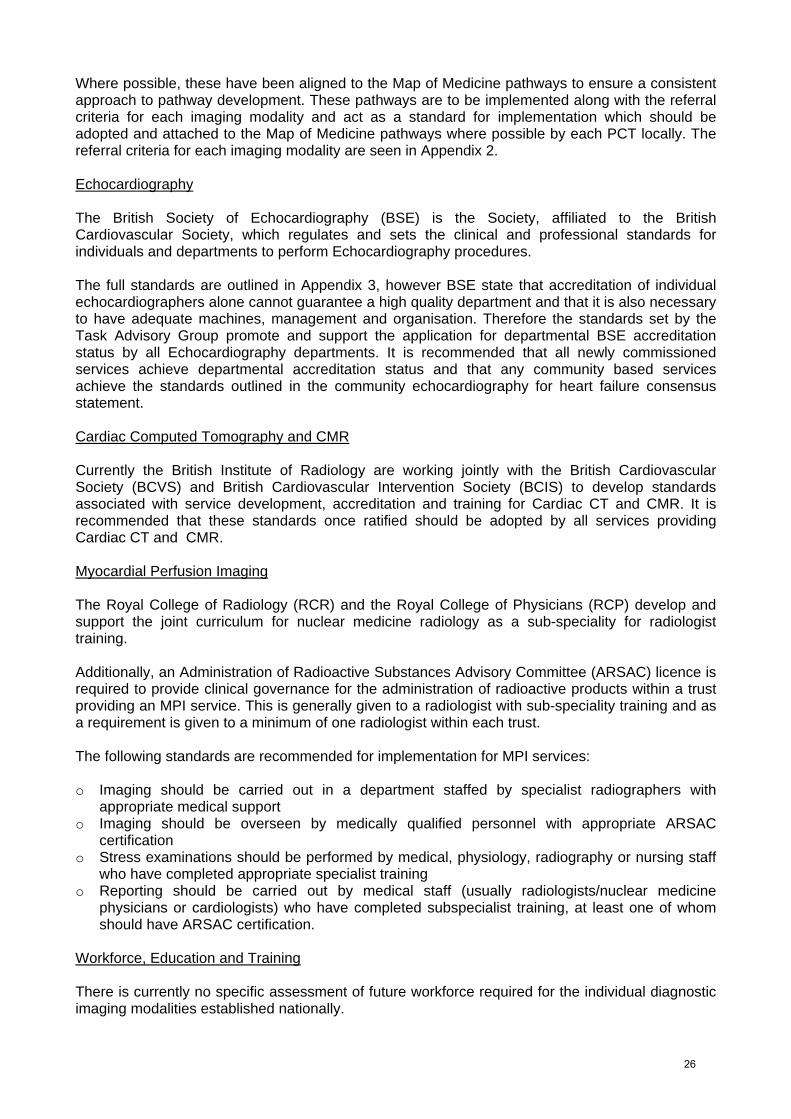
The Task advisory group recommend development of Stress Echocardiography and Cardiac CT services at every acute trust. This will alleviate the demands placed upon MPI, reduce the need for invasive diagnostic angiography and will increase clinical choice available locally whilst retaining the educational and speciality support available within the network, underpinned and supported by the development of cross trust MDT meetings. As can be seen below, this also leads to a saving and is therefore a cost effective solution. Future Modelling Cost Assessment By assessing the potential shift of 15% diagnostic angiography to Cardiac CT angiography, the potential savings for one year for the Network is highlighted below. (Table 6) Table 6
As established in Table 3, the activity target for MPI can be divided between the three imaging modalities, MPI, CMR and SE. Table 7 assesses potential savings over one year if activity was split between these three modalities. Table 7
Benefits to Patients, Clinicians and PCTs • Extended clinical choice of diagnostics to support individual patient clinical requirement • Local developments will enhance local services and support development of MDT
environments • Local developments will enhance access to services, reduce the potential for patient travel and
deliver more equitable provision of imaging modalities across the Network. • Access to non-invasive imaging modalities, in particular Cardiac CT, will reduce the need for
current and future invasive diagnostic angiography by an estimated 15%.
30
Strategy for Future Service Provision - Imaging Diagnostics During the development of this Strategy for imaging diagnostics it has become clear that no established referral criteria, pathways or clinical standards exist for all the different modalities discussed. The use of these diagnostics varies in use and is often dependant on local provision, availability and waiting times rather than clinically directed. Therefore the recommendations below aim to redirect this inconsistent approach and are developed to support both clinicians and commissioners when developing or expanding local services. Recommendations 1. To develop and establish multidisciplinary (MDT) environments with input from all imaging
modalities and where reporting can take place particularly for Cardiac CT and Cardiac MR considering the following; o Teleconferencing facilities, with viewing access to angiograms, cardiac CT, CMR and
Echocardiography at all sites o The assessment of existing and new consultant cardiologists and radiologists’ job plans to
ensure MDT forms a part of weekly workload, embedding MDT into practice. Each trust should identify appropriate radiologist support for cardiac imaging modalities
o Attendance by multidisciplinary healthcare professionals is essential o A ‘Hub and Spoke’ model may be of value for all imaging modalities. This will support new
developments, act as a platform for continued training and development and may be supported through MDT meetings.
2. Common protocols, pathways and standards (outlined within this strategy paper) to be
developed and adopted throughout the Network to support new developments and expansion of current services and modalities. Those standards currently being developed and ratified by the professional societies and bodies should be adopted by the Network and implemented into any service development or expansion. o Pathways developed along with referral criteria for each imaging modality should be
adopted and attached to the Map of Medicine pathways where possible by each PCT locally
o It is recommended that all newly commissioned services achieve departmental accreditation status and that any community based services achieve the standards outlined in the Community echocardiography for heart failure consensus statement (Appendix 3).
3. Support a significant planned increase in the availability of Cardiac CT, and stress
Echocardiography for Lancashire and Cumbria within the next five years as a phased approach ensuring sufficient capacity and appropriate equipment is considered in business and workforce planning: o As previously mentioned, the lack of availability of Stress Echo and Cardiac MRI has
historically driven clinical choice towards MPI and this may not be able to continue if radioisotope shortages persist. Clinical choice is currently restricted and availability of a wider range of diagnostic modalities across the Network should be accessible taking the inconvenience and cost incurred for patients travelling to other trusts into consideration
o Cardiac CT and Stress Echo should be developed in all sites. If current scanners available are capable of performing cardiac CT it should be planned to implement software within two years. New or replacement scanners/hardware should be commissioned with cardiac capabilities and planned to be established within 5 years
o In the absence of national tariffs, PCTs and acute trusts should consider Network agreed tariffs to support the development of cardiac CT and SE imaging modalities
o It is a recommendation that each trust should appoint at least one cardiologist with a special interest in imaging either from the existing cardiologist workforce or as additional staffing and also that each trust identify or appoint a radiologist with a special interest in cardiovascular imaging in particular, Cardiac CT and Cardiac CT angiography.
31

This would underpin the development and provide continuing clinical support for stress echocardiography services and allow jointly developed cardiology and radiology CT Angiography services.
32


CARDIAC ARRHYTHMIAS AND DEVICES
Introduction The National Service Framework (NSF) for Coronary Heart Disease (CHD) was published in March 2000. 61 However, arrhythmias and sudden cardiac death was omitted as the first seven chapters focussed on coronary artery disease prevention, diagnosis and treatment. Chapter 8 was later published in 2005 and extended the scope of the NSF to establish a blueprint for provision of fairer, faster high quality services for cardiac arrhythmias and sudden cardiac death. Cardiac arrhythmia affects more than 700,00062 people in England and is consistently within the top ten reasons for hospital admission. The most common arrhythmia is Atrial Fibrillation (AF) and although in 2005 affected 1% of the population (rising to 4% in the over 65s), recent work undertaken by NHS Improvement63 highlighted that it is an under recognised and under-treated arrhythmia and that systematic screening increases the detection of new cases by approximately 60%.63 Local work undertaken within our Network demonstrated a relative increase in prevalence by 5.3% in all ages (and by 10.2% in patients over 75 years of age). As AF is an important risk factor for stroke, this section will also recommend improvements that will assist in the diagnosis and treatment of patients with this particular arrhythmia. Finally, the treatment of arrhythmias often culminates in device implantation. These include bradycardia pacemakers for slow rhythm disturbances, implantable cardioverter defibrillators (ICDs) for tachycardia and life threatening arrhythmias and cardiac resynchronisation therapy (CRT) devices that treat patients suffering from heart failure and conduction disorders. Whilst there is clear overlap for CRT provision within the heart failure strategy, it will primarily be discussed here. CRT The treatment for heart failure aims to improve life expectancy and quality of life. Heart failure should be managed pharmacologically in accordance with the NICE clinical guideline ‘Chronic heart failure: management of chronic heart failure in adults in primary and secondary care’.64 However, as the condition becomes more severe, symptoms may no longer be controlled by pharmacological treatment. The aim of CRT is to improve the heart’s pumping efficiency by resynchronising the pumping action of the chambers and can either provide a pacing function alone (CRT-P) or also include an ICD (CRT-D). The benefits of implantation of a CRT device are related to improvements in the symptoms of heart failure, the extension of life of those with heart failure and a reduction in the incidence of sudden cardiac death. 65 This section of the Strategy will therefore highlight gaps in current provision and describe requirements for future service provision for the following: • Arrhythmia services • Atrial Fibrillation • Device implantation National Drivers As previously mentioned, Chapter 8 of the National Service Framework will be utilised to assess current gaps in service provision for arrhythmia services and will form the basis for a gap analysis and highlight the requirement for development of new arrhythmia services and support. 62
33

The Heart and Stroke Improvement Programme have developed national reports and commissioning guides to support the management of Atrial Fibrillation63 as a result from work undertaken across the country both with our local and other Networks. The results from the local project undertaken will highlight the support required in primary care for both Atrial Fibrillation patients and those with arrhythmia. Published NICE guidance and Technology Appraisals NICE Guidance will be used to support and influence the development of this Strategy. These will be considered and include: • NICE technology appraisal 95, Implantable cardioverter defibrillators for arrhythmias66 (Review
of technology appraisal 11). • NICE clinical guideline 36, Atrial Fibrillation: The management of Atrial Fibrillation.57 • NICE technology appraisal guidance 120, Cardiac Resynchronisation therapy for the treatment
of heart failure. 65 Finally, the Central Cardiac Audit Database (CCAD) has published national and locally commissioned device implantation activity reports. The National Heart Rhythm Devices: UK National Survey 200767 and the local review of pacemaker and ICD implantation practice in 200768 reports will be used to highlight the gaps in current provision and benchmark nationally, but will also be used to project and recommend future implantation rates. Gap Analysis Against Current Local Provision Arrhythmia Services Chapter 8 of the NSF identifies three quality requirements that address patient support, diagnosis and treatment and sudden cardiac death.62 The current provision within Lancashire and Cumbria will be matched against markers of good practice outlined within the NSF and recommendations made to support achievement of these. Key Quality Markers that are felt to have the most benefit to assist achieving the quality requirements are highlighted below within the gap analysis. Quality requirement one: Patient Support People with arrhythmias receive timely and high quality support and information based on assessment of their needs.
Markers Of Good Practice Current provision Recommendations to support this • People with arrhythmias
receive formal assessment of their support needs and those at significantly increased risk of anxiety, depression or a poor quality of life receive appropriate care
• People with long-term conditions receive support in managing their illness from a named arrhythmia care co-ordinator
• Good quality, timely information about arrhythmic conditions is given by appropriately trained staff
• No arrhythmia care co-ordinator or support posts are established within the Network
• Currently only one PCT provides a local arrhythmia clinic within the Network
• Develop joint commissioning for tertiary based arrhythmia nurses/practitioners to support device patients where local implantation does not exist
• Develop arrhythmia clinics and arrhythmia nurses/practitioners across 1° and 2° care within each health economy to support device implantation and arrhythmia patients locally
• Establish requirements for psychology services to support patients, particularly those with ICDs
34

Quality requirement two: Diagnosis and Treatment People presenting with arrhythmias, in both emergency and elective settings, receive timely assessment by an appropriate clinician to ensure accurate diagnosis and effective treatment and rehabilitation.
Markers Of Good Practice Current provision Recommendations to support this • Patients who survive out-
of-hospital cardiac arrest and patients presenting with pre-excited atrial fibrillation are assessed by a heart rhythm specialist prior to hospital discharge
• Patients are assessed urgently by a heart rhythm specialist if they have any of the findings in note (1)
• Patients are referred to a heart rhythm specialist if they have any of the findings in note (2)
There is limited provision of an electrophysiology service at Lancashire Cardiac Centre. Full EP service including surgical ablation of atrial fibrillation within the Network does not exist or is not commissioned and patients are required to travel out of Network for EP procedures. Complex invasive pacing procedures often require surgical intervention which is currently performed in cardiac surgical theatres
• Consider the development of a surgical AF ablation service in conjunction with an electrophysiology service at LCC
• Consider the development of a ‘hybrid’ theatre-laboratory to support invasive complex surgical pacing procedures
• Support referrals to tertiary centre in Network once electrophysiologist is established
Note (1) Patients with the following:
• Syncope or any other symptom(S) suggestive of an arrhythmia and a personal history of structural heart disease or a family history of Sudden Cardiac Death (SCD)
• Recurrent syncope associated with palpitations • Syncope and pre-excitation • Documented 3rd degree AV Block (not associated with acute MI) • Recurrent syncope in whom a life-threatening cause has not been excluded • Documented Ventricular Tachycardia (VT)
Note (2) Patients with the following:
• A presumed diagnosis of VT • Wolffe-Parkinson-White (WPW) syndrome or asymptomatic pre-excitation • Symptomatic regular recurrent supraventricular tachycardia (SVT) which is unsuccessfully treated with one type
of medication or who would prefer not to take long-term medication • Recurrent atrial flutter • Symptomatic atrial fibrillation despite optimal medical therapy • First degree relatives of victims of sudden cardiac death who died below the age of 40 years • Recurrent unexplained falls
Quality requirement three: Sudden Cardiac Death When sudden cardiac death occurs, NHS services have systems in place to identify family members at risk and provide personally tailored, sensitive and expert support, diagnosis, treatment, information and advice to close relatives.
35
Markers Of Good Practice Current provision Recommendations to support this
• Individuals who experience episodes of sustained palpitation and/or unexplained impaired consciousness, particularly if repeated or triggered by exercise, have rapid access to cardiac evaluation, including 12 lead, continuous ECG monitoring and 2D Echo
• Suitable bereavement services are available for those who have lost a family member
• •An expert post mortem is carried out and appropriate tissue retained if informed consent is given
• Evaluation of families who may have inherited cardiac disease takes place in a dedicated clinic
• Cardiac service provision exists at each acute trust; however local assessment of bereavement and dedicated clinic assessment will need to be assessed.
• Genetic counselling and further genetic testing is available for the North West at MRI
Local assessment of bereavement services and consideration be given to development of dedicated clinics to aid the diagnosis, management and support for the families
Atrial Fibrillation Chapter 8 of the CHD NSF also highlights that cardiac arrhythmia affects more than 700,000 people in England and is consistently in the top ten reasons for hospital admission, using up significant A&E time and bed days. 62 Atrial fibrillation (AF), the most common arrhythmia, affects up to 1% of the population (rising to 4% in the over 65s) and absorbs almost 1% of the entire budget of the NHS.69 AF is the most common sustained cardiac arrhythmia and, if left untreated, is a significant risk factor for stroke and other morbidities and accounts for 14% of all strokes.83 In recent years there have been significant improvements in both technology and clinical skills that are enabling improved prevention, diagnosis and treatment of these conditions62. However it is important to highlight that AF is both under recognised and under treated. Arrhythmias, or irregular heartbeats, range in their severity – from a minor inconvenience or discomfort to a potentially fatal problem. The symptoms a person may experience include palpitations, dizziness or blackouts. They are very common, particularly among older people. They can have a profound effect on the quality of life of the people who suffer from them and there is a good deal that the NHS can do to tackle them. 62 Following the release in 2006 of the NICE Guidelines for Atrial Fibrillation, the Fylde Coast Health Economy produced an algorithm and supporting guidance, based on the NICE recommendations, but specifically aimed at facilitating their uptake in primary care. These was subsequently adapted and adopted by the Cardiac and Stroke Network and implementation of this guideline became the focus of the National Project with the Heart Improvement Team. The project set out to establish a baseline against which progress and improvement in the identification and management of patients with AF could be measured.
36

The chart below details the comparison between prevalence of AF in the six Lancashire and Cumbria pilot practices at the beginning and the end of the project.
The outcomes from the project include the following and these should form the basis of recommendations for implementation: • As a result of opportunistic screening and raising awareness of the condition, AF registers at
the end of the project revealed a relative increase in prevalence of 5.3% of the total population. This increased to a relative increase in prevalence of 10.2% in the over 75 age group.
• Prescribing data illustrated that Warfarin prescribing, in particular in the >75s was below the level that is expected and although that level rose by the end of the project, there is further work to be done to support the decision making process in Primary Care. NICE estimate that 46% of patients that should be on Warfarin are not receiving it
• Each of the practice teams identified a training need in relation to ECG recording and interpretation and this led to four the practices undertaking a Telemedicine pilot. This provided the opportunity to evaluate ECG interpretation skills and also test out the benefit of Telemedicine through a single lead monitoring device to diagnose arrhythmias. In view of the limitations of the pilot the outcomes in relation to ECG interpretation were not entirely conclusive, however, the single lead arrhythmia monitoring device proved to be effective, in obtaining a conclusive diagnosis in all patients and allowed access to an earlier diagnosis than current pathways provide
Key Recommendations • PCTs are advised to recommend that practices undertake validation of their AF registers and
undertake medication reviews in order to ensure that medication is being appropriately prescribed for rate control and anticoagulation; Medicines Management should provide support in this process
• Opportunistic screening for AF should be encouraged and adopted by all members of the primary care teams
• Manual pulse check prompts should be inserted into all appropriate long term conditions monitoring templates and be embedded in daily practice particularly for those as high risk
• PCTs should review ECG recording and interpretation competencies across primary care and consider the benefits of telemedicine to support GPs and ensure an equitable service
• Access to ambulatory monitoring in the community for the diagnosis of arrhythmias should be considered, ensuring all services achieve the same clinical standards of service delivery as currently provided by the acute trusts
• PCTs are advised to implement the Network AF Guidelines to provide support to primary care practitioners in the management of AF
37

• The Heart and Stroke Improvement team have made a national recommendation that PCTs should consider the use of the GRASP – AF tool (available from NHS Improvement)70 to facilitate audit and aid identification of high risk patients that would benefit from Warfarin.
Devices A review of pacemaker and implantable cardioverter defibrillator implantation practice in 2007 was undertaken by the Cardiac Network’s Device Survey Group and published a local audit report for Lancashire and Cumbria in April of this year63. As can be seen in Figure 1, activity rates for pacemaker implantation (blue), ICD implantation (red) and cardiac resynchronisation therapy (CRT) devices (green) display our networks position when compared nationally. The low implanting Networks are displayed at the top and our Network performs poorly for both pacing and ICD device implantation rates, yet relatively well for CRT implantation. However further analysis of the data will demonstrate that all PCTs do not achieve recommended target levels set by Heart Rhythm UK (HRUK) and NICE. Figure 1 - The Range of New Implant Rate across Networks in 2007
38
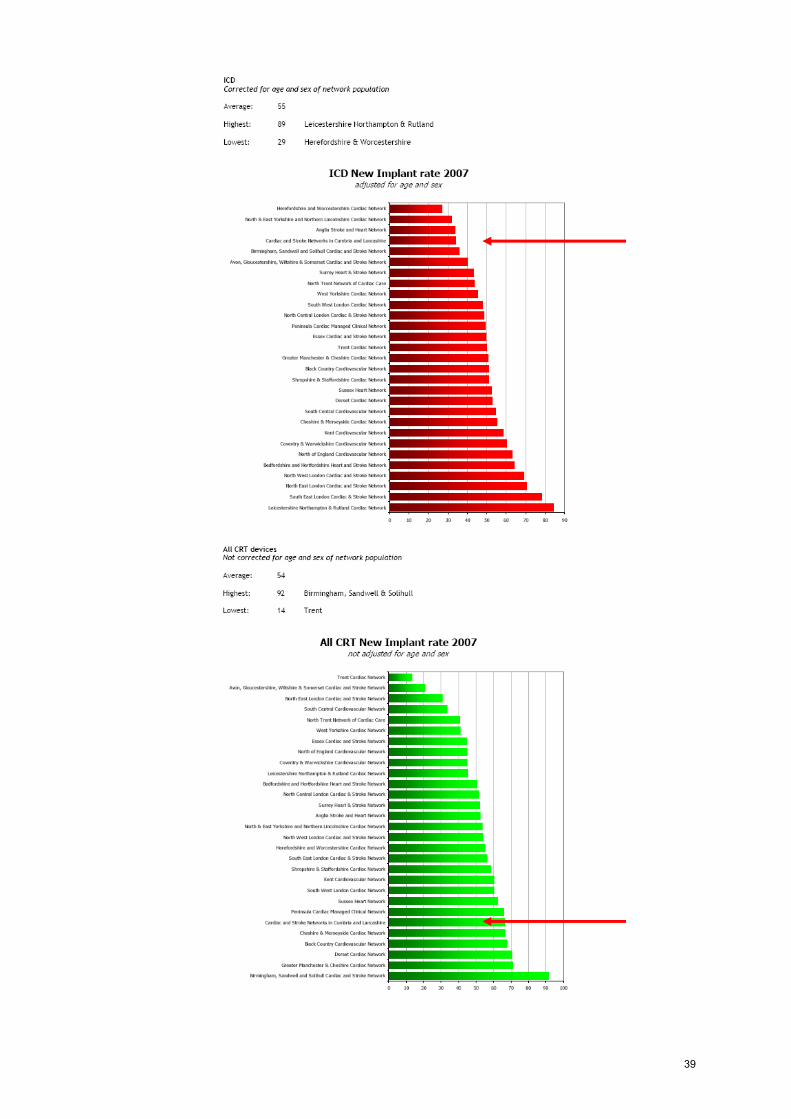
39
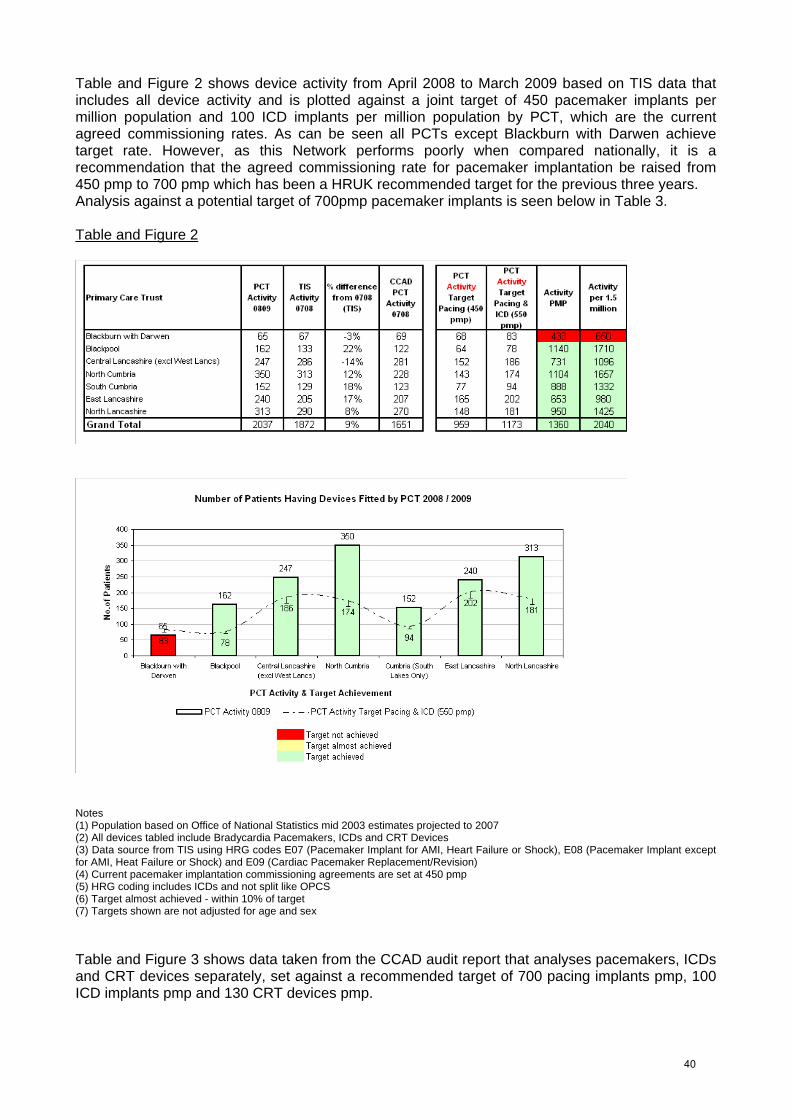
Table and Figure 2 shows device activity from April 2008 to March 2009 based on TIS data that includes all device activity and is plotted against a joint target of 450 pacemaker implants per million population and 100 ICD implants per million population by PCT, which are the current agreed commissioning rates. As can be seen all PCTs except Blackburn with Darwen achieve target rate. However, as this Network performs poorly when compared nationally, it is a recommendation that the agreed commissioning rate for pacemaker implantation be raised from 450 pmp to 700 pmp which has been a HRUK recommended target for the previous three years. Analysis against a potential target of 700pmp pacemaker implants is seen below in Table 3. Table and Figure 2
Notes (1) Population based on Office of National Statistics mid 2003 estimates projected to 2007 (2) All devices tabled include Bradycardia Pacemakers, ICDs and CRT Devices (3) Data source from TIS using HRG codes E07 (Pacemaker Implant for AMI, Heart Failure or Shock), E08 (Pacemaker Implant except for AMI, Heat Failure or Shock) and E09 (Cardiac Pacemaker Replacement/Revision) (4) Current pacemaker implantation commissioning agreements are set at 450 pmp (5) HRG coding includes ICDs and not split like OPCS (6) Target almost achieved - within 10% of target (7) Targets shown are not adjusted for age and sex Table and Figure 3 shows data taken from the CCAD audit report that analyses pacemakers, ICDs and CRT devices separately, set against a recommended target of 700 pacing implants pmp, 100 ICD implants pmp and 130 CRT devices pmp.
40

As can be seen, NHS Central Lancashire achieves this target for pacing, no PCT achieves the target for ICD implants and both NHS Blackpool and NHS North Lancs achieve CRT targets. The Task Advisory Group responsible for developing this part of the Strategy suggest that NICE guidance supporting implantation of CRT devices for heart failure has led to a change in clinical practice raising the implant levels of CRT and decreasing those for ICDs. Therefore it was requested that these two targets be merged and levels reassessed. The final graph displays this joint target and shows Blackpool as the only PCT achieving target. Table and Figures 3 Strategy Recommended Commissioning Targets for all Devices Activity taken from January 07 to December 07
Notes (1) Population based on Office of National Statistics mid 2003 estimates projected to 2007 (2) Heart Rhythm UK (HRUK) targets are set at 700 pmp for pacing implants. (3) NICE recommended targest are set at 100 pmp for ICD Implants. (4) HRUK recommended targest are set at 130 pmp for CRT Implants. (5) Current commissioning agreements are set at 450 pmp for Bradycardia pacing Implants, a recommendation to increase commissioning agreements to 700 pmp will be part of the cardiac strategy. (6) Joint ICD & CRT targets reflect a chnge in clinical practice, recommended by the clinicians from the Strategy Task Advisory Group (TAG) (7) Targets shown are not adjusted for age and sex
41
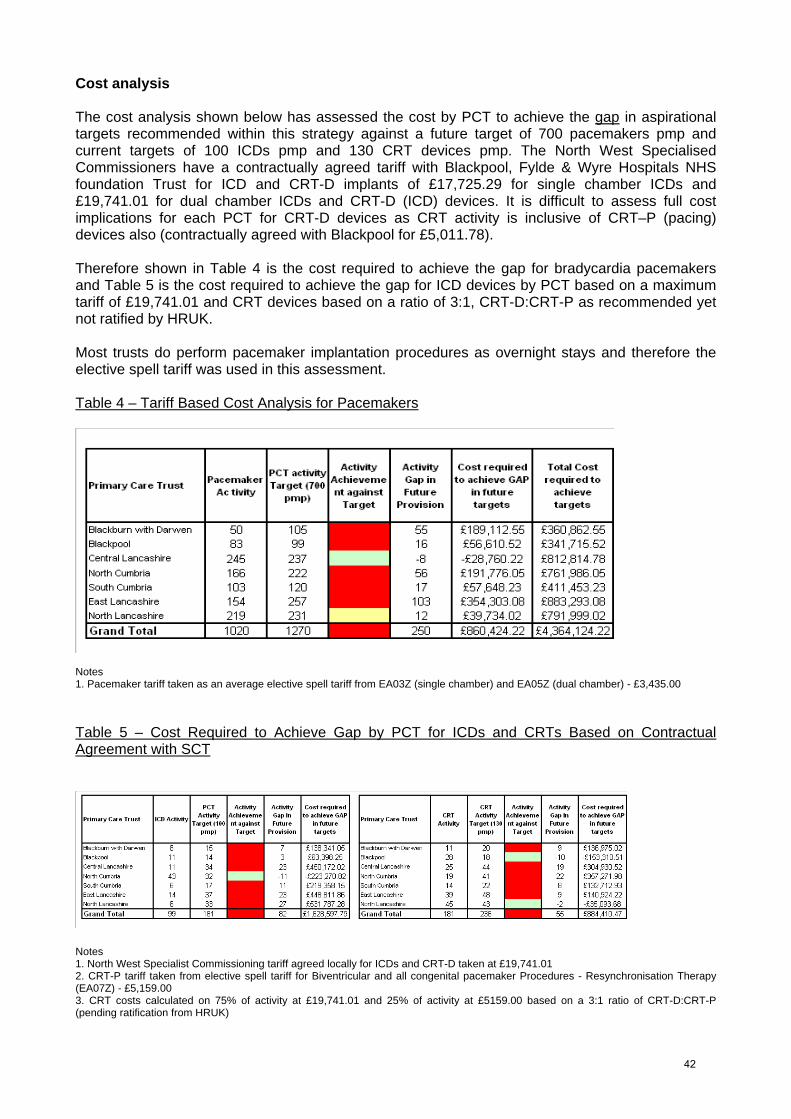
Cost analysis The cost analysis shown below has assessed the cost by PCT to achieve the gap in aspirational targets recommended within this strategy against a future target of 700 pacemakers pmp and current targets of 100 ICDs pmp and 130 CRT devices pmp. The North West Specialised Commissioners have a contractually agreed tariff with Blackpool, Fylde & Wyre Hospitals NHS foundation Trust for ICD and CRT-D implants of £17,725.29 for single chamber ICDs and £19,741.01 for dual chamber ICDs and CRT-D (ICD) devices. It is difficult to assess full cost implications for each PCT for CRT-D devices as CRT activity is inclusive of CRT–P (pacing) devices also (contractually agreed with Blackpool for £5,011.78). Therefore shown in Table 4 is the cost required to achieve the gap for bradycardia pacemakers and Table 5 is the cost required to achieve the gap for ICD devices by PCT based on a maximum tariff of £19,741.01 and CRT devices based on a ratio of 3:1, CRT-D:CRT-P as recommended yet not ratified by HRUK. Most trusts do perform pacemaker implantation procedures as overnight stays and therefore the elective spell tariff was used in this assessment. Table 4 – Tariff Based Cost Analysis for Pacemakers
Notes 1. Pacemaker tariff taken as an average elective spell tariff from EA03Z (single chamber) and EA05Z (dual chamber) - £3,435.00 Table 5 – Cost Required to Achieve Gap by PCT for ICDs and CRTs Based on Contractual Agreement with SCT
Notes 1. North West Specialist Commissioning tariff agreed locally for ICDs and CRT-D taken at £19,741.01 2. CRT-P tariff taken from elective spell tariff for Biventricular and all congenital pacemaker Procedures - Resynchronisation Therapy (EA07Z) - £5,159.00 3. CRT costs calculated on 75% of activity at £19,741.01 and 25% of activity at £5159.00 based on a 3:1 ratio of CRT-D:CRT-P (pending ratification from HRUK)
42

Age Adjusted Cost Analysis Table 6 has considered using age adjusted targets, taken from ‘A Review of Pacemaker and Implantable Cardioverter Defibrillator Implantation Practice in 2007‘ which has calculated the relative need for bradycardia pacemakers and ICDs only. 68 Each PCT’s relative need is shown in Table 7. Table 6 -Age Adjusted Cost Required to Achieve Gap by PCT for Pacemakers and ICDs
Notes 1. Pacemaker tariff taken as an average elective spell tariff from EA03Z (single chamber) and EA05Z (dual chamber) - £3,435.00 2. North West Specialist Commissioning tariff agreed locally for ICDs taken at £19,741.01 3. Age and sex adjusted targets, against England average, are established by PCT as the "relative need" for pacemakers and ICDs - shown below Table 7 -Relative need for Pacemakers and ICDs by PCT
As can be seen using age adjusted targets based on a recommended 700pmp pacemaker implants requires a further investment of £300,186 and for ICDs a further £209,815 is required to achieve the gap against future targets recommended across the Network. Cost – Patient Benefit of CRT Implantation The NICE technology appraisal guidance, cardiac resynchronisation therapy for the treatment of heart failure65, highlights the benefits of CRT implantation are related to improvements in the symptoms of heart failure, the extension of life of those with heart failure and a reduction in the incidence of sudden cardiac death. In assessments undertaken to support NICE guidance, CRT-P was associated with an incremental cost of £11,630 and a quality–adjusted life year (QALY) gain of 0.70 (equivalent to 256 days of full health) compared with optimal pharmacological therapy alone. This equated to an incremental cost-effectiveness ratio (ICER) of £16,735 per QALY over a lifetime time horizon of 5 years. CRT-D was associated with an incremental cost of £23,320 and a QALY gain of 0.99 (equivalent to 361 days of full health) compared with optimal pharmacological therapy alone. This equated to an ICER of £26,350 per QALY when a lifetime time horizon of 5 years was considered.
43
Recommendations The Task Advisory Group by majority consensus has agreed the following recommendations that are based on gap analysis undertaken and successful outcomes from the national AF Management in Primary Care project and it is recommended these be implemented over the next five years according to each individual PCT’s priorities. These include: 1. Recommend introduction of support for device/arrhythmia patients, and address gap in
arrhythmia service provision against Chapter 8 of the NSF ° Develop joint commissioning for tertiary (acute) based arrhythmia nurses/practitioners to
support device patients where local implantation does not exist ° Develop arrhythmia nurses/care co-ordinators across 1° and 2° care within each health
economy – important if ICD/CRT developed locally ° Establish requirements for psychology services to support patients, particularly those with
ICDs 2. Recommend the introduction of arrhythmia clinics in each health economy to address gap in
arrhythmia service provision against Chapter 8 of the NSF ° Consider specialist accredited practitioner led services and clinics (e.g. GPwSI or PwSI), all
such clinics should have close links and interaction with their local secondary/tertiary centres as joint ownership
° Ensure audit of new clinics is undertaken to benchmark against current outpatient delivery (use the Network developed database to provide audit comparison across the Network)
° Expand cardiac physiology and specialist practitioner workforce to support these clinics ° Consider link to syncope/care of elderly clinics as referral pathway
3. Support the development of a full EP service at the tertiary centre
° Consider the development of a surgical AF ablation service in conjunction with an electrophysiology service at LCC
° Consider the development of a ‘hybrid’ Theatre-Laboratory to undertake complex, invasive pacing procedures at the Lancashire Cardiac Centre
° Support referrals to tertiary centre in Network once electrophysiologist is established. 4. Support the promotion of the management of AF in Primary Care
° Implement recommendations made as result of the Network AF in Primary Care project and the Heart and Stroke Improvement Programme, Commissioning for Stroke Prevention – The Role of Atrial Fibrillation document
° Each PCT to adopt Network AF Guidelines and attach locally to Map of Medicine and ensure robust pathways for investigation and referral are established
° Each PCT should assess the requirement of telemedicine to support ECG interpretation. If a cross PCT implementation approach is not taken, consider acute trust provision or private provider for those ECGs that GPs have difficulty with rather than all ECGs
° Each PCT to have ready access to a range of ambulatory monitoring devices to assist in the detection of arrhythmias and for all diagnostic service providers to achieve the same standards of competency and clinical delivery as those provided by the acute trusts
° Robust mechanisms for continuing education to be in place to support the identification and management of arrhythmia patients
5. Increase commissioning agreements to 700 pacemaker implants per million population (pmp) from 450 pmp to be aligned with HRUK recommended levels
44

6. Increase device implantation rates for all devices, Bradycardia pacemakers, Implantable Cardioverter Defibrillators (ICD) and Cardiac Resynchronisation Therapy (CRT) devices to reach recommended aspirational target levels (NICE and HRUK) within the next five years ° Increase education within 1° care ° Establish links in 2° care to MAU/care of elderly and syncope clinics ° Establish link with heart failure practitioners, pathway and strategy for heart failure to
increase implant rates ° Use Map of Medicine/locally agreed established pathways in 1° care to direct referrals for
assessment and potential implantation ° Support devolvement of ICD/CRT services to DGHs to generate extra activity
7. Support acute trusts to develop ICD/CRT services if there is a clinical need to do so to address
gap in service provision against recommended target levels (NICE and HRUK) ° Develop standards national/local to support implementation of services (including NICE) ° Provide training and service specification guidance ° Ensure clear pathway of referral is established and access to service meets 18 week
targets ° Ensure trained specialist workforce achieves standards of expertise expected matched to
current tertiary centre provision Summary By adopting and implementing these recommendations, primary care and acute trusts will assist in achieving national targets, fulfil the quality requirements set within national guidance and policy and improve access and quality of care to patients with arrhythmias and those benefiting from device implantation within Lancashire and Cumbria.
45


REVASCULARISATION AND CARDIAC SURGERY
Introduction Coronary heart disease is a narrowing or blockage of the coronary arteries by atheroma, which can lead to angina, and blood clots (coronary thrombosis), which in turn, can lead to heart attack, heart failure, and/or sudden death. Revascularisation encompasses any intervention to improve the coronary circulation and includes thrombolysis, angioplasty and coronary artery bypass graft surgery. This section of the strategy will explore emergency and elective aspects of the patient pathway, focusing first on acute coronary syndromes, treatment of ST-segment-elevation myocardial infarction (STEMI) including thrombolysis and primary angioplasty. It will then look at diagnostic angiography, angioplasty and cardiac surgery. The cardiac surgery section will also consider valve surgery and other recent surgical developments such as Trans-catheter Aortic Valve Implant (TAVI) and Port Access Mitral Valve/Tricuspid Valve surgery (PA MV/TV). Surgical ablation for atrial fibrillation is considered in the Arrhythmia section of the strategy. Angiography An angiogram is a diagnostic procedure in which a fine catheter (tube) is inserted via a peripheral artery and manipulated by the operator such that the tip of the catheter engages the origins of the coronary arteries, which run over the surface of the heart. X-ray opaque dye is then injected into the coronary arteries to obtain an image of their anatomy and to assess the presence of any coronary narrowing (atheroma). It has guided and informed the treatment of coronary angioplasty for many years and is also utilised to assist in pacemaker and device implantation, electrophysiology and cardioversion procedures as well as assessing myocardial function structure and cardiac anatomy. Percutaneous Coronary Intervention (PCI) Percutaneous coronary intervention (PCI) encompasses a variety of procedures used to treat patients with diseased coronary arteries caused by a build-up of cholesterol, inflammatory material and scar tissue in the walls of arteries, (plaque) that can reduce blood flow. When plaque becomes ‘unstable’ and initiates blood clot formation within a coronary artery, the artery can become occluded, causing a heart attack. PCI involves the insertion of a small balloon-tipped catheter, from the femoral or radial artery into coronary arteries. It is then inflated, which squashes the fatty tissue out of the way and widens the artery. In most cases a stent is then implanted - a very fine stainless steel mesh tube that stays permanently in place to keep the artery wide open. Treatment thus aims to prevent the arteries blocking (which might cause a heart attack) and improve flow to the heart muscle to alleviate the symptoms of angina. Coronary Artery Bypass Graft (CABG) CABG is an open heart operation in which blockages to the coronary arteries are bypassed by grafting on a length of artery or vein to bring increased blood supply to the heart muscle. Any treatment involving the coronary arteries may be associated with complications such as stroke, heart attack or death. As demonstrated by the National Angioplasty Audit,72 some patients are at higher risk of developing complications than others. For example, the treatment of a patient in a stable situation is associated with complication rates of less than 1% but, in the context of an acute heart attack, this may rise to 10% or more.
46
National Drivers The National Service Framework (NSF) for Coronary Heart Disease (CHD)61 was published in 2000. Its focus was coronary artery disease prevention, diagnosis and treatment. The NSF established a non Standardised Mortality Ratio (SMR) adjusted target for all coronary revascularisation of 1,500 pmp.61 It is established practice to adjust this for need. Within Lancashire and Cumbria application of SMRs increases this revascularisation target to 3,356 per annum. The following NICE guidelines relate to this section and have been considered during development of the strategy: • Technology Appraisal Guidance 71 – Guidance on the Use of Coronary Artery Stents. 55 • Interventional Procedure Guidance 266 – Transcatheter aortic valve implantation for aortic
stenosis71 • Acute Coronary Syndromes, final publication expected Feb 201058 Current Revascularisation Levels In June 2009 the Access to Cardiac Care in the UK (ACCUK) 73 report, commissioned by the British Cardiovascular Society, the British Heart Foundation and the Cardio and Vascular Coalition identified the wide range of programmes to modernise and improve cardiac services that were put in place following publication of the NSF. These included:- • A centrally funded capital project to improve facilities and increase capacity at existing
cardiothoracic centres. • An increase in the number of catheter laboratories in both cardiothoracic centres and district
general hospitals with the aim of improving local access. • An increase in the number of consultant cardiologists in England from 483 full time equivalents
(fte) in 2000 to 783 fte in 2008 (up 62%). • An increase in the number of cardiothoracic surgeons in England from 183 full time equivalents
(fte) in 2000 to 270 fte in 2008 (up 47%). • A reduction in waiting times for interventions. It is widely accepted that the impact of these developments significantly contributed to the achievement of the public services agreement target, a 40% reduction of mortality from circulatory diseases in the under 75s by 2010, five years ahead of schedule. Despite this investment and expansion of capacity regional variations in revascularisation rates have continued to the extent that in 2006 these rates in London were 40% above expected levels and in Lancashire and Cumbria 18% below.
47
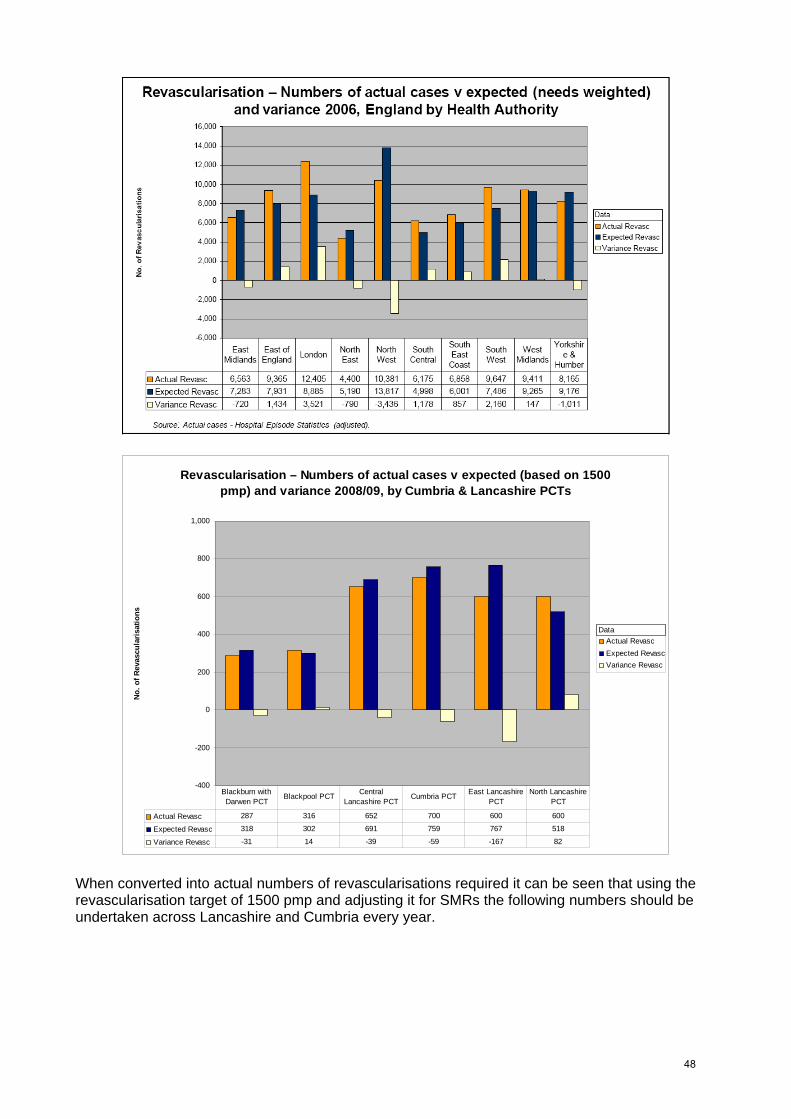
Revascularisation – Numbers of actual cases v expected (based on 1500 pmp) and variance 2008/09, by Cumbria & Lancashire PCTs
-400
-200
0
200
400
600
800
1,000
No. o
f Rev
ascu
laris
atio
ns
Actual RevascExpected RevascVariance Revasc
Actual Revasc 287 316 652 700 600 600
Expected Revasc 318 302 691 759 767 518
Variance Revasc -31 14 -39 -59 -167 82
Blackburn with Darwen PCT
Blackpool PCT Central Lancashire PCT
Cumbria PCT East Lancashire PCT
North Lancashire PCT
Data
When converted into actual numbers of revascularisations required it can be seen that using the revascularisation target of 1500 pmp and adjusting it for SMRs the following numbers should be undertaken across Lancashire and Cumbria every year.
48
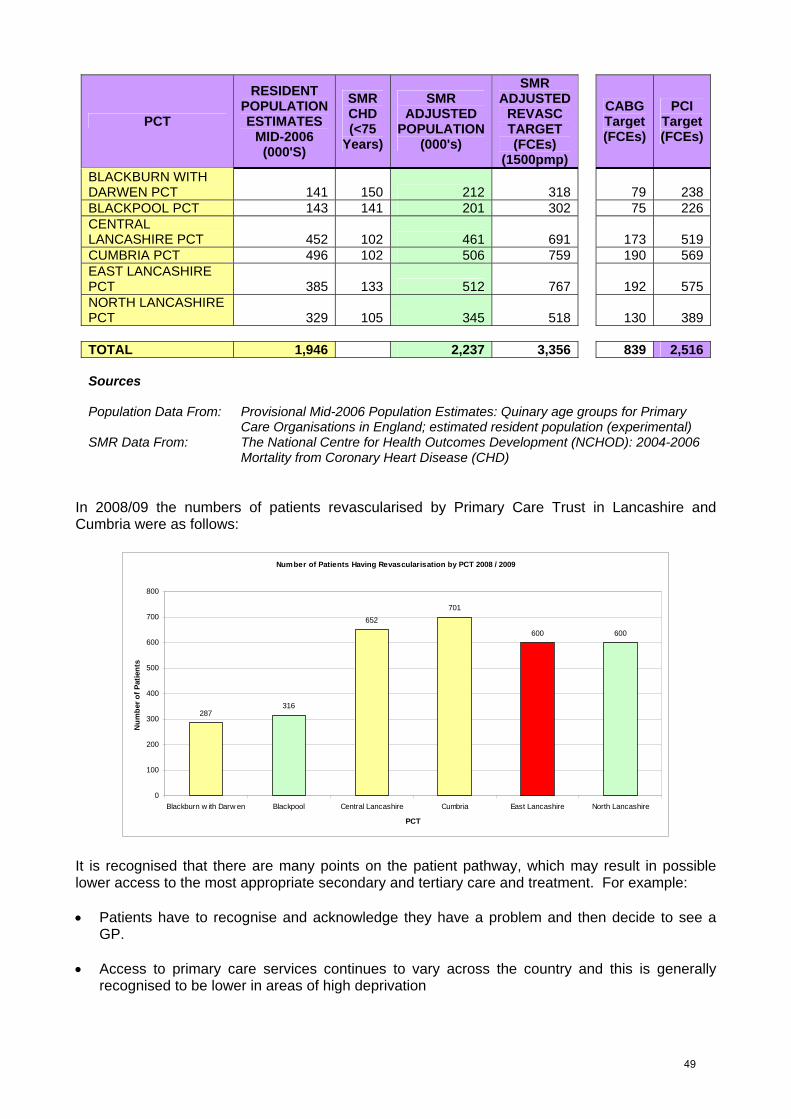
PCT
RESIDENT POPULATION ESTIMATES
MID-2006 (000'S)
SMR CHD (<75
Years)
SMR SMR ADJUSTED CABG PCI ADJUSTED REVASC
POPULATION (000's)
TARGET (FCEs)
(1500pmp)
Target Target (FCEs) (FCEs)
BLACKBURN WITH DARWEN PCT 141 150 212 318 79 238BLACKPOOL PCT 143 141 201 302 75 226CENTRAL LANCASHIRE PCT 461 691 173 519452 102CUMBRIA PCT 496 102 506 759 190 569EAST LANCASHIRE PCT 385 133 512 767 192 575NORTH LANCASHIRE PCT 345 518 130 389329 105 TOTAL 1,946 2,237 3,356 839 2,516 Sources Population Data From: Provisional Mid-2006 Population Estimates: Quinary age groups for Primary
Care Organisations in England; estimated resident population (experimental) SMR Data From: The National Centre for Health Outcomes Development (NCHOD): 2004-2006
Mortality from Coronary Heart Disease (CHD) In 2008/09 the numbers of patients revascularised by Primary Care Trust in Lancashire and Cumbria were as follows:
Number of Patients Having Revascularisation by PCT 2008 / 2009
287316
652701
600 600
0
100
200
300
400
500
600
700
800
Blackburn w ith Darw en Blackpool Central Lancashire Cumbria East Lancashire North Lancashire
PCT
Num
ber o
f Pat
ient
s
It is recognised that there are many points on the patient pathway, which may result in possible lower access to the most appropriate secondary and tertiary care and treatment. For example: • Patients have to recognise and acknowledge they have a problem and then decide to see a
GP. • Access to primary care services continues to vary across the country and this is generally
recognised to be lower in areas of high deprivation
49

• The availability of access to specialist cardiac care locally influences the levels of primary to secondary referrals and cardiology services
• The type of treatment patients presenting with a first heart attack receive is determined by the
type of specialist they see. Those that see a cardiologist are 50% more likely to be referred for an angiogram than those seen by a general physician.
• The provision of more local specialist services affects demand, increases general awareness,
referral and treatment and therefore access rates. In England between 2000 and 2006: • Angiography numbers increased by 49% • PCI numbers increased by 149% • CABG increased by 11% • Overall revascularistaion rates rose by 60% to 1,642 pmp Despite these positive changes the ACCUK report on benchmarking, the UK internationally ranked it 20th in a comparison of revascularisation rates per million population for 22 of the 30 OECD countries.72
Both local, national and international data demonstrate that in Cumbria and Lancashire, despite the good progress made since the appointment of additional cardiologists and the expansion of district general catheter laboratories, inequalities of access remain and revascularisation rates in the most deprived communities have yet to reach the NSF target, whilst those closest to tertiary centres have achieved or exceeded it. Martin et al’s work72, which used the incidence of indications approach, analysis of national trends in revascularisation, international comparisons and clinical consensus modelled three possible growth assumptions. Within the north west to achieve equity of access, relative to need, year on year growth from 2006 to 2015 of 4% (1,900 pmp), 5% (2,200 pmp) or 6% (2,500 pmp) would be necessary.
50

The north west of England has a projected need which is 22% higher than the UK average by 2020. Future Revascularisation Targets for Lancashire & Cumbria In order to address the inequities that exist between local health economies in Lancashire and Cumbria and within England, revascularisation rates across the Network should be increased to 1,500 pmp in 2009 to 1,900 pmp by 2011 and 2,250 pmp by 2015. This would equate to the following revascularisation activity by PCT.
SMR SMR SMR
PCT ADJUSTED
REVASC TARGET (FCEs)
(1500pmp)
ADJUSTED ADJUSTED REVASC REVASC TARGET TARGET (FCEs) (FCEs)
(1900pmp) (2250pmp)
BLACKBURN WITH DARWEN PCT 318 402 477 BLACKPOOL PCT 302 382 453 CENTRAL LANCASHIRE PCT 691 876 1,037 CUMBRIA PCT 759 962 1,139 EAST LANCASHIRE PCT 767 972 1,151 NORTH LANCASHIRE PCT 518 656 777 TOTAL 3,356 4,250 5,033
Local provision of services and facilities Revascularisation is offered to patients in both elective and non elective circumstances. The following table shows the current services offered. Diagnostic angiography for non elective acutely ill patients are only, on the whole, undertaken in Blackpool, Middlesbrough and Newcastle, which are the tertiary centres serving the Network’s population. Approximately 10% of patients living in Lancashire and Cumbria access revascularisation at centres outside of Network tertiary flows, e.g. Liverpool.
51
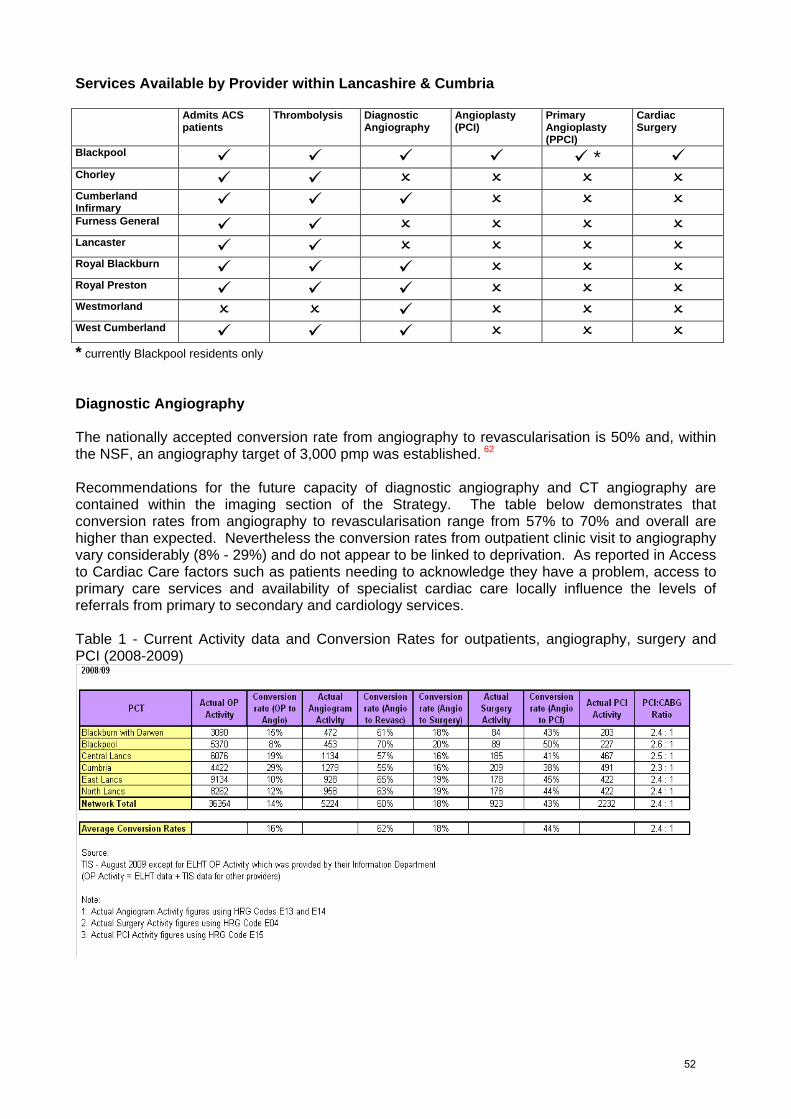
Services Available by Provider within Lancashire & Cumbria
Admits ACS patients
Thrombolysis Diagnostic Angiography
Angioplasty Primary Angioplasty
Cardiac (PCI) Surgery
(PPCI)
* Blackpool
Chorley
Cumberland Infirmary
Furness General
Lancaster
Royal Blackburn
Royal Preston
Westmorland
West Cumberland
* currently Blackpool residents only Diagnostic Angiography The nationally accepted conversion rate from angiography to revascularisation is 50% and, within the NSF, an angiography target of 3,000 pmp was established. 62 Recommendations for the future capacity of diagnostic angiography and CT angiography are contained within the imaging section of the Strategy. The table below demonstrates that conversion rates from angiography to revascularisation range from 57% to 70% and overall are higher than expected. Nevertheless the conversion rates from outpatient clinic visit to angiography vary considerably (8% - 29%) and do not appear to be linked to deprivation. As reported in Access to Cardiac Care factors such as patients needing to acknowledge they have a problem, access to primary care services and availability of specialist cardiac care locally influence the levels of referrals from primary to secondary and cardiology services. Table 1 - Current Activity data and Conversion Rates for outpatients, angiography, surgery and PCI (2008-2009)
52

Routes to Revascularisation Acute Coronary Syndrome (ACS) ACS is a clinical condition, usually a combination of chest pain and other features, which occur as a result of abrupt impairment or cessation of blood flow to the heart. The subtypes of ACS include unstable angina (UA) and two types of heart attack, in which the heart muscle is damaged as a consequence of the impairment of blood flow. Damage is indicated by a rise in cardiac enzymes, as measured on a blood sample. The two types of myocardial infarction are named according to the appearance of the electrocardiogram (ECG) as ST segment elevation myocardial infarction (STEMI) and non- ST segment elevation myocardial infarction (NSTEMI). The Network ACS Protocol gives guidance for the investigation and treatment of patients, which may include angiography and revascularisation. For the purpose of this Strategy, this ACS section will not cover STEMI. NSTEMI is incorporated into the North West SHA Advancing Quality initiative and clearer insight into provider performance of quality care will be possible when performance data is made public in spring 2010. Currently different definitions for MI are used within provider sites causing coding discrepancies and making benchmarking difficult. Agreement has been reached within the Cardiac Clinical Advisory Group to work on the production of a Network wide definition of MI including collaborative working with the Pathology Commissioning Network to establish standardised assays for Troponin levels. Reported Incidence of Angina, Chest Pain & NSTEMI in Lancashire & Cumbria 2007/08
PCT Angina Chest Pain NSTEMI Blackburn with Darwen 315 1096 219 Blackpool 175 840 120 Central Lancashire 1105 1998 320 Cumbria 919 2372 444 East Lancashire 656 2150 458 North Lancashire 470 1432 269
2008/09
PCT Angina Chest Pain NSTEMI Blackburn with Darwen 290 985 179 Blackpool 199 863 113 Central Lancashire 910 1948 339 Cumbria 975 2822 522 East Lancashire 664 1958 317 North Lancashire 446 1572 268
Current Position In 2006 Making Moves - a national audit of interhospital arrangements for cardiac patients was published. This showed Lancashire and South Cumbria as the Cardiac Network with the longest median length of wait from admission to procedure for ACS patients in the country. Since then waits have been reduced significantly through a number of initiatives including:
53
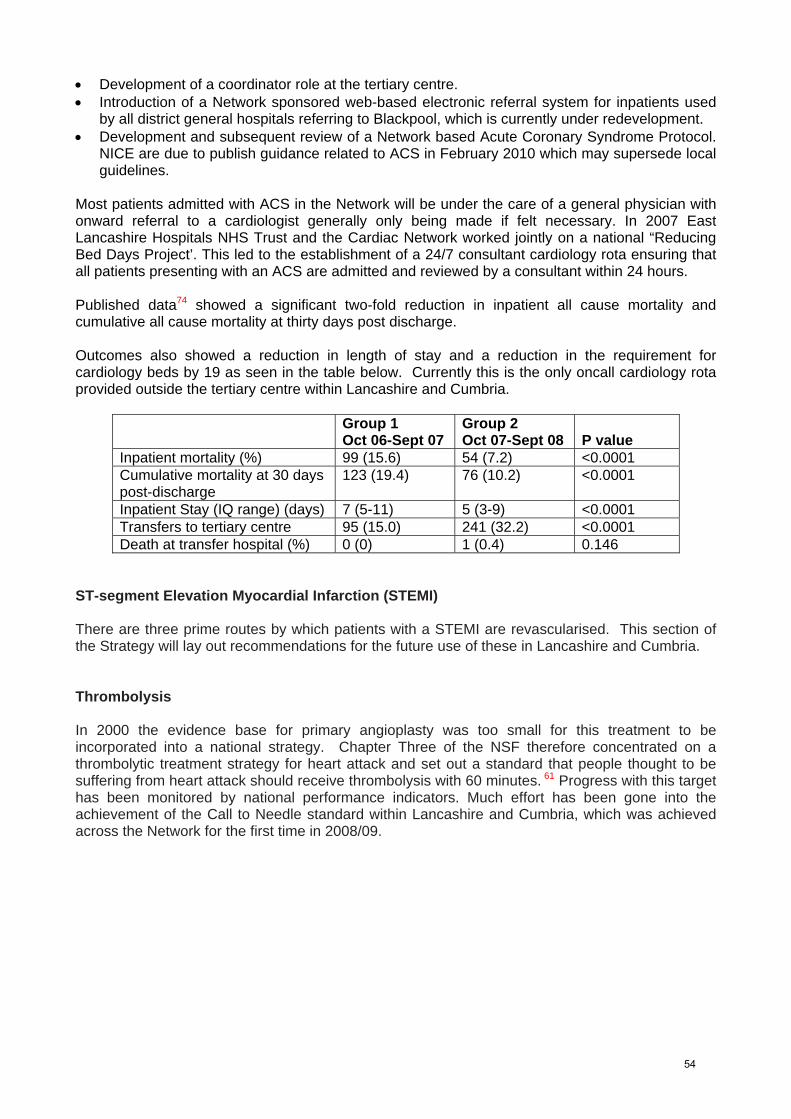
• Development of a coordinator role at the tertiary centre. • Introduction of a Network sponsored web-based electronic referral system for inpatients used
by all district general hospitals referring to Blackpool, which is currently under redevelopment. • Development and subsequent review of a Network based Acute Coronary Syndrome Protocol.
NICE are due to publish guidance related to ACS in February 2010 which may supersede local guidelines.
Most patients admitted with ACS in the Network will be under the care of a general physician with onward referral to a cardiologist generally only being made if felt necessary. In 2007 East Lancashire Hospitals NHS Trust and the Cardiac Network worked jointly on a national “Reducing Bed Days Project’. This led to the establishment of a 24/7 consultant cardiology rota ensuring that all patients presenting with an ACS are admitted and reviewed by a consultant within 24 hours. Published data74 showed a significant two-fold reduction in inpatient all cause mortality and cumulative all cause mortality at thirty days post discharge. Outcomes also showed a reduction in length of stay and a reduction in the requirement for cardiology beds by 19 as seen in the table below. Currently this is the only oncall cardiology rota provided outside the tertiary centre within Lancashire and Cumbria.
Group 1 Group 2
Oct 06-Sept 07 Oct 07-Sept 08 P value Inpatient mortality (%) 99 (15.6) 54 (7.2) <0.0001 Cumulative mortality at 30 days post-discharge
123 (19.4) 76 (10.2) <0.0001
Inpatient Stay (IQ range) (days) 7 (5-11) 5 (3-9) <0.0001 Transfers to tertiary centre 95 (15.0) 241 (32.2) <0.0001 Death at transfer hospital (%) 0 (0) 1 (0.4) 0.146
ST-segment Elevation Myocardial Infarction (STEMI) There are three prime routes by which patients with a STEMI are revascularised. This section of the Strategy will lay out recommendations for the future use of these in Lancashire and Cumbria. Thrombolysis In 2000 the evidence base for primary angioplasty was too small for this treatment to be incorporated into a national strategy. Chapter Three of the NSF therefore concentrated on a thrombolytic treatment strategy for heart attack and set out a standard that people thought to be suffering from heart attack should receive thrombolysis with 60 minutes. 61 Progress with this target has been monitored by national performance indicators. Much effort has been gone into the achievement of the Call to Needle standard within Lancashire and Cumbria, which was achieved across the Network for the first time in 2008/09.
54

The table below illustrates the Lancashire and Cumbria 2008/2009 performance against the national targets:
Percentage of Patients Receiving Thrombolysis within 60 Mins of Calling for Help
93%
75%80% 78%
57%51% 50%
0%10%20%30%40%50%60%70%80%90%
100%
Blackpool VictoriaHospital
Royal PrestonHospital
Chorley & SouthRibble District
General Hospital
Royal BlackburnHospital
Cumberland Infirmary West CumberlandHospital
University Hospitalsof Morecambe Bay
Hospital
% o
f Pat
ient
s
Percentage of Patients Receiving Thrombolysis within 30 Mins of Arriving at Hospital
92% 94%
79%89%
65%
90%
76%
0%10%20%30%40%50%60%70%80%90%
100%
Blackpool VictoriaHospital
Royal PrestonHospital
Chorley & SouthRibble District
General Hospital
Royal BlackburnHospital
Cumberland Infirmary West CumberlandHospital
University Hospitalsof Morecambe Bay
Hospital
% o
f Pat
ient
s
55

Percentage of Patients Arriving at Hospital within 30 Mins of Calling For Help
26%
16% 17%
29%
63%
91%
7%
0%10%20%30%40%50%
60%70%80%90%
100%
Blackpool VictoriaHospital
Royal PrestonHospital
Chorley & SouthRibble District
General Hospital
Royal BlackburnHospital
Cumberland Infirmary West CumberlandHospital
University Hospitalsof Morecambe Bay
Hospital
% o
f Pat
ient
s
Gap Analysis Performance against the Call to Door standard remains a significant challenge in Lancashire and Cumbria, particularly in the most remote areas of the Network. Work is ongoing with the North West Ambulance Service (NWAS) to reduce these times. With the rollout of primary angioplasty (PPCI) pre hospital thrombolysis is likely to remain a treatment strategy for a very small number of patients in the Network prior to immediate transfer to a PPCI centre. Nevertheless work to improve/maintain performance should continue until PPCI is in place across Lancashire and Cumbria.
Primary Angioplasty (PPCI) In 2008 the Department of Health guidance ‘Treatment of Heart Attack’75 reported the outcomes of the National Infarct Angioplasty Project (NIAP) were reported. Analysis of the evidence showed that: • PPCI reduces mortality and improves longer-term outcome compared with Thrombolysis when
delivered within a similar timeframe. • In-hospital mortality for patients undergoing PPCI was 5.2% and 7.1% for those given
Thrombolysis. At 18 months mortality rates were 9.9% for patients who had received PPCI and 14.8% for those who had been thrombolysed.
• Patients who were admitted directly to the catheter laboratory bypassing accident and emergency departments had the lowest mortality.
• More patients are potentially suitable for PPCI than Thrombolysis and PPCI is associated with fewer strokes and recurrent heart attacks during the hospital admission.
• The greatest delay in providing effective treatment is often the time taken for patients to recognise that they have a problem and call for help.
The report also found and concluded that • PPCI is more expensive to deliver than thrombolysis but is both clinically and cost-effective
when delivered within 120 minutes of patient call for help, this timeframe has subsequently been raised to 150 minutes.
• National rollout of PPCI is feasible over the next three years but may be logistically challenging in some parts of the country.
Since April 2009, PPCI has been carried out at Lancashire Cardiac Centre (LCC), Blackpool 24/7 for local residents only. To date 112 patients (excluding rescue PCI following thrombolysis) have received PPCI, achieving an average call to balloon time of 103 minutes.
56

Due to the complexity of system change required to plan for PPCI, working through the Network, the PCTs commissioned Capgemini Consultancy to assess the logistical requirements of roll-out to the rest of Lancashire and Cumbria. This work has assessed: • The expected patient volumes and ambulance operating hours, including:
° Additional capacity and vehicle requirements for North West Ambulance Service (NWAS), and changes to volumes and capacity requirements within all tertiary centres and the district general hospitals.
° Financial implications of the above. A Task Advisory Group was established and, in line with NIAP’s recommendation that PPCI is more appropriately provided in specialist centres, they agreed that modelling should be undertaken on the basis of patient flows to Blackpool, Middlesbrough and Newcastle. Analysis of the Isochrones and other data provided by NWAS has demonstrated that the majority of the Network population would be able to access PPCI within the timeframes shown to provide the best outcomes. Approximately 30 patients per annum in West Cumbria would require the “Drip and Ship” approach which involves administration of thrombolytics and immediate transfer to a PPCI centre. “Drip and Ship” has been shown to have better outcomes for patients than the traditional pathway of Thrombolysis followed by rescue PCI for those patients who do not reperfuse. The process for modelling the impact of PPCI recommended within Lancashire and Cumbria is a four stage approach: • Conceptual Modelling – developed the logic to be used, mapped historical patient flows and
defined the scenarios considered. Five scenarios, which had been developed by the Revascularisation Task Advisory Group, were evaluated.
• Volumetric Modelling – analyses the patient flow volumes for patients who have had heart attacks through the system.
• Simulation Modelling – models the flows of patients through A&Es, trust sites and tertiary centres under each scenario
• Output Modelling – collates the simulation model outputs including the projections for future bed and transport capacity.
The scenarios used during the modelling were: 1) Treat & Transfer– Blackpool, Middlesbrough and Newcastle 2) Treat & Discharge back to DGHs from Blackpool, Middlesbrough and Newcastle 3) Development of a PPCI centre in Carlisle 4) Exclusion of patients over 80 5) Exclusion of Drip and Ship Once the scenarios were developed the model to analyse the patient flow volumes for each was constructed using actual patient activity collected through MINAP and NWAS data. The logic applied was then verified with clinicians currently responsible for the care of these patients. An example of one scenario within the volumetric modelling is shown below to demonstrate the complexity and rigour used during this process.
57
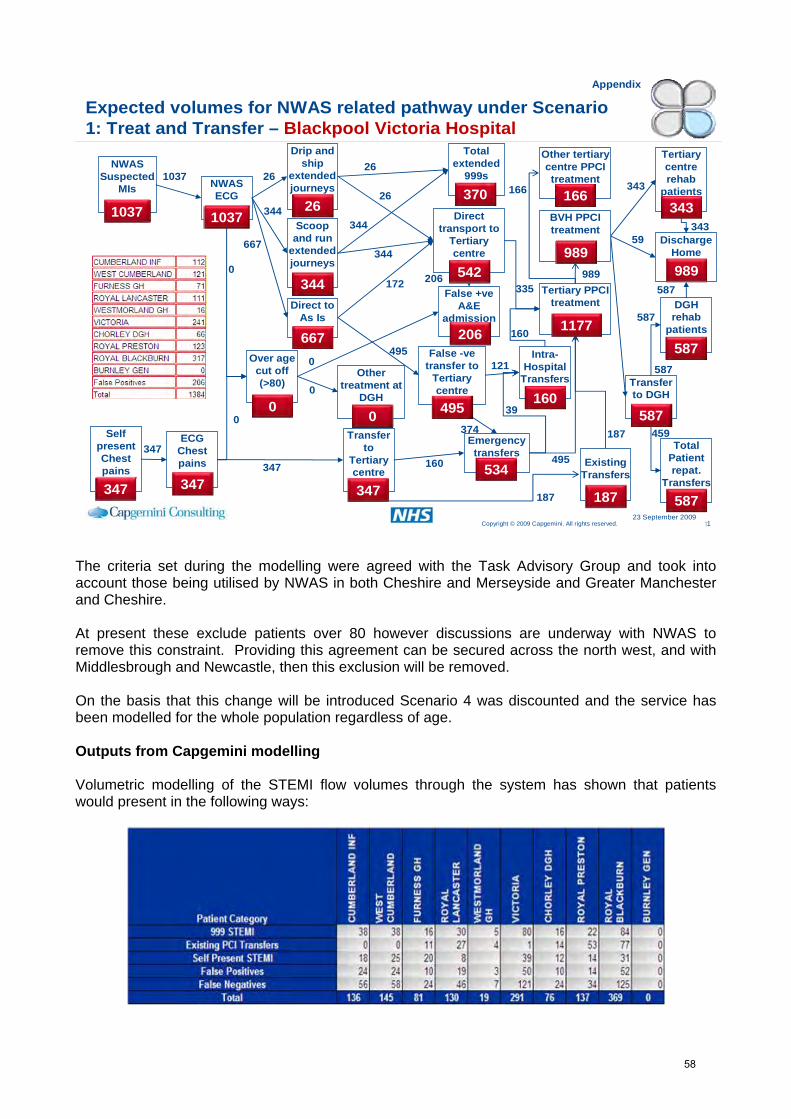
11Copyright © 2009 Capgemini. All rights reserved.23 September 2009
Expected volumes for NWAS related pathway under Scenario 1: Treat and Transfer –
Appendix
Blackpool Victoria HospitalDrip and
ship extended journeys
Total extended
999sNWAS
Suspected MIs
Self present Chest pains
NWAS ECG
ECG Chest pains
Direct to As Is
False -ve transfer to
Tertiary centre
Scoop and run
extended journeys
Transfer to
Tertiary centre
Tertiary PPCI treatment DGH
rehab patients
Transfer to DGH
Discharge Home
Other treatment at
DGH
Emergency transfers
Total Patient repat.
Transfers
Direct transport to
Tertiary centre
False +ve A&E
admission
Tertiary centre rehab
patients
Over age cut off (>80)
1037
347
0
0
26
344
667
344
26
347
347495
534
26
344
206
344
26343
343
0
0
206
495
495
172
59
587
587
1037
Other tertiary centre PPCI treatment
Existing Transfers
187187
187
335
Intra-Hospital
Transfers
39
587
587
459
160
374
166BVH PPCI treatment
989
160
166
989
370343
1037
989542
1177667
587
160
121
00
347 347587
The criteria set during the modelling were agreed with the Task Advisory Group and took into account those being utilised by NWAS in both Cheshire and Merseyside and Greater Manchester and Cheshire. At present these exclude patients over 80 however discussions are underway with NWAS to remove this constraint. Providing this agreement can be secured across the north west, and with Middlesbrough and Newcastle, then this exclusion will be removed. On the basis that this change will be introduced Scenario 4 was discounted and the service has been modelled for the whole population regardless of age. Outputs from Capgemini modelling Volumetric modelling of the STEMI flow volumes through the system has shown that patients would present in the following ways:
58

These patients are attributable to PCTs as follows:
Existing PCI False Self Present STEMI volumes 999 STEMI Transfers Negatives STEMI Total BLACKBURN
WITH DARWEN 37 42 57 15 151PCT
BLACKPOOL 39 1 56 22 118PCT
CENTRAL LANCASHIRE
63 50 92 30 234PCT CUMBRIA
75 18 115 69 277TEACHING PCTEAST
LANCASHIRE 60 39 93 16 207TEACHING PCT
NORTH LANCASHIRE
56 26 88 25 195TEACHING PCT Patients whose ECG proves to be a ‘false positive’, whilst requiring transport to the tertiary centres, will not undergo PPCI and are therefore not counted in the numbers of patients expected to receive treatment, although they have been factored into the transport requirements. The costings for PPCI are complex as they consist not only of the tariff for treatment but also transport costs, which are higher than a traditional MI service model due to the fact that patients will be being taken past their closest hospital and straight to a tertiary centre. The costings for vehicle capacity for both the Treat and Transfer and Treat and Discharge models have been calculated and are as follows: Scenario Ambulance
Capital Cost (£) Ambulance Operational Cost (Recurrent) (£)
Patient Transfer Service Recurrent (£)
Patient Transfer Service for Discharge Recurrent (£)
Treat and Transfer
260K 546 (operating hours) 114K 0K
Treat and Discharge
260K 546 (operating hours) 0K 34K
The requirement for the operational costs has been calculated on the prediction of the number of additional shifts that need to be staffed to maintain evidenced based clinically effective PPCI call to balloon times. In terms of vehicles two will need to be commissioned but the PPCI service will only require 70% of this additional capacity. The operational cost of the remaining 30% has not been factored into the cost of the PPCI service and the funding and use of this capacity will need to be subject to discussions between NWAS and commissioners. Bed Capacity Requirements Within Lancashire and Cumbria the majority of the population will access PPCI in Blackpool. As part of the modelling the numbers of additional Coronary Care Unit (CCU) beds has been calculated as this is a major factor in understanding the viability of the potential models.
59
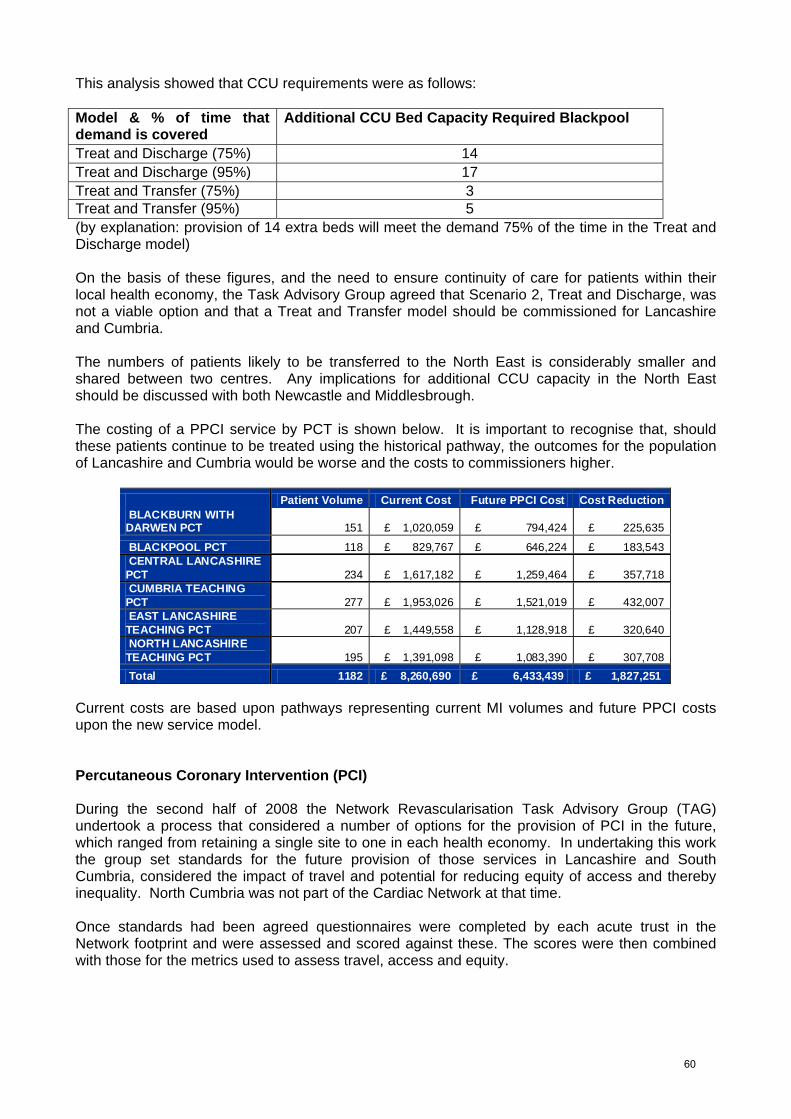
This analysis showed that CCU requirements were as follows: Model & % of time that demand is covered
Additional CCU Bed Capacity Required Blackpool
Treat and Discharge (75%) 14 Treat and Discharge (95%) 17 Treat and Transfer (75%) 3 Treat and Transfer (95%) 5 (by explanation: provision of 14 extra beds will meet the demand 75% of the time in the Treat and Discharge model) On the basis of these figures, and the need to ensure continuity of care for patients within their local health economy, the Task Advisory Group agreed that Scenario 2, Treat and Discharge, was not a viable option and that a Treat and Transfer model should be commissioned for Lancashire and Cumbria. The numbers of patients likely to be transferred to the North East is considerably smaller and shared between two centres. Any implications for additional CCU capacity in the North East should be discussed with both Newcastle and Middlesbrough. The costing of a PPCI service by PCT is shown below. It is important to recognise that, should these patients continue to be treated using the historical pathway, the outcomes for the population of Lancashire and Cumbria would be worse and the costs to commissioners higher.
Patient Volume Current Cost Future PPCI Cost Cost Reduction BLACKBURN WITH DARWEN PCT 151 £ 1,020,059 £ 794,424 £ 225,635
BLACKPOOL PCT 118 £ 829,767 £ 646,224 £ 183,543 CENTRAL LANCASHIRE PCT 234 £ 1,617,182 £ 1,259,464 £ 357,718 CUMBRIA TEACHING PCT 277 £ 1,953,026 £ 1,521,019 £ 432,007 EAST LANCASHIRE TEACHING PCT 207 £ 1,449,558 £ 1,128,918 £ 320,640 NORTH LANCASHIRE TEACHING PCT 195 £ 1,391,098 £ 1,083,390 £ 307,708 Total 1182 £ 8,260,690 £ 6,433,439 £ 1,827,251
Current costs are based upon pathways representing current MI volumes and future PPCI costs upon the new service model. Percutaneous Coronary Intervention (PCI) During the second half of 2008 the Network Revascularisation Task Advisory Group (TAG) undertook a process that considered a number of options for the provision of PCI in the future, which ranged from retaining a single site to one in each health economy. In undertaking this work the group set standards for the future provision of those services in Lancashire and South Cumbria, considered the impact of travel and potential for reducing equity of access and thereby inequality. North Cumbria was not part of the Cardiac Network at that time. Once standards had been agreed questionnaires were completed by each acute trust in the Network footprint and were assessed and scored against these. The scores were then combined with those for the metrics used to assess travel, access and equity.
60
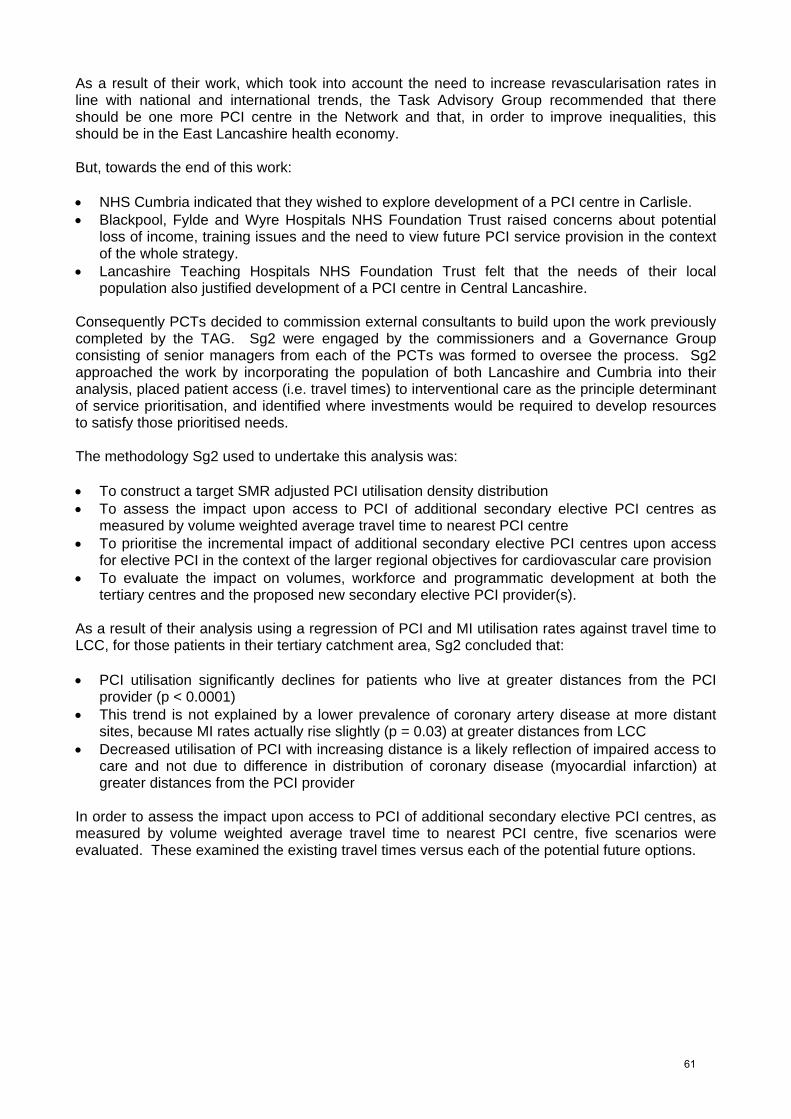
As a result of their work, which took into account the need to increase revascularisation rates in line with national and international trends, the Task Advisory Group recommended that there should be one more PCI centre in the Network and that, in order to improve inequalities, this should be in the East Lancashire health economy. But, towards the end of this work: • NHS Cumbria indicated that they wished to explore development of a PCI centre in Carlisle. • Blackpool, Fylde and Wyre Hospitals NHS Foundation Trust raised concerns about potential
loss of income, training issues and the need to view future PCI service provision in the context of the whole strategy.
• Lancashire Teaching Hospitals NHS Foundation Trust felt that the needs of their local population also justified development of a PCI centre in Central Lancashire.
Consequently PCTs decided to commission external consultants to build upon the work previously completed by the TAG. Sg2 were engaged by the commissioners and a Governance Group consisting of senior managers from each of the PCTs was formed to oversee the process. Sg2 approached the work by incorporating the population of both Lancashire and Cumbria into their analysis, placed patient access (i.e. travel times) to interventional care as the principle determinant of service prioritisation, and identified where investments would be required to develop resources to satisfy those prioritised needs. The methodology Sg2 used to undertake this analysis was: • To construct a target SMR adjusted PCI utilisation density distribution • To assess the impact upon access to PCI of additional secondary elective PCI centres as
measured by volume weighted average travel time to nearest PCI centre • To prioritise the incremental impact of additional secondary elective PCI centres upon access
for elective PCI in the context of the larger regional objectives for cardiovascular care provision • To evaluate the impact on volumes, workforce and programmatic development at both the
tertiary centres and the proposed new secondary elective PCI provider(s). As a result of their analysis using a regression of PCI and MI utilisation rates against travel time to LCC, for those patients in their tertiary catchment area, Sg2 concluded that: • PCI utilisation significantly declines for patients who live at greater distances from the PCI
provider (p < 0.0001) • This trend is not explained by a lower prevalence of coronary artery disease at more distant
sites, because MI rates actually rise slightly (p = 0.03) at greater distances from LCC • Decreased utilisation of PCI with increasing distance is a likely reflection of impaired access to
care and not due to difference in distribution of coronary disease (myocardial infarction) at greater distances from the PCI provider
In order to assess the impact upon access to PCI of additional secondary elective PCI centres, as measured by volume weighted average travel time to nearest PCI centre, five scenarios were evaluated. These examined the existing travel times versus each of the potential future options.
61
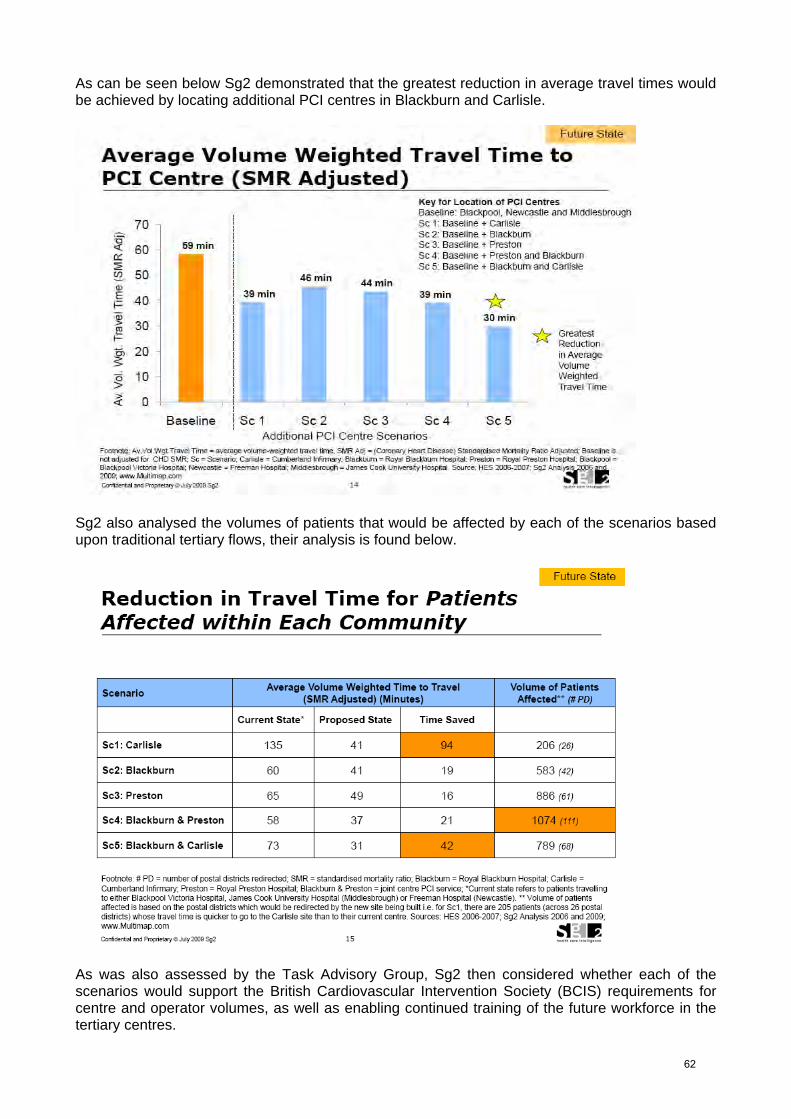
As can be seen below Sg2 demonstrated that the greatest reduction in average travel times would be achieved by locating additional PCI centres in Blackburn and Carlisle.
Sg2 also analysed the volumes of patients that would be affected by each of the scenarios based upon traditional tertiary flows, their analysis is found below.
As was also assessed by the Task Advisory Group, Sg2 then considered whether each of the scenarios would support the British Cardiovascular Intervention Society (BCIS) requirements for centre and operator volumes, as well as enabling continued training of the future workforce in the tertiary centres.
62

Sg2 utilised the 2005 BCIS and British Cardiac Society (BCS) recommended standards for good practice and training for percutaneous coronary intervention, which outline a minimum of 200 cases per annum per centre76 (BCIS does however advocate all centres should be encouraged to aim for a minimum of 400 cases per year and it is anticipated that this will shortly become their recommendation). The Network’s Task Advisory Group had previously agreed a requirement for a minimum of 400 cases per annum in line with the emerging evidence that outcomes for patients improve in higher volume centres. On the basis of their analysis however Sg2 suggested that all centres would be likely to meet BCIS required volumes (200 cases), although they cautioned that Carlisle is at risk of not being able to do so. Sg2 also specifically calculated the numbers of patients they anticipate would be accessing PCI at LCC in the future, both electively and non-electively suggesting that both numbers for operator volume and training requirements would meet BCIS requirements. On the basis of this work Sg2 made the following recommendations for the healthcare economy of Lancashire and Cumbria. • Optimal access to elective PCI and maximal savings in travel times for redirected patients
favour: ° Carlisle as the highest priority for developing a single new elective PCI site ° If two sites are developed, independent sites at Carlisle and Blackburn would be the
highest priority followed by a combined Blackburn and Preston site
• Conservative (SMR adjusted) volume estimates predict adequate numbers to meet minimal standards of institutional and operator PCI competency consistent with BCIS and ACC guidelines73,76
• Carlisle strategy least impacts PCI volumes (and turnover) at LCC. All strategies meet minimal
volume standards for BVH interventional training • Execution of Carlisle strategy requires investment in a new interventional catheter laboratory,
recruitment of three interventional cardiologists, development of transfer agreements with Newcastle cardiac surgery and training of infrastructure personnel
• Execution of Blackburn/Preston strategy requires investment in a new interventional catheter
laboratory at Preston. Whilst the remit for Sg2’s work varied in that it incorporated the whole population of Cumbria it is reassuring that, in relation to the original Network footprint of Lancashire and South Cumbria, and even though a different methodology was applied, the suggested recommendation to prioritise development of a catheter laboratory in East Lancashire prior to any other has been confirmed. Elective PCI constitutes only part of interventional revascularisation and with the anticipated national development of PPCI future catheter laboratory calculations of catheter laboratory PCI volumes need to be calculated on the basis that non elective PCI numbers will rise and that unless revascularisation rates in Lancashire and Cumbria are increased in line with both national and international trends the number of patients undergoing elective PCI will reduce in the future. The following table identifies by PCT the numbers of patients who would be expected to undergo revascularisation through interventional cardiology at rates of 1,500, 1,900 and 2,250 pmp.
63
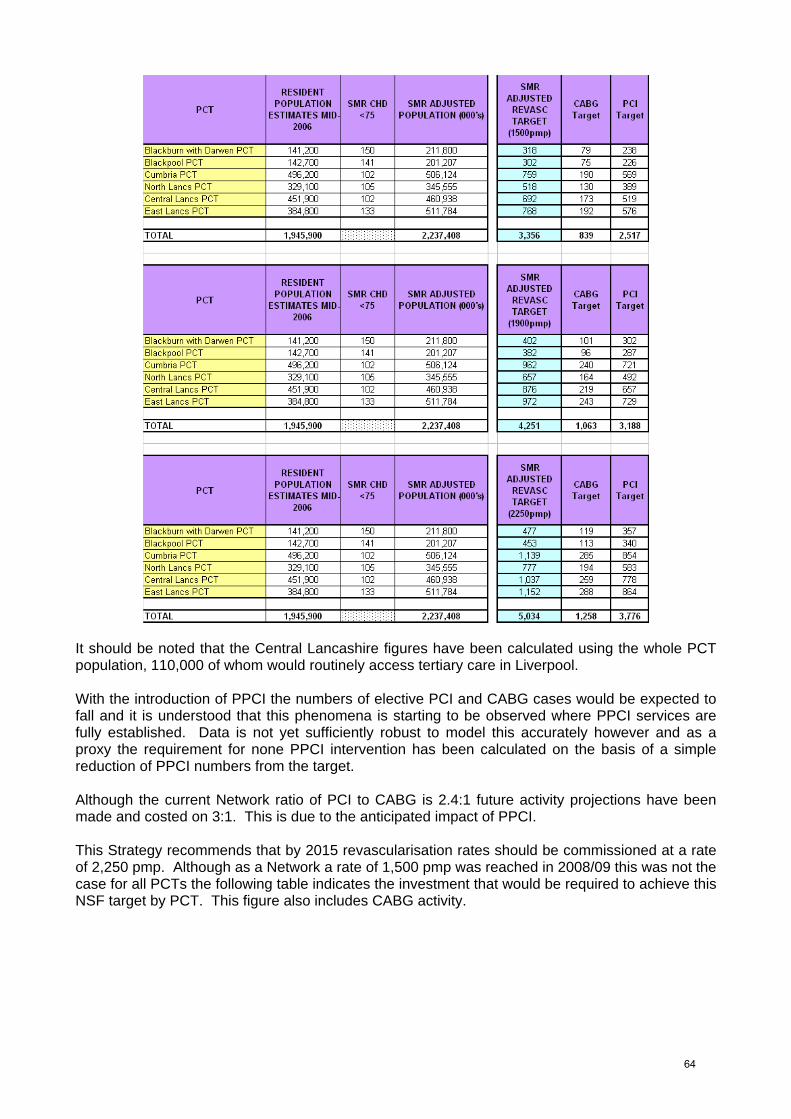
It should be noted that the Central Lancashire figures have been calculated using the whole PCT population, 110,000 of whom would routinely access tertiary care in Liverpool. With the introduction of PPCI the numbers of elective PCI and CABG cases would be expected to fall and it is understood that this phenomena is starting to be observed where PPCI services are fully established. Data is not yet sufficiently robust to model this accurately however and as a proxy the requirement for none PPCI intervention has been calculated on the basis of a simple reduction of PPCI numbers from the target. Although the current Network ratio of PCI to CABG is 2.4:1 future activity projections have been made and costed on 3:1. This is due to the anticipated impact of PPCI. This Strategy recommends that by 2015 revascularisation rates should be commissioned at a rate of 2,250 pmp. Although as a Network a rate of 1,500 pmp was reached in 2008/09 this was not the case for all PCTs the following table indicates the investment that would be required to achieve this NSF target by PCT. This figure also includes CABG activity.
64

Once a revascularisation rate of 1,500 pmp has been achieved the numbers of PCI (other than PPCI) needed to be commissioned can be calculated and the table below indicates the capacity required by PCT.
65
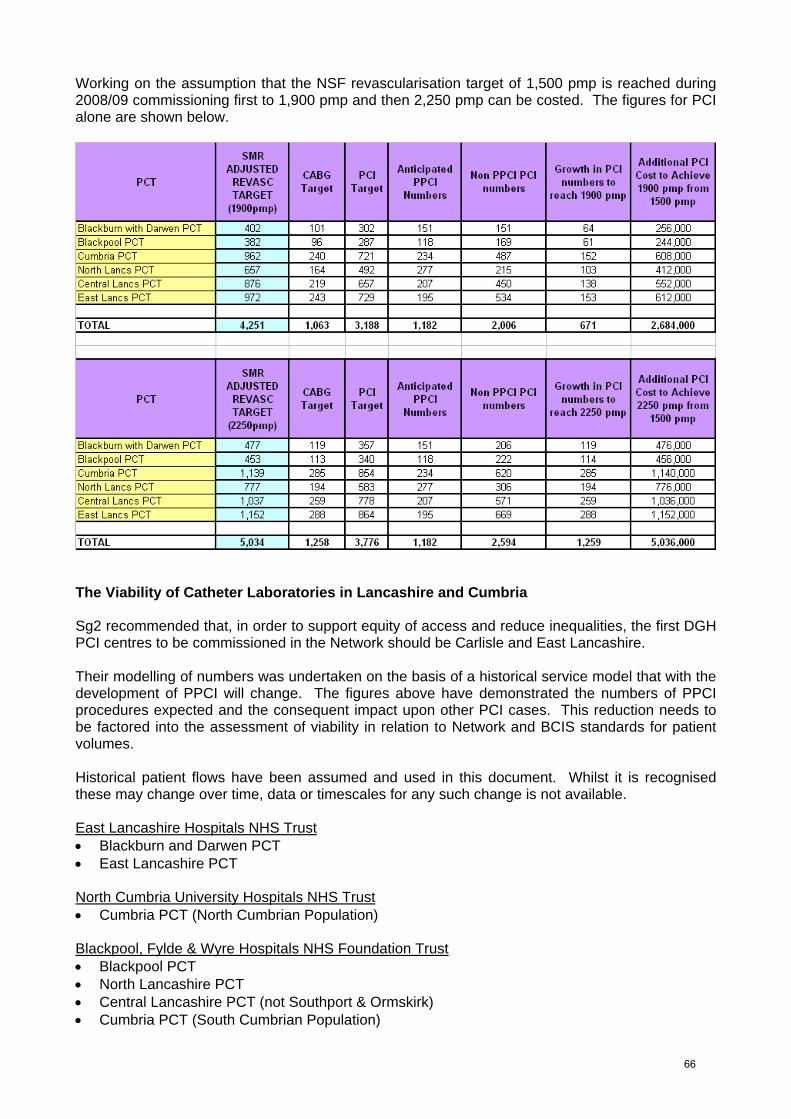
Working on the assumption that the NSF revascularisation target of 1,500 pmp is reached during 2008/09 commissioning first to 1,900 pmp and then 2,250 pmp can be costed. The figures for PCI alone are shown below.
The Viability of Catheter Laboratories in Lancashire and Cumbria Sg2 recommended that, in order to support equity of access and reduce inequalities, the first DGH PCI centres to be commissioned in the Network should be Carlisle and East Lancashire. Their modelling of numbers was undertaken on the basis of a historical service model that with the development of PPCI will change. The figures above have demonstrated the numbers of PPCI procedures expected and the consequent impact upon other PCI cases. This reduction needs to be factored into the assessment of viability in relation to Network and BCIS standards for patient volumes. Historical patient flows have been assumed and used in this document. Whilst it is recognised these may change over time, data or timescales for any such change is not available. East Lancashire Hospitals NHS Trust • Blackburn and Darwen PCT • East Lancashire PCT North Cumbria University Hospitals NHS Trust • Cumbria PCT (North Cumbrian Population)
Blackpool, Fylde & Wyre Hospitals NHS Foundation Trust • Blackpool PCT • North Lancashire PCT • Central Lancashire PCT (not Southport & Ormskirk) • Cumbria PCT (South Cumbrian Population)
66

This approach equates to the following numbers of cases per annum dependent upon commissioned revascularisation rates.
DGH Lab Revascularisation NSTEMI and Proposed PCI Centre Rate pmp elective
activity
East Lancashire 1500 468 1900 685 2250 875 Carlisle 1500 218 1900 317 2250 403
These figures show that, following the introduction of PPCI, an East Lancaster catheter laboratory would be on the cusp of achieving the Network standards of 400 cases per annum, which have been shown to demonstrate improved patient outcomes. It is recommended therefore that the revascularisation rates commissioned for the population of East Lancashire should be extended to 1,900 pmp at the earliest opportunity. The position in Carlisle is different. Sg2 recommend the commissioning of a PCI service here as they were able to demonstrate a direct correlation between revascularisation rates and travel times. Their assessment of viability was based upon the BCIS minimum recommendations (200 cases per annum) which have now widely lost support due to the emerging evidence about outcomes. NHS Cumbria has clearly voiced its desire to commission a PCI service in Carlisle and has been in discussion with its stakeholders about this for some time. As commissioners, should they wish to pursue this option, achievement of the standards agreed by the Task Advisory Group would require urgent development of a PCI pathway to increase revascularisation to 2,250 pmp, with the potential to offer this service to populations from outside Cumbria being a route to explore. Lancashire Teaching Hospitals NHS Foundation Trust has previously indicated its desire to become a PCI centre and Sg2 suggested that this should be considered in the future. Modelling suggests that, with the development of capacity in East Lancashire and maintenance of existing revascularisation rates, a further centre is not yet required. As commissioning intentions for revascularisation are clarified it is recommended that the need for further PCI capacity is re-evaluated across Lancashire and Cumbria by 2012.
67
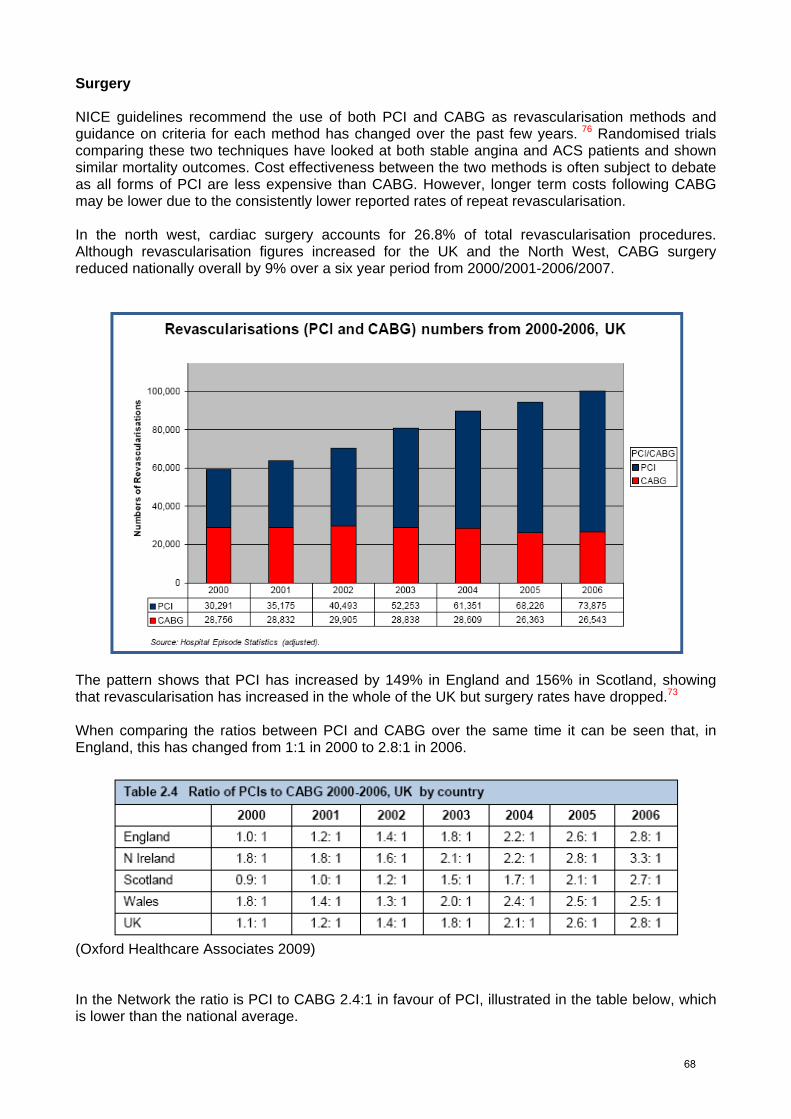
Surgery NICE guidelines recommend the use of both PCI and CABG as revascularisation methods and guidance on criteria for each method has changed over the past few years. 76 Randomised trials comparing these two techniques have looked at both stable angina and ACS patients and shown similar mortality outcomes. Cost effectiveness between the two methods is often subject to debate as all forms of PCI are less expensive than CABG. However, longer term costs following CABG may be lower due to the consistently lower reported rates of repeat revascularisation. In the north west, cardiac surgery accounts for 26.8% of total revascularisation procedures. Although revascularisation figures increased for the UK and the North West, CABG surgery reduced nationally overall by 9% over a six year period from 2000/2001-2006/2007.
The pattern shows that PCI has increased by 149% in England and 156% in Scotland, showing that revascularisation has increased in the whole of the UK but surgery rates have dropped.73 When comparing the ratios between PCI and CABG over the same time it can be seen that, in England, this has changed from 1:1 in 2000 to 2.8:1 in 2006.
(Oxford Healthcare Associates 2009) In the Network the ratio is PCI to CABG 2.4:1 in favour of PCI, illustrated in the table below, which is lower than the national average.
68
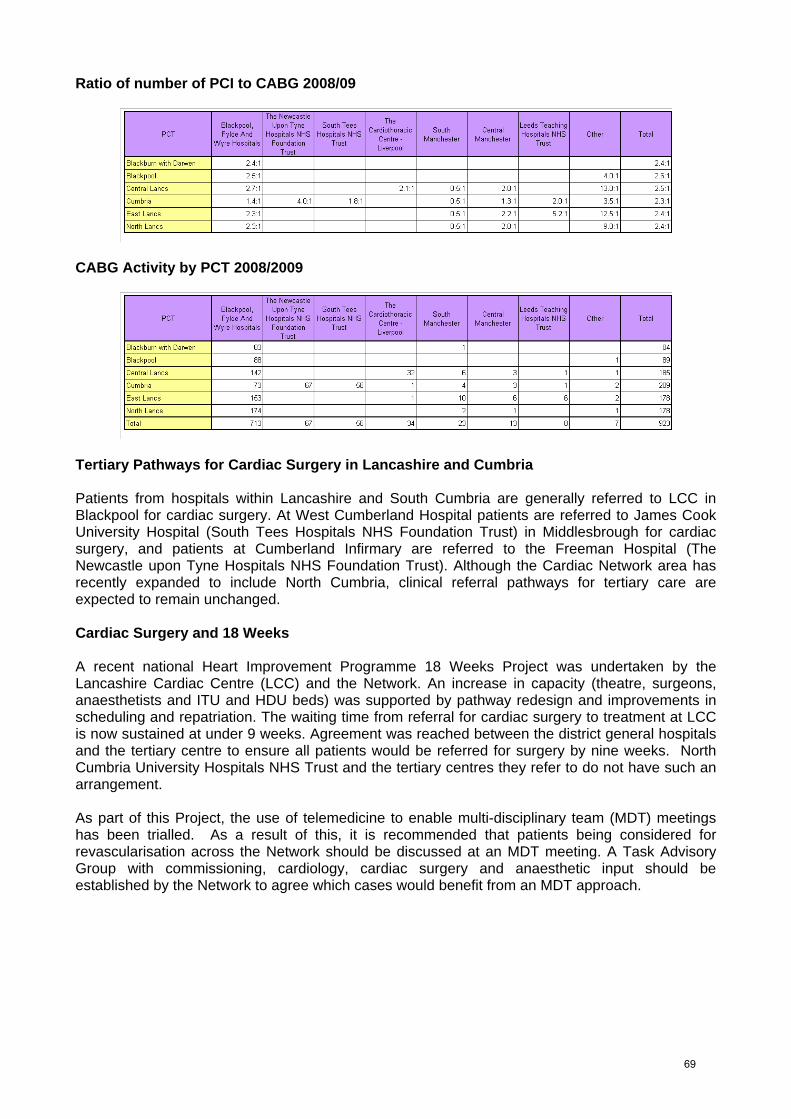
Ratio of number of PCI to CABG 2008/09
CABG Activity by PCT 2008/2009
Tertiary Pathways for Cardiac Surgery in Lancashire and Cumbria Patients from hospitals within Lancashire and South Cumbria are generally referred to LCC in Blackpool for cardiac surgery. At West Cumberland Hospital patients are referred to James Cook University Hospital (South Tees Hospitals NHS Foundation Trust) in Middlesbrough for cardiac surgery, and patients at Cumberland Infirmary are referred to the Freeman Hospital (The Newcastle upon Tyne Hospitals NHS Foundation Trust). Although the Cardiac Network area has recently expanded to include North Cumbria, clinical referral pathways for tertiary care are expected to remain unchanged. Cardiac Surgery and 18 Weeks A recent national Heart Improvement Programme 18 Weeks Project was undertaken by the Lancashire Cardiac Centre (LCC) and the Network. An increase in capacity (theatre, surgeons, anaesthetists and ITU and HDU beds) was supported by pathway redesign and improvements in scheduling and repatriation. The waiting time from referral for cardiac surgery to treatment at LCC is now sustained at under 9 weeks. Agreement was reached between the district general hospitals and the tertiary centre to ensure all patients would be referred for surgery by nine weeks. North Cumbria University Hospitals NHS Trust and the tertiary centres they refer to do not have such an arrangement. As part of this Project, the use of telemedicine to enable multi-disciplinary team (MDT) meetings has been trialled. As a result of this, it is recommended that patients being considered for revascularisation across the Network should be discussed at an MDT meeting. A Task Advisory Group with commissioning, cardiology, cardiac surgery and anaesthetic input should be established by the Network to agree which cases would benefit from an MDT approach.
69
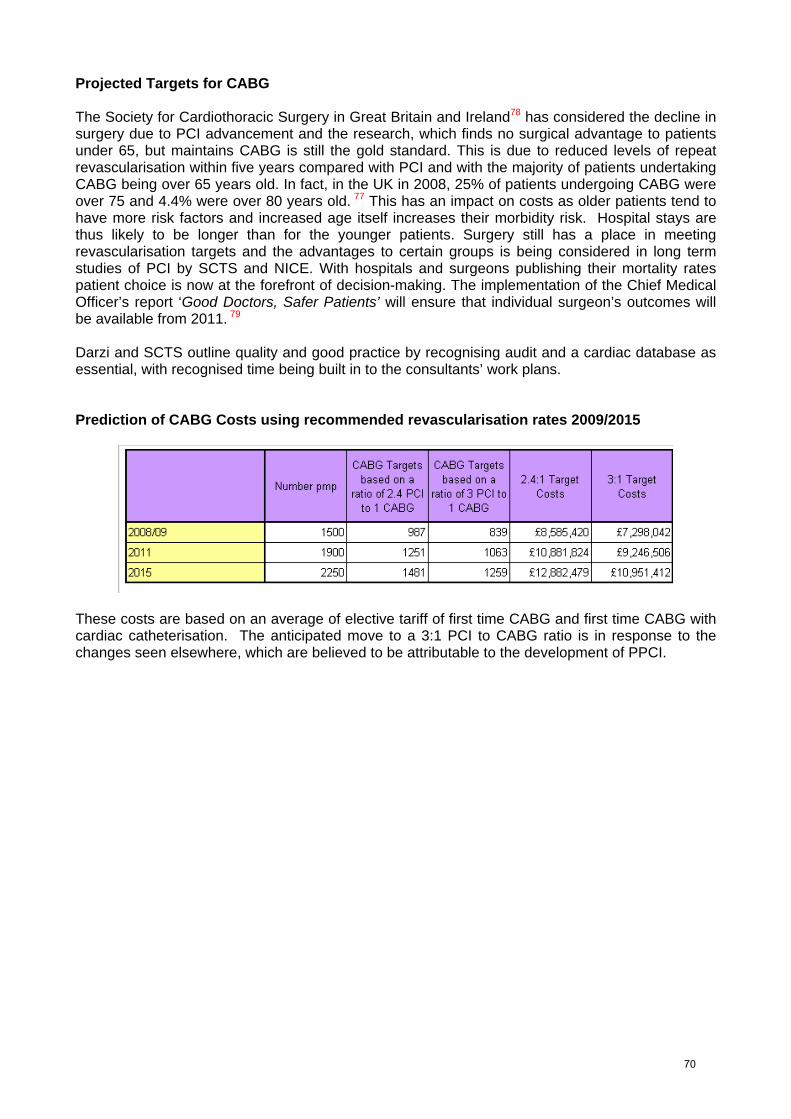
Projected Targets for CABG The Society for Cardiothoracic Surgery in Great Britain and Ireland78 has considered the decline in surgery due to PCI advancement and the research, which finds no surgical advantage to patients under 65, but maintains CABG is still the gold standard. This is due to reduced levels of repeat revascularisation within five years compared with PCI and with the majority of patients undertaking CABG being over 65 years old. In fact, in the UK in 2008, 25% of patients undergoing CABG were over 75 and 4.4% were over 80 years old. 77 This has an impact on costs as older patients tend to have more risk factors and increased age itself increases their morbidity risk. Hospital stays are thus likely to be longer than for the younger patients. Surgery still has a place in meeting revascularisation targets and the advantages to certain groups is being considered in long term studies of PCI by SCTS and NICE. With hospitals and surgeons publishing their mortality rates patient choice is now at the forefront of decision-making. The implementation of the Chief Medical Officer’s report ‘Good Doctors, Safer Patients’ will ensure that individual surgeon’s outcomes will be available from 2011. 79 Darzi and SCTS outline quality and good practice by recognising audit and a cardiac database as essential, with recognised time being built in to the consultants’ work plans. Prediction of CABG Costs using recommended revascularisation rates 2009/2015
These costs are based on an average of elective tariff of first time CABG and first time CABG with cardiac catheterisation. The anticipated move to a 3:1 PCI to CABG ratio is in response to the changes seen elsewhere, which are believed to be attributable to the development of PPCI.
70

Valve Surgery Nationally valve surgery is on the increase. Projections for the years 2010, 2015 and 2020 are applied with a growth of 5% per year for the overall rate pmp from 2006-2020. This is in line with the average UK growth of 6% per year. In the north west, valve surgery exceeded expectations by 7%.78
Aortic valve surgery is more likely to be performed on elderly, high risk patients (SCTS 2008), comprising of 62% of the workload, with mitral valve surgery taking 29% and tricuspid 9%. Mitral valve surgery has increased twofold between 2001-2008 (SCTS 2008) Many of these patients will now receive mitral valve repair rather than replacement. 77 Future Predictions of Case Mix (Oxford Healthcare Associates 2009)
0
100
200
300
400
500
600
Aortic Mitral Tricuspid Root Total
Valve Data
ReplacementRepair OthersTotal
71

The valve activity can also be split by PCT. The Network’s tertiary centres also take referrals from outside the area and patients who are away from home when they require surgery. All Valve Surgery 2008/09
Valve Costs by PCT in 2008/09
These figures have been based on an average cost of HRG tariff for cardiac valve procedures and valves and catheterisation. With recommendations of valve growth nationally of 5% over the next six years78 the figures below show the predicted cost by PCT and the total cost for the Network of this increase. With new developments in valve techniques and changing practices, valve surgery has increased. Dual procedures are more common within the Network (approx 38%), and the costs of these are decided by the leading procedure.
Valve cost prediction (based on predicted 5% growth per annum)
72
Minimal Access and Port Access LCC and the Freeman Hospital in Newcastle have introduced minimally invasive and port access mitral and tricuspid valve surgery. Around 100 of these cases were performed last year at LCC. Although current costs of these procedures are approximately £8,000 greater per case than conventional valve surgery, as valve activity is predicted to increase, PCTs are advised to explore minimally invasive and port access techniques as these will reduce hospital costs through: • shorter lengths of stay • reduced infection rates • reduced re-admission rates. The impact of this approach has the potential to reduce the need to increase both theatre and bed capacity, which would be required to treat an ageing population, whose recovery from surgery tends to be longer. Trans-catheter Aortic Valve Implant (TAVI) TAVI is a hybrid procedure usually performed in the catheter laboratory. This procedure is offered to a defined criteria of patients who are at a very high risk for conventional aortic valve replacement surgery. Risk factors include age, co-morbidities and anaesthetic considerations. The procedure is carried out under general anaesthetic and involves a catheter being inserted into the groin. The tissue valve is then inserted through the catheter into the site of the faulty narrowed aortic valve.81
NICE offer guidance on this technique and have set stringent standards: • Clinical governance leads at any centre must be informed. • Patients should have strict informed consent about the uncertainty of the procedure’s long-term
efficacy and its risks. • Patient selection should only be carried out through an MDT process, including interventional
cardiologist, cardiac surgeon and cardiac anaesthetist. • Clinicians carrying out this procedure require specialist training and experience in interventional
cardiology. • Units undertaking this procedure need both vascular and cardiac surgical support. By fulfilling the criteria, the development of this technique, which Blackpool, Fylde and Wyre Hospitals NHS Foundation Trust is currently supporting, appears to have demonstrated improved quality of life for the small number of patients who have undergone this procedure to date. This procedure will be examined nationally for its benefits, costs and governance issues. The cost for TAVI is in the region of £20,000 per case. Should it become a recommended procedure, as a specialised service it would be commissioned on a north west footprint. It is recommended that local commissioners should support a centre within Lancashire and Cumbria to reduce the inequalities of access likely to be found if a service is developed elsewhere in the north west. Developing a hybrid theatre for collaboration between cardiology and cardiac surgery offers potential for improving patient care for these and other technically complex procedures, e.g. arrhythmia ablation.
73
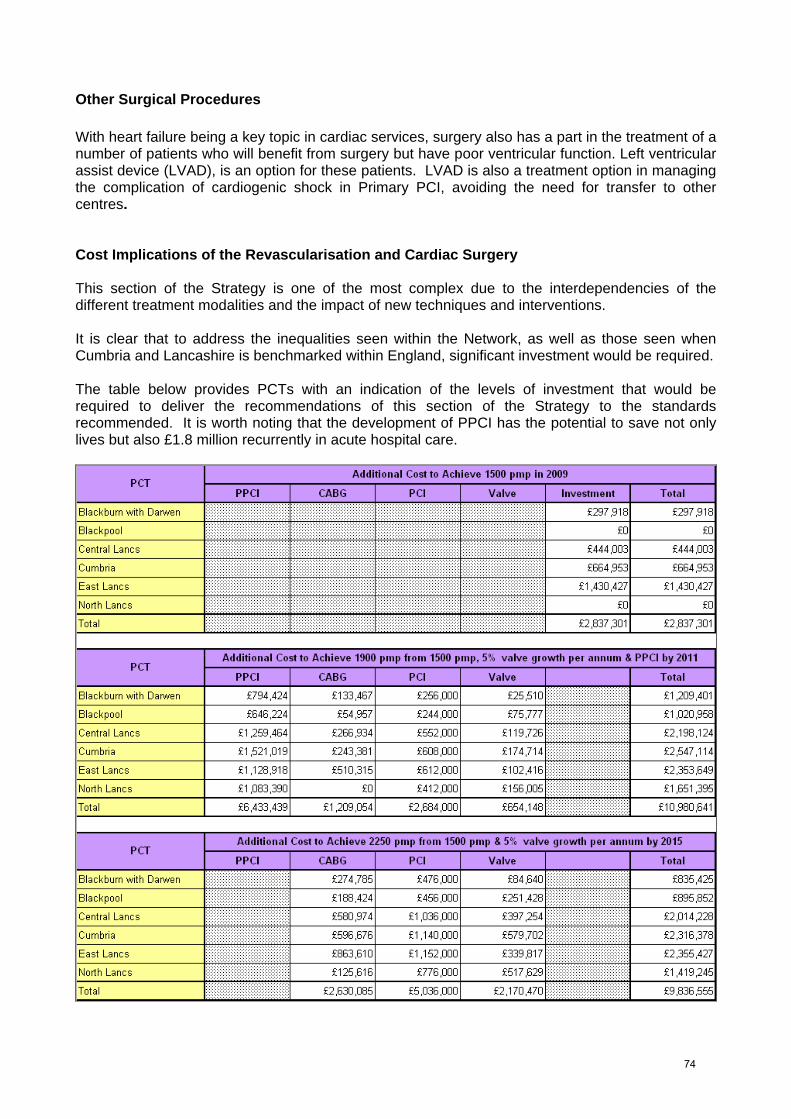
Other Surgical Procedures With heart failure being a key topic in cardiac services, surgery also has a part in the treatment of a number of patients who will benefit from surgery but have poor ventricular function. Left ventricular assist device (LVAD), is an option for these patients. LVAD is also a treatment option in managing the complication of cardiogenic shock in Primary PCI, avoiding the need for transfer to other centres. Cost Implications of the Revascularisation and Cardiac Surgery This section of the Strategy is one of the most complex due to the interdependencies of the different treatment modalities and the impact of new techniques and interventions. It is clear that to address the inequalities seen within the Network, as well as those seen when Cumbria and Lancashire is benchmarked within England, significant investment would be required. The table below provides PCTs with an indication of the levels of investment that would be required to deliver the recommendations of this section of the Strategy to the standards recommended. It is worth noting that the development of PPCI has the potential to save not only lives but also £1.8 million recurrently in acute hospital care.
74

Recommendation for Revascularisation 1. In order to address the inequalities that exist between local health economies in Lancashire &
Cumbria, and within England, revascularisation rates across the Network should be increased to 1,500 pmp in 2009 to 1900pmp by 2011 and 2,250 pmp by 2015.
Recommendations for ACS 2. Patients admitted in Lancashire and Cumbria with a diagnosis of ACS must be treated in line
with the Network ACS protocol. This includes risk stratification, investigation and secondary prevention.
3. The development of a new electronic referral system should include real time monitoring of waiting times for referral to treatment for high risk ACS patients.
4. The Network ACS protocol recommends that all patients with a diagnosis of ACS should be seen by the local cardiology team within 24 hours of admission. Commissioners and providers must develop mechanisms to ensure this happens. Multiple site organisations may consider the use of telemedicine to ensure access to specialist review.
5. Upon publication of the NICE Clinical Guideline for ACS: the management of unstable angina and non-ST-segment-elevation myocardial infarction, commissioners and providers must ensure that local chest pain pathways are meeting the guidance.
6. A Network wide definition of MI should be developed and adopted by all Network organisations. Recommendations for Thrombolysis 7. Until pathways change with the rollout of PPCI, all health economies should ensure regular
multidisciplinary meetings, which involve NWAS, Emergency Departments and Cardiology to review performance and ensure robust performance data are established.
8. Service improvement work should be undertaken, with the support of the Network, in any units struggling to achieve the 30 minute door to needle target.
Recommendations for Primary Angioplasty 9. Primary Angioplasty using a 24/7 Treat and Transfer Model should be commissioned by 2011
for all patients with ST elevation MI (STEMI) across Lancashire and Cumbria, including the use of Drip and Ship for those living in the most remote areas.
10. A Network wide agreement should be reached to “share” the PPCI tariff between Tertiary Providers who will be repatriating patients after 24 hours and DGHs who should be funded for bed days used and Phase 1 cardiac rehabilitation.
11. In order to deliver the best outcomes for patients PPCI should be provided by existing Tertiary Centres i.e. Lancashire Cardiac Centre, James Cook University Hospital and the Freeman Hospital. This should be reviewed by 2013 and any change should be dependent upon evidence of improved outcomes, workforce and centre viability.
12. Commissioners should ensure there is sufficient ambulance capacity available to meet evidence based call to balloon time and to prevent any detrimental impact on other ambulance linked performance targets.
13. Commissioners should ensure access to all phases of Cardiac Rehabilitation is offered to patients following PPCI.
14. Commissioning of PPCI should incorporate a process for operational and performance review as agreed in NWAS Commissioning Principles. This work should be led by the Cardiac and Stroke Network which is working with other Networks to standardise this across the North West.
15. The Network should lead a piece of work to develop a single pathway for PPCI for the population of Lancashire and Cumbria. This should be undertaken at the earliest opportunity.
75
Recommendations for PCI 16. All PCI centres within the Network should meet the standards set by the Network’s
Revascularisation Task Advisory Group which require a minimum of 400 cases per annum rather than 200 cases per annum contained within the British Cardiovascular Intervention Society Recommendations for Good Practice and Training (2005) as it is anticipated this will shortly become the BCIS recommendation. These numbers should be achieved within 2 years of the development of a PCI centre. Given the evidence base that higher volume centres achieve improved outcomes any centre failing to achieve these standards within this timeframe should be de-commissioned.
17. All PCI centres in the Network should participate in both local and national audit and share their outcomes with the Network Board.
18. A PCI (not PPCI) centre should be commissioned in East Lancashire at the earliest opportunity. Commissioners should plan to increase revascularisation rates to 1900pmp within two years to guarantee a minimum of 400 cases per annum are treated.
19. NHS Cumbria should continue to assess the viability of establishing a PCI (not PPCI) centre in Carlisle. Commissioners should aim to increase revascularisation rates to 2250pmp within two years to guarantee a minimum of 400 cases per annum are treated, as well as exploring the delivery of this care to populations from outside Cumbria.
20. In those health economies where existing diagnostic catheter laboratories are due for replacement, but have not been recommended as PCI centres at this point in time, an assessment should be made of any new laboratories’ financial viability once local commissioning intentions linked to this strategy have been agreed. In order to maintain the diagnostic and device implantation capacity already in existence if business cases are non-viable within tariff commissioners and providers should explore the requirement for enhanced payments.
21. As commissioning intentions for revascularisation are clarified it is recommended that the need for further PCI capacity is re-evaluated across Lancashire and Cumbria by 2012.
Recommendations for Surgery 22. The NCEPOD recommendation that patients being considered for revascularisation should be
discussed at a Multi-disciplinary Team meeting (MDT) should be implemented across the Network. A Task Advisory Group with commissioning, cardiology, cardiac surgery and anaesthetic input should be established by the Network to agree which cases would benefit from an MDT approach.
23. Commissioners should plan for a 5% growth rate in valve surgery over the next five years due to the aging population of Lancashire and Cumbria
24. Commissioners should monitor the benefits of minimally invasive surgical techniques and support their expansion
25. Commissioners should ensure that sufficient surgical capacity is available to meet future revascularisation targets
26. A robust Network wide system for tracking 18 weeks Referral to Treatment times should be developed.
27. Should TAVI be commissioned on a North West basis local commissioners should support a location within Lancashire and Cumbria to prevent inequalities of access that may arise if it is provided elsewhere.
76

CARDIAC REHABILITATION
Introduction The aim of this section of the Strategy is to provide a sound evidence base for the effective commissioning of cardiac rehabilitation services across Lancashire and Cumbria that meet current guidelines and provide patients with appropriate and timely access over the next five years. ‘If there was a pill that cost very little, reduced cardiac deaths by 27 per cent, improved quality of life, and reduced anxiety and depression, every patient in Europe would be expected to take it. There is no such pill, but taking part in a cardiac rehabilitation programme can provide all of these benefits, in the UK only a small number of those in need are offered the chance to take part in it’. 82
Professor Lewin, European Society of Cardiology, Amsterdam 2005 National Policy In March 2000 the National Service Framework (NSF) for Coronary Heart Disease (CHD) 83 recommended that ‘NHS Trusts should put in place agreed protocols/systems of care so that, prior to leaving hospital, people admitted to hospital suffering from coronary heart disease have been invited to participate in a multidisciplinary programme of secondary prevention and cardiac rehabilitation. The aim of the programme will be to reduce their risk of subsequent cardiac problems and to promote their return to a full and normal life.’ A cardiac rehabilitation programme should begin as soon as possible after someone is admitted to hospital with CHD (Phase 1), continue through the early discharge period (Phase 2) and the formal rehabilitation programme (Phase 3) and extend into the long-term maintenance of the best possible health (Phase 4). Cardiac rehabilitation has been shown to improve prognosis and function for many people with CHD84. Evidence suggests that, when cardiac rehabilitation is provided well by appropriately trained staff and people are offered comprehensive and tailored help with lifestyle modification involving education and psychological input as well as exercise training, cardiac rehabilitation can reduce mortality by as much as 20% to 25% over three years.85,86 The patient experience of cardiac rehabilitation is also an overwhelmingly positive one.. The NSF83 goal set for cardiac rehabilitation recommends that every hospital should ensure: • that more than 85% of people discharged from hospital with a primary diagnosis of AMI or after
coronary revascularisation are offered cardiac rehabilitation • that one year after discharge at least 50% of people are non-smokers, exercise regularly and
have a BMI <30 kg/m2; these should be demonstrated by clinical audit data no more than 12 months old.
The NSF83 states that ‘once trusts have an effective system for recruiting people who have survived a myocardial infarction or have undergone coronary revascularisation to high quality cardiac rehabilitation, they should extend their rehab services to people admitted with other manifestations of coronary heart disease e.g. angina and heart failure.’
77

The National Audit of Cardiac Rehabilitation (NACR) The NSF CHD83 set out audit requirements for cardiac rehabilitation programmes. Performance against these standards is audited via the National Audit of Cardiac Rehabilitation (NACR) and published annually by the British Heart Foundation. 87 The NACR has two main components: an electronic database that staff use to input data electronically and an annual paper survey that collects data from those centres not yet linked electronically. The report also indicates that 39% of programmes had no clerical support. NICE Guidance for Myocardial Infarction: Secondary Prevention (2007:6) 88 recommends that: • All patients who have had an acute M.I should be given advice about cardiac rehabilitation
programmes, and offered a programme with an exercise component. (Individual assessment is necessary to ascertain the patient’s suitability for the exercise component of a CR programme)
• Programmes should:
- Provide a range of options - Encourage patients to attend all options appropriate to their needs - Not exclude patients from programmes if they chose not to attend certain components
• Patients with LV dysfunction who are stable can safely be offered the exercise component
British Association of Cardiac Rehabilitation Standards and Core Components for Cardiac Rehabilitation. (2007) The British Association of Cardiac Rehabilitation89 defined minimum standards and core components for cardiac rehabilitation (CR) services in order to ensure that all service providers, health professionals and service users understand the requirements for cardiac rehabilitation. Achieving such standards is a big challenge for many services and the delivery of CR will vary in response to different environments, differing population characteristics and local resources. The practice and science underpinning CR, albeit evidence based, 88,90-93 are constantly evolving and these standards aim to maintain a flexible approach and, at the same time, avoid being overly prescriptive. The integrity of CR needs to be assured by offering clearly defined core components that are sufficiently resourced. The aim of setting a minimum standard was to help clarify the provision for providers and enable a more equitable service. These standards are aimed at protecting services by establishing the baseline for what can be described as a rehabilitation programme and enable those who are seeking improved funding to demonstrate that their provision falls below the minimum acceptable level. 89
The BACR89 minimum standards relate to the infrastructure to support CR and the contents of a programme are defined by the recommended core components. Full CR programme status is dependent on meeting the minimum standards of the provision and delivery of the core components.
78
BACR Minimum Standards for Cardiac Rehabilitation These are the minimum standards for the successful delivery of CR (updated 2009). 94 To qualify as a full CR programme the providers must ensure that all the standards are achieved and that the programme adheres to the core requirements. 1. A co-ordinator who has overall responsibility for the CR service 2. A CR core team of professionally qualified staff with appropriate skills and competences to
deliver the service (Appendix 7) 3. A standardised assessment of individual patient needs (Appendix 8) 4. Referral and access for targeted patient population (Appendix 9) 5. Registration and submission of data to the National Audit for Cardiac Rehabilitation (NACR)
(Appendix 7) 6. A CR budget appropriate to meet the full service costs (Appendix 8) Local Provision There are currently nine cardiac rehabilitation programmes across Lancashire and Cumbria, mainly led by acute trusts to provide cardiac rehabilitation programmes in both the hospital and community settings. It should also be noted that Phase 4 CR is also provided by local authorities, community enterprises and the charity Heartbeat UK for patients in Blackpool and Central Lancashire. In some parts of the Network a creative approach bridging the gaps in access to cardiac rehabilitation has been adopted where health visiting/community nursing staff deliver Phase II CR via the Heart Manual. The Heart Manual is a six week, facilitated self-help rehabilitation programme for people recovering from a heart attack. It is based on a cognitive-behavioural model. Although all CR teams in Lancashire and Cumbria adopt a multi disciplinary approach either within the team, or via formally agreed input from or appropriate referral pathways to other disciplines i.e. dieticians, pharmacy, psychology, none of the cardiac rehabilitation teams are staffed in line with Scottish Intercollegiate Guidelines Network (SIGN) 95,96 and BACR89 recommendations
79

Cardiac Rehabilitation activity in Lancashire & Cumbria by provider 2007/08 Cardiac Rehabilitation
Programmes No. patients
2007/08 Phases offered Setting
1 Hospital 2 Phone, home visit 3 Community Blackpool87 1834*
4 Local authority Heartbeat *Number inflated by tertiary Phase 1 admissions
1 Hospital 2 Phone, home visit or clinic 3 Hospital and community East Lancashire87 959
4 Local authority
1 Hospital 2 Phone, home visit 3 Hospital Royal Preston Hospital87 662
4 Local authority Heartbeat
1 Hospital 2 Phone, home visit 3 Hospital and community Chorley Hospital87 568
4 Local authority Heartbeat
1 Hospital Furness General Hospital87 2 Home visit, clinic appt, phone
3 Six week hospital programme (inc CR funded by
Cumbria PCT)
440
4 Local authority Home base
Heart Manual
1 Hospital
2 Phone, Home visit, clinic
appt, 3 Six week hospital programme Royal Lancaster Infirmary 547
4
Lancaster & Morecambe College
Provided by volunteers
1 N/A 2 Phone, home visit, clinic 3 Community Westmorland General
Hospital 278
4 Local authority or voluntary
sector
1 Hospital 2 Phone, Home Visits 3 Six week hospital programme
West Cumberland Hospital 402
4 Local authority
1 Hospital 2 Phone, home visit, 3 6 week hospital programme
Cumberland Infirmary87 452
4 Local authority Lancashire & Cumbria
Network Total 5595
80

Of the nine programmes in Lancashire and Cumbria only the Cumberland Infirmary programme does not currently submit data electronically to the NACR. The NACR data shows cardiac rehabilitation activity, particularly around Phase III, but does not include overall demand. Unfortunately this is a national data collection issue, which causes difficulty in identifying to what extent the 85% NSF83 goal is being met. Current systems do not allow a robust analysis of whether services are meeting the health economy needs, or any benchmarking with other Cardiac Rehabilitation services within the Network. It should also be noted that figures appear to indicate that current data collection methods may lead to double counting of some MI/Revascularisation patients. This therefore produces a false positive relating to the actual number of patients being offered cardiac rehabilitation and masks the number of patients who are either declining or not being offered the opportunity to participate in a cardiac rehabilitation. For this reason now NACR87 recommend that all events within a 20 week period should be classified as one event. NACR87 have also experienced difficulty in monitoring performance against the NSF outcome goals relating to smoking, exercise and BMI. This has arisen because data 12 months post discharge has not been collected effectively as this group of patients have no further contact with the cardiac rehabilitation team after the end of the programme at 12 weeks. It should however be noted that, in light of this issue, NACR will now be collecting 12 week data to produce a quarterly outcome report. What is clear from the Lancashire and Cumbria data, in line with the findings of the National Audit of Cardiac Rehabilitation (NACR) (2009), 87 is that CR service provision across the Network is concentrated around myocardial infarction (MI), angioplasty (PCI) and bypass surgery (CABG) and patients with conditions such as heart failure or angina are not routinely offered cardiac rehabilitation. See chart below. National Audit of Cardiac Rehabilitation (NACR) Annual Statistical Report 2009. Cardiac Rehabilitation Activity in Lancashire & South Cumbria 2007-2008
MICABG & other surgeryPCIACSAnginaHeart FailurePacemakerOther
37%
36%
23%
2%
81
N.B. The above chart is based on NACR87 electronic data and does not include information about cardiac rehabilitation activity in 2007/08 for West Cumberland Hospital and Cumberland Infirmary, however, data provided for the BACR postal survey by these organisations also indicates the same trend. 97 It should be highlighted that although MI patients are seen in all nine hospital sites providing cardiac rehabilitation a large percentage of patients flow to the tertiary centre at Blackpool for revascularisation interventions. The impact of this trend is clearly reflected in the cardiac rehabilitation activity recorded for the Blackpool Victoria Hospital CR programme. New developments of new specialist cardiac services at the tertiary centre, particularly Primary PCI, will influence patient flow and, as a result, increase demand for acute CR interventions (Phase I) at the tertiary centre. This will also need to be balanced with the further development and maintenance of Phase III & IV CR programmes which will need to provide CR programmes post discharge in the patient’s local health economy. It is important to note that HRG4 is available to cover acute CR interventions only, i.e. whilst the patient is still occupying a hospital bed. The full reference costs for HRG4 acute CR is £250 per patient and will be triggered by recording the tariff code in the patient’s notes for the discrete CR intervention. The HRG4 acute tariff is not in the HRG lists for 2009/10 but this should not stop commissioners from using the HRG4. One of the challenges of the acute tariff is that the coding guidance narrative, which was set by the Information Centre (IC), requires that a rehabilitation consultant on a rehabilitation ward actions the HRG in the patient’s notes. This situation does not reflect clinical practice as patients are not admitted to specific rehabilitation wards but are admitted to a range of possible wards including coronary care, cardiology, medicine and elderly wards. Work is underway with the Information Centre to alter the text informing the HRG4 guidance and request that ‘rehabilitation consultant’ should be replaced with ‘cardiologist’ For the cases where acute CR is being requested by non cardiology consultants the tariff can still be triggered by a referral to cardiology. The acute CR tariff is unbundled and non-mandatory which, although not considered a position of strength, it nevertheless does allow commissioners and providers to negotiate delivery locally which will have a better fit with existing resources and staffing. Based on the range of CR provision a national mandatory tariff, setting out what should be delivered would only lead to further frustration in commissioning local services. The next phase of development is ongoing via a workstream aimed at developing a tariff for Phase II and III. The Heart Improvement team, BACR, BCS, NACR and the BHF are working towards a positive outcome in respect of a comprehensive tariff and commissioners will need to be aware that there will be further changes to the CR tariff in the near future. (Prof. Patrick Doherty. NCL for Cardiac Rehabilitation) Extending Provision to Other Cardiac Conditions It should also be noted that, as the trigger point for most referrals for CR is a hospital admission, there are currently no CR programmes across the Network routinely providing dedicated CR for heart disease patients managed in primary care. Quality Outcomes Framework (QOF) data indicates that across Lancashire and Cumbria there are a further 17,067 patients on heart failure registers98 and at least 9,50099 newly diagnosed stable angina patients each year, many of whom would benefit from a cardiac rehabilitation programme. It is therefore essential that each health economy develops systems to identify those patients from these groups who would benefit from cardiac rehabilitation. This information will enable commissioners to make informed decisions about the expansion of capacity within CR teams in line with identified need.
82
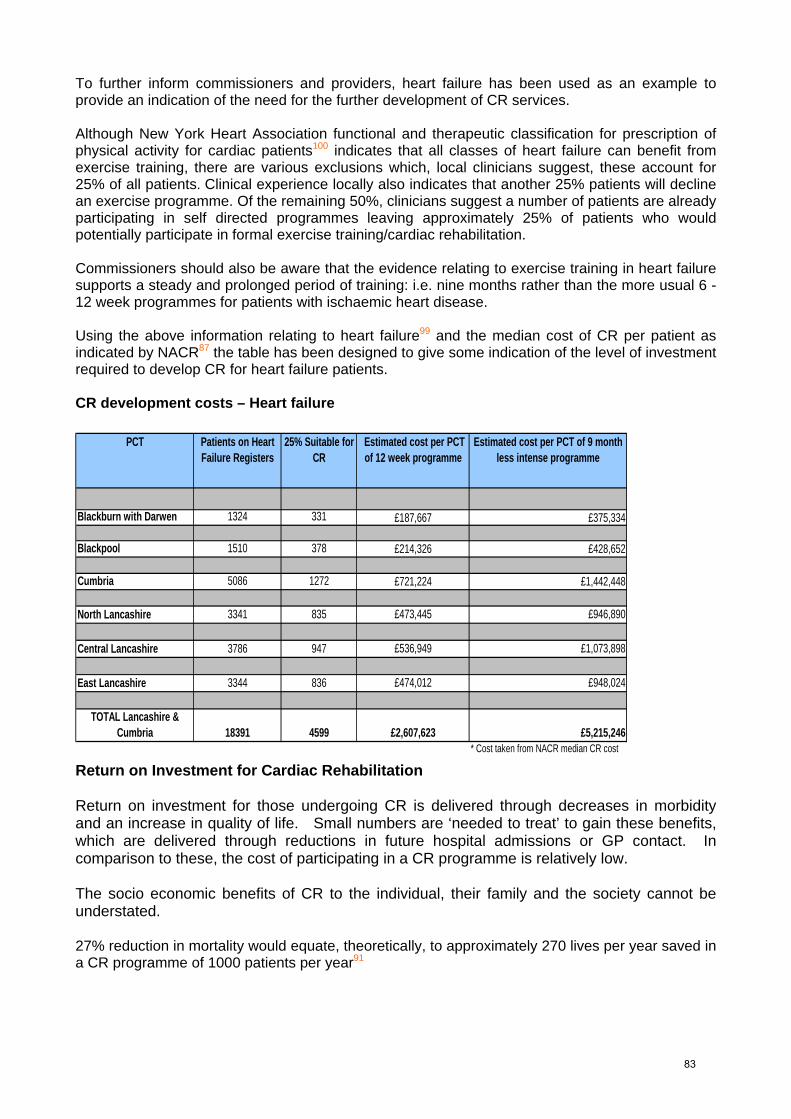
To further inform commissioners and providers, heart failure has been used as an example to provide an indication of the need for the further development of CR services. Although New York Heart Association functional and therapeutic classification for prescription of physical activity for cardiac patients100 indicates that all classes of heart failure can benefit from exercise training, there are various exclusions which, local clinicians suggest, these account for 25% of all patients. Clinical experience locally also indicates that another 25% patients will decline an exercise programme. Of the remaining 50%, clinicians suggest a number of patients are already participating in self directed programmes leaving approximately 25% of patients who would potentially participate in formal exercise training/cardiac rehabilitation. Commissioners should also be aware that the evidence relating to exercise training in heart failure supports a steady and prolonged period of training: i.e. nine months rather than the more usual 6 - 12 week programmes for patients with ischaemic heart disease. Using the above information relating to heart failure99 and the median cost of CR per patient as indicated by NACR87 the table has been designed to give some indication of the level of investment required to develop CR for heart failure patients. CR development costs – Heart failure
PCT Patients on Heart Failure Registers
25% Suitable for CR
Estimated cost per PCT of 12 week programme
Estimated cost per PCT of 9 month less intense programme
Blackburn with Darwen 1324 331 £187,667 £375,334
Blackpool 1510 378 £214,326 £428,652
Cumbria 5086 1272 £721,224 £1,442,448
North Lancashire 3341 835 £473,445 £946,890
Central Lancashire 3786 947 £536,949 £1,073,898
East Lancashire 3344 836 £474,012 £948,024
TOTAL Lancashire & Cumbria 18391 4599 £2,607,623 £5,215,246
* Cost taken from NACR median CR cost
Return on Investment for Cardiac Rehabilitation Return on investment for those undergoing CR is delivered through decreases in morbidity and an increase in quality of life. Small numbers are ‘needed to treat’ to gain these benefits, which are delivered through reductions in future hospital admissions or GP contact. In comparison to these, the cost of participating in a CR programme is relatively low. The socio economic benefits of CR to the individual, their family and the society cannot be understated. 27% reduction in mortality would equate, theoretically, to approximately 270 lives per year saved in a CR programme of 1000 patients per year91
83

Costs per quality adjusted life year: • £22,000 for coronary artery bypass surgery101 • £47,000 for percutaneous coronary intervention (angioplasty) 102 • £15,700 approximately for cardiac rehabilitation (averaged up at 5% from 1997 costs). 103 CR assists patients to recover psychologically.101 Patients who do not make a full psychological recovery cost society more than those who do. For example, a cohort of anxious and depressed patients followed over a year accrued four times the healthcare costs of the patients who were not anxious or depressed. These extra costs were all attributed to additional emergency admissions, tests and procedures, and not to psychological help. 104
Modelling done in Scotland from a randomised trial of a home-based rehabilitation programme showed that, depending on the grade of staff and the use of home visits, was cost saving due to the 30 per cent reduction in unplanned readmissions to hospital found in the trial. 105
Recommendations The CSNLC supports the BHF description of cardiac rehabilitation as ‘unfinished business’87
The CSNLC makes the following recommendations: 1. All health economies in Lancashire and Cumbria should refer to the National Service
Framework for Cardiac Rehabilitation, SIGN guidelines NICE guidelines and BACR Standards and Core Components for Cardiac Rehabilitation as a framework on which to base their model of service provision.
2. Working in conjunction with local commissioners and public health specialists the Network
should undertake a review of Cardiac Rehabilitation services, looking at demand, current and future capacity and workforce establishments, in line with SIGN/BACR guidelines.
3. Rehabilitation should be an integral part of the patient pathway with robust referral mechanisms
for patients admitted to hospital – ACS, heart failure, PCI and CABG as well as those with implanted cardiac devices.
4. Rehabilitation programmes should be extended to incorporate those patients identified as living
with a cardiac condition in primary care – heart failure, stable angina and include community based exercise programmes.
5. In line with NACR recommendations all CR events within a 20 week period should be classified
as one event. 6. Data collection - All CR teams in Lancashire and Cumbria should submit data electronically to
the NACR, allowing commissioners to use NACR quarterly outcome reports to monitor the effectiveness of CR interventions. This would allow benchmarking comparisons to be made from which informed commissioning plans can be developed.
84

HEART FAILURE
Introduction This chapter of the Strategy outlines the current provision of heart failure services across Lancashire and Cumbria and makes clinical and commissioning recommendations that support the identification, diagnosis and management of heart failure patients both within primary and secondary care. The recommendations are aligned to the work carried out by the National Technology Adoption Centre (NTAC). This work assessed the heart failure clinical pathways established through Map of Medicine and established future requirements for local services across Lancashire and Cumbria (Appendix 10).
Also assessed are the requirements for further identification of patients with heart failure earlier in the disease process and streamlining the medicines and potential interventional clinical management of these patients. National drivers National Service Framework The National Service Framework for Coronary Heart Disease (DH, 2000) 61 addresses heart failure services in chapter 6. One standard (Standard 11) is established within the NSF; however a systematic approach - to the delivery of care, the services and systems of care that should be used – is highlighted as essential. Standard 11 – ‘Doctors should arrange for people with suspected heart failure to be offered appropriate investigations (e.g. electrocardiography, echocardiography) that will confirm or refute the diagnosis. For those in whom heart failure is confirmed, its cause should be identified – the treatments most likely to both relieve symptoms and reduce their risk of death should be offered.’ National Institute of Clinical Excellence The following NICE guidance and technology appraisals relate to the care of heart failure patients:
(1) NICE clinical guideline CG5 on chronic heart failure (2003) 64 recommends that heart failure
care should be delivered by a multidisciplinary team with an integrated approach across the healthcare community and the management of heart failure should be seen as a shared responsibility between patient and healthcare professional. The guideline gives a series of evidence based recommendations for all aspects of patient care and service design. The guideline is in the process of being updated currently in 2009.
(2) NICE technology appraisal 120 gives guidance on the use of cardiac resynchronisation therapy (CRT) in-patients with heart failure (2007). 65
(3) NICE technology appraisal 95 gives guidance on the use of internal cardioverter defibrillators (ICDs), including patients with heart failure (2006). 66
Healthcare Commission Heart Failure Audit ‘Pushing the boundaries: improving services for people with heart failure’ was published by the Healthcare Commission in 2007 and indicated that further improvements are still required in the care of heart failure patients, and recommended that the NICE guideline was more effectively implemented. 106 The Healthcare Commission identified considerable variation in the prevalence of heart failure by primary care trust and that patients are not always receiving optimal levels of care. It recommended that commissioners develop strategies to manage this unmet need and the expected rise in the number of people with heart failure over the next 20 years.
85

Department of Health Priorities and Initiatives
World class commissioning 'The NHS in England: The operating framework for 2009/10’ (2008) 107 Delivering the 18 week patient treatment pathway The ‘Care Closer to Home’ initiative outlined in chapter 6 of the white paper ‘Our health, our
care, our say’ (2006)108 ‘Commissioning framework for health and well-being’(2007) 109 Transforming Community Services Advancing Quality Considering the impact of patient choice The Expert patients programme ‘A stronger local voice: a framework for creating a stronger local voice in the development of
health and social care services’ (2006) 110 ‘Standards for better health’ (2004, 2006) 111 Focus on: Heart Failure, NHS Institute for Innovation and Improvement (2009) 112
Prevalence of Heart Failure and Current Service Provision within Network Prevalence data for heart failure is available from research studies and registries. There is not as yet a comprehensive national heart failure database; although this is in development and is partially used by some heart failure teams across the Network. In the Healthcare Commission Heart Failure Audit the national recorded prevalence (1.8%) of heart failure was lower than that predicted by the analysis of research studies (2.3%). This suggests that improvements in the diagnosis and identification of patients with heart failure are still required. The Healthcare Commission also identified considerable variation in the prevalence of heart failure by PCT (0.19% to more than 5%). Some of this may be legitimate local variation secondary to public health differences but such a wide variation would suggest considerable differences in referral for or access to diagnostics. The GMS QOF data provides one potential national data source for heart failure but the data is limited in its scope and completeness. Using the QOF data the prevalence for the Lancashire and Cumbria Network is 0.9%; or 18,391 patients and it is expected that this is a substantial underestimate of the true prevalence level. Assessing the Network prevalence against the national average, double the number of patients identified on QOF would be expected (36,782). Taking the upper prevalence level of 5%, the numbers in the region would need to be five times that reported in QOF (91,955).
As previously noted, the GMS QOF data provides one potential national data source for heart failure but the data is limited in its scope and completeness and local work undertaken has shown that validation of registers is required to ensure those registered with HF1 are also receiving correct treatment and care. Coding and discharge summaries provided by the acute trusts should support primary care practices to readily identify those patients with heart failure and provide clarity of diagnosis supported by Echocardiography reporting. Communication from secondary care to primary care should be standardised across the Network.
86
Network QOF Data by PCT 2007/2008 The table shows the Network QOF heart failure data by PCT HF1 - Practices that have a heart failure register HF2 - Patients with heart failure confirmed by echo or specialist HF3 - Patients with heart failure prescribed ACE-I
Prevalence
Numerator Denominator National Centile
HF1 0.8% 3786 464629 53 HF2 94.6% 610 645 11
Central Lancs
HF3 87.6% 1576 1800 5 HF1 0.9% 3344 387543 63 HF2 96.8% 519 536 53
East Lancs
HF3 89.1% 1355 1521 24 HF1 0.8% 1324 165500 NA HF2 95.9% 213 222 NA
Blackburn with Darwen HF3 89.6% 587 655 NA
HF1 1% 3341 337196 86 HF2 97.8% 581 594 82
North Lancs
HF3 88.6% 1518 1713 16 HF1 1% 1510 152140 88 HF2 95.2% 257 270 18
Blackpool
HF3 86.9% 677 779 2 HF1 1% 5086 518293 85 HF2 96.8% 763 788 52
Cumbria
HF3 90.1% 1845 2047 49 HF1 0.9% 18 391 2025301 HF2 96.2% 2 943 3055
Network Total
HF3 88.7% 7558 8515 Source - NHS Quality and Outcomes Framework Information Centre for Health and Social Care. In order to scope current specialist heart failure service provision across the Network, a questionnaire was circulated and completed by the members of the Network Heart Failure group. There is a range of service provision across the Network. All patients with heart failure will be managed by their primary care team but may also be under the care of generalist secondary care medical team, a cardiology team or a specialist heart failure team in primary or secondary care. Some patients may also be receiving care from one of the tertiary cardiac centres. Research has consistently shown that patients receiving only generalist primary care tend to have lower levels of optimised treatment and access to treatments compared with patients who are also seen by a specialist heart failure service113,114. Within the Network there is a diversity of heart failure service models and provision. There are six services based in primary care: five using a specialist nurse model and one using a community matron model. There are two secondary care based services. All the services are nurse-led apart from three, which are multi-disciplinary, as they have part-time medical staff in the team (1 x Consultant Cardiologist; 2 x GPwSI). The table below outlines the services provided in each health economy.
87
Primary care NHS Blackburn with
Darwen Heart Failure Specialist Nursing Service with in-reach services to the acute trust (provided by NHS East Lancs)
NHS Blackpool Community Matron with Special Interest led NHS Central Lancs Heart Failure Specialist nurse led with in-reach
services to the acute trust NHS Cumbria (North) GPwSI and Heart Failure Specialist nurse led
with in-reach services to the acute trust NHS East Lancashire Heart Failure specialist nurse led with in-reach
services to acute trust NHS North Lancs GPwSI and Heart Failure Specialist nurse led
(North) Community Matron led (South) Secondary care Blackpool, Fylde & Wyre
Hospitals NHS Foundation Trust
Heart Failure specialist – Consultant Cardiologist and Heart Failure Specialist nurse led
North Cumbria University Hospitals Trust
Staff Grade Cardiologist led one stop Heart Failure clinic
Lancashire Teaching Hospitals NHS Foundation Trusts
Heart Failure Specialist nurse led (1 site only)
There is a variation of referral criteria for the services across Lancashire and Cumbria. All the services expect a definitive diagnosis of heart failure prior to accepting referrals but some impose further referral criteria restrictions such as systolic dysfunction and a level of reduction in left ventricular ejection fraction, commonly less than 40%. Consideration may and should be given to the level of symptoms experienced by the patient. Those services based on the community matron model can also have additional criteria: such as the patient being older, or having more than one chronic long term condition, or had a recent hospital admission. There is considerable variation in caseload between services. The community matron based services tend to have a smaller number on caseload than the specialist nurse based services. Three established community specialist nurse services have over 500 patients registered (NHS Central Lancashire, NHS East Lancashire/Blackburn with Darwen and NHS Cumbria (North) and the community matron services report caseloads of between 50 to100 at present. As there are variations in referral criteria this may reflect a difference in patient characteristics or dependencies. The combined caseloads of all the services in the Network are over 2,500 heart failure patients. This represents less than 15% of the patients with heart failure in the Network as identified in the combined QOF data. Staffing of services also varies considerably. The largest team is one that contains five nurses plus administrative support (NHS East Lancashire and NHS Blackburn with Darwen) and the smallest services are single-handed (Lancashire Teaching Hospitals NHS Foundation Trust). None of the teams at present have any Allied Health Professionals directly as part of their staffing - although this is budgeted for in one service (NHS Central Lancashire, physiotherapist 0.2 WTE). The staff-patient ratio varies from 1:20 to 1:500 with the average being 1:187. Not all of the services operate in both primary and secondary care. Not all the services offer exercise training or palliative care for their patients. All services are involved in education and training but only two services are participating in research. Most services are, or plan to, link with Map of Medicine.
88

Gap Analysis It is clear that there is considerable variation across the Network in model and scope of heart failure services. Whilst some local variation is legitimate, based on differing needs, it may also be due to a lack of clarity about what is a good standard service or having the commitments from commissioners to fund such services. Generalists must be involved in the care of patients with heart failure - especially to raise the diagnosis and monitor ongoing treatments and complications. However, all patients with heart failure should receive the same standards of care no matter who is caring for them and most generalists will not be able to treat all patients with heart failure in accordance with the guidelines: establishing aetiology, maximising treatments and ensuring access to and implementing all evidence based treatments - without specialist involvement (Hanumanthu et al 1997, Jaarsma et al, 2006).113,114 The level of specialist involvement will depend upon the scope of the services involved.
The guidelines state all areas should have access to a dedicated heart failure service staffed by specialists in heart failure. It is not yet the case throughout the Network that all areas have access to a dedicated heart failure service. Coverage, staffing and caseloads of services are a matter for local commissioners. Services should be planned to be adequate for the current and future heart failure population based on the principles of equitable, fair and timely access to those services. As heart failure has a comparable mortality and morbidity impact to cancer, specialist heart failure services should be planned to provide the same level of support as those for cancer patients. It is recommended that commissioners continue to scope and plan to provide a robust heart failure service that meets the needs of the patients. Workforce considerations Services should, wherever possible, be multi-disciplinary: either directly within a dedicated team; with ring-fenced time; or with effective referral systems. All services must be robust enough to cope with staff absences and single-handed services are particularly vulnerable to this. Most of the services within the Network are highly vulnerable to staff absences because of their small size and the difficulties of arranging cross-cover from suitably qualified staff. All services should be developed that provide appropriate staffing levels. There is a small amount of research being undertaken and this lacks co-ordination. As the services currently contain more than 2,000 patients and there are many unknowns about heart failure this is a missed opportunity and heart failure research should be considered when establishing new or developing current services. Education and training, including utilising established Multi-disciplinary Team (MDT) meetings and available videoconferencing as a platform to develop and train staff as well as providing valuable clinical support should be considered. Standards for Service Development
The outcomes for effective Heart Failure management should include the following: Prolonging life and improving the quality of life Heart failure is not a curable condition for most patients. It is however manageable and, with timely and accurate diagnosis and treatment, prognosis can be improved. Improvements in prognosis are very difficult to judge in individual patients but data trends can be monitored in the overall heart failure population by area.
89

As important to most patients as length of life is quality of life. Effective treatment and review of heart failure can make substantial improvements to patients’ quality of life. It is unrealistic to expect all patients to be free of problems but it should be the aim of treatment to reduce symptoms and promote adaptation and independence. This can be monitored through NYHA (New York Heart Association, symptom classification, Appendix 11) 100 class questionnaires and other self-reporting mechanisms. Reduce Unnecessary Hospital Readmissions Hospital admissions with acute heart failure are sometimes unavoidable and can be the correct pathway to access certain treatments. However, it is known that many hospital admissions with heart failure, especially readmissions, are avoidable. It is usually the patients who wish to avoid hospital and it is generally in the interests of the NHS to avoid unnecessary hospital admissions. Unnecessary admissions in patients with heart failure can be avoided by providing co-ordinated specialist care, including support for high risk patients, by optimising their management plan and communicating effectively with the primary care team, patient and carers. Improving Clinical Outcomes The natural history of heart failure is complex: depending upon the aetiology of the heart failure and is multi-factorial with maturation biases and interactions with other co-morbidities to consider. In looking for improvements in clinical outcomes the general aim should be to improve cardiac function or at least slow down the rate of deterioration. This can be monitored through functional testing and objective investigations. It can also be implied through rates of eligible patients receiving optimal treatment. (NICE, 2003). 64 Reducing Inequalities The Healthcare Commission Audit of Heart Failure showed variations in access to diagnosis and therefore treatment. Research also shows these variations in access to diagnostics and treatments: for example, angiotensin converting enzyme (ACE) inhibitors for women, who are less likely to receive them than men106, and exercise or programmes of rehabilitation and palliative care115. There is also a need to improve knowledge of heart failure among patients from ethnic minority groups where there is evidence of deficiencies in the information being given116. Evidence of the effectiveness of interventions to reduce inequalities can be gained from audit and public health data. Increasing Patient Choice Services should be designed around patients rather than vice versa. This may require an analysis of the fitness-for-purpose of service design in areas that have services that have been established for some time. Patients should be offered reasonable choice and flexibility in the services they receive and be fully participatory in treatment decisions. This can be demonstrated through improving partnership working, patient experience and engagement. Supporting Patients at End of Life The Gold Standards Framework (GSF) is a framework designed to help primary care teams deliver the best possible care for people nearing the end of their lives. Its aims are to provide consistent high quality care in alignment with patients’ preferences, encouraging pre-planning and anticipation of needs and offering improved staff confidence and teamwork. One clearly defined measure of outcome benefit is more home-based and less hospital-based care. Currently 90% of practices nationally claim the Quality and Outcomes Framework (QOF) palliative care points in the GP Contract (equates to 90% adoption of GSF Level 1). Over 60% of practices in the UK are using GSF more fully, and 10-15% have fully embedded it.
90

Providing Cost Effective Services Services should have data available to analyse the cost effectiveness of their model of care, their services and the treatments they offer. Establishing cost effectiveness can be complex and it is important to look at all stages of the patient pathway to establish whether costs from one sector are being displaced in to another and whether the services are using the most appropriate model for their locality and individual circumstances. Below is an overview of the financial considerations for the development and implications of the management and care of heart failure patients.
Cost Analysis 64 - General economic considerations Improved symptom control and patient education are likely to result in fewer unplanned admissions and result in potential cost savings. Direct costs (potential savings) will depend on the morbidity burden relating to the condition, specific costs, e.g. GP visits, hospitalisation and the efficacy of treatment in relation to morbidity. Finally the slowing of progression of heart failure from mild (NYHA I and II) to more severe (NYHA III and IV) will reduce all forms of healthcare utilisation including hospitalisation which clearly has a high cost impact. Additional costs include those of treatments provided and ongoing utilisation of healthcare resources for life years extended. ACE Inhibitors Evidence shows that the use of ACE inhibitors in heart failure reduces hospitalisation by slowing disease progression, improves Quality of Life (QoL) and extends length of life. Hospitalisation accounts for 60-70% of all NHS heart failure expenditure in the UK. A reduction in hospitalisation for progressive heart failure has been shown in patients taking ACE inhibitors. Beta Blockers Evidence suggests that beta blockers can improve symptoms, prolong survival and reduce hospitalisation, whilst increasing the use of beta blockers will increase treatment costs, some or all of this will be offset largely by reduced hospitalisation. Specialist Heart Failure Services 117 The data supporting the widespread introduction of services based on the expert management applied by specialist heart failure programmes of care achieve benefits for patients and carers. Furthermore, these services have the potential to deliver significant cost savings. The figure below shows the expected cost benefits of a UK wide heart failure service. The graph shows the approximate savings achieved via a 20 – 50% reduction in the typical pattern of recurrent hospital stay seen in patients with heart failure in the UK.
Source: The European Journal of Heart Failure (2005)
91
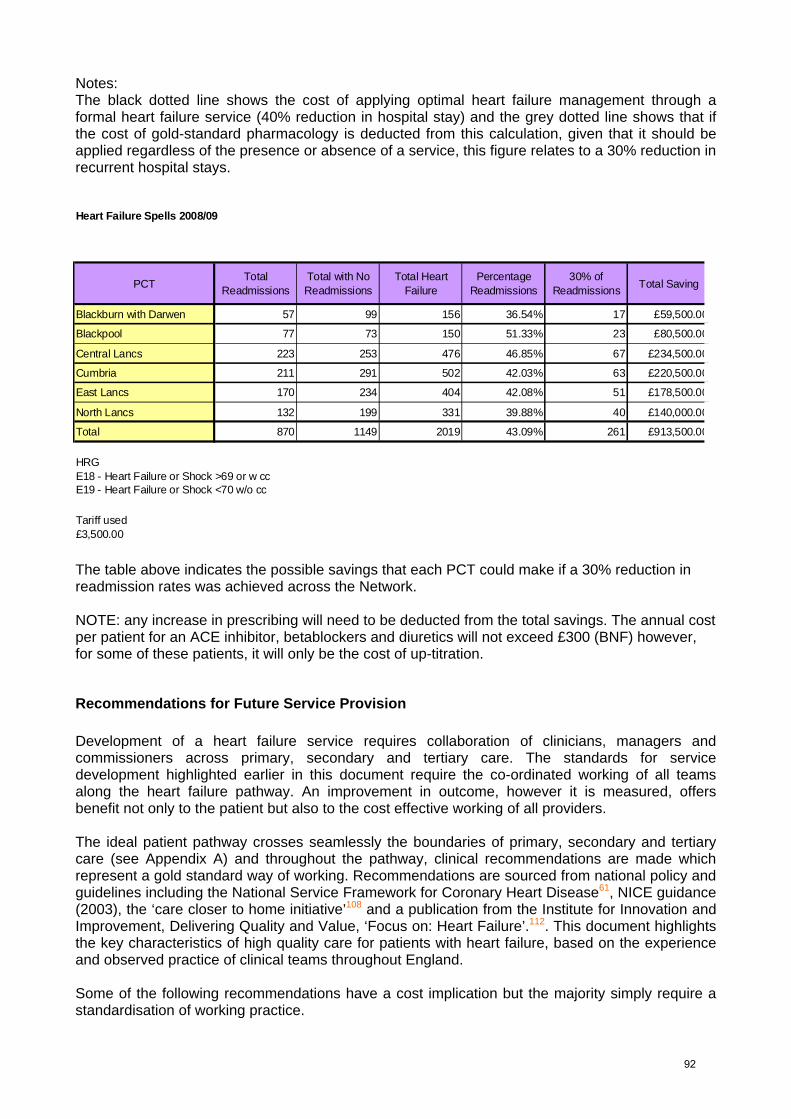
Notes: The black dotted line shows the cost of applying optimal heart failure management through a formal heart failure service (40% reduction in hospital stay) and the grey dotted line shows that if the cost of gold-standard pharmacology is deducted from this calculation, given that it should be applied regardless of the presence or absence of a service, this figure relates to a 30% reduction in recurrent hospital stays.
PCTTotal
ReadmissionsTotal with No Readmissions
Total Heart Failure
Percentage Readmissions
30% of Readmissions Total Saving
Blackburn with Darwen 57 99 156 36.54% 17 £59,500.00
Blackpool 77 73 150 51.33% 23 £80,500.00
Central Lancs 223 253 476 46.85% 67 £234,500.00
Cumbria 211 291 502 42.03% 63 £220,500.00
East Lancs 170 234 404 42.08% 51 £178,500.00
North Lancs 132 199 331 39.88% 40 £140,000.00
Total 870 1149 2019 43.09% 261 £913,500.00
HRG
Tariff used£3,500.00
Heart Failure Spells 2008/09
E18 - Heart Failure or Shock >69 or w ccE19 - Heart Failure or Shock <70 w/o cc
The table above indicates the possible savings that each PCT could make if a 30% reduction in readmission rates was achieved across the Network. NOTE: any increase in prescribing will need to be deducted from the total savings. The annual cost per patient for an ACE inhibitor, betablockers and diuretics will not exceed £300 (BNF) however, for some of these patients, it will only be the cost of up-titration.
Recommendations for Future Service Provision Development of a heart failure service requires collaboration of clinicians, managers and commissioners across primary, secondary and tertiary care. The standards for service development highlighted earlier in this document require the co-ordinated working of all teams along the heart failure pathway. An improvement in outcome, however it is measured, offers benefit not only to the patient but also to the cost effective working of all providers. The ideal patient pathway crosses seamlessly the boundaries of primary, secondary and tertiary care (see Appendix A) and throughout the pathway, clinical recommendations are made which represent a gold standard way of working. Recommendations are sourced from national policy and guidelines including the National Service Framework for Coronary Heart Disease61, NICE guidance (2003), the ‘care closer to home initiative’108 and a publication from the Institute for Innovation and Improvement, Delivering Quality and Value, ‘Focus on: Heart Failure’.112. This document highlights the key characteristics of high quality care for patients with heart failure, based on the experience and observed practice of clinical teams throughout England. Some of the following recommendations have a cost implication but the majority simply require a standardisation of working practice.
92

Early diagnosis It is known that early diagnosis of heart failure improves all outcomes. This is expressed in the ACC/AHA grading scheme that includes patients at risk of heart failure (grade A) and with asymptomatic heart failure (grade B) before those with symptomatic (grade C) and end-stage (grade D) heart failure. Traditionally specialist services are often involved at too late a stage of the patient’s progression and this should be overcome by changes in service design and clinical practices. It is recommended that: • Routine screening for heart failure should occur in all chronic disease management clinics that
are known aetiologies for heart failure (i.e. hypertension, coronary artery disease, cardiovascular disease, atrial fibrillation, diabetes and chronic obstructive airways disease) and for other specific patient groups at risk (i.e. post chemotherapy, alcohol excess, rheumatoid arthritis).
• For symptomatic patients self-assessment using NYHA class (see Appendix 11) should be implemented.
• B-type Natriuretic Peptide (BNP) assessment should be available to all clinicians. A recent Health Technology Assessment (2009)118 (Appendix 12) reviewed the role of BNP as a cost effective rule out for heart failure in primary care. Patients who have symptoms consistent with heart failure should have BNP assessment as a first line investigation. BNP testing results should also direct further investigation and management.
• All practices should have access to either secondary care or primary care (supported by secondary care) based specialist heart failure services. Diagnosis will usually be made by echocardiography. This must be provided by sonographers using clinical governance processes and regulations that ensure a high standard of scanning and reporting. (Appendix 3)
• Where appropriate a Heart Failure Diagnostic Clinic (HFDC) model should be ‘one-stop’: providing point of care (PoC) BNP testing to systematically screen symptomatic patients for heart failure but should also provide formal diagnosis by echocardiogram.
• Comprehensive assessment with regard to aetiology and a management plan, including first line therapy and eligibility for advanced heart failure treatment, along with initial patient education and lifestyle advice should be provided.
• Consideration should be given to those patients with heart failure and preserved systolic function. This patient group often requires costly hospital admission and, if untreated, have similar prognosis to those with impaired systolic function. The same evidence base for treatment of this group is not yet available but symptom control and cardiovascular risk assessment, particularly appropriate to the treatment of hypertension for example, has been shown to improve outcome.
Often patients with symptomatic heart failure access primary care services with other conditions but despite this identification and diagnosis of patients with heart failure may still occur at a late stage requiring a higher level of care to be provided.
Primary Care/Intermediate Care The majority of heart failure patient care can and should be provided in a primary care setting as this is the context in which patients live for most of the time. Appropriate community heart failure services and effective treatment are clinically and cost effective as they reduce the need for secondary care services. Community based services are the preferred choice of most patients and fit with Department of Health policy. Research shows that generalist care in isolation does not consistently offer the high quality care that is required for heart failure patients: patients are under-diagnosed, under treated with medication, have more acute admissions, and lower chance of being referred for device and surgical treatments. Generalists should be supported by a dedicated heart failure specialist service in each locality: working as partners with each other and the patient.
93

Improvement in the primary care management of heart failure relies on robust standardised systems of diagnosis and management and these include: • Simple and accessible diagnostic pathway/service supported by referral to and from a
specialist heart failure services to provide a management plan. • Strong two-way communication links between providers in the primary care setting; General
Practitioners (including those with Special Interest), Specialist Nurses, District Nurses, Palliative Care, Community Matrons, Social Care etc. When developing new or existing services, the availability to access and transfer information between primary and secondary care ensuring all IT systems are linked and accessible by all healthcare professionals should be considered
• A comprehensive, primary care delivered, standardised heart failure management programme, delivered by a multidisciplinary team, with systems to provide optimisation of medication and regular follow up of patients to ensure optimisation of care – including ongoing review of suitability for new treatments and referral on to specialist services as appropriate.
• Heart Failure Specialist Nurses (HFSN) have a clear role in the management of complex heart failure patients or for follow up of those who have required hospital admission. There is considerable evidence to support Specialist Nurse led programmes to both reduce the admission and readmission rate119 for these groups of patients. Heart failure services are comparatively under resourced, despite the overwhelming evidence of benefit, when compared, for example, with services for cancer care.
• Heart failure services have greater reflexivity when located in primary care and this includes cardiac rehabilitation programmes for heart failure patients. Long term compliance with an exercise programme should be facilitated. Some patients will not be suitable for exercise programmes and others choose not to participate: it is estimated that 25% of all patients will take up exercise training. Exercise training has benefits to prognosis, quality of life, functional capacity and improvement in cardiac performance in patients with heart failure. This includes patients with severe heart failure (NYHA class III and IV). Routine use of a structured exercise programme, following implant of biventricular pacemaker, has been shown to further improve outcomes in those patients120. Extensive patient registries show that exercise training is safe in cardiac patients. The cost of exercise training programmes is not prohibitive and existing services can be extended at an even lower cost than setting up new services. Within the Network not all areas have equitable access to cardiac rehabilitation programmes for patients with heart failure. All patients should be assessed for exercise training classes and those who are suitable should be able to access these reasonably locally.
• For stable and optimised patients, routine review every six months should be provided. This should include assessment of symptoms (including NYHA class), compliance with treatment/ side effects, renal function and, where indicated, ECG recording giving consideration to the rhythm and QRS duration as indicators for Cardiac Resynchronisation Therapy. Chronic heart failure is a recognised risk factor for developing chronic kidney disease (CKD) and its associated complications such as anaemia, bone disease and acidosis. People identified with heart failure should be routinely offered testing for CKD and referred to a renal specialist if necessary121. (Please refer to Cumbria & Lancashire CKD Algorithm – accessed at http://nwwlancashireteachinghospitals.nhs.uk/renal)
• Each health economy should demonstrate a robust GSF system that clearly links to the locally provided heart failure service. PCTs should ensure existing palliative care services link with heart failure services using audit data showing use of GSF and end-of-life tools in non-malignant terminal care.
• All areas should have arrangements in place to facilitate timely switch-off of Implantable Cardioverter Defibrillators (ICDs), where appropriate at the end-of-life. (Appendix 13)
94

Secondary Care Secondary care services support primary care by offering diagnostics to confirm heart failure; confirmation of aetiology; a management plan; ongoing care for complex patients; inpatient care for acutely ill patients; and assessment of and referral for advanced therapies. Within secondary care, patients may receive treatment in a number of settings: in the Accident and Emergency Department or Medical Assessment Units initially and then either under the care of general physicians or cardiologists. Heart failure is not always the primary reason for admission and these patients may be managed on non-medical wards or by specialists in other fields. There is clear evidence supporting the specialist care of these patients and consideration should be given to the implementation of the most cost effective, practical model that has clear benefit to patient outcomes. Hospitals should be encouraged to put in place systems, such as Advancing Quality, designed to audit and encourage good and consistent practice.
• Acute trusts should directly offer, or closely support a primary care led Heart Failure Diagnostic Clinic. The HFDC model should ideally, depending upon local factors, be ‘one-stop’, encouraging early return to local clinicians. The HFDC must provide not only formal diagnosis by echocardiogram but comprehensive assessment with regard to aetiology, early symptom control and comprehensive management plan, including first line therapy and eligibility for advanced heart failure treatment if a patient does not improve. It must also provide patient education and lifestyle advice – bearing in mind follow-up will be needed within the heart failure pathway to ensure understanding and concordance.
• Secondary care inpatient and outpatient services for patients with heart failure must be provided in accordance with NICE guidance – regardless of the staff specialities. The following audit requirements for heart failure are mandated in the Advancing Quality system.
• All patients admitted to hospital should be given (with clear documentation of the same): a. A diagnosis b. Education regarding their diagnosis c. ACE inhibitor (or an alternative if not tolerated) d. A comprehensive plan at discharge including appropriate follow up
(Beta blocker therapy is soon to be added as a requirement). • Adherence to heart failure guidelines would be best achieved by ensuring that all patients
have initial contact, at least, with a heart failure specialist during every admission. This may be a Heart Failure Specialist Nurse or Cardiologist who will ensure optimisation of care as required and consider advanced management options as appropriate
• The heart failure team should liaise with any community specialists who have been involved in the patient’s care leading up to admission. Discharges should be planned: a Rapid Discharge Plan is appropriate for some patients but not for all. The heart failure team should be responsible, in consultation with the admitting team for triage of patient follow up to primary/ intermediate/secondary care at the time of discharge. There must be a management plan, in line with NICE Guidelines and Map of Medicine, which is communicated to the patient and General Practitioner at discharge. The electronic summary provided by the National Heart Failure Audit Database may meet this need.
• Echocardiogram should be available during admission or shortly after discharge, for all patients who have not had this investigation previously.
• Cardiac rehabilitation programmes specifically designed for heart failure patient should be available to all suitable patients. Identification of suitable patients should begin during admission and be implemented as outpatients or in the community.
• Ideally patients who are reaching end of life will have been registered on the Gold Standards Framework, thus avoiding admission unless dictated by patient choice. Some patients will approach EOL during admission and these patients should receive appropriately adjusted treatment and be offered the choice and support to be transferred to their preferred place of care at EOL.
95
• Ideally an ‘EOL’ team, specific to heart failure would be best placed to provide this service. This might include a Heart Failure Specialist Nurse, a Palliative Care Nurse, a Cardiology Consultant, a Palliative Care Consultant and a discharge co-ordinator. Communication with colleagues in primary care, including General Practitioners and District Nurses is essential.
Note: Device therapy may be offered in a secondary care setting by those with the necessary training and in accordance with local clinical governance. In this chapter it is considered under the heading of tertiary care and is discussed in more detail within the Arrhythmias and Devices chapter of this Network Strategy.
Tertiary Care Tertiary level care is to optimise treatment in complex patients and those refractory to standard therapy, by using advanced therapies. In addition to optimisation of pharmacological therapy, patients may be referred for consideration of device therapy. Device therapy includes cardiac resynchronisation therapy (CRT, biventricular pacemaker), implantable cardioverter defibrillator (ICD) and in the acute setting perhaps, left ventricular assist device (LVAD). Those offering this service must ensure standardised referral streams are easily accessible and that all healthcare professionals within each health economy involved in the management of heart failure patients are aware of the indications for such therapy. It is incumbent on those offering device therapies to offer a comprehensive service beyond just the implant procedure itself. This must include: • Patient education, consultation and support before, during and after implant. • Patient follow-up; by appropriately experienced cardiac physiologists and by heart failure
specialists, to include further assessment and management of any patient in whom significant improvement is not seen.
At present patients are referred to South Manchester University Hospitals NHS Trust, the regional transplant centre, for assessment with regard to cardiac transplantation. Patients attend South Manchester frequently for standard follow-up pre and post transplantation. It is proposed that the Heart Failure Specialist Team at the Lancashire Cardiac Centre, in close contact with the transplant team in South Manchester, offer assessment and support to these patients closer to home. Specialists in the management of heart failure based in a tertiary centre must facilitate the optimal management of all patients through staff education and supporting research throughout Lancashire and Cumbria.
96
Recommendations All providers should ensure robust systems of diagnosis and management of heart failure are implemented by: 1. It is recommended that validation of registers within GP practices in primary care are
undertaken and that routine screening for symptomatic heart failure patients be part of all long term chronic disease management clinics.
2. Robust coding and diagnostic reporting systems provided by secondary care that support
practices readily identify those patients with heart failure should be established.
3. Two-way communication links, including data and IT links, to allow transfer of information between providers in both the primary and secondary care settings should be established.
4. Readily accessible referral streams to and from a higher level care aligned with the Map of
Medicine pathways implemented within primary care are established.
5. Ensure safe and appropriate optimisation of medication, regular and comprehensive follow-up of the stable patient ensuring early identification of the need for up-regulation of care to be provided in primary care. Patients should be reviewed on a six monthly basis.
6. All practices should have access to specialist heart failure services for diagnosis, either
secondary care or primary care (GPwSI) based, utilising a heart failure diagnostic one-stop clinic model and also to support those patients requiring a higher level of care than that provided at practice level.
7. Cardiac rehabilitation programmes should be accessible to all heart failure patients.
8. The Gold Standards Framework for End of Life should be implemented within each health
economy and robust arrangements for timely switch off of ICD devices must be in place. Systems assessing those patients in hospital at EOL to arrange timely and accessible transfer of the patient to their preferred place of care is required.
9. All acute trust based services should be compliant with the National Heart Failure Database
requirements
10. Acute trusts should provide ready access to echocardiography for all patients admitted with acute heart failure, and provide a comprehensive management plan at discharge, communicated to the patient and General Practitioner as a Advancing Quality requirement
11. Acute trusts developing device implantation services should ensure accessible standardised
referral pathways are implemented and that patient support, advice and education is provided. Robust patient follow up by specialist cardiac physiologists and Cardiologists to ensure optimisation of device and clinical management is achieved
12. Consider tertiary service development to locally provide care for pre and post cardiac
transplant patients in collaboration with South Manchester University Hospitals NHS Trust as part of any north west service development model.
97


ADULT CONGENITAL HEART DISEASE
Introduction Congenital heart disease describes a range of heart conditions resulting from an abnormality of the heart structure or function that is present from birth. It has been estimated that eight out of every 1,000 babies born have a heart defect although some of these will not need any treatment or surgery. The majority of conditions are diagnosed in infancy or early childhood but occasionally it is not found until adulthood. The American College of Cardiology has produced a Bethesda classification system122 which classifies adult congenital heart disease (ACHD) into three categories according to severity: simple, moderate and complex. There are around 135,000 young people and adults currently living in England with congenital heart disease. Due to the improvements in surgical interventions and medical practice more children with congenital heart disease are surviving into adulthood, although not all patients are having the regular medical reviews that are recommended by the Department of Health. It has now been established that there are more adults than children with congenital heart disease. Up to one-third of those with more complex problems will require further intervention later in life.123 Using the Department of Health forecasting model, the ACHD prevalence in North West England and North Wales population (including Isle of Man) can be subdivided into simple, moderate and complex conditions.123 It has been estimated that there will be approximately 22,600 adults in the region by 2010/11. This is based on birth prevalence and survival rates, and includes 10% of new cases diagnosed in adulthood.
ACHD ESTIMATED PREVALENCE IN THE REGION
2007/08
2010/11
Transition
Newly Diagnosed
Simple 10,418 10,903 146 16 Moderate 8,293 8,768 142 16 Complex 2,795 2.988 58 6 Total 21.507 22,659 346 38 Services for children with congenital heart disease are well established and are available throughout the country. In 2006 the Department of Health issued a document providing advice and guidance so that NHS services could be organised to improve the quality of care for adults with congenital heart disease. The document clearly states that “all adults with congenital heart disease whatever the level of complexity are seen by an expert from a specialist centre at least once and receive a written care plan” 123. ACHD specialist ‘hub and spoke’ services are being developed for patients in the North West of England and North Wales. The specialist centre (hub) is in Manchester with local centres (spokes) being developed in Lancashire, Merseyside and North Wales to provide local specialist services. Each centre will be staffed by a multi-disciplinary team of experts in diagnosing and treating ACHD patients. District general hospitals will also play a role in supporting this new service by providing diagnostic tests nearer to home and by looking after patients who have a written care plan under a shared care arrangement with the hub or spoke hospital.
98
National Guidance The National Service Framework for Coronary Heart Disease61 was published in March 2000 and considerable progress has been made in prevention, treatment, quality of care and access to care in this important area of heart disease. One topic that the Framework did not address was that of congenital heart disease. Historically, services for ACHD have been somewhat fragmented and the experiences of families as they pass through the transition from paediatric to adult services have been less than ideal. ACHD patient groups are quite clear that they wish to see better organisation of services, including a concentration of expertise, so that clinical services can properly meet the complex needs of such patients. At the same time, attention needs to be paid to the detail so that generic care such as anticoagulant control can be delivered close to home.
A Commissioning Guide for Services for Young People and Grown Ups with Congenital Heart Disease (GUCH) was published by the Department of Health in May 2006. 124 This document aims to assist commissioners of NHS services in monitoring, planning and developing services, and inform patient expectations focusing on the following key points:
• The number of adults with congenital heart disease is increasing and now exceeds the number of children.
• Adult patients need a more cohesive service, which recognises that congenital heart disease is a life long condition, which affects quality of life.
• To achieve this more cohesive service, the suggested direction of travel involves concentrating expertise in a small number of specialist centres and developing shared care arrangements between these specialist centres and more local centres.
The document also suggests indicators of high quality care to enable local planning, assessment and improvement of services, including: transition between children's and adult services; specialist and local centres (i.e. hub and spokes), primary care, oral healthcare, obstetric care and people with learning disabilities or other special needs123.
Local Service Provision
Currently, there is an under-developed system of local ACHD delivery across Lancashire and Cumbria. Much of this stems from the historically low availability of facilities and staff for ACHD care, as well as a lack of clear pathways, protocols and guidelines to promote seamless, consistent and equitable management across organisational boundaries. It is recognised that arrangements outside of the ACHD Hub is fragmented between a number of different providers, which is not sustainable clinically or financially in the long term. Current service provision arrangements for ACHD patients in this region are predominantly provided from Central Manchester & Manchester Children’s/Manchester Royal Infirmary – the designated specialist ACHD Hub, and from Liverpool Heart & Chest Hospital. Local ACHD outpatient clinics have recently been set up within Blackpool, Fylde & Wyre Hospital, which are accessed by a relatively small number of ACHD patients, led by adult cardiologist with a special interest in ACHD. There are no local ACHD inpatient services in the region, with these services being provided in an unplanned way and with ad hoc treatment decisions being made on a case-by-case basis. Additionally, South Manchester University Hospital, Wrightington, Wigan and Leigh Hospital, and Pennine Acute Hospitals provide cardiac care for ACHD patients from the Lancashire and Cumbria region. However, there are general Cardiologists in local district general hospitals in the area who carry out a small caseload of ACHD patients, but are not yet routinely reported.
99

Gap Analysis In order to address the current service gap, Specialised Commissioners sought support from the four Cardiac and Stroke Networks in the North West to progress the development of a suitable North West ‘hub and spoke’ service model for ACHD. The North Wales Cardiac Network has been working with the North West Networks over the last 12 months to develop this service model. In response to the Department of Health commissioning guidance in England (2006) and the Updated CHD NSF Standard 7 in Wales (2008) for services for adults with congenital heart disease, first steps have been undertaken by the ACHD Implementation Group to support the development of the hub and spoke model. The process to develop an ACHD service specification and identification of spokes was initiated in response to a number of factors facing the North West and North Wales ACHD service model: • The need to develop ACHD hub and spokes to effectively manage the projected growing
number of adult patients with congenital heart disease. • The recognised need to support local designation of hub and spokes which responds to local
and national agenda and strengthen the North West and North Wales position nationally. • The need to ensure local planning, commissioning and delivery of all ACHD specialist services
meets the needs of patients by providing the most appropriate level of care across hub and spokes.
• The need to support the delivery of equitable, locally accessible ACHD specialist services in spokes to cater for changes and growth in the service user population now and in the future.
The Options Appraisal exercise undertaken scored different options available to identify the number of Spokes, their site locations and sequence of development. A preferred option for four Spokes across the North West and North Wales, in order to provide equitable access for this group of patients, was produced: • Manchester Royal Infirmary (MRI), the designated specialist Hub, should be developed to co-
ordinate all spoke services for the Greater Manchester and Cheshire Cardiac Network footprint. MRI would operate as a host organisation collaboratively delivering ACHD services from one site utilising existing staff who have ACHD clinical expertise and currently work for other Trusts in Greater Manchester. This is considered to be the best option to (1) optimise clinical governance arrangements; maximise effective deployment of specialist ACHD resources and utilise existing ACHD expertise; and improve patient access, (2) given the centrality of this site and ease of geographical access from all parts of the network area, and (3) strengthen the North West case for national designation.
• Develop Blackpool Fylde and Wyre Hospital NHS Trust, Liverpool Heart and Chest Hospital NHS Trust, and North Wales NHS Trust at the Glan Clwyd Hospital as the ACHD spoke centres for their Cardiac Network footprint.
Development of this service model will: • Provide the highest possible quality care to adult patients with congenital heart defects across
the whole region. Care should be delivered in an environment, which is appropriate to the complexity of their condition, but still be as close to their home as possible.
• Ensure equity of access to care across the region • Provide a forum for training for medical staff and allied health care professionals • Enhance strategic planning for future needs • Provide a forum for patients to influence planning of their services
100

Additional work to support the implementation and delivery of the hub and spoke model includes: establishment of an educational and workforce development programme; development of a service evaluation and audit framework; development of ACHD patient and carer information and communication; and the development of a multi-site intranet/ web-based ACHD database across hub and spokes in the first instance. ACHD Recommendation 1. Cumbria and Lancashire should contribute to the work of the North West, Isle of Man and North
Wales Adult Congenital Heart Disease Implementation Group to ensure the implementation of the agreed Hub & Spoke model for ACHD
101
Cardiac and Stroke Networks in Lancashire & Cumbria
APPENDIX 1
Current/Future Cardiac Imaging Pathways
The following standards need to be developed for all aspects of the Imaging Strategy: • Image storage and access • Multi Disciplinary Team environments to be established
• Clinical Governance – standards for service development for all modalities
These maps have been aligned to the map of medicine pathways where available. Map of medicine pathways allow localisation of pathways, enable PCTs to attach referral forms and guidance and contain information regarding the procedures highlighted and clinical conditions associated with this chapter of the strategy.
Map of Medicine Key: Green – Primary Care Blue – Secondary Care Diagonal - Primary or Secondary Care This relates to where the diagnostic is requested, not where performed
102

Cardiac and Stroke Networks in Lancashire & Cumbria
Current/Future Cardiac Imaging Pathways
ECG
Chronic chest pain
(suspected CAD)
ETT
Stress Echo
MPI
MR
CT
Angiography
Unsuitable and inappropriate
for ETT
Suitable and
appropriate for ETT
Improvement in pathway; With increasing use of non-invasive highly specific diagnostics, the use of invasive diagnostic angiography activity may decrease
Map of Medicine Pathway for suspected angina is currently under review It was removed February 09
Patients unsuitable for ETT include • Inability to exercise • LBBB • Advanced age • Pre-menopausal women
103
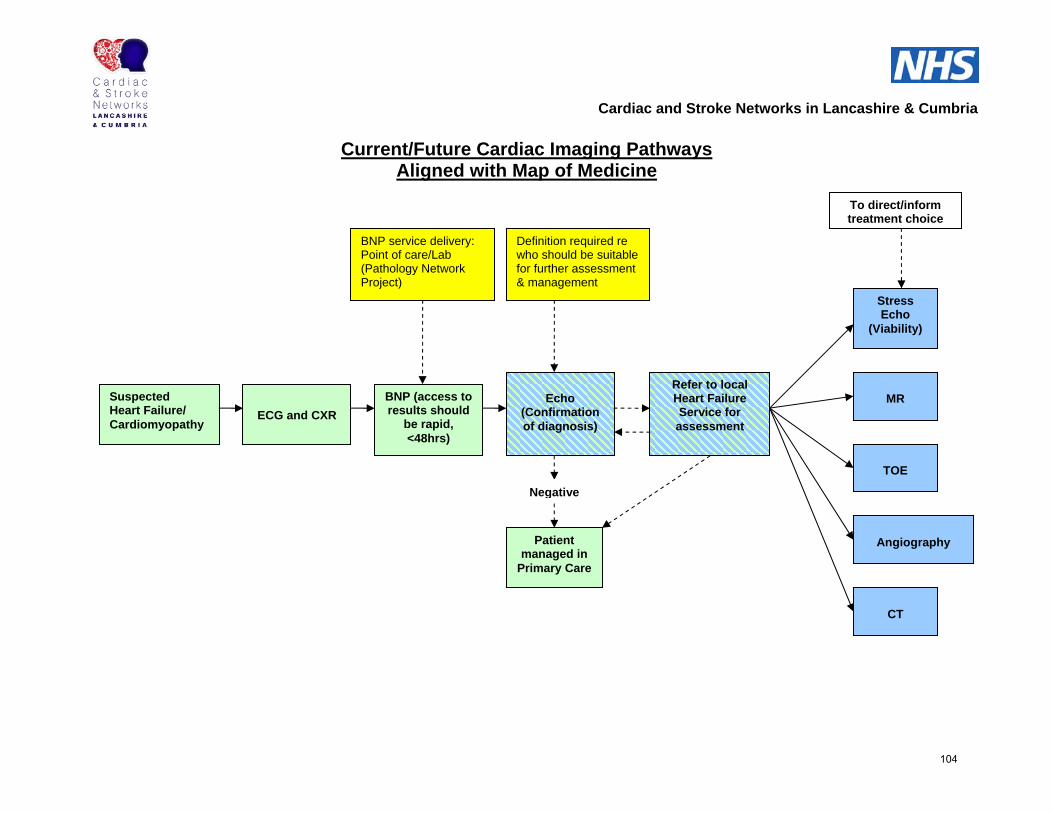
Cardiac and Stroke Networks in Lancashire & Cumbria
Current/Future Cardiac Imaging Pathways
Aligned with Map of Medicine
To direct/inform treatment choice
Suspected Heart Failure/ Cardiomyopathy
ECG and CXR
BNP (access to results should
be rapid, <48hrs)
Echo (Confirmation of diagnosis)
Stress Echo
(Viability)
MR
TOE
CT
Refer to localHeart Failure Service for assessment
Angiography Patient
managed in Primary Care
Negative
BNP service delivery: Point of care/Lab (Pathology Network Project)
Definition required re who should be suitable for further assessment & management
104

Cardiac and Stroke Networks in Lancashire & Cumbria
Current/Future Cardiac Imaging Pathways Aligned with Map of Medicine
To direct / inform treatment choice
ECG – CXR if symptomatic
Echo
Angiography
MR
CT
Stress Echo Refer to
Cardiology
Reassess if symptomatic
Negative
Primary Care
ETT
TOE
Murmurs/ Suspected
Valvular Heart Disease
105
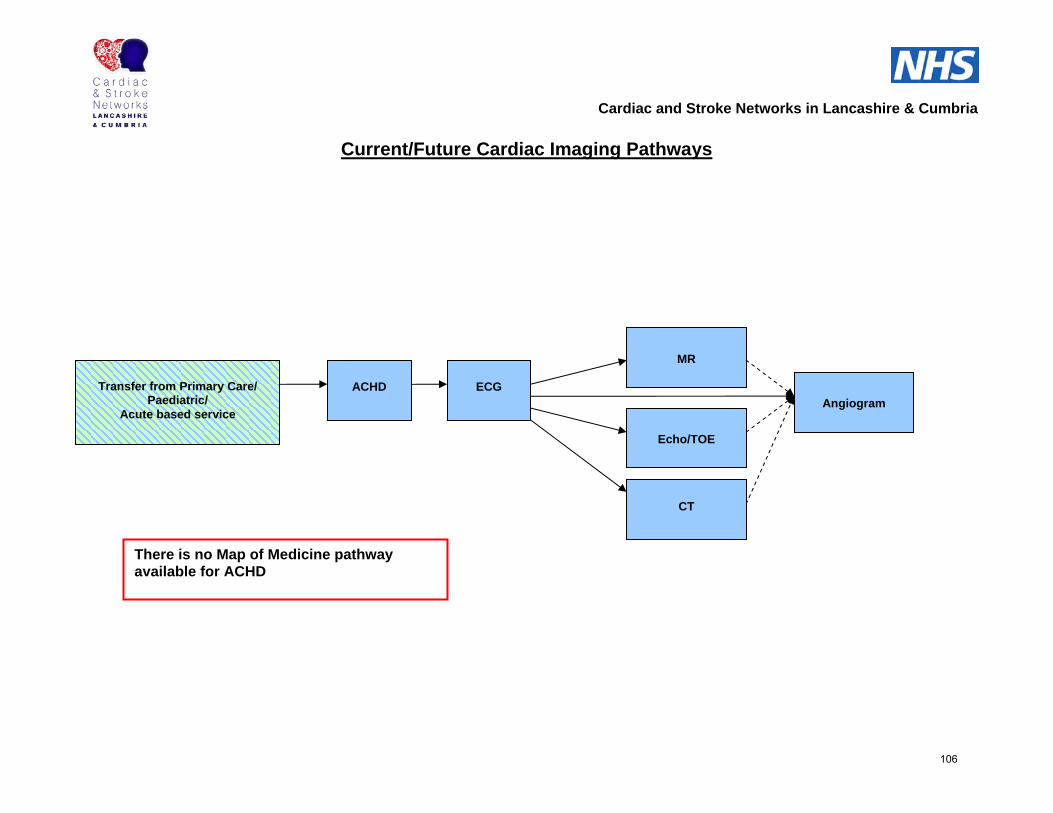
Cardiac and Stroke Networks in Lancashire & Cumbria
Current/Future Cardiac Imaging Pathways
There is no Map of Medicine pathway available for ACHD
CT
Echo/TOE
MR
MR
Angiogram
ACHD
ECG
Transfer from Primary Care/
Paediatric/ Acute based service
106
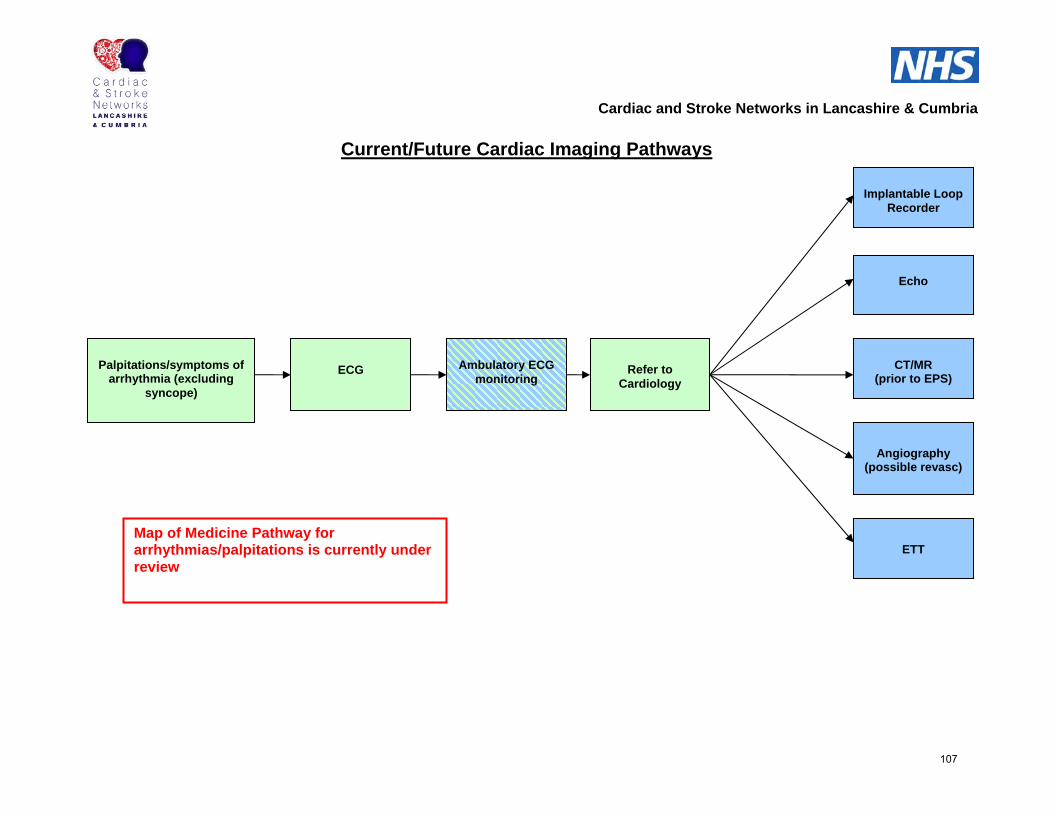
Cardiac and Stroke Networks in Lancashire & Cumbria
Current/Future Cardiac Imaging Pathways
Map of Medicine Pathway for arrhythmias/palpitations is currently under review
Echo
CT/MR
(prior to EPS)
Angiography
(possible revasc)
ECG Ambulatory ECG
monitoring
Palpitations/symptoms of
arrhythmia (excluding syncope)
ETT
Refer to
Cardiology
Implantable Loop Recorder
107
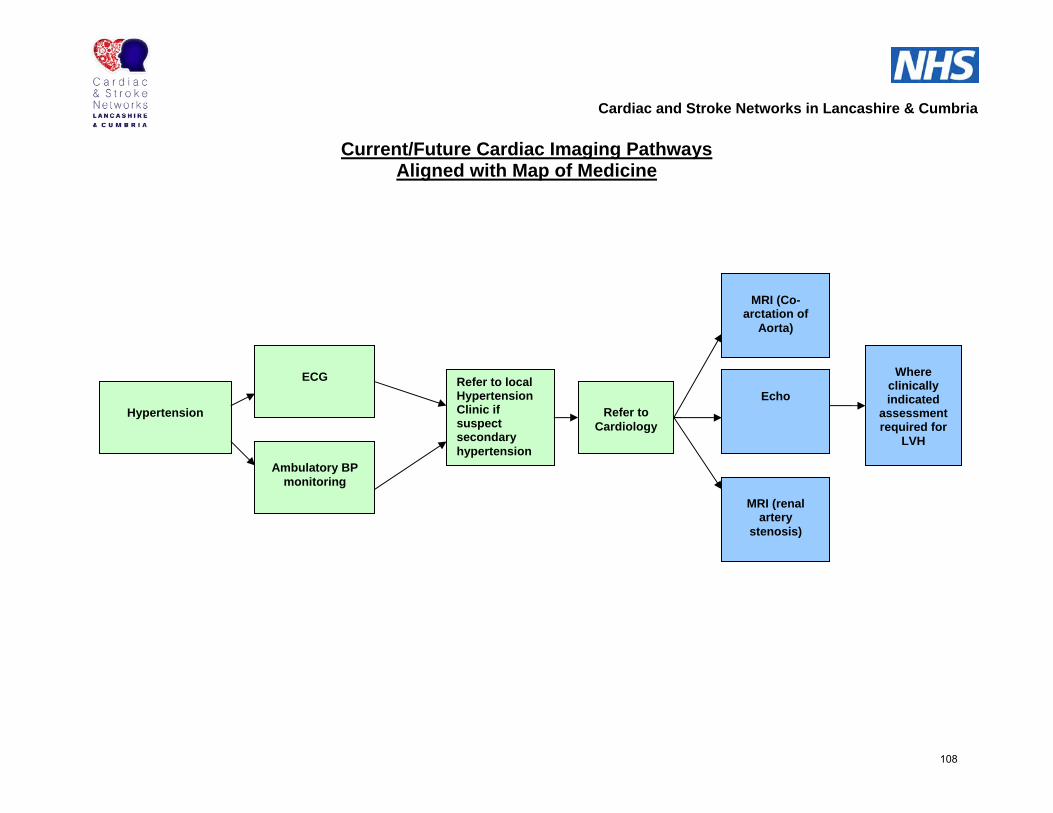
Cardiac and Stroke Networks in Lancashire & Cumbria
Current/Future Cardiac Imaging Pathways
Aligned with Map of Medicine
ECG
Ambulatory BP
monitoring
Hypertension
Refer to local Hypertension Clinic if suspect secondary hypertension
Echo
MRI (Co-arctation of
Aorta)
MRI (renal artery
stenosis)
Where clinically indicated
assessment required for
LVH
Refer to
Cardiology
108

Cardiac and Stroke Networks in Lancashire & Cumbria
Current/Future Cardiac Imaging Pathways
Aligned with Map of Medicine
Echo
CSM
Tilt Testing
ECG
Syncope
ETT
Refer to
Cardiology
ILR
109

APPENDIX 2 Criteria for Referral for Imaging Modalities Echocardiography The following patient groups should be considered for Stress Echocardiography and these include: • Those patients who require assessment of the presence and degree of coronary artery
obstruction in patients with suspected coronary artery disease ° When Exercise Tolerance (treadmill) Testing is inconclusive ° When the patient is unable to undertake treadmill testing e.g. mobility problems ° When resting ECG changes would make Exercise tolerance testing ECG interpretation
difficult e.g. LBBB, LVH • Aid management of patients with known or suspected coronary artery disease
° For risk stratification e.g. post MI or prior to non cardiac surgery ° To give guidance of revascularisation procedure ° For the assessment of adequacy of revascularisation procedure ° To assess myocardial viability and hibernation especially with reference to planned
myocardial revascularisation Cardiac MR (CMR) The list below is presently used for locally in MR.
1. Guch follow-up co-aoratation patients 2. Myocardial viability post infarct – sufficient myocardium to justify surgery for either bypass
of LV re-viability 3. Myocardial hydration/viability pre angioplasty/CABG 4. Problem solving
• Cardiac mass • Chamber thrombosis • ?coronary artery fistula • Assessment of difficult cardiac tumours • Pericardiac assessment – may require CT • Valvular assessment • Follow up of patients with aortic dissection • Assessment of cardiac myopathy •
National guidance from BSMR & BSI will be published later in the year. This information will be updated in accordance. Myocardial Perfusion Imaging (MPI) • Those patients who require assessment of the presence and degree of coronary artery
obstruction in patients with suspected coronary artery disease ° When Exercise Tolerance (treadmill) Testing is inconclusive ° When the patient is unable to undertake treadmill testing e.g. mobility problems ° When resting ECG changes would make Exercise tolerance testing ECG interpretation difficult e.g. LBBB, LVH
110
° As part of an investigational strategy for the diagnosis of suspected CAD in people with a low to moderate likelihood of CAD and of future cardiac events (Radionucleide MPI has a greater sensitivity for CAD than exercise ECG)
• To aid the management of patients with known coronary disease
° To determine the likelihood of future coronary events, for instance after myocardial infarction or related to proposed non-cardiac surgery
° To guide strategies of myocardial revascularisation by determining the haemodynamic significance of coronary lesions
° To assess the adequacy of percutaneous and surgical revascularisation ° To assess myocardial viability and hibernation, particularly with reference to planned
myocardial revascularisation • Special indications
° E.g. to assess the haemodynamic significance of known or suspected anomalous coronary arteries and muscle bridging
Cardiac Computed Tomography The following patient groups are suitable for cardiac Computed Tomography and should be considered for referral for this modality. • CT Coronary angiography
CT coronary angiography has been seen to have a high negative predictive value, thus may be used to avoid invasive coronary angiography in patients being assessed for cardiomyopathy, pre-surgical assessment of patients undergoing aortic valve surgery and suspected aberrant course of the coronary arteries. CT coronary angiography is being used increasingly in the assessment of patients presenting with atypical thoracic chest pain with a low to intermediate or intermediate risk and an inconclusive Exercise Treadmill test.
• Triple rule out Triple rule out refers to the fact that patients presenting with unexplained chest pain may be assessed by thoracic CT to assess the coronary arteries, to exclude thoracic dissection and to exclude pulmonary embolism.
• Coronary artery bypass graft assessment Up to 30% of patients have repeat symptoms of chest pain and possible recurrent angina within one year of CABG which may be secondary to a blocked graft or progressive atherosclerosis. During this procedure, the field of view is increased to include the lung apices down to the diaphragm. This allows a rapid outpatient assessment of CABGs, clearly demonstrating whether a graft is patent or not. It may also reduce the possible radiation dose to the patient that may occur at the time of catheterisation if grafts cannot be cannulated easily. In addition pre-surgical assessment of graft position may be useful to avoid surgical trauma during sternotomy procedures.
• Pre-thoracic aortic surgical assessment This allows assessment of the aortic dimensions, extent of aortic disease and wall calcification for siting of grafts and arterial clamping. It may also be of use when planning for percutaneous aortic valve repair.
• Quantification and cardiac myocardial viability imaging Cardiac CT can be used to assess perfusion, viability and function as well as to define abnormal myocardium in Acute Myocardial Infarction (AMI)
111
APPENDIX 3
British Society of Echocardiography Affiliated to the British Cardiac Society
Departmental Accreditation 02.2008
The British Society of Echocardiography (“BSE”) is offering any Echocardiography Department in the UK (“Department”) the opportunity to apply for accreditation in accordance with these guidelines (“Applicant”). The BSE grants such accreditation on a purely voluntary basis (“Accreditation”). There may be other Departments which have not sought Accreditation but which offer an excellent echocardiography service. The decision of the BSE to grant accreditation to a Department is only an indication of the BSE’s opinion of the standard of that Department. The BSE does not intend the outcome of the Departmental Accreditation process to be relied upon by any person under any circumstance. This shall include, but not be limited to, any Department, any individual medical practitioner, including GPs, any patient, referring health authority and any member of the public. The Accreditation shall be based on sufficient information being provided to the BSE by Applicants in accordance with Appendix A and/or, as the case may be, as a result of an inspection of a Department. 1 Introduction 1.1 The BSE cannot guarantee, or be liable in respect of, the quality, efficacy or performance of an Applicant and/or Department either prior to Accreditation or otherwise. 1.2 Accreditation of an Applicant or Department shall be determined by all relevant information provided by such Applicant or Department and it is the responsibility of that Applicant or Department to ensure that such information is accurate and up-to-date. The BSE shall not be liable in respect of any decisions made based on such information received. 1.3 A process for accreditation in adult echocardiography has been in place since 1994 and for transoesophageal echocardiography since 2003. 1.4 However, accreditation of individual echocardiographers alone cannot guarantee a high quality Department. It is also necessary to have adequate machines, management and organisation. 1.5 The assessment of cardiac departments as a whole already occurs as part of the British Cardiac Society’s (“BCS”) Peer Review scheme. More detailed accreditation of Departments could provide the following advantages: 1.5.1 To devolve echocardiographic control giving more local autonomy 1.5.2 To empower an increasing number of Departments to mark log-books and videos for adult accreditation thus accelerating the process and also bringing it more into line with European practice 1.5.3 To facilitate the negotiation of contracts with commissioners and bodies such as Primary Care Trusts 1.5.4 To certify non-cardiac practitioners (e.g. GPwSI, PwSI, nurses) and maintain quality control and continued learning 1.5.5 To encourage improvements in standard by comparison against a nationally-agreed yard-stick 1.6 Departmental Accreditation may be applied for in respect of the following four modules: 1.6.1 Transthoracic echocardiography 1.6.2 Transoesophageal echocardiography 1.6.3 Stress echocardiography 1.6.4 Training to BSE adult proficiency standard
112

If the Department is carrying out any Transoesophageal Echocardiogram (“TOE”) or Dobutamine Stress Echocardiogram (“DSE”) then the relevant module form must be
completed irrespective of whether specific accreditation in these areas is being sought. 1.7 Recommendations in respect of the standards required for each of these modules are given in sections 3-6. It should be noted that the recommendations contained in section 3- 6 below are guidance only and that the standards required for each of the modules may be subject to change at the discretion of the BSE. 1.8 The standards to which the Departments will be compared against are set out below in the separate section ‘Criteria for Grading’. There are two levels of grading: standard and
advanced. To achieve advanced Accreditation, all aspects of a Department’s work must be accredited at standard level and the requirements for advanced transthoracic accreditation met. Standard Accreditation fulfils the basic requirements for an adequate echo service, while advanced accreditation offers a higher level of service including more rigorous quality control.
Please note that, as stated above, Departmental Accreditation is a voluntary process. Whilst the BSE is keen to work with Departments to help them achieve these standards and does not expect all departments to reach all standards in all areas, it has the ultimate discretion as to whether to accredit a Department.
1.9 Throughout this document, the term ‘sonographer’ is used to mean a non-medical echocardiographer and subsumes the terms clinical physiologist, cardiac or echocardiography technician and radiographer. 1.10 It should be noted that Echocardiography is changing rapidly and it is expected that this document will be reviewed in response to developments including screening
echocardiography, portable systems, agenda for change and the training of GPwSI and other non-cardiologists in echocardiography. This document should therefore only be viewed as a general guide and the guidance and criteria for Accreditation contained in this document may be subject to change at the ultimate discretion of the BSE.
1.11 The registration fee for Departmental Accreditation is £500. These fees will cover the cost of administration and also of organising accreditation visits where applicable. 2 Process 2.1 The Applicant completes an application form, in substantially the same format as set out in Appendix A, and pays a non-refundable registration fee. 2.2 The BSE Accreditation Committee assesses the application against the standards set out
in the ‘Criteria for Grading’ section below and decides whether the institution deserves Accreditation and to what level. If it is felt that an Inspection is needed in order to clarify or confirm information supplied on the application form, this will be undertaken at a mutually agreeable time. It should be noted that BSE has the ultimate discretion as to whether to inspect and also to decide whether a department deserves Accreditation. The ‘Criteria for Grading’ set out below should be viewed as guidance only.
2.3 The Applicant is informed whether or not Accreditation is awarded and at which level for
each of the specialty areas for which it has been requested. 2.4 A Department can claim BSE Accreditation for those areas in which BSE is of the opinion
that it has reached the required standard e.g. ‘BSE-Accredited department for the provision of transthoracic echocardiography in adults and for training to BSE adult proficiency level’.
2.5 An unsuccessful Applicant may be notified of the areas requiring improvement and invited
to reapply when these have been addressed. The BSE will use its best endeavours to offer advice and support to help achieve this. An unsuccessful applicant may Appeal the decision of the Accreditation Committee on the grounds, and following the process set out in section 8.
2.6 Inspection of an Accredited Department may be performed as part of the BCS peer review
113

process or on a random basis following reasonable notice by the BSE (see section 7). Following inspection, a Department will be assessed as satisfactory or unsatisfactory in the areas in which it has been accredited. An ‘unsatisfactory’ department will be given up to 12 months, during which time its Accreditation may be suspended, to remedy areas of concern. Failure to demonstrate the required improvement will result in loss of Accreditation.
2.7 A department whose Accreditation has been suspended or removed may appeal the decision, following the procedure laid down in section 8. 2.8 Accreditation lasts for 5 years, and can then be re-applied for. 2.9 If there is a change of Technical or Clinical Head of Department during an Accreditation period, the BSE should be informed within 6 months. 2.10 The BSE has the right to suspend a Department’s accredited status under the following circumstances: 2.10.1 In accordance with section 2.6 above, if following inspection, a Department is assessed as unsatisfactory in the areas in which it has been accredited; 2.10.2 If it has reason to believe that that the safety of the public, or the public interest is seriously endangered. The BSE may suspend a Department while it decides whether or not to withdraw approval, where it has decided to withdraw approval but before the decision takes effect, or while any appeal is pending; 2.10.3 If it believes that its reputation is being damaged or likely to be damaged in any way whatsoever as a result of Accreditation of a Department; 2.10.4 If a Department or any member of such Department is subject to any investigation, formal
or otherwise; or 2.10.5 If it does not reasonably consider a Department to be worthy of Accreditation, for any
reason whatsoever. 2.11 The BSE may remove a Department’s accredited status in the following circumstances: 2.11.1 In accordance with section 2.6 above, if following inspection, a Department is assessed as unsatisfactory in the areas in which it has been accredited and is consequently suspended, and it fails to remedy the areas of concern within 12 months; 2.11.2 If it has reason to believe that that the safety of the public, or the public interest is seriously endangered; 2.11.3 If it believes that its reputation is being damaged or likely to be damaged in any way whatsoever as a result of Accreditation of a Department; 2.11.3 If a Department or any member of such Department is subject to any investigation, formal
or otherwise; or 2.11.4 If it does not reasonably consider a department to be worthy of Accreditation, for any r
reason whatsoever. 2.12 The BSE shall comply with the provisions of the Data Protection Act 1998 (“DPA”) and, to the extent that it is a Data Processor (which has the meaning given to it under the DPA), it shall put in place: 2.12.1 Appropriate technical and organisational measures against the processing of Personal Data (which has the meaning given to it under the DPA) and against unauthorised, accidental or unlawful access to the Personal Data (having regard to the state of technological development and the costs of implementing any such measures) as well as reasonable security programmes and procedures for the purpose of ensuring that only authorised personnel have access to the Personal Data processing equipment and that any persons whom it authorises to have access to the Personal Data shall respect and maintain due confidentiality;
114

2.12.2 A level of security programmes and procedures which reflect: (a) the level of damage which may be suffered by a Data Subject (which has the meaning given to it under the DPA) to whom the Personal Data relates as a result of unauthorised or unlawful possession of the Personal Data; and (b) the state of technological development and the costs of implementing such procedures and programmes; and 2.12.3 As required by the DPA, such security programmes and procedures which specifically address the nature of any Sensitive Personal Data (which has the meaning given to it
under the DPA). 2.13 The Applicant acknowledges that it shall comply with the relevant data protection statement as set out in Appendix A. 3 Standard 1 -Transthoracic Echocardiography 3.1 Recommendations for staffing and training. 3.1.1 All centres should have both a specialist Technical and Clinical Head of Department. 3.1.2 The Clinical Head should have specialist echocardiographic training and ideally hold individual Accreditation. His/her job description should include setting clinical guidelines and policy, performing studies, training doctors and sonographers, audit, clinical meetings and quality control. He/she should set up a system for reviewing requests and reports, and urgent clinical review in response to findings at echocardiography. In a District General Hospital performing 3000 studies per year, at least one session per week should usually be allocated directly to echocardiography. 3.1.3 The Technical Head should be responsible for performing studies, audit, service improvement, training doctors and sonographers and liaising with Occupational Health and the Works Department. The Technical Head should hold BSE accreditation and be graded at least Band 7. 3.1.4 Sonographers performing and reporting studies unsupervised should be BSE accredited and at least band 6 and typically band 7. 3.1.5 Continuing education should be provided (and funded) to fulfil BSE re-accreditation requirements or to a similar level. There should be a small library of relevant reference textbooks within the Department. 3.1.6 The job profile of a sonographer includes training, self-education, audit, and quality control in addition to performing echocardiograms. 3.2 Recommendations for organisation and equipment. 3.2.1 Echo rooms used for inpatients on beds should be at least 20 m2 in area 3.2.2 Ventilation, heating, lighting and ancillary facilities must be appropriate (see Appendix A) 3.2.3 Echo machines must have the capacity for imaging including second harmonic imaging, colour mapping, pulsed Doppler and both steerable and stand-alone continuous wave Doppler. Ideally tissue Doppler should also be available. 3.2.4 A single echo machine can handle up to a maximum of 2500 studies each year but this figure will be lower if there is a significant ward-based or complex workload 3.2.5 The machine should be serviced regularly, and be replaced or have a major upgrade at least every 5 years 3.2.6 There must be consideration of patient comfort, privacy, dignity and provision of adequate information
115
3.2.7 There must be awareness of health and safety issues especially relating to back and eye problems and adequate liaison with occupational health and risk management departments (see appendix B) 3.2.8 A report database should exist, with facilities for storing and retrieving specific echo studies. 3.2.9 A separate viewing room is recommended for reviewing studies and off-line reporting 3.2.10 There should be appropriate storage space 3.2.11 A patient information leaflet should be available 3.3 Recommendations for performing studies. 3.3.1 A standard transthoracic study (one TTE equivalent) takes 30 minutes. Training may prolong this to 45 minutes (1.5 TTE equivalents). A complex study (e.g. including contrast injection or detailed valve haemodynamic assessment) may take up to 1 hour (two TTE equivalents). As an ideal, allowing for all aspects of the job profile, a sonographer will perform no more than 2000 studies per year 3.3.2 A list of indications for echocardiograms should be agreed 3.3.3 Prioritising and filtering, of inappropriate requests should be performed by sonographers supported by the Clinical Head 3.3.4 Minimum standards for studies should be established. Study protocols appropriate to specific clinical conditions should be established 3.3.5 A format for reports should be established, including who should issue conclusions and who is qualified to sign reports 3.3.6 The requirements of the Data Protection Act 1998 must be complied with regarding data storage 3.3.7 Reports from routine studies should usually be issued on the day of the examination. For urgent or inpatient studies, at least a preliminary report should usually be issued immediately. 3.3.8 A mechanism must be in place for reporting cases that require urgent clinical attention. 3.3.9 Regular meetings, ideally weekly, should be held to review unusual, challenging or otherwise difficult cases. 3.3.10 A formal quality assurance system should be in place with regular blind over reading of selected studies to ensure consistency of performance and interpretation. Meetings should take place at least 4 times per year with all echocardiographers attending at least 50%. 4 Standard 2 -Transoesophageal Echocardiography (TOE) All the standards for transthoracic echocardiography in addition to the following: 4.1 Recommendations for staffing and training. 4.1.1 All centres should have a designated Head of TOE. This will usually be the Clinical Head of Echocardiography 4.1.2 Outpatient TOE studies require an operator with appropriate training, a cardiac-trained nurse with experience in managing airways and, ideally, sonographers 4.1.3 Continuing education must be provided for the operators
116

4.1.4 Each operator should perform or directly supervise at least 50 studies per annum 4.1.5 Ideally operators should have BSE/ACTA/EAE TOE accreditation 4.1.6 A list of indications for TOE should be agreed 4.2 Process 4.2.1 Minimum standards for studies should be established and the head of TOE must be responsible for ensuring that all operators adhere to them 4.1.1 A preoperative checklist should be used 4.1.2 Whenever sedation is used, it should be in accordance with the recommendations given in ‘Implementing and Ensuring Safe Sedation Practice for Healthcare Procedures in Adults’ published by the Academy of the Royal Colleges in 2001 4.1.3 The TOE probe must be checked electrically at a frequency dependent on usage. A log of these checks must be kept 4.1.4 The TOE probe should be cleaned regularly 4.2 Recommendations for organisation and equipment 4.2.1 There should be appropriate provision of: • Room (ideally > 25 m2 in area) • Couch with facility for head-down tilt • Facilities for cleaning and sterilising the probe. • Storage cupboard for the probe • Resuscitation apparatus and drugs • Lockable drug cupboard • Suction • Oxygen • Pulse oximeter • Sphygmomanometer • Facilities for recovery of the patient • Protocols for patient care (example Appendix C). 5 Standard 3 - Stress Echocardiography All the standards for transthoracic echocardiography in addition to the following: 5.1 Recommendations for staffing and training. 5.1.1 All centres should have a designated Head of Stress Echocardiography, normally the Clinical Head of Department 5.1.2 Stress echocardiography studies require an experienced operator and a sonographer or trained nurse 5.1.3 The study reporter must be specially trained in stress echocardiography 5.1.4 There must be a mechanism in place for feedback to assess clinical correlation 5.1.5 Each operator/reporter should perform or directly supervise at least 100 studies per Annum 5.1.6 Continuing education must be provided for the interpreter 5.1.7 At least one member of staff performing the study should possess at least Immediate Life Support (ILS) Training or be a specialist cardiologist 5.1.8 A list of indications for stress echocardiograms should be agreed
117

5.1.9 Appropriate protocols for studies should be established and the Head of Stress Echocardiography must be responsible for ensuring that all operators adhere to them 5.2 Recommendations for organisation and equipment Ideally there should be appropriate provision of • Designated room (size >25 m2) • Stress echocardiography software • Contrast agents and contrast specific software • Infusion syringe for pharmacological stress or equipment for exercise stress e.g. bicycle • ECG monitor and recorder • Sphygmomanometer • Resuscitation apparatus and drugs readily available 6 Standard 4 –Training to BSE Proficiency Standard The centre must be accredited in transthoracic echocardiography at standard level. 6.1 Recommendations for staffing and training 6.1.1 Each centre must have a BSE Accredited individual responsible for training. This person may be from a Clinical or Technical background 6.1.2 Staffing levels and workload appropriate to the number of trainees to ensure adequate clinical capacity. A guide would be two BSE accredited staff and 2000 echoes p.a. for a department to accommodate one trainee 6.1.3 At least one, and ideally two protected tutorial half-day sessions per week for both trainer and trainee 6.1.4 Access for both trainer and trainees to local, national and international meetings 6.1.5 Regular weekly Departmental case review sessions 6.2 Recommendations for equipment 6.2.1 Core library e.g. 3 up to date echo textbooks and 1 general cardiology textbook in the Department and access to cardiology journals electronically or within the hospital 6.2.2 Training material-tapes/CDs/digital cases, etc. 6.2.3 Internet access should be available to all staff 6.3 Performance 6.3.1 History of success in training students to BSE proficiency/similar level 7 Departmental Inspections (“Inspection”) 7.1 Purpose The purpose of an Inspection is solely to determine whether or not information submitted on Accreditation Application Forms is currently accurate. It should be noted that Inspections will be undertaken at the ultimate discretion of BSE.
118
7.1.1 Process 7.1.2 Most Inspections will be randomly selected, but they may also be undertaken if the Department appears to have changed significantly since the original submission. 7.1.3 At least 28 working days’ notice will be given of any Inspection visit. Proposed visits will be re-scheduled only in special circumstances (e.g. Technical Head on leave) 7.1.4 Inspections will normally be undertaken by two people nominated by the BSE Accreditation Committee, one of whom will normally be a doctor who is him/herself a Clinical Head of Echocardiography in a department of similar size, and the other a sonographer who is him/herself a Technical Head of a similar department. 7.1.5 The costs of an Inspection initiated by the BSE will be borne by the society. 7.1.6 Inspectors will bring with them copies of Accreditation Forms submitted, together with any amendments. They will: • Check that equipment and facilities are as claimed • Observe selected patient studies • Check a sample of clinical and technical reports • Interview Clinical and Technical heads of Department, plus approximately one- third of other staff and trainees • Inspect daybooks, appointment diaries, etc. • At the end of the Inspection, hold a meeting with the Clinical and Technical Heads, at which any apparent discrepancies between data on the Accreditation Application and observed practice will be highlighted This list is not exclusive and that Inspections will differ from time to time. 7.2 Assessment 7.2.1 The inspectors will submit a written report of their findings to the BSE Accreditation Committee. After discussion within the Committee, the Chairman will write to the Clinical and Technical Heads of the department concerned. This letter will be sent within 60 days of the Inspection and will offer one of the following conclusions for each category of Accreditation applied for or held: 7.2.1.1 Confirmation of Accreditation at the level already assigned 7.2.1.2 Re-grading of the Department’s rating (see 2.3) 7.2.1.3 Suspension of Accreditation in accordance with section 2.10 above. Suspension will normally be for a period of six months. When the department believes that the deficiencies have been addressed, the Clinical or Technical Head can apply in writing to the Accreditation Committee to request removal of the suspension 7.2.1.4 Removal of Accreditation in accordance with section 2.11 above. In this case a new Application (and accompanying Fee) will have to be made. 7.2.1.5 A certificate signed by the President of the BSE will be provided following grant of any application and indicating the standard achieved in each discipline. 8 Appeals (“Appeals”) 8.1 Where a Department considers that the BSE has unfairly refused, regraded, suspended or removed Accreditation, written appeal to the BSE Council. Appeals may be made only on the following grounds: 8.1.1 That the decision was affected by bias or breach of the Society’s guidelines for Centre Accreditation
119

8.1.2 At an Inspection, the inspectors did not carry out the inspection in accordance with the procedure set out in section 7 8.1.3 That conditions prevailing at the time of the inspection were unusual and temporary (e.g. several key staff off sick) 8.1.4 That information provided to the inspectors was incomplete or inaccurate 8.2 An Appeal will be considered by the BSE Council at its discretion (or a panel nominated by the Council for this purpose and containing at least 3 elected Council members). No member of the Appeal panel shall have taken part in the Inspection, or have any current or past association with the Centre concerned. The findings of the Appeal panel will be sent to the Department within 90 days of the Appeal being lodged and shall be final.
120

APPENDIX 4 Cardiac Rehabilitation Team A comprehensive CR team of appropriately qualified core staff including: a cardiac specialist nurse, physiotherapist, dietician, administrator and a designated clinical lead (cardiologist or GP specialist in cardiology).
The team should also include, where appropriate, referral to a psychologist, pharmacist, occupational therapist and physical activity-exercise specialist. The full CR team should be involved with the development of CR educational materials. The time allocated per professional should be in agreement with the established guidelines. The Agenda for Change bands are a guide to the minimum requirement and may vary locally. The BACR 2009 update clarified that the interpretation and implementation of these recommendations will always be influenced by local resources, the existing profile of staff involved in the specific comprehensive CR teams and referral pathways to other key professional groups. Appendix 1 of the standards states that referral, based on the assessment of patient needs, should be made to appropriate health professionals. If, based on effective CR referral trends and clinical outcomes, service providers feel that their programmes require additional or, in some cases, alternative professional representation within their CR core team then this would be appropriate for that service and not in conflict with the BACR standards. An important caveat is that all CR core team members treating and managing patients should be professionally qualified, work within their professional scope of practice and have evidence-based professionally verified CR education, training and competences aimed at reducing risks to patients undergoing CR and achieving effective sustainable clinical outcomes and patient benefits.
121

APPENDIX 5 Assessment of individual needs The assessment of individual needs should be agreed collectively by the CR team and include all the relevant aspects of the core requirements. The assessment should, at the very least, include the core items of the NACR (Appendix 4). Competent staff should carry out the assessment and appropriate action be taken to ensure prompt intervention and or referral of patients to meet identified needs.
122
APPENDIX 6 Target Patient Population Types of patients suitable for cardiac rehabilitation irrespective of age, sex, ethnic group and condition are: • Coronary heart disease (CHD) • Exertional angina • Acute coronary syndrome (unstable angina or NSTEMI or STEMI) following medical/surgical • management • Before and after revascularisation – Percutaneous revascularisation or surgery • Following any stepwise alteration in CHD condition • Other atherosclerotic disease e.g. peripheral arterial disease • Stable heart failure and cardiomyopathy • Congenital heart disease • Following implantable device interventions
123

APPENDIX 7 Cardiac Rehabilitation Audit The BACR consider registration with the National Audit Cardiac Rehabilitation (NACR) as mandatory. Each CR service should be collecting audit data of individual outcomes for every patient and should be willing to provide this information to the NACR. The BHF Cardiac Care and Education Research group, based at the University of York, are managing the dataset. http://www.cardiacrehabilitation.org.uk/. Assistance is available from the NACR team to overcome IT issues.
124
APPENDIX 8 Cardiac Rehabilitation Budget This can take the form of annually allocated budgets or cost per case tariffs. It should be sufficient to meet CR costs for core staff, referral staff and appropriate resources to deliver a safe and effective service. The budget will, at the very least, have to meet the costs associated with the minimum standards and core components.
125
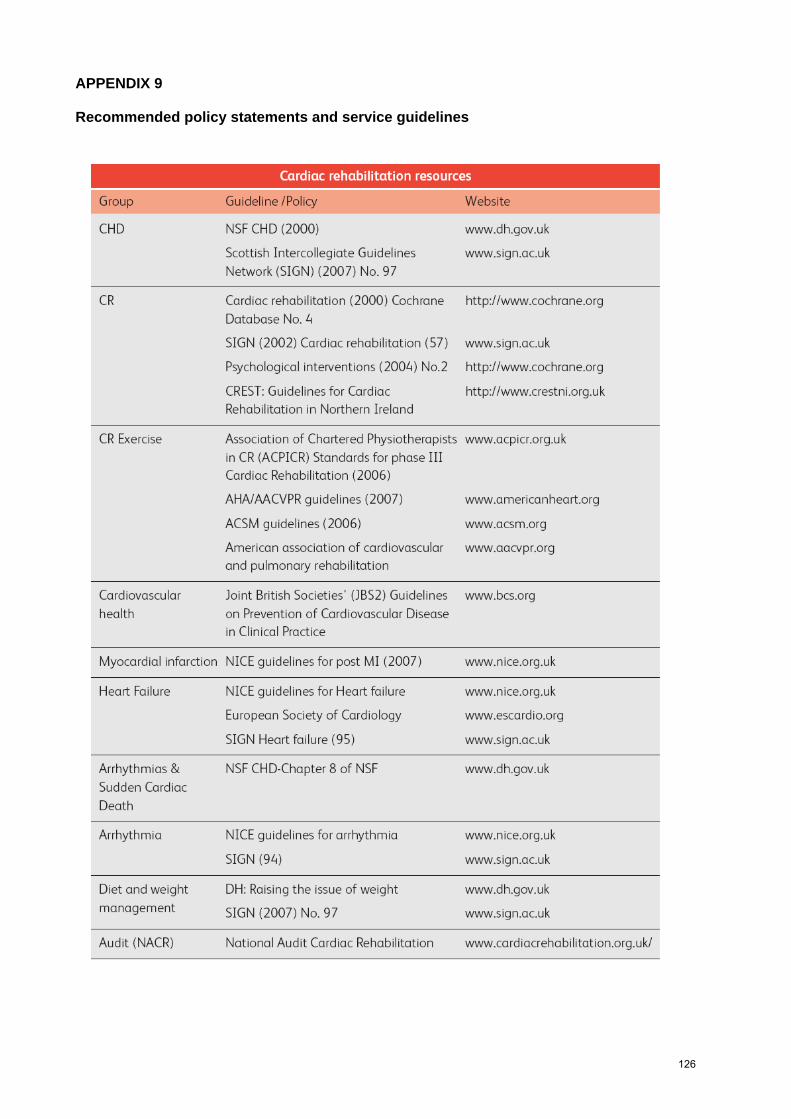
APPENDIX 9 Recommended policy statements and service guidelines
126

Cardiac and Stroke Networks in Lancashire & Cumbria HEART FAILURE STRATEGY
APPENDIX 10
Future technologies that may be applied to all Heart Failure Maps • Image and information transfer/availability between Primary and Secondary Care ensuring all IT systems are linked and accessible by all
healthcare professionals required. • Availability of video conferencing for MDT meetings/advice between healthcare professionals across both Primary and Secondary Care. • Consideration of a one-stop diagnostic Heart Failure clinic, Consultant Heart Failure Specialist, GPwSI led.
Primary Care
Secondary Care
Present state
Future state
KEY
127

Cardiac and Stroke Networks in Lancashire & Cumbria HEART FAILURE STRATEGY
APPENDIX 10
HEART FAILURE – SUSPECTED
Risk factors (2)
Primary prevention in patients at risk (3)
Clinical presentation (4)
Go to cardiovascular risk assessment
Examination (6)
History (5)
Consider differential diagnoses (7)
Alarm features? (8)
Present (9)
Absent (10)
GP surgery/other - Self assessment NYHA questionnaire AF screening, pulse palpation
BNP/Echo
Practice based registers – ensure robust and complete
Use of Telemedicine for ECG interpretation and triggering ECG QRS width on this or other IT system
ECG & BNP – ensure widely adopted
Heart Failure suspected (1)
128

Cardiac and Stroke Networks in Lancashire & Cumbria HEART FAILURE STRATEGY
APPENDIX 10
HEART FAILURE – SUSPECTED (cont)
Investigation (11)
Initial investigations (12)
Refer immediately to A&E (13)
Consider commencing treatment (14)
Refer for echocardiogram (15)
Echocardiogram (16)
Consider additional investigations (17)
Manage according to severity and stage of heart failure (18)
Symptomatic patients with preserved LV systolic function (21)
Symptomatic patients with LV systolic dysfunction (20)
Asymptomatic patients with LV dysfunction on echo (19)
Go to asymptomatic LV dysfunction
Go to symptomatic LV dysfunction
Refer to cardiology
Echo triggered LV function assessment and suitability for CRT device
Echo usually performed – ensure rapid access to echo across the Network
Trigger Heart Failure Specialist assessment
(22)
129
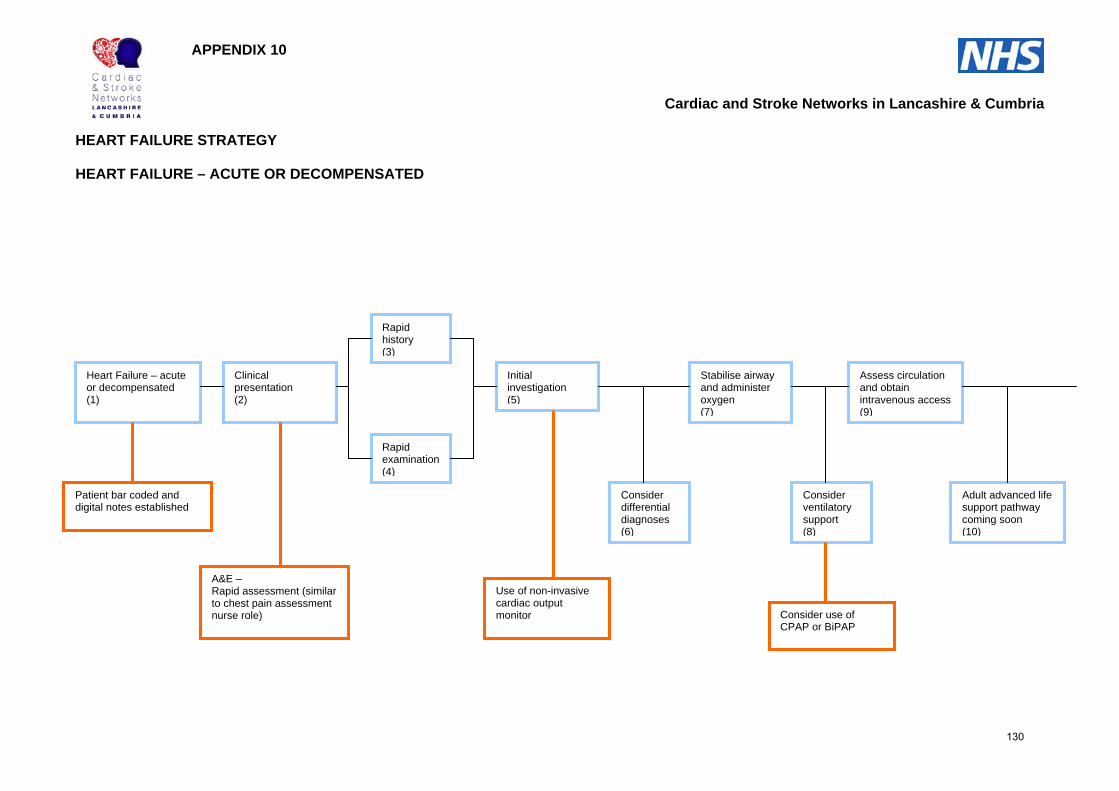
Cardiac and Stroke Networks in Lancashire & Cumbria HEART FAILURE STRATEGY
APPENDIX 10
HEART FAILURE – ACUTE OR DECOMPENSATED
Heart Failure – acute or decompensated (1)
Clinical presentation (2)
Rapid history (3)
Rapid examination (4)
Initial investigation (5)
Consider differential diagnoses (6)
Stabilise airway and administer oxygen (7)
Consider ventilatory support (8)
Assess circulation and obtain intravenous access (9)
Adult advanced life support pathway coming soon (10)
A&E – Rapid assessment (similar to chest pain assessment nurse role)
Patient bar coded and digital notes established
Use of non-invasive cardiac output monitor Consider use of
CPAP or BiPAP
130

Cardiac and Stroke Networks in Lancashire & Cumbria HEART FAILURE STRATEGY
APPENDIX 10
HEART FAILURE – ACUTE OR DECOMPENSATED (Cont)
Consider morphine for severe dyspnoea agitation or pain (11)
Systolic BP less than 100mmHg (12)
Systolic BP more than 100mmHg (13)
Consider fluid challenge if no pulmonary congestion (14)
Administer intravenous (IV) diuretics if pulmonary congestion (15)
Administer inotropic agent (16)
Administer IV diuretics if pulmonary congestion (17)
Administer vasodilators (18)
Consider adrenaline or noradrenaline if unresponsive (19)
Third line agents if unresponsive (20)
Further investigation and intervention as required (21)
Non-pharmacological management (22)
Considerations for discharge when stable (23)
Go to non-pharmacological intervention
Go to symptomatic LV dysfunction
BNP
Echo availability in A&E
CPAP
131

Cardiac and Stroke Networks in Lancashire & Cumbria HEART FAILURE STRATEGY
APPENDIX 10
SYMPTOMATIC LV SYSTOLIC DYSFUNCTION - MANAGEMENT Indications for
specialist referral (2)
Refer to cardiology (3)
Consider all of the following (4)
Lifestyle modifications and immunisation (5)
Pharmacological management of heart failure (6)
Management of comorbidity (7)
Patient communication and multidisciplinary care (8)
Commence diuretics if signs of fluid retention (10)
Commence an ACE inhibitor (11)
Ischaemic heart disease with LV dysfunction (9)
Hypertension or diabetes with LV dysfunction (12)
Review and monitor (13)
Use of Choose & Book
Primary Care registers, call and recall
IT referral/advice line with HF Specialist
Access to electronic rapid protocol of pharmacological treatment
Quality of life assessment
Ensure rapid protocol for up-titration is followed
IT referral advice line with HF specialist
Ensure repeat ECG at this stage, assess QRS width
Symptomatic LV systolic dysfunction – management (1)
132
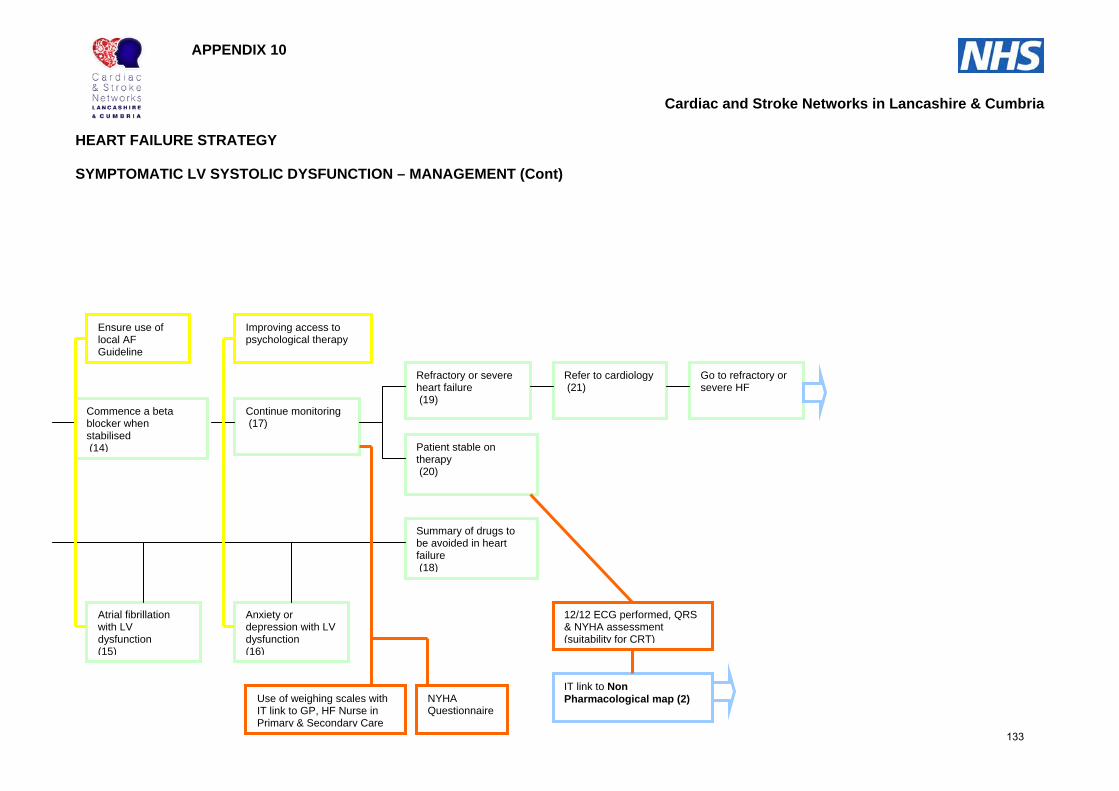
Cardiac and Stroke Networks in Lancashire & Cumbria HEART FAILURE STRATEGY
APPENDIX 10
SYMPTOMATIC LV SYSTOLIC DYSFUNCTION – MANAGEMENT (Cont)
Commence a beta blocker when stabilised (14)
Continue monitoring (17)
Atrial fibrillation with LV dysfunction (15)
Anxiety or depression with LV dysfunction (16)
Refractory or severe heart failure (19)
Patient stable on therapy (20)
Summary of drugs to be avoided in heart failure (18)
Refer to cardiology (21)
Go to refractory or severe HF
12/12 ECG performed, QRS & NYHA assessment (suitability for CRT)
IT link to Non Pharmacological map (2)
Ensure use of local AF Guideline
Improving access to psychological therapy
NYHA Questionnaire
Use of weighing scales with IT link to GP, HF Nurse in Primary & Secondary Care
133
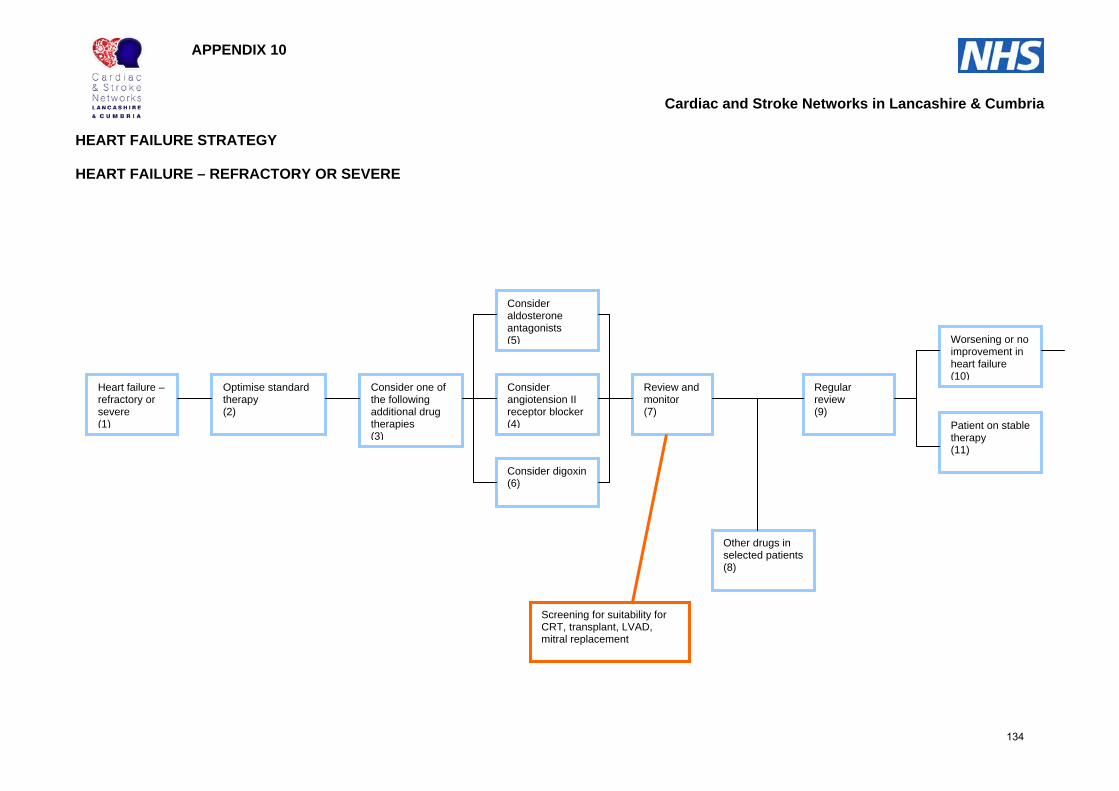
Cardiac and Stroke Networks in Lancashire & Cumbria HEART FAILURE STRATEGY
APPENDIX 10
HEART FAILURE – REFRACTORY OR SEVERE
Optimise standard therapy (2)
Consider one of the following additional drug therapies (3)
Consider angiotension II receptor blocker (4)
Consider aldosterone antagonists (5)
Consider digoxin (6)
Review and monitor (7)
Other drugs in selected patients (8)
Regular review (9)
Worsening or no improvement in heart failure (10)
Patient on stable therapy (11)
Screening for suitability for CRT, transplant, LVAD, mitral replacement
Heart failure – refractory or severe (1)
134

Cardiac and Stroke Networks in Lancashire & Cumbria HEART FAILURE STRATEGY
APPENDIX 10
HEART FAILURE – REFRACTORY OR SEVERE (Cont)
Assess quality of life and life expectancy (12)
Non-pharmacological intervention (13)
Terminal care for refractory or end stage heart failure (14)
Go to non-pharmacological intervention
Go to palliative care
135
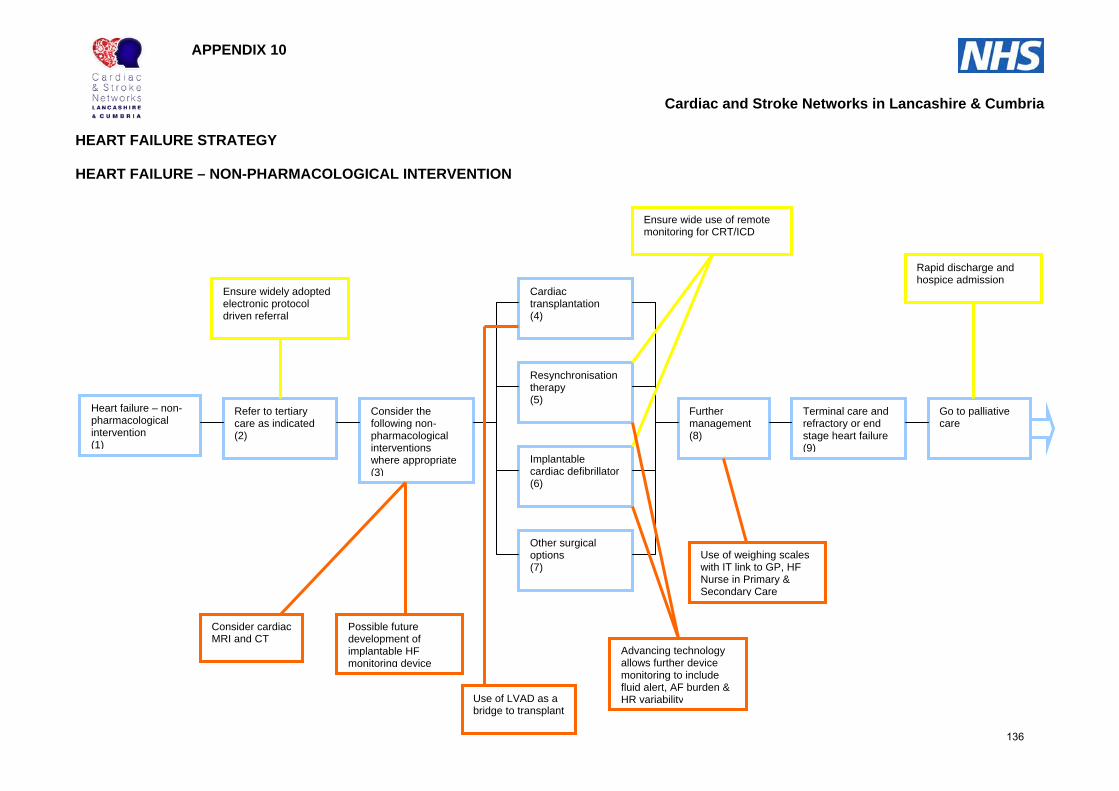
Cardiac and Stroke Networks in Lancashire & Cumbria HEART FAILURE STRATEGY
APPENDIX 10
HEART FAILURE – NON-PHARMACOLOGICAL INTERVENTION
Heart failure – non-pharmacological intervention (1)
Refer to tertiary care as indicated (2)
Consider the following non-pharmacological interventions where appropriate (3)
Cardiac transplantation (4)
Resynchronisation therapy (5)
Implantable cardiac defibrillator (6)
Other surgical options (7)
Further management (8)
Terminal care and refractory or end stage heart failure (9)
Go to palliative care
Ensure widely adopted electronic protocol driven referral
Consider cardiac MRI and CT
Use of LVAD as a bridge to transplant
Advancing technology allows further device monitoring to include fluid alert, AF burden & HR variability
Use of weighing scales with IT link to GP, HF Nurse in Primary & Secondary Care
Rapid discharge and hospice admission
Possible future development of implantable HF monitoring device
Ensure wide use of remote monitoring for CRT/ICD
136

Appendix 11 NYHA (NEW YORK HEART ASSOCIATION) Symptom classification
Class Symptom
1 No limitation Ordinary physical activity does not cause tiredness, breathlessness, chest discomfort or palpitation (an unexpected awareness of your heartbeat).
2 Slight limitation You are comfortable at rest but ordinary physical activity causes some tiredness, breathlessness, chest discomfort or palpitation (an unexpected awareness of your heartbeat).
3 Marked limitation You are comfortable at rest, but ordinary physical activity causes marked fatigue, breathlessness, chest discomfort or palpitation (an unexpected awareness of your heartbeat).
4 Inability to carry out any physical activity without discomfort
You have significant breathlessness or chest discomfort at rest. Any physical activity causes your symptoms to get worse.
137
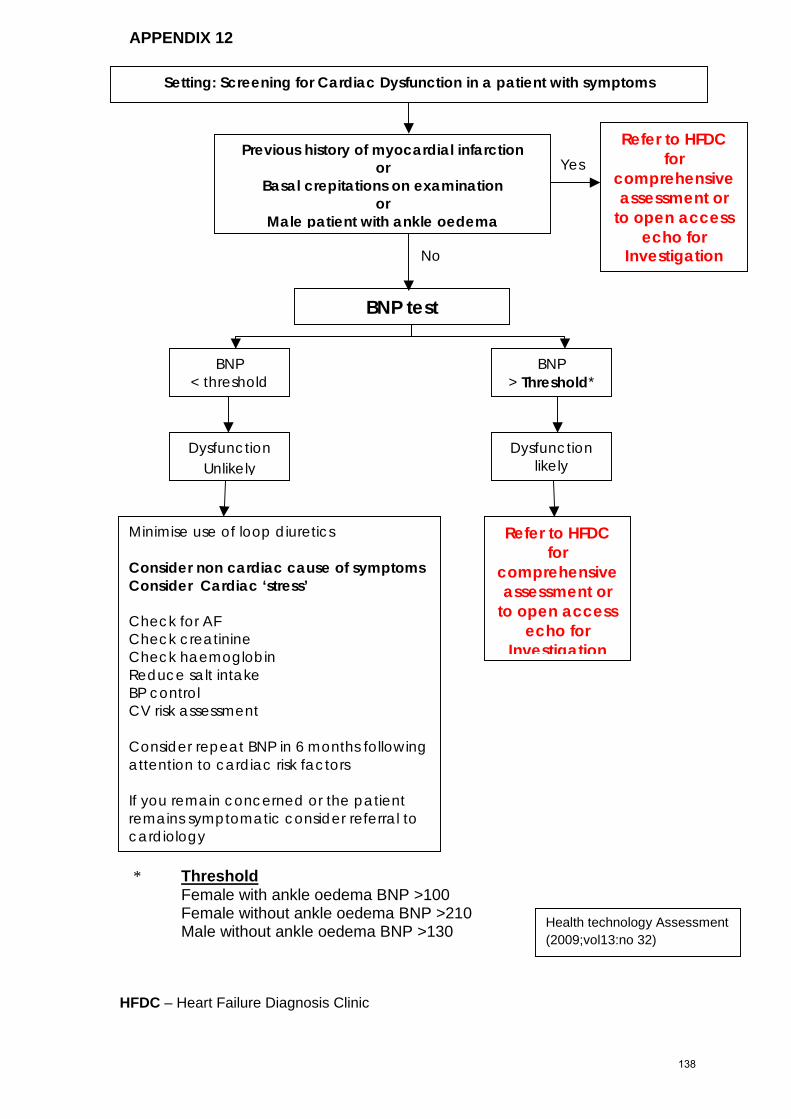
Appendix C * Threshold
APPENDIX 12
HFDC – Heart Failure Diagnosis Clinic
Female with ankle oedema BNP >100 Female without ankle oedema BNP >210 Male without ankle oedema BNP >130
BNP test
BNP < threshold
BNP > Threshold*
Dysfunction Unlikely
Minimise use of loop diuretics Consider non cardiac cause of symptoms Consider Cardiac ‘stress’ Check for AF Check creatinine Check haemoglobin Reduce salt intake BP control CV risk assessment Consider repeat BNP in 6 months following attention to cardiac risk factors If you remain concerned or the patient remains symptomatic consider referral to cardiology
Dysfunction likely
Setting: Screening for Cardiac Dysfunction in a patient with symptoms
Refer to HFDC for
comprehensive assessment or
to open access echo for
Investigation
Previous history of myocardial infarction or
Basal crepitations on examination or
Male patient with ankle oedema
Refer to HFDC for
comprehensive
No
Yes
assessment or to open access
echo for Investigation
Health technology Assessment (2009;vol13:no 32)
138
APPENDIX 13
Document Type: GUIDELINE
Unique Identifier: CORP/GUID/086
Version Number: 1
Title: Implantable Cardioverter Defibrillator (ICD) Reprogramming Guidelines Status:
Ratified Scope: Lancashire and South Cumbria Cardiac Network-wide
Classification: Organisational
Author/Originator and Title: Lauren Butler Angelic Delaney
Responsibility: Cardiac Network
Replaces: New Guideline
Description of amendments:
Risk Assessment: Not Applicable
Name of Committee: Divisional/Directorate/ Working Group: Cardiac Network Arrhythmia Group
Date of Meeting: Ongoing – bi-annual meetings Financial
Implications Not Applicable
Validated by: Sally Chisholm, Cardiac Network Programme Director
Validation Date: January 2008
Ratified by: Clinical Governance Committee
Ratified Date: 17/01/2008
Date of Issue: 17/01/2008 Review Date:01/05/2010
2006
2007
2008
2009
2010
2011
2012
2013
2014
2015
Review Dates: Review dates may alter if any significant changes are made
Does this document meet with the Race Relation Amendment Act (2000) Religious Discrimination Act, Age Discrimination Act, Disability Discrimination Act and Gender Equality Regulations? Not Applicable
139

Blackpool Fylde and Wyre Hospitals NHS Trust
Revision No: 1 Review Date:01/12/2008
I.D. No: CORP/GUID/086
Title: Implantable Cardioverter Defibrillator (ICD) Reprogramming Guidelines
Do you have the up to date version? See the intranet for the latest version Page 2 of 7
1 PURPOSE. To provide guidance to medical and clinical staff in acute and primary care trusts who are responsible for the management of patients in whom an Implantable Cardioverter Defibrillator has been implanted. This guidance outlines the situations in which reprogramming or withdrawal of Implantable Cardioverter Defibrillator therapy is required, the procedures to follow and personnel to contact is held within the guidance.
2 SCOPE. Acute and Primary Care Trusts within Lancashire and South Cumbria.
3 GUIDELINE
Clinical Requirement The clinical requirement for reprogramming an Implantable Cardioverter Defibrillator (ICD) should assess the clinical status of patients, underlying cardiac rhythm and whether detection and therapy is required or not and, if ICD therapy is delivered, whether it is appropriate. The clinical requirements include the following: (1) Routine reprogramming for optimisation of device settings (2) Switch off (withdrawal of therapy) during routine surgery/treatment (3) Switch off (withdrawal of therapy) device due to death of patient (4) Switch off (withdrawal of therapy) device due to end stage heart failure (5) Emergency reprogramming of detection or therapy parameters due to Ventricular
Tachycardia (VT) (6) Emergency reprogramming/application of magnet during emergency surgery If the patient has an episode of Ventricular Fibrillation (VF) and the device fails to deliver therapy or if the shock therapy fails, immediate external Direct Current (DC) defibrillation should be delivered and this does not fall within the remit of this guidance. Routine Reprogramming For Optimisation Of Device Settings This includes all reprogramming undertaken as part of follow up at ICD clinic which assesses therapies delivered, effectiveness of therapy, symptoms during arrhythmia and therapies and haemodynamic status of patient in relation to both ICD therapies and pacing modalities. Patients requiring follow up to assess ICD function and settings can access the ICD clinic at the Lancashire Cardiac Centre. Currently clinics are held on Wednesdays and Thursdays, 9.00 am to 12.00 noon but patients may be seen Monday to Friday, between 9.00 am and 5.00 pm by appointment with the Cardiac Physiology Pacing Team. Contact details – Lancashire Cardiac Centre Pacing Manager - Angelic Delaney 01253 657739
140

Blackpool Fylde and Wyre Hospitals NHS Trust
Revision No: 1 Review Date:01/12/2008
I.D. No: CORP/GUID/086
Title: Implantable Cardioverter Defibrillator (ICD) Reprogramming Guidelines
Do you have the up to date version? See the intranet for the latest version Page 3 of 7
Once devolvement of ICD follow up to District General Hospitals occurs, routine reprogramming may take place at district general hospital level. Switch Off (Withdrawal Of Therapy) During Routine Surgery/Treatment This involves programming the device to prevent detection of all incoming signals to the device. This ensures any noise entering the device from diathermy etc may not be considered an arrhythmia and prevents inappropriate shocks and collection of inappropriate data. However this does prevent the device from delivering any therapies and the device is effectively switched off. If during surgery the patient requires a shock due to an arrhythmia, the clinical condition and haemodynamic status of the patient should be considered and emergency external DC defibrillation delivered if required. If the patient is stable during the arrhythmia, consideration should be considered to programming the device and allowing shocks/therapy to be delivered by the device itself. Reprogramming to original settings should take place as soon as possible post – op. The time taken for the cardiac physiologist to return to reprogram the device should be taken into consideration during this decision making process. The Cardiac Physiologist at each District General Hospital should be contacted to perform the programming procedure.
Switch Off (Withdrawal Of Therapy) Of Device Due To Death Of Patient When a patient dies with an active ICD the Specialist Cardiac Physiologist at each trust needs to be informed as the device requires deactivation before removal by mortuary or undertaker staff. Relatives should be made aware that cremation is not possible with an ICD in situ. ICDs should always be deactivated in the event of the patient’s death, as towards battery end of life it will emit an audible bleep every day. Switch Off (Withdrawal Of Therapy) Of Device Due To End Stage Heart Failure Defibrillators are increasingly commonplace in the care of heart failure especially those combined with cardiac resynchronisation pacing (CRT). Withdrawal or deactivating implantable defibrillators can be difficult for patients and their relatives and should be addressed on an individual patient basis. Patients often report a perceived dependence on the device. Not all deaths from heart failure result in tachyarrhythmia as final mode of death Principles: Eventual withdrawal of ICD therapy should be discussed prior to initial implant, in all ICD recipients with heart failure. Patient information should be provided regarding the device activity, its function and its withdrawal prior to implantation. It is appropriate but not always essential to deactivate ICDs in patients with end stage heart failure. ICD patients should be encouraged to express their concerns especially in relation to their mode of death and shocks. Where the focus of care is more terminal, it should be explained: Deactivation of their ICD device does not mean that they will die imminently
141

Blackpool Fylde and Wyre Hospitals NHS Trust
Revision No: 1 Review Date:01/12/2008
I.D. No: CORP/GUID/086
Title: Implantable Cardioverter Defibrillator (ICD) Reprogramming Guidelines
Do you have the up to date version? See the intranet for the latest version Page 4 of 7
The ICD may have been of value in prolonging their life in the past, it may no longer be in their best interest for them to receive painful and often traumatic shocks Pacing functions including CRT should be left active with tachyarrhythmia therapies turned off Should the patient change their mind at any stage re-activation can easily be performed. When antiarrhythmic medical therapy is being withdrawn patients should be aware that device activation is more likely and they may consider switching off shock therapy. Deactivation of the device in the community setting is problematic, it should be considered and discussed at the same time as do not resuscitate decisions are made; and ideally discussed if being discharged from hospital to palliative community care it is incompatible that a patient should have a active ICD but otherwise be not for resuscitation. The specialist cardiac physiologists and specialist nursing staff should be liaised with along with the supervising electrophysiologist/device physician when deactivation is being considered. Magnets are only of value in temporarily deactivating defibrillators and should only be used by emergency personnel. Emergency Reprogramming Of Detection Or Therapy Parameters Due To Ventricular Tachycardia Clinical consideration should be given to the clinical and haemodynamic status of the patient and if emergency external defibrillation is required, this should be delivered. For patients with stable, incessant VT (VT storm) the device may be triggered to deliver multiple shocks, which may be ineffective and painful for the patient. Programming the device to inhibit delivery of shocks should be undertaken and medical management of the arrhythmia commenced. Initially, application of a magnet will deactivate the device temporarily until programming can take place and should only be used by emergency personnel. For patients with stable VT where the device is failing to deliver therapy, programming to ensure detection and termination of the arrhythmia should be undertaken. Emergency Reprogramming/Application Of Magnet To Suspend Therapy During Emergency Surgery As recommended in the associated document ‘Guidelines for the perioperative management of patients with implantable pacemakers or implantable cardioverter defibrillators, where the use of surgical diathermy/electrocautery is anticipated. (March 2006)’, it is recommended that if the ICD device cannot be programmed by available personnel, e.g. out of hours, then application of a magnet over the device will temporarily deactivate the device. In the event that the device is programmed to be unresponsive to magnet application, a follow up ICD check should be performed as soon as possible.
142
Blackpool Fylde and Wyre Hospitals NHS Trust
Revision No: 1 Review Date:01/12/2008
I.D. No: CORP/GUID/086
Title: Implantable Cardioverter Defibrillator (ICD) Reprogramming Guidelines
Do you have the up to date version? See the intranet for the latest version Page 5 of 7
Documentation Clear documentation of programming undertaken by the Cardiac Physiologist should be documented in any medical notes, heart failure notes, patient held records or GP notes if available. All records available at the time should have an entry of the procedure undertaken and should be signed by the Cardiac Physiologist and accompanying health care professional. A letter should be sent to the patients GP outlining the procedure undertaken at the earliest opportunity, a copy sent to the tertiary centre and a copy saved in the patient’s hospital notes. Lone working The Cardiac Physiologist should ensure another healthcare professional is present when attending a patient’s home. Ideally this should be someone who knows the patient and should be discussed and arranged with the personnel requesting the programming procedure. Medical consent Agreement for the withdrawal of ICD device therapy has to be obtained from a clinician treating the patient, Consultant or General Practitioner. It is recommended that discussion with the Acute Trust Cardiologist be obtained if possible prior to deactivation. Tertiary Centre Support Support will always be available at the tertiary centre if any issues arise or if any follow up checks are required at the times listed below. For all emergency out of hours care, the clinician at the District General Hospital should call the on-call cardiology registrar at Lancashire Cardiac Centre for advice/discussion regarding emergency transfer of the patient. Arrangements with the on-call cardiac physiologist at Lancashire Cardiac Centre will then be made. As recommended in the associated document ‘Guidelines for the perioperative management of patients with implantable pacemakers or implantable cardioverter defibrillators, where the use of surgical diathermy/electrocautery is anticipated. (March 2006)’, it is recommended that if the ICD device cannot be programmed by available personnel, e.g. out of hours, then application of a magnet over the device will temporarily deactivate the device. In the event that the device is programmed to be unresponsive to magnet application, a follow up ICD check should be performed as soon as possible.
4. ATTACHMENTS.
Appendix 1 – ICD Re Programming Guidelines, Contact Details
5. ELECTRONIC AND MANUAL RECORDING OF INFORMATION. Database for Policies, Procedures, Protocols and Guidelines Archive/Policy Co-ordinators office
143

Blackpool Fylde and Wyre Hospitals NHS Trust
Revision No: 1 Review Date:01/12/2008
I.D. No: CORP/GUID/086
Title: Implantable Cardioverter Defibrillator (ICD) Reprogramming Guidelines
Do you have the up to date version? See the intranet for the latest version Page 6 of 7
Archived at: Lancashire & South Cumbria Cardiac Network office, Room 244 Preston Business Centre, Watling Street Road, Preston PR2 8DY or via the Cardiac Network website – www.lsccn.nhs.uk
6. LOCATIONS THIS DOCUMENT ISSUED TO.
Copy No Location Date Issued 1 Intranet 17/01/2008 2 17/01/2008
8. OTHER RELEVANT /ASSOCIATED DOCUMENTS.
Procedure
No. Title
Symptom Control Guidelines For Patients With End-Stage Heart Failure (March 2007)
Guidelines for the perioperative management of patients with implantable pacemakers or implantable cardioverter defibrillators, where the use of surgical diathermy/electrocautery is anticipated. (March 2006)
British Heart Foundation – Implantable cardioverter defibrillators in patients who are reaching the end of life (July 2007)
6 AUTHOR//DIVISIONAL/DIRECTORATE MANAGER APPROVAL.
Issued By Lauren Butler Checked By Sally Chisholm
Job Title Cardiac Physiology Training & Development Manager
Job Title Cardiac Network Programme Director
Signature Signature
Date January 2008 Date January 2008
144
Blackpool Fylde and Wyre Hospitals NHS Trust
Revision No: 1 Review Date:01/12/2008
I.D. No: CORP/GUID/086
Title: Implantable Cardioverter Defibrillator (ICD) Reprogramming Guidelines
Do you have the up to date version? See the intranet for the latest version Page 7 of 7
APPENDIX 1 –ICD Re Programming Guidelines, Contact Details
Lancashire & South Cumbria Cardiac Physiologist and emergency contact details: Lancashire Cardiac Centre Monday – Friday 9am - 5 pm Angelic Delaney – 01253 657739 Out of Hours: On call SpR 01253300000 DGH Cardiac Physiologist contact details: Monday – Friday 9am – 5pm University Hospitals of Morecambe Bay Kay Smith – 01524 583026 East Lancashire Hospitals Trust Tracy Doherty – 01254 733309 Lancashire Teaching Hospitals Angela Reed – 01772 522253 Out of Network contact details for patients who had the device implanted at other tertiary centres and information regarding manufacturer and model of device is required. Wythenshawe hospital, Manchester Monday - Friday 9am - 5pm Pacing/ICD Physiologists: 0161 291 2545
ICD Nurse Specialists: 0161 291 2752 Out of hours (Clinical Emergency only) On-call Cardiology SpR: 0161 998 7070 Manchester Royal Infirmary Monday – Friday 8.30am-5pm Ros Hirst ([email protected]) 0161 276 4611 Karen Toombs 0161276 905/7900 Out of hours CCU: 0161 276 4200 CTC, Liverpool Monday – Friday 9am - 5pm Sue Hughes 0151 600 1701 Sandra Bellchambers 0151 600 1701 Out of hours CCU: 0151 2281616 Pacing/EP SpR Leeds General Infirmary Monday – Friday 9am – 5pm Ann Nicholls 0113 3925449 or page 6389 via switch (0113 802243) Out of hours CCU: 01133927117
145

REFERENCES
1. Department of Health (2007) World Class Commissioning Vision Summary. The Stationary
Office. London 2. Department of Health (2008) High Quality Care for All. The Stationary Office. London 3. Source: Lancashire & Cumbria PCT websites - Accessed 08.06.09
4. Deacon, L., Harrison, R., Timpson, C., Tocque, K., Bellis, M.A. (2009) Health and Lifestyles in the North West. North West Public Health Observatory.
5. Cumbria & Lancashire Public Health Network (2009) Business Plan 2008 -2009.
6. Department of Health (2008) Putting prevention first -Vascular Checks: risk assessment and management. Crown Copyright, London
7. Cardiac Networks Devices Survey Group (2009). A review of pacemaker and ICD implantation practice in 2007.
8. World Health Organisation (2008). The Atlas of Heart Disease and Stroke.
http://www.who.int/cardiovascular_diseases/en/cvd_atlas_11_socioeconomics.pdf?bcsi_scan_BAD3F111D6E143DB=0&bcsi_scan_filename=cvd_atlas_11_socioeconomics.pdf Accessed 08.06.09
9. Lancashire County Council website. Population Life Expectancy and Ethnicity.
http://www.lancashire.gov.uk/office_of_the_chief_executive/lancashireprofile/monitors/lifeexpectethnic.asp Accessed 08.06.09
10. Cumbria Intelligence Observatory. Presenting Ethnicity Data for Cumbria and Districts 2007
Estimates. http://www.cumbriaobservatory.org.uk/elibrary/Content/Internet/536/673/1756/39759153033.pdf Accessed 08.06.09
11. Wild S, McKeigue P (1997) Cross sectional analysis of mortality by country of birth in England
and Wales, 1970-92. BMJ 314: 705-10. cited by Allender, S., Peto, V., Scarborough, P., Kaur, A., Rayner, M., (2008) Coronary heart disease statistics. BHF: London
http://www.heartstats.org/datapage.asp?id=7998 Accessed 08.06.09
12. The Information Centre and Office for National Statistics (2008). Health Survey for England 2006: Volume 1 - Cardiovascular disease and risk factors in adults. Leeds: The Information Centre.
13. National Statistics. Mortality statistics: cause. Review of the Registrar General on deaths by
cause, sex and age, in England and Wales, 2005. Series DH2 no. 32. Office for National Statistics, London, 2007. www.statistics.gov.uk/downloads/theme_health/Dh2_32/DH2_No32_2005.pdf Accessed 08.06.09
14. Department of Health. (1999).Saving Lives: Our Healthier Nation. The Stationery Office,
London. 15. Department of Health. (2007) Shaping the future progress report 2006. The Coronary Heart
Disease National Framework. DH, London,
146
16. Department of Health (2008). The Coronary Heart Disease National Service Framework: Building for the Future - Progress Report for 2007. London: Department of Health Publications.
17. Clinical and Health Outcomes Knowledge Base - Managed for The Information Centre for health and social care by the National Centre for Health Outcomes Development. Crown Copyright, February 2009. www.nchod.nhs.uk, Mortality from all Circulatory Disease –Direct Standardised Rate 1993 -2007 All persons http://www.nchod.nhs.uk/NCHOD/Compendium.nsf/($All)/EC0C09D9C4D6E258802575640032601A/$File/06A_076DRT00++_07_V1_D.xls?OpenElement Accessed 26.05.09
18. North West Public Health Observatory
http://www.nwph.net/nwpho/Lists/Health_calendar_list/DispForm.aspx?ID=7850 Accessed 26.05.09
19. Modelled estimates of prevalence of CHD for PCTs in England. Eastern Region Public
Health Observatory, November 2008. http://www.erpho.org.uk/Download/Public/17903/1/Modelled%20CHD%20by%20PCT%20v2.xls Accessed 26.05.09
20. Department of Health (2002). Tackling Health Inequalities: 2002 Cross-Cutting Review. DH.
London 21. Department of Health Publications Department of Health (2004). Choosing Health: Making
healthy choices easier. DH. London 22. National Institute for Health and Clinical Excellence (2006) Public Health Programme Draft
Guidance. Smoking Cessation Services Including the use of Pharmacotherapies, in Primary Care, Pharmacies. Local Authorities and Workplaces Available at http://guidance.nice.org.uk/download.aspx?0=42978
23. Twigg L, Moon G and Walker S (2004). The Smoking Epidemic England. London: Health
Development Agency 24. Radke PW and Schunkert H (2006). Public Smoking Ban: Europe on the Move. European
Health Journal, 27, 2358-2386. 25. Parrot S, Godfrey C, Raw M, West R and McNeill A (1998). Guidance for Commissioners
on the Cost Effectiveness of Smoking Cessation Interventions. Thorax, 53[5(part 2)], 1-38. 26. Wood J, Hennell T, Jones A, Hooper J, Tocque K and Bellis MA (2006). Where Wealth
Means Health: Illustrating Inequality in the North West. Liverpool: Centre for Public Health, Liverpool John Moores University
27. Office on Smoking and Health, National Center for Chronic Disease Prevention and Health
Promotion, Centers for Disease Control and Prevention. The health benefits of smoking cessation: a report of the Surgeon General. Atlanta, GA, National Center for Chronic Disease Prevention and Health Promotion, 1990 (DHHS publication no. (CDC) 90–8416).8,
28. Department of Health (1998). Smoking Kills: White Paper on Tobacco. London: Department
of Health Publications. 29. Action on Smoking and Health (ASH) (2008). Tobacco economics [Online]. Available at
www.ash.org.uk/files/documents/ASH_95.pdf 30. Department of Health (2008) Health Profile 2008 – North West. Association of Public Health
Observatories. www.healthprofiles.info
147

31. Blood Pressure Association website.www.bpassoc.org.uk 32. Department of Health (2004). National Standards Local Action - Health and Social Care
Standards and Planning Framework 2005/06-2007/08. London: Department of Health Publications.
33. National Institute for Health and Clinical Excellence (2006). Hypertension: Management of
Hypertension in Adults in Primary Care [Online]. Available at www.nice.org.uk/CG034. Accessed16.06.2009.
34. Department of Health (2008). Carers at the heart of 21st century families and communities:
a caring system on your side, a life of your own Available at www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_085345
35. Unadjusted Disease Prevalence. Quality and Outcomes Framework (QOF) for April 2007 -
March 2008, England. Numbers of QOF disease registers and unadjusted prevalence rates by Primary Care Trust http://www.ic.nhs.uk/webfiles/QOF/2007-08/NewFilesGS/QOF0708_PCTs_Prevalence.xls
36. Faculty of Public Health hypertension prevalence model
http://www.fphm.org.uk/resources/AtoZ/toolkit_hypertension/tools.asp 37. http://www.erpho.org.uk/Download/Public/17923/1/Hypertention%20prevalence%20modelli
ng%20briefing%20document%20v2.doc?bcsi_scan_DFE16166FCC0B4CE=0&bcsi_scan_filename=Hypertention%20prevalence%20modelling%20briefing%20document%20v2.doc
38. World Health Organisation. The world health report 2002: Reducing risks, promoting health
life. WHO, Geneva, 2002. www.who.int/whr/2002/en 39. National Institute for Health and Clinical Excellence. (2008) NICE clinical guideline 67: Lipid
modification: cardiovascular risk assessment and the modification of blood lipids for the primary and secondary prevention of cardiovascular disease. http://www.nice.org.uk/nicemedia/pdf/CG067NICEGuideline.pdf Accessed 02.07.09
40. QRESEARCH and The Health and Social Care Information Centre (2008) Final Report to
the NHS Information Centre and Department of Health. Public Health Indicators Project. Key Fact Reports. A summary of public health indicators using electronic data from primary care. The NHS Information Centre. http://www.ic.nhs.uk/webfiles/publications/A%20summary%20of%20public%20health%20indicators%20using%20electronic%20data%20from%20primary%20care.pdf Accessed 02.07.09
41. Department of Health (2008) Putting prevention first. Vascular Checks: risk assessment
and management ‘Next Steps’ Guidance for Primary Care Trusts. Crown Copyright, London 42. National Institute of Clinical Excellence (2006) Press release: NICE guidance on the use of
statins set to benefit millions of adults. http://www.nice.org.uk/nicemedia/pdf/2006_002_Launch_of_statins.pdf Accessed 22.06.09
43. Scottish Intercollegiate Guidelines Network (SIGN) (2007) Risk estimation and the
prevention of cardiovascular disease. A National Guideline No.97. NHS Quality Improvement. Scotland.
44. National Prescribing Centre (2009) Increasing low cost prescribing for lipid modification.
www.npc.co.uk; www.institute.nhs.uk.
148

45. Regional Drug & Therapeutics Centre (2009) North West SHA Annual Prescribing Report. 46. World Health Organisation (2007) Prevention of cardiovascular disease: guidelines for
assessment and management of total cardiovascular risk. WHO Press, Switzerland. 47. McGee DL, (2005) Diverse Populations Collaboration. Body mass index and mortality: a
meta-analysis based on person-level data from twenty-six observational studies. Ann Epidemiol.; 15(2):87–97.
48. Wilson PW et al. (2002) Overweight and obesity as determinants of cardiovascular risk: the
Framingham experience. Arch Intern Med.;162(16):1867–1872. 49. Hu G et al. (2004) Joint effects of physical activity, body mass index, waist circumference
and waist-to-hip ratio with the risk of cardiovascular disease among middle-aged Finnish men and women. Eur Heart J; 25(24):2212–2219.
50. Haslam DW, James WPT. (2005) Obesity. Lancet.; 366:1197–1209. 51. Government Office for Science & Department of Innovation, Universities and Skills (2007).
Foresight. Tackling obesities: future choices. Project report: 2nd edition www.foresight.gov.uk/Obesity/obesity_final/17.pdf Accessed 15.06.09
52. North West Public Health Observatory (2008) Healthy weight in the North West Population.
Synthesis November 53. The NHS Information Centre for Health and Social Care (IC) (2007) Model-Based
Estimates of Obesity for PCOs in England, 2003-2005. Source: Health Surveys for England 2003 to 2005. Produced by National Centre for Social Research (NatCen), May 2008 http://www.ic.nhs.uk/webfiles/Popgeog/Model%20Based%20Estimates%20of%20Obesity%20%28adults%29%20for%20PCOs%20in%20England%2C%202003-2005.xls Accessed 03.07.09
54. The NHS Information Centre for Health and Social Care (IC) (2007)
http://www.ic.nhs.uk/statistics-and-data-collections/population-and-geography/neighbourhood-statistics/neighbourhood-statistics:-model-based-estimates-of-healthy-lifestyle-behaviours-at-pco-level-2003-05
55. National Institute of Clinical Excellence (2003) Technology Appraisal Guidance 71 –
Guidance on the Use of Coronary Artery Stents available at www.nice.org.uk 56. North West Strategic Health Authority (2008) Healthier Horizons for the North West. Our
NHS, Our Future. A new vision for health and healthcare in the North West. 57. National Institute of Clinical Excellence Guidance (2006) Atrial Fibrillation: The
Management of Atrial Fibrillation (AF) which outlines those patients with AF whom require Echocardiography (36). Available at www.nice.org.uk
58. National Institute of Clinical Excellence (2009) Draft Acute Coronary Syndroms available at
www.nice.org.uk 59. Hackett, D. (2005) Cardiac workforce requirements in the UK. British Cardiac Society 60. National Institute of Clinical Excellence Guidance (2003) Myocardial perfusion scintigraphy
for the diagnosis and management of angina and myocardial infarction (Technology Appraisal 73) http://www.nice.org.uk/nicemedia/pdf/TA073guidance.pdf Accessed 22.09.09
149
61. Department of Health (2000) National Service Framework for Coronary Heart Disease. Crown, London
62. Department of Health, (2000 and 2005) National Service Framework for Coronary Heart
Disease. Chapter 8. Crown. London 63. NHS Improvement, (May 2009) Commissioning for Stroke. Prevention in Primary Care –
The role of Atrial Fibrillation 64. National Institute for Health and Clinical Excellence, (2003) NICE Clinical guideline 5.
Chronic Heart Failure; National clinical guideline for diagnosis and management in primary and secondary care
65. National Institute for Health and Clinical Excellence, (May 2007) NICE technology appraisal
guidance 120. Cardiac resynchronisation therapy for the treatment of heart failure. 66. National Institute for Health and Clinical Excellence, (Jan 2006) NICE technology appraisal
95, Review of Technology appraisal 11. Implantable cardioverter defibrillators for arrhythmias
67. Department of Health, (Dec 2008) Heart Rhythm Devices; UK National Survey 2007 68. Department of Health, (April 2009) A review of pacemaker and ICD implantation practice in
2007; Cardiac and Stroke Networks in Lancashire and Cumbria in 2007 69. Stewart S, Murphy N, Walker A, McGuire A, McMurray JJ. (2004) Cost of an emerging
epidemic: an economic analysis of atrial fibrillation in the UK. Heart. Mar; 90(3):286-92. 70. NHS Improvement www.improvement.nhs.uk 71. National Institute for Health and Clinical Excellence, (2008) Transcatheter aortic valve
implantation for aortic Stenosis (IPG 266) http://www.nice.org.uk/nicemedia/pdf/IPG266Guidance.pdf Accessed 22.09.09
72. The Information Centre for Health & Social Care, National Coronary Angioplasty Audit,
January to December 2005 73. Oxford Healthcare Associates (2009) Access to Cardiac Care in the UK (ACCUK)
http://www.bcs.com/documents/Access_to_Cardiac_Care_in_the_UK_-_Full_Version_FINAL_1_07_09.pdf?bcsi_scan_BAD3F111D6E143DB=0&bcsi_scan_filename=Access_to_Cardiac_Care_in_the_UK_-_Full_Version_FINAL_1_07_09.pdf Accessed 21.09.09
74. Balachandran, K. (June 2009) Abstract 54. British Cardiac Society Annual Conference 75. Department of Health (2008) Treatment of heart attack national guidance: final report of the
National Infarct Angioplasty Project (NIAP) http://www.dh.gov.uk/prod_consum_dh/groups/dh_digitalassets/@dh/@en/documents/digitalasset/dh_089454.pdf?bcsi_scan_BAD3F111D6E143DB=0&bcsi_scan_filename=dh_089454.pdf Accessed 21.09.09
76. British Cardiovascular Intervention Society (BCIS) (2005) Recommendations for Good
Practice and Training 77. National Institute of Clinical Excellence Guidance to the NHS on Coronary Artery Stents,
NICE 2000/014 Issued: 11 May 2000 available at www.nice.org.uk
150
78. The Society for Cardiothoracic Surgery in Great Britain and Ireland (2008). Sixth National Adult Cardiac Surgical database report – Demonstrating quality
79. Department of Health (2007) Chief Medical Officers Report: Good Doctors safer Patients
available at http://www.dh.gov.uk 80. National Confidential Enquiry into Patient Outcome and Death (NCEPOD) (2008) 81. National Institute of Clinical Excellence Guidance (2008) Transcatheter aortic valve
implantation for aortic Stenosis available at www.nice.org.uk 82. British Heart Foundation (2007) Cardiac Rehabilitation…recovery or bypass? National
Campaign for Cardiac Rehabilitation. The evidence.
83. Department of Health (2000) National Service Framework for Coronary Heart Disease Modern Standards & Service Models., HMSO
84. NHS Centre for Reviews and Dissemination. (1998) Cardiac rehabilitation. Effective Health Care; 4 (4):1-11.
85. Oldridge NB, Guyatt GH, Fisher ME, Rimm AA. (1988) Cardiac rehabilitation after
myocardial infarction: combined experience of randomized clinical trials. JAMA; 260:945-50.
86. O’Connor GT, Buring GE, Yusuf S et al. (1989) An overview of randomized trials of
rehabilitation with exercise after myocardial infarction. Circulation; 80:234-44. 87. British Heart Foundation (2009) The National Audit of Cardiac Rehabilitation. Annual
Statistical Report 2009. 88. NICE. (2007) MI: secondary prevention: secondary prevention in primary and secondary
care for patients following a myocardial infarction. National Institute for Health and Clinical Excellence, Crown copyright.
89. The British Association of Cardiac Rehabilitation (2007) Standards and Core Components
for Cardiac Rehabilitation 90. Balady GJ, Williams MA, Ades PA, Bittner V, Comoss P,Foody JM, et al.( 2007) Core
components of cardiac rehabilitation/secondary prevention programs: 2007 update: a scientific statement from the American Heart Association Exercise, Cardiac Rehabilitation, and Prevention Committee, the Council on Clinical Cardiology; the Councils on Cardiovascular Nursing, Epidemiology and Prevention, and Nutrition, Physical Activity, and Metabolism; and the American Association of Cardiovascular and Pulmonary Rehabilitation. Circulation. May 22;115 (20):2675-82.
91. Jolliffe JA, Rees K, Taylor RS, Thompson D, Oldridge N, Ebrahim S. (2000) Exercise-
based rehabilitation for coronary heart disease. Cochrane Database System Rev. 2000(4):CD001800.
92. Oldridge NB, Guyatt GH, Fischer ME, Rimm A.A. (1988) Cardiac rehabilitation after
myocardial infarction. Combined experience of randomized clinical trials. Jama. Aug19;260(7):945-50.
93. Rees K, Taylor RS, Singh S, Coats AJ, Ebrahim S. (2004) Exercise based rehabilitation for
heart failure. Cochrane Database System Rev. 2004(3):CD003331.
151
94. The British Association of Cardiac Rehabilitation (2009) Standards and Core Components for Cardiac Rehabilitation update. Staffing of Cardiac Rehabilitation Programmes
95. http://www.theheartmanual.com/ 96. SIGN. Scottish Intercollegiate Guidelines Network (SIGN) (2002) Cardiac rehabilitation: A
national clinical guideline No. 57. Scottish Intercolllegiate Guidelines Network. 97. British Association Cardiac Rehabilitation (BACR) (2007-2008) Survey of Cardiac
Rehabilitation. 98. Clinical and Health Outcomes Knowledge Base - Managed for The Information Centre for
health and social care by the National Centre for Health Outcomes Development. Crown Copyright, May 2009. www.nchod.nhs.uk, Source of data: Quality and Outcomes Framework. Prevalence: heart failure 2007/2008. http://www.nchod.nhs.uk/NCHOD/compendium.nsf/($All)/8988DC94EF606317802575EB003C0C16/$File/09T_655PC_08_V1_D.xls?OpenElement Accessed 27.08.09
99. Clinical and Health Outcomes Knowledge Base - Managed for The Information Centre for
health and social care by the National Centre for Health Outcomes Development. Crown Copyright, May 2009. www.nchod.nhs.uk, Source of data: Quality and Outcomes Framework Exercise testing / specialist referral for patients with newly diagnosed angina: http://www.nchod.nhs.uk/NCHOD/compendium.nsf/($All)/0C573BDDA9110864802575EB003C0BDB/$File/09I_601PC_08_V1_D.xls?OpenElement#a417 Accessed 27.08.09
100. New York Heart Association functional and therapeutic classification for prescription of physical
activity for cardiac patients. http://www.hcoa.org/hcoacme/chf-cme/chf00070.htm Accessed 14.09.09
101. The British Heart Foundation (2007) Cardiac Rehabilitation…recovery or bypass? National
Campaign for Cardiac Rehabilitation. The evidence. 102. Griffin SC, Barber JA,Manca A, et al. (2007) Cost effectiveness of clinically appropriate
decisions on alternative treatments for angina pectoris: prospective observational study. BMJ 5 March..
103. Gray AM, Bowman GS, Thompson DR. (1997) The cost of cardiac rehabilitation services in
England and Wales. J R Coll Physicians London 31:57–61. 104. Allison TG,Williams DE,Miller TD, et al.Medical and economic costs of psychologic distress
in patients with coronary artery disease. Mayo Clin Proc 1995;70:734–42. 105. Lewin B, Robertson IH, Cay EL, et al. Effects of self-help post-myocardial infarction
rehabilitation on psychological adjustment and use of health services. Lancet 1992;339:1036–40.
106. Healthcare Commission (2007) Pushing the boundaries: improving services for people with
heart failure. London: Commission for Healthcare Audit and Inspection. 107. Department of Health (2008) The operating Framework for the NHS in England 2009/10:
high quality care for all. 108. Department of Health (2006) Our health, our care, our say: a new direction for community
services. 109. Department of Health (2007) Commissioning framework for Health and Well being.
152
110. Department of Health (2006) A stronger local voice: a framework for creating a stronger local voice in the development of health and social care services.
111. Department of Health (2004, updated 2006) Standards for better health. 112. NHS Institute for innovation and Improvement (2009) delivering Quality and Value, Focus
on: Heart Failure. 113. Hanumanthu S, Butler J, Chomsky D et al. (1997) Effect of heart failure program on
hospitalisation frequency and exercise tolerance. Circulation, 96 (9), pp. 2842-2848.
114. Jaarsma T, Stromberg A, DeGeest S et al (2006) Heart Failure management programmes in Europe. European Journal of Cardiovascualr Nursing, 5 (3) pp. 197-205.
115. Nicol ED, Fittall B, Roughton M et al. (2008) NHS heart failure survey: a survey of acute heart failure admissions in England, Wales and Northern Ireland. Heart 94: 172–7.
116. Lip GYH, Khan H, Bhatnagar A, et al. (2004) Ethnic differences in patient perceptions of heart failure and treatment: the West Birmingham heart failure project. Heart 90: 10.
117. Stewart, S (2005) Financial aspects of heart failure programs of care. The European
Journal of Heart Failure 7:423 -428.
118. Health Technology Assessment (2009) Systematic review and individual patient data meta – analysis of diagnosis of heart failure, with modelling of implications of different diagnostic strategies in primary care.
119. Stewart S, Horowitz JD (2003) Specialist nurse management programmes: economic
benefits in the management of heart failure. Pharmacoeconomics 21: 225–40.
120. Patwala AY et al, (2009) Maximising patient benefit from cardiac resynchronisation therapy with the addition of structured exercise training. J Am Coll Cardiol; 53:2332-2339.
121. National Institute for Health and Clinical Excellence, (2008) NICE clinical guideline 73. Early identification and management of chronic kidney disease in adults in Primary and Secondary care.
122. 32nd Bethesda Conference: Care of the adult with Congenital Heart Disease. Oct 2000,
Journal of American Cardiology, 2001:37(5);11161-98. 123. DH Vascular Programme Team (2006) Adult congenital Heart Disease A commissioning
guide for services for young people and Grown Ups with Congenital Heart Disease (GUCH), Department of Health
153


















