
Cardiac Positron Emission Tomography Positron Emission Tomography Frank M. Bengel, MD, Takahiro...
15
STATE-OF-THE-ART PAPER Cardiac Positron Emission Tomography Frank M. Bengel, MD, Takahiro Higuchi, MD, Mehrbod S. Javadi, MD, Riikka Lautamäki, MD, PHD Baltimore, Maryland Positron emission tomography (PET) is a powerful, quantitative imaging modality that has been used for de- cades to noninvasively investigate cardiovascular biology and physiology. Due to limited availability, method- ologic complexity, and high costs, it has long been seen as a research tool and as a reference method for valida- tion of other diagnostic approaches. This perception, fortunately, has changed significantly within recent years. Increasing diversity of therapeutic options for coronary artery disease, and increasing specificity of novel thera- pies for certain biologic pathways, has resulted in a clinical need for more accurate and specific diagnostic tech- niques. At the same time, the number of PET centers continues to grow, stimulated by PET’s success in oncol- ogy. Methodologic advances as well as improved radiotracer availability have further contributed to more widespread use. Evidence for diagnostic and prognostic usefulness of myocardial perfusion and viability assess- ment by PET is increasing. Some studies suggest overall cost-effectiveness of the technique despite higher costs of a single study, because unnecessary follow-up procedures can be avoided. The advent of hybrid PET-computed tomography (CT), which enables integration of PET-derived biologic information with multislice CT-derived mor- phologic information, and the key role of PET in the development and translation of novel molecular-targeted imaging compounds, have further contributed to more widespread acceptance. Today, PET promises to play a leading diagnostic role on the pathway toward a future of high-powered, comprehensive, personalized, cardiovas- cular medicine. This review summarizes the state-of-the-art in current imaging methodology and clinical applica- tion, and outlines novel developments and future directions. (J Am Coll Cardiol 2009;54:1–15) © 2009 by the American College of Cardiology Foundation That is gold which is worth gold. —George Herbert, English poet, 1593 to 1633 (1) Since the introduction of the first positron emission tomogra- phy (PET) scanner in 1975 (2), PET has been used for noninvasive imaging of the heart (3,4). It has often helped reveal groundbreaking basic science in the areas of myocardial blood flow regulation (5–9), myocardial substrate metabolism (10 –14), and cardiac autonomic innervation (15–18). Due to its inherently quantitative nature, its superior detec- tion sensitivity, and its advantageous spatial and temporal resolution over conventional nuclear techniques, PET has been considered a “gold standard” for noninvasive assessment of myocardial perfusion and viability. In the past, multiple new imaging techniques have been validated with PET as the gold standard (19 –26). And in the near future, PET imaging is expected to play a key role in the introduction of novel, molecular-targeted imaging approaches (27,28). Despite its undisputed value as a high-end diagnostic tool, PET has struggled for many years to expand from its role as a reference standard to broader clinical application. Impeding factors have been the complexity and limited availability of PET cameras, the complexity of production and delivery of short-lived positron-emitting radiotracers, and concerns related to the high cost of the test. Approval of PET radiotracers for clinical cardiac application by the U.S. Food and Drug Administration (FDA) in 1989 and 2000, followed by reimbursement of their use for myocar- dial perfusion and viability imaging by the Centers for Medi- care and Medicaid Services (CMS) (Table 1), were important first steps toward clinical success (29). In recent years, contin- uous improvement of scanner systems, commercial marketing of the tracers fluorodeoxyglucose (FDG) and rubidium-82 ( 82 Rb), and increasing availability of the technique, mostly due to its tremendous success in oncology, have all contributed to a rapid growth of PET for clinical cardiac imaging. Today, many leading nuclear cardiology institutions run high-throughput PET programs and create further evidence for its clinical usefulness (30 –33). Large sample-size studies and randomized trials are underway or have been published (34). Industry is introducing novel radiotracers for future commercialization (35). Technical advances such as hybrid imaging systems (36) and molecular-targeted probes (28) From the Division of Nuclear Medicine/PET, Russell H. Morgan Department of Radiology and Radiological Science, Johns Hopkins University, Baltimore, Maryland. Dr. Bengel receives research grants from Lantheus Medical Imaging and GE Healthcare, and has received speaker honoraria from GE Healthcare, BayerSchering Pharma, and Siemens Medical Solutions. Manuscript received November 13, 2008; revised manuscript received January 27, 2009, accepted February 23, 2009. Journal of the American College of Cardiology Vol. 54, No. 1, 2009 © 2009 by the American College of Cardiology Foundation ISSN 0735-1097/09/$36.00 Published by Elsevier Inc. doi:10.1016/j.jacc.2009.02.065
Transcript of Cardiac Positron Emission Tomography Positron Emission Tomography Frank M. Bengel, MD, Takahiro...
Spnrb(
trcmisem
FRDHP
2
Journal of the American College of Cardiology Vol. 54, No. 1, 2009© 2009 by the American College of Cardiology Foundation ISSN 0735-1097/09/$36.00P
STATE-OF-THE-ART PAPER
Cardiac Positron Emission Tomography
Frank M. Bengel, MD, Takahiro Higuchi, MD, Mehrbod S. Javadi, MD,Riikka Lautamäki, MD, PHD
Baltimore, Maryland
Positron emission tomography (PET) is a powerful, quantitative imaging modality that has been used for de-cades to noninvasively investigate cardiovascular biology and physiology. Due to limited availability, method-ologic complexity, and high costs, it has long been seen as a research tool and as a reference method for valida-tion of other diagnostic approaches. This perception, fortunately, has changed significantly within recent years.Increasing diversity of therapeutic options for coronary artery disease, and increasing specificity of novel thera-pies for certain biologic pathways, has resulted in a clinical need for more accurate and specific diagnostic tech-niques. At the same time, the number of PET centers continues to grow, stimulated by PET’s success in oncol-ogy. Methodologic advances as well as improved radiotracer availability have further contributed to morewidespread use. Evidence for diagnostic and prognostic usefulness of myocardial perfusion and viability assess-ment by PET is increasing. Some studies suggest overall cost-effectiveness of the technique despite higher costsof a single study, because unnecessary follow-up procedures can be avoided. The advent of hybrid PET-computedtomography (CT), which enables integration of PET-derived biologic information with multislice CT-derived mor-phologic information, and the key role of PET in the development and translation of novel molecular-targetedimaging compounds, have further contributed to more widespread acceptance. Today, PET promises to play aleading diagnostic role on the pathway toward a future of high-powered, comprehensive, personalized, cardiovas-cular medicine. This review summarizes the state-of-the-art in current imaging methodology and clinical applica-tion, and outlines novel developments and future directions. (J Am Coll Cardiol 2009;54:1–15) © 2009 by theAmerican College of Cardiology Foundation
ublished by Elsevier Inc. doi:10.1016/j.jacc.2009.02.065
trIaaa
badcfiuo(tr
hfa(c
That is gold which is worth gold.
—George Herbert, English poet, 1593 to 1633 (1)
ince the introduction of the first positron emission tomogra-hy (PET) scanner in 1975 (2), PET has been used foroninvasive imaging of the heart (3,4). It has often helpedeveal groundbreaking basic science in the areas of myocardiallood flow regulation (5–9), myocardial substrate metabolism10–14), and cardiac autonomic innervation (15–18).
Due to its inherently quantitative nature, its superior detec-ion sensitivity, and its advantageous spatial and temporalesolution over conventional nuclear techniques, PET has beenonsidered a “gold standard” for noninvasive assessment ofyocardial perfusion and viability. In the past, multiple new
maging techniques have been validated with PET as the goldtandard (19–26). And in the near future, PET imaging isxpected to play a key role in the introduction of novel,olecular-targeted imaging approaches (27,28).
rom the Division of Nuclear Medicine/PET, Russell H. Morgan Department ofadiology and Radiological Science, Johns Hopkins University, Baltimore, Maryland.r. Bengel receives research grants from Lantheus Medical Imaging and GEealthcare, and has received speaker honoraria from GE Healthcare, BayerScheringharma, and Siemens Medical Solutions.
iManuscript received November 13, 2008; revised manuscript received January 27,
009, accepted February 23, 2009.
Despite its undisputed value as a high-end diagnosticool, PET has struggled for many years to expand from itsole as a reference standard to broader clinical application.mpeding factors have been the complexity and limitedvailability of PET cameras, the complexity of productionnd delivery of short-lived positron-emitting radiotracers,nd concerns related to the high cost of the test.
Approval of PET radiotracers for clinical cardiac applicationy the U.S. Food and Drug Administration (FDA) in 1989nd 2000, followed by reimbursement of their use for myocar-ial perfusion and viability imaging by the Centers for Medi-are and Medicaid Services (CMS) (Table 1), were importantrst steps toward clinical success (29). In recent years, contin-ous improvement of scanner systems, commercial marketingf the tracers fluorodeoxyglucose (FDG) and rubidium-8282Rb), and increasing availability of the technique, mostly dueo its tremendous success in oncology, have all contributed to aapid growth of PET for clinical cardiac imaging.
Today, many leading nuclear cardiology institutions runigh-throughput PET programs and create further evidenceor its clinical usefulness (30–33). Large sample-size studiesnd randomized trials are underway or have been published34). Industry is introducing novel radiotracers for futureommercialization (35). Technical advances such as hybrid
maging systems (36) and molecular-targeted probes (28)
cacwdcrqtmc
tcmr2iiircit
dbm
bigaEprif
nkaPTaa
P
aspt(firuerr
oNiea9rt8
u1
F
CR
2 Bengel et al. JACC Vol. 54, No. 1, 2009Cardiac PET June 30, 2009:1–15
continue to drive the field for-ward. Based on these develop-ments, the notion that PET is“worth gold” to advance cardio-vascular medicine stays strong.
Part 1: State-of-the-Artin Imaging Technology
Strengths of PET methodology.Beta (�) decay of a nucleus re-sults in emission of a positron,which rapidly annihilates with anelectron, giving off two 511-keVphotons, which travel in oppositedirections. The basic principle ofPET is detection of these pho-tons as coincidences in a ringscanner (Fig. 1A). The spatialresolution of reconstructed clini-cal PET images is currently inthe range of 4 to 7 mm (37), andit is superior to conventional nu-
lear imaging techniques. Superior detection sensitivityllows for identification of radiotracer at nano- to picomolaroncentrations. PET also has high temporal resolution,hich allows for creation of dynamic imaging sequences toescribe tracer kinetics. Together with readily availableorrection algorithms for photon attenuation, scatter, andandom events, these characteristics make PET a trulyuantitative imaging tool that measures absolute concentra-ions of radioactivity in the body and allows for kineticodeling of physiologic parameters such as absolute myo-
ardial blood flow or glucose use.In recent years, several technical innovations have con-
ributed to a steady improvement in the performance oflinical PET systems (Figs. 1B to 1D). New detectoraterials have enhanced coincidence detection yield and
educed system dead time (37). Three- rather than-dimensional coincidence detection is being used to max-mize count yield, improve image statistics, and/or reducenjected dose (38,39). Reconstruction algorithms have beenntroduced that decrease noise and correct for geometry-elated loss of resolution with increasing distance from theenter of the field-of-view (40). All of these advances makemplementation of the time-of-flight (the difference be-ween arrivals of coincidence photons on both sides of the
Abbreviationsand Acronyms
CAD � coronary arterydisease
CFR � coronary flowreserve
CMS � Centers forMedicare and MedicaidServices
CT � computedtomography
FDA � Food and DrugAdministration
FDG � fluorodeoxyglucose
MBF � myocardial bloodflow
PET � positron emissiontomography
SPECT � single-photonemission computedtomography
DA-Approved Cardiac PET Tracers
Table 1 FDA-Approved Cardiac PET Tracers
Tracer Half-LifeTissue Positron
Range (mm) Myocardi82Rb 78 s 2.6 Na/K-ATPase13NH3 10 min 0.7 Diffusion/met18F-FDG 110 min 0.2 Glucose transp
MS � Centers for Medicare and Medicaid Services; FDA � Food and Drug Administration; FDG � fluorodb � rubidium.
etector ring, which is in the range of picoseconds) close toecoming a clinical reality. This will increase spatial infor-ation and improve the signal/noise ratio (37).On the acquisition side, collection of data in list mode has
ecome available for routine use, allowing for multiplemage reconstructions from a single dataset, including static,ated, and dynamic images (Fig. 2). This increases flexibilitynd provides various options for advanced image processing.lectrocardiogram-gated datasets can be created for com-lementary functional analysis (41). The addition of respi-atory gating may allow for creation of “motion-frozen”mages, which will reduce distortion and facilitate correctionor respiratory misalignment (42).
These advantages may be combined with creation of dy-amic imaging sequences for routine measurement of tracerinetics and noninvasive absolute quantification of biologicalnd physiological processes by compartmental modeling (43).ositron-emitting radiotracers for cardiac imaging.able 1 lists current FDA-approved tracers for cardiac PET,
nd Table 2 lists other cardiac tracers that are not FDApproved but have been successfully applied in humans.
ET PERFUSION TRACERS. FDA-approved 82Rb and 13N-mmonia (13NH3) allow for short imaging protocols andame-day repeated studies due to their short half-lives. A PETerfusion study can be readily accomplished in a fraction of theime necessary for single-photon emission tomographySPECT) myocardial perfusion imaging (29,44). 13NH3 has arst-pass extraction of 80% and requires energy for myocardialetention. The images are of high quality and resolution, andptake is linear over a wide range of myocardial blood flowxcept at very high flow rates (45). Imaging with 13NH3
equires either an on-site cyclotron or close proximity to aegional radiopharmaceutical production center.
82Rb is a potassium analog that has a first-pass extractionf 65% and also requires energy for myocardial uptake viaa/K-ATPase. With 82Rb, the extraction fraction decreases
n a nonlinear manner with increasing blood flow, and thisffect is more pronounced when compared with ammonia,lthough still superior when compared with technetium-9m (99mTc)-labeled SPECT compounds (46,47). Imageesolution and quality are somewhat compromised due tohe high energy of positrons emitted during the decay of2Rb and due to lower count rates as a result of theltrashort half-life (Fig. 3). A major advantage of 82Rb over3NH3 is that it is produced by an 82Sr/82Rb generator
ke Mechanism FDA ApprovalCMS Reimbursement
Since
ion) December 1989 March 1995
trapping (perfusion) March 2000 October 2003
xokinase (viability) March 2000 July 2001
al Upta
(perfus
abolic
ort/he
eoxyglucose; Na/K-ATPase � sodium/potassium-ATPase; PET � positron emission tomography;
w8
ec
pm
bdipph
P
gawibu
tduonagsrhRadtttbuttgssw
P
MD
ptssr8woswS
3JACC Vol. 54, No. 1, 2009 Bengel et al.June 30, 2009:1–15 Cardiac PET
ithout the need for a cyclotron. Commercial availability of2Rb generators in the U.S. has been considered a keylement for more widespread application of clinical myo-ardial perfusion PET.
Another well-established perfusion tracer, H215O, is
otentially superior to 82Rb and 13NH3 because it is
e +
e -Positron
(Neutrino)
Electron(511keV) γ (511keV)
A
B
t2
t1
TOF
No TOF
C D
γ
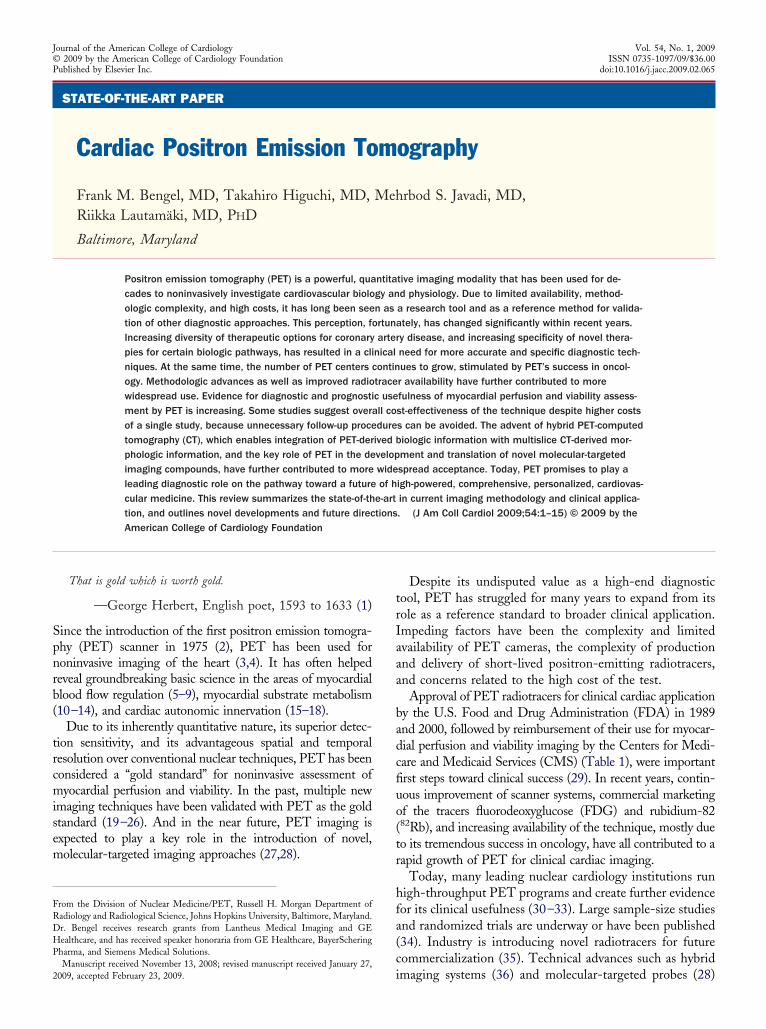
Figure 1 Advances in PET Technology
(A) Basic positron emission tomography (PET) principle: a positron (e�) isemitted from the atomic nucleus together with a neutrino. The positron movesrandomly through the surrounding matter, where it hits electrons (e�) until itfinally loses enough energy to interact with a single electron. This process,called “annihilation,” results in 2 diametrically emitted photons with an energyof 511 keV each. These photons are detected as coincidences in the detectorring of the PET camera. (B) Traditional 2-dimensional imaging (left) uses onlycoincidences that occur within the same axial detector ring. Adjacent detectorrings are separated by septa. Advanced 3-dimensional imaging (right) usescoincidences from all possible detector pairs. This increases sensitivity andcount density but is demanding and requires correction for the higher amountof scatter and inhomogeneity at the axial edge of the field of view. (C) Inhomo-geneity of in-plane spatial resolution is a function of a broader line of responsefor detector pairs toward the edge of the field of view (pink line vs. blue line).System matrix resolution modeling has been developed to correct for thiseffect and increase resolution. (D) Time-of-flight (TOF) PET increases the signal-to-noise ratio. This has become a reality since the introduction of novel detec-tors with high time resolution of 500 picoseconds or less. In traditional non-TOF PET, the only spatial information is derived from the line of response ofthe detector pair (green). The system has to assume that the annihilation mayhave occurred anywhere along this line of response. However, if TOF informa-tion is available, location of annihilation can be narrowed to several centime-ters along the line of response (red), by taking into account the time differencebetween arrivals of coincidence photons at opposite detectors (t1–t2).
etabolically inert and freely diffusible across cell mem- h
ranes. However, the tracer is not accumulated in myocar-ium and instead reaches equilibrium between extra- andntravascular compartments. Images of regional myocardialerfusion are not readily obtained, and processing for bloodool subtraction is needed (6). The lack of FDA approvalas limited this compound to research applications in the U.S.
ET VIABILITY TRACERS. 18F-FDG is an FDA-approvedlucose analogue that is widely available due to its success asmetabolic imaging tracer in clinical oncology. The tracer isell established to determine myocardial glucose use as an
ndicator of myocardial viability. Increased FDG uptake cane observed in ischemic tissue; markedly reduced or absentptake indicates scar formation (11,48).FDG uptake is heterogeneous in normal myocardium in
he fasting state, so oral glucose loading, nicotinic aciderivatives, or infusion of insulin and glucose have beensed to enhance myocardial FDG uptake (44,49). Imagesbtained in nondiabetic patients and in patients withoninsulin-dependent diabetes are of higher quality afterdditional insulin infusion than those obtained after orallucose loading alone. Bolus injections of insulin have beenuggested (44,50). When such protocols for patient prepa-ation are followed, cardiac FDG images are generally ofigh diagnostic quality.adiation exposure. Radiation exposure from cardiac im-
ging procedures has increasingly become a matter ofiscussion (51). An in-depth review of this topic is beyondhe scope of this article, and the interested reader is referredo dedicated literature (51). It should be noted, however,hat positron emitting tracers typically provide less radiationurden to the patient when compared with SPECT tracerssed for the same diagnostic purpose, which is, in part, dueo their much shorter half-lives. Also, the radiation burdeno staff involved in cardiac PET imaging has been investi-ated, and due to differences in radiotracer administration,can acquisition, and stress-testing tasks, doses with PETeem to be lower for staff (as for patients) when comparedith single-photon emitting tracers (52).
art 2: State-of-the-Art in Clinical Application
yocardial perfusion. DIAGNOSIS OF CORONARY ARTERY
ISEASE (CAD). In a 2005 review, 8 studies that comparederfusion PET with coronary angiography, representing aotal of nearly 800 patients, were summarized, and a meanensitivity of 93% and specificity of 92% for detection ofignificant CAD were observed (29). A more recent review,eporting a weighted sensitivity of 90% and specificity of9% from 9 studies including 877 patients, scanned mostlyith 82Rb PET, confirmed these results (36). For detectionf myocardial ischemia, myocardial perfusion PET is con-idered to have superior diagnostic accuracy when comparedith the more widely available and more frequently usedPECT technique (Fig. 4).Available published reports comparing PET and SPECT
ave also been recently reviewed (36). The robust methods

fffipftrfehtpuao
P
hgpmaalnt
o8
m0appihdoaenptaf
A
m(Pmi
4 Bengel et al. JACC Vol. 54, No. 1, 2009Cardiac PET June 30, 2009:1–15
or attenuation correction with PET reduce the number ofalse-positive scans due to attenuation artefacts, and speci-city is increased. This is of particular importance in obeseopulations and women, where attenuation artefacts arerequent. Perfusion PET also tends to be more sensitivehan SPECT, which can be explained by better spatialesolution and better tracer extraction at high flow, allowingor detection of more subtle perfusion abnormalities. How-ver, the existing literature comparing SPECT and PETas either been published before 1992 or compared bothechniques in different, retrospectively matched groups. Arospective head-to-head comparison or randomized studysing current state-of-the-art for both techniques is missingnd would be desirable to further support the superiorityf PET.
ROGNOSTIC VALUE. Although meta-analyses confirm a veryigh diagnostic accuracy, it should be emphasized that thereatest value of perfusion imaging is considered to be itsotential to predict adverse cardiac events (53). This incre-ental outcome information has been shown to be useful asgatekeeper for invasive procedures and as a guide to
ppropriate therapy based on individual risk. Studies in veryarge patient groups have supported the incremental prog-ostic value for SPECT perfusion imaging, and confirma-
Time after injection
Resp
iratory
cycle
Cardiac
cycle
Cardiac
cycle
A Static
C ECG-Gated
ED
ED
ES
Prescan delay
Figure 2 Multidimensional List-Mode PET Acquisition
Scanner coincidences are continuously recorded along with information about thebreathing position (optional). Data can then be resampled in multiple formats at aall information after a pre-defined pre-scan delay (delay time after tracer injection).times after injection. This is used for tracer kinetic analysis. (C) Electrocardiograpventricular function. (D) Respiratory gated images can be obtained at different phatole; ES � end systole; EXSP � expiratory phase; INSP � inspiratory phase; PET �
ory data for myocardial perfusion PET are also available. In p
ne study, 685 patients were scanned with dipyridamole2Rb PET and follow-up was obtained over a mean of 41onths. The annual mortality rate for a normal scan was
.9%; it was 4.3% for an abnormal scan. After a multivariatenalysis, PET results had an independent and incrementalrognostic value (54). In a more recent study in 367atients, 3 groups with different stress perfusion abnormal-ties (normal, mild, moderate to severe) had annual rates ofard event of 0.4%, 2.3%, and 7%, respectively, and PETata were the strongest predictors of total cardiac events. Inbese patients, a preferred target group for PET imagingnd a group of individuals at higher risk, the annual totalvent rate was 11% with an abnormal scan and 1.5% with aormal scan (32). Another very recent study confirmed therognostic value of dipyridamole 82Rb PET in 1,441 pa-ients with suspected or known CAD, and it demonstratedn incremental value of stress left ventricular ejectionraction from gated PET (55).
BSOLUTE FLOW QUANTIFICATION. The ability to quantifyyocardial blood flow (MBF) and coronary flow reserve
CFR) in absolute terms is another powerful feature ofET. This is achieved by compartmental modeling ofultiframe dynamic acquisitions (47,56–60), and it has
nitially been limited to research applications in selected
Time after injection
Resp
iratory
Dynamic
Respiratory Gating
INSP
EXSP
EXSP
fter the start of acquisition, the electrocardiographic signal, and the signal aboute of the acquisition. (A) High-count static images are reconstructed by summingynamic imaging sequences are obtained by serial temporal sampling at differentgated images are obtained at multiple phases of the cardiac cycle to assessf the breathing cycle in order to correct for respiratory motion. ED � end dias-tron emission tomography.
cycle
B
D
time any tim(B) D
hicallyses o
posi
opulations. Early studies showed adverse effects on CFR
fsmsts
earqpp
cicaeubmcrTmilor
S
cMs
OW
Fe
5JACC Vol. 54, No. 1, 2009 Bengel et al.June 30, 2009:1–15 Cardiac PET
or multiple risk factors such as hyperlipidemia, diabetes, ormoking and supported the beneficial effects of risk-factorodifications and novel medical therapies (61–73). These
tudies have contributed to a paradigm shift in the percep-ion of CAD, away from a pure macroscopic view of luminaltenoses and toward an emphasis on microcirculation and
82Rb
13NH3
18F-FBnTP
SA VLA HLA
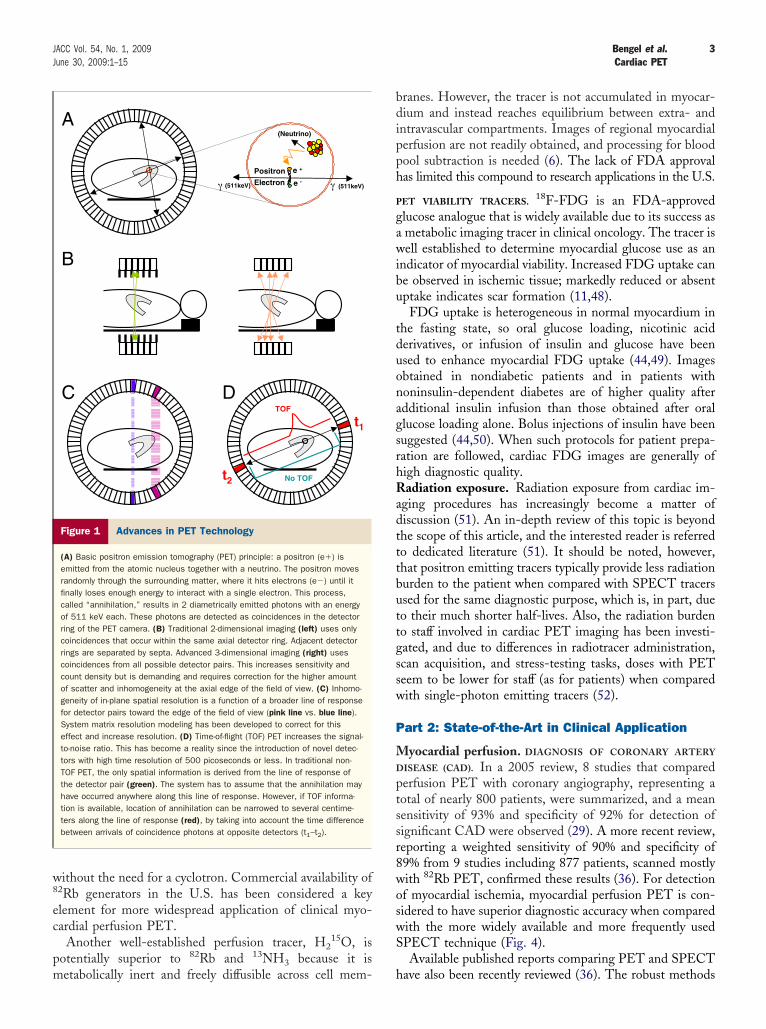
Figure 3 PET Perfusion Tracers
Tomographic positron emission tomography (PET) images of myocardial perfusionafter administration of adenosine using 3 different tracers, the Food and DrugAdministration-approved agents 82rubidium (82Rb) (top) and 13N-ammonia (13NH3)(middle), and the novel compound 18F-fluorobenzyl-triphenylphosphonium (18F-FBnTP) (bottom). All images were obtained in a dog model of hemodynamicallyrelevant left circumflex coronary artery stenosis, resulting in reduced perfusion ofinferolateral myocardium, as shown by all 3 tracers. Since the canine cardiac anat-omy is different from human anatomy, the septum is displayed more superiorly inshort axis (SA) images. HLA � horizontal long axis; VLA � vertical long axis.
ther Cardiac PET Tracersith Reported Human Application
Table 2 Other Cardiac PET TracersWith Reported Human Application
Tracer Half-Life, min Myocardial Uptake Mechanism
H215O 2 Free diffusion (perfusion)
62Cu-PTSM 9.7 Intracellular binding (perfusion)18F-BMS747158 110 Mitochondrial binding (perfusion)11C-acetate 20 Krebs cycle flux, oxidative metabolism11C-palmitate 20 Fatty acid metabolism11C-glucose 20 Glucose metabolism18F-FTHA 110 Fatty acid uptake11C-hydroxyephedrine 20 Sympathetic neuronal catecholamine
uptake11C-epinephrine 20 Sympathetic neuronal catecholamine
storage11C-phenylephrine 20 Sympathetic neuronal catecholamine
turnover18F-fluorodopamine 110 Sympathetic neuronal uptake and
function11C-CGP12177 20 �-adrenergic receptor density11C-CGP12388 20 �-adrenergic receptor density11C-GB67 20 �1-adrenergic receptor density11C-MQNB 20 Muscarinic receptor density
THA � fluorothiaheptadecanoic acid; MQNB � methylquinuclidinyl benzilate; PET � positronmission tomography; PTSM � pyruvaldehyde bis(N4-methylthiosemicarbazone).
s
ndothelial function. These are both determinants of CFRnd MBF and are key mediators of disease progression andisk. Several studies have suggested the prognostic value ofuantitative PET measurements of MBF and CFR forrogression toward clinically overt CAD (74) and in idio-athic and hypertropic cardiomyopathies (75,76).The growing use of myocardial perfusion PET for the
linical workup of CAD has resulted in stronger efforts tonclude absolute flow quantification in the analysis oflinical studies. Technical improvements (i.e., more rapidnd robust processing and analysis of dynamic data) havexpedited these efforts. Algorithms for the most frequentlysed clinical cardiac PET tracer, 82Rb, are increasinglyeing validated and used (43,47,60). Quantitative floweasurements may be useful and complementary to the
urrent standard of visual/semiquantitative analysis. Theireproducibility has been demonstrated repeatedly (77–79).hey may be useful for detection and evaluation of extensiveultivessel CAD with balanced ischemia on qualitative
mages (80) (Fig. 5), evaluation of the significance of a givenesion (81), evaluation of collateral flow (82), identificationf endothelial dysfunction in pre-clinical disease, as well aseliable monitoring of therapeutic strategies.
UMMARY. Table 3 summarizes the evidence and potentiallinical role of PET myocardial perfusion imaging.
yocardial viability. CLINICAL VALUE. Therapeutic deci-ion making is difficult in patients with advanced CAD and
99mTc-MIBI SPECT 82Rb PET
Stress
Rest
Stress
Rest
A
B
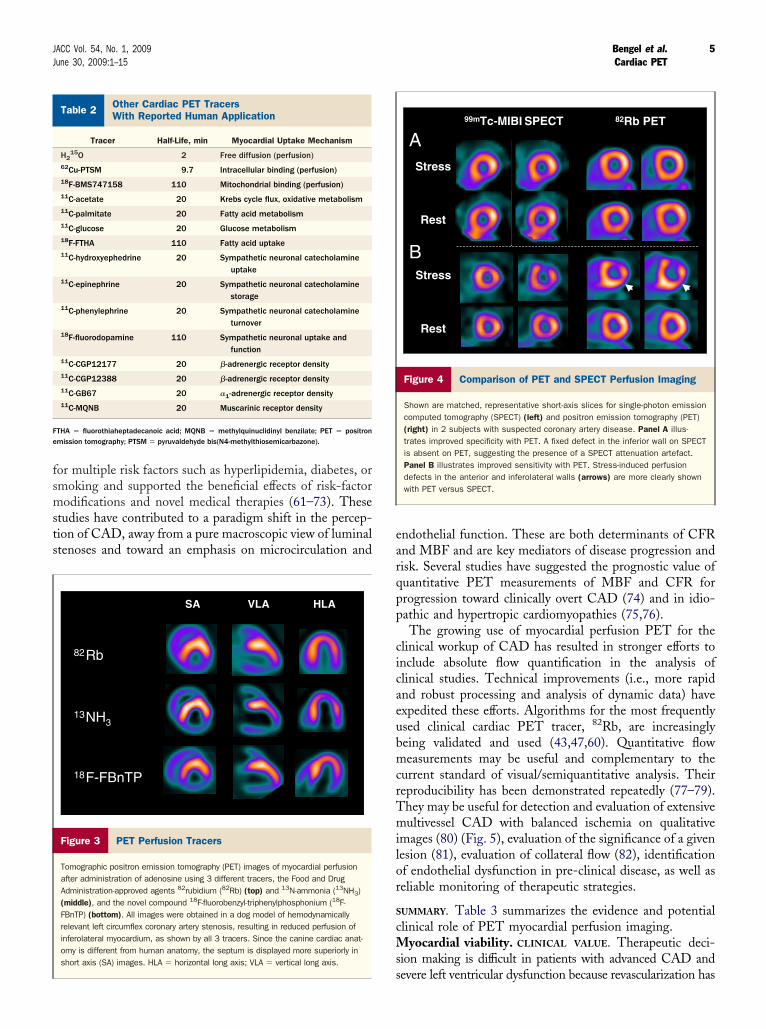
Figure 4 Comparison of PET and SPECT Perfusion Imaging
Shown are matched, representative short-axis slices for single-photon emissioncomputed tomography (SPECT) (left) and positron emission tomography (PET)(right) in 2 subjects with suspected coronary artery disease. Panel A illus-trates improved specificity with PET. A fixed defect in the inferior wall on SPECTis absent on PET, suggesting the presence of a SPECT attenuation artefact.Panel B illustrates improved sensitivity with PET. Stress-induced perfusiondefects in the anterior and inferolateral walls (arrows) are more clearly shownwith PET versus SPECT.
evere left ventricular dysfunction because revascularization has

aoItedteTcd
twrveof
ibr
rr2srp
wbdcaPo
6 Bengel et al. JACC Vol. 54, No. 1, 2009Cardiac PET June 30, 2009:1–15
high procedure-related risk. Viability testing has been devel-ped to serve as a guide to the most appropriate therapy.nitially, PET techniques played a key role in understandinghe myocardial response to severe ischemic damage and instablishing the identification of myocardial viability as aiagnostic target. Metabolic imaging has been used to supporthe notion that assessment of perfusion alone may not benough to predict functional recovery after revascularization.he pathophysiology of hibernating myocardium has been
haracterized by PET imaging as resting hypoperfusion andysfunction with preserved glucose metabolism (11) (Fig. 6).It is now well known that PET, using the metabolic
racer FDG, is accurate to predict improvement of regionalall motion and global left ventricular ejection fraction after
evascularization. When comparing PET with alternativeiability imaging techniques such as low-dose dobutaminechocardiography, SPECT imaging with perfusion tracers,r delayed enhancement magnetic resonance imaging, dif-
Qualitative Perfusio
Stress
Rest
SA VLA H
L fo %0010
Stress
Rest
SA VLA
A
B
Figure 5 Flow Quantification by PET
Qualitative and quantitative assessment of myocardial perfusion by rest/dipyridamand (B) in a subject with angiographically proven triple-vessel disease and balanceual left ventricular (LV) maximum and show no significant regional perfusion heterodynamic images (right), are all normalized to the same flow range of 0 to 3 ml/mreserve. Abbreviations as in Figure 3.
erences exist that are mostly related to the pathophysiolog- w
cal target of each imaging test. A detailed comparisonetween techniques is beyond the scope of this article, andeaders are referred to dedicated reviews (83–85).
PET is most predictive of improvement of function afterevascularization when blood flow is reduced by �50%, withelatively high glucose uptake. A recent pooled analysis of4 studies in 756 patients, demonstrated a weighted meanensitivity and specificity of 92% and 63%, respectively, foregional functional recovery, with positive and negativeredictive values of 74% and 87%, respectively (85).It has been shown that it is critical to revascularize patients
ith PET-defined hibernating myocardium as soon as possibleecause improvement is less likely to occur when surgery iselayed after documentation of dysfunctional but viable myo-ardium (86). This has recently been confirmed in a large studynalyzing more than 700 patients who all underwent 18F-FDGET. Patients with rapid intervention had significantly betterutcomes when compared with a propensity-matched group
Quantitative Flow
g/nim/lm 30
Polarmaps
1.2 ml/min/g
Flow Reserve: 1.2
1.0 ml/min/g
LV Average
2.3 ml/min/g
Flow Reserve: 3.3
0.7 ml/min/g
ress and 82Rb PET (A) in a subject with low likelihood of coronary artery disease,emia. Qualitative static tomographic images (left) are normalized to the individ-
ty in either case. Polar maps of absolute myocardial blood flow, determined fromnd show significant reduction of stress flow in B, resulting in blunted flow
n
LA
xaM V
HLA
ole std ischgenei
in/g a
ith delayed or no intervention (33).

ppsitmfmftuv
R
Ped(fistci
piHsn
pbspscPnaPsttAsisvl
S
c
CS
P
7JACC Vol. 54, No. 1, 2009 Bengel et al.June 30, 2009:1–15 Cardiac PET
Other studies have shown that PET can also be used toredict improvement of heart failure symptoms and im-rovement of exercise capacity (87). Several retrospectivetudies have focused on the outcome of patients withschemic heart disease and ventricular dysfunction relative toheir PET results and their treatment strategy. A recenteta-analysis summarized 10 studies in 1,046 patients and
ound annualized mortality rates of 4% for those with viableyocardium who underwent revascularization versus 17%
or those with viability who did not undergo revasculariza-ion. The mortality was 6% for those without viabilityndergoing revascularization versus 8% for those withoutiability not undergoing revascularization (85).
ANDOMIZED TRIALS. Assessment of myocardial viability byET is one of the few diagnostic approaches that have beenxplored in randomized diagnostic studies. Such studies areifficult to design because therapeutic decision makingwhich will influence outcome) is difficult to control. Theeld should be commended for having conducted suchtudies. Despite the strength of randomization, results ofhese studies must be interpreted with caution. Inclusionriteria as well as management algorithms need to be taken
linical Myocardial Perfusion PET:ummary of Evidence and Potential Clinical Role
Table 3 Clinical Myocardial Perfusion PET:Summary of Evidence and Potential Clinical Role
Imaging technique High temporal resolution enables dynamic imagingand absolute blood flow quantification.
Spatial resolution superior to SPECT.Well-established attenuation correction increases
specificity.
Radiotracers Extraction fraction superior to SPECT tracers (44–46).Short half-life enables shorter imaging protocols and
lower radiation exposure, but complicates use ofexercise stress (vasodilator stress preferred) (28).
Diagnostic accuracy Meta-analyses suggest sensitivity and specificity fordetection of coronary artery stenosis is around90% (28,35).
Comparison to SPECT suggests superiority (35), butrecent prospective head-to-head comparison is notavailable.
Prognostic value Predictive of risk for cardiac events, supported bysome studies (30,31,54,55). Less evidence tosupport PET when compared with SPECT.
Cost-effectiveness Some older studies support cost savings despite highsingle-test costs (93,94); more recent analyses arenot available.
Superior accuracy helps avoid unnecessarysubsequent procedures (95).
Randomized trials None available.
Suggestions forcurrent clinical use
Second-line test after equivocal SPECT or otherequivocal perfusion studies.
First-line test in groups where SPECT is frequentlyequivocal (obese patients).
First-line test in situations where quantification andreproducibility are important (suspected balancedischemia, longitudinal follow up studies) (76–78).
Potential future use May be used as first-line test in all cases if diagnosticsuperiority to SPECT is confirmed in head-to-heador randomized trials and if cost-effectiveness isproven in the present health care environment.
ET � positron emission tomography; SPECT � single-photon emission computed tomography.
nto consideration. One early randomized study assigned
atients to either SPECT or PET and found no differencen accuracy between techniques for viability assessment (88).
owever, the study included patients with relatively pre-erved ejection fractions, where differences between tech-iques may be minimal.The benefits of PET are expected to be greater in a target
opulation with severe heart failure and an ejection fractionelow 35%. A group of patients fulfilling these criteria wastudied in another recent randomized trial that assigned 430atients to either management assisted by FDG PET ortandard care. The study overall showed only a nonsignifi-ant trend toward reduction in cardiac events for FDGET-assisted management versus standard care. But iteeds to be emphasized that alternative viability testing wasllowed in the control arm and that nonadherence toET-based recommendations was found in a significantubfraction of patients in the PET arm. Importantly, inhose who adhered to PET recommendations regardingherapy, significant survival benefits were observed (34).lthough PET has been used in large and powerful viability
tudies, the results of these studies are still controversial andt is difficult to find a unifying conclusion. The evidence inupport of the usefulness of PET is growing, but the use ofiability imaging at a given center is still defined mostly byocal expertise and availability.
UMMARY. Table 4 summarizes the evidence and potentiallinical role of PET myocardial viability imaging.
Match
Mismatch
SA VLA HLA
Metabolism(18F-FDG)
Perfusion(82Rb, Rest)
Perfusion(82Rb, Rest)
Metabolism(18F-FDG)
Figure 6 PET Perfusion/Metabolism Imagingfor Assessment of Myocardial Viability
(Top) A mismatch with reduced rest perfusion (measured by 82Rb) and pre-served/increased metabolism (measured by 18F-FDG) is shown in the inferolat-eral wall, indicating ischemically compromised but viable “hibernating”myocardium. (Bottom) A matched perfusion/metabolism defect is shown inthe inferior wall, indicating nonviable scar. FDG � 18F-deoxyglucose; otherabbreviations as in Figure 3.

OPtamciasn
Cortriamt
soioscfvqfo
cSTuwatlCdfwecb
o1wTdr
mttbptmvrO
CMP
Ffit
8 Bengel et al. JACC Vol. 54, No. 1, 2009Cardiac PET June 30, 2009:1–15
ther clinical applications. Apart from its use in CAD,ET has also been used for less frequent diseases involving
he heart and cardiovascular system. Low radiation exposurend short imaging protocols make it attractive for assess-ent of perfusion and metabolism in selected pediatric
ardiac patients (89,90). Also, the ability to do whole bodymaging in addition to dedicated cardiac imaging makes itttractive for evaluation of systemic inflammatory diseaseuch as sarcoidosis, in which cardiac involvement is prog-
linical Use of PET Imaging for Assessment ofyocardial Viability: Summary of Evidence andotential Clinical Role
Table 4Clinical Use of PET Imaging for Assessment ofMyocardial Viability: Summary of Evidence andPotential Clinical Role
Imaging technique Spatial resolution superior to SPECT but inferior toMRI or echocardiography.
Well-established attenuation correction increasesspecificity.
Radiotracers Metabolic tracer 18F-FDG indicates preservedglucose use in ischemically compromised butviable myocardium.
Should be combined with a perfusion study.Metabolic preconditioning required (glucose
and/or insulin).
Diagnostic accuracy Meta-analyses suggest sensitivity around 90% andspecificity of 60% to 70% for prediction ofregional functional recovery afterrevascularization (83–85).
Targeted biomechanism needs to be consideredfor comparison with other techniques(metabolism may be preserved whencontractile reserve is already absent, explaininglower specificity but higher sensitivity whencompared with functional techniques usinglow-dose dobutamine) (83).
Prognostic value Supported by many retrospective studies (85).Predictive of functional and symptomatic
improvement.Better overall outcome for revascularized vs.
nonrevascularized when PET used to determineviable myocardium.
Cost-effectiveness Limited evidence (guidance to appropriate therapymay improve medical care and costs).
Randomized trials Randomized comparison to SPECT failed to showsuperiority, probably due to inclusion ofpatients with higher ejection fraction (88).
PARR2 trial: No significant difference betweenPET-assisted and standard care in general, butsignificant benefit when PET recommendationswere followed (33).
Suggestions for currentclinical use
Type of viability testing still depends on localexpertise and availability.
First-line test in severely impaired ischemicLV dysfunction (LVEF �35%); most beneficialwhen adherence to results is achieved.
Second-line test if therapeutic decision remainsdifficult after a first test.
Potential future use May be used more broadly if cost-effectivenessis proven.
May be integrated into diagnostic algorithms withother tests such as MRI or echocardiography,but requires prospective validation.
DG � fluorine-18-fluoro-deoxyglucose; LV � left ventricular; LVEF � left ventricular ejectionraction; MRI � magnetic resonance imaging; PARR � PET and Recovery Following Revascular-zation; PET � positron emission tomography; SPECT � single-photon emission computedomography.
ostically very relevant (91,92). m
ost-effectiveness considerations. In cardiology, imagingptions are extensive and often redundant. Because financialesources in health care are increasingly limited, the ques-ion of cost-effectiveness is crucial. The value of PET as aesearch tool and as a gold standard for other diagnosticmaging techniques is not in question, but reimbursementnd general clinical application of the technique is underore scrutiny because a PET procedure is more expensive
han other noninvasive procedures.Looking only at the costs of a single test is a short-
ighted, incomplete approach. Estimation of the total costf diagnostic tests for CAD requires consideration ofndirect and induced costs of management algorithms basedn the test. False positives may result in unnecessaryubsequent diagnostic or therapeutic procedures, whicharry additional costs and risks. A missed diagnosis due to aalse-negative test, on the other hand, may result in pre-entable adverse events that could impair life duration anduality. A comprehensive analysis of utility has to accountor the impact of medical care on quality as well as quantityf life.Patterson et al. (93) used a mathematical model to
ompare cost-effectiveness of exercise electrocardiography,PECT, PET, and invasive angiography to diagnose CAD.heir model accounted for costs per effect or cost per utilitynit (including cost of diagnostic and therapeutic measures,hich included those that yield false-positive results as well
s those that yield false-negative results). They observedhat PET, despite the high cost of a single test, shows theowest cost per effect in patients with a pre-test likelihood ofAD below 70%. This was attributed to its superioriagnostic accuracy and avoidance of false-positive andalse-negative studies. Only when the pre-test likelihoodas above 70% was direct angiography the most cost-
ffective approach. Gould et al. (94), using a somewhat lessomplex model, had earlier come to similar conclusions, butoth studies were published more than 13 years ago.Merhige et al. (95) more recently compared the frequency
f diagnostic arteriography, revascularization, costs, and-year clinical outcomes in 2,159 patients studied with PETith an internal and an external SPECT control group.hey showed reduced use of downstream invasive proce-ures when using perfusion PET versus SPECT, whichesulted in lower costs with comparable outcomes.
Similar issues need to be considered for PET imaging ofyocardial viability. The costs of a single test are high, but
he costs and risk of avoidable surgical or interventionalreatment may be even higher. Avoidance of an unnecessaryypass operation, or even of an unnecessary cardiac trans-lantation, may justify conducting numerous noninvasiveests if they are appropriate for guidance of clinical decisionaking. It has clearly been shown that PET assessment of
iability influences decision making (96), and if PETecommendations are followed, outcomes will improve (34).ne study in the United Kingdom applied an economic
odel and compared 3 strategies (bypass for all patients,
mfmv
cpibruau
ea(seSdh
P
HaoTrcoPch
rmpsCa
cpTwcaf
ipptl
rPw2Pms
uacwPC
tsittoianbsilahioNplttcosgrhe1siPwc
ctfii
9JACC Vol. 54, No. 1, 2009 Bengel et al.June 30, 2009:1–15 Cardiac PET
edical therapy for all patients, and PET-guided decisionor bypass or medical therapy). It was concluded that PETay be cost-effective to select patients with poor left
entricular function for coronary artery bypass grafting (97).Hence, there is some evidence for cost-effectiveness of
ardiac PET in the clinical setting. Factors such as higheratient throughput and patient comfort due to shortermaging protocols for PET versus SPECT have not eveneen considered in the above analyses. But cost-effectivenessemains complex and difficult to generalize. Further studiessing updated clinical algorithms and updated values forccuracy and procedure costs are necessary to support these of PET in the actual health care environment.Target populations in which perfusion PET may be
specially cost-effective are obese patients and women,lthough it should be noted that computed tomographyCT) angiography may emerge as a competitor to PET inuch situations (98). For viability imaging, end-stage isch-mic cardiomyopathy may be the most useful situation.tudying cost-effectiveness in these specific groups in moreetail might further support an efficient clinical use of theigh-end technique.
art 3: New Developments and Future Directions
ybrid PET-CT: the merging of morphology, functionnd biology. Due to their success in oncology, all currentlyffered PET imaging systems are hybrid PET-CT scanners.his has brought challenges for cardiac imaging that are
elated mainly to the use of a separate CT for attenuationorrection of subsequently acquired PET data. Respiratoryr patient motion may result in misalignment of CT andET and artificial heterogeneity in CT-attenuation–orrected cardiac PET images (99). Corrective algorithmsave been proposed to address this issue (99–101).More importantly, the advent of hybrid PET-CT has
esulted in the unique opportunity to combine CT-derivedorphologic information with PET-derived functional,
hysiological and biological information. Most PET-CTcanners are now equipped with multislice CT, allowing forT measurement of coronary calcium and/or CT coronary
ngiography in addition to PET imaging procedures.Schenker et al. (31) measured myocardial perfusion and
oronary calcium in a single cardiac PET-CT study in 695atients with an intermediate pre-test likelihood of CAD.hey observed an increasing prevalence of abnormal PETith increasing coronary calcium scores. In about 50% of
ases with very high calcium, myocardial perfusion wasbnormal. But interestingly, abnormal perfusion was alsoound in 16% of patients with absent calcium.
Risk-adjusted survival analysis demonstrated a stepwisencrease in cardiac events with increasing calcium scores inatients with and without ischemia on PET. Amongatients with normal PET myocardial perfusion imaging,he annualized event rate in patients with no calcium was
ower than in those with high calcium (2.6% vs. 12.3%, tespectively). In patients with ischemia demonstrated onET, the annualized event rate in those with no calciumas also lower than in those with high calcium (8.2% vs.2.1%). These data suggest that CT calcium scoring andET perfusion imaging are complementary for the assess-ent of cardiovascular risk. Both can be integrated to
tratify patients into different risk-based categories.There is less evidence at the moment for the integrated
se of CT coronary angiography and perfusion PET,lthough initial studies suggest that both tests may also beomplementary rather than competitive. Not all patientsith obstructive atherosclerosis on CT show ischemia onET and, vice versa, not all patients with nonobstructiveAD have no perfusion abnormalities (102).Contrast-enhanced CT angiography enables the detec-
ion of noncalcified plaque and, if imaging is repeatedeveral minutes after injection, it may allow for detection ofnfarcts by delayed contrast enhancement (103,104). Howhis information is best combined with PET for maximiza-ion of diagnostic and prognostic accuracy will be a matterf further research in the future. It is likely, however, thatncreasing availability of 64-slice CT in PET-CT systems,long with new prospectively gated CT acquisition tech-iques, which lower radiation exposure for CT angiographyy more than 70% (105), will contribute to a more wide-pread use in hybrid PET-CT protocols (Fig. 7). Innovativentegrated imaging protocols may include CT for morpho-ogic assessment of coronary arteries and PET for functionalssessment of myocardial blood flow. A CT delayed en-ancement study may be done after CT angiography to
dentify the presence or absence of scar (104). This maybviate the need for a rest perfusion study.ovel myocardial perfusion tracers. All established PET
erfusion tracers have half-lives that are very short. Thisimits their applicability for exercise stress, so clinical pro-ocols usually use pharmacologic stress with the patient onhe camera table, followed by immediate imaging. Anotheronsequence of the short half-lives is the limited availabilityf tracers because they require an on-site cyclotron or aignificant financial commitment to a strontium/rubidiumenerator, which needs to be replaced every month andequires high-throughput imaging to be cost-effective. Thisas generated interest in fluorine-18-labeled perfusion trac-rs, which may overcome both problems due to a longer,10-min half-life. Like FDG, which has already beenuccessfully commercialized, these tracers can be producedn regional centers for dose-by-dose delivery to multipleET sites. Also, they may be injected during exercise stressith enough time to move the patient to the camera after
ompletion of the stress protocol.Currently, data are available on 2 18F-labeled perfusion
ompounds. 18F-BMS747158 is a pyridazinone derivativehat avidly binds to mitochondrial complex-1 (106). Itsrst-pass extraction fraction is very high at 94% (107), and
t yields high and stable myocardial uptake that is propor-
ional to myocardial blood flow. Myocardial uptake is
g9
mt
opctbatMrsuDkmos
nprc
ro(aepiidfau
ti
10 Bengel et al. JACC Vol. 54, No. 1, 2009Cardiac PET June 30, 2009:1–15
reater than that of the SPECT tracers thallium-201 and9mTc-sestamibi (35). The compound is very promising foryocardial perfusion PET imaging and it is currently being
ested in clinical phase 1 and 2 studies (Fig. 8).18F-fluorobenzyl triphenyl phosphonium (FBnTP) is an-
ther compound that is taken up rapidly by myocardium inroportion to myocardial blood flow (108), with highontrast that is superior to the SPECT tracer 99mTc-etrofosmin. It also targets mitochondria (109) and seems toe promising for myocardial perfusion imaging (Fig. 3),lthough, unlike BMS747158, it has not entered clinicalrials yet.
olecular imaging. Cardiovascular molecular imaging is aapidly emerging discipline that aims toward visualization ofpecific molecular targets and pathways that precede ornderlie changes in morphology, physiology, and function.ue to its high detection sensitivity, PET is considered a
ey player in the development and introduction of novelolecular-targeted imaging approaches. The introduction
f dedicated small animal imaging systems, which allow for
anterior
lateral
Obliqu
Ramus Int
CT Angiography
Figure 7 Hybrid PET-CT Imaging
Integrated assessment of vascular anatomy and myocardial perfusion using hybridonset of chest pain after 4� coronary artery bypass grafting. Anterior and lateral vthe left internal mammary artery graft (only clips, indicated by white arrows, are vises). The most severe native coronary lesion is found in a ramus intermedius, whsoft plaque in the proximal segment). Fusion images of CT anatomy and stress pehighlight a mild perfusion defect in the territory of the ramus intermedius as the p
erial in vivo imaging in rodents and facilitate translation of e
ew diagnostic compounds from experimental to clinicalractice (Fig. 9), has further contributed to increasingecognition of the future potential of molecular imaging inardiovascular research and patient care (110–113).
Due to the wide spectrum of novel approaches, a detailedeview of PET-based molecular imaging is beyond the scopef this article, and the reader is referred to dedicated articles27,28,114,115). Some key principles and some examplesre highlighted below. First, molecular imaging places anmphasis on the diagnosis (and subsequent treatment) ofrecursors or the earliest stages of the disease, as opposed tots sequelae. Examples are the use of neuronal imaging todentify subjects at risk for ventricular arrhythmia (116), theevelopment of compounds targeting plaque vulnerability be-ore rupture and subsequent myocardial infarction (117,118),nd the targeting of biomechanisms that precede left ventric-lar remodeling and development of heart failure (119,120).
Second, molecular imaging has great potential to facili-ate discovery and development of novel therapies throughmproved target identification and implementation of more
anterior
lateral
w
dius
Stress PET/CT Fusion
on emission tomography (PET)-computed tomography (CT) in a patient with newrendered CT angiographic images are shown on the left and indicate failure ofd), and failure of venous grafts (white arrows show occluded aortic anastomo-urther illustrated by a curved oblique view in the center (yellow arrow shows a
measured by dipyridamole 82Rb PET are shown on the right. Green arrowse correlate of the patient’s symptoms.
e Vie
erme
positrolumesualizeich is frfusionrobabl
fficient end points for clinical trials. Examples are the

mfib
sc
11JACC Vol. 54, No. 1, 2009 Bengel et al.June 30, 2009:1–15 Cardiac PET
easurement of myocardial efficiency to identify the bene-ts of therapies for heart failure (121,122) and imaging theeneficial effects of metabolic interventions (123).
18F-BMS747158 PE
ExerciseStress
Rest
SA VLA
Figure 8 PET-CT Perfusion Imaging at Rest and With Physical E
The injected dose was 1.5 mCi at rest and 3.5 mCi at peak stress. Shown are staas well as PET-CT fusion images documenting good alignment of PET and CT (righphase-1 study in healthy volunteers. Abbreviations as in Figures 3 and 7.
mc 01
A
B
11C-Ep
Figure 9 Translational Molecular Cardiac PET Imaging
Shown are representative midventricular short-axis slices of myocardial sympathetFor size comparison, images are shown at the same scale (A) and after zoomingner and the rat heart with a dedicated small animal scanner.
Third, visualization of cellular and subcellular targettructures has contributed to advances in fundamentalardiac research such as cell trafficking, myocardial regen-
PET-CT
coronalaxial
ise Using the Novel 18F-Labeled Compound BMS747158
enuation-corrected PET images acquired from 5 to 10 min after injection (left),t and stress studies were obtained on subsequent days as part of a clinical
mc 1mc 01
phrine PET
rvation imaged with 11C-epinephrine, in the healthy human, pig, and rat heart.parable image size (B). Human and pig hearts were imaged with a clinical scan-
T
HLA
xerc
tic attt). Res
ine
ic inneto com

epil(
mardp
wdktSAaartoatSiwAPbbdbhis
S
CiavishC
ip
ATDf
RDDkm
R
12 Bengel et al. JACC Vol. 54, No. 1, 2009Cardiac PET June 30, 2009:1–15
ration, and heart failure-specific functional genomics androteomics. Examples are the development of reporter genemaging techniques (28) and the implementation of cellabeling for imaging of engraftment after transplantation28,124).
And fourth, the need to visualize small amounts ofolecular-targeted compounds in small target areas drives
dvances in the imaging sciences such as instrumentation,econstruction algorithms, and probe design to improve theetection sensitivity, molecular specificity, and translationalotential of molecular imaging.The vision is that novel molecular-targeted approaches
ill guide early disease detection and therapeutic/preventiveecision making based on an individual’s biology. PET as aey modality may thereby contribute to further personaliza-ion of cardiovascular medicine.ynergies between oncologic and cardiovascular PET.lthough PET is on the move in cardiovascular medicine
nd new developments are likely to increase its applicationnd impact in clinical practice, some similarities and inter-elationships between its cardiac applications and applica-ions for tumor imaging should be noted. First, the successf PET as a key modality in tumor staging and evaluation ofnti-tumor therapy has resulted in dissemination of theechnique and in improved availability for cardiac imaging.econd, expensive equipment, such as scanners, radiochem-
stry laboratories, and cyclotrons, is most effectively usedhen it serves multiple areas of PET imaging applications.nd finally, many existing and novel biologic targets forET imaging are important not only in heart and vessels,ut also in tumors (Table 5). This is highly relevant not onlyecause advances in tumor biology may help advance car-iovascular biology via improved understanding of relatediomechanisms, but also because multiple applications ineart, vessels, and tumors will be helpful to stimulate
nterest in commercialization of compounds with a broaderpectrum of target groups.
ummary and Conclusions
ardiac PET is a powerful, quantitative, noninvasive imag-ng technique that is increasingly penetrating the clinicalrena. For clinical assessment of myocardial perfusion andiability, evidence for diagnostic and prognostic usefulness isncreasing and cost-effectiveness due to high accuracy de-pite high single-test costs is suggested. The advent ofybrid imaging enables routine combination of PET with
Examples of Common Imaging Targets in Myoca
Table 5 Examples of Common Imaging Targ
Biologic target Myocardium
Glucose use 1 (when dama
Apoptosis 1 (when dama
Integrin expression/angiogenesis 1 (when dama
Matrix metalloproteinase expression 1 (when dama
T-derived morphologic parameters. New molecular imag-
ng compounds will be key elements in the emergingaradigm of personalized medicine.
cknowledgmenthe authors would like to thank Mrs. Judy Buchanan,ivision of Nuclear Medicine, Johns Hopkins University,
or her valuable editorial support.
eprint requests and correspondence: Dr. Frank M. Bengel,irector of Cardiovascular Nuclear Medicine, Russell H. Morganepartment of Radiology and Radiological Science, Johns Hop-
ins University, 601 North Caroline Street/JHOC 3225, Balti-ore, Maryland 21287. E-mail: [email protected].
EFERENCES
1. World of Quotes. George Herbert quotes. Available at: http://www.worldofquotes.com/author/George-Herbert/1/index.html. Ac-cessed May 5, 2009.
2. Ter-Pogossian MM, Phelps ME, Hoffman EJ, Mullani NA. Apositron-emission transaxial tomograph for nuclear imaging (PETT).Radiology 1975;114:89–98.
3. Schelbert HR, Phelps ME, Hoffman E, Huang SC, Kuhl DE.Regional myocardial blood flow, metabolism and function assessednoninvasively with positron emission tomography. Am J Cardiol1980;46:1269–77.
4. Weiss ES, Siegel BA, Sobel BE, Welch MJ, Ter-Pogossian MM.Evaluation of myocardial metabolism and perfusion with positron-emitting radionuclides. Prog Cardiovasc Dis 1977;20:191–206.
5. Schelbert HR, Phelps ME, Huang SC, et al. N-13 ammonia as anindicator of myocardial blood flow. Circulation 1981;63:1259–72.
6. Bergmann SR, Fox KA, Rand AL, et al. Quantification of regionalmyocardial blood flow in vivo with H215O. Circulation 1984;70:724–33.
7. Uren NG, Melin JA, de Bruyne B, Wijns W, Baudhuin T, CamiciPG. Relation between myocardial blood flow and the severity ofcoronary-artery stenosis. N Engl J Med 1994;330:1782–8.
8. Gould KL, Ornish D, Scherwitz L, et al. Changes in myocardialperfusion abnormalities by positron emission tomography after long-term, intense risk factor modification. JAMA 1995;274:894–901.
9. Tamaki N, Yonekura Y, Senda M, et al. Myocardial positroncomputed tomography with 13N-ammonia at rest and during exer-cise. Eur J Nucl Med 1985;11:246–51.
10. Schelbert HR, Henze E, Sochor H, et al. Effects of substrateavailability on myocardial C-11 palmitate kinetics by positron emis-sion tomography in normal subjects and patients with ventriculardysfunction. Am Heart J 1986;111:1055–64.
11. Tillisch J, Brunken R, Marshall R, et al. Reversibility of cardiacwall-motion abnormalities predicted by positron tomography.N Engl J Med 1986;314:884–8.
12. Buxton DB, Schwaiger M, Nguyen A, Phelps ME, Schelbert HR.Radiolabeled acetate as a tracer of myocardial tricarboxylic acid cycleflux. Circ Res 1988;63:628–34.
13. Schwaiger M, Fishbein MC, Block M, et al. Metabolic and ultra-structural abnormalities during ischemia in canine myocardium:
, Vessel Wall, and Tumors
Myocardium, Vessel Wall, and Tumors
Vessel Wall Tumor
1 (when inflamed) 1
1 (when inflamed) 1 (in therapy response)
1 (when damaged) 1 (some tumors)
1 (when vulnerable) 1 (some tumors)
rdium
ets in
ged)
ged)
ged)
ged)
noninvasive assessment by positron emission tomography. J Mol CellCardiol 1987;19:259–69.

13JACC Vol. 54, No. 1, 2009 Bengel et al.June 30, 2009:1–15 Cardiac PET
14. Nuutila P, Koivisto VA, Knuuti J, et al. Glucose-free fatty acid cycleoperates in human heart and skeletal muscle in vivo. J Clin Invest1992;89:1767–74.
15. Schwaiger M, Kalff V, Rosenspire K, et al. Noninvasive evaluation ofsympathetic nervous system in human heart by positron emissiontomography. Circulation 1990;82:457–64.
16. Goldstein DS, Chang PC, Eisenhofer G, et al. Positron emissiontomographic imaging of cardiac sympathetic innervation and func-tion. Circulation 1990;81:1606–21.
17. Merlet P, Delforge J, Syrota A, et al. Positron emission tomographywith 11C CGP-12177 to assess beta-adrenergic receptor concentra-tion in idiopathic dilated cardiomyopathy. Circulation 1993;87:1169–78.
18. Syrota A, Comar D, Paillotin G, et al. Muscarinic cholinergicreceptor in the human heart evidenced under physiological conditionsby positron emission tomography. Proc Natl Acad Sci U S A1985;82:584–8.
19. Klein C, Nekolla SG, Bengel FM, et al. Assessment of myocardialviability with contrast-enhanced magnetic resonance imaging: com-parison with positron emission tomography. Circulation 2002;105:162–7.
20. Knuesel PR, Nanz D, Wyss C, et al. Characterization of dysfunc-tional myocardium by positron emission tomography and magneticresonance: relation to functional outcome after revascularization.Circulation 2003;108:1095–100.
21. Schwitter J, DeMarco T, Kneifel S, et al. Magnetic resonance-basedassessment of global coronary flow and flow reserve and its relation toleft ventricular functional parameters: a comparison with positronemission tomography. Circulation 2000;101:2696–702.
22. Vogel R, Indermuhle A, Reinhardt J, et al. The quantification ofabsolute myocardial perfusion in humans by contrast echocardiogra-phy: algorithm and validation. J Am Coll Cardiol 2005;45:754–62.
23. Baer FM, Voth E, Deutsch HJ, Schneider CA, Schicha H, Sechtem U.Assessment of viable myocardium by dobutamine transesophageal echo-cardiography and comparison with fluorine-18 fluorodeoxyglucosepositron emission tomography. J Am Coll Cardiol 1994;24:343–53.
24. Baer FM, Voth E, Schneider CA, Theissen P, Schicha H, Sechtem U.Comparison of low-dose dobutamine-gradient-echo magnetic resonanceimaging and positron emission tomography with [18F]fluorodeoxyglu-cose in patients with chronic coronary artery disease. A functional andmorphological approach to the detection of residual myocardial viability.Circulation 1995;91:1006–15.
25. Bonow RO, Dilsizian V, Cuocolo A, Bacharach SL. Identification ofviable myocardium in patients with chronic coronary artery diseaseand left ventricular dysfunction. Comparison of thallium scintigraphywith reinjection and PET imaging with 18F-fluorodeoxyglucose.Circulation 1991;83:26–37.
26. Dilsizian V, Arrighi JA, Diodati JG, et al. Myocardial viability inpatients with chronic coronary artery disease. Comparison of 99mTc-sestamibi with thallium reinjection and [18F]fluorodeoxyglucose.Circulation 1994;89:578–87.
27. Higuchi T, Bengel FM. Cardiovascular nuclear imaging: fromperfusion to molecular function: non-invasive imaging. Heart 2008;94:809–16.
28. Wu JC, Bengel FM, Gambhir SS. Cardiovascular molecular imaging.Radiology 2007;244:337–55.
29. Machac J. Cardiac positron emission tomography imaging. SeminNucl Med 2005;35:17–36.
30. Bateman TM, Heller GV, McGhie AI, et al. Diagnostic accuracy ofrest/stress ECG-gated Rb-82 myocardial perfusion PET: comparisonwith ECG-gated Tc-99m sestamibi SPECT. J Nucl Cardiol 2006;13:24–33.
31. Schenker MP, Dorbala S, Hong EC, et al. Interrelation of coronarycalcification, myocardial ischemia, and outcomes in patients withintermediate likelihood of coronary artery disease: a combinedpositron emission tomography/computed tomography study. Circu-lation 2008;117:1693–700.
32. Yoshinaga K, Chow BJ, Williams K, et al. What is the prognosticvalue of myocardial perfusion imaging using rubidium-82 positronemission tomography? J Am Coll Cardiol 2006;48:1029–39.
33. Tarakji KG, Brunken R, McCarthy PM, et al. Myocardial viabilitytesting and the effect of early intervention in patients with advanced
left ventricular systolic dysfunction. Circulation 2006;113:230–7.34. Beanlands RS, Nichol G, Huszti E, et al. F-18-fluorodeoxyglucosepositron emission tomography imaging-assisted management of pa-tients with severe left ventricular dysfunction and suspected coronarydisease: a randomized, controlled trial (PARR-2). J Am Coll Cardiol2007;50:2002–12.
35. Yu M, Guaraldi MT, Mistry M, et al. BMS-747158-02: a novelPET myocardial perfusion imaging agent. J Nucl Cardiol 2007;14:789–98.
36. Di Carli MF, Hachamovitch R. New technology for noninvasiveevaluation of coronary artery disease. Circulation 2007;115:1464–80.
37. Pichler BJ, Wehrl HF, Judenhofer MS. Latest advances in molecularimaging instrumentation. J Nucl Med 2008;49 Suppl 2:5S–23S.
38. Schepis T, Gaemperli O, Treyer V, et al. Absolute quantification ofmyocardial blood flow with 13N-ammonia and 3-dimensional PET.J Nucl Med 2007;48:1783–9.
39. Knesaurek K, Machac J, Krynyckyi BR, Almeida OD. Comparison of2-dimensional and 3-dimensional 82Rb myocardial perfusion PETimaging. J Nucl Med 2003;44:1350–6.
40. Rahmim A, Tang J, Lodge MA, et al. Analytic system matrixresolution modeling in PET: an application to Rb-82 cardiac imag-ing. Phys Med Biol 2008;53:5947–65.
41. Chander A, Brenner M, Lautamaki R, Voicu C, Merrill J, BengelFM. Comparison of measures of left ventricular function fromelectrocardiographically gated 82Rb PET with contrast-enhancedCT ventriculography: A hybrid PET/CT analysis. J Nucl Med2008;49:1643–50.
42. Schafers KP, Stegger L. Combined imaging of molecular functionand morphology with PET/CT and SPECT/CT: image fusion andmotion correction. Basic Res Cardiol 2008;103:191–9.
43. Lautamaki R, George RT, Kitagawa K, et al. Rubidium-82 PET-CTfor quantitative assessment of myocardial blood flow: validation in acanine model of coronary artery stenosis. Eur J Nucl Med MolImaging 2008;36:576–86.
44. Machac J, Bacharach SL, Bateman TM, et al. Positron emissiontomography myocardial perfusion and glucose metabolism imaging.J Nucl Cardiol 2006;13:e121–51.
45. Nienaber CA, Ratib O, Gambhir SS, et al. A quantitative index ofregional blood flow in canine myocardium derived noninvasively withN-13 ammonia and dynamic positron emission tomography. J AmColl Cardiol 1991;17:260–9.
46. Goldstein RA, Mullani NA, Marani SK, Fisher DJ, Gould KL,O’Brien HA Jr. Myocardial perfusion with rubidium-82. II. Effectsof metabolic and pharmacologic interventions. J Nucl Med 1983;24:907–15.
47. Lortie M, Beanlands RS, Yoshinaga K, Klein R, Dasilva JN, deKempRA. Quantification of myocardial blood flow with 82Rb dynamicPET imaging. Eur J Nucl Med Mol Imaging 2007;34:1765–74.
48. Egert S, Nguyen N, Brosius FC III, Schwaiger M. Effects ofwortmannin on insulin- and ischemia-induced stimulation ofGLUT4 translocation and FDG uptake in perfused rat hearts.Cardiovasc Res 1997;35:283–93.
49. Knuuti J, Schelbert HR, Bax JJ. The need for standardisation ofcardiac FDG PET imaging in the evaluation of myocardial viabilityin patients with chronic ischaemic left ventricular dysfunction. EurJ Nucl Med Mol Imaging 2002;29:1257–66.
50. Hesse B, Tagil K, Cuocolo A, et al. EANM/ESC proceduralguidelines for myocardial perfusion imaging in nuclear cardiology.Eur J Nucl Med Mol Imaging 2005;32:855–97.
51. Einstein AJ, Moser KW, Thompson RC, Cerqueira MD, HenzlovaMJ. Radiation dose to patients from cardiac diagnostic imaging.Circulation 2007;116:1290–1305.
52. Schleipman AR, Castronovo FP Jr., Di Carli MF, Dorbala S.Occupational radiation dose associated with Rb-82 myocardial per-fusion positron emission tomography imaging. J Nucl Cardiol 2006;13:378–84.
53. Shaw LJ, Iskandrian AE. Prognostic value of gated myocardialperfusion SPECT. J Nucl Cardiol 2004;11:171–85.
54. Marwick TH, Shan K, Patel S, Go RT, Lauer MS. Incremental valueof rubidium-82 positron emission tomography for prognostic assess-ment of known or suspected coronary artery disease. Am J Cardiol1997;80:865–70.
55. Lertsburapa K, Ahlberg AW, Bateman TM, et al. Independent andincremental prognostic value of left ventricular ejection fraction
determined by stress gated rubidium 82 PET imaging in patients
14 Bengel et al. JACC Vol. 54, No. 1, 2009Cardiac PET June 30, 2009:1–15
with known or suspected coronary artery disease. J Nucl Cardiol2008;15:745–53.
56. Muzik O, Beanlands RS, Hutchins GD, Mangner TJ, Nguyen N,Schwaiger M. Validation of nitrogen-13-ammonia tracer kineticmodel for quantification of myocardial blood flow using PET. J NuclMed 1993;34:83–91.
57. Iida H, Takahashi A, Tamura Y, Ono Y, Lammertsma AA.Myocardial blood flow: comparison of oxygen-15-water bolus injec-tion, slow infusion and oxygen-15-carbon dioxide slow inhalation.J Nucl Med 1995;36:78–85.
58. Yoshida K, Mullani N, Gould KL. Coronary flow and flow reserve byPET simplified for clinical applications using rubidium-82 ornitrogen-13-ammonia. J Nucl Med 1996;37:1701–12.
59. Herrero P, Markham J, Shelton ME, Bergmann SR. Implementationand evaluation of a two-compartment model for quantification ofmyocardial perfusion with rubidium-82 and positron emission to-mography. Circ Res 1992;70:496–507.
60. El Fakhri G, Sitek A, Guerin B, Kijewski MF, Di Carli MF, MooreSC. Quantitative dynamic cardiac 82Rb PET using generalizedfactor and compartment analyses. J Nucl Med 2005;46:1264–71.
61. Pitkanen OP, Raitakari OT, Niinikoski H, et al. Coronary flowreserve is impaired in young men with familial hypercholesterolemia.J Am Coll Cardiol 1996;28:1705–11.
62. Campisi R, Czernin J, Schoder H, et al. Effects of long-term smokingon myocardial blood flow, coronary vasomotion, and vasodilatorcapacity. Circulation 1998;98:119–25.
63. Kaufmann PA, Gnecchi-Ruscone T, di Terlizzi M, Schafers KP,Luscher TF, Camici PG. Coronary heart disease in smokers: vitaminC restores coronary microcirculatory function. Circulation 2000;102:1233–8.
64. Tsukamoto T, Morita K, Naya M, et al. Myocardial flow reserve isinfluenced by both coronary artery stenosis severity and coronary riskfactors in patients with suspected coronary artery disease. Eur J NuclMed Mol Imaging 2006;33:1150–6.
65. Kjaer A, Meyer C, Nielsen FS, Parving HH, Hesse B. Dipyridamole,cold pressor test, and demonstration of endothelial dysfunction: aPET study of myocardial perfusion in diabetes. J Nucl Med 2003;44:19–23.
66. Schindler TH, Nitzsche EU, Olschewski M, et al. Chronic inflam-mation and impaired coronary vasoreactivity in patients with coronaryrisk factors. Circulation 2004;110:1069–75.
67. Di Carli MF, Afonso L, Campisi R, et al. Coronary vasculardysfunction in premenopausal women with diabetes mellitus. AmHeart J 2002;144:711–8.
68. Di Carli MF, Bianco-Batlles D, Landa ME, et al. Effects ofautonomic neuropathy on coronary blood flow in patients withdiabetes mellitus. Circulation 1999;100:813–9.
69. Momose M, Abletshauser C, Neverve J, et al. Dysregulation ofcoronary microvascular reactivity in asymptomatic patients with type2 diabetes mellitus. Eur J Nucl Med Mol Imaging 2002;29:1675–9.
70. Bengel FM, Abletshauser C, Neverve J, et al. Effects of nateglinideon myocardial microvascular reactivity in type 2 diabetes mellitus—arandomized study using positron emission tomography. Diabet Med2005;22:158–63.
71. Lautamaki R, Airaksinen KE, Seppanen M, et al. Insulin improvesmyocardial blood flow in patients with type 2 diabetes and coronaryartery disease. Diabetes 2006;55:511–6.
72. Higuchi T, Abletshauser C, Nekolla SG, Schwaiger M, Bengel FM.Effect of the angiotensin receptor blocker valsartan on coronarymicrovascular flow reserve in moderately hypertensive patients withstable coronary artery disease. Microcirculation 2007;14:805–12.
73. Yoshinaga K, Beanlands RS, deKemp RA, et al. Effect of exercisetraining on myocardial blood flow in patients with stable coronaryartery disease. Am Heart J 2006;151:1324–8.
74. Schindler TH, Nitzsche EU, Schelbert HR, et al. Positron emissiontomography-measured abnormal responses of myocardial blood flowto sympathetic stimulation are associated with the risk of developingcardiovascular events. J Am Coll Cardiol 2005;45:1505–12.
75. Neglia D, Michelassi C, Trivieri MG, et al. Prognostic role ofmyocardial blood flow impairment in idiopathic left ventriculardysfunction. Circulation 2002;105:186–93.
76. Cecchi F, Olivotto I, Gistri R, Lorenzoni R, Chiriatti G, Camici PG.Coronary microvascular dysfunction and prognosis in hypertrophic
cardiomyopathy. N Engl J Med 2003;349:1027–35.77. Sawada S, Muzik O, Beanlands RS, Wolfe E, Hutchins GD,Schwaiger M. Interobserver and interstudy variability of myocardialblood flow and flow-reserve measurements with nitrogen 13ammonia-labeled positron emission tomography. J Nucl Cardiol1995;2:413–22.
78. Kaufmann PA, Gnecchi-Ruscone T, Yap JT, Rimoldi O, CamiciPG. Assessment of the reproducibility of baseline and hyperemicmyocardial blood flow measurements with 15O-labeled water andPET. J Nucl Med 1999;40:1848–56.
79. Manabe O, Yoshinaga K, Katoh C, Naya M, deKemp RA, Tamaki N.Repeatability of rest and hyperemic myocardial blood flow measure-ments with 82Rb dynamic PET. J Nucl Med 2009;50:68–71.
80. Parkash R, deKemp RA, Ruddy TD, et al. Potential utility ofrubidium 82 PET quantification in patients with 3-vessel coronaryartery disease. J Nucl Cardiol 2004;11:440–9.
81. Muzik O, Duvernoy C, Beanlands RS, et al. Assessment of diagnos-tic performance of quantitative flow measurements in normal subjectsand patients with angiographically documented coronary artery dis-ease by means of nitrogen-13 ammonia and positron emissiontomography. J Am Coll Cardiol 1998;31:534–40.
82. Demer LL, Gould KL, Goldstein RA, Kirkeeide RL. Noninvasiveassessment of coronary collaterals in man by PET perfusion imaging.J Nucl Med 1990;31:259–70.
83. Bax JJ, Wijns W, Cornel JH, Visser FC, Boersma E, Fioretti PM.Accuracy of currently available techniques for prediction of functionalrecovery after revascularization in patients with left ventriculardysfunction due to chronic coronary artery disease: comparison ofpooled data. J Am Coll Cardiol 1997;30:1451–60.
84. Kaandorp TA, Lamb HJ, van der Wall EE, de RA, Bax JJ.Cardiovascular MR to access myocardial viability in chronic isch-aemic LV dysfunction. Heart 2005;91:1359–65.
85. Schinkel AF, Bax JJ, Poldermans D, Elhendy A, Ferrari R, Rahim-toola SH. Hibernating myocardium: diagnosis and patient outcomes.Curr Probl Cardiol 2007;32:375–410.
86. Beanlands RS, Hendry PJ, Masters RG, deKemp RA, Woodend K,Ruddy TD. Delay in revascularization is associated with increasedmortality rate in patients with severe left ventricular dysfunction andviable myocardium on fluorine 18-fluorodeoxyglucose positron emis-sion tomography imaging. Circulation 1998;98:II51–6.
87. Di Carli MF, Asgarzadie F, Schelbert HR, et al. Quantitativerelation between myocardial viability and improvement in heartfailure symptoms after revascularization in patients with ischemiccardiomyopathy. Circulation 1995;92:3436–44.
88. Siebelink HM, Blanksma PK, Crijns HJ, et al. No difference incardiac event-free survival between positron emission tomography-guided and single-photon emission computed tomography-guidedpatient management: a prospective, randomized comparison of pa-tients with suspicion of jeopardized myocardium. J Am Coll Cardiol2001;37:81–8.
89. Hernandez-Pampaloni M, Allada V, Fishbein MC, Schelbert HR.Myocardial perfusion and viability by positron emission tomographyin infants and children with coronary abnormalities: correlation withechocardiography, coronary angiography, and histopathology. J AmColl Cardiol 2003;41:618–26.
90. Hauser M, Bengel FM, Kuhn A, et al. Myocardial blood flow andflow reserve after coronary reimplantation in patients after arterialswitch and ross operation. Circulation 2001;103:1875–80.
91. Ohira H, Tsujino I, Ishimaru S, et al. Myocardial imaging with18F-fluoro-2-deoxyglucose positron emission tomography and mag-netic resonance imaging in sarcoidosis. Eur J Nucl Med Mol Imaging2008;35:933–41.
92. Ishimaru S, Tsujino I, Takei T, et al. Focal uptake on 18F-fluoro-2-deoxyglucose positron emission tomography images indicates car-diac involvement of sarcoidosis. Eur Heart J 2005;26:1538–43.
93. Patterson RE, Eisner RL, Horowitz SF. Comparison of cost-effectiveness and utility of exercise ECG, single photon emissioncomputed tomography, positron emission tomography, and coronaryangiography for diagnosis of coronary artery disease. Circulation1995;91:54–65.
94. Gould KL, Goldstein RA, Mullani NA. Economic analysis of clinicalpositron emission tomography of the heart with rubidium-82. J NuclMed 1989;30:707–17.
95. Merhige ME, Breen WJ, Shelton V, Houston T, D’Arcy BJ, Perna
AF. Impact of myocardial perfusion imaging with PET and (82)Rb
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
K
15JACC Vol. 54, No. 1, 2009 Bengel et al.June 30, 2009:1–15 Cardiac PET
on downstream invasive procedure utilization, costs, and outcomes incoronary disease management. J Nucl Med 2007;48:1069–76.
96. Beanlands RS, deKemp RA, Smith S, Johansen H, Ruddy TD.F-18-fluorodeoxyglucose PET imaging alters clinical decision mak-ing in patients with impaired ventricular function. Am J Cardiol1997;79:1092–5.
97. Jacklin PB, Barrington SF, Roxburgh JC, et al. Cost-effectiveness ofpreoperative positron emission tomography in ischemic heart disease.Ann Thorac Surg 2002;73:1403–9.
98. Danciu SC, Herrera CJ, Stecy PJ, Carell E, Saltiel F, Hines JL.Usefulness of multislice computed tomographic coronary angiogra-phy to identify patients with abnormal myocardial perfusion stress inwhom diagnostic catheterization may be safely avoided. Am J Cardiol2007;100:1605–8.
99. Lautamaki R, Brown TL, Merrill J, Bengel FM. CT-based attenu-ation correction in (82)Rb-myocardial perfusion PET-CT: incidenceof misalignment and effect on regional tracer distribution. Eur J NuclMed Mol Imaging 2008;35:305–10.
00. Martinez-Moller A, Souvatzoglou M, Navab N, Schwaiger M,Nekolla SG. Artifacts from misaligned CT in cardiac perfusionPET/CT studies: frequency, effects, and potential solutions. J NuclMed 2007;48:188–93.
01. Gould KL, Pan T, Loghin C, Johnson NP, Guha A, Sdringola S.Frequent diagnostic errors in cardiac PET/CT due to misregistrationof CT attenuation and emission PET images: a definitive analysis ofcauses, consequences, and corrections. J Nucl Med 2007;48:1112–21.
02. Di Carli MF, Dorbala S, Curillova Z, et al. Relationship between CTcoronary angiography and stress perfusion imaging in patients withsuspected ischemic heart disease assessed by integrated PET-CTimaging. J Nucl Cardiol 2007;14:799–809.
03. Lardo AC, Cordeiro MA, Silva C, et al. Contrast-enhanced multi-detector computed tomography viability imaging after myocardialinfarction: characterization of myocyte death, microvascular obstruc-tion, and chronic scar. Circulation 2006;113:394–404.
04. Holz A, Lautamaki R, Sasano T, et al. Expanding the versatility ofcardiac PET/CT: feasibility of delayed contrast enhancement CT forinfarct detection in a porcine model. J Nucl Med 2009;50:259–65.
05. Javadi M, Mahesh M, McBride G, et al. Lowering radiation dose forintegrated assessment of coronary morphology and physiology: firstexperience with step-and-shoot CT angiography in a rubidium 82PET-CT protocol. J Nucl Cardiol 2008;15:783–90.
06. Yalamanchili P, Wexler E, Hayes M, et al. Mechanism of uptake andretention of F-18 BMS-747158-02 in cardiomyocytes: a novel PETmyocardial imaging agent. J Nucl Cardiol 2007;14:782–8.
07. Huisman MC, Higuchi T, Reder S, et al. Initial characterization ofan 18F-labeled myocardial perfusion tracer. J Nucl Med 2008;49:630–6.
08. Madar I, Ravert H, Dipaula A, Du Y, Dannals RF, Becker L.Assessment of severity of coronary artery stenosis in a canine modelusing the PET agent 18F-fluorobenzyl triphenyl phosphonium:
comparison with 99mTc-tetrofosmin. J Nucl Med 2007;48:1021–30. m09. Madar I, Ravert H, Nelkin B, et al. Characterization of membranepotential-dependent uptake of the novel PET tracer 18F-fluorobenzyl triphenylphosphonium cation. Eur J Nucl Med MolImaging 2007;34:2057–65.
10. Stickel JR, Qi J, Cherry SR. Fabrication and characterization of a0.5-mm lutetium oxyorthosilicate detector array for high-resolutionPET applications. J Nucl Med 2007;48:115–21.
11. Riemann B, Schafers KP, Schober O, Schafers M. Small animal PETin preclinical studies: opportunities and challenges. Q J Nucl MedMol Imaging 2008;52:215–21.
12. Tai YC, Laforest R. Instrumentation aspects of animal PET. AnnuRev Biomed Eng 2005;7:255–85.
13. Rowland DJ, Cherry SR. Small-animal preclinical nuclear medicineinstrumentation and methodology. Semin Nucl Med 2008;38:209–22.
14. Knuuti J, Bengel FM. Positron emission tomography and molecularimaging. Heart 2008;94:360–7.
15. Dobrucki LW, Sinusas AJ. Molecular cardiovascular imaging. CurrCardiol Rep 2005;7:130–5.
16. Sasano T, Abraham MR, Chang KC, et al. Abnormal sympatheticinnervation of viable myocardium and the substrate of ventriculartachycardia after myocardial infarction. J Am Coll Cardiol 2008;51:2266–75.
17. Nahrendorf M, Zhang H, Hembrador S, et al. NanoparticlePET-CT imaging of macrophages in inflammatory atherosclerosis.Circulation 2008;117:379–87.
18. Rudd JH, Warburton EA, Fryer TD, et al. Imaging atheroscleroticplaque inflammation with [18F]-fluorodeoxyglucose positron emis-sion tomography. Circulation 2002;105:2708–11.
19. Dilsizian V, Eckelman WC, Loredo ML, Jagoda EM, Shirani J.Evidence for tissue angiotensin-converting enzyme in explantedhearts of ischemic cardiomyopathy using targeted radiotracer tech-nique. J Nucl Med 2007;48:182–7.
20. Peterson LR, Herrero P, Schechtman KB, et al. Effect of obesity andinsulin resistance on myocardial substrate metabolism and efficiencyin young women. Circulation 2004;109:2191–6.
21. Sundell J, Engblom E, Koistinen J, et al. The effects of cardiacresynchronization therapy on left ventricular function, myocardialenergetics, and metabolic reserve in patients with dilated cardiomy-opathy and heart failure. J Am Coll Cardiol 2004;43:1027–33.
22. Beanlands RS, Nahmias C, Gordon E, et al. The effects of beta(1)-blockade on oxidative metabolism and the metabolic cost ofventricular work in patients with left ventricular dysfunction: adouble-blind, placebo-controlled, positron-emission tomographystudy. Circulation 2000;102:2070–5.
23. Tuunanen H, Engblom E, Naum A, et al. Trimetazidine, a metabolicmodulator, has cardiac and extracardiac benefits in idiopathic dilatedcardiomyopathy. Circulation 2008;118:1250–8.
24. Beeres SL, Bengel FM, Bartunek J, et al. Role of imaging in cardiacstem cell therapy. J Am Coll Cardiol 2007;49:1137–48.
ey Words: positron emission tomography y myocardial perfusion y
yocardial viability y hybrid imaging y molecular imaging.

















