Cardiac Inflammation Contributes to Changes in the Extracell
10
1941-3297 American Heart Association. All rights reserved. Print ISSN: 1941-3289. Online ISSN: 2011 Copyright © TX 72514 Circulation: Heart Failure is published by the American Heart Association. 7272 Greenville Avenue, Dallas, DOI: 10.1161/CIRCHEARTFAILURE.109.931451 2011;4;44-52; originally published online November 12, 2010; Circ Heart Fail Heinz-Peter Schultheiss and Carsten Tschöpe J. von Schlippenbach, C. Skurk, Paul Steendijk, Alexander Riad, Wolfgang Poller, Dirk Westermann, Diana Lindner, Mario Kasner, Christine Zietsch, K. Savvatis, F. Escher, With Heart Failure and Normal Ejection Fraction Cardiac Inflammation Contributes to Changes in the Extracellular Matrix in Patients http://circheartfailure.ahajournals.org/content/4/1/44.full on the World Wide Web at: The online version of this article, along with updated information and services, is located http://www.lww.com/reprints Reprints: Information about reprints can be found online at [email protected] 410-528-8550. E-mail: Health, 351 West Camden Street, Baltimore, MD 21201-2436. Phone: 410-528-4050. Fax: Permissions: Permissions & Rights Desk, Lippincott Williams & Wilkins, a division of Wolters Kluwer http://circheartfailure.ahajournals.org/site/subscriptions/ Subscriptions: Information about subscribing to Circulation: Heart Failure is online at by guest on January 20, 2011 circheartfailure.ahajournals.org Downloaded from
description
Cardiac Inflammation Contributes to Changes in the Extracell
Transcript of Cardiac Inflammation Contributes to Changes in the Extracell

1941-3297American Heart Association. All rights reserved. Print ISSN: 1941-3289. Online ISSN: 2011 Copyright ©
TX 72514Circulation: Heart Failure is published by the American Heart Association. 7272 Greenville Avenue, Dallas,
DOI: 10.1161/CIRCHEARTFAILURE.109.931451 2011;4;44-52; originally published online November 12, 2010;Circ Heart FailHeinz-Peter Schultheiss and Carsten Tschöpe
J. von Schlippenbach, C. Skurk, Paul Steendijk, Alexander Riad, Wolfgang Poller, Dirk Westermann, Diana Lindner, Mario Kasner, Christine Zietsch, K. Savvatis, F. Escher,
With Heart Failure and Normal Ejection FractionCardiac Inflammation Contributes to Changes in the Extracellular Matrix in Patients
http://circheartfailure.ahajournals.org/content/4/1/44.full
on the World Wide Web at: The online version of this article, along with updated information and services, is located
http://www.lww.com/reprintsReprints: Information about reprints can be found online at
[email protected]. E-mail:Health, 351 West Camden Street, Baltimore, MD 21201-2436. Phone: 410-528-4050. Fax: Permissions: Permissions & Rights Desk, Lippincott Williams & Wilkins, a division of Wolters Kluwer
http://circheartfailure.ahajournals.org/site/subscriptions/Subscriptions: Information about subscribing to Circulation: Heart Failure is online at
by guest on January 20, 2011circheartfailure.ahajournals.orgDownloaded from

Cardiac Inflammation Contributes to Changes in theExtracellular Matrix in Patients With Heart Failure and
Normal Ejection FractionDirk Westermann, MD*; Diana Lindner, PhD*; Mario Kasner, MD; Christine Zietsch, PhD;
K. Savvatis, MD; F. Escher, MD; J. von Schlippenbach, MD; C. Skurk, MD; Paul Steendijk, PhD;Alexander Riad, MD; Wolfgang Poller, MD; Heinz-Peter Schultheiss, MD; Carsten Tschope, MD
Background—The pathophysiology of heart failure with normal ejection fraction (HFNEF) is still under discussion. Herewe report the influence of cardiac inflammation on extracellular matrix (ECM) remodeling in patients with HFNEF.
Methods and Results—We investigated left ventricular systolic and diastolic function in 20 patients with HFNEF and 8control patients by conductance catheter methods and echocardiography. Endomyocardial biopsy samples were alsoobtained, and ECM proteins as well as cardiac inflammatory cells were investigated. Primary human cardiac fibroblastswere outgrown from the endomyocardial biopsy samples to investigate the gene expression of ECM proteins afterstimulation with transforming growth factor-�. Diastolic dysfunction was present in the HFNEF patients compared withthe control patients. In endomyocardial biopsy samples from HFNEF patients, we found an accumulation of cardiaccollagen, which was accompanied by a decrease in the major collagenase system (matrix metalloproteinase-1) in theheart. Moreover, a subset of inflammatory cells, which expressed the profibrotic growth factor transforming growthfactor-�, could be documented in the HFNEF patients. Stimulation of primary human cardiac fibroblasts from HFNEFpatients with transforming growth factor-� resulted in transdifferentiation of fibroblasts to myofibroblasts, whichproduced more collagen and decreased the amount of matrix metalloproteinase-1, the major collagenase in thehuman heart. A positive correlation between cardiac collagen, as well as the amount of inflammatory cells, anddiastolic dysfunction was evident and suggests a direct influence of inflammation on fibrosis triggering diastolicdysfunction.
Conclusions—Cardiac inflammation contributes to diastolic dysfunction in HFNEF by triggering the accumulation ofECM. (Circ Heart Fail. 2011;4:44-52.)
Key Words: collagen � inflammation � remodeling � diastolic dysfunction
Patients with heart failure with normal ejection fraction(HFNEF) have increased mortality,1–4 and morbidity has
also been found to be higher compared with patients with HFand reduced EF.5 One of the underlying mechanisms leadingto the clinical symptomatology in patients with HFNEF isdiastolic function abnormality with increased diastolic stiff-ness, but nondiastolic function abnormalities with exercise-induced changes in systolic velocity, chronotropic incompe-tence, and ventricular-vascular uncoupling have also beendemonstrated to contribute to this disease.6–17 Despite thegrowing prevalence of HFNEF in the past 15 years, a diseaseaffecting about half of the HF population, knowledge aboutits molecular mechanisms is still limited, especially becausethe pathways leading to HFNEF are not confined to 1pathology. Intracellular changes with elevated cardiomyocyte
resting tension, as well as a shift in titin isoforms, areimportant in patients with severe HFNEF.19,20 Furthermore,accumulation of cardiac collagen was shown to be present inthis disease and to contribute to the aggravation of diastolicfunction.21–23 Enhanced endothelial migration of inflamma-tory cells into the myocardium might influence the develop-ment of these changes, especially in regard to changes in theextracellular matrix (ECM).24,25
Editorial see p 5Clinical Perspective on p 52
We hypothesized that inflammation is 1 important triggerof cardiac fibrosis and therefore it plays an important role inHFNEF. We show herein that increased inflammation trig-gers collagen accumulation in HFNEF patients and that both
Received December 15, 2009; accepted September 29, 2010.From the Department of Cardiology and Pneumology (D.W., D.L., M.K., C.Z., K.S., F.E., J.v.S., C.S., A.R., W.P., H.-P.S., C.T.), Charite,
Universititats-Medizin Berlin, Campus Benjamin Franklin, Berlin, Germany, and Department of Cardiology (P.S.), Leiden University Medical Center,Leiden, The Netherlands.
*Drs Westermann and Lindner contributed equally to this work.Correspondence to Dirk Westermann, MD, Department of Cardiology, Campus Benjamin Franklin, Hindenburgdamm 30, 12200 Berlin, Germany.
E-mail [email protected]© 2011 American Heart Association, Inc.
Circ Heart Fail is available at http://circheartfailure.ahajournals.org DOI: 10.1161/CIRCHEARTFAILURE.109.931451
44 by guest on January 20, 2011circheartfailure.ahajournals.orgDownloaded from

inflammation and fibrosis are correlated to diastolic dysfunc-tion. We show that inflammatory cells express transforminggrowth factor (TGF)-�, which directly induces changes incardiac fibroblasts as increasing collagen accumulation anddecreasing the degradation system (matrix metalloproteinase[MMP]-1 and their tissue inhibitor [TIMP]). This was asso-ciated with a transdifferentiation of cardiac fibroblasts tomyofibroblasts, known to be a potent contributor of patho-logical remodelling in diseased tissues. These findings sug-gest that cardiac inflammation by increased transendothelialmigration is 1 potent trigger of diastolic dysfunction in theHFNEF population.
MethodsStudy PopulationPatients presenting with New York Heart Association class II and IIIHF, an EF �50%, and diastolic dysfunction on echocardiographywere evaluated for participation in this study. Persistent atrialfibrillation and pulmonary diseases were excluded. Significant cor-onary artery disease or heart valve diseases were ruled out byangiography. Clinically relevant parvovirus B19 infection with agenome equivalent �500 was ruled out in all patients included in thestudy.26 Twenty patients met the inclusion criteria, were enrolled,and are referred to as the HFNEF group, with respect to recentguidelines.27 In addition, 8 patients without signs of congestive HFwho underwent coronary angiography for evaluation of chest painwere also enrolled in this study and served as controls. In all patients,endomyocardial biopsy samples were obtained the day after hemo-dynamic function was analyzed. Cardiac conditions were stablebefore catheterization in all patients. All patients gave informed,written consent. The research protocol was approved by the localinstitutional review board.
Pressure-Volume Measurementsand EchocardiographyThe conductance catheter was used to assess pressure-volumemeasurements in all patients, as recently described in more detail.6 Inbrief, left ventricular (LV) diastolic function was characterized byLV end-diastolic pressure and isovolumetric relaxation (�). Further-more, we calculated the exponential curve fit to the diastolic LVpressure-volume points during a transient preload reduction todetermine the load-independent diastolic stiffness constant (LVstiffness constant �). We analyzed LV end-systolic pressure and EFas a parameter of systolic function. The slope of the end-systolicpressure-volume relation was calculated as a load-independent pa-rameter for cardiac contractility. Mitral and pulmonary venousDoppler flow velocities were recorded in the apical 4-chamber viewwith a VingMed System FiVe (GE Healthcare, Chalfont St. Giles,UK) as well as the LV filling index by the ratio of transmitral flowvelocity to annular velocity (E/E� lateral), as previously described.7
Right ventricular systolic pressure (in mm Hg) was measured beforethe endomyocardial biopsy samples were taken.
Endomyocardial BiopsyEndomyocardial biopsy samples were obtained from the right side ofthe ventricular septum of each patient with use of a flexible bioptome(Westmed) via the femoral vein approach. Right ventricular systolicpressure was measured. The tissue pieces were frozen in LN2 andstored at �70°C for subsequent analysis.28 From all patients, 1endomyocardial biopsy sample was used for immunohistologicalstaining, and 1 was used for measuring gene expression. (Allmeasurements were performed once, n�20 in HFNEF and n�8 incontrols.)
Cell CulturePrimary cardiac fibroblasts were obtained by outgrowth from biopsyspecimens from 5 HFNEF patients and were incubated in Iscove’sbasal medium (Biochrom AG, Berlin, Germany) containing 10%human serum, 10% fetal calf serum (FCS), 100 U/mL penicillin(Biochrom AG), and 100 �g/mL streptomycin (Biochrom). Thecardiac fibroblasts were seeded in 24-well plates, and when theculture was �80% confluent, they were serum-starved in Iscove’sbasal medium containing 0.5% FCS (PAA, Colbe, Germany) for 16hours. They were then stimulated with 5 ng/mL TGF-�1 (PeproTech,Hamburg, Germany) for 6 or 24 hours compared with no stimulationfor 6 or 24 hours. All experiments were done with cells between thesecond and fourth passage with n�6 wells per experiment for alltime points and all patients. For each patient, a mean was calculatedfrom the 6 cell culture wells for each experiment (basal conditionsand stimulated for all time points), and the means of all patients arepresented in the figures.
Native fibroblasts were stained with antibodies against CD31,desmin, vimentin, P4HB, and �-smooth muscle actin and comparedwith HL1 (experimental atrial cardiomyocytes) as well as withendothelial cells. The monocyte cell line THP-1 was cultured inRPMI 1640 medium (PAA) containing 10% FCS (PAA), 100 U/mLpenicillin, and 100 �g/mL streptomycin (PAA).
Type I Carboxy-Terminal Telopeptide of Collagenand Propeptide of Procollagen Type I in SerumSerum was collected 1 hour before invasive measurements, and typeI carboxy-terminal telopeptide as a breakdown product of collagentype 1, as well as procollagen type I as a marker of type I collagensynthesis, was measured as described previously.29
RNA IsolationTotal RNA was extracted from the myocardial biopsy samples or cellculture wells by the Trizol method (GIBCO BRL, Carlsbad, Calif).
20
25
III
15
I
P=0.01 P=0.02
10
15
Col
lage
n ty
pe I
% A
F
5
10
Col
lage
n ty
pe
% A
F
2.03
control HFNEF0
5C
control HFNEF0
C
P=0.03P<0.001
1.0
1.5
gen
type
III
expr
essi
one
to c
ontr
ol
2
gen
type
Iex
pres
sion
e to
con
trol
control HFNEF0.0
0.5Col
lag
gene
ere
lativ
e
control HFNEF0
1
Col
lag
gene
ere
lativ
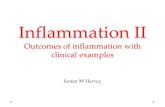
eFigure 1. Box-and-whisker plots showing increased levels of col-lagen types I and III proteins in endomyocardial biopsy samplesfrom patients with HFNEF compared with controls. Increases in thecollagen I to III ratio as well of collagen type I C-telopeptide weremeasured in serum. The mRNA abundance of collagen types I andtype III was increased in HFNEF compared with control subjects.AF indicates area fractions. *P�0.05 vs controls.
Westermann et al Inflammation and Fibrosis in HFNEF 45
by guest on January 20, 2011circheartfailure.ahajournals.orgDownloaded from

Additional purification was performed with the ChargeSwitch totalRNA cell kit (Invitrogen, Karlsruhe, Germany). The yield of purifiedtotal RNA was analyzed by checking the UV absorbance at 260 nmon a NanoDrop ND-1000 (Agilent Technologies, Boeblingen, Ger-many) spectrophotometer.
Real-Time Reverse Transcription–PolymeraseChain ReactionThe ABI-inventoried TaqMan gene expression assays (each includedforward and reverse primers as well as a fluorescently marked probe)used for preamplification (from the biopsy samples) and for thereal-time reverse transcription–polymerase chain reaction were ob-tained from Applied Biosystems. Prior real-time reverse transcrip-tion–polymerase chain reaction cDNA samples (1 to 250 ng) of thebiopsy samples were preamplified with pooled gene expressionassays with the TaqMan PreAmp Master Mix (early access) in a finalvolume of 25 �L. Quantification of housekeeping CDKN1B tran-scripts as an internal control for the amount and quality of cDNA wasperformed for all samples. Gene expression for collagen types I andIII was analyzed from cardiac biopsy samples (primers from AppliedBiosystems). Data for cell culture were also normalized to humanCDKN1B mRNA levels as an endogenous control (unaffected byTGF-� treatment) and are expressed relative to untreated controlsaccording to the formula 2���CT.
TGF-� ELISAThe THP-1 cells were starved in Iscove’s medium containing 0.5%FCS (PAA), 100 U/mL penicillin, and 100 �g/mL streptomycin(PAA) 16 hours before the experiment. THP-1 cells (3 millions [ml])were treated with 100 ng/mL phorbol 12-myristate 13-acetate
(Sigma-Aldrich) for 12, 24, or 48 hours. The cell culture supernatantwas then used for measuring the total TGF-�1 concentration with theTGF�1 Emax immunoassay system (Promega). The cell culturesupernatant was first diluted 1:5 in Dulbecco’s phosphate-bufferedsaline (PAA) and then acidified with HCl to pH 2.6 for 15 minutes,followed by neutralization with NaOH before using the sample forthe TGF�1 Emax immunoassay system.
HistologyImmunohistological staining was performed by standard techniques.The antibodies were purchased from Chemicon (anti-MMP1, CD3,CD11a, CD45, vascular cell adhesion molecule [VCAM]-1, andcollagen types I and III) and Calbiochem (anti-TIMP-1 and anti–MMP-2). Immunohistochemical staining images were quantified bydigital image analysis. For double immunofluorescence, we usedTissue Tec–embedded cryosections. The following primary antibod-ies were used: mouse anti–�-sarcomere actin (1:50, Santa Cruz) andmouse–anti–TGF-� (1:50, Serotec). The secondary antibodies werelabeled with fluorescein isothiocyanate and tetramethylrhodamineisothiocyanate (Sigma, St. Louis, Mo). Nuclei were visualized with4�,6-diamidino-2-phenylindole (Sigma). Slides were embedded influorescent mounting medium (DakoCytomation, Glostrup, Den-mark), coverslipped, and analyzed by fluorescence microscopy(Zeiss, Jena, Germany). Sections were incubated with 10 �mol/Ldihydroethidium to detect O2
� and visualized by fluorescencemicroscopy, whereby DHE-positive nuclei were counted with re-spect to the number of total nuclei.
Statistical AnalysisData are shown in box-and-whisker plots (Figures 1 through 3) andas mean�SEM (Figures 4 and 5). For comparison of the HFNEF
401520P=0.04 P=0.02 P=0.01
10
20
30
MM
P-2
% A
F
5
10
TIM
P-1
% A
F
5
10
15
MM
P-1
% A
F
control HFNEF0
10
control HFNEF0
control HFNEF0
5
15
20
25
ve n
ucle
i
0 15
0.20
0.25
1
P=0.04 P=0.01
5
10
15
% D
HE
posi
tv
0.05
0.10
0.15
VCAM
-%
AF
control HFNEF0
control HFNEF0.00
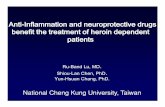
Figure 2. Decreases in protein levels of MMP-1and increases in levels of MMP-2 and TIMP-1were found in endomyocardial biopsy samplesfrom patients with HFNEF compared with con-trols. Increased oxidative stress by DHE stain-ing was documented in HFNEF compared withcontrol subjects. The adhesion moleculeVCAM-1 was also increased in HFNEF com-pared with control subjects. AF indicates areafractions. *P�0.05 vs controls.
40
50
m2
60
80
m2
30
2
P<0.001 P=0.002 P<0.001
20
30
D45
+ cells
/ m
m
20
40
60
D11
a+ cells
/ m
m
10
20
D3+ ce
lls /
mm
control HFNEF0
10CD
control HFNEF0
20
CD
control HFNEF0
C
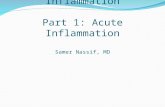
Figure 3. Increased numbers of CD3, CD11,and CD45 cells were found in endomyocardialbiopsy samples from patients with HFNEF com-pared with controls. *P�0.05 vs controls.
46 Circ Heart Fail January 2011
by guest on January 20, 2011circheartfailure.ahajournals.orgDownloaded from

group with the control group, the nonparametric Mann–Whitney Utest was used for data that were not normally distributed. Fisher’sexact test was used to analyze categorical variables. A probabilityvalue �0.05 was considered statistically significant. Data wereanalyzed with Graphpad 5.01 (PRISM, San Diego, Calif) and SPSS(version 15.0; SPSS Inc, Chicago, Ill).
ResultsPatient DemographicsPatient characteristics are summarized in Table 1. There wereno significant differences between HFNEF patients andcontrols with respect to age, sex, or body surface area. Theprevalence of hypertension and diabetes mellitus was notstatistically different between the groups (Table 1).
Hemodynamic DataSystolic function was not changed in HFNEF compared withcontrols. In contrast, diastolic dysfunction was evident in theHFNEF group, with an increased LV stiffness constant �,increased LV end-diastolic pressure, and prolonged isovolu-metric relaxation. Echocardiography revealed that the cardiacdimensions of both groups were not significantly different.Diastolic dysfunction with increased E/E� lateral was docu-mented in the HFNEF group. Moreover, significant cardiachypertrophy was documented in HFNEF compared withcontrol subjects (Table 2). Right ventricular systolic pressure,as 1 parameter of pulmonary hypertension, was not signifi-cantly different in HFNEF and controls (29.7; range, 24 to33 mm Hg, vs 25; range, 21 to 28.5 mm Hg; P�0.4).
Figure 5. In vitro cell culture experi-ments of primary cardiac fibroblastsstimulated with TGF-� for 6 or 24 hours.Increased gene expression of �-smoothmuscle actin (a-SMA), connective tissuegrowth factor (CTGF), and collagen typeI (Col I) were found in stimulated cellscompared with unstimulated cells.MMP-1 was decreased after stimulationwith TGF-�. MMP-2 was increased afterstimulation. *P�0.05 compared to therelative controls.
Figure 4. A, Representative histologic image with double staining of CD11 cells with the profibrotic growth factor TGF-�. B, In vitroexperiments with phorbol 12-myristate 13-acetate–activated monocytes (THP-1 cells) showed increased production of TGF-� mRNAand protein levels of TGF-� in a time-dependent manner. *P�0.05 vs individual controls.
Westermann et al Inflammation and Fibrosis in HFNEF 47
by guest on January 20, 2011circheartfailure.ahajournals.orgDownloaded from

Extracellular MatrixCollagen type I and III expression in the cardiac biopsysamples was significantly higher in patients with HFNEFthan in controls. Moreover, mRNA abundance of both colla-gen subtypes was increased in HFNEF patients (Figure 1).The ratio of collagen type I to type III was increased inHFNEF patients. TGF-� mRNA expression in the biopsysamples was increased in HFNEF patients compared withcontrols (59% compared with controls, P�0.004). Histologicexpression levels of cardiac MMP-1, the major humancollagenase, were decreased in HFNEF, whereas TIMP-1 wasincreased in HFNEF individuals compared with controls(Figure 2).
Type I carboxy-terminal telopeptide, as 1 serum marker forcollagen degradation, was increased in the sera of HFNEFpatients compared with controls (mean�SEM, 5.9�2.1 vs2.3�1.4 �g/L; P�0.025). Procollagen type I, a serum markerfor collagen production, was also increased in the HFNEFgroup compared with controls (mean�SEM, 128.9�26 vs65.1�21 �g/L; P�0.018).
InflammationThe inflammatory cells marked by CD3, CD11a, and CD45were all increased in the cardiac tissues of the HFNEFpatients compared with controls (Figure 3). Moreover, theadhesion molecule VCAM-1 was increased in HFNEF com-pared with control patients (Figure 2). In double staining,inflammatory cells revealed a secretion of the profibroticgrowth factor TGF-� (Figure 4). More cells (mostly cardio-myocytes and endothelial cells) in the HFNEF group werepositive after DHE staining as a marker of oxygen radicalproduction in comparison with controls (Figure 2). No changein systemic inflammation as measured by C-reactive proteinwas found between the groups (1.3�0.5 vs 1.1�0.3 mg/dL;P�NS).
Fibroblast Cell CultureAfter stimulation with TGF-� for 6 or 24 hours, connectivetissue growth factor and collagen type 1A1 mRNAs wereupregulated compared with controls. The transdifferentiationto myofibroblasts, as suggested by �-smooth muscle actinmRNA expression, was observed after 24 hours of stimula-tion with TGF-�. MMP-1 was not increased after 6 or 24hours, but MMP-2 was upregulated after 24 hours. With anincreased TIMP-1 expression, the MMP-1 to TIMP-1 ratio as1 indicator of MMP-1 activity was downregulated afterstimulation with TGF-� for 6 or 24 hours (Figure 5).
THP-1 Cell CultureActivated THP-1 cells produced TGF-� mRNA comparedwith their nonactivated controls. This was followed by atime-dependent production of TGF-� protein, which showedsignificantly increased protein levels 24 hours after stimula-tion of the THP-1 monocytes (Figure 4B).
DiscussionThe salient finding of the current study is that cardiacinflammatory cells documented in endomyocardial biopsysamples from patients with HFNEF induce extracellularremodelling with increased accumulation of collagen.TGF-�, excreted by inflammatory cells, is 1 potent stimulusfor the regulatory changes of the ECM, as shown in cellculture experiments with primary cardiac fibroblasts derivedfrom endomyocardial biopsy samples of patients with HFNEF.These changes contribute to diastolic dysfunction, which is 1of the underlying pathologies of HFNEF, which was docu-mented by a correlation between collagen (as well as inflam-matory cells) and diastolic dysfunction.
Table 1. Characteristics of the HFNEF and Control Groups
CharacteristicsControl(n�8)
HFNEF(n�20) P Value
Age, y 56 (50–69) 60 (43–68) 0.21*
NYHA class II 0 12
NYHA class III 0 8
NT-pro-BNP, pg/mL 51 (28–67) 573 (389–949) �0.001*
Medications
�-blockers 1 14 0.018†
ACE inhibitors/ARBs 2 17 0.0048†
Ca2 channel blockers 0 3 0.536
Diuretics 2 16 0.011†
Concomitant diseases
Hypertension 2 12 0.20†
Diabetes mellitus 0 6 0.14†
NYHA indicates New York Heart Association; NT-pro-BNP, NT-pro-brainnatriuretic peptide; ACE, angiotensin-converting enzyme; and ARB, angiotensinreceptor blocker. Patient characteristics and data are shown as median(25%–75% percentile).
*t test.†Fisher’s exact test.
Table 2. Echocardiographic and Hemodynamic Results
Control HFNEF P Values
Chamber dimensions,mm
LVEDD 47 (42–49) 46 (40–50) 0.573*
Septum 9.8 (8.3–10.2) 12.3 (10.5–13.6) �0.001*
Posterior wall 9.2 (8.6–9.5) 11.4 (10.2–12.2) �0.001*
Tissue Doppler E/E�(lateral)
6.1 (4.7–7.5) 13.9 (11.4–17.4) 0.011*
Pressure-volume loops
LVP, mm Hg 131 (117–145) 136 (124–159) 0.412
dP/dtmax, mm Hg/s 1783 (1509–2106) 1882 (1639–2117) 0.535
ESPVR, mm Hg/mL 1.1 (0.8–1.3) 1.2 (1–1.5) 0.386
LVEDP, mm Hg 6 (4–9) 16 (14–24) �0.001*
�, ms 48 (40–49) 64 (63–78) �0.001*
Diastolic stiffness 0.01 (0.006–0.04) 0.06 (0.03–0.12) �0.001*
LVEDD, LV end-diastolic diameter; LVP, LV pressure; ESPVR, end-systolicpressure volume relation; LVEDP, LV end-diastolic pressure; and �, isovolu-metric relaxation time. Data are shown as median (25%–75% percentile).
*t test.
48 Circ Heart Fail January 2011
by guest on January 20, 2011circheartfailure.ahajournals.orgDownloaded from

The molecular changes leading to diastolic dysfunction arestill debated, and different pathways can affect the pathologyof HFNEF. Altered isoform expression of the giant muscleprotein titin can determine the elastic properties of the heart.19
Moreover, increased myocyte tension, which can be pre-vented by experimental phosphorylation of titin, contributesto diastolic dysfunction in patients with severe HFNEF.20,30
Additional modulatory effects on titin stiffness may arisefrom disulfide bonding under oxidant stress also affectingLV compliance.31 Nevertheless, the steep part of thediastolic pressure-volume relation is mainly modified bythe ECM, as can be observed when comparing stretchlengths between whole-muscle stripes and single myo-cytes,32 suggesting that excess collagen might furtheraggravate diastolic dysfunction.
Cardiac collagen is a stable protein with a low turnover (80to 120 days),33 but its balance can be disrupted in pathologicalconditions. Next to ischemia, which may lead to replacingfibrosis, for example, increased wall stress, angiotensin II,and TGF-� may induce profibrotic processes leading topathological tissue fibrosis.34 The tensile strength of collagentype 1 approximates that of steel. Therefore, LV chamberstiffness in vivo will be affected by the amount of cardiacECM.35 In this study, we showed that total cardiac collagencontent was increased in patients with HFNEF, in agreementwith other work that showed increased fibrosis in thisdisease.19,21,36 Furthermore, not only was collagen type Ifound to be increased in this study population, but also therewas a change in the collagen type I to III ratio in favor ofthe stiffer collagen type I, similar to that in patients withsystolic HF.37 In addition to increased protein levels ofcollagen types I and III, their mRNA abundance was alsoincreased in endomyocardial biopsy samples from patientswith HFNEF compared with controls. Another marker ofexcessive collagen production is type I carboxy-terminaltelopeptide, a degradation product of collagen with in-creased collagen turnover together with propeptide ofprocollagen type I, a serum marker of collagen production,both of which were increased in the HFNEF group.Oxidative stress was increased in HFNEF patients, as DHEstaining revealed, which might be the result of increasedLV stiffness.
Multiple studies have shown that 1 of the best-knowninducers of collagen production is the profibrotic growthfactor TGF-�. It also has profound effects on ECMhomeostasis, in part through its ability to alter the balancebetween MMPs and their TIMP inhibitors. The endoge-nous collagen degradation system is regulated by increasedactivity of MMPs overcoming their tissue inhibitors.38
Nevertheless, there are different MMPs, and the substrateaffinity of those proteases is different.39 MMP-1 (intersti-tial collagenase) is known to degrade collagen fibers, andtherefore it likely favors collagen degradation. Throughthe activity of the activator protein-1 transcription factor,TGF-� can, on one hand, repress MMP-1 gene expres-sion40 and, on the other hand, increase TIMP-1 expression.Congruent with these ex vivo data, we have show anupregulation of TIMP-1 protein and a downregulation ofMMP-1 protein levels in the biopsy samples from HFNEF
patients, which leads to a significant decrease in theMMP-1–TIMP-1 ratio. This inhibition of the collagendegradation system could be 1 mechanism contributing tothe accumulation of ECM in HFNEF patients and theinitiation of diastolic dysfunction over a longer timeperiod.41 Interestingly, Lopez and colleagues22 showed thatthis ratio was increased in patients with systolic HF,whereas it was unchanged in their hypertensive HF group.Whether this process is dynamic or changes with time, orwhether this mechanism represents a distinct differencebetween both HF subtypes remains to be clarified.
Furthermore, and in contrast to the activator protein-1–mediated downregulation of MMP-1, we found increasedlevels of MMP-2 (controlled by activator protein-2), which isa known gelatinase and has substrate affinity for denaturedfibrillar collagen as well as for the basement membrane.42
Some studies have described MMP-2 serum levels in patientswith hypertensive and diastolic HF, but the results areinconsistent, with some studies showing an increase,43 andothers showing no difference or even a decrease in MMP-2.33
Recently, increased levels of MMP-2 were shown to predictHF in patients with diastolic dysfunction and hypertension.In that study, MMP-2 was a better prognostic marker thanthe well-known HF biomarker brain natriuretic peptide.29
Several experimental studies in MMP-2– knockout animalshave helped to advance understanding of the molecularfunction of MMP-2. Matsumura and colleagues44 showedin MMP-2– knockout mice a decrease in invading inflam-matory cells and a decrease in LV rupture after myocardialinfarction. Those authors demonstrated that destruction ofbasement membrane proteins facilitates the transendothe-lial migration of immunocompetent cells, thereby trigger-ing cardiac inflammation.
In light of such findings, we investigated the number ofinflammatory cells in our patients and showed that HFNEFis associated with increased cardiac inflammation, withhigh numbers of CD3, CD11a, and CD45 cells.Moreover, the adhesion molecule VCAM-1, which attractsimmunocompetent cells to the endothelium and initiatestransendothelial migration, was also increased in theHFNEF group. This result is especially interesting, be-cause VCAM-1 is upregulated by angiotensin II, whichmay be increased in regard to known risk factors likehypertension and diabetes mellitus in HFNEF. Recently, itwas shown that immunocompetent cells like T-cells(CD3) can indeed alter tissue remodelling in vitro,45 andwe have shown that cardiac inflammation is associatedwith excessive collagen accumulation in experimentaldiabetic cardiomyopathy in 1 animal model of HFNEF.25
There is experimental and clinical evidence that inflam-matory cells might modulate cardiac function in HF withreduced46,47 and normal48,49 EF. The direct effects of thesecells are still under debate, but it has been suggested thatincreased inflammation is associated with the developmentof systolic HF by distinct changes in the ratio of MMP toTIMP.50,51 In line with these data, we have demonstratedherein that these inflammatory cells express TGF-� incardiac tissue, as shown by immunohistochemical doublestaining. Moreover, THP-1 cells, when they become acti-
Westermann et al Inflammation and Fibrosis in HFNEF 49
by guest on January 20, 2011circheartfailure.ahajournals.orgDownloaded from

vated, which is 1 hallmark of transendothelial migration,produce TGF-� on the mRNA and protein level, asevidenced by in vitro studies of phorbol 12-myristate13-acetate–activated THP-1 cells. In addition, TGF-� geneexpression was increased in the HFNEF biopsy samples.
To test the direct effect of TGF-� expressed by inflam-matory cells in this study, we performed experiments in acell culture system with primary human cardiac fibroblastsderived from endomyocardial biopsy samples of HFNEFpatients. After stimulation with TGF-�, fibroblasts ex-pressed increased amounts of �-smooth muscle actin, 1marker for their transdifferentiation into pathologicallyactivated myofibroblasts. Connective tissue growth factorwas concomitantly increased, leading to higher collagengene expression after 6 and 24 hours, which explains thecollagen accumulation found in the endomyocardial biopsysamples. On the other hand, the degradation system ofcollagen, especially the MMP-1 to TIMP-1 ratio, wasdownregulated after stimulation with TGF-� in the cellculture system, which is another explanation for theextensive fibrosis seen in HFNEF hearts. MMP-2, in linewith its known function in degrading the basement mem-brane to allow for easier transendothelial migration ofinflammatory cells into cardiac tissue, was upregulatedafter TGF-� stimulation. Interestingly, TGF-� gene ex-pression was increased after stimulation, which suggeststhat the already transdifferentiated myofibroblasts mighthave induced further activation of fibroblasts and thereforeenhanced the profibrotic process in a paracrine fashion.
Viral agents are 1 possible inducer of cardiac inflam-mation. The parvovirus B19, which is associated withendothelial and diastolic dysfunction,28 is known to causemyocarditis. Nevertheless, it was recently shown that inpatients with dilated cardiomyopathy, a viral load of only�500 genome equivalents is a clinically relevant thresholdfor the maintenance of myocardial inflammation.26 Be-cause this extent of viral load was ruled out in all patients,the exact mechanism of cardiac inflammation has still to bedetermined, although animal models of HF are oftenassociated with cardiac inflammation.24 Recently, it wasshown52 that activated myofibroblasts also produce che-mokines to fuel the inflammatory process, which mightinduce a vicious circle of inflammation triggering fibrosisand diastolic dysfunction. If hemodynamic changes inHFNEF induce proinflammatory changes to start cardiacinflammation, these have to be determined in detail infurther studies.
We suggest that small numbers of invading inflammatorycells stimulate cardiac fibrosis by expressing TGF-� andinducing a pathological transdifferentiation from fibroblaststo myofibroblasts. This will not only stimulate gene expres-sion of collagen but also induce a decline in MMP-1 activityand an increase in MMP-2 mRNA abundance, as well asparacrine TGF-� production. Increased stiffness due to ECMaccumulation will increase oxidative stress, suggested to beassociated with increased endothelial activation. Togetherwith increased MMP-2, which has been suggested to disruptthe basal membrane, this might induce a vicious circle
fuelling inflammation leading to fibrosis and ultimately, toprogression of the disease.
ConclusionsIn this study, HFNEF was characterized by an increase incardiac inflammation. This inflammatory process triggerscardiac collagen accumulation by inducing collagen geneexpression and inhibiting the cardiac degradation system.Inhibiting the transendothelial migration of inflammatorycells into cardiac tissue might be a future therapeutic conceptin HFNEF.
Sources of FundingThis study was supported by the Deutsche Forschungsgemeinschaft(SFB-TR-19, A2, and B5) and by the European Commission,Research Directorate General, FP7-Health-2010, MEDIA (261409),Brussels, Belgium.
DisclosuresNone.
References1. Owan TE, Hodge DO, Herges RM, Jacobsen SJ, Roger VL, Redfield M.
Trends in prevalence and outcome of heart failure with preserved ejectionfraction. N Engl J Med. 2006;355:251–259.
2. Bhatia RS, Tu JV, Lee DS, Austin PC, Fang J, Haouzi A, Gong Y, LiuP. Outcome of heart failure with preserved ejection fraction in apopulation-based study. N Engl J Med. 2006;355:260–269.
3. Tribouilloy C, Rusinaru D, Mahjoub H, Souliere V, Levy F, Peltier M,Slama M, Massy Z. Prognosis of heart failure with preserved ejectionfraction: a 5 year prospective population-based study. Eur Heart J.2008;29:339–347.
4. Gaasch WH, Delorey DE, Kueffer FJ, Zile R. Distribution of leftventricular ejection fraction in patients with ischemic and hyper-tensive heart disease and chronic heart failure. Am J Cardiol. 2009;104:1413–1415.
5. Ahmed A, Zile MR, Rich MW, Fleg JL, Adams KF Jr, Love TE, YoungJB, Aronow WS, Kitzman DW, Gheorghiade M, Dell’Italia LJ. Hospi-talizations due to unstable angina pectoris in diastolic and systolic heartfailure. Am J Cardiol. 2007;99:460–464.
6. Westermann D, Kasner M, Steendijk P, Spillmann F, Riad A, WeitmannK, Hoffmann W, Poller W, Pauschinger M, Schultheiss HP, Tschope C.Role of left ventricular stiffness in heart failure with normal ejectionfraction. Circulation. 2008;117:2057–2060.
7. Kasner M, Westermann D, Steendijk P, Gaub R, Wilkenshoff U,Weitmann K, Hoffmann W, Poller W, Schultheiss HP, Pauschinger, M.Tschope C. Utility of Doppler echocardiography and tissue Dopplerimaging in the estimation of diastolic function in heart failure with normalejection fraction: a comparative Doppler-conductance catheterizationstudy. Circulation. 2007;116:637–647.
8. Zile MR, Baicu CF, Gaasch H. Diastolic heart failure–abnormalities inactive relaxation and passive stiffness of the left ventricle. N Engl J Med.2004;350:1953–1959.
9. Lam CS, Roger VL, Rodeheffer RJ, Bursi F, Borlaug BA, Ommen SR,Kass DA, Redfield M. Cardiac structure and ventricular-vascular functionin persons with heart failure and preserved ejection fraction from OlmstedCounty, Minnesota. Circulation. 2007;115:1982–1990.
10. Phan TT, Abozguia K, Nallur Shivu G, Mahadevan G, Ahmed I, WilliamsL, Dwivedi G, Patel K, Steendijk P, Ashrafian H, Henning A, FrenneauxM. Heart failure with preserved ejection fraction is characterized bydynamic impairment of active relaxation and contraction of the leftventricle on exercise and associated with myocardial energy deficiency.J Am Coll Cardiol. 2009;54:402–409.
11. Wachter R, Schmidt-Schweda S, Westermann D, Post H, Edelmann F,Kasner M, Luers C, Steendijk P, Hasenfuss G, Tschope C, Pieske B.Blunted frequency-dependent upregulation of cardiac output is related to
50 Circ Heart Fail January 2011
by guest on January 20, 2011circheartfailure.ahajournals.orgDownloaded from

impaired relaxation in diastolic heart failure. Eur Heart J. 2009;30:3027–3036.
12. Borlaug BA, Melenovsky V, Russell SD, Kessler K, Pacak K, Becker LC,Kass A. Impaired chronotropic and vasodilator reserves limit exercisecapacity in patients with heart failure and a preserved ejection fraction.Circulation. 2006;114:2138–2147.
13. Tschope C, Westermann D. Heart failure with normal ejection fraction:pathophysiology, diagnosis, and treatment. Herz. 2009;34:89–96.
14. Borlaug BA, Lam CS, Roger VL, Rodeheffer RJ, Redfield M. Contrac-tility and ventricular systolic stiffening in hypertensive heart disease:insights into the pathogenesis of heart failure with preserved ejectionfraction. J Am Coll Cardiol. 2009;54:410–418.
15. Tan YT, Wenzelburger F, Lee E, Heatlie G, Leyva F, Patel K, FrenneauxM, Sanderson E. The pathophysiology of heart failure with normalejection fraction: exercise echocardiography reveals complex abnor-malities of both systolic and diastolic ventricular function involvingtorsion, untwist, and longitudinal motion. J Am Coll Cardiol. 2009;54:36–46.
16. Tschope C, Paulus WJ. Is echocardiographic evaluation of diastolic functionuseful in determining clinical care? Doppler echocardiography yields dubiousestimates of left ventricular diastolic pressures. Circulation. 2009;120:810–820; discussion 820.
17. Penicka M, Bartunek J, Trakalova H, Hrabakova H, Maruskova M,Karasek J, Kocka V. Heart failure with preserved ejection fraction inoutpatients with unexplained dyspnea: a pressure-volume loop analysis.J Am Coll Cardiol. 2010;55:1701–1710.
18. Deleted in proof.19. van Heerebeek L, Borbely A, Niessen HW, Bronzwaer JG, van der
Velden J, Stienen GJ, Linke WA, Laarman GJ, Paulus J. Myocardialstructure and function differ in systolic and diastolic heart failure.Circulation. 2006;113:1966 –1973.
20. Borbely A, van der Velden J, Papp Z, Bronzwaer JG, Edes I, Stienen GJ,Paulus J. Cardiomyocyte stiffness in diastolic heart failure. Circulation.2005;111:774–781.
21. van Heerebeek L, Hamdani N, Handoko ML, Falcao-Pires I, Musters RJ,Kupreishvili K, Ijsselmuiden AJ, Schalkwijk CG, Bronzwaer JG,Diamant M, Borbely A, van der Velden J, Stienen GJ, Laarman GJ,Niessen HW, Paulus J. Diastolic stiffness of the failing diabetic heart:importance of fibrosis, advanced glycation end products, and myocyteresting tension. Circulation. 2008;117:43–51.
22. Lopez B, Gonzalez A, Querejeta R, Larman M, Diez J. Alterations in thepattern of collagen deposition may contribute to the deterioration ofsystolic function in hypertensive patients with heart failure. J Am CollCardiol. 2006;48:89–96.
23. Muller-Brunotte R, Kahan T, Lopez B, Edner M, Gonzalez A, Diez J,Malmqvist K. Myocardial fibrosis and diastolic dysfunction in patientswith hypertension: results from the Swedish Irbesartan Left VentricularHypertrophy Investigation versus Atenolol (SILVHIA). J Hypertens.2007;25:1958–1966.
24. Heymans S, Hirsch E, Anker SD, Aukrust P, Balligand JL, Cohen-Tervaert JW, Drexler H, Filippatos G, Felix SB, Gullestad L, Hilfiker-Kleiner D, Janssens S, Latini R, Neubauer G, Paulus WJ, Pieske B,Ponikowski P, Schroen B, Schultheiss HP, Tschope C, Van Bilsen M,Zannad F, McMurray J, Shah M. Inflammation as a therapeutic target inheart failure? a scientific statement from the Translational ResearchCommittee of the Heart Failure Association of the European Society ofCardiology. Eur J Heart Fail. 2009;11:119–129.
25. Westermann D, Rutschow S, Jager S, Linderer A, Anker S, Riad A,Unger T, Schultheiss HP, Pauschinger M, Tschope C. Contributions ofinflammation and cardiac matrix metalloproteinase activity to cardiacfailure in diabetic cardiomyopathy: the role of angiotensin type 1 receptorantagonism. Diabetes. 2007;56:641–646.
26. Bock CT, Klingel K, Kandolf R. Human parvovirus B19-associatedmyocarditis. N Engl J Med. 2010;362:1248–1249.
27. Paulus WJ, Tschope C, Sanderson JE, Rusconi C, Flachskampf FA,Rademakers FE, Marino P, Smiseth OA, De Keulenaer G, Leite-MoreiraAF, Borbely A, Edes I, Handoko ML, Heymans S, Pezzali N, Pieske B,Dickstein K, Fraser AG, Brutsaert L. How to diagnose diastolic heartfailure: a consensus statement on the diagnosis of heart failure withnormal left ventricular ejection fraction by the Heart Failure and Echo-cardiography Associations of the European Society of Cardiology. EurHeart J. 2007;28:2539–2550.
28. Tschope C, Bock CT, Kasner M, Noutsias M, Westermann D,Schwimmbeck PL, Pauschinger M, Poller WC, Kuhl U, Kandolf R,Schultheiss P. High prevalence of cardiac parvovirus B19 infection in
patients with isolated left ventricular diastolic dysfunction. Circulation.2005;111:879–886.
29. Martos R, Baugh J, Ledwidge M, O’Loughlin C, Murphy NF, Conlon C,Patle A, Donnelly SC, McDonald K. Diagnosis of heart failure withpreserved ejection fraction: improved accuracy with the use of markers ofcollagen turnover. Eur J Heart Fail. 2009;11:191–197.
30. Jaber WA, Maniu C, Krysiak J, Shapiro BP, Meyer DM, Linke WA,Redfield M. Titin isoforms, extracellular matrix, and global chamberremodeling in experimental dilated cardiomyopathy: functional impli-cations and mechanistic insight. Circ Heart Fail. 2008;1:192–199.
31. Grutzner A, Garcia-Manyes S, Kotter S, Badilla CL, Fernandez JM,Linke A. Modulation of titin-based stiffness by disulfide bondingin the cardiac titin N2-B unique sequence. Biophys J. 2009;97:825– 834.
32. Kruger M, Linke WA. Titin-based mechanical signalling in normal andfailing myocardium. J Mol Cell Cardiol. 2009;46:490–498.
33. Laurent GJ. Dynamic state of collagen: pathways of collagen degradationin vivo and their possible role in regulation of collagen mass. Am JPhysiol. 1987;252:C1–C9.
34. Weber KT. Extracellular matrix remodeling in heart failure: a role for denovo angiotensin II generation. Circulation. 1997;96:4065–4082.
35. Zile MR, Brutsaert DL. New concepts in diastolic dysfunction and dia-stolic heart failure, part I: diagnosis, prognosis, and measurements ofdiastolic function. Circulation. 2002;105:1387–1393.
36. Querejeta R, Lopez B, Gonzalez A, Sanchez E, Larman M, Martinez UbagoJL, Diez J. Increased collagen type I synthesis in patients with heart failureof hypertensive origin: relation to myocardial fibrosis. Circulation. 2004;110:1263–1268.
37. Pauschinger M, Knopf D, Petschauer S, Doerner A, Poller W, SchwimmbeckPL, Kuhl U, Schultheiss P. Dilated cardiomyopathy is associated withsignificant changes in collagen type I/III ratio. Circulation. 1999;99:2750 –2756.
38. Spinale FG. Matrix metalloproteinases: regulation and dysregulation inthe failing heart. Circ Res. 2002;90:520–530.
39. Westermann D, Savvatis K, Schultheiss HP, Tschope C. Immunomodu-lation and matrix metalloproteinases in viral myocarditis. J Mol CellCardiol. 2010;48:468–473.
40. Hall MC, Young DA, Waters JG, Rowan AD, Chantry A, Edwards DR,Clark M. The comparative role of activator protein 1 and Smad factors inthe regulation of TIMP-1 and MMP-1 gene expression by transforminggrowth factor-�1. J Biol Chem. 2003;278:10304–10313.
41. Heymans S, Schroen B, Vermeersch P, Milting H, Gao F, Kassner A,Gillijns H, Herijgers P, Flameng W, Carmeliet P, Van de Werf F, PintoYM, Janssens S. Increased cardiac expression of tissue inhibitor ofmetalloproteinase-1 and tissue inhibitor of metalloproteinase-2 is relatedto cardiac fibrosis and dysfunction in the chronic pressure-overloadedhuman heart. Circulation. 2005;112:1136–1144.
42. Spinale FG. Myocardial matrix remodeling and the matrix metallopro-teinases: influence on cardiac form and function. Physiol Rev. 2007;87:1285–1342.
43. Martos R, Baugh J, Ledwidge M, O’Loughlin C, Conlon C, Patle A,Donnelly SC, McDonald K. Diastolic heart failure: evidence of increasedmyocardial collagen turnover linked to diastolic dysfunction. Circulation.2007;115:888–895.
44. Matsumura S, Iwanaga S, Mochizuki S, Okamoto H, Ogawa S, Okada Y.Targeted deletion or pharmacological inhibition of MMP-2 preventscardiac rupture after myocardial infarction in mice. J Clin Invest. 2005;115:599–609.
45. Mikko M, Fredriksson K, Wahlstrom J, Eriksson P, Grunewald J, SkoldM. Human T cells stimulate fibroblast-mediated degradation of extra-cellular matrix in vitro. Clin Exp Immunol. 2008;151:317–325.
46. Abbate A, Bonanno E, Mauriello A, Bussani R, Biondi-Zoccai GG,Liuzzo G, Leone AM, Silvestri F, Dobrina A, Baldi F, Pandolfi F,Biasucci LM, Baldi A, Spagnoli LG, Crea F. Widespread myocardialinflammation and infarct-related artery patency. Circulation. 2004;110:46–50.
47. Lisman KA, Stetson SJ, Koerner MM, Farmer JA, Torre-Amione G. Therole of inflammation in the pathogenesis of heart failure. Curr CardiolRep. 2002;4:200–205.
48. Sciarretta S, Ferrucci A, Ciavarella GM, De Paolis P, Venturelli V, TocciG, De Biase L, Rubattu S, Volpe M. Markers of inflammation and fibrosisare related to cardiovascular damage in hypertensive patients with met-abolic syndrome. Am J Hypertens. 2007;20:784–791.
49. Westermann D, Van Linthout S, Dhayat S, Dhayat N, Schmidt A,Noutsias M, Song XY, Spillmann F, Riad A, Schultheiss HP, Tschope C.
Westermann et al Inflammation and Fibrosis in HFNEF 51
by guest on January 20, 2011circheartfailure.ahajournals.orgDownloaded from

Tumor necrosis factor-� antagonism protects from myocardial inflam-mation and fibrosis in experimental diabetic cardiomyopathy. Basic ResCardiol. 2007;102:500–507.
50. Heymans S, Pauschinger M, De Palma A, Kallwellis-Opara A, RutschowS, Swinnen M, Vanhoutte D, Gao F, Torpai R, Baker AH, Padalko E,Neyts J, Schultheiss HP, Van de Werf F, Carmeliet P, Pinto M. Inhibition ofurokinase-type plasminogen activator or matrix metalloproteinases prevents
cardiac injury and dysfunction during viral myocarditis. Circulation. 2006;114:565–573.
51. Towbin JA. Inflammatory cardiomyopathy: there is a specific matrixdestruction in the course of the disease. Ernst Schering Research Foun-dation Workshop. Springer, Heidelberg, Germany. 2006:219–250.
52. Souders CA, Bowers SL, Baudino A. Cardiac fibroblast: the renaissancecell. Circ Res. 2009;105:1164–1176.
CLINICAL PERSPECTIVEHeart failure with normal ejection fraction (HFNEF) can be diagnosed in �50% of patients with the clinical syndrome ofHF. Nevertheless, the HFNEF syndrome seems to be heterogeneous and therefore will present with different pathologiesleading to the disease. It is assumed that an accumulation of cardiac collagen is 1 important mediator in the developmentof HFNEF. We show here that increased transendothelial migration of inflammatory cells triggers a profibrotic phenotypeby activating fibroblasts into myofibroblasts in cardiac tissue. Activated myofibroblasts, characterized by �-smooth muscleactin, are well known for excessive collagen production in other diseased tissues and express significantly more collagencompared with normal cardiac fibroblasts. Moreover, inflammatory cells reduced the expression of the collagendegradation system, the matrix metalloproteinases, again promoting cardiac fibrosis as 1 trigger for a stiff andnoncompliant ventricle. This transdifferentiation was induced by transforming growth factor-�, which was expressed byinflammatory monocytes in the heart. Interestingly, we document here that these inflammatory cells can be found morefrequently in cardiac tissue of the HFNEF group than in the control group. Therefore, continuous low-grade inflammationmight be 1 key player in the development and/or progression of HFNEF. This would make anti-inflammatory strategiesinhibiting transendothelial migration of cells into the cardiac tissue an interesting approach in treating HFNEF, a diseaseplagued by limited data.
52 Circ Heart Fail January 2011
by guest on January 20, 2011circheartfailure.ahajournals.orgDownloaded from