Cardiac Anatomy & Physiology
204
Cardiac Anatomy & Physiology
-
Upload
marcia-anderson -
Category
Documents
-
view
44 -
download
1
description
Cardiac Anatomy & Physiology. The Heart. Hollow, four chambered, muscular organ. The heart is found in the mediastinum between the right and left lungs. The four chambers are subdivided 2 atria (right & left) 2 ventricles (right & left). Atria. - PowerPoint PPT Presentation
Transcript of Cardiac Anatomy & Physiology
Cardiac Anatomy & Physiology





The Heart
Hollow, four chambered, muscular organ. The heart is found in the mediastinum
between the right and left lungs. The four chambers are subdivided
2 atria (right & left)2 ventricles (right & left)
Atria
Each atrium has thin-walls and is separated by the interatrial septum.
The atria act as collecting or holding chambers.
Ventricles
Each ventricle has thick muscular walls and is separated by the interventricular septum.
The ventricles act as pumps.The right ventricle pumps the unoxygenated blood
from your organs and tissues to the lungs.The left ventricle pumps the oxygenated blood
from your heart to your organs and tissues.


Circulation
The vasculature of your lungs is called pulmonary circulation.
The vasculature that supplies the heart with oxygen and nutrients is called coronary circulation.
The vasculature of all of your organs and tissues (everything besides your lungs and heart) is called systemic circulation.

Circulation
The right ventricle is responsible for pulmonary circulation.
The left ventricle is responsible for systemic & coronary circulation.


Valves of the Heart
You have four valves that separate the four chambers of the heart.Atrioventricular Valves (tricuspid and
bicuspid)
Semilunar Valves (pulmonic and aortic valves)


The Valves of the Heart
Atrioventricular Valves (tricuspid and bicuspid)
Semilunar Valves (pulmonic and aortic valves)


Valves
The first valve is between the right atrium & right ventricle. This valve is called the tricuspid valve. The valve is called tricuspid because the valve has three
flaps. The flaps are held in place by tendinous cords called
chordae tendinae. The chordae tendinae are secured to the walls of the
ventricle by the papillary muscles. When the ventricles contract the tricuspid valve closes. When the ventricles relax the tricuspid valve opens.

Valves
The second valve is between the right ventricle and the pulmonary trunk. This valve is called the pulmonary semilunar. The valve is called semilunar because of it’s new moon
shape. When the ventricles contract the pulmonary semilunar
valve opens. This allows the blood from the right side of the heart to be
pumped to the lungs. When the ventricles relax the pulmonary semilunar
valve closes.

Valves
The third valve is between the left atrium and the left ventricle. This valve is called the mitral or bicuspid valve. The valve is called bicuspid because the valve has two
flaps. The two flaps connect to the left ventricle by the same
principle as the tricuspid valve. When the ventricles contract the bicuspid valve closes. When the ventricles relax the bicuspid valve opens

Valves
The forth valve is between the left ventricle and the aortic trunk. This valve is called the aortic semilunar. The valve is called semilunar because of it’s new moon
shape. When the ventricles contract the aortic semilunar valve
opens. This allows the blood from the left side of the heart to be pumped
to the body.
When the ventricles relax the aortic semilunar valve closes.
Valves
Valves are suppose to be one-way however they can malfunction.Valve regurgitation = weak & leaky valveValve stenosis = constriction or narrowing of
passageway

Valves
Why do valves leak?Rheumatic feverAgingCongenital heart defects

Layers of the Heart
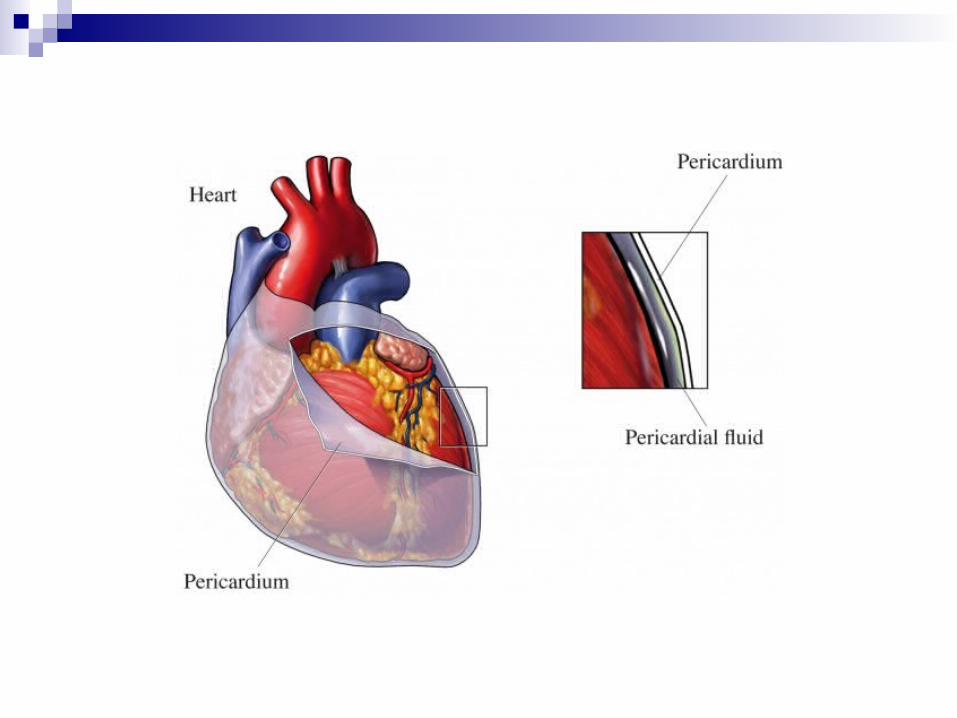
The heart is enclosed in a double walled sac called the pericardium. It consist of 2 layers
The outer layer is called the fibrous pericardium. The inner layer is called the serous pericardium.
The serous pericardium consist of 2 layers Parietal layer Visceral layer; also called epicardium.

Layers of the Heart
What is Pericarditis? It is inflammation of the double walled sac called the
pericardium. What causes pericarditis?
Trauma Infection Tumors
What are the symptoms? Chest pain Audible friction rub

Layers of the Heart
If worsening pericarditis or pericardial effusion can result in cardiac tamponade.
Cardiac tamponade = intrapericardial pressures increase to the point that it impairs the filling of the heart
Cardiac Tamponade is life threatening and is sometimes treated with pericardiocentesis.

Layers of the heart
The wall of the heart is made up of three layers.
Epicardium Corresponds to the visceral pericardium. Functions as an outer protective layer. Serous membrane that consists of connective tissue
covered by epithelium. Includes blood capillaries, lymph capillaries, and
nerve fibers.

Layers of the heart
The wall of the heart is made up of three layers.
Myocardium Relatively thick. Consists largely of cardiac muscle tissue responsible for
forcing blood out of the heart chambers. Muscle fibers are arranged in planes, separated by
connective tissues that are richly supplied with blood capillaries, and nerve fibers.

Layers of the heart
The wall of the heart is made up of three layers.
Endocardium Consists of epithelial and connective tissue that contains
many elastic and collagenous fibers. Connective tissue also contains blood vessels and some
specialized cardiacmuscle fibers called Purkinje fibers. Lines all of the heart chambers and covers heart valves. Is continuous with the inner lining of blood vessels--
endothelium.


Wall of the Heart
What is endocarditis? It is an infection and inflammation of the heart's inner lining
(endocardium). It is most common in people with damaged, diseased, or artificial heart valves.
What causes it? It is caused by bacteria that enter the bloodstream and settle on the heart
valves. What are the symptoms?
Chills & Fever Fatigue Weight loss Painful joints Persistent cough and SOB
How is it treated? IV Antibiotics
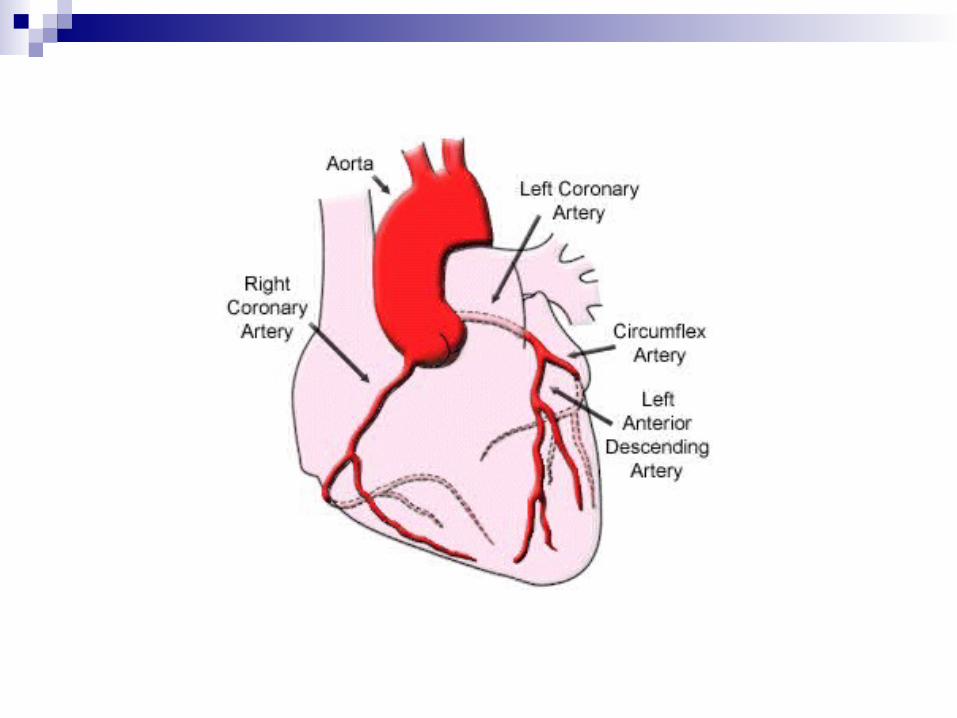
Blood supply to the Heart
The two main arteries that feed the heart:Left coronary artery
Circumflex branch Anterior interventricular branch
Right coronary artery Marginal branch Posterior interventricular branch

Blood supply to the Heart
The main veins that drain “used” blood from the heart: Great cardiac veins
drains the anterior side of the heart Middle cardiac vein
Drains the posterior side of the heart
The great cardiac and middle veins merge together into a cavity called the coronary sinus.
The thebesian vein then carries the “used” blood into the left and right atria.

Disorders
Atherosclerosis = hardening of the arteries which promotes clots and/or occlusions.
Thrombosis = a clot /coagulation of blood Embolism = thrombosis that has traveled from
location it was formed. Myocardial Ischemia = decreased oxygen availability
to the heart because of decreased blood flow or decreased oxygen in blood.
Myocardial Infarction = tissue death due to a loss of blood & glucose to the heart muscle.

Disorders
Congestive Heart Failure (CHF) = condition where the left side of the heart is damaged.
Cor Pulmonale = condition where the right side of the heart has decreased function.
Angina Pectoris = a severe pain or pressure in the chest caused by inadequate blood flow and oxygen content to the heart muscle.

Treatment for Disorders
Coronary Angioplasty = treats blockages of vasculature with a catheter or balloon.
Coronary Artery Bypass Graft (CABG) = artery graft from the leg or arm is inserted into coronary vasculature to bypass blocked arteries.




Blood flow through the Heart
Inferior Vena Cava/ Superior Vena Cava Right Atrium Tricuspid Valve Right Ventricle Pulmonary Semilunar Valve Pulmonary artery trunk Pulmonary artery Left/Right pulmonary artery Lungs
Blood flow through the Heart
Left/Right pulmonary vein Left Atrium Bicuspid/Mitral Valve Left Ventricle Aortic Semilunar Valve Aortic artery trunk Ascending Aorta
Brachiocephalic artery Left common carotid artery Left Subclavian artery
Descending Aorta xxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxx

Show cardiac cycle video

Cardiac Cycle
Cardiac cycle is the term referring to all or any of the events related to the flow of blood that occur from the beginning of one heartbeat to the beginning of the next

The frequency of the cardiac cycle is the heart rate
Every single 'beat' of the heart involves three major stages: atrial systole ventricular systole complete cardiac diastole The term diastole is synonymous with relaxation of a
muscle.It is the period of time when the heart relaxes after contraction in preparation for refilling with circulating blood.

The term systole is synonymous with contraction (movement or stretching) of a muscle. Think squeeze
The term diastole is synonymous with relaxation of a muscle. Think dilate.
It is the period of time when the heart relaxes after contraction in preparation for refilling with circulating blood.

Heart Rate
Heart rate is a term used to describe the frequency of the cardiac cycle.
It is considered one of the four vital signs Usually it is calculated as the number of
contractions (heart beats) of the heart in one minute and expressed as "beats per minute" (bpm).
Normal Heart rate in adults 60-100 bpm
Stroke Volume
Stroke volume is the amount of blood pumped by the left ventricle of the heart in one contraction
The heart does not pump all the blood out of the ventricle. Normally, only about two-thirds of the blood in the ventricle is put out with each beat Normal range
60 -120mL

Cardiac Output (Qt)
Cardiac output is the volume of blood being pumped by the heart, in particular a ventricle in a minute.
Cardiac Output (CO) = SV × HR Normal range is 4-6 lpm

Electrophysiology of the Heart
Contraction of the heart is initiated by an electrical stimulus
These contractions are a function of action potentials (electrical currents)
Action potentials consist of 5 phases0 = depolarization1-4 represent polarization
Electrical System of the Heart
Depolarization = electrical activity that triggers contraction of the heart muscle. Depolarization typically results from the influx of
positively charged sodium ions into the cell.
Repolarization = The restoration of a polarized state across a membrane, as in a muscle fiber following contraction. Repolarization results from the movement of
positively charged potassium ions out of the cell.

DEPOLARIZATION
REPOLARIZATION
RESTORATION OF IONIC BALANCE

Cardiac Cell Types
Contractile Muscle Fibers Bulk of myocardium responsible for the pumping
activity of the heart
Autorhythmic cells Pacemaker cells 1% of tissue, mostly located in the SA node Unique ability to spontaneously initiate an action
potential which in turn cause muscle fibers to contract
Cardiac Cells Four Properties
Automaticity Generates an action potential without stimulation
Excitability Irritability; lower stimulus needed to activate cell
Conductivity Transmits electrical current effectively; intercalated
disksContractility
Shortening and contraction in response to stimulus

Electrical Conduction System of the Heart
There are four structures embedded in the walls of the heart muscles that generate strong impulses and conduct them rapidly through the heart wall.
Electrical System of the Heart
Sino-atrial NodeSA node
Pacemaker 60 -100 bpm
Atrioventricular NodeAV node 40- 60 bpm
Bundle of HisAV bundle 20 – 40 bpmRight and Left bundle branches
Purkinje Fibers

Electrical System of the Heart

EKG
Electrocardiogram = graphic representation of the electrical activity of the heart’s conductive system over time. “electrical NOT mechanical” EMD/PEA
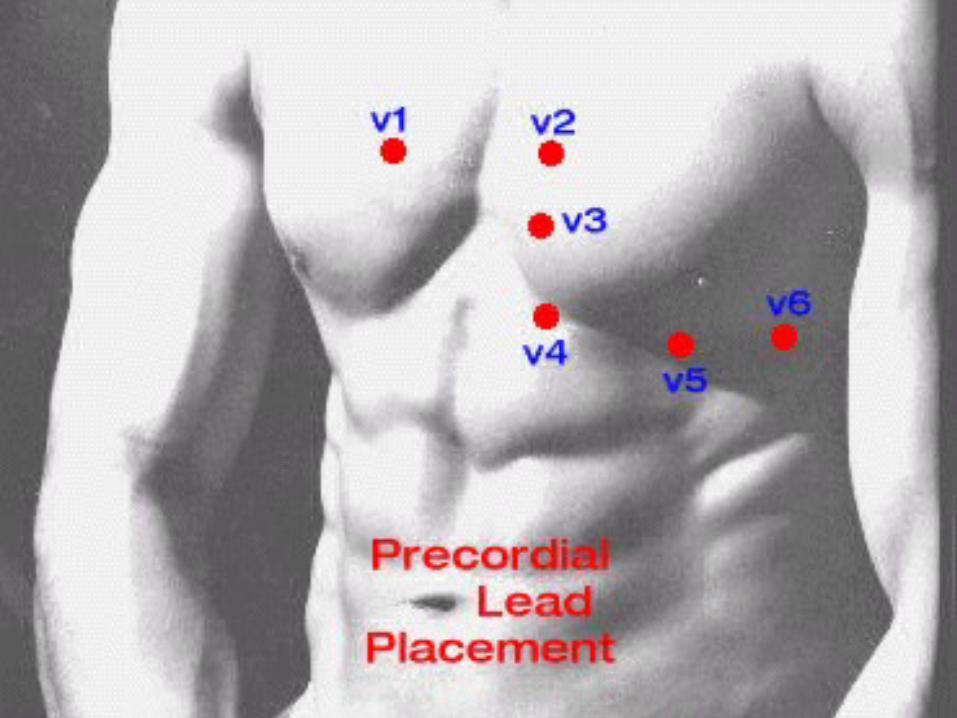
Leads are placed on the patient to evaluate the electrical system of the heart. 3 lead (monitoring) 12 lead (diagnostic)

standard limb lead configurations

A typical ECG tracing of a normal heartbeat (or cardiac cycle) consists of
a P wave, a QRS complex a T wave.
A small U wave is normally visible in 50 to 75% of ECGs.
The baseline voltage of the electrocardiogram is known as the isoelectric line.
Typically the isoelectric line is measured as the portion of the tracing following the T wave and preceeding the next P wave.

EKG

EKG


EKG
Des Jardins Pg. 416-417 Normal durations
P wave = 0.08 – 0.11 secP-R interval = 0.12 – 0.20 secQRS complex = < 0.10 secS-T segment = < 0.12 secT wave = < 0.20Q-T interval = < 0.38

EKG BASICS
EKGs are printed on standardized graph paper
The Y axis represents VOLTAGE The X axis represents TIME The Y axis is generally set at 5 or 10
mm/mV The X axis units are seconds

There are two sized boxes. 5 small boxes make up one large box Each small box equals 40 msec. Each large box equals 200 msec 5 large boxes equals 1 second

ECG paper is designed to move through the ECG machine at 25 mm per second.
Each of the smallest boxes are l mm square making the darker lined boxes 5 mm square.
Thus, at the usual rate of 25 mm/second flow of the paper through the machine, 5 large boxes pass through the machine per second or (5 x 60 seconds) 300 boxes
per minute.


Large boxes are used to estimate heart rate. Measure from QRS to QRS. Rates are approximate:
1 large box = 300 bpm.2 large boxes = 150 bpm.3 large boxes = 100 bpm.4 large boxes = 75 bpm.5 large boxes = 60 bpm.

Basic ECG Interpretation

NORMAL SINUS RHYTHM
Impulses originate at S-A node at normal rate. All complexes normal and evenly spaced.Rate 60 - 100/min

SINUS BRADYCARDIA
Impulses originate at S-A node at slow rate. All complexes normal and evenly spaced.Rate < 60/min

CAUSES OF SINUS BRADYCARDIA Coronary artery disease Increased intracranial pressure Hypothyroidism Hypoxemia Vagal stimulation
Gagging Coughing Suctioning

SINUS TACHYCARDIA
Impulses originate at S-A node at rapid rate. All complexes normal and evenly spaced.Rate 100-160/min

CAUSES OF SINUS TACHYCARDIA Fever Sepsis Hypoxemia CHF Shock Fear Exercise

ATRIAL FLUTTER
Impulses travel in circular course in atria. Rapid flutter waves and ventricular response can be irregular.

ATRIAL FIBRILLATION
Impulses have chaotic, random pathways in atria. Baseline irregular; ventricular response irregular.

PREMATURE VENTRICULAR CONTRACTION (PVC) A single impulse originates in the right ventricle. Time
interval between normal R peaks is a multiple of R-R intervals.

VENTRICULAR TACHYCARDIA
Impulse originates at ventricular pacemaker. Wide ventricular complexes. Rate here is> 120/min

VENTRICULAR FIBRILLATION
Chaotic ventricular depolarization. Rapid, wide, irregular ventricular complexes.

ASYSTOLE
Rate: none P wave: may be seen, but there is no ventricular response QRS: none Conduction: none Rhythm: none

Neural Control of the Heart
Many things play a role in controlling heart rate.Autonomic nervous systemBaroreceptorsAnxietyBody temperature


Baroreceptors
Arterioles are controlled by sympathetic impulses.
There are sympathetic fibers located in the vessels.
The medulla receives information from the baroreceptors located in the carotid & the aorta.
The medulla (vasomotor center) then feeds the impulses to the vessels based on the information.


Baroreceptors
The vessels either dilate or constrict based on the area of the body. In the heart, brain, and skeletal muscles:
↑ sympathetic impulses = vasodilatation ↓ sympathetic impulses = vasoconstriction
In the rest of the body: ↑ sympathetic impulses = vasoconstriction ↓ sympathetic impulses = vasodilatation

Baroreceptors
Normally there is a continuous stream of impulses which cause the vessels of the body to always be slightly constricted.This is called vasomotor tone.
xxxxxxxxxxxxxxxxxxxxxxxxxxxxxx

BLOOD
Blood is a highly specialized circulating tissue consisting of several types of cells suspended in a fluid medium known as plasma.
Responsible for transportation and protection The cellular constituents are:
red blood cells (erythrocytes), white blood cells (leukocytes), platelets (thrombocytes –cell fragments),
Blood Volumes
Blood volumesWhole blood
4 to 6 L average 7 to 9% of total body weight
Normal volumes of blood fractions Plasma = 2.6 L Formed elements = 2.4 L


Blood Plasma Liquid fraction of whole blood minus formed
elements. 55% of total blood volume Composition
90% water 10% dissolved substances
Foods & Salts About 3% O2 carried in plasma About 5% CO2 carried in plasma Most abundant solutes dissolved in plasma are plasma
proteins: Albumins Globulins Fibrinogen Prothrombin

Blood Plasma
Plasma minus clotting factors, proteins, is called serum.
Serum is liquid remaining after whole blood clots. Serum contains antibodies.

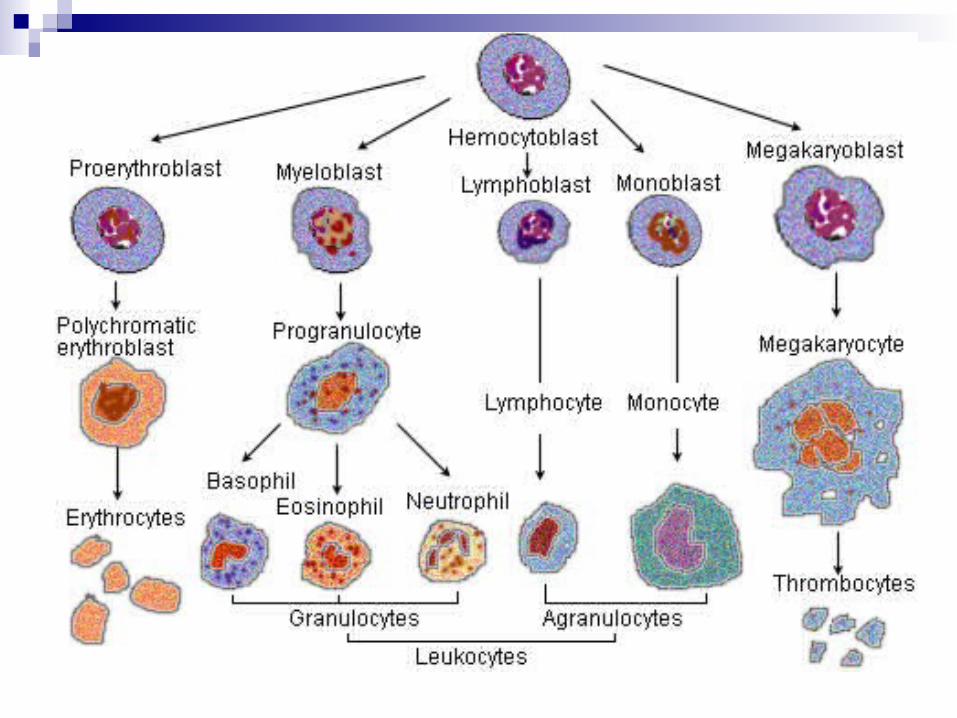
Formed Elements
Red Blood Cells (erythrocytes) White BloodCells (leukocytes)
Granular leukocytes Neutrophils Eosinophils Basophils
Nongranular leukocytes Lymphocytes Monocytes
Platelets (thrombocytes)

Erythrocytes (RBCs)
Characteristics:
Biconcave disk shape (thin center and thicker edges) results in large cellular surface area.
Tough and flexible plasma membrane deforms easily allowing RBCs to pass through small diameter capillaries.
Absence of nucleus and cytoplasmic organelles limits life span to about 120 days but provides more cellular space for iron containing hemoglobin.

Erythrocytes (RBCs)
Named according to size: normocytes (normal size about 7-9 μm in diameter) microcytic (small size) macrocytic (large size)
Named according to hemoglobin content of cell:
normochromic (normal Hb content) hypochromic (low Hb content) hyperchromic (high Hb content)

Erythrocytes
Erythrocytes (RBCs)
Hematocrit Percentage of RBCs in relation to total blood volume
Normal Men 45% Women 42%
Hemoglobin the iron-containing oxygen-transport metalloprotein in the red blood cells
of the blood Measured as weight per 100 ml
Men 14-18 gm/dl women: 12-16 gm/dl
Content Men 5,000,000 mm3 Women 4,000,000 mm3

Erythrocytes (RBCs)
General functions:Transportation of O2 and CO2
Combined with hemoglobin Oxyhemoglobin (Hb + O2) Carbaminohemoglobin (Hb + CO2)
Important role in homeostasis & acid base balance.

Leukocytes or WBCs
General function is protection of body from microorganisms by phagocytosis or antibody formation.
WBC normal range is 5,000 to 10,000/mm3 of blood. Leukopenia—total numbers below 5,000/mm3 of blood.
Infrequent but may occur with malfunction of blood forming tissues or diseases affecting immune system, such as AIDS.
Leukocytosis—total numbers over 10,000/mm3 of blood. Frequent finding in bacterial infections Classic sign in blood cancers (leukemia)
Differential WBC count is a component test in CBC; measures proportions of each type of WBC in blood sample.
Leukocytes

Leukocytes or WBCs
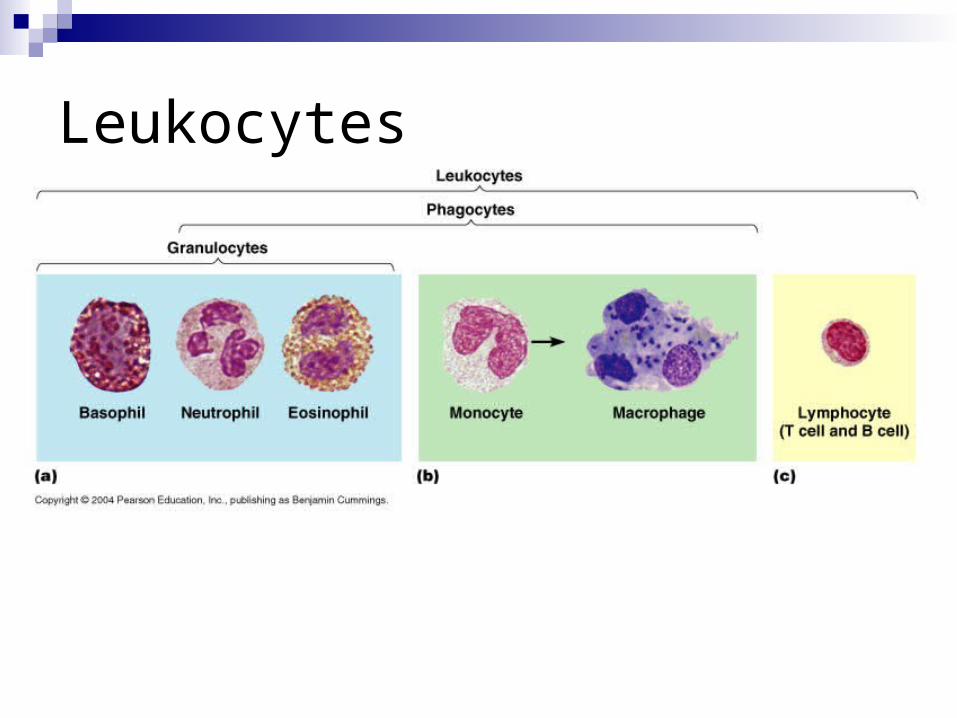
Leukocyte types and functions: Granulocytes
Neutrophils Eosinophils Basophils
Agranulocytes Monocytes in peripheral blood (macrophages in tissues) Lymphocytes
B lymphocytes (Plasma cells) T lymphocytes

Leukocytes or WBCs Functions of WBCs
Neutrophils Most numerous type of phagocyte Numbers increase in bacterial infections
Monocytes Largest leukocyte Aggressive phagocyte—capable of engulfing larger
bacteria and cancer cells Develop into much larger cells called macrophages after
leaving blood & entering tissue spaces

Leukocytes or WBCs
Eosinophils Weak phagocyte Active against parasites and
parasitic worms Involved in allergic reactions
Basophils Related to mast cells in tissue
spaces Both mast cells and basophils
secrete histamine (causes inflammation)
Basophils also secrete heparin (an anticoagulant)

Leukocytes or WBCs
Lymphocytes B lymphocytes involved in
immunity against disease by secretion of antibodies
Mature B lymphocytes are called plasma cells
T lymphocytes involved in direct attack on bacteria or cancer cells (not antibody production)

Platelets and Blood Clotting
Platelets Play essential role in blood clotting
Normal platelet count 150,000—340,000/mm3
Blood vessel damage causes platelets to become sticky and form a “platelet plug”
Accumulated platelets release additional clotting factors that enter into the clotting mechanism
Platelets ultimately become a part of the clot itself
Platelets

Platelets and Blood Clotting
Clotting in a nutshell Damaged tissue cells along with platelets release
prothrombin activator. Prothrombin activator, along with calcium converts
prothrombin the thrombin Thrombin combines with fibrinogen to form fibrin Fibrin creates a “net” that begins to form the “plug”.



Altering the blood clotting mechanism
Application of gauze (rough surface) to wound causes platelet aggregation and release of clotting factors
Administration of Vitamin K will increase synthesis of prothrombin
Coumadin will delay clotting by inhibiting prothrombin synthesis
Heparin delays clotting by inhibiting conversion of prothrombin to thrombin
A drug called tissue plasminogen activator (TPA) is used to dissolve clots that have already formed

Red Blood Cell Disorders
Most often related to either: overproduction of RBCs, called polycythemia low oxygen carrying capacity of blood,called
anemia

Polycythemia
Cause is generally cancerous transformation of red bone marrow Dramatic increase in RBC numbers—often in excess of 10
million/mm3 of blood—hematocrit may reach 60% Signs and symptoms include:
Increased blood viscosity or thickness Slow blood flow and coagulation problems Frequent hemorrhages Distension of blood vessels and hypertension
Treatment may include: Blood removal Irradiation and chemotherapy to suppress RBC production

Polycythemia
Anemia
Caused by either: low numbers or abnormal RBCs low levels or defective types of Hb
Normal Hb levels 12-14 g/100 ml of blood Low Hb level (below 9 g/100 ml of blood) classified as
anemia Majority of clinical signs of anemia related to low
tissue oxygen levels Fatigue; skin pallor Weakness; faintness; headache Compensation by increasing heart and respiratory rates

Types of Anemia
TypesHemorrhagic anemiaAplastic anemiaDeficiency anemiaHemolytic anemia

Hemorrhagic anemia
AcuteBlood loss is either:
immediate surgery or trauma
chroniculcers or cancer

Aplastic anemia
Characterized by low RBC numbers and destruction of bone marrow
Often caused by: toxic chemicals irradiation certain drugs

Aplastic anemia

Deficiency anemia
Caused by inadequate supply of some substance needed for RBC or hemoglobin production.
Types: Pernicious anemia Iron deficiency anemia Folate deficiency anemia

Iron deficiency anemia
Caused by deficiency or inability to absorb iron needed for Hb synthesis (dietary iron deficiency is common worldwide)
RBCs are microcytic and hypochromicHematocrit is decreasedTreatment is oral administration of iron
compounds

Iron deficiency anemia

Pernicious anemia
Caused by Vitamin B12 deficiency Genetic related autoimmune disease Decreased RBC, WBC, and platelet
numbers RBCs are macrocytic Classic symptoms of anemia coupled with
CNS impairment Treatment is repeated Vitamin B12 injections

Folate deficiency anemia
Folate, also called folic acid, is necessary for red blood cell formation and growth.
RBCs are macrocytic. Some medications, such as Dilantin (phenytoin),
interfere with the absorption of this vitamin. Because folate is not stored in the body in large amounts, a continual dietary supply of this vitamin is needed.

Vitamin B12 and folate deficiency anemia.

Hemolytic anemia Caused by either:
decreased RBC life span increased RBC rate of destruction
Symptoms are related to retention of RBC breakdown products: Jaundice Swelling of spleen Gallstone formation Tissue iron deposits
Types: Sickle Cell Anemia Thalassemia Erythroblastosis fetalis

Hemolytic anemia

Sickle Cell Anemia
Genetic disease resulting in formation of abnormal hemoglobin (HbS) primarily in the African American race
RBCs become fragile and assume sickled shape when blood oxygen levels decrease
Sickle cell trait is mild (one defective gene) Sickle cell disease more serious (two defective
genes); causes blood stasis, clotting and “crises” that may be fatal
Affects 1 in every 600 African American newborns

Sickle cell anemia


White Blood Cell Disorders
Two major types of WBC cancers or neoplasmsLymphoid (lymphatic cells) neoplasms—result
from B and T lymphocyte precursor cells or their descendent cell types
Myeloid (bone marrow cells) neoplasms—result from the malignant transformation of precursor cells of granulocytic WBCs, monocytes, RBCs, and platelets

White Blood Cell Disorders
Multiple myeloma Cancer of B lymphocytes (plasma cells) Most “deadly” blood cancer in people over age 65 Causes bone marrow disfunction and production of
defective antibodies Characterized by:
Recurrent infections and anemia Destruction and fracture of bones
Treatment includes chemotherapy, drug antibody therapy, and marrow and stem cell transplantation
White Blood Cell Disorders
Leukemias—WBC related blood cancersCharacterized by marked leukocytosis Identified as:
Acute = rapid development of symptoms Chronic = slow development of symptoms Lymphoid = lymphatic cells Myeloid = bone marrow cells

Chronic Lymphocytic Leukemia (CLL)
Average age of onset is 65; rare under age 30 More frequent in men than women Often diagnosed unexpectedly in routine physical
exams with discovery of marked B lymphocytic leukocytosis
Generally mild symptoms include anemia, fatigue, and enlarged often painless lymph nodes
Most patients live many years following diagnosis Treatment of severe cases involves chemotherapy
and radiation

CLL

Acute Lymphocytic Leukemia (ALL)
Primarily a disease of children between 3 and 7 years of age; 80% of children who develop leukemia have this form of the disease
Highly curable in children but less so in adults Onset is sudden—marked by fever, leukocytosis,
bone pain and increased infections Lymph node, spleen and liver enlargement is
common Treatment includes chemotherapy, radiation, and
bone marrow or stem cell transplants

ALL

Chronic Myeloid Leukemia (CML) Accounts for about 20% of all cases of leukemia Occurs most frequently in adults between 25 and 60
years of age Caused by cancerous transformation of granulocytic
precursor cells in the bone marrow Onset and progression of disease is slow with
symptoms of fatigue, weight loss and weakness Diagnosis often made by discovery of marked
granulocytic leukocytosis and extreme spleen enlargement
Treatment by new “designer drug” Gleevec or bone marrow transplants is curative in over 70% of cases

CML

Acute myeloid leukemia (AML)
Accounts for 80% of all cases of acute leukemia in adults and 20% of acute leukemia in children
Characterized by sudden onset and rapid progression Symptoms include leukocytosis, fatigue, bone and
joint pain, spongy bleeding gums, anemia and recurrent infections
Prognosis is poor with only about 50% of children and 30% of adults achieving long term survival
Bone marrow and stem cell transplantations have increased cure rates in selected patients

AML

White Blood Cell Disorders
Infectious mononucleosis Noncancerous WBC disorder Highest incidence between 15 and 25 years of age Caused by virus in saliva Leukocytosis of atypical lymphocytes with abundant
cytoplasm and large nuclei Symptoms include fever, severe fatigue, sore throat,
rash, and enlargement of lymph nodes and spleen Generally self-limited and resolves without
complications in about 4 to 6 weeks

“mono”

Leukocytes or WBCs
Lymphocytes B lymphocytes involved in
immunity against disease by secretion of antibodies
Mature B lymphocytes are called plasma cells
T lymphocytes involved in direct attack on bacteria or cancer cells (not antibody production)

Clotting disorders
Hemophilia A X-linked inherited disorder results from inability to produce
Factor VIII (a plasma protein) responsible for blood clotting In severely affected individuals frequent and extensive
episodes of bleeding can be life threatening Characterized by easy bruising, deep muscle hemorrhage,
blood in urine, and repeated episodes of bleeding into joints causing pain and deformity
Treatment includes administration of Factor VIII, injury prevention, and avoiding drugs like aspirin that alter the clotting mechanism

hemophilia

Hemophilia and inheritance

Clotting disorders
Thrombocytopenia—caused by reduced platelet counts Characterized by bleeding from small blood vessels,
most visibly in the skin and mucous membranes Platelet count below 20,000/mm3 may cause
catastrophic bleeding (Normal platelet count 150,000—340,000/mm3)
Most common cause is bone marrow destruction by drugs, chemicals, radiation, and diseases such as cancer, lupus, and HIV/AIDS
Treatment may involve transfusion of platelets, corticosteroid type drugs, or removal of the spleen.

Blood Types
ABO system Type A blood—type A antigens in RBCs; anti-B type
antibodies in plasma Type B blood—type B antigens in RBCs; anti-A type
antibodies in plasma Type AB blood—type A and type B antigens in RBCs;
no anti-A or anti-B antibodies in plasma universal recipient blood
Type O blood—no type A or type B antigens in RBCs; both anti-A and anti-B antibodies in plasma
universal donor blood


Blood Types
Rh systemRh-positive blood
Rh factor antigen present in RBCsRh-negative blood
No Rh factor present in RBCs No anti-Rh antibodies present naturally in plasma Anti-Rh antibodies, however, appear in the plasma
of Rh-negative persons if Rh-positive RBCs have been introduced into their bodies (pregnancy)

Erythroblastosis Fetalis
Hemolytic disease of newborn Caused by blood ABO or Rh factor incompatibility during
pregnancy between developing baby and mother The maternal antibodies fighting against “foreign” fetal
RBCs or Rh factor can cross placenta, enter the fetal circulation, and destroy the unborn baby’s RBCs
Symptoms in developing fetus related to decline in RBC numbers and Hb levels; jaundice, intravascular coagulation, and heart and lung damage are common
Treatment may include utero blood transfusions and early delivery of the baby
Prevention of Rh factor incompatibility now possible by administration of RhoGAM to Rh negative mothers
xxxxxxxxxxxxxxxxxxxxxxxxxxx

Rh factor

Rh factor


Erythroblastosis fetalis

Erythroblastosis fetalis

Blood Pressure
“pressure generated by the blood” Highest in the arteries Lowest in the veins
Blood pressure gradient = difference between two blood pressures The difference between the beginning pressure and
the ending pressure within a circuit. What two pressures would we look at to compute the
systemic blood pressure gradient?

Blood Pressure
The maximum pressure generated during ventricular contraction is called the systolic pressure.
The lowest pressure that remains prior to the next ventricular contraction is called the diastolic pressure.

Blood Pressure
Hypertension = increased arterial pressureCan lead to ruptured vessels & stroke
Hypotension = decreased arterial pressureCan lead to the loss of circulation & life will
cease.Commonly seen with massive hemorrhage.
Blood Pressure
Factors that affect blood pressure Blood volume
Directly related to BP Force of heart contractions
Affects cardiac output directly, unless there is a noted decrease in blood volume i.e. hemorrhage
Heart rate Affects cardiac output directly. This is only true if the stroke
volume does not decrease sharply when the heart rate increases, due to less fill time.
Blood viscosity Directly related to BP

Pulse and Pulse points
Temporal Facial Carotid Brachial Radial Femoral Popliteal Posterior tibial Dorsal pedal


Circulatory Shock
Failure of the circulatory system to deliver oxygen to the tissues adequately, resulting in cell impairment.
Types Cardiogenic Shock Hypovolemic Shock Neurogenic Shock Anaphylactic Shock Septic Shock

Neural Control of Vascular System
Vasomotor center (medulla) coordinates vasodilatation & vasoconstriction by controlling the # of sympathetic impulses.
Systemic = increased impulses will vasoconstrict Systemic = decreased impulses will vasodilate
HOWEVER… Heart, brain, & skeletal muscle = increased
impulses will vasodilate Heart, brain, & skeletal muscle = decreased
impulses will vasoconstrict

Baroreceptor Reflex
Baroreceptors regulate the arterial BP by initiating reflex adjustments.
“stretch receptors” Found in:
Walls of the aortic arch Impulses travel along the vagus nerve
Walls of the carotid artery Impulses travel along the glossopharyngeal nerve

Effects of cardiac cycle on BP
BP rises & falls in a pattern like the phases of cardiac cycle.
When ventricles contract blood is forced into pulmonary trunk & aorta. At this point the pressure in the arteries increases sharply.
Pulmonary Blood Flow
Distribution of pulmonary blood flowProgressively decreases from the base to the
apex. Factors affecting distribution:
GravityCardiac outputPulmonary vascular resistance

Pulmonary Blood Flow
Blood is gravity dependant because it is relatively heavy.
Average lung is 30cm from the base to the apex. If blood was to fill the lung form the base to the apex it
would need 30cmH2O of pressure (22mmHg) to over come the gravitational force.
The pulmonary artery enters in the middle (hilum) so the blood that reaches the apex needs at least 11mmHg to over come the gravitational force.

Pulmonary Blood Flow
The vessels @ the base have greater pressure than those @ the apex.
The increased pressure in the vessels of the bases cause the vessels to widen, which decreases pulmonary vascular resistance.
These factors change based on lung position.


Zones of Pulmonary Circulation*These factors due change based on lung position
Zone 1 Least gravity dependant Worst perfusion Best aeration
Zone 2 Good perfusion Good aeration
Zone 3 Most gravity dependant Best perfusion Worst aeration
xxxxxxxxxxxxxxxxxxxxxxxxxxxxx

Lung zones

Hemodynamics
The study of the forces that influence the circulation of blood.Consist of measurements and calculations.
A pulmonary artery catheter (Swan-ganz catheter) is used to collect hemodynamic measurements in critically ill patients.

Hemodynamics
Units used in hemodynamics:mmHgDyne
A unit of force which accelerates a mass of 1 gram @ a rate of 1cm/sec.

Hemodynamics
Hemodynamics are either measured or calculated.Measured = an instrument is used to collect
information.Calculated = measurements are used in
formulas to compute additional information Because hemodynamic parameters will vary with
the size of the patient, some hemodynamic values are “indexed” by body surface area (BSA)

Hemodynamics
Calculation for BSA (m2)Centimeters & Kilograms
(Height (cm) X Weight (kg) /3600) .5
Inches & Pounds (Height (in) X Weight (lb) /3131) .5

For example… Me! I weigh about 100 kg, and my height is
about 188 cm (1in = 2.54 cm). So, my BSA is (188X100)/3600, then take
the square root of this… Answer is approximately 2.3m squared

Swan-ganz catheter

Swan-ganz catheter
Inserted into the internal jugular or the subclavian vein
Very invasive procedure; only used in critically ill patients under constant observation.
Complications include: Pneumothorax / Hemothorax Air emboli Infection Pulmonary artery rupture



Hemodynamics
Directly measured:Central Venous Pressure CVPRight Atrial Pressure RAPMean Pulmonary Artery Pressure PAPulmonary Capillary Wedge Pressure PCWPCardiac Output CO

Hemodynamics
Computed:Stroke Volume SVStroke Volume Index SVICardiac Index CIPulmonary Vascular Resistance PVRSystemic Vascular Resistance SVR
p.459 Des Jardins

Central Venous Pressure & Right Atrial Pressure (measured) RAP is very close to CVP CVP is a measure of atrial preload. Atrial preload is determined;
distribution of blood within the body total blood volume presence and force of atrial contraction

Mean Pulmonary Artery Pressure & Pulmonary Capillary Artery Wedge Pressure (measured)
PCWP
End-diastole represents the moment in the cardiac cycle when the ventricle contains the greatest volume of blood, just before it contracts and ejects its volume.
The wedged pulmonary artery catheter reflects LVEDP because at end-diastole, the mitral valve is open and this creates communication between the left atria, left ventricle, and pulmonary vascular bed. In other words, “the doors are all open” from the LV to the pulmonary capillary.
The “window into the left heart”


Cardiac Output
A bolus of sterile solution that is colder than the patients blood is injected into the proximal port of a pulmonary artery catheter located in the right atrium.
In the atrium, the solution mixes with the blood and passes through the tricuspid valve into the right ventricle.
A thermistor within the catheter senses the change in blood temperature as the blood passes the catheter tip located in the pulmonary artery.
The change in temperature over time is calculated by a computer and converted into a measurement of cardiac output.

Cardiac Output (measured)

Stroke Volume (computed)
Volume of blood ejected by ventricle with each contraction. Normal 40-80 mL
Stroke volume is derived by dividing the cardiac output by the heart rate
Determinants of stroke volume: Preload Afterload Myocardial contractility

Determinants of stroke volume
Preload = how much blood is returning to the heart, and how well can the heart muscle accommodate it
“rubber band” Afterload = the forces “past the heart” which the
ventricles must fight against Viscosity & volume = Pulling/pushing ketchup vs. water
through a straw Vascular cross-sectional surface area = Long straw vs. short
straw Vascular resistance = Coffee straw vs. Slurpee straw
Myocardial contractility Contractility = inotropism

Stroke Volume Index (computed)
A patient has a stroke volume of 40mL This patient is 6’5” 280lb Is this a good value for this patient? NO! How do we know if a stroke volume is
appropriate? Stroke Volume Index

Stroke Volume Index (computed)
SVI = SV/BSANormal = 30 – 65 Ml/beat/m2

Cardiac Index (computed)
Normalizes Cardiac Output (measured) to body surface area.
CI = CO/BSA
Normal 2.5-4.2 L/min/m2
Vascular resistance
Pulmonary system low resistance system “short straw”
Systemic system high resistance “long straw”

Vascular resistance (computed)
Blood pressure is directly related to vascular resistance.When vascular resistance increases this will
cause BP to increase. When the straw diameter gets smaller, you have to
pull/push harder!

Vascular resistance
Vascular resistance = blood pressure
cardiac output
You are looking at what pressure it takes to
eject a liter of blood.

Pulmonary vascular resistance
The PVR reflects the afterload of the right ventricle.
When looking at PVR, you must have your pressures represent the “beginning to the end” of the pulmonary circuit.
What is the beginning of the pulmonary circuit? What is the end of the circuit?

Pulmonary vascular resistance
PVR = (PA – PCWP/CO) X 80
The constant 80 is a conversion factor for adjusting to the unit of dyne/sec/cm-5

Systemic Vascular Resistance
The SVR reflects the afterload of the left ventricle.
When looking at SVR, you must have your pressures represent the “beginning to the end” of the systemic circuit.
What is the beginning of the systemic circuit? What is the end of the circuit?

Systemic Vascular Resistance
SVR = (MAP – CVP/CO) X 80
The constant 80 is a conversion factor for adjusting to the unit of dyne/sec/cm-5