CapRI - Final Results of the Open-label, Multi-center, Randomized Phase III Trial of Adjuvant...
25
CapRI - Final Results of the Open-label, Multi-center, Randomized Phase III Trial of Adjuvant Chemoradiation Plus Interferon-2b (CRI) versus 5-FU/FA for Patients with Resected Pancreatic Adenocarcinoma gela Märten, Jan Schmidt, Jürgen Debus, Sabine Harig, Thomas Herrmann, tja Lindel, Justus Klein, Detlef Bartsch, Lorenzo Capussotti, Carl Zülke, iner Kunz, Ulrich Mansmann, Markus W. Büchler University of Heidelberg, Hospital of Bielefeld, University of Regensburg, Istituto per la Ricerca e la Cura del Cancro, Torino St. Joseph Hospital, Berlin,
-
Upload
sharleen-harrison -
Category
Documents
-
view
219 -
download
0
description
Virginia Mason ESPAC-1chemotherapy Neoptolemos et al., 2004, NEJM Picozzi et al., 2003, Am J Surg a adjuvant CRI p ChemoRadioImmunotherapy of pancreatic carcinoma CapRI Rationale 5-FU/Cisplatin/RT/IFN- 5-FU
Transcript of CapRI - Final Results of the Open-label, Multi-center, Randomized Phase III Trial of Adjuvant...

CapRI -Final Results of the Open-label, Multi-center,
Randomized Phase III Trial of Adjuvant Chemoradiation Plus Interferon-2b (CRI)
versus 5-FU/FA for Patients with Resected Pancreatic Adenocarcinoma
Angela Märten, Jan Schmidt, Jürgen Debus, Sabine Harig, Thomas Herrmann, Katja Lindel, Justus Klein, Detlef Bartsch, Lorenzo Capussotti, Carl Zülke, Reiner Kunz, Ulrich Mansmann, Markus W. Büchler
University of Heidelberg, GermanyHospital of Bielefeld, Germany
University of Regensburg, Germany Istituto per la Ricerca e la Cura del Cancro, Torino, Italy
St. Joseph Hospital, Berlin, Germany

Financial DisclosureRelated to the trial:
– Travel Grants from Essex Pharma
Unrelated to the trial– Boehringer Ingelheim (employment since 2009)– Roche (research funding)– Novartis (research funding)– Amgen (advisor)– Morphotek (advisor)– Bayer (honoraria)– …
This trial was supported by – Manfred-Lautenschläger Foundation, Germany

Virginia MasonVirginia MasonESPAC-1 ESPAC-1 chemotherapychemotherapy
Neoptolemos et al., 2004, NEJMPicozzi et al., 2003, Am J Surg
aadjuvant CChemoRRadioIImmunotherapy of ppancreatic carcinoma
CapRICapRI
Rationale
5-FU/Cisplatin/RT/IFN-5-FU/Cisplatin/RT/IFN-
5-FU5-FU

Study type Open, prospective, randomized, controlled, multi-center IIT
Recruitment August 2004-December 2007Sample size 110 (=0.05; power = 80%)Primary endpoint Overall survival in both armsSec. endpoints Safety, DFS, QoL, Screening for predictive
markersStudy centers Heidelberg, Berlin, Torino, Bielefeld,
RegensburgData Manage-ment/Biometrics
Institutes for Medical Biometrics, Universities of Heidelberg and Munich
DSMB Two oncologists, 1 biometricianOn-site monitoring
Independent CRO
Study Design

Inclusion Criteria• R0 or R1 pancreatic adenocarcinoma• Treatment start within 12 weeks after surgery• Performance status: Karnofsky 70• Creatinine 1.5 mg/dL, CrCl ≥ 60 ml/min
Exclusion Criteria• Residual metastatic or incompletely resected local disease• Former radiotherapy in respective region• Patients with severe pulmonary disease• Patients with significant cardiovascular disease • Patients with immunodeficiencies or autoimmune diseases• Presence or history of severe depression
Eligibility

study-arm A
study-arm B
week 0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23
FA 20 mg/m² as bolus injection, followed by5‑FU 425 mg/m² as short infusion 5 days/week
X X X X X X
All patients are treated as outpatients
Cisplatin 30 mg/m² over 60‘ IFN-2b s.c. 3 Mio Units 3/week (total 17x)
EBRT 50.4 Gy in 28 fractions
5-FU 200 mg/m²/day CI
Knaebel et al., BMC Cancer 2005
R
x x x x x x-------------------
Treatment Scheme
O
low dose Interferon(LDI) prior to therapy
cycle 1 CRI

*Screening-log was only kept at Heidelberg
Allocated to intervention 67Received allocated intervention 57Did not receive allocated intervention 10
-not meeting inclusion criteria 3-Withdrawal 7
Allocated to intervention 65Received allocated intervention 53Did not receive allocated intervention 12
-not meeting inclusion criteria 5-Withdrawal 7
Analyzed 53Excluded from analysis 0
Assessed for eligibility510 patients*
Lost to follow-up 0Discontinued intervention 7
Lost to follow-up 1Discontinued intervention 9
Analyzed 57Excluded from analysis 0
Excluded: 378*-Not meeting incl. crit.: 227*
Histology 167General condition 48Others 12
-Refused to participate: 151*Distance 62Concers about trial 62Other trials 17Others 15
Arm BArm A

A B both arms p-valueage 63 [37;74) 63 [33;77] 63 [33;77] 0.95femalemale
19 (36%)34 (64%)
31 (54%)26 (46%)
50 (45%)60 (55%) 0.09
R0R1
29 (55%)24 (45%)
37 (66%)19 (34%)
66 (61%)43 (39%) 0.25
T1T2T3T4
1 (2%)2 (4%)
49 (92%)1 (2%)
0 (0%)1 (2%)
55 (96%)1 (2%)
1 (1%)3 (3%)
104 (95%)2 (2%) 0.71
N0N1
11 (21%)42 (79%)
12 (21%)45 (79%)
23 (21%)87 (79%) 1.00
G1G2G3
1 (2%)34 (64%)18 (34%)
1 (2%)40 (70%)16 (28%)
2 (2%)74 (68%)33 (31%) 0.77
pp WhippleWhippleleft resection
35 (66%)4 (8%)
14 (26%)
39 (69%)11 (19%)
7 (12%)
74 (67%)15 (14%)21 (19%) 0.06
treatment start [days] 58.8 ± 14.2 57.3 ± 15.2 58.0 ± 14.7 0.50CA 19.9 preop [U/ml] 991 +/- 2574 409 ± 613 693 ± 1865 0.58Diabetes Mellitus-pankreopriv -no
16 (30%)9 (17%)
28 (53%)
17 (30%)3 (5%)
31 (54%)
33 (30%)12 (11%)59 (54%) 0.54
BMI <20BMI <25BMI <30BMI >30
7 (13%)32 (60%)12 (23%)2 (4%)
10 (18%)27 (47%)16 (28%)4 (7%)
17 (16%)59 (54%)28 (26%)6 (6%) 0.58
Patient’s Demographics

External ValiditySelection bias Are the populations representative?
–Eligibility criteria are limited to the (unavoidable) restrictions for safety reasons and clinical restrictions
–CapRI patients do not differ from the ‘average patient’.–No evidence of recruiting bias
Performance bias Are the interventions feasible under ‚real world’ conditions?
–Only in specialized centers
Attrition bias Are under ‘real world conditions’ similar drop-outs to be expected?
–Rather more. Therefore, no impact on transferability into ‘real world’.
Detection bias Are the endpoints relevant?
–Definitely
External validity is given
Sorg et al., Pancreas, 2009

Drug-Administration
Dose administeredcycle 1 arm
Acycle 2-3
arm A arm B% patients that received total dose 5.7% 11.3% 56.1%
% of administered drugIFN-2b 95 ±12%
5-FU 72 ± 23% 81 ± 26% 86 ± 23%
Cisplatin 75 ± 19%
Radiation 98 ± 7%

Toxicitycycle 1 arm AN = 53
cycle 2 arm AN = 51
cycle 3 arm AN = 46
arm B N = 57
Pts experienced CTC grade ¾ 17 (32.1%) 2 (3.9%) 2 (4.3%) 9 (15.8%) Grade 3 toxicities in >5% of patients:
Neutropenia 28 (52.8%) - - -
Hypovolemia / electrolyte disturbances*
8 (15.1%) - - -
Nausea / vomiting 8 (15.1%) - - -
Anaemia 3 (5.7%) - - -
Diarrhoea 3 (5.7%) - - 6 (10.5%)
Thrombopenia 3 (5.7%) - - -
Grade 4 toxicities 11 (20.8%) - - 1 (1.8%)Acute renal insufficiency 1 (1.9%) - - -
Neutropenia 7 (13.2%) - - -
Hypovol. / electrolytes 1 (1.9%) - - -
Hand Foot Syndrome 1 (1.9%) - - -
Nausea / vomiting 1 (1.9%) - - -
Diarrhoea - - - 1 (1.8%)
*Hoffmann et al., BMC Cancer 2006

EORTC QLQ C30
0
10
20
30
40
50
60
70
80
90
100
day 0day 15
day 38
day 64
day 120
FU 1FU 2
FU 3FU 4
FU 5FU 6
FU 7FU 8
scor
e
Physical functioning - A Physical functioning - B Role functioning Arm ARole functioning Arm B Emotional functioning - A Emotional functioning - BCognitive functioning - A Cognitive functioning - B Social functioning - ASocial functioning - B Global Health Status - A Global Health Status - B
Follow-up every 3 monthscycle 2-3cycle 1
• Decrease in QoL during cycle 1 • Recovery after end of cycle 1• Similar to better QoL during follow-up (p = 0.02)

CES-D Depression Scale
• Increase of depression score during IFN-therapy
• Complete recovery after end of cycle 1
0
2
4
6
8
10
12
14
16
18
20
day 0 day 15 day 38 day 64 day 120 FU 1 FU 2 FU 3 FU 4 FU 5 FU 6 FU 7 FU 8
scor
e
arm Aarm B
Depression
Follow-up (every 3 months)
cycle 2-3cycle 1

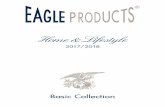
No at riskArm A 53 53 47 39 33 24 16 12 8 6 3Arm B 57 56 45 35 29 23 17 11 7 5 3
Median Follow-up: 26.9 mo
Overall Survival
MedianMedian 95% CI95% CIpp--
valuevalueArm A 32.1 [22.8; 42.2] 0.490
Arm B 28.4 [19.5; 38.6]

No at riskArm A 53 53 45 36 29 20 14 10 7 6 3Arm B 57 56 43 32 26 18 11 6 5 3 1
Disease Free Survival
MedianMedian 95% CI95% CI pp-value-valueArm AArm A 24.8 [19.3; 32.1] 0.4302
Arm BArm B 22.1 [17.5; 29.3]

Localisation of relapse
Arm AN = 41
Arm BN = 45
TotalN = 86 p-value
Local 12 (29.3%) 25 (55.6%) 37 (43.0%) 0.014
Liver 17 (41.5%) 10 (22.2%) 27 (31.4%) NS
Lung 5 (12.2%) 2 (4.4%) 7 (8.1%) NS
Lymph node 1 (2.4%) 5 (11.1%) 6 (7.0%) NS
Peritoneal carcinoma
5 (12.2%) 1 (2.2%) 6 (7.0%) NS
Unknown 1 (2.4%) 2 (4.4%) 3 (3.5%) NS

Resection margins
Arm A: R0 --- R1 ---Arm B: R0 --- R1 ---
R1 N Median 95% CI p-ValueArm AArm A 24 33.0 [18.6; ] 0.1317
Arm BArm B 19 16.8 [10.4; 27.9]

Treatment start
--- < 8 weeks--- > 8 weeksp = 0.023
--- arm A > 8 weeks--- arm B > 8 weeksp = 0.12

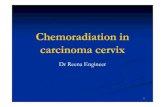
Comparison
ESPAC-1 No CTCONKO 001 BSC ESPAC-1 CT
CONKO 001 GemESPAC-3 5-FUESPAC-3 Gem
Virginia Mason-CRI
CapRI-CRI
CapRI- 5FU
ESPAC1 5-FU
CONKO-1 Gem
ESPAC3 5-FU/Gem
CapRI 5-FU
CapRI CRI
V. Mason CRI
Recruit. 2/94-6/00 7/98-12/04 7/00-1/07 8/04-12/07 8/04-12/07 7/95-12/02
2ys 39% 48% 50% 52% 62% 64%mOS 20 23 23 28 32 44

MonocytesCD40+Dendritic CellsNK cell lysis
IL-12TNF-
CD8:CD4Effector memory T cells
MUC-1 specific T cellsDendritic Cells
Zhu et al., JIT, 2008Hoffmann et al., Antican Res, 2008Märten et al., JIT, 2010
Translational ResearchSignificant specific and unspecific immune responses
Ma et al., WJG, 2005Schmidt et al., CII, 2006Zhu et al., JIT, 2007Schmidt et al., JIT, 2007

Predictive Markers
Patients with a pronounced increase in cytotoxicity after 1st IFN- challenge had a significant longer DFS
arm A
0%
10%
20%
30%
40%
10:1 20:1 40:1 80:1
effector to target ratio
lysi
s of
K56
2 ce
llspre LDI
24hrs after LDI
pre 1st cycle
after 1st day oftherapypre 2nd cycle
--- increase of cytotoxicity after 1st IFN- > 7%--- < 7%
DFS
p = 0.03NK cell mediated cytotoxicity increased within 24hrs after IFN-administration
No change in arm Barm B
0%
10%
20%
30%
40%
10:1 20:1 40:1 80:1
effector to target ratio
lysi
s of
K56
2 ce
lls
pre 1st cyclepre 2nd cyclepre 3rd cycle
No change in arm B

Predictive MarkersDecrease of CD4 cells
(>6.8 percentage points) and decrease of CD4+CD152+ cells
were associated with significant longer OS
--- no decrease --- decrease in CD4+CD152+ cells after 1st IFN-
p = 0.018p = 0.037
--- slight or no decrease in CD4+ cells --- pronounced decrease in CD4+ cells

Summary• The CapRI regimen is toxic• However, toxicity is definitely manageable• Decrease in QoL during cycle 1 but patient recover completely• Primary endpoint not reached; no significant difference in mOS• However, no overlapping curves underpowered trial?• And, best survival data even for classical CT • Trend for better control of R1 resected patients • Association between immune response to IFN- and survival• Confirmatory phase III trial needed

Thanks to
• Our patients
• Manfred Lautenschläger
• The lab team

And to the InvestigatorsSurgery Oncology Radiooncology Biometry/DM
Jan Schmidt Sabine Harig Jürgen Debus Ulrich Mansmann
Markus Büchler Thomas
Herrmann Katja Lindel Ulrich Abel
Detlef Bartsch Dirk JägerRobert
Krempien Karin Hörner Lorenzo
Capussotti Manfred Görner Justus Klein
Carsten Zülke Katrin Hoffmann Peter Hirnle DSMB
Reiner Kunz Florian Lordick Marc MünterMarie von Lilienfeld-
Toal
Paolo Massucco Sabine Kümmel Carsten Ziske
Christin Tjaden Fabio Leone Lutz Edler
… … ….