Descriptive Epidemiology of Multiple Sclerosis (MS) Multiple Sclerosis.
C H A P T E R
893
Handbook of Cannabis and Related Pathologies. http://dx.doi.org/10.1016/B978-0-12-800756-3.00108-3Copyright © 2017 Elsevier Inc. All rights reserved.
93Cannabidiol and Multiple Sclerosis
M. Mecha, A. Feliú, F.J. Carrillo-Salinas, C. GuazaNeurobiology and Functional Systems Department, Cajal Institute, CSIC, Madrid, Spain
SUMMARY POINTS
• Multiplesclerosis(MS)isthemostfrequentchronicneurologicaldiseaseamongyoungandmiddle-agedpeopleinthenorthernindustrializedcountries.
• MSispathologicallycharacterizedbymultifocalinflammation,demyelinationandneuronalinjuryinthecentralnervoussystem(CNS).
• Thefirst-linediseasemodifyingtherapiesforMSpatientsincludeimmunomodulatoryandimmunosuppressivemedications.
• Cannabidiol(CBD),whichconstitutesupto40%ofCannabis sativaextract,mayrepresentapromisingagentforhumantherapeuticuseduetothelackofpsychoactiveactions.
• Uptodate,thereisnoevidenceaboutthefullbindingofCBDtoanyknownreceptorsite,andthemolecularpharmacologyofCBDhasnotbeenwelldefined.
• Experimentalautoimmuneencephalomyelitis(EAE)andTheiler’smurineencephalomyelitisvirus-induceddemyelinatingdisease(TMEV-IDD)aretwoexperimentalmodelsofMSthatincludeclassicalMShallmarkslikeinflammation,neuronaldamage,anddemyelination.
• CBDhasbeenshowntoameliorateEAEandTMEV-IDDmodelsymptomatologybydiminishinginflammation,microglialactivity,andleukocytehoming.
• SativexisusedforthetreatmentofsymptomsofMS,particularlyspasticityandneuropathicpain.
KEY FACTS OF NEUROLOGY• Multiplesclerosisisacomplexheterogeneous
demyelinatingautoimmunediseasethatprimarilyaffectsthemyelininthecentralnervoussystem(CNS).
• CNSdemyelination,thepathologicalprocessinwhichmyelinsheathsarelost,istheconsequenceofadirectinsulttargetedattheoligodendrocyte.
• Axonaldegenerationisacceptedasthemajorcauseofirreversibleneurologicaldisabilityinmultiplesclerosis(MS)patients.
• Autoantigen-specificTh17andTh1,Bcellsandmonocytes/macrophageshavemajorpathologicalroles.
• PharmacologicaltreatmentoptionsapprovedforMSaimatlimitinginflammationanddecreasingrelapserate,but,nocurrenttherapiescancurethedisease.
KEY FACTS OF CNS REPAIR• Remyelinationistheprocessinwhichmyelinsheaths
arerestoredtodemyelinatedaxonsrestoringfunctionaldeficits.
• Remyelinationinvolvesthegenerationofnewmatureoligodendrocytesfromoligodendrocyteprogenitors.
• Akeyfunctionofremyelinationinmultiplesclerosisisaxonsurvival.
• Theefficiencyofremyelinationisaffectedbyage,sex,andgeneticbackgroundregardlessofthediseaseprocess.
• Themostsignificantapproachtoenhanceremyelinationistotargettheendogenousregenerativeprocess.

894 93. Cannabidiol and Multiple SCleroSiS
VII. MEDICINAlCANNABISUSE
LIST OF ABBREVIATIONS
AD AlzheimerdiseaseCBD CannabidiolCNS CentralnervoussystemEAE Experimentalautoimmune
encephalomyelitisEDSS ExpandeddisabilitystatusscaleFAAH FattyacidamidehydrolaseGPCR G-proteincoupledreceptorIFN-β Interferon-betaMCA Middle-cerebral-arteryMHC MajorhistocompatibilitycomplexMRI MagneticresonanceimageMS MultiplesclerosisPPAR PeroxisomeproliferatoractivatedreceptorsPPMS PrimaryprogressivemultiplesclerosisRRMS RemittentrecurrentmultiplesclerosisSPMS SecondaryprogressivemultiplesclerosisTHC TetrahydrocannabinolTMEV-IDD Theiler´smurineencephalomyelitis
virus-induceddemyelinatingdiseaseTPVR-1 Transientpotentialvanilloidreceptor-1
INTRODUCTION
Multiple sclerosis (MS) is the most frequent chronicneurologicaldiseaseamongyoungadultsinthenorthernindustrializedcountries.MSispathologicallycharacter-ized by multifocal inflammation, demyelination, andneuronalinjuryintheopticnerves,brainandspinalcord,
andisconsideredtobeanautoimmunediseasewithacomplex pathophysiology (Compston & Coles, 2002).Thepathologicalhallmarksofthediseaseresultinanaf-fectationofwhitemattertractsandinjurytothecorticalanddeepgraymatter,generatingneurologicsymptomsanddisabilityinpatientswithMS(Table93.1).
MSoccurs ina female–male ratioof3 to1,andhasanestimatedprevalenceofmorethan2.1millionpeopleworldwide (Niedziela, Adamczyk-Sowa, & Pierzcha-la, 2014). It is widelyaccepted that MS cause is multi-factorial,includingmultiplegeneticandenvironmentalriskfactorslikeriskallelesingenesformajorhistocom-patibility complex (MHC), and interleukin-2 and 7 re-ceptorsamongothers(Beechametal.,2013).Moreover,thegeographiclocationofresidencebeforeadolescencemayalsobepredictiveofMSrisk,asithasbeenfound
KEY FACTS ON THE CANNABINOID SYSTEM• Thecannabinoidsystemisaregulatorysystem
identifiedfollowingthestudyofCannabis sativaderivativesinvolvedinthehomeostasiscontrol.
• Theendocannabinoidsignalingsystemiscomposedofcannabinoidreceptors,theirendogenousligandsandtheenzymesthatproduceandinactivatetheseligands.
• Thereare>60cannabinoidcompoundspresentinextractsofC. sativa,and∆9-tetrahydrocannabinol(∆9-THC)isresponsibleforthepsychoactiveeffectsofcannabis,andformanyofthepotentialmedicinaleffects.
• Thenonpsychoactivecannabidiol(CBD)istheothercannabinoidderivedfromC. sativaofcurrentmedicalinterestinMS.
• Sativexisanoromucosalspray,constitutedbyanequimolecularcombinationof∆9-THCandCBD-enrichedbotanicalextractsapprovedforthetreatmentofspasticityandpainassociatedtoMS.
TABLE 93.1 expanded disability Status Scale (edSS) in patients With MS
TheKurtzke’sEDSSscores8functionalsystemsandtheperson’sabilitytowalk.From0.0to4.0,peopleareabletowalkwithoutassistance.From4.0to7.5,peoplecanwalkbutwithassistance.Mainly,point6onthescalerepresentswalkingwithacane,andthispointisoftenusedasanendpointoftheprogressionofdisability.From7.5to10,themaindeterminantofEDSSistheperson’sabilitytotransferfromwheelchairtobedandself-care.AnEDSSof10isnotincludedinthistablebecauseitmeansdeathofthepatientduetoMS.

Cbd pharMaCology and MeChaniSMS of aCtion 895
VII. MEDICINAlCANNABISUSE
increasedratesofthediseaseinnorthernandsouthernlatitudescomparedwithequatorialcountries,probablylinkedtoavitaminDdeficiency(VanderMeietal.,2003).Additionally, the risk to MS may be influenced by theexposuretoparticularinfectiouslikeEpstein–Barrvirus(lassmann,Niedobitek,Aloisi,&Middeldorp,2011)andHerpesvirus6(Tait&Straus,2008).
Thefirst-linediseasemodifying therapies forMSpa-tientsincludeimmunomodulatoryandimmunosuppres-sive medications like interferon-β (IFN-β) or glatirameracetateamongothers(Table93.2),whichhasbeenshowntoreducebothriskofrelapseandnewlesionformationonMRIscans.Paradoxically,antiinflammatorytreatmentmightcontribute to the failureof repair,as results fromstudiesofpatientswithMS indicate that the inflamma-tionblockademighttriggercounter-regulatoryinflamma-torymechanismsusedtohealtheinjuredtissue(Martinoetal.,2002),andsuggestingthattissueintegrityisrestoredby the conversionof the inflammatory response fromadamagingtoarepairingone(Nathan,2002).
Evidencesuggestthatneuroinflammation,demyelin-ation,andneurodegenerationmayoccurinparallel,thecombination of antiinflammatory, oligoprotective andneuroprotectivestrategiesariseasanemergingtherapyforthesymptomaticandtherapeutictreatmentofMS.Inthisline,C. sativaderivativeshaveattractedspecialinterest regardingputative therapeuticproperties,de-spitethefactthatthesecompoundshavealwaysraisedbothethicalandpracticalproblemsfor theirpotentialabuse and unavoidable psychotropic effects. Amongmarijuanacompounds,cannabidiol(CBD),whichcon-stitutesupto40%ofcannabisextract,mayrepresentapromisingagentforhumantherapeuticuseasitlacksanycognitiveandpsychoactiveactions,andhasanex-cellent tolerability profile in humans (Mechoulam &Hanus,2002).
AlargenumberofclinicaltrialshavebeenperformedtoassesstheclinicalefficacyofCBDindifferentpathol-ogies.Mostof themhasbeen focusedonSativexcom-pounds (GW Pharmaceuticals; Salisbury, United King-dom),acommerciallyavailablepreparationcontainingCBDand∆9-THCunderfourdifferentformulationsthatdiffersintheconcentrationofCBDand∆9-THC(tetrahy-drocannabinol).TheoromucosalsprayadministrationofSativexhasbeenagreedin2005forthetreatmentofpainand spasticity in MS (Perras, 2005). In the central ner-voussystem(CNS),CBDhasbeenreportedtoactasanantiinflammatorycompound,thusbeingusefulforneu-roinflammatorydisordersbutalsoasaneuroprotectiveagentbynormalizingglutamatehomeostasis,reducingoxidativestress,andattenuatingglialactivationandtheoccurrence of local inflammatory events (reviewed byFernandez-Ruizetal., 2013).All thesepropertiespointoutCBDasapromisingtherapeuticagentforthetreat-mentofneuroinflammatorydisorderslikeMS.
CBD PHARMACOLOGY AND MECHANISMS OF ACTION
Isolated in across the 1930s and 1940s from C. sativa,the structure and configuration of CBD was fully eluci-dated by Mechoulam et al. in the 1960s (Mechoulam &Shvo,1963;Mechoulam,Shani,Edery,&Grunfeld,1970).ThefirststudyfocusingonCBDpharmacologywaspub-lished in 1981, regarding hypnotic and anticonvulsantproperties(Carlini&Cunha,1981).Alongthistime,sev-eral studieshavebeendone to identify themechanismsthroughwhichCBDexertsitsactions.Uptodate,thereisnoevidenceaboutthefullbindingofCBDtoanyknownreceptorsite.ThemolecularpharmacologyofCBDhasnotbeenwelldefinedyet,andlittleisknownaboutapossibleCBD-receptor-mediated signaling pathway. It is knownthat many of the CBD effects are associated with bothcentralandperipheralactions,andnumerousstudieshasbeenreportedtryingtoelucidatesomeofitsmechanismsofaction(Table93.3),thataredetailedlaterinthechapter.
CBD is a Potent Antioxidant
PioneerworksbyHampson,Grimaldi,Axelrod,andWink(1998)showedthatCBDhasantioxidantpropertiesthathavebeenconfirmedalongseveralpublications.Theplantcannabinoids,beingmonophenols,monophenolicesthers(likeTHC),orresorcinols(likeCBD)arelikewisepotentantioxidants.Hampsonetal.(1998)demonstrat-edthatCBDexertedapotentantioxidantactivitythatre-sultedmoreprotectivethaneitherascorbate(vitaminC)orα-tocopherol(vitaminE)againstglutamate-mediatedneurotoxicity.TheseobservationssuggestthatCBDmaybeapotentialtherapeuticagentforthetreatmentofoxi-dativeneurologicaldisorderslikecerebralischemia,andfordiseasesthatcoursewithoxidativedamage.
CBD Potentiates the Endocannabinoid Signaling System
Intheimmaturedamagedbrain,CBDhasshowndi-rectactivitybindingtotheCB2receptor,andanindirectactivitythroughaninhibitoryeffectonthemechanismsofinactivationofendocannabinoids(transporter,FAAHenzyme)(Bisognoetal.,2001;DeFilippisetal.,2008).Inthisline,theenhancementoftheendocannabinoidtonemaymediatesomeoftheantiinflammatoryandneuro-protectiveeffectsofCBD.
CBD Binds With Low Affinity to Both CB1 and CB2 Cannabinoid Receptors
At concentrations in the micromolar range, CBDshows weak ability to remove 3[H]CP55940, a not se-lective ligand for CB receptors from both CB1 and

VII.M
ED
ICIN
AlC
AN
NA
BISU
SE
TABLE 93.2 Currently available MS treatments
Treatment
Year of FDA approval Type
Route of administration Implications Mechanism of action Side effects
Acute Methylprednisolone(Solu-Medrol)
1959 Glucocorticoid Intravenous(3–5days)
Acuterelapse StabilizingtheBBB,decreasingproinflammatorycytokines,andinducingTcellapoptosis
Disturbanceoftaste,facialflushing,insomnia,psychiatricdisturbance,exacerbationofacne,transienthyperglycemia,andhypertension
ACTH(H.P.Acthar) 1978 Hormone Intramuscularorsubcutaneous(5–15days)
Acuterelapse Stimulatestheadrenalcortexglandtosecretecortisol,corticosterone,andaldosterone
Vomiting,changeinappetite,diarrhea,constipation,restlessness,difficultysleeping,sweating
Plasmaexchange / / Intravenous Acuterelapse Exchangeofimmunoglobulins Hypocalcemia,hypovolemia,andanaphylactoidreactions
Chronic IFNβ-1a(Avonex) 1996 Cytokine(lowdose) Intramuscularinjection
RRMSfirstline
Suppressestheproliferationofmyelin-basicprotein-specificTcells.Reducestheproductionofproinflammatorycytokines,andinducesantiinflammatorycytokines.EffectsontheendothelialcellsoftheBBB
ProductionofNAb(IFNβ1AlessthanIFNβ1B)Influenza-likesymptoms.Headache,injectionsitereaction,asthenia,lymphopenia,depression,hepaticinjury,congestiveheartfailure,anaphylacticshock,andpain
IFNβ-1a(Rebif) 2002 Cytokine(highdose) Subcutaneousinjection
IFNβ-1b(Betaseron) 1993 Cytokine(highdose) Subcutaneousinjection
Glatirameracetate(Copaxone)
1996 Syntheticpolymerofrandomsequencesof4aa(l-tyr,l-glutl-Ala,l-lys)
Subcutaneousinjection
RRMSfirstline
Unknown,possiblebindingtothemajorMHC-IIcompetingwiththeotherMSputativeAg
Injectionsitereactions,tightness,anxiety,dyspnea,palpitation,vasodilation
Mitoxantrone(Novantrone)
2000 Antineoplasticdrug Intravenousinfusion
RRMSSPMS InhibitBcell,Tcell,macrophageproliferation.Impairantigenpresentation,andthesecretionofIFN-γ,TNFα,andIl-2
Cardiotoxicity,myelogenousleukemia,gonadaldysfunction
Natalizumab(Tysabri)
2006 Humanizedanti-VlA-4monoclonalantibody
Intravenousinfusion
RRMSfirstline
Targetstheα4-chainofα4β1integrindecreasingtheaccumulationofactivatedleukocyteswithintheCNS
Headache,fatigue,arthralgia,urinarytractinfection,lowerrespiratoryinfections,gastroenteritis,vaginitis,diarrhea,hypersensitivityreactions,hepatotoxicity,PMl
Dalfampridine(Ampyra)
2010 4-aminopyridine(4-AP)
Oralcapsule Chronicprogressive
Potassiumchannelblocker,potentcalciumactivator
Dizziness,nervousness,nauseaurinarytractinfection
Fingolimod(Gilenya)
2010 Sphingosine-1-phosphate(SIP)receptormodulator
Oralcapsule RRMSsecondline
SIPreceptorantagonistinlymphocytes.Itblockstheabilityoflymphocytestoleavelymphnodes
Headache,infections,bradycardiabradyarrhythmias,macularedema
Teriflunomide(Aubagio)
2012 Drug Oralcapsule RRMS BindstoDHODHproteininhibitingpyrimidinesynthesisinproliferatingcellssuchasTandBlymphocytes(immunomodulatory)
Dyspnea,diarrhea,nausea,alopecia,hepatotoxicity,acuterenalfailure,hypertension,leukopenia
Dimethylfumarate(Tecfidera,BG12)
2013 α,β-unsaturatedester
Oralcapsule RRMSfirstline
ReducetransendothelialmigrationofactivatedleukocytesthroughtheBBB.Neuroprotectiveeffectsviaactivationofantioxidativepathways
Gastrointestinaldisorders,lymphopenia,flushing,pruritus,rash,erythema
AcuteandchronictreatmentsavailableforMSpatients(reviewedinDamal,Stoker,&Foley,2013;Kantarci,Pirko,&Rodriguez,2014).PMl,progressivemultifocalleukoencephalopathy;ACTH,adrenocorticotropichormone;DHODH,dihydroorotatedehydrogenaseBBB,blood–brainbarrier.Intravenousimmunoglobulins(IVIG)andcyclophosphamideforacuterelapsesarenotcoveredinthistable.

Cbd pharMaCology and MeChaniSMS of aCtion 897
VII. MEDICINAlCANNABISUSE
TABLE 93.3 Cbd Molecular Mechanism of actions and effects
Targets Mechanisms Affinity/dose Effect
Receptors and channels
CB1/CB2 Antagonist KB79nM(CB1);138nM(CB2) Antagonizescannabinoidinduceantispas-modiceffect
CB2 Inverseagonist EC50:503nM Antiinflammatoryeffect
GPR55 Antagonist IC50:350nM Antagonisticactivityinhumanosteoclasts
5-HT3Aligand-gatedchannel Allostericinhibition IC50:0.6µM Modulationofnociceptionandemesis
TRPM8cationchannel Antagonist EC50:80–140nM;IC50:60nM Analgesiceffects
TRPA1cationchannel Agonist EC50:110nM;IC50:160nM Analgesiceffects
PPARγnuclearreceptor Agonist IC50:±5µM Vasorelaxationantiinflammatoryeffect
T-typeCa2+channel Inhibitor IC50:±1µM Nociceptiveandantiepilepticeffects,sleepregulation
TRPV1cationchannel Agonist EC50:1µM;IC50:0.6µM Antipsychoticandanalgesiceffects
TRPV2cationchannel Agonist EC50:1.25µM;IC50:4.5µM Antiinflammatory/analgesic/antinocicep-tiveeffect
5-HT1Areceptor Agonist 80%displacementat16µM Antiischemicandanxioliticproperties.Neuroprotective
µandδopioidreceptors Allostericmodulation EC504.38(µ);4.10(δ) Potentiallyenhancetheeffectsofopiates
α1andα1βglycineligand-gatedchannels
Positiveallostericmodulation
EC50:12.3µM(α1);18.1(α1β) Roleinchronicpainafterinflammationornerveinjury
Abnormal-CBDreceptor Antagonist Effectat1µM Attenuatesthevasodilatorresponsetoanandamide
Targets Mechanisms Affinity/dose Effect
Enzymes
CYP1A1 Competitiveinhibitor IC50:0.41µM MightleadtointeractionofdrugsortoxicantsmetabolizedbyCYPenzymes.PossibleadverseeffectsorintoxicationCYP1A2andCYP1B1 Competitiveinhibitor IC50:3.8µM(A2);5.96µM(B1)
CYP2B6 Inhibitor Ki:0.694µM
CYP2D6 Competitiveinhibitor IC50:6.65µM
CYP3A5 Inhibitor IC50:1.65µM
CYP2A6 Inhibitor Ki:55µM
CYP3A4andCYP3A7 Inhibitor IC50:11.7µM(A4)23–31µM(A7)
FAAH Inhibitor IC50:15.2µM IncrementofAEAtone.Analgesic,antiinflammatoryeffects
Mg2+-ATPase Inhibitor Effectat50µM Anticonvulsanteffect
AANAT Inhibitor 65%reductionat10µM Reducesmelatoninbiosynthesis
5-lipoxygenase Inhibitor IC50:73.73µM Antimitoticeffectingliomacells
15-lipoxygenase Inhibitor IC50:2.56µM Involvedinatherosclerosis
PhospholipaseA2 Activator/inhibitor EC50:6.4µM(+)134µM(−) Antiinflammatoryeffects
Indoleamine-2,3-dioxygenase Inhibitor IC50:2.8µM/ml Enhanceoftryptophanandthereforeserotonin.Improvementofmooddisturbances
(Continued)

898 93. Cannabidiol and Multiple SCleroSiS
VII. MEDICINAlCANNABISUSE
CB2 receptor sites (Thomas, Gilliam, Burch, Roche, &Seltzman,1998).
CBD Antagonizes CB1 and CB2 Receptor Agonists, and Can Act as an Inverse Agonist of CB2 Receptor
CBDattenuatestheeffectsofWIN55212andCP55940(CB1agonists)atprejunctionalsitesinmousevasdefer-ens(Pertwee,Ross,Craib,&Thomas,2002).Moreover,at concentration values in low nanomolar range, CBDcouldworkasaninverseagonistofCB2receptor,as ithasbeendemonstratedinwhole-brainmembranesandmembranes from CHO cells transfected with humanCB2 receptors (Thomas et al., 2007). This mechanismmayexplainsomeofthepharmacologicaleffectsofCBDsuchasitsantiinflammatoryproperties.
CBD Enhances Adenosine Signaling
CBD binds to the equilibrative nucleoside-trans-porter-1 with a Ki value below 250 nM, which in turnled to the increase of extracellular adenosine (Carrier,Auchampach,&Hillard,2006).NeuroprotectiveeffectsofCBDinhypoxic–ischemicbraindamagealsoinvolve
adenosineA2receptors(Castillo,Tolon,Fernandez-Ruiz,Romero,&Martinez-Orgado,2010).Moreover,CBDdi-minishesinflammationinacutemodelsofinjury(Ribeiroetal.,2012)andinaviralmodelofMSthroughadenos-ineA2receptors(Mechaetal.,2013b).
CBD Interacts With the Transient Potential Vanilloid Receptor Type-1 (TPVR-1), and With 5-HT1A Serotonin Receptor
BothCBDandits(+)enantiomerinteract(EC50esti-matedbetween3.2and3.5µM)withTPVR-1 receptor,withamaximaleffectthatissimilartothenaturalago-nist capsaicin. These effects have been confirmed bothin vitro (Bisogno et al., 2001) and in a model of acuteinflammationinrats(Costa,Giagnoni,Franke,Trovato,&Colleoni,2004).
In relation to 5HT1A serotonin receptors, Russo,Burnett,Hall,andParker(2005)demonstratedthatCBDdisplacestheagonist([3H]-8-OH-DPAT)fromthehumanclonedreceptor inaconcentration/dependentmanner,and that it increases [35S]GTPgSbinding in thisG-pro-tein-coupledreceptor(GPCR)systemdecreasingcAMPconcentrationatsimilarapparentlevelsofreceptoroccu-pancy.Inaddition,CBDsignificantlyreducestheinfarct
Targets Mechanisms Affinity/dose Effect
Glutathioneperoxidase Activator Effectat10and25µM ROSproductionandcaspaseactivationintumorcells
Glutathionreductase Activator
Superoxidedismutase Inhibitor Effectat100µM GeneratesROSandinducescelltoxicityintumorcells
Catalase Inhibitor
NAD(P)H-quinonereductase Inhibitor
Progesterone17α-hydrolase Inhibitor Effectat1M Interactionwithsteroidmetabolism.InhibitsthetestosteronesynthesisinrattestisTestosterone6β-hydrolase Inhibitor
Testosterone16α-hydrolase Inhibitor
Targets Mechanisms Affinity/dose Effect
Transporters and cellular uptake
Adenosineuptake Competitiveinhibitor IC50:120nM Incrementofadenosinetoneantiinflammatoryeffect
IntracellularCa2+uptake Inhibition Effectat1µM Neuroprotectiveandantiepilepticproperties
Anandamidereuptake Inhibitor IC50:28µM IncrementofAEAtone
Cholineuptake Inhibitor EC50:1.6pM IncrementofAchtone
P-glycoprotein(drugeffluxtransporter)
Inhibitor IC50:39.6µM PotentiallyinfluencetheabsorptionanddispositionofcompoundsthatareP-gpsubstrates
MoleculartargetsofCBD,includingcannabinoidandnoncannabinoidreceptors,enzymes,transporters,andcellularuptakeproteins(reviewedinIzzo,Borrelli,Capasso,DiMarzo,&Mechoulam,2009;Mechoulam,Petersa,Murillo-Rodriguez,&Hanus,2007;Hill,Williams,Whalley,&Stephens,2012).CYP,CytochromeP450enzymes;AANAT,arylalkylamineN-acetyltransferase;FAAH,fattyacidamidehydrolase;AEA,N-arachidonoylethanolamide;Ach,acetylcholine;ROS,reactiveoxygenspecies.
TABLE 93.3 Cbd Molecular Mechanism of actions and effects (cont.)

Cbd and aniMal ModelS of MS 899
VII. MEDICINAlCANNABISUSE
volume induced by middle-cerebral-artery (MCA) oc-clusion(Mishimaetal.,2005),exertinganeuroprotectiveeffectthatwasinhibitedbytheserotonin5-HT1Arecep-tor antagonist WAY100135, but not by capsazepine, avanilloid-receptorantagonist.
CBD Allosterically Modulates µ and δ Opioid Receptors
Data from Kathmann, Flau, Redmer, Tränkle, andSchlicker(2006)showthat,onratcerebralcortexmem-brane homogenates, CBD accelerated the dissociationof both the µ opioid receptor agonist [3H]DAMGO in-duced by naloxone, and the δ opioid receptor agonist[3H] naltrindole induced by naltrindole. Interestingly,this property was shared by THC, but not by the CB1cannabinoid-receptor antagonist rimonabant. As thismodulationofopioidreceptorsoccursatveryhighlev-elsofCBD,itcannotbeexpectedtocontributemarkedlytothephytocannabinoidactionsinvivo.
CBD Affects Nuclear Receptors of the Peroxisome Proliferator-Activated Receptors (PPAR-g), and Antagonizes the Orphan Receptor GPR55
Recently, it has been discovered the ability of dif-ferent endocannabinoids and phytocannabiniods, in-cluding CBD, to display an extra-cannabinoid recep-torbindingactivitybytheinteractionwithperoxisomeproliferator-activated receptors (PPARs) (O’Sullivan &Kendall, 2010). PPARs belong to the family of nuclearhormone receptors, and have been reported to controlthe expression of genes related to inflammatory re-sponses. Esposito et al. (2011) reported that the block-adeofPPARγinaratmodelofAlzheimerdisease(AD),bluntedCBDeffectsonreactivegliosisandsubsequentlyonβ-amyloid-inducedneurotoxicity.Moreover,andduetotheinteractionofCBDwithPPARγ,thiscannabinoidwasobservedtostimulatehippocampalneurogenesis.
Additionally, CBD displays GPR55 antagonistic ac-tivityinhumanosteoclasts(Whyteetal.,2009),andhasnoGPR55agonisticactivitywhenassayedinβ-arrestinrecruitment and calcium mobilization assays (Yinetal.,2009;Kapuretal.,2009),demonstratingthatCBDcanactasanantagonistoftheorphanreceptorGPR55.
CBD TOXICITY AND PHARMACOKINETIC
InviewofthepotentialtherapeuticuseofCBD,andencouragedbythelackofitsundesiredpsychotropicef-fects,severalstudieshavebeenperformedtodeterminethetoxicologicalprofileofthisphytocannabinoid.
VerylowtoxicityofCBDhasbeenfoundbothinhu-manandinotherspecies,withanlD50of212mg/kgwhen intravenously injected into rhesus monkey(Rosenkrantz, Fleischman, & Grant, 1981). The oraltoxicity of CBD had not been clearly established, butRosenkrantz et al. (1981) showed that an oral dose of20–50 times larger than the intravenous route of CBDis required to initiate severe intoxication.Additionally,CBDdoesnotcauserelevantCNSalterations,anddoesnotdisplaymutagenicorteratogenicactivities(Dalterio,Steger,Mayfield,&Bartke,1984;Matsuyama&Fu,1981).
In regards of the pharmacokinetic of CBD, reviewedbyGrotenhermen(2003),onceorallygivenandduetoamarked first-pass effect, CBD bioavailability ranges be-tweenvaluesof13%and19%,whilethesystemicbioavail-abilityofinhaledCBDhasarangeof11–45%makingforthisreasontheintravenouslyadministrationrouteprefer-able.WithplasmapatternsimilartothatofTHC,afteritsadministrationCBDisrapidlydistributed,andduetoitslipophilicnaturecaneasilypass theblood–brainbarrier.ThebiotransformationroutesforCBDarethosetypicallyobserved forphytocannabinoids,withmultiplehydroxi-lations,oxidationstocarboxylicacids,β-oxidation,conju-gationandepoxidation(Harvey&Mechoulam,1990;Sa-mara,Bialer,&Harvey,1990a).ThisturnsintoaprolongedeliminationofCBD,withaterminalhalf-lifeofabout9h,being preferentially excreted in the urine as free and itsglucuronidecompound(Samara,Bialer,&Harvey,1990b).
CBD AND ANIMAL MODELS OF MS
TheuseofanimalmodelstostudyacomplexdiseaselikeMShasallowednotonlytoabetterunderstandingaboutthepathophysiologyofthehumandisease,butalsotothedevelopment of preclinical testing of disease therapies.TherearetwomainanimalmodelstostudyMS:experi-mentalautoimmuneencephalomyelitis(EAE),inducedbyimmunizationagainstmyelin,andexperimentalviralin-fectionliketheoneinducedwithTheiler’smurineenceph-alomyelitisvirus(TMEV)insusceptiblemice(reviewedinMecha, Carrillo-Salinas, Mestre, Feliu, & Guaza, 2013a).Both animal models include classical MS hallmarks likeinflammation,neuronaldamageanddemyelination,andithasbeendescribedtheabilityofcannabinoidstoexhibittherapeuticpotentialusingthesetwomodels.
TheenhancedleukocytetraffickingisakeyfeatureinMS,andthereareavailabletherapiesdesignedtotargetCNSinflammationinitsearlyevents,suchasnatalizum-ab(Tysabri),whichinterfereswiththehomingofimmunecellstotheCNSandiscurrentlyprescribedforthetreat-ment of relapsing remitting MS (Krumbholz, Derfuss,Hohlfeld,&Meinl,2012).Inthisline,thetreatmentwithcannabinoidagonistshasbeenshowntobeeffective intheleukocyterollingandadhesiontoendothelialcellsin
900 93. Cannabidiol and Multiple SCleroSiS
VII. MEDICINAlCANNABISUSE
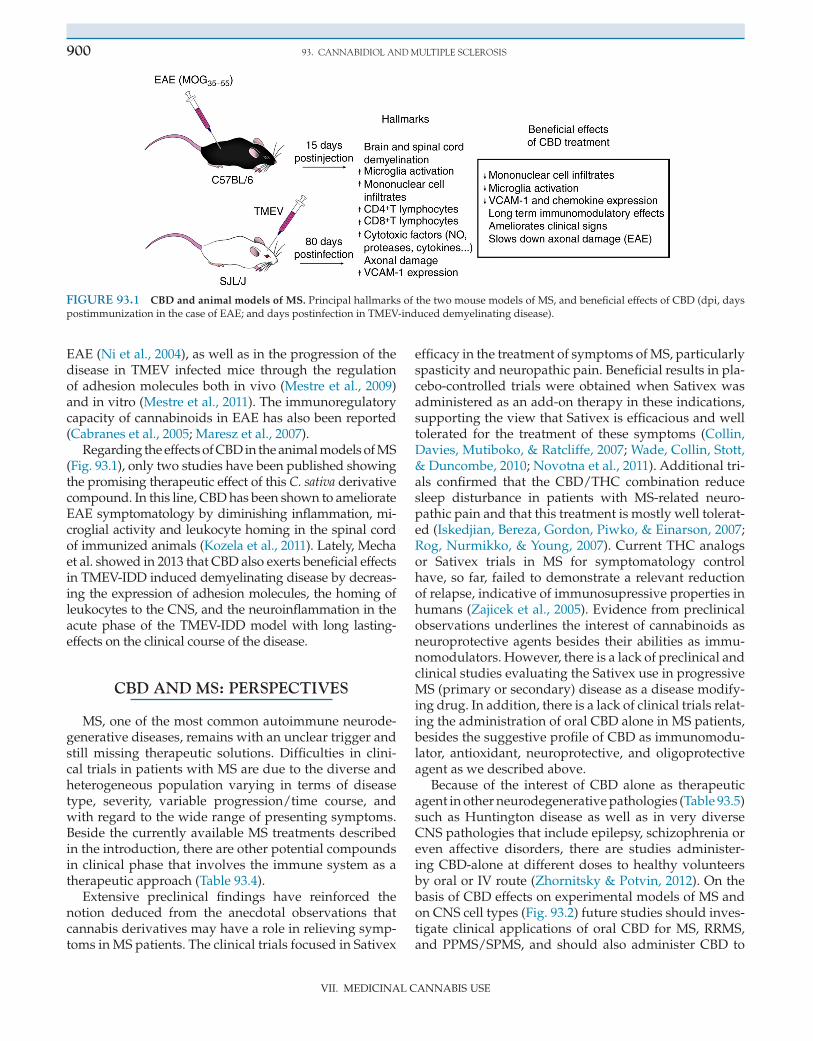
EAE(Nietal.,2004),aswellasintheprogressionofthedisease in TMEV infected mice through the regulationofadhesionmoleculesbothinvivo(Mestreetal.,2009)andinvitro(Mestreetal.,2011).TheimmunoregulatorycapacityofcannabinoidsinEAEhasalsobeenreported(Cabranesetal.,2005;Mareszetal.,2007).
RegardingtheeffectsofCBDintheanimalmodelsofMS(Fig.93.1),onlytwostudieshavebeenpublishedshowingthepromisingtherapeuticeffectofthisC. sativaderivativecompound.Inthisline,CBDhasbeenshowntoameliorateEAEsymptomatologybydiminishinginflammation,mi-croglialactivityandleukocytehominginthespinalcordofimmunizedanimals(Kozelaetal.,2011).lately,Mechaetal.showedin2013thatCBDalsoexertsbeneficialeffectsinTMEV-IDDinduceddemyelinatingdiseasebydecreas-ingtheexpressionofadhesionmolecules,thehomingofleukocytestotheCNS,andtheneuroinflammationintheacute phase of the TMEV-IDD model with long lasting-effectsontheclinicalcourseofthedisease.
CBD AND MS: PERSPECTIVES
MS,oneofthemostcommonautoimmuneneurode-generativediseases,remainswithanuncleartriggerandstill missing therapeutic solutions. Difficulties in clini-caltrialsinpatientswithMSareduetothediverseandheterogeneous population varying in terms of diseasetype, severity, variable progression/time course, andwithregardtothewiderangeofpresentingsymptoms.BesidethecurrentlyavailableMStreatmentsdescribedintheintroduction,thereareotherpotentialcompoundsinclinicalphasethat involvestheimmunesystemasatherapeuticapproach(Table93.4).
Extensive preclinical findings have reinforced thenotion deduced from the anecdotal observations thatcannabisderivativesmayhavearoleinrelievingsymp-tomsinMSpatients.TheclinicaltrialsfocusedinSativex
efficacyinthetreatmentofsymptomsofMS,particularlyspasticityandneuropathicpain.Beneficialresultsinpla-cebo-controlled trialswereobtainedwhenSativexwasadministeredasanadd-ontherapyintheseindications,supportingtheviewthatSativexisefficaciousandwelltolerated for the treatment of these symptoms (Collin,Davies,Mutiboko,&Ratcliffe,2007;Wade,Collin,Stott,&Duncombe,2010;Novotnaetal.,2011).Additionaltri-als confirmed that the CBD/THC combination reducesleep disturbance in patients with MS-related neuro-pathicpainandthatthistreatmentismostlywelltolerat-ed(Iskedjian,Bereza,Gordon,Piwko,&Einarson,2007;Rog,Nurmikko,&Young,2007).CurrentTHCanalogsor Sativex trials in MS for symptomatology controlhave,sofar, failedtodemonstratearelevantreductionofrelapse,indicativeofimmunosupressivepropertiesinhumans(Zajiceketal.,2005).Evidencefrompreclinicalobservationsunderlinestheinterestofcannabinoidsasneuroprotectiveagentsbesides theirabilitiesas immu-nomodulators.However,thereisalackofpreclinicalandclinicalstudiesevaluatingtheSativexuseinprogressiveMS(primaryorsecondary)diseaseasadiseasemodify-ingdrug.Inaddition,thereisalackofclinicaltrialsrelat-ingtheadministrationoforalCBDaloneinMSpatients,besidesthesuggestiveprofileofCBDasimmunomodu-lator, antioxidant, neuroprotective, and oligoprotectiveagentaswedescribedabove.
Because of the interest of CBD alone as therapeuticagentinotherneurodegenerativepathologies(Table93.5)such as Huntington disease as well as in very diverseCNSpathologiesthatincludeepilepsy,schizophreniaoreven affective disorders, there are studies administer-ingCBD-aloneatdifferentdoses tohealthyvolunteersbyoralorIVroute(Zhornitsky&Potvin,2012).OnthebasisofCBDeffectsonexperimentalmodelsofMSandonCNScelltypes(Fig.93.2)futurestudiesshouldinves-tigate clinical applications of oral CBD for MS, RRMS,and PPMS/SPMS, and should also administer CBD to
FIGURE 93.1 CBD and animal models of MS.PrincipalhallmarksofthetwomousemodelsofMS,andbeneficialeffectsofCBD(dpi,dayspostimmunizationinthecaseofEAE;anddayspostinfectioninTMEV-induceddemyelinatingdisease).

Cbd and MS: perSpeCtiveS 901
VII. MEDICINAlCANNABISUSE
patientsforprolongedperiodoftimeinordertosimu-latethechronicconditionofthisdisease.AmongC. sa-tivaderivedcompounds,CBDwhichlacksanyunwant-edpsychotropiceffectmayrepresentapromisingagentwith the highest prospect for therapeutic use but thishypothesisneedstobeproved.
TABLE 93.4 MS therapy pipeline
Name TypeRoute of administration Pending indications Phase Mechanism of action
laquinimod Derivativeoflinomide Oral RRMS III Inducesantiinflammatorycytokineprofileinhumans.InhibitsTh1andTh2leukocytemigrationintodeCNS.
Rituximab(Zituxam)
Chimerichuman/mouseanti-CD20monoclonalantibody
Intravenous RRMS(approvedbyFDAforlymphomaandarthritisrheumatoid)
III DepletesCD20+Blymphocytesviacell-mediatedandcomplement-dependentcytotoxiceffects,andpromotesapoptosisofthesecellsintheperipheralcirculation
Daclizumab(Zenapax)
Humanizedanti-CD25monoclonalantibody
Subcutaneous RRMS III TargetstheαsubunitofIl2RCD25onactivatedTlymphocytes.BlockingtheCD25downregulatestheproliferationofBandTlymphocytesviareductionthesecretionofproinflammatorycytokines.ProductionofCD56positivenaturalkillercellswithregulatoryfunction
Alemtuzumab(Campath-1H)
Humanizedanti-CD52monoclonalantibody
Intravenous RRMS(approvedbyFDAforleukemia;betterthanRebif)
III TargetsthemoleculeCD52,expressedonthesurfaceofmaturelymphocytes,monocytes,andmacrophages.Itdepletesthesecellsviacomplement-mediatedlysisantibody-dependentcelltoxicityandapoptosis.InducestheproductionofneurotrophicfactorsbythereconstitutedautoreactiveTlymphocytes
Ocrelizumab Humanizedanti-CD20monoclonalantibody
Intravenous RRMS II DepletesCD20+Blymphocytes
PerspectivesfornewtreatmentsforMSpatients,includingthephaseoftheclinicaltrialandtheexpectedmechanismofaction(reviewedinMinagar,2013).
TABLE 93.5 potential beneficial effects of Cbd in humans
Ischemia
Huntingtondisease
Parkinsondisease
Multiplesclerosis
Alzheimerdisease
Priondiseases
PsychiatricdisordersObsessivecompulsivebehaviorDepressionSchizophreniaAnxietyPsychosis
Epilepsy
Cancer
Diabetes
Rheumatoidarthritis
Amyotrophiclateralsclerosis
DifferentdiseasesinwhichthetreatmentwithCBDcanbetherapeuticbasedontheeffectsonmousemodels(reviewedinFernandez-Ruizetal.,2013andPertwee,2012).
FIGURE 93.2 Cellular targets of CBD.Neurons,oligodendrocytes,microglialandendothelialcellscanbetargetsoftheeffectsofCBDintheCNS.Theactionsonastrocytecellshavenotyetbeendetermined.

902 93. Cannabidiol and Multiple SCleroSiS
VII. MEDICINAlCANNABISUSE
MINI-DICTIONARY
Autoimmune disease Anabnormalimmuneresponseofthebodytotissuesandmoleculesnormallypresentinthebody.ItcompromisestheproductionofautoantibodiesfromtheB-cellsoftheimmunesystem.Thetreatmentofautoimmunityincludesimmunosuppresion,todecreasetheimmune“self”response.Cannabidiol Oneofatleast60activecannabinoidsidentifiedinCannabis sativa,countingforupto40%oftheplant’sextract,consideredtohaveawiderscopeofmedicalapplicationsthanTHCwithnopsychoactiveeffects.Demyelination Damagetothemyelinsheaththatcoversnervefibersinbrainandspinalcord.Thisprovokesthatnerveimpulsessloworevenstop,causingneurologicalalterations.EAE model AnanimalmodelofCNSautoimmuneinflammationthatcourseswithinflammationanddemyelination,andisusedasanexperimentalmodelforthehumaninflammatorydemyelinatingdiseaseMS.Mainlyinducedbyinoculationwithspinalcordhomogenatesormyelinproteinsorpeptides,thatresultsindistinctmodelsofdiseasecoursedependingofthegeneticbackgroundofmice.Endocannabinoid system lipidsystemofintercellularcommunicationconstitutedbyendogenousligands,receptors,andthemachineryofsynthesisanddegradationenzymes.It´sinvolvedinavarietyofphysiologicalprocessesincludingmemory,mood,pain-sensation,andappetite.CannabinoidsextractedfromC. sativausethisendogenoussystemtoexerttheircentralandperipheralactions.Multiple Sclerosis Chronicneurologicaldiseasethatispathologicallycharacterizedbymultifocalinflammation,demyelination,andneuronalinjuryinopticnerves,brain,andspinalcord.Mainlyconsideredasanautoimmunedisease.Neurodegeneration Aconditionthatresultinprogressivelossofneuronalstructureandfunctionwithneuronaldeath.SomeneurodegenerativedisordersincludeParkinson,Alzheimer,andHuntingtondisease.Neuroinflammation Inflammationofthecentralorperipheralnervoussystem.Itcanbeinitiatedinresponsetoinfection,autoimmunity,traumaticbraininjuryortoxicmetabolitesamongothers.Neuroinflammationcompromisesmicroglialcells,theresidentinnateimmunecellsoftheCNS,andcirculatingperipheralimmunecellsthatinfiltratethroughthebloodbrainbarrier.Oligodendrocyte MyelinatingcelloftheCNS.Myelinactsasaninsulatorofaxonalsegmentsandisaprerequisiteforthehighvelocityofnerveconduction.Sativex CannabinoidmedicineforthetreatmentofspasticityduetoMSwhichisalsoindevelopmentforcancerpainandneuropathicpain.CommercializedbyGWPharmaceuticals,thepreparationcontainingCBDand∆9-THCisavailableunderfourdifferentformulationsthatdifferintheconcentrationofCBDand∆9-THC.TMEV-IDD model Ananimalmodelofprimarychronic-progressivediseasethatcourseswithinflammation,demyelination,andneurodegenerationinbothbrainandspinalcord,usedasanexperimentalmodelforthehumandiseaseMS.InducedbytheintracerebralinoculationofdifferentstrainsoftheTheiler’svirusinsusceptiblemice.
ReferencesBeecham, A. H., Patsopoulos, N. A., Xifara, D. K., Davis, M. F.,
Kemppinen, A., Cotsapas, C., International Multiple SclerosisGeneticsConsortium(IMSGC),etal.(2013).Analysisofimmune-related loci identifies 48 new susceptibility variants for multiplesclerosis.Nature Genetics,45,1353–1360.
Bisogno,T.,Hanus,l.,DePetrocellis,l.,Tchilibon,S.,Ponde,D.E.,Brandi,I.,Moriello,A.S.,Davis,J.B.,Mechoulam,R.,&DiMarzo,V. (2001).Moleculartargetsforcannabidiolanditssyntheticana-logues:effectonvanilloidVR1receptorsandonthecellularuptakeandenzymatichydrolysisofanandamide.British Journal of Pharma-cology,134,845–852.
Cabranes,A.,Venderova,K.,delago,E.,Fezza,F.,Sanchez,A.,Mestre,l.,Valenti,M.,Garcia-Merino,A.,Ramos,J.A.,DiMarzo,V.,&Fer-nandez-Ruiz,A. (2005). Decreased endocannabinoid levels in thebrainandbeneficialeffectsofagentsactivatingcannabinoidand/orvanilloidreceptorsinaratmodelofmultiplesclerosis.Neurobiology of Disease,20,207–217.
Carlini,E.A.,&Cunha,J.M.(1981).Hypnoticandantiepilepticeffectsofcannabidiol.Journal of Clinical Pharmacology,21,417S–427S.
Carrier,E.J.,Auchampach,J.A.,&Hillard,C.J.(2006).Inhibitionofanequilibrativenucleosidetransporterbycannabidiol:amechanismofcannabidiolimmunosuppresion.Proceedings of the National Acad-emy of Sciences of the United States of America,103,7895–7900.
Castillo,A.,Tolon,M.R.,Fernandez-Ruiz,J.,Romero,J.,&Martinez-Orgado,J.(2010).Theneuroprotectiveeffectofcannabidiolinaninvitromodelofnewbornhypoxic-ischemicbraindamageinmiceismediatedbyCB(2)andadenosinreceptors.Neurobiology of Disease,37,434–440.
Collin,C.,Davies,P.,Mutiboko,I.K.,&Ratcliffe,S.SativexSpasticityinMSStudyGroup.(2007).Randomizedcontrolledtrialofcanna-bis-basedmedicineinspasticitycausedbymultiplesclerosis.Euro-pean Journal of Neurology,14,290–296.
Compston,A.,&Coles,A.(2002).Multiplesclerosis.Lancet,359,1221–1231.Costa,B.,Giagnoni,G.,Franke,C.,Trovato,A.E.,&Colleoni,M.(2004).
Vanilloid TRPV1 receptor mediates the antihyperalgesic effect ofthe nonpsychoactive cannabinoid, cannabidiol, in a rat model ofacuteinflammation.British Journal of Pharmacology,143,247–250.
Dalterio,S.,Steger,R.,Mayfield,D.,&Bartke,A.(1984).Earlycanna-binoidexposureinfluencesneuroendocrineandreproductivefunc-tionsinmalemice:I.Prenatalexposure.Pharmacology Biochemistry and Behavior,20,107–113.
Damal,K.,Stoker,E.,&Foley,J.F.(2013).Optimizingtherapeuticsinthe management of patients with multiple sclerosis: a review ofdrugefficacy,dosing,andmechanismsofaction.Biologics: Targets and Therapy,7,247–258.
DeFilippis,D.,Iuvone,T.,d’Amico,A.,Esposito,G.,Steardo,l.,Her-man,A.G.,Pelckmans,P.A.,deWinter,B.Y.,&deMan,J.G.(2008).Effect of cannabidiol on sepsis-induced motility disturbances inmice:involvementofCBreceptorsandfattyacidamidehydrolase.Neurogastroenterology and Motility,20,919–927.
Esposito, G., Scuderi, C., Valenza, M., Togna, G. I., latina, V., DeFilippis,D.,Cipriano,M.,Carratu,M.R.,Iuvone,T.,&Steardo,l.(2011). Cannabidiol reduces Ab-induced neuroinflammation andpromoteshippocampalneurogenesisthroughPPARginvolvement.PLoS One,6(12),e28668.
Fernandez-Ruiz,J.,Sagredo,O.,Pazos,M.R.,Garcia,C.,Pertwee,R.,Mechoulam, R., & Martinez-Orgado, J. (2013). Cannabidiol forneurodegenerative disorders: important new clinical applicationsforthisphytocannabinoid?British Journal of Clinical Pharmacology,75(2),323–333.
Grotenhermen,F.(2003).Pharmacokineticsandpharmacodynamicsofcannabinoids.Clinical Pharmacokinetics,42,327–360.
Hampson,A.J.,Grimaldi,M.,Axelrod,J.,&Wink,D.(1998).Cananbi-dioland(−)Delta9-tetrahydrocannabinolareneuroprotectiveanti-oxidants.Proceedings of the National Academy of Sciences of the United States of America,95(14),8268–8273.
Harvey,D.J.,&Mechoulam,R.(1990).Metabolitesofcannabidioliden-tifiedinhumanurine.Xenobiotica,20,303–320.
Hill,A.J.,Williams,C.M.,Whalley,B.J.,&Stephens,G.J.(2012).Phy-tocannabinoidsasnoveltherapeuticagentsinCNSdisorders.Phar-macology and Therapeutics,133(1),79–97.

VII. MEDICINAlCANNABISUSE
referenCeS 903
Iskedjian, M., Bereza, B., Gordon, A., Piwko, C., & Einarson, T. R.(2007).Meta-analysisofCannabis-basedtreatmentsforneuropathicand multiple sclerosis-related pain. Current Medical Research and Opinion,23(1),17–24.
Izzo,A.A.,Borrelli, F.,Capasso,R.,DiMarzo,V.,&Mechoulam,R.(2009).Non-psychotropicplantcannabinoids:newtherapeuticop-portunitiesfromanancientherb.Trends in Pharmacological Sciences,30(10),515–527.
Kantarci,O.H.,Pirko,I.,&Rodriguez,M.(2014).Novelimmunomod-ulatoryapproachesforthemanagementofmultiplesclerosis.Clini-cal Pharmacology and Therapeutics,95(1),32–44.
Kapur,A., Zhao, P., Sharir, H., Bai,Y., Caron, M. G., Barak, l. S., &Abood,M.E.(2009).Atypicalresponsivenessoftheorphanrecep-tor GPR55 to cannabinoid ligands. Journal of Biological Chemistry,284,29817–19827.
Kathmann,M.,Flau,K.,Redmer,A.,Tränkle,C.,&Schlicker,E.(2006).Cannabidiol is an allosteric modulator at mu- and delta-opioidreceptors. Naunyn Schmiedebergs Archives of Pharmacology, 372(5),354–361.
Kozela,E.,lev,N.,Kaushanski,N.,Eilam,R.,Rimmerman,N.,levy,R.,Ben-Nun,A.,Juknat,A.,&Vogel,Z.(2011).Cannabidiolinhib-its pathogenic T cells, decreases spinal microglial activation andamelioratesmultiplesclerosis-likediseaseinC57Bl/6mice.British Journal of Pharmacology,163(7),1507–1519.
Krumbholz,M.,Derfuss,T.,Hohlfeld,R.,&Meinl,E.(2012).Bcellsandantibodies inmultiple sclerosispathogenesis and therapy. Nature Reviews Neurology,8(11),613–623.
lassmann,H.,Niedobitek,G.,Aloisi,F.,&Middeldorp,&The,J.M.NeuroproMISEEBVWorkingGroup.(2011).Epstein–Barrvirusinthemultiplesclerosisbrain:acontroversialissue.Brain,134(Pt9),2772–2286.
Maresz,K.,Pryce,G.,Ponomarev,E.D.,Marsicano,G.,Croxford,J.l.,Shriver,l.P.,etal.(2007).DirectsuppressionofCNSautoimmuneinflammation via the cannabinoid receptor CB1 on neurons andCB2onautoreactiveTcells.Nature Medicine,13,492–497.
Martino,G.,Adorini,l.,Rieckmann,P.,Hillert,J.,Kallmann,B.,Comi,G., & Filippi, M. (2002). Inflammation in multiple sclerosis: thegood,thebad,andthecomplex.Lancet Neurology,1,499–509.
Matsuyama,S.S.,&Fu,T.K.(1981).Invivocytogeneticeffectsofcan-nabinoids.Journal of Clinical Psychopharmacology,1,135–140.
Mecha, M., Carrillo-Salinas, F. J., Mestre, l., Feliu, A., & Guaza, C.(2013a).Viralmodelsofmultiplesclerosis:neurodegenerationanddemyelination in mice infected with Theiler’s virus. Progress in Neurobiology,101,46–64.
Mecha,M.,Feliu,A.,Iñigo,P.M.,Mestre,l.,Carrillo-Salinas,F.J.,&Guaza, C. (2013b). Cannabidiol provides long-lasting protectionagainstthedeleteriouseffectsofinflammationinaviralmodelofmultiplesclerosis:aroleforA2Areceptors.Neurobiology of Disease,59,141–150.
Mechoulam,R.,&Hanus,l.(2002).Cannabidiol:anoverviewofsomechemical and pharmacological aspects. Part I: chemical aspects.Chemistry and Physics of Lipids,121(1–2),35–43.
Mechoulam, R., Petersa, M., Murillo-Rodriguez, E., & Hanus, l. O.(2007). Cannabidiol – recent advances. Chemistry and Biodiversity,4(8),1678–1692.
Mechoulam,R.,Shani,A.,Edery,H.,&Grunfeld,Y.(1970).Chemicalbasisofhashishactivity.Science,169,611–612.
Mechoulam,R.,&Shvo,Y.(1963).Hashish.I.Thestructureofcannabi-diol.Tetrahedron,19,2073–2078.
Mestre, l., Docagne, F., Correa, F., loria, F., Hernangomez, M., Bor-rell, J.,&Guaza,C. (2009).Acannabinoidagonist interfereswiththeprogressionofachronicmodelofmultiplesclerosisbydown-regulatingadhesionmolecules.Molecular and Cellular Neuroscience,40(2),258–266.
Mestre, l., Iñigo, P. M., Mecha, M., Correa, F. G., Hernangomez-Herrero,M.,loria,F.,Docagne,F.,Borrell, J.,&Guaza,C. (2011).
Anandamide inhibits Theiler’s virus induced VCAM-1 in brainendothelialcellsandreducesleukocytetransmigrationinamodelof blood brain barrier by activation of CB(1) receptors. Journal of Neuroinflammation,8,102.
Minagar,A.(2013).Currentandfuturetherapiesformultiplesclerosis.Scientifica,2013,249101.
Mishima,K.,Hayakawa,K.,Abe,K.,Ikeda,T.,Egashira,N.,Iwasaki,K.,&Fujiwara,M.(2005).Cannabidiolpreventscerebralinfarctionvia a serotonergic 5-hydroxytryptamine1A receptor-dependentmechanism.Stroke,36(5),1077–1082.
Nathan,C.(2002).Pointsofcontrolininflammation.Nature,420,846–852.
Ni,X.,Geller,E.B.,Eppihimer,M.J.,Eisenstein,T.K.,Adler,M.W.,&Tuma,R.F.(2004).Win55212-2,acannabinoidreceptoragonist,at-tenuatesleukocyte/endothelialinteractionsinanexperimentalau-toimmuneencephalomyelitismodel.Multiple Sclerosis,10,158–164.
Niedziela,N.,Adamczyk-Sowa,M.,&Pierzchala,K.(2014).Epidemi-ologyandclinicalrecordofmultiplesclerosisinselectedcountries:a systematic review. International Journal of Neuroscience, 124(5),322–330.
Novotna, A., Mares, J., Ratcliffe, S., Novakova, I., Vachova, M.,Zapletalova, O., Gasperini, C., Pozzilli, C., Cefaro, l., Comi, G.,Rossi,P.,Ambler,Z.,Stelmasiak,Z.,Erdmann,A.,Montalban,X.,Klimek,A.,&Davies,P.SativexSpasticityStudyGroup.(2011).Arandomized double blind, placebo controlled, parallel-group, en-riched-design study of Nabiximols (Sativex®) as an add therapyinsubjectswithrefractoryspasticitycausedbymultiplesclerosis.European Journal of Neurology,18,1122–1131.
O’Sullivan,S.E.,&Kendall,D.A. (2010).Cannabinoidactivationofperoxisomeproliferator/activatedreceptors:potentialformodula-tionofinflammatorydisease.Immunobiology,215,611–616.
Perras, C. (2005). Sativex for the management of multiple sclerosissymptoms.Issues in Emerging Health Technologies,72,1–4.
Pertwee,R.G.(2012).Targetingtheendocannabinoidsystemwithcan-nabinoidreceptoragonists:pharmacologicalstrategiesandthera-peuticpossibilities.Philosophical Transactions of the Royal Society B,367(1607),3353–3363.
Pertwee,R.G.,Ross,R.A.,Craib,S.J.,&Thomas,A.(2002).(−)-canna-bidiol antagonizes cannabinoid receptor agonists and noradrena-line in the mouse vas deferens. European Journal of Pharmacology,456,99–106.
Ribeiro,A.,Ferraz-de-Paula,V.,Pinheiro,M.l.,Vitoretti,l.B.,Mari-ano-Souza,D.P.,Quinteiro-Filho,W.M.,Akamine,A.T.,Almeida,V.I.,Quevedo,J.,Dal-Pizzol,F.,Hallak,J.E.,Zuardi,A.W.,Crippa,J.A.,&Palermo-Neto, J. (2012).Cannabidiol, anon-psychotropicplant-derived cannabinoid, decreases inflammation in a murinemodelofacutelunginjury:rolefortheadenosineA(2A)receptor.European Journal of Pharmacology,678,78–85.
Rog,D.J.,Nurmikko,T.J.,&Young,C.A.(2007).Oromucosaldelta9-tetrahydrocannabinol/cannabidiolforneuropathicpainassociatedwithmultiplesclerosis:anuncontrolled,open-label,2-yearexten-siontrial.Clinical Therapeutics,29,2068–2079.
Rosenkrantz,H.,Fleischman,R.W.,&Grant,R. J. (1981).Toxicityofshort-termadministrationofcannabinoidstorhesusmonkeys.Tox-icology and Applied Pharmacology,58,118–131.
Russo,E.B.,Burnett,A.,Hall,B.,&Parker,K.K.(2005).Agonisticprop-ertiesof cannabidiolat5-HT1Areceptors.Neurochemical Research,8,1037–1043.
Samara, E., Bialer, M., & Harvey, D. J. (1990a). Pharmacokinetics ofurinarymetabolitesofcannabidiolinthedog.Biopharmaceutics and Drug Dispositions,11,785–795.
Samara,E.,Bialer,M.,&Harvey,D.J.(1990b).Identificationofglucoseconjugatesasmajorurinarymetabolitesofcannabidiolinthedog.Xenobiotica,20,177–183.
Tait,A.R.,&Straus,S.K.(2008).PhosphorylationofU24fromHumanHerpesVirus type6 (HHV-6)and itspotential role inmimicking

904 93. Cannabidiol and Multiple SCleroSiS
VII. MEDICINAlCANNABISUSE
myelin basic protein (MBP) in multiple sclerosis. FEBS Letters,582(18),2685–2688.
Thomas,A.,Baillie,G.l.,Phillips,A.M.,Razdan,R.K.,Ross,R.A.,&Pertwee,R.G. (2007).CannabidioldisplaysunexpectedlyhighpotencyasanantagonistofCB1andCB2receptoragonistsinvitro.British Journal of Pharmacology,150,613–623.
Thomas,B.F.,Gilliam,A.F.,Burch,D.F.,Roche,M.J.,&Seltzman,H.H. (1998).Comparativereceptorbindinganalysesofcannabinoidagonistsandantagonists.Journal of Pharmacology and Experimental Therapeutics,285,285–292.
VanderMei,I.A.,Ponsonby,A.l.,Dwyer,T.,Blizzard,l.,Simmons,R.,Taylor,B.V.,Butzkueven,H.,&Kilpatrick,T.(2003).Pastexpo-sure to sun, skin phenotype, and risk of multiple sclerosis: case-controlstudy.British Medical Journal,327(7410),316.
Wade,D.T.,Collin,C.,Stott,C.,&Duncombe,P.(2010).Meta-analysisoftheefficacyofSativex(Nabiximols),onspasticityonpeoplewithmultiplesclerosis.Multiple Sclerosis Journal,16,707–714.
Whyte,l.S.,Ryberg,E.,Sims,N.A.,Ridge,S.A.,Mackie,K.,Greasley,P.J.,Ross,R.A.,&Rogers,M.J.(2009).TheputativecannabinoidreceptorGPR55affectsosteoclastfunctioninvitroandbonemassinvivo.Proceedings of the National Academy of Sciences of the United States of America,106,16511–16516.
Yin,H.,Chu,A.,li,W.,Wang,B.,Shelton,F.,Otero,F.,Nguyen,D.G.,Caldwell,J.S.,&Chen,Y.A.(2009).lipidGprotein-coupledrecep-torligandidentificationusingβ-arrestinPathHunterassay.Journal of Biological Chemistry,284,12328–12338.
Zajicek, J. P., Sanders, H. P., Wright, D. E., Vickery, P. J., Ingram, W.M.,Reilly,S.M.,Nunn,A.J.,Teare,l.J.,Fox,P.J.,&Thompson,A.J.(2005).Cannabinoidsinmultiplesclerosis(CAMS)study:safetyandefficacydatafor12monthsfollowup.Journal of Neurology, Neu-rosurgery and Psychiatry,76,1664–1669.
Zhornitsky,S.,&Potvin,S.(2012).Cannabidiolinhumans:thequestfortherapeutictargets.Pharmaceuticals (Basel),5(5),529–552.