Cancer pain พระนั่งเกล้า
48
แนวทางเวชปฏิบัติ การดูแลรักษาผู ้ป่ วยปวดจากมะเร็ง พญ.ฉันทนา หมอกเจริญพงศ์ กลุ ่มงานเวชศาสตร์ประคับประคอง สถาบันมะเร็งแห่งชาติ กรมการแพทย์ กระทรวงสาธารณสุข
-
Upload
pain-clinic-pnk -
Category
Health & Medicine
-
view
78 -
download
0
Transcript of Cancer pain พระนั่งเกล้า

แนวทางเวชปฏบตการดแลรกษาผปวยปวดจากมะเรง
พญ.ฉนทนา หมอกเจรญพงศ
กลมงานเวชศาสตรประคบประคอง
สถาบนมะเรงแหงชาต
กรมการแพทย กระทรวงสาธารณสข

ความปวด ***** PAIN
An unpleasant sensory and
emotional experience associated with
actual or potential tissue damage, or described in terms of such damage
ประสบการณทไมสบายกาย ไมสบายใจ ทเกดจากการบาดเจบของเนอเยอหรอศกยภาพทจะท าใหมการบาดเจบของเนอเยอ หรอประหนงวามการบาดเจบ

Facts about cancer pain
Frequency of occurrence varies with ;
• stage of the disease• primary site of the tumor
Frequency of occurrence varies with ;
• stage of the disease• primary site of the tumor
Moderate or severe pain occurs in 30 - 40%
of the patients at the time of diagnosis and 60 - 100% with advanced cancer
Moderate or severe pain occurs in 30 - 40%
of the patients at the time of diagnosis and 60 - 100% with advanced cancer
Most cancer patients have more than one painMost cancer patients have more than one pain

ความปวดทพบในผปวยมะเรงเกดจากหลายสาเหต

Causes of Pain
1. Due to tumor involvement 78%
• bone, nerve, soft tissue, viscera
2. Associated with treatment 19%
• diagnosis and staging procedures
• surgery
• chemotherapy; mucositis, phlebitis,
tissue necrosis, myalgia, arthralagia
• radiotherapy; mucositis, neuropathy,
myelopathy

3. Due to general illness but not cancer (10%)
• constipation
• pressure
• gastric distention
• reflux esophagitis
• bladder spasm (with catheterization)
• musculoskeletal pain
• thrombosis and embolism
• mucositis
• post herpetic neuralgia
4. Unrelated to cancer or its treatment(10%)
Causes of Pain
ความปวดจากมะเรงมผลเสยทางดานความเปนอย จตใจ อารมณ สงคม ของผปวยและผใกลชด

Assessment: Review of the systems
1. Systemic/constitutional– anorexia เบออาหาร– weight loss น าหนกลด– cachectic ผอมหนงหมกระดก– fatigue/weakness ความลา / ออนแรง– insomnia นอนไมหลบ
2. Neurologic– sedation งวงซม– confusion มนงง สบสน– hallucination ประสาทหลอน– headache ปวดศรษะ– motor weakness กลามเนอออนแรง– altered sensation การรบความรสกเปลยนแปลง– incontinence กลนไมอย
Assessment: Review of the systems
3. Respiratory– dyspnea, cough, hiccough
4. Gastrointestinal– dysphagia - dehydration
– nausea/vomiting - constipation/diarrhea
5. Psychological– irritability - depression
– anxiety - dementia
6. Integument– decubitus
– dry, sore mouth

Physical
well-beingPsychological
well-being
Social
well-beingSpiritual
well-being
Quality of life for cancer patients in pain

Pain
Total suffering
Psychological problems
Physical symptoms
Spiritual concerns
Cultural factors
Social difficulties

การประเมนความปวด

Pain Assessment
• Location of all the pain
• How the pain feels
• Intensity of the pain
• When, frequency, duration
• What ease the pain, what worsen
the pain
• Medications taking
• Side effects of pain medications
• Quality of life issues
• Pain diary!

Pain Assessment
• Chronicity: Acute vs Chronic pain
• Pain intensity
• Pathophysiology:
somatic vs. visceral
nociceptive vs. neuropathic
• Course of the disease: continuous,
breakthrough, incident pain.
• Pain syndrome: brain metastasis,
bone pain

ChronicityChronicity
Acute pain Chronic pain
Onset well-defined ill-defined
Cause acute injury or illness
chronic progress
Duration days/weeks
predictable
months/years
unpredictable
Physiological
sympathetic over activity
no sympathetic over activity
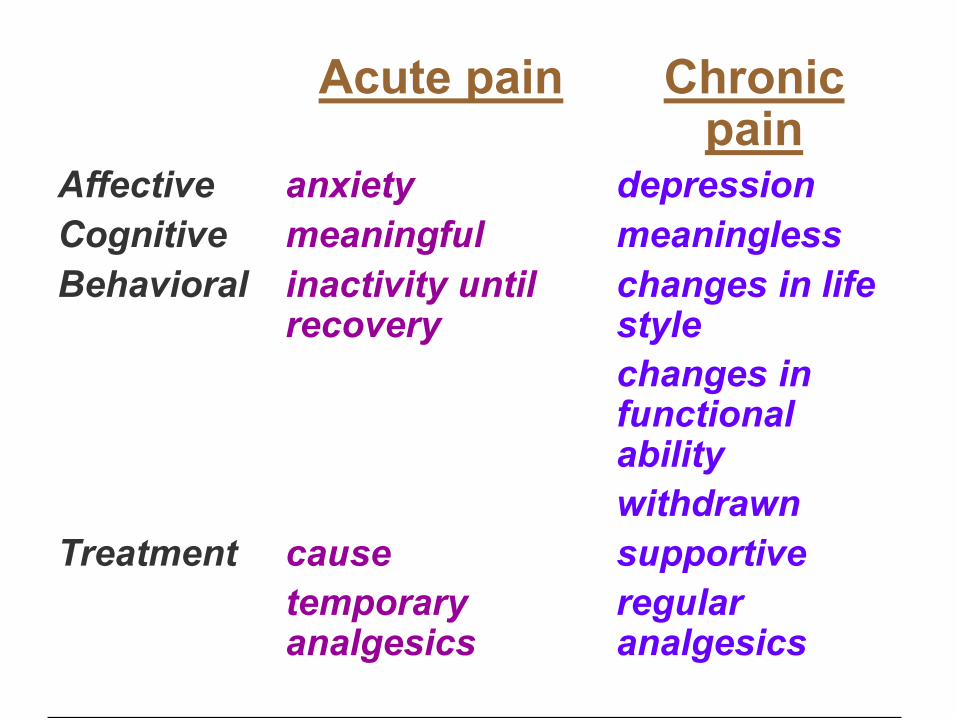
Acute pain Chronic pain
Affective anxiety depression
Cognitive meaningful meaningless
Behavioral inactivity until recovery
changes in life style
changes in functional ability
withdrawn
Treatment cause
temporary analgesics
supportive
regular analgesics

Categoral scales
• Verbal rating scale (VRS)
(verbal descriptor scale)
• 2 – 7 words
None Mild Moderate Severe
• Pain relief
None Slight Moderate Good Complete
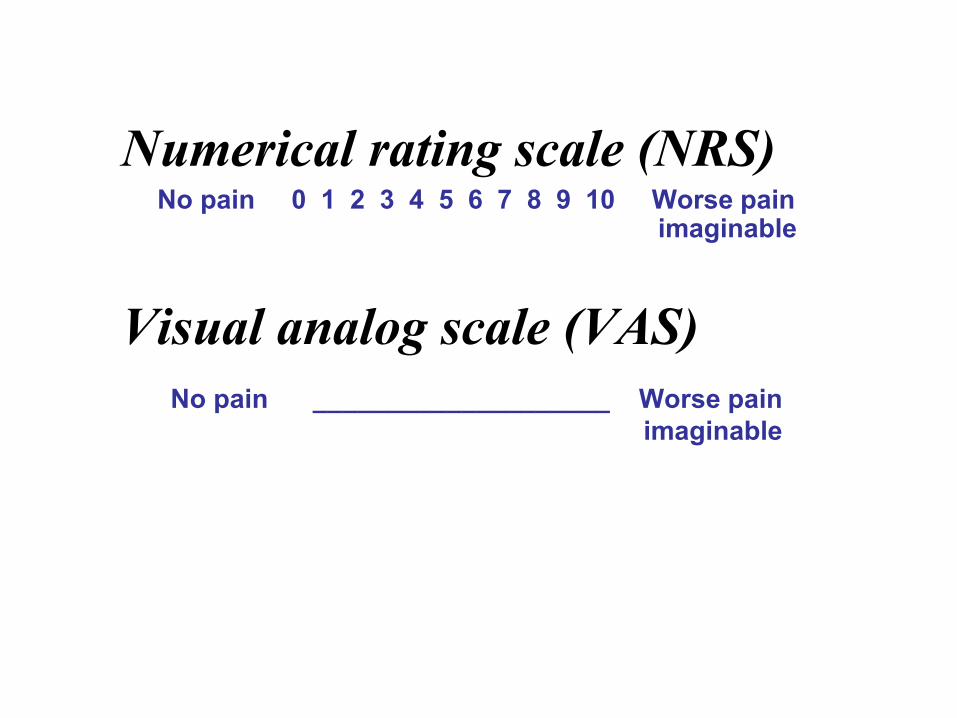
Numerical rating scale (NRS)No pain 0 1 2 3 4 5 6 7 8 9 10 Worse pain
imaginable
Visual analog scale (VAS)
No pain ____________________ Worse pain
imaginable

Happy/sad faces.

Pain Assessment
• Chronicity: Acute vs Chronic pain
• Pain intensity
• Pathophysiology:
somatic vs. visceral
nociceptive vs. neuropathic
• Course of the disease: continuous,
breakthrough, incident pain.
• Pain syndrome: brain metastasis,
bone pain
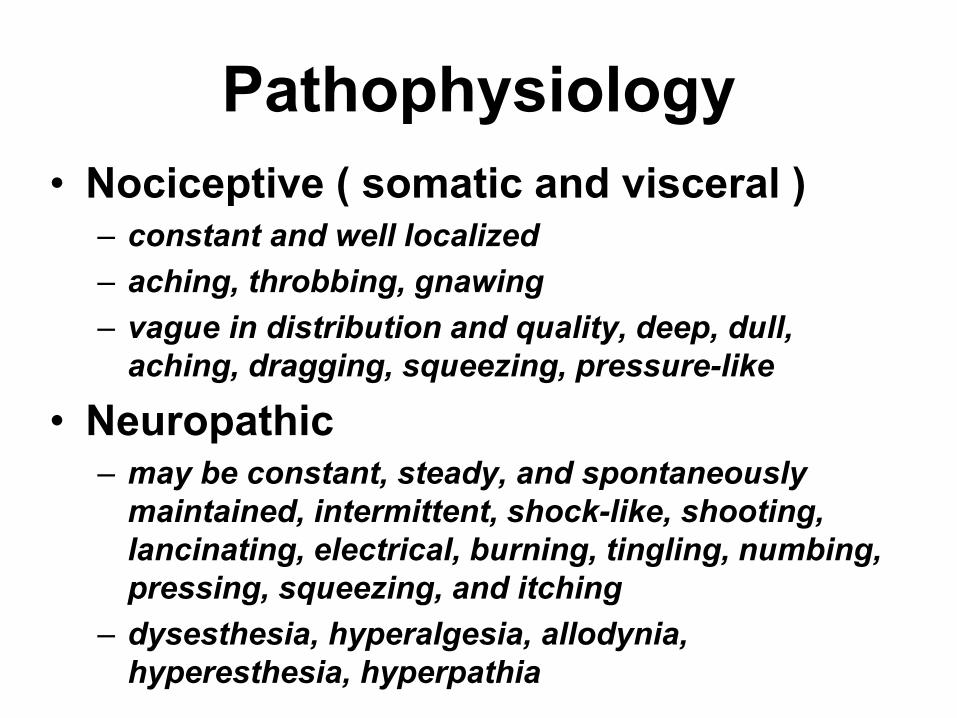
Pathophysiology
• Nociceptive ( somatic and visceral )– constant and well localized
– aching, throbbing, gnawing
– vague in distribution and quality, deep, dull,
aching, dragging, squeezing, pressure-like
• Neuropathic– may be constant, steady, and spontaneously
maintained, intermittent, shock-like, shooting,
lancinating, electrical, burning, tingling, numbing,
pressing, squeezing, and itching
– dysesthesia, hyperalgesia, allodynia,
hyperesthesia, hyperpathia

Neuropathic Pain
• Hardest mechanism to treat
• Diagnose straightforward: nerve or
dermatome distribution, no local tenderness
but referred
• Two types
– Mixed: nociceptive/neuropathic due to tumor
invasion or compression of nerve pathway;
brachial, lumbosacral plexus, chest wall invasion,
spinal cord compression
– Pure (Deafferentation): no nociceptive element;
PHN, post-thoracotomy syndrome, phantom pain


Bone Pain
• Most common cause of pain in advanced
cancer
• Most common malignancies metastasize to
bone: breast, prostate, lung, kidney, thyroid
• Common problems: chronic bone pain,
pathologic fracture, hypercalcemia
• Treatment includes: NSAIDs, opioids,
radiotherapy, Strontium-89, bisphosphonate,
corticosteroids, calcitonin.
• Early Orthopedic consultation and treatment
is important
Pattern of pain
Constant pain
Breakthrough and
incident pain
Intermittent pain
หลกการระงบปวดในผปวยมะเรง

Principle of Analgesic Use
• Define the nature of pain
• Maximize the current regimen
• Understand the drug Pharmacology
– Speed of onset and duration of action
– Management of side effects
– Beware of the drug interactions
• Emphasize patient education

Cancer Pain Management
• Pharmacologic
treatment
• Non-
Pharmacologic treatment

WHO Analgesic Ladder (1992--)
Non-opioid+ Adjuvants
Opioid for mild to moderate pain
+ Non-opioid + Adjuvants
Opioid for Moderate to severe pain
+ Non-opioid + Adjuvants
Pain
Pain persist
Pain persist
Freedom from
cancer pain
Morphine เปนยาแกปวดรนแรงทดทสดในปจจบน
ใชกนไดสะดวกบรหารไดหลายวธ
Essential concepts in the WHO approach to drug therapy
• By the mouth
• By the clock
• By the ladder
• For the individual
• With attention to detail

Principles of analgesic used
• Administer on strict schedule to
prevent pain, not PRN
• Give instructions for treatment of
breakthrough pain
• Following analgesic ladder
• Review & assess
GENERAL RECOMMENDATIONS
• Oral medications should be used as the first line approach.
• Any proposed systemic regimen must be individualized.
• There is no predetermined maximum dose of an opioid.
• Dose titration may be required periodically.

Adverse drug effects from opioid therapy
• Tolerance
• Physical dependence
• Addiction
• Constipation
• Sedation
• Nausea-vomiting
• Mental clouding
• Myoclonus, pruritus, urinary retention
• respiratory depression

Nausea
• Moderate to severe 8.3 – 18.3%
• Direct effect of opioids on CTZ
• Decrease quality of life, limit food
intake
• Other underlying conditions; electrolyte imbalance, dehydration, brain metastasis, intestinal obstruction, ileus, chemotherapy, tumor of the GI, constipation, infection, blood poisoning, kidney problems, anxiety, etc.

Nausea
• Usually subside within few days
• Treatment; – Metoclopramide ( block in GI tract and CTZ)
– Butyrophenones (haloperidol, droperidol) (at CTZ)
– Phenothiazine (CTZ, GI, vestibular)
– Antihistamine (dramamine,hydroxyzine) (H1 blockade and VC)
– Hyoscine, scopolamine (VC and GI)
– Ondansetron (5HT3 in GI and CTZ)– Benzodiazepine (lorazepam) GABA agonist

Constipation
• The most troublesome, almost
everyone is involved, will not develop
tolerance

Treatment of Constipation
• Stimulant laxatives• Senokot 1 tab hs – 4 tab tid orally
• Dulcolax 1 tab hs – 3 tab tid orally
• Bulk-forming laxatives• Metamucil 1 tsp in 8 oz water OD – tid
• Bran
• Saline or osmotic cathartics• MOM 15 – 40 ml OD – bid
• Magnesium citrate solution 240 ml OD
CNS effects
• Aggravating factors;
– High doses opioid
– Psychoactive drugs
– Renal failure
• Slow down of cognitive function, sedation,
hallucination and delirium, fluctuation of
consciousness, change in sleep-wake cycle,
agitation, myoclonus.
• Improve spontaneously

CNS effects
• Role of M-3-G
• Management;
– Opioid rotation
– Dose reduction
– Circadian modulation
– Hydration
– Psychostimulants
– Other drugs; haloperidol, midazolam, baclofen, clonazepam,clonidine

Adjuvants
• Antidepressants : tricyclic antidepressant (amitriptyline), SSRI (Fluoxitine)
• Anticonvulsants : Carbamazepine (tegretol), Hydantion (dilantin), Gabapentin (Neurontin)
• Sedatives, hypnotics, tranquilizers
• Steriod
• Muscle relaxants
ADJUVANTS
DRUGS
- Anticonvulsants
- Antidepressants
- Local anesthetics
- Corticosteroids
- Antihistaminics
- Muscle relaxants
- Psychostimulants
- Drug action on bone
INDICATIONS
- neuropathic pain
- neuropathic pain
- neuropathic pain
- multiple
- coanalgesic, antiemetic
- muscle spasm
- opioid sedation
- bone pain

Antidepressants
• Used in neuropathic pain ; several studies in
Diabetic neuropathy, Post-herpetic neuralgia,
phantom limb pain, migraine headache
• Reduce insomnia and anxiety
• 1-2 weeks lag time for clinical effects
• Start 10-20 mg hs
• Escalated 4-5 day intervals to doses 100- 150
mg
• Abrupt escalation not recommended

TCA Uses Limited by Side Effects
• Anticholinergic : dry mouth, visual
changes, constipation, tachycardia, urinary
retention, reduced gastric motility, worsen
narrow angle glaucoma
• Antihistamine : sedation
• Alpha adrenergic blockade :orthoststic hypotension
• Sodium channel blockade :prolonged QT and QRS

สรปแนวทางการระงบปวดผปวยโรคมะเรง
• มะเรงเปนโรคทมผลรายตอชวต มะเรงระยะทายท าใหผปวยจ านวนมากมความปวด
• ความปวดทพบในผปวยมะเรงมหลายสาเหต รกษาตามความเหมาะสมของแตละสาเหต
• การประเมนความปวดมทงทางกายและทางใจ
• ปรมาณความปวดดไดจาก VAS ฯ

สรปแนวทางการระงบปวดผปวยโรคมะเรง
• การระงบปวดใชยาเปนหลก
• ใหยาระงบปวดตามความรนแรง ตามเวลาอยางตอเนอง เสรมเมอตองการเพม และประเมนผลการรกษาบอยๆ
• ยงมการระงบปวดโดยไมใชยาอกหลายวธ
• ดแลคณภาพชวตของผปวย

Thank you