CANCER OF THE RECTUM - Postgraduate Medical Journalquadrant of the rectum or the whole...
22
17 CANCER OF THE RECTUM Bv RONALD W. RAVEN. O.B.E.. F.R.C.S. Surgeon to the Royal Cancer Hospital (Free), Assistant Surgeon to the Gordon Hospital for Diseases of Rectum and Colon, Surgeon to Out-Patients, the French Hospital General Features of the Disease Cancer of the rectum is seen frequently in this country and it is one of the commonest forms of malignant disease, accounting for a total number of more than 6,ooo deaths during the year i942. The number of deaths occurring during 1942 as a result of cancer in the common sites is shown in Table i. TABLE I CANCER AND OTHER MALIGNANT TUMOURS. DEATHS FROM CERTAIN SITES. (REGISTRAR-GENERAL'S STATISTICAL REVIEW OF ENGLAND AND WALES, 1I942) NUMBER OF DEATHS SITE OF DISEASE Male Female Digestive organs and peri- toneum 1.. .. .. I9,43 17,055 Oesophagus .. .. .. I,584 68i Stomach and duodenum .. 7,151 5,586 Intestines other than duo- denum and rectum .. 4,432 5,453 Rectum .. . . 3,698 2,442 Liver and Biliary passages .. I,249 1,625 Pancreas .. .. .. 1,146 I,056 Breast.. .. .. .. 6o 7,203 Uterus - . .. .. 4,575 Specified as cancer of cervix 1,884 Other or unspecified cancer of uterus .. .. 2,69I Respiratory System .. .. 5,596 1,525 Prostate .. .. 2,388 Urinary organs . . .. 1,623 907 The figures in Table i show that males are affected more frequently than females, there being 3,698 deaths in males and 2,442 in females. The age incidence is shown in Table 2. TABLE II CANCER OF RECTUM. AGE INCIDENCE. (REGISTRAR-GENERAL S STATISTICAL REVIEW OF ENGLAND AND WALES, 1I942) SEX AGES AT DEATH Males Females 20- 5 7 25 14 8 30- I9 29 35- 47 45 40- 68 8o 45 92 114 50- 185 i 82 55 346 256 6o 56I 317 65- 8o6 414 70- 788 412 75- 500 336 8o 200 159 85- 67 83 The disease is more frequently seen in females under the age of 40 vears than in males. Cuthbert Dukes' has called attention to the correlation which exists between the extent of lymphatic metastases and the age of the patient, and by analysis it was shown that in patients under the age of 40 years lymphatic metastases were found in 7I.8 ± 4.3 per cent., and in the age-group 40 to 59 years they were present in 50.9 ± 2.4 per cent. This observa- tion is in line with the general rule that cancer is often more virulent in the young than the old. Pathological Considerations The initial lesion. Carcinoma of the rectum commences in one of two ways, namely, as a copyright. on July 27, 2021 by guest. Protected by http://pmj.bmj.com/ Postgrad Med J: first published as 10.1136/pgmj.23.255.17 on 1 January 1947. Downloaded from
Transcript of CANCER OF THE RECTUM - Postgraduate Medical Journalquadrant of the rectum or the whole...

17
CANCER OF THE RECTUMBv RONALD W. RAVEN. O.B.E.. F.R.C.S.
Surgeon to the Royal Cancer Hospital (Free), Assistant Surgeon to the Gordon Hospital forDiseases of Rectum and Colon, Surgeon to Out-Patients, the French Hospital
General Features of the DiseaseCancer of the rectum is seen frequently in
this country and it is one of the commonestforms of malignant disease, accounting for atotal number of more than 6,ooo deaths duringthe year i942. The number of deaths occurringduring 1942 as a result of cancer in the commonsites is shown in Table i.
TABLE I
CANCER AND OTHER MALIGNANTTUMOURS. DEATHS FROM CERTAIN
SITES.
(REGISTRAR-GENERAL'S STATISTICAL REVIEW OFENGLAND AND WALES, 1I942)
NUMBER OF DEATHSSITE OF DISEASE
Male Female
Digestive organs and peri-toneum 1.. .. .. I9,43 17,055
Oesophagus .. .. .. I,584 68i
Stomach and duodenum .. 7,151 5,586
Intestines other than duo-denum and rectum .. 4,432 5,453
Rectum .. . . 3,698 2,442
Liver and Biliary passages .. I,249 1,625
Pancreas .. .. .. 1,146 I,056
Breast.. .. .. .. 6o 7,203
Uterus - . .. .. 4,575
Specified as cancer of cervix 1,884
Other or unspecified cancer ofuterus .. .. 2,69I
Respiratory System .. .. 5,596 1,525
Prostate .. .. 2,388
Urinary organs . . .. 1,623 907
The figures in Table i show that males areaffected more frequently than females, therebeing 3,698 deaths in males and 2,442 infemales.The age incidence is shown in Table 2.
TABLE IICANCER OF RECTUM. AGE INCIDENCE.
(REGISTRAR-GENERAL S STATISTICAL REVIEW OFENGLAND AND WALES, 1I942)
SEXAGES AT DEATH
Males Females
20- 5 725 14 830- I9 2935- 47 4540- 68 8o45 92 11450- 185 i8255 346 2566o 56I 31765- 8o6 41470- 788 41275- 500 3368o 200 15985- 67 83
The disease is more frequently seen infemales under the age of 40 vears than inmales. Cuthbert Dukes' has called attentionto the correlation which exists between theextent of lymphatic metastases and the age ofthe patient, and by analysis it was shown thatin patients under the age of 40 years lymphaticmetastases were found in 7I.8 ± 4.3 per cent.,and in the age-group 40 to 59 years they werepresent in 50.9 ± 2.4 per cent. This observa-tion is in line with the general rule that canceris often more virulent in the young than theold.
Pathological ConsiderationsThe initial lesion. Carcinoma of the rectum
commences in one of two ways, namely, as a
copyright. on July 27, 2021 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.23.255.17 on 1 January 1947. Dow
nloaded from

POST-GRADUATEI MEDICAL JOURNAL
nodular thickening in the mucous membrane,or as a malignant degenerative process in apre-existing lesion such as an adenoma or avillous papilloma. In the first type, as thelesion increases in size it becomes a raisedswelling which becomes ulcerated at a laterstage. It is now a recognized fact that anadenoma or papilloma of the rectum must beregarded as a precancerous lesion and dealtwith accordingly.The author? has reported the case record of
a patient with a very early carcinoma of therectum for which a perineal excision of therectum was performed following exploratorylaparotomy and left inguinal colostomy. Thespecimen shows a small carcinomatous ulcerI in. in diameter with a proliferating edge.Microscopical examination of vertical sectionspassing through the centre of the small tumourshow portions of a columnar celled adeno-carcinoma invading the submucous layer. Asmall group of the tumour cells suriounded bysmall round cells, evidently representing thebase of a crypt in which the epithelium hasundergone malignant change, is seen alsowithin the upper limit of the circular musclelayer. Two lymph nodes were present andshowed no sign of carcinomatous invasion.
Multiple lesions. The occurrence of mul-tiple carcinomata of the rectum, or of therectum and colon, is of more than academicinterest owing to its frequency. Thus Dukes"in a series of i,ooo cases of carcinoma of therectum reported the presence of more than onefocus of carcinoma in 29 cases (2.9 per cent.);four of these were associated with familialpolyposis intestini and in the remainder onlytwo carcinomata were found in each specimen,these were separated by at least an inch ormore of normal bowel. It was found that thetwo growths were usually similar in size andshape and of equal duration, but in others oneof the neoplasms was at an 'earlier stage ofdevelopment. Gabriel3 considers that the in-cidence of simultaneous double rectal car-cinoma is probably more than 5 per cent., andin a--series of ioo one stage excisions of therectum by the perineoabdominal route no lessthan eight double carcinomata of the rectumitself or of the rectum and pelvic colon werefound. The subject has been reviewed byNorbury4 who called attention to certain
important matters as follows. Multiple polypiare commonly associated with carcinoma of thelarge bowel and one or more may undergomalignant transformation producing multiplecarcinomata. A study of the literature showedthat in the' majority of cases of multiplemalignant growths of the large bowel, thelesions are situated usually in the rectum orpelvirectal region. Norbury stresses thepractical implications of the incidence ofmultiple neoplasms. Thus sigmoidoscopyshould be carried out to exclude adenomatosisor the presence of a second neoplasm in therectum or lower part of the pelvic colon. Whenan operation is planned for excision of therectum, or resection of the colon for malignantdisease, the possibility that multiple neoplasmsmay be present must be considered, and headvocates the routine examination of thewhole of the colon in such cases through anadequate abdominal incision.
Relation with familial polyposis intestini.This condition is characterized by the piesencein the rectum and colon of multiple adenomata,either sessile or pedunculated, and of varioussizes. Often the larger neoplasms are in thedistal colon and they may project into therectum. It is recognized that this disease hasa familial incidence and it may occur in severalgenerations. A very important aspect is therelationship which exists between this con-dition and carcinoma. Malignant changesmay occur in one or more of these neoplasmsand a number of cases have been reported inthe literature of multiple carcinomata of thebowel in association with polyposis and theage of such patients may be younger than thenormal age at which carcinoma of the rectumocours.
Types of growthThere are several types of carcinoma of the
rectum which can be distinguished on macro-scopic examination. These are described asfollows:-
Ulcerative type. In this variety of neoplasmthe main feature is ulceration, round or ovalin shape. The depth of the ulcer varies, itmay penetrate through the entire thickness ofthe wall of the rectum and involve the peri-rectal tissves and adjacent structures. Themargins of the ulcer are raised, nodular and of
.7anuary, 1947
copyright. on July 27, 2021 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.23.255.17 on 1 January 1947. Dow
nloaded from

CANCER OF THE RECTUM
irregular outline; the central zone of thelesion being excavated and depressed.
Polypoidal type. This variety presents as alarge tumour mass which projects into thelumen of the rectum, the surface being some-what smooth or markedly irregular. Thetumour may be pedunculated, semipeduncu-lated or sessile, and various degrees of dis-tension of the lumen of the bowel are seenabove the neoplasm. It may spring from onequadrant of the rectum or the whole circum-ference may be involved in the malignantprocess. The surface of the tumour may beulcerated of varying degrees.
Stenotic type. In this variety of neoplasm ahard ring like carcinoma is formed which en-circles the wall of the rectum transversely andcauses a marked degree of stenosis withdilatation of the bowel above the stricture.There is marked fibrosis in the wall of therectum involved in the neoplastic process andthe growth may show a very moderate degreeof surface ulcel ation.
Complex type. In certain cases there is acomplex tumour mass composed of seveialtypes. One portion of the neoplasm is of thepolypoid type forming multiple pedunculatedpapillomata which project into the lumen of thebowel. In another part the features of theulcerative type may be seen, with raised,nodular margins which are sometimes under-mined. In addition the lumen of the bowelmay be occluded to varying degrees, the bowelabove being distended.
Histologically there are two main types ofcarcinoma of the rectum, namely the columnarcelled type and the mucoid type. Fuither, thetypes of cells vary considerably, in sometumours there is a preponderance of ar,aplasticcells and in others the majority of cells are wellaiffelentiated. Ihere are also maiy tumourswhich contain both varieties of cells in varyingproportions. An attempt has been made toapply the histological grading of Broders butthis has not been entirely satisfactory as anindex of prognosis, it is better to rely on adetailed study of the specimen with specialregard to invasion of the extrarectal tissues,regional lymph nodes and the rectal veins asdescribed by Dukes.
The Spread of the DiseaseImportant contributions to our knowledge
concerning the mode of spread of carcinoma ofthe rectum have been made by Miles5 andDukes. There are three main ways by whichthe disease progresses which will now bedescribed.
Spread by direct extension. The neoplasmspreads locally in the mucous and submucoustissues both longitudinally and transversely.Infiltration through the wall of the rectum isprogressive, each of the components beingpenetrated in their turn until the perirectalfatty tissues are involved, and subsequently thefascia propia and neighbouring structures,urinary bladder, prostate, uterus, vagina orsacrum.
Dukes has introduced a method whereby thedegree of local spread can be assessed. Hedistinguishes three groups of cases based on theextent of the disease. In group A are included-those:in which the growth is confined to thewall of the rectum and there is no extension tothe extrarectal tissues or regional lymph nodes.In group B are cases where the growth hasspread by direct extension into the extra-rectal tissues but there are no metastases in theregional lymph nodes. In group C are caseswhere there are metastases in the regionallymph nodes and in this category are two sub-divisions, namely group C.I in which there isat least one lymph node below the point ofligature of the vascular pedicle which is freefrom carcinoma; group C.2 in which all lymphnodes as high as the point of ligature of thevascular pedicle are involved by metastases.Dukes found that of the cases of carcinoma ofthe rectum which were operable, I5 per cent.were in group A, 35 per cent. in group B, and50 per cent. in group C.
Spread by the lymphatic system. This is avery important method of dissemination andexcept in neoplasms of a high grade ofmalignancy, the regional lymph nodes areusually not involved until the carcinoma hasinvaded the extrarectal tissues. The spreadappears to take place slowly from node to nodecommencing in the retiorectal group upwardsto the lymphatics of the pelvic mesocolon, thenthe paracolic nodes, the nodes situated at thebifurcation of the left common iliac artery and
.7anuary, 1947copyright.
on July 27, 2021 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.23.255.17 on 1 January 1947. D
ownloaded from

POST-GRADUATE MEDICAL JOURNAL
finally the aortic group is affected. Mileshas stressed the importance of a thorough re-moval of the whole of the pelvic mesocolon onthe ground that there is scarcely a part of itin which metastases have not been found.Spread by venous system. Extension of the
malignant process through the venous systemoccurs by a process of thrombosis or embolism.In a series of 539 cases reported by Dukes inwhich the veins were dissected out and ex-amined microscopically there was evidence ofsuch extension in 17.8 per cent. It seems thatinvasion of the veins does not occur until thegrowth has invaded the extrarectal tissues andit is related with spread along the lymphatics.The importance of this method of spread isexemplified by the frequency of metastases inthe liver.
The Early SymptomatologySuccess in the treatment of cancer largely
depends upon early diagnosis and the in-stitution of treatment during the initial phasesin the development of the neoplasm. Thisstatement applies to cancer of the rectum andif the survival rate from this disease is to beimproved materially then patients must presentthemselves for treatment at an earlier stage inthe disease. Careful study should be given tothe early symptomatology so that in thepresence of these indications of serious diseasea complete investigation can be carried out. Itis a distressing fact that so many patients arein an advanced stage of the disease when theypresent themselves, rendering the performanceof radical surgical extirpation impossible.The disease is often insidious in onset and
there may be a latent period during which thesymptoms are: minimal or absent altogether.The significance of the first symptom must berecognized in order that a complete investiga-tion may be' instituted and the diagnosis made.If some other abnormality of the ano-rectalregion is present this must not be allowed tomask the underlying major 'lesion. Forexample, a patient may be treated for haemor-rhoids and a carcinoma higher in the rectummissed until late in its development. TooTmuch stress has been given to symptoms, suchas haemorrhage, alternating diarrhoea and con-stipation and a change in the size of the stools,
in the past, and it is necessary to emphasizethat these are often late symptoms or indica-tions that the disease is well established. It islikely that a more detailed enquiry into changesin the function of the bowel will lead to earlierdiagnosis in many more patients in the future.The symptomatology varies with the site of
the disease in the rectum but attention iscalled to certain general early symptoms whichmay be present wherever the disease issituated.A change in bowel habit. The significance of
a change in bowel habit must be understoodclearly, and careful enquiries made concerningthe way in which the patient's bowel usuallyfunctioned before the change occurred. Thusa patient may state that he had an action of thebowel once or more every day and thenobserved that he became constipated or that thebowels were loose. In other cases a patientwho has been constipated notices that thischanges to diarrhoea; on the other hand apatient with loose bowels becomes constipated.Other points to remember when considerationis given to the bowel habits of these patientsare:-a change may occur in the timing ofdefaecation during the day, for example thebowel action occurs later than has been usual;there may be urgency of defaecation or asudden desire to defaecate occurs immediatelyafter the ingestion of food.Haemorrhagefrom the anus. I his may be the
first and an early symptom of the disease. Inthe earliest carcinoma of the rectum which theauthor has operated on the patient gave thehistory of slight bleeding from the anusextending over a period of several weeks, butone week before she attended hospital therewas an attack of severe bleeding. The bowelswere opened regularly with aperients, therewas no discharge, diarrhoea or pain. Sig-moidoscopy revealed a small ulcer with aproliferating edge and bleeding occurred whenit was touched.Mucoid discharge. In the early phases of the
development of a carcinoma of the rectumthere may be a slight discharge of mucous fromthe anus. This is'also present in certainbenign conditions such as an adenoma of therectum.
Pain. This is not a symptom of earlycarcinoma of the rectum except when the neo-
.7anuarY) 1947copyright.
on July 27, 2021 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.23.255.17 on 1 January 1947. D
ownloaded from

CANCER OF THE RECTUM
plasm involves the anal canal or anus. Inthese patients there may be an ache in therectum with sharp pain during defaecation. Inthe later phases of the disease the pain may bevery severe especially when the carcinoma in-filtrates through the anterior wall of the rectuminto the prostate, urinary bladder or urethra,or when it involves the sacrum.
Correlation of symptomatology and site ofcarcinoma. The symptomatology of carcinomaof the rectum varies according to its site, sothat there is no complete train of symptomswhich is applicable to all cases. Thus acarcinoma at the recto-sigmoidal junction tendsto be of the stenotic variety and producessvmptoms of intestinal occlusion. When theneoplasm is of the proliferating type there isusually a mucoid discharge and diarrhoea.Bleeding may' also occur; later an attack ofintestinal occlusion may develop due to faecalimpaction above the neoplasm or from intus-susception. A carcinoma situated in theampulla may be present for several monthsbefore causing symptoms. When tne surfacebecomes ulceiated, bleeding occurs. When theneoplasm is situated low in the rectum close tothe anal canal there may be a sense of fullnesspersisting in the rectum' following defaecation.There is also pain which is experienced duringdefaecation and this often persists for sometime afterwards.
The late symptomatology. When the diseaseis well-established or advanced the symptomsbecome more severe. The bowels arevery irregular with severe diarrhoea andthe passage of blood and mucous. There maybe incontinence or faeces and a marked dis-charge from the anus. The patient maycomplain of the sensation of a tumour in therectum. Pain becomes severe and may be ex-perienced in several situations including theano-rectal region, the lower part of the back,the perineum or abdomen. Pain may bereferred to the lower extremity. The generalcondition of the patient deteriorates fairlyrapidly, wasting and secondary anaemia soondevelop. Inflammatory complications mayoccur including the development of an ischio-rectal abscess and an ano-rectal fistula.
Physical examination. An assessment ismade of the general physical condition of thepatient including the nutrition, cardio-
vascular, respiratory and urinary systems. Incertain cases there is extension of the diseaseto the left supraclavicular lymph nodes. Theabdomen is examined critically to determinewhether there are any abdominal extensions ofthe disease especially to the liver or regionallymph nodes, or secondary deposits in thegreat omentum and peritoneum. Anyabdominal distension is noted and the con-dition of the inguinal lymph nodes is deter-mined. Routine matters such as oral sepsisare dealt with as in any surgical patient.
Digital examination of the rectum is carriedout with the patient in the right lateral positionand every segment of the rectum palpatedcritically with the index finger. If a neoplasmis palpable, its type, extent, size and indura-tion, together with the degree of mobility orfixity which is present are determined. En-larged lymph nodes in the mesorectum will befelt posteriorly or posterolaterally.
Proctoscopy and sigmoidoscopy. These ex-aminations must always be carried out so thatthe carcinoma can be visualized and the find-ings on digital examination can be confirmed.When the sigmoidoscope can be introducedinto the rectum at a higher level thar thecarcinoma, the bowel can be inspected for thepresence or other abnormalities such as anadenoma, polyp or a second carcinoma. Manycases or carcinoma high in the rectum whichare beyond the reach of the index finger willbe discovered by the use of the sigmoidoscope.
Biopsy. The removal of a small portion of acarcinoma of the rectum can be done withBriining's forceps through the sigmoidoscope.By this means the diagnosis can be confirmed.
Radiological examination after a bariumenema. This method of investigation is un-necessary in cases ofcarcinoma ofthe rectum butit is sometimes useful in rectosigmoidal car-cinoma when the growth is not seen with thesigmoidoscope which cannot reach this regionon account of spasm or kinking of the bowel.This region of the bowel is difficult to visualizeradiologically and the examination must becarried out by an expert radiologist. It ispointed out that a negative examination doesnot exclude the presence of a carcinoma. Whena malignant neoplasm is present it will giverise to a filling defect in the bowel or a stricturewill be seen.
.7anuary, 1947 21
copyright. on July 27, 2021 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.23.255.17 on 1 January 1947. Dow
nloaded from

POST-GRADUATE MEDICAL JOURNAL
Treatment. The only method of treatmentavailable at present for the cure of carcinomaof the rectum is radical surgical excision.Discussing this matter Miles5 states that therectum is especially amenable to radical ex-tirpation for malignant disease, owing to thefact that the main line of advance in the in-vasion of the extra-mural tissues takes place instructures which are not only removable, butare also remote from the primary diseasenecessitating the lapse of a certain length oftime before the invading cells have progressedbeyond the limits of the field of possibleoperation. Indeed, Miles considers that noother organ in the body is so favourably placedin this. respect. The radical operation forcarcinoma of the rectum must be planned withregard to the spread of the disease to structuresremoved from the primary site. It must em-brace all the tissues which pathological studieshave shown to be prone to carcinomatous in-vasiorl. In describing the evolution of theabdomino-perineal excision of the rectum,Miles, who so brilliantly conceivec andexecuted it, stated he was impressed by thefrequency of recurrences after perineal excisionoperations and was convinced that the fault layin technique and probably in conservatism inthe removal of the tissues surrounding thediseased portion of the bowel.At the present time there are two standard
operations for the radical excision of therectum for carcinoma, namely, the abdomino-perineal operation (Miles) and the perinco-abdominal operation in one stage developed byGabriel. Both operations may be carried outas two-stage procedures if it is necessary owingto the poor general condition of the patient.There are certain disadvantages associatedwith a two-stage operation, chiefly due to thepresence of a colostomy and the risk of septiccomplications developing in consequence.
The synchronous abdomino-perineal excisionoperation. During recent years this modi-fication has been developed and is practisedfrequently. In this method two surgeonsare operating at the same time, one carryingout the abdominal, and the other perform-ing. the perineal part of the procedure.By this technique the time taken for theoperation is diminished and the average caseshould be completed in one hour. There is
another important and distinct advantage,however, namely in the case of a carcinoma ofdoubtful operability due to local fixation it ismost helpful for one surgeon to separate thegrowth from surrounding tissues working fromthe abdominal aspect and the other surgeon todo the same from the perineal aspect. Usingthis technique it is probable that neoplasms ofbordel-line operability can be removed satis-factorily.
Conservative Resections of the Rectumwith Preservation of the Sphincters
From time to time there has been anadvocacy of these operations for certain casesof early carcinoma of the rectum. The objectof these procedures is to avoid the establish-ment of a permanent colostomy. A number ofsuccessful conservative resections have beenreported in the literature, the patients re-maining alive and free from recurrent diseaseover a large number of years. There are twochief methods, namely the Kraske operationembodying sacral excision with conservationof the sphincters and circular rectorrhaphy,and the combined abdomino-sacral excision.On general principles. it appears sounder toperform a radical excision of the rectum withevery prospect of cure than to temporize witha conservative operation and run the risk ofrecurrent carcinoma in an early case.
The Abdomino-Perineal Excision of theRectum
The technical details of this operation, soably worked out and described by Miles, arewell-known and widely applied. The operationis of considerable magnitude and no effortmust be spared in the pre- and post-operativetreatment if a successful result is to beachieved. Doiring recent years thern has beena fall in the operative mortality and due creditis given to. the contribution made by thistreatment before and after operation which willbe described.
Pre-operative care. The patient is admittedto hospital for a period of ten days before theoperation is performed to allow investigatior sand treatment to be carried out including anassessment of the patient's general health andnutritional state. If protein deficiency and
YanuarY) 1947
copyright. on July 27, 2021 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.23.255.17 on 1 January 1947. Dow
nloaded from

Yanuary, 1947 CANCER OF THE RECTUM 23
| - | | | -N - N | *| - | | |- - - l - - l -E - | | | | -E - | I | || - | , * | -E - S , * * IS - | I | | -- - - 1 * * --| - - ! | |e - | | | | -- - | . . I -- * i i | -
E - E I | || - | ! | |- * l * * -N - | l | l -l | l l | 11V.w-. - E s a . - S . -
| R i l | 11 11 -| | | I | I 111| | | | | ! i *;* | | | - | -| - 111 3 -1- . . - l -- - . -- . . . -. . . l - I. . - , -- - . , - ,
--,- - |3 | |
| | | |- -- -- * - -s * * l | - l -- - | - | - -* * l - l - -
w |-
CARCINOMA OF RECTUM.-Microscopic section showinga small metastasis in a lymph node.
copyright. on July 27, 2021 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.23.255.17 on 1 January 1947. Dow
nloaded from

24 POST-GRADUATE MEDICAL JOURNAL January, I1947
M.............
..aU 6. 8i.#3 .: .-
it'n'. .-
CARCINOMA OF RECTUM.-Microscopic section showinga malignant lymphatic embolus.
copyright. on July 27, 2021 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.23.255.17 on 1 January 1947. Dow
nloaded from

January, 1947 CANCER OF THE RECTUM 25
R U:..:Mlif:..:.;%,
...
Mk ,.zm
Md.
CARCINOMA OF RECTUM.-Microscopic section showingabrupt transition from normal to malignant rectal
mucosa.
copyright. on July 27, 2021 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.23.255.17 on 1 January 1947. Dow
nloaded from

26 POST-GRADUATE MIEDICAL JOURNAL January, 1947
4....
CARCINOMA OF RECTUNI. Microscopic section showingabrupt transition from normal to malignant rectal
mucosa.
copyright. on July 27, 2021 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.23.255.17 on 1 January 1947. Dow
nloaded from

January, 1947 CANCER OF THE RECTUM 27
|............. ....................
0C...
5/ Z..............
CARCINOMA OF THE RECTUM.-Flat nodular type.(Museum of the Royal Cancer Hospital.)
copyright. on July 27, 2021 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.23.255.17 on 1 January 1947. Dow
nloaded from

28 POST-GRADUATE MEDICAL JOURNAL Jlanuary, 1947
CARCINOMA OF THE RECTUM.-Annular fibro-carcinomatype.
(Museum of The Royal Cancer Hospital.)
copyright. on July 27, 2021 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.23.255.17 on 1 January 1947. Dow
nloaded from

J'anuary, I947 CANCER OF THE RECTUM 29
CMCINOMA OF THE RECTtUM.-Ulcerative type.(Museum of the Royal Cancer Hospital.)
copyright. on July 27, 2021 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.23.255.17 on 1 January 1947. Dow
nloaded from

30 POST-GRADUATE MEDICAL JOURNAL anuary, I947
............. .......'-:.'-''-:...,.....:.:.::.f.....:.:..:::::.::.:..:::..:.:;.:...;.:..::..l.....:;.:.:::.:.,-.,:..:...:::::::.,.,.:.::.:.....:.::..::.:,..:..:.-:.':-::.:,.....,,,, ,:,. .".%::.,:,.... .......,-,.,,..: -....... ... :..
,-, ... -...:::. .-. ...".............:.--.::,.... ....,,...... .:.:::;:...,:.::i::..:..::...:::....,...,.:.;:...,:.::.::...:..:::-........,.i.:.:;.".,.-.'..;,,...:..-..-......:..;:.::.:.",;::;;."..:-:..-;?.....:.....:.....: ......;....::,.:... ,:, ::.:::-, ....... ,-.. -,,... ..:..:..-!:, -,::-,Fx::-.:::: .:::::::..::.,-.,;,..".-'.i..:;...:-.'-.'......,-.-...,...,:::..":..,,-...'.".,;:...:-...-'-.'.....-'...,."..,..,.".,..,...'.....'.'...i....::..'.-,.,L..,.-,.;,.-:;...'..'.'..,:.iK:..:.:,.,j.::.::::.::.,.: .: :,::,.:. ...:............,K::...
...:"I:::. ,.::-`:.:.,:-:7'. .":: '-:x--.'-':.'..::...j.::-.....::!;.!.a.::..-:.' '.': -.,:.,. -:...:. -'..'.-'..".:..:.:.-.,.-,-s. -'...'..' ".. -',..' -.".-."--. !'- .:.:- .,:....... .::, .:. ;:: -:.:--'-. ..".,-,.,.,:""::-k ",l':.---.-*-.--,.,- -.-,.-:::g:i. .. .'."..",'. -'.'.x.."-.":A..'. -'..;;..-.'.'..,::.-....:..'.E.:..:.::..::.:..:.:: '..... ..:. -:............ -.,.-..:....: -:1:.;.,....%;...,:,.;:.'.;.,.,..,..,......,.::,-..,-,....... ....... .,: ...--, ..-.' .i..:-........ i:!. ...;n ....6. .-.. ... -.':...." ...: .:. 1-::,: :::.--' .` .-:.:.'..:.% ..:......s"...-.'-..-.'-..':::...'..': :,.-,.---,2..,-.,..:...--::T,W-,K. ."!."-".-".". .";.,- "-,:..". :.,..:-- :...:-..,. --. .-..,,-'--. ----.z.:::.:::-::- ,,-,.:.... ....i.! ...'..:..:.::. "-:-...: :.4--.'-.:- .'-'-...,:.,..,.-.-:i:;..,-.,-.,;!;..,-.,::..",...,..'.....-.-...,...:..,....,..-.:,..;'.-';..-.".,;.,.,....-:.-..,-.....,...,.- :."$:.::;.....'s.:,.-.....--.....,..,..,.,..,:s:.,..,..,....",.!..,.-,...:..,.",:,: .......---.: I.. I.'....,,..::m..,...!. ............:..:::..;.: .....,:...::...,... ""'," ,:. ....
...""' ---.-..,.-..-.:......., --..., -"-' ..-." -,,.::.....-..:...-.,:;:.,....,.%,.,.-.::::....'..,.::.".,:..'.-,......... :...... ::, ..:. ..:,:. ..::,. ..,:. .... ,.:. -'.'...'..'..:-, --:-- ,,..-, -...,,,,.,,,-,.." .-...","",,.......,:,:, :-:.::%-.:-...,,,..,,,.. -::-:'-'..,.,:,.,:.:.'-..---- ..-..-.. .-.-.-.--.-4. .....-..,::,::....,.. -...-.' .-...-...-,.....'.-..-.:;...,;..,.;.:.- ......::::.. -"- ..,:,,"",,,,... ...:., ,-,---s-,-,,-,---,-,,:-, ...'.",...?..::-:.....::.......: .......-""', ",:. .:....:-.,..,.,.,.,.,..'..-..'..'..'.'.....'...'.-,:...,-..-...-.'-,.'..:..-..,.,.,:.:,."e.-'-,'..-',-'.-..-.':!.-.'..-....,4.: .:.::..."... :.......... ..-.:: .-..-..-..... ....-.. .r..-,................-- c..... ......,-,,.....-..--.. ......,,-, ,-,'.'.' ......-.:....:..-.. ......:"-...%..: ........:.....-...--:4.,:.:..::.,.,.-..."-,.-.:.:;,-.,:.:,.. -.,. -,..-.,:.:,..-' -.'. .-'..' ..'....,....,.,-.'....'...,:.-,.......",.,..;."..,.-..,..,. :%.::..:.....:,:::. .":.:..:,--- -5.. ...... :........--".:-... ..... ...... ......:X:.".....:--: i...;!.. -...::..:::....,"........:...,."-.,:.:.-.:;.."..,....:,...,.-..: "..,:: ..- .'--. -.- -'.-:::,-,.,-.,..-,:,-..,-..,:,., "...,.,...-.-, ,--""'-",".'-".'k".,."., .: ... .........:....--.::,!.,,,-,........:..-...4.......... :, -.. ..:..--..- ----.--.:.:.:.:-....--.:::..-.........:::..,.- !.:,,: ..:..,....... ... ......., .........., ;:4-...... ...:...,.:..,-.::..:--.;:- .:'.-.-.,.,......,", ,,, ,,--:u:l:. ........ ... ----..: .-'-. -,-:---,;:::.:,,, ::..,.....:.-.,::.:::::.:,..,.-.: -,..,:.,.,.,-.",:, ".":", -... --s.: ..%..,.. ,;: -:........-.... -....... ...-.... .. .....:.....-,..... ...4...;.---.-.-. ....'-.-...--..-'.'....'.-'..'.-.., .,.". ---':.`..,.-'::: 1::,:..
"-...::.:. .......:.:,." -":,.,--.-..-..---....: .: -, .,;..,.::..- '-': '...:.I., ..-..:...,.. .:---.-...-::-.::....:........:.........- ::::::7, .:: .::.: -'.'-.: .:.. -, ,.",.........:.., ,":. :,: ..::: ..:::......%,...:::.;.:. ::.: ,;::..-...-':'.-.. -----:. ---,-!:,--,--..'- ..'.".:.:-`.":!..".A;.- .".,: ::.,..,::,..: .....,".' ..:..:. ...E...,:::.....?. 1. ... .......:, ...-.--.: .:.U'.'-.-':i.Z.:.:,;..::.!.!.'.."::-.,,.,:.-;.- -:-:.:. .:.-.,:.-,..:,.,-,.-,.,.."-.,:: :;,-,. ......-- ..;-:..:.:. ... "',........",-.."........,..: ....... ...... ....:::::-.--.-,.-.-..--.,:: .:....:... ....,.... ....... .: -.'...'..' :.:.:.:;:....,--..,:,-,..,-.,..:...'.::;..:.:,::,:"..,,, .......:. '. "._'.." '.. ,,,.-.: .: -.. ': -':..-.. .:::-......:,.: -.% .":: .,-,.,.; i....:.:...........--4':i.., .-..'.";:: .: .:..:.::..--....:......7'...........-'...-'..._....::. ..------.,-.,::;::: ..:.:.- M. .. ."!..::j::!..::,. ..,...,-, :..;.::..::..,:..:,-.. ..:.: -:.,.:-F .. ::::...:.. .--:.? .",:,:::
.I.:..... :..' :..-::.:.,..,;:.:.,..: .-.:-::;.,:,-.,-.:;:.: .:.. ..,-........." ,:-..-.--,::.;:-;... :. --.-.'-.: :...... :.: ,.,.. :-.:,,..: ................"", :....:,:....:.--.---. .----.- --.. ... -.-s ..,.::::' -.. .. .-":..:..:-::-:;- .: :.;:..,:.:....: :.:-%.. ::: :.::..'. .-.'.' ....-..-.." ---:.:.;.;,.;. :.4.. .; ;;:::.;:-...:.: .:....:-.: ..-.. :...:.:....- ..:.....:---'.,;,::: .:-:.'--' ,,,::.:: :": -...:.:....-:-,--.:-:.-::-;:-.- :....:.: :::..:. ,:: .:..;:. ..::... ::..--' ::...':-.,:..:.:.:-:; ....'..::." ....:.,:,i.::4.:....'.....:-:-.::i...:..:............;.: ..-.... '-'-.--:-:-:-.::.--.-.:: .:.: ::.-.:::.::.::-:-..:.,..::: :...,.:::-. '..-:,:..::.::::::"... -.:.:-.: ... :.... ..-::,.,:.-..'.. :..::.-..--:.-: -:.:..:: ::::.;-:-.,-.'i.-..:::,.
.."...",:-::..:.%::.:.:.%:% ::::.::: ........::;:.,..,...: ..:: :.-..:? ..,.-'--': -..; .;:.:;.:.::- --:. ...::: :" .., .!:: ,.'. .:--:.-::-.:.--'.;..:;:..: ...,....... -..., .:...::::.:.. .:..:.::.::.:-:.:..-.::-::--. ,!--.:.......... .:,i.........:: .::....?.:..- :.:.,.:.::.:.--..:..:.:..:!.;.::.::.:..-.;;:.-,'.,.........%... --,;-,.,-,---,.:..:'..,-;. ..-:..;:.;::.:....::. .:.-..:;.:..::.::.;.:..i.!i."..,.,...,:!.."...'.:.i;..::...:,:.::..:.:: .:... ,:.. .": :....:.:. -...C::-,;...:.:,: .. ::...:?-...'.: -.i- ..::.;::,:: :.,.:.: :.:::. %:."?'. .:..-;:::..: .:..:i... ..:.....:... .."'; '.,. :., .j: .,:. .... ..:.:.i:...:.,.:..:.....::...-..,... :..:.:.!.::....:r.: .N .: :.-.:-:...---. ---,---,:;--. ;,--,:::... ::;'...-M...: ..:. ....:..::.". '..:::::,..i,:-:..;,%;- -:.-:::i:-:--"- :..- ---..: :........::::.:;,....:..:..:.;:,:.:". :.:-,.: ::Ij:.:, ..-, .....- ..-':!' .%. !::... %.... ::::.. .: :.:":;.:.:.:,-::-:.- .:.:::..."..,:,:..:;.;-,.-'...'. :, :." .... :-:.:. :...:::iA: "; ..- i. .:;.:I:. .;i. ::. .--::;.-.::........:.? .N.:;.,:;: .: ..!:. ..'..:, .:,-:::...:.:4.:::..:..:::. ..::.-.,,. ....: ..,::--: ::..-..::..,;,-.:-;::;.-... ...'. :,-ji.,::..:.::-::,---- :,:..: .:....:: ,'..
::,.-:::,..-;..:..:::,.::...::.l...:.:1.F:,:: ,.:: .: 1. i:i: ::.::.:..:j,:i::. ;.:--. ,:. :.:. :. :...-i:. :-.: .":.: .!;: .- ;...:.,.:.:....?':::..::.4...". ,:.:::..::..;::::':::;.:,....:,.:,: -.-::. ::,..::-. .:::, ,.: .........--:......i?:...:.;...;...;::.:...: :.:: :i.i. ....:: .:..:::...:::::..: :;-:;:..::..'....::.::.::.....'..:;";; -,,,--,.:...:; .!:.- ...: .j i..", ': .: ..:: 1: :. :i..,.....::.::,:;.:;!:,:.::.;.::.:.:.:.."::. :..:;. -.! ..;:.: ,,... ... .:.! ::..: ..: :.:,:: :::.:!! :iL ....:..:. .:%:;;:;; -D-".;:;..:.:...:Z:: ::..;..::?.. ::.i%..;.:.PPA. '-. .:. .:.: ,..:::.- .'t .,::: ".:. .f ....::::::.-:.:. :;.::..;:.::.: ..;...... .;i.§.i.;:;;..,.:,! :-.-.. :.:..!..:::.:,F. :...,,-.h-. ,:::-:.-.-. -'.'..:..'..'.:::: ': :.:.....,.:.:;....'..'...'.:.:,:,..:.::- ...:.,...:... :..-.. ...;:;.......:.i...,..,-.,..;..:..".".....;!..i:..:;..;......; :.;;:..::-..:::..:...:i.:.!.:.....:.:: ::::.i.,:, ::.....;:.;;...:...........:....;.'-.....:.ii..:..;.:ii....:,::!t:!-.i-..-:-i:-:!::!:.:.!:.. :.:;:..;:- ....:.....:..;....;;..;.;;:..::..::::.::,::..:., '..,::....::::.::.:.....:....;.:.."...,:....J..x-..j.:... .:::::i:; .:::.x:.:;::::;i;::::..- -:::...'-.'.:.::, .:..:.: :i:::.::!:j.:.,. .i. 1: .. j: ..:i. .-:.:.:.-:...:;::.:::::.....:::...i::..::!....:;,...-.,.:..!...i..::.:::.::.:-;.: -.'- -.< ":.:::. ...: ?.-..:::..:::...:.i;:::;:;..-....:...:..::?.:....:;..;. .i:.: i.. i. !'.::.,:j :::!;.;:..! .:..: .; ":. .;:,...!..!,:....:.;...:::::...i:..::.,....,,:.:-.i.,.;..;..:: %:.:::.:.: ..::..:.!.. :i...'..".....;..;.;::.!:i.,:.j..i:!:!:..;.;.!:...:...:!.'..j....... .:..;;...:..;.:::.........,:.:.4.:,...::::..-. :":- .::i:j.::..:.,:.';.: -.'..:.-..::?.!..::.! :.".",-....,.,...... .,:..:.;2;;.;.::.!:..n::.-:!;.:!.;!-. .;:. ;.::...:: ii:.: i.,: !n.:..;.;.E .:. i::: i:.iSi iui :.;: ';.:. i.': :: !..: i:-.:- .-!::.:.:::.ij:.: .::!..:..:;:,.,.,...:.'-.';:....'.:.:::::;;::.:...:..:.: .--
;;.;;:i:; !..!:.;....:;::;..;..:i.:::..:;;!.i::..i:..!.:::;:i...:.:.;......i.j..!:: !::..:.!.:T::F:,-.:i ::i....::. :::.:i:.i.:...h .... --.:il."....:?.ii.:,.:.;......!:i:..2::.,.:::. --E-.!:.::':::.:--,--,;-:--- .--::.....-.:.;iii:,i -p.l:.!.i::;;,.:i.:.....i.:::.::..i.j..i::::,;..!:.:!.5 :-..'...:: :K: .;-. .:%,::: -.-,.-,:..;;:-: --
:::..::.:.:..:...:...i..;:.::.:;.;::....;:......::;.E.::,.; :-:.-::;:..:!.::5.:].:::.::.;.:.:....Ei...,:,:-:.J;:- .:. i.:. :..: .:.!,:. -Tijj.;..:- ..; ..:. ..!i: ::..:.:,.,..!i.!..!...;:,;:!..:'.,:.::!:..:.::.; ,..i:.,;::::..;:::::;g:.i:......:..."..,:.:.,.-::...::.: .-:. :::.;:-:.:;:::;::;.i.:.: .:..!i.'ji:::. .::: -... ... :.:! :.:. i.-. !.,-::.: .........:......:..:..::i.....;...:.:. :".;.-::`:?:: ... ..:.::,p..:%..-,j,.i...-"..-.:.....::::.:.:...:..:::.:
1!,:::...::x..;:j::..:;:...,.:.:: ;:; .:!; .::: .. :.::.,...::.:. .::: ..-.:::.:'...:.::..........;..:.i..:.;;.... ..::..;..:..::..: .:. :;X1 :.,:.:::.s.Ai.§' .;:. ..::- -,"',".......;:;:;::: ::i!:!:!;:: ..'- ;;..-i:.. !,.;-:'.!.::i...:.....: .x:;:,::.;:;,:...:...:,::.. .:.:..;i:!::I:s!::!.:.:;.:f::i:.:::.:,.: -..... -:,:,!--.;: ..:!:..:... :...,::!;;:-,:....i.....;;.:.:...:...,-.,.:::.:!,: ,'.:.., -.:,.:.,:..:.:;:::....::?:.:...:...::..:: :"D;.- :---.:-.:.--.,:.:g;: :.'. .:.:....:...:...;4......... .:: ...: .:: ..;. :-:.....;.::...:.:i,.,:.:..:::.:.::.:: :::.K- "::,!;!; ... .- .:;:::: ..Ii: ::.. :::.:;:;;..::,..;.E.-;::;.-.:-:.:-.,...:!,:::...: ...-:. .::::.:..:K.: ... V..:,.i:. ... ::.::.::,..."".i.ii !i.i:;,::,:.:.,: i.;: i':'.:.: .E...:-::., :7..':.:-:;,.:;::.;::... -:.:?.:;. :.:. ..::.;..:,:.,:."::-.,..::j:.:..-: :....::::.::::..;:: :: .... ..:.: ..:: !--. -... ..:; ..i;..:::" -?!.;:.. .::.:.:i..:....m-:..N :. :- .......
...... N. .,:,: ;-,.;.! .;I:::!.:. i.:..,.! :!.i.!::.s.::.l..!.:..:,:;..i...:.i:.:..: :.:.:::..::.:,:;.;::,.::.::::.:: ...::..:,-::: ::.:.: ;.%: .::. .-;: :,!..!,: !,...;.,..!::--:!::: j.:::: ':".:::: ::::::.::: -:..... ..,,
......... :::.-:.. ..:.,: .... :. .: ...:;.;-. ....:.::..::.:...-:::.:.:.:..: ;. :.'...,:.". .:!; .; i! .i:!; i.,..:..i:.-,,,. ..*........:...:::,"" ,,.:..:..:,.'-:. ': ::,. :. :::'.::.... ...: .:: ..::. ;;.:!.:.:..!. -.---.---..d..!i.;;.:.: ,..:.: ::-,.....:...::. ::..:. .::: .:.:: ': -":"..:...:. .....::,. --]::i:.:;::;- .:!..:: .. i!.i..!i...:.:..: ,... ..:- ;-,:.:,.-,-:; .-:! !,.:.;,::;i:.::.:.:..:.....:.;...:.; :- ::! .: :.:..,:, -,:-.:,-:.:: .:: :,::!:,. .: :"?,.::,. .:,: ,.: I...--
,"' "',.. :... :-.:n:..::. ::..:-.:.:-..-: -.. -,.:::': ;:: --.:-:..-.;..i.:.::.:'.:.:..-:, .,!,::. .:; ::..% ':: !:::-:;,:%'. -.:..,': .,. '.., -, .: .: ..... :-'.::.:::::: :..:,:::..... .-,.-..: .------.!--- :.--',,"', "i.! --,.:;.: ::..:: ::..,. :.: ..: ...... -------.--'.::---, .." ....'.....".."'...,., :.:';- '-:-.-:..:-..-. ...,..,:. :.: :: :-...: .:,: '..:..'..:.: .:::... .. ,.:,.::.. ...:::N::...: ....:.! ::::,: '..: ::. .!.:....-1: ,:: :.,: ::.:.-:.:. .:: !:...... .:: :..:...::..: .:..:-..::::....,.,..... ..:.::.:.:.-:.-......:.. ...... :.:!.:..": .....
.::.... .... .... .::::,.. :::..,,,:,:":,.:, :.Q::.,-.:, ..-,..::-.: .'-.::.:.. :.. .:: ::: :.
--...:.:,,: ,'. :..:.., '.-........... :.::: i..F..::::: .:,..:: :-.:..::: ...:... :,::....:.:.. :. 'v, .1::.::':....;.;..;.:..:.....,:: ......:.::.; ;::...-:.. .'t'-.. .::: -...-: -.. ..:... ... -!.':.;.... ...: ......:,....-..:.-:--.-- -.:..;.:: :..;..::., -i.iF...P.:-k- :.:...",,.........::::,>:: :::: .j: ,:::.%.::......:..: :.; .:::i.---....."..:.. .....:-...:!: :::.: ,..:.. :....:.... :.:! .,! .j:-X: ;..: ...::.:: :...:.: .:: :... ..,
..,.. :.-::-:.,;;:.: :...-.:..... .:........,,:,,..:. .h.,, ,. :-:,...:......:..:. -:- .: ......,:"."...:.:...:: .:: :.".%.:.. ..: ............:...: .:,!":.:,....: :-, ... .... i:: '... .... ..: ::. ... ... -.::.:...,: ..:.....::... -..:....-.......: ..:..;;:: ..----:!:..: -::.: ,::".:, ........
... .......-..-.-::...:..-:.'. ":.!-;,-:.:. ... .::.-- ...:..: :.' ..': .::.: ,.-........:::-'- ........ .....:.:.!:.::,..-,,. .----. .::f:"::...-..I...,.. ..:::...: .:.:-'-.-, ........ .....,.,,,,,.......- ..:..... ...,........'. '.. ..'.: -':. ':......?. .!....... ;."---""..,.:..-.,,......:-,:1-...:,.--,...-..... :.....: ,:. ..........,.':...... :: .::. ..'. .::::F. :.,. .-:,-.-:-.-,:-l?:::-::. ......... :. ............. ::-- .:::.- .:... -:::::s.--,;,--,.,-,: ::....
1:.X,.:".:... .."': :;! .--.. .:.:... ::V: ::..:..-:. .,-,.: -----.-:.' -.:- ,,,,:.:: I.:,.,.:."::. ":;'K....-......:::.: :: ': ,, -:,.:::::,.,.:.... -.--,-. .4... :...... ..: ";, -,---'-.:.:.'. i.. .:... ....:... ............'. :..., ::........ .: ...... ..: :.. .... .-...-...... ..... .:::......:;:....:..- 7... ....
... .::%..-4-:,i-:;. ,%:.;::- ... :::.,.;:.. ,... .-.. .........:..........:;... ....-......:.- ...:.."
..:.....: ........"". ,:; .-..--"., -. ': :....:. .. .. .. ..:....:.--.. ...::3., --:::::t.'--..- ..:O. ..::.:.:-.-:-c .... -.-.
............, ..:7.: ..:,---.........."..-'.:.........., N....:.:.:.........:..........:...--,:,!:.,- ,j:,,.:::.'.-.:--:::.r:§ --..-,,.:L ,... ::..:......I"".,,--- ..-:-:..-,:: ".,, ,,.I ...:,...::. -, .-- ..-.,4!.,.,- .,...:::::,.: ::-.-. -'.%'..:. .,,. ......-
.. -...,.r... U.,...:.. .,..-:-----. ,.:-:. ,F,:.!., ,:,...... ..i :.......:. ....- ::. ---.2:--,--:-,-,v ...;.,. -',.,, ,,,.:. .....:... :. ::.....:.. ...:i;...,,..................:.....: .....,......... ........I. :.: :%.-"...- .:: ,..I.. :.:;:,-N.-'-...,:.:::,-,.-.-.,....-..:.'.....- ....:: .........-.........%:-, `:.....:...,:.: :.. .....; !- .. .;,: 'r......:..i--'i;:....!;'..-"",..,.'-.'..,,...-'.: ,:, -,.- ,.....- --.%...........:.- -:.:.--.'.:.,..4..:".........: .'.:.:.:..::... .;..' ...:,.,...........,.".! :t :.4.......4:.:. ::,.. ,:.
..,::--......:. -.....%:. '. .:i:.-' ....,.-.:..:F-,: .N .:.:.-.- ..y.'y .:.:.:......:.:.... .:.::,.. ::......,., -.. ....
.......:.. :'...... ,:!,.:,.-,. .. ..-",.,-,":..-."ff.r,.-- ,:. .-.i: .: .,: ..... .:.:.:.....:::.i"' -,..F.M ,,,, .,....:....., :I ::-:,::-!;..;...'.'. '......-.....'....,: .:.,:--..:- ': .. ,:.;I;:..:;!::;::..!..j:; ,:.:.:..:. .:;.. .. .:- .........%..:.".,k?.:i:;.::.,:."4.'...,.-..., ...'---x.......'. .::'::;:.-.,::::.:,:..::::;......:.::-:.,..:::I..., --'N:..'.i-, i...:...i..--,,-:;s:...:::: -: :::---:-::.:.:.:.;,:. .:,:..: ':.:j,.?.:,:, ...::.::,:.!-:......:......... ....:..::::.,;.. ..::.:. :,:.::.::..::....."... :.. ..:,i.... -:;.;:..:..:;i ..:.:..;..;! :.:-.: %;-.-.. .:..;;: :.. .:!!.:.:;.:g;..:..:...%.: :z.,:;::,-;;fi-.D:::Z.:.:-..!:ri
"::,:.:.: :..:..::... :.....; .::, "' .,..:::.: ::....-;:-:- -::.-.-: -::..":.::,:K!.:- `. .;.::,i.i.....i..::.i;:...:..A;!""..:.-.-..-':..-..:.:... .::.... .%..:.:::.: -.i.?.%-.I:. .:::,::,: ": i::. ..,..,: ;:.: ..::,: :.....,.,:;;:i.::,:...;!::.i..i.......".., .,.:..... .i,..i- i::.:: .:!F:"::j;Vj::i,.f:::: .....::.:.: ":,-:,:..::::.:'-' :::::::i:::::::-:.'..'... .i::D::: i:.i.::.::::::l.-.:..:: .:::.:.. ..': "i-,: ,.;i:D. ::i. ..-.' .:.:.:: ..::!::. '::' i": ?:.-.-,:;:.:: .:. i.::.;.:.. .;!:;:: -.- .j.;:::&;. -:.",!;i.!.:. :.:.nikiil!K---.. ....:
..:: ........ :-- ..:..:..:.:...:. ...0-:-"--,:.:.,.-::.::::::-:..: ..:.;::; -:..:.%;-:--..- ,.::f;:::,;;:;:!,.;:!::R!i:.:ii;.;...r....:....:-- ..:...::. .:;.:...'..'.....:.....;......,.,..,!......-.'.i.."..,L.".,?..::.,.,:.:..:.:- ::.!:::-:::.:'..-.....:::. ?4.,-,-,;;-..::..:: .::.?.: .:- .-::.:-:;!; ,:::.!121':.;.i.:i::.....i.",.:i.pl',..g.!.jj .... ...::.;-::::.-;::::..::.:..:..:-::.-.,.. .:.:. :..... .:. .. .::...!..::.i, ii.;. ijg:.,:.-: .:;j:..]f.i:jj:-,.i..;!.:....:i. .::' i-:i ,:::,..::.YiJ:,il:ii. ....... .:.,!;..j.;'!..i,;;.:..::ii:i,..::..:.:::..:: :;-. -..
.:. ,,;.:X:.!.:.: .:. .: .!:. :!:.-!.:-:.:!;.;.--..:::.:;:::.:.!..:...........:.:j;: .,.i:..i.i.!!E:,! f.:;i,......:;: :. .:...:...,...ff.::.-i:§..;...;',. -:-.E.:!:.i ::-::-:!I-.. .:..
CARCINOMA OF THE RECTUM.-Sessile papilliferous type.(Museum of the Royal Cancer Hospital.)
copyright. on July 27, 2021 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.23.255.17 on 1 January 1947. Dow
nloaded from

January, I947 CANCER OF THE RECTUM
.. ..D.
*:.... ... :. ...:..
PAPILLOMA OF THE RECTUM.
(Museum of the Royal Cancer Hospital.)
copyright. on July 27, 2021 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.23.255.17 on 1 January 1947. Dow
nloaded from

32 POST-GRADUATE MEDICAL JOURNAL January, I947
CARCINOMA AND PAPILLOMA OF THE RECTUM.
(Museum of the Royal Cancer Hospital.)
copyright. on July 27, 2021 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.23.255.17 on 1 January 1947. Dow
nloaded from

January, 1947 CANCER OF THE RECTUM 33
.. .^'.H
........ .................:
:; ..;...:::
:~~ ............
!P.>
..:::
~~~~~~~~~~~~~~~~~~........................... ....... ......
Polyposis coli with a carcinoma at the lower end of the rectum.
copyright. on July 27, 2021 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.23.255.17 on 1 January 1947. Dow
nloaded from

34 POST-GRADUATE MEDICAL JOURNAL January, 1947
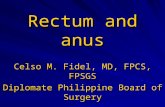
Affected)lymph-node
Haemorrhoidal /vessels
Periton ealref le c tion
-bearing area
Ballooningof rectal .' . ,ampulla
CARCINOMA OF RECTUM.-Schematic representation ofspecimen for pathological report.
CARCINOMA OF RECTUM.-Specimen removed at operationstretched for fixation.
..... .......... ....... ..... .. ........';
¢StS...H ,,gl,,,S
i i .e ,...l.l t:.r..:...
i......
. ........ .
..... .. ........... ...
~~~~~.......:::::
.. .. !.l. ....
-
..1 .... ..........
...
.. ...... ..-.- v
..I .
*4I;;..
I::
I,',0: }ll.l
'F§'
copyright. on July 27, 2021 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.23.255.17 on 1 January 1947. Dow
nloaded from

CANCER OF THE RECTUM
dehydration are present, they must becorrected together with any degree ofsecondary anaemia for which blood transfusionmay be required. The cardiovascular systemis examined, and the cardiac index isestimated; if this is less than 25, the operationcarries a considerable risk. The function ofthe kidneys is assessed and any oral sepsisis dealt with. Breathing exercises are in-stituted under the supervision of a physio-therapist. The patient's blood group isdetermined and cross-matching carried outwith one or more donors. The diet should beof low-residue character and of high caloricvalue containing an adequate amount of pro-tein, glucose and vitamins. A minimumamount of ioo gm. of protein should be takendaily. If the patient is apprehensive regardingthe operation a sedative such as luminal (gr. i 2should be prescribed. A laxative like senna isgiven and on alternate days a simple enema isadministered until the day preceding theoperation.
The use of sulfasuxidine. This substancewas introduced in 194I by Poth and Knotts asan intestinal antiseptic and it is now widelyused to modify the bacterial flora of the colonand to prepare the colon and rectum foroperation. The gram-negative flora of thebowel are inhibited and both aerobic andanaerobic organisms are affected. The drugis given in doses of 3 gm. orally every fourhours for seven days before the operation, ifno observations are made on the coliform con-tent of the faeces. Poth carried out quantita-tive bacteriological studies on the faeces of350 patients which showed less than i ,ooocoliform organisms per gram of wet faecesafter the following periods of treatment:37 per cent. within three days of treatment;8o per cent. within five days and 94 per cent.within seven days. If the coliform count isfollowed by the streak technique, Poth advisesthat the drug is given until the number ofcoliform colonies on the streaked plate is lessthan 20. The streaked technique is carried outas follows. A small particle of faeces is mixedwith a drop of sterile water containing 5 mg.per cent. of para-aminobenzoic acid on asterile slide and streaking a 2 mm. loopful ofthis triturate on a desoxycholate or eosin-methylene blue agar plate. This procedure
transfers approximately O.0I gm. of faeces onto the plate. Thex plate' count multiplied byioo gives the approximate number of coliformorganisms per gram of faeces. If waterydiarrhoea is present sulfathalidine 3.0 gm.every four hours is substituted for the sulfa-suxidine; if the diarrhoea ceases the dose isreduced to I.5 gm.These drugs are important adjuvants in the
surgery of the colon and rectum and it isstressed that meticulous attention must still begiven to surgical technique.On the evening before the operation the last
bowel w'ash-out is given and all the fluid mustbe syphoned away. The abdominal andperineal fields of operation are prepared in theusual way and sterile dressings are applied.One hour before the operation commences ahypodermic injection of omnopon (gr. '/3) andscopolamine (gr. I/I 50) is given. Shortlyafterwards a gum-elastic coude catheter (No. 8)is passed so that the urinary bladder can beemptied completely when the patient is placedon the operation table. The catheter is closedwith a sterile spigot and enclosed within asterile towel. The patient is anaesthetized inbed with pentothal-sodium given intra-venously, taken to the operating theatre and aspinal anaesthetic is then given unless thisform of anaesthesia is contra-indicated. Ifdesirable nitrous oxide and oxygen can beadministered during the operation to keep thepatient asleep. Before the operation is com-menced the urinary bladder is emptied byapplying suprapubic pressure while thecatheter is removed slowly. In patients whoare in poor general condition and spinalanaesthesia is contra-indicated, nitrous oxide,oxygen and ether anaesthesia should be used.
Post-operative care. When the operation iscompleted in the perineum a square of oiledsilk is invaginated into the cavity which ispacked lightly with rolled gauze. The laparo-tomy wound is covered with a double layer ofgauze and sealed off with elastoplast in orderto prevent contamination from the colostomy.The clamp is removed from the terminalcolostomy which is thereby opened. Thepatient is transferred to a warmed bed broughtto the operation theatre. During transportback to the ward all rough and unnecessarymovements must be avoided together with any
W.-
january, 1947 35
copyright. on July 27, 2021 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.23.255.17 on 1 January 1947. Dow
nloaded from

POST-GRADUATE MEDICAL JOURNAL
unnecessary exposure. If ' shock' is presentthe foot of the bed is elevated on blocks andresuscitation carried out. A blood transfusionof one pint is administered as a routinemeasure followed by glucose-saline infusionwhich is continued until peristalsis returns,normally after 48 to 72 hours. The blood isgiven at the rate of 30 drops each minute. Forthis purpose one ot the veins of the forearm isused so that the patient can be out of bed at anearly stage. During the first 48 hours nothingis given by mouth and frequent rinsing iscarried out. The patient is allowed to chewraw pineapple and chewing gum but fluid isnot taken until active peristalsis returns whensmall quantities are given. For the relief ofpain -during the initial post-operative phasehypodermic injections of heroin (gr. I/I2) aregiven at intervals of four hours. The patientis instructed to carry out breathing exercisesat frequent intervals and pulmonary ventila-tion may be increased by giving inhalations ofa mixture of oxygen and carbon dioxide (5 percent.) for periods of ten minutes at intervals oftwo hours. The position of the patient in bedmust be changed so that he does not lie on theback for a period longer than six hours andfrequent changes on to the side are made. Thelower extremities are moved actively so thatthe calves of the legs do not press against thebed for long periods. Care is taken in liftingthe patient, which is performed by placingarms under the knees and round the posterioraspect of the chest.At the end of eight hours following opera-
tion attention is given to the urinary bladderand the patient is encouraged to void uririe.When mucturition cannot be performednormally, a catheter is passed under strictaseptic conditions at intervals of eight hoursfor a few days, the bladder being irrigated witha solution of mercury oxycyanide (strength iin io,ooo) on each occasion.
After 24 hours have elapsed after operation,one-half of the gauze packing is removed fromthe perineal wound. In order that the recon-structed pelvic floor shall become a lining ofthe pelvis it is advisable for the patient tostand out of bed at this time, or as soon after-wards as the general condition will allow. Atthe end of 48 hours all the gauze packing andoiled-silk is removed. The perineal wound is
then irrigated with a pint of h'ydrogen peroxidefollowed by a pint of a solution of mercuryperchloride (strength I in 500) and finally witha pint of a solution of normal saline. Theseirrigations are carried out using a douche-canand catheter. Care is taken to prevent theretention of exudate in the wound. At the endof the first week the solution of mercuryperchloride is replaced by a solution oftincture of iodine (strength 2 drachms in i pintof water). From the third week onwards thesolution of hydrogen peroxide and saline areomitted and the tincture of iodine is reducedto one-half strength. The sutures are removedfrom all the wounds on the tenth post-operativeday; when Michel's clips are used for thelaparotomy wound they are removed on thethird post-operative day.The colostomy may act spontaneously
during the first few days, but in any case anaperient of either senna or cascara is given onthe fourth post-operative day and on the fi*:thday and onwards the colostomy is washed outdaily. During the initial 14 days this is per-formed with a pint of a solution of soft soapand substituted later by normal saline solution.The patient is instructed in colostomy manage-ment and after the morning wash-out 'nofurther attention is required during the ensuingday. On the tenth post-operative day thecolostomy is trimmed and any excessivelength of bowel is removed so that the openingis on a level with the skin; no anaesthetic isrequired for this procedure. The index fingeris passed into the colostomy every day toprevent cicatricial contraction occurring andmeasurements are taken for a colostomy beltwhich is then ordered.
The Palliative TreatmentIt is an unfortunate fact that many patients
still apply for treatment when the disease is sofar advanced that only palliative treatmn-ent ispossible. Owing to the large number in thisgroup of patients this part of our subject is animportant one and much can be done toameliorate their symptoms which are often ofa distressing nature.
The general management of the patient.Care is taken to preserve as far as possible thegeneral health and the patient is placed undergood hygienic conditions and given plenty of
36 Yanuary, 1947
copyright. on July 27, 2021 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.23.255.17 on 1 January 1947. Dow
nloaded from

CANCER OF THE RECTUM
fresh air; mild exercises are of value.Diet. This must be of a nutritious nature
and of high caloric value. A chirt is maintainedshowing the amount of food taken and itscaloric content; records are kept of thepatient's body weight and of the serum proteincontent, these investigations being carried outat weekly intervals. The food is easilydigested and of small residue with a caloricvalue of the order of 3,500 in 24 hours. Thediet should contain creamed soups, creamedvegetables, chicken, mutton, beef, sweet-breads, liver, cereals, cheese and an adequateamount of sugar.
Care of the bowels. In the absence ofobstructive symptoms a good bowel actionshould be achieved daily, the patient beinggiven plenty of fluid and a daily dose of one-half ounce of liquid paraffin. If obstructivesymptoms are present salines are of value, andwhen faecal stasis occurs above a neoplasmenemata are required for relief. When thefaecal mass is hard and dry, disintegration maybe effected by an enema of hydrogen peroxide(strength 25 per cent.). If there is a tendencyto form hard lumpy stools, or when diarrhoeaand an excessive discharge of mucous arepresent, irrigation Qf the bowel is of valueusing a lotion composed of potassium per-manganate (strength i in io,ooo) and lysol(strength i in 200).
The relief of pain. The amount of pain ex-perienced by these patients is variable and maybe extremely severe. When it is relativ lymild the weaker analgesics are used, such asaspirin, pyramidon and codeine. Later asthe pain worsens morphine in adequate dosesshould be given. If the pain is situated in thesacro-coccygeal region, prostate, urinarybladder or vagina, suppositories containingmorphine (gr. i) and belladonna (gr. i) areused. There are certain patients, however,who will not obtain sufficient relief from thesemeasures and more requires to be done. Twoadditional methods of treatment for the reliefof severe pain not controlled by analgesics aredescribed.
The intrathecal injection of alcohol. Theauthor has used this method of treatment in anumber of patients with some measure ofsuccess so that it is well worthy of a trial. Thetechnique is as follows :-the patient is placed
in the left lateral position and the fourthlumbar interspace is defined. An injection ofabsolute alcohol is given into the subarachnoidspace, the solution being injected drop by dropup to ten minims. The patient remains in thelett lateral position for a period of 20 minutes,and after this he is placed on his' back for twohours. After the' injection there may be mildmotor effects and diminution in the tendonreflexes or these may be lost; zones ofanaesthesia or hyperaesthesia may appear butall these effects are usually of a transitorynature and disappear after a few days at 'themost. There is no disturbance of bladder orbowel functions in the average case althoughretention of urine has been reported. If norelief from pain follows this injection, it isrepeated after the lapse of two weeks and onthis occasion the patient is placed in the rightlateral position. When relief from pain isachieved the benefit often lasts for a period ofsix months.
Cordotomy. In a small number of patientsthe pain is so severe and unrelieved by themethods of treatment described already thatthis operation is indicated. It is pointed outthat in the case of a mid-line structure such asthe rectum, it is necessary to section bothspino-thalamic tracts leaving one segment ofthe spinal cord between these levels. Theauthor has in mind one patient with an in-operable carcinoma of the rectum ca2singvery severe pain unrelieved by all othermethods, for whom he performed this opera-tion, the spino-thalamic tracts being sectionedat the levels of D.4 and D.6 with completerelief from pain. After this operation everyattention must be given to the prevention ofpressure sores.
Insomnia. This may be a distressingsymptom, not necessarily' caused by thepresence of pain. When this is the case variousremedies are tried including allonal, medinal,luminal or bromides.
Secondary anaemia. There are severalfactors which contribute to the progressivesecondary anaemia which is present in thesepatients. Iron and vitamin therapy is in-stituted and in certain patients a blood trans-fusion is helpful.
Apart from the general management of thepatient thus outlined there are three operations
)Ianuary, 1947 37copyright.
on July 27, 2021 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.23.255.17 on 1 January 1947. D
ownloaded from

38 POST-GRADUATE MEDICAL JOURNAL January, 1947
of definite palliative value which are nowdescribed.Palliative Radical Excision of the RectumThere is a group of patients with carcinoma
of the rectum giving rise to. hepatic metastases,but the local lesion can be removed. Theargument is advanced that by removing therectum the patient is made more comfortablein that a bleeding, discharging, ulceratingneoplasm is no longer present and the possi-bility of further local complications developingis obviated. Thus it is justifiable to performa palliative radical excision of the rectum inthese cases providing it is judged that thepatient is fit enough for the operation andpossesses a reasonable period of expectation oflife. The patients must be chosen carefullyand in' some the final decision will be made atexploratory laparotomy. By this means agreat deal of suffering will be ameliorated.ColostomyThis is a valuable method of treatment in
advanced carcinoma of the rectum for severalreasons. Relief is afforded those patients whohave developed various degrees of intestinalobstruction or when fistulae-recto-vesical,recto-vaginal or vesico-colic-have occurred.If colostomy is performed many distressinglocal complications will bv averted, especiallyof an inflammatory nature. Further, it isfound: there is often a temporary improvementin the patient's general health, for more sleepis obtained, an increased diet is taken and abetter evacuation of the bowel is achieved.The question must be answered concerning thetime at which colostomy should'be performed,and it is laid down that when a carcinoma ofthe rectum is considered to be inoperable, thesooner colostomy is carried 'out the better.The words of Miles should be remembered
when he said, 'from what I have seen of thesecases I am convinced that, as soon as car-cinoma of the rectum is found to be in-operable, every day lost before resorting tocolostomy is a day to the bad.' With modemmanagement, a colostomy is no longer anintolerable burden for the patient to carry, andhe is given full instructions concerning thesubject before leaving hospital.Diathermy of the carcinoma. A very dis-
tressing svmptom seen frequently in patientswith advanced carcinoma of the rectum isexcessive discharge of blood and mucous. Itis found that destruction of the projecting,fungating portion of the neoplasm is a valuablemethod of palliation in these cases. Theoperation is performed through a sigmoido-scope and the object of the procedure is totransform a large fungating growth into a flatulcer. If the symptoms recur at a later datethe operation can be repeated.
Irradiation treatment. Over a period of a,number of years investigations cor.cerning thevalue of irradiation treatment in carcinoma ofthe rectum have been carried out. Severalmethods of treatment have been, tried includingirradiation by means of radon seeds, radiumneedles and high voltage X-irradiation. Theresults achieved in columnar celled adeno-carcinoma of the rectum ;have been dis-appointing.
I wish to record my thanks to Dr.Woodhouse Price, Pathologist to the RoyalCancer Hospital for help with the illustrations.'
REFERPNCESi. DUKES, CUTHBERT E. (I940), Cancer of the Rectum, An
Analysis of x,o0o cases, Jour. Path. and Bact., 5o, No. 3, 527.2. RAVEN, RONALD W. (1939), Early Carcinoma of the Rectum,
Proc. Roy. Soc. Med., 32, 907.3. GABRIEL, W. B., The Principles and Practice of Rectal
Surgery, London, p. 263.4. NORBIURY, L. E. C. (1930-3I), Multiple Primary Malignant
Growths, with Special Reference to the Colon and Rectum,Proc. Roy. .Soc. Med., 24, Pt. I, 198.
5. MILES, W. ERNEST (1939), Rectal Surgery, London, p. 244.
A Clinic for the diagnosis and treatment of Internal Diseases (except Mental or Infectious Diseases). TheClinic is provided with a staff of doctors, technicians and nurses.
The surroundings are beautiful. The climate is mild. There is central heating throughout. The annualrainfall is 30.5 inches, that is, less than the average for England.
The Fees are inclusive and vary according to the room occupied.
For particulars apply to THE SECRETARY, Ruthin Castle, North Wales.Telegrams: Castle, Ruthin. Telephone: Ruthin 66.
copyright. on July 27, 2021 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.23.255.17 on 1 January 1947. Dow
nloaded from