Cancer of nasopharynx in young patients
5
Journal of Surgical Oncology 27:181-185 (1984) Cancer of Nasopharynx in Young Patients PEDRO MORALES, MD, ANTONIO BOSCH, MD, SANTIAGO SALAVERRY, MD, From the Department of Radiotherapy, Gonzalez Martinez Oncologic Hospital, San Juan (P.M., A.B.), Cancer Control Program, Puerto Rico Department of Health, San Juan (I.M.), and the Department of Radiotherapy, Ponce Oncologic Hospital, Ponce, Puerto Rico (S.S., J.N.C.) JOSE N. CORREA, MD, AND ISIDRO MARTI'NEZ, MD - From 1961 to 1980 17 patients with nasopharyngeal carcinoma who were less than 30 years old at time of diagnosis were treated at the two oncologic hospitals in Puerto Rico. Fourteen of the tumors were lymphoepitheliomas and the remaining three were anaplastic carcinomas. Ninety-four percent of the patients were found to have neck adenopathy at the initial examina- tion and in 65 % of them the adenopathy was bilateral. The 5-year actuarial survival was 14. The main cause of failure was the distant metastasis. Seventy-one percent of our patients developed distant metastasis sometime during the course of their disease. Carcinoma of the nasopharynx is uncommon in Puerto Rico as in other western countries. The post-adolescent age incidence peak reported from different countries is also present among Puerto Ricans. -~ -- KEY WORDS: nasopharyngeal carcinoma; radiation therapy INTRODUCTIQN Carcinoma of the nasopharynx is a relatively rare tu- mor except for certain areas of Southeast Asia. A post- adolescent age incidence peak has been reported [l-51 from different countries, but no such age peak has been described in Chinese populations [6,7]. Although some reports suggest a more favorable prognosis in the young patient [8-151, this is not the case in others [16-181. The incidence of cancer of the nasopharynx in Puerto Rico is 0.5 (in 100,OOO) [19]. Figure 1 shows a distribu- tion by age of Puerto Rican patients with microscopically confirmed carcinoma of the nasopharynx during the pe- riod 1960-1980. This bimodal age curve reveals: l) no patient under the age of 10; 2) a small peak between 10 and 30 years; 3) a large peak between 50 and 70 years. There were 155 males and 70 females, a ratio of 2.2:l. There were 26 patients under the age of 30; 14 males and 12 females, a ratio of 1.2:l. In this paper we will report the experience of the two oncologic hospitals in Puerto Rico in treating this disease in the young patient. MATERIALS AND METHODS From 1961 to 1980 inclusive, 17 patients with naso- pharyngeal carcinoma who were less than 30 years old at diagnosis were sequentially registered and treated at the 0 1984 Alan H. Liss, Inc. 70 - 60 - v) + 50- z Y - 40- a U 0 30- 0 z 20 - 10- CARCINOMA OF THE NASOPHARYNX AGE Fig. 1. Distribution of patients by age. Carcinoma of the nasopharynx in Puerto Rico, 1960-1980. Accepted for publication January 6, 1984. Address reprint requests to Pedro Morales, MD, Oncologic Hospital, P.O. Box 1811, Hato Rey, Puerto Rico 00919.
-
Upload
pedro-morales -
Category
Documents
-
view
215 -
download
0
Transcript of Cancer of nasopharynx in young patients

Journal of Surgical Oncology 27:181-185 (1984)
Cancer of Nasopharynx in Young Patients
PEDRO MORALES, MD, ANTONIO BOSCH, MD, SANTIAGO SALAVERRY, MD,
From the Department of Radiotherapy, Gonzalez Martinez Oncologic Hospital, San Juan (P.M., A.B.), Cancer Control Program, Puerto Rico Department of Health, San Juan (I.M.),
and the Department of Radiotherapy, Ponce Oncologic Hospital, Ponce, Puerto Rico (S.S., J.N.C.)
JOSE N. CORREA, MD, AND ISIDRO MARTI'NEZ, MD
--
From 1961 to 1980 17 patients with nasopharyngeal carcinoma who were less than 30 years old at time of diagnosis were treated at the two oncologic hospitals in Puerto Rico. Fourteen of the tumors were lymphoepitheliomas and the remaining three were anaplastic carcinomas. Ninety-four percent of the patients were found to have neck adenopathy at the initial examina- tion and in 65 % of them the adenopathy was bilateral. The 5-year actuarial survival was 14. The main cause of failure was the distant metastasis. Seventy-one percent of our patients developed distant metastasis sometime during the course of their disease.
Carcinoma of the nasopharynx is uncommon in Puerto Rico as in other western countries. The post-adolescent age incidence peak reported from different countries is also present among Puerto Ricans.
-~ -- KEY WORDS: nasopharyngeal carcinoma; radiation therapy
INTRODUCTIQN Carcinoma of the nasopharynx is a relatively rare tu-
mor except for certain areas of Southeast Asia. A post- adolescent age incidence peak has been reported [l-51 from different countries, but no such age peak has been described in Chinese populations [6,7]. Although some reports suggest a more favorable prognosis in the young patient [8-151, this is not the case in others [16-181.
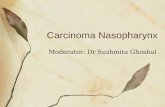
The incidence of cancer of the nasopharynx in Puerto Rico is 0.5 (in 100,OOO) [19]. Figure 1 shows a distribu- tion by age of Puerto Rican patients with microscopically confirmed carcinoma of the nasopharynx during the pe- riod 1960-1980. This bimodal age curve reveals: l ) no patient under the age of 10; 2) a small peak between 10 and 30 years; 3) a large peak between 50 and 70 years. There were 155 males and 70 females, a ratio of 2.2:l. There were 26 patients under the age of 30; 14 males and 12 females, a ratio of 1.2:l.
In this paper we will report the experience of the two oncologic hospitals in Puerto Rico in treating this disease in the young patient.
MATERIALS AND METHODS From 1961 to 1980 inclusive, 17 patients with naso-
pharyngeal carcinoma who were less than 30 years old at diagnosis were sequentially registered and treated at the
0 1984 Alan H. Liss, Inc.
70 -
60 -
v) + 5 0 - z Y -
40- a U 0 30-
0 z 20 -
10-
C A R C I N O M A O F T H E N A S O P H A R Y N X
A G E
Fig. 1. Distribution of patients by age.
Carcinoma of the nasopharynx in Puerto Rico, 1960-1980.
Accepted for publication January 6, 1984. Address reprint requests to Pedro Morales, MD, Oncologic Hospital, P.O. Box 1811, Hato Rey, Puerto Rico 00919.

182 Modes et a1
TABLE I. TNM Classification for Nasopharyngeal Carcinoma ( N C )
Primary tumor (T): TX To Tls Carcinoma in situ. T ,
T2
T, T4
Tumor that cannot be assessed. No evidence of primary tumor.
Tumor confined to one site of nasopharynx or no tumor visible (positive biopsy only). Tumor involving two sites (both posterosuperior and lateral walls). Extension of tumor into nasal cavity or oropharynx. Tumor invasion of skull or cranial nerve involvement, or both.
Nodal involvement (N) NX Nodes cannot be assessed. No No clinically positive node. N ,
N,
Single clinically positive homolateral node 3 cm or less in diameter. Single clinically positive homolateral node more than 3 cm but not more than 6 cm in diameter or multiple clinically positive homolateral nodes, none more than 6 cm in diameter. Single clinically positive homolateral node more than 3 cm but not more than 6 cm in diameter. Multiple clinically positive homolateral nodes, none more than 6 cm in diameter. Massive homolateral node(s), bilateral nodes, or contralateral node(s). Clinically positive homolateral node(s). one more than 6 cm in diameter. Bilateral clinically positive nodes (in this situation, each side of the neck should be staged separately; that is. N3B: right, N2a: left, Nl). Contralateral clinically positive node(s) only.
N z ,
NZb
N3
N,,
N3b
N3c Distant Metastasis (M)
NX Not assessed. Mo No (known) distant metastasis. M I Distant metastasis present.
Oncologic Hospital I. Gonzalez Martinez in San Juan and Clinica Oncol6gica Andres Grillasca in Ponce, Puerto Rico. They constitute the primary base of this report.
The anatomical extent of disease at diagnosis was staged retrospectively according to the TNM System of the American Joint Committee (Table I). Clinical data for the 17 patients is summarized in Table 11.
Presenting Symptoms The initial presentation was manifested in ten patients
by cervical adenopathy. In five instances the original complaint was nasal obstruction or nasal bleeding. One patient presented with cough and chest pain as the first symptoms. In one patient the presenting symptoms were not recorded.
Histopathology All 17 patients had biopsy proven carcinoma. Ten pa-
tients had biopsy of the nasopharynx and the neck aden-
opathy. Six patients had a biopsy of the nasopharynx only and in one patient only the neck adenopathy was biop- sied. Pathology was reported as lymphoepithelioma in 14 patients. In the remaining three patients the pathology was read as anaplastic carcinoma.
Staging The distribution of cases according to extent of the
primary tumor was as follows (Table In): T1-two pa- tients; T2-seven patients; T3-seven patients, and T4- one patient. Sixteen (94%) patients were found to have clinically positive regional adenopathy at the initial ex- amination. In 11 (65%) patients the adenopathy was bi- lateral. Two patients presented with lung metastasis at diagnosis.
The resulting stage distribution was stage 11-one pa- tient; stage 111-one patient; and stage IV-15 patients (Table IV).
Treatment External irradiation as primary treatment with curative
intent was planned in 15 patients and completed in 14 patients because patient no. 13 developed liver metastasis while receiving irradiation. In the remaining two patients treatment was carried out only as palliation, and patient no. 8 received chemotherapy only. Patient no. 10 was irradiated palliatively.
Megavoltage irradiation was used in all the irradiated patients. The primary fields were the lateral portals from the base of the skull to the supracalvicular fossae. Their sizes depended on the length of the patient’s neck: they were usually 8 to 12 cm wide and 15 to 18 cm long. Only patient no. 11 did not receive irradiation to the lower neck.
The lateral portals were the only fields used in patients treated at the Hospital Oncol6gico in San Juan (patient nos. 1 to 11 inclusive). Patient no. 7 received 3,000 rad at 0.75 cm from mucosal surface as boost treatment using intracavitary radium. Intracavitary radium was planned but not done in patient No. 3 because he developed distant metastasis at the completion of the external irradiation.
An anterior facial and one anterior neck field to boost the primary tumor and to boost the neck respectively, were added to the lateral portal when the dose to the nasopharynx approached 4,500-5,OOO rad in the patients treated at the Clinica Oncologica in Ponce (patients nos. 12 to 17 inclusive). All patients treated at the Hospital Oncol6gico received a continuous course of irradiation with five fractions per week. Five of the patients treated at the Clinica Oncol6gica received split-course irradia- tion and two of them received only 4 fractions per week. Patient No. 16 was treated over a period of 102 days because she did not keep the planned appointments.

Cancer of Nasopharynx in Young Patients 183
TABLE 11. Carcinoma of the Nasopharynx, Summary of Patient Data
Site and time oE appearance of
metastasis
Bone, brain, retroperitoneum,
mediastinum--13 m None
Bone, nodes, bone marrow-2 in
None Pleura, bone mediastinuni,
scv nodes-26 m None
Bone, adrenal, liver, nodes,
retroperitoneum, niediastinum-8 m
Sub- sequent
treatment
XRT*
Pt . No.
1
- Age at DX .
12
Sex
F __ Primaryb
U 13m
Neckb
U 16m
Outcome'
DWD 31 m
Neck
5,700120140
Primary
5.700120140
Stage
T3N3BM0
2 3
16 17
F M
LE LIE
6,000130140 5,500127151
6,000130140 5,250125149
U 4 m U 4 m
C U 4 m
None Chemo.
DWD 8 m DWD 7 m
19 19
M M
LE LE
6,000142163 7.000140156
6,000142163 7,000139160
U 22 m C
C C
Chemo. XRT
Chemo.
DWD 30 m DWM 32 m
4 5
6 7
19 20
F F
LE LE
6,600133147 6,ooO/21/47 f 3,000
with intracavitary
radiation
6.680136153 3,0001 6/12 6,00012 1147 5,70001311
60 3,4201 19/28 6,400132165 6,5001261102
-
5,000125136 6.00012 1 I4 I
C C
C U 11 in
None XRT
Chemo.
NED 63 m DWD 16 ni
8 9 10 11 12
21 22 27 29 15
F M F F F
AN LE AN LE L.E
U I m C
U l m C C
U I m C
U I m C C
Lung Bone, scalp-4 m
Lung None
Lung-43 ni
Liver-1 in None
Bone-4 m
DWD 3 m DWM 15 m DWD 3 m NED 161
DWM 43 in
-
6,680136153 3,0001 6/12 6,00012 1 147 5,900132161
XRT None None None
3,420119128 6,400132165 6,5001261
102 6,520128150 5.850126165
DWD l m NED 28 m DWD 13 m
13 14 15
18 19 19
M M M
L,E LE LE
U l m C
U 2 m
U I m C
U 2111
None None
Chemo.
16 17
22 28
F M
L.E AN
6,520128150 5.850126165
C U 3 m
C U 3 m
Lung-43 in
Lung, bone-3 m DWM 43 m DWD 16 m
None XRT
Chemo.
"LE, lymphoepit helioma; AN, anaplastic carcinoma. hU, uncontrolled; C. controlled; m, months. 'NED, no evidence of disease; DWD, dead with disease; DWM. dead with metastasis. dXRT. X-ray therapy.
TABLE 111. Carcinoma of the Nasopharynx, TNM Distribution of Cases
TABLE IV. Carcinoma of the Nasopharynx, Distribution of Cases by Staging
Number of cases
NO Nl N2 N3 Total
2
7 7
- 2 - - TI Tz 1 1 1 4" 7" T3 T4
- - -
I" Total -- 1 2" 3 119 17a
"Distant metastasis.
- - la -
Staee
Stage I (TINo) Stage I1 (T2No) Stage 111 (T3No or T1,2,3NI) Stage IV (T4 or N2 or N3 of MI) Total
0 1 1
15 17
RESULTS than 3,500 rad because of the presence of distant metas- tasis (patient nos. 8, 10, 13). There is good correlation between the TN classification and the locoregional con- trol. The control rate for primary tumor was 100% for TI; 80% for TZ; and 29% for T3.
In summary, 12 (71 %) of the 17 patients in this series developed distant metastasis before, at, or after the treat- ment. Of the remaining five patients, three are NED at
The overall 5-year actuarial survival was 14 (Fig. 2). The 5-year acutarial survival was 16 if only the 15 pa- tients who were Mo at the initial presentation are considered.
Table V shows the loco-regional control. Excluded from the analysis are the three patients who received less

184 Moraleset al
C A R C I N O M A O F T H E N A S O P H A R Y N X
A C T U A R I A L S U R V I V A L
T O T I L NO. O F P A T I E N T S . I 7
0 I 2 3 4 5 Y E A R S 12 24 36 40 60 M O N T H S
Fig. 2. Carcinoma of the nasopharynx. actuarial survival.
TABLE V. Carcinoma of the Nasopharynx, Locoregional Control
Extent of Both Only Only Neither disease T + N T N T o r N Total
2
I
- - - TIN2 2
T2No I - - -
T3N3 1 1 2 3 7
7 (50%) I 2 4(28%) 14
26, 63, and 161 months, while two died with the primary tumor uncontrolled.
DISCUSSION Carcinoma of the nasopharynx is rare in Puerto Rico.
This is in contrast with the high incidence of carcinoma of the tongue, tonsil, and hypopharynx. When comparing the age-adjusted (1970 standard) cancer incidence rates of all Surveillance, Epidemiology, and End Results (SEER) areas except Puerto Rico with those of Puerto Rico, Puerto Rican people show incidence ratios of 2 or greater for cancer of the tongue, tonsil, and hypophar- ynx. However. the incidence ratio for carcinoma of the nasopharynx is 0.8. The post-adolescent peak in the age distribution curve reported by others [ 1-51 is also present among Puerto Ricans with nasopharyngeal carcinoma.
TABLE VI. Carcinoma of Nasopharynx in Young, Results Taken from Medical Literature
5 Y' actuarial
No. of survival patients Age ( % )
Berry et a1 [ 81 25 30 70
Fernandez et al [ 1 I ] 10 15 70
Castro et al [ 131 27 20 64
Princess Margaret Hospaai
M.D. Anderson Hospital
Emory University, Atlanta, and other institutions
Commonwealth University of Virginia
Istituto Nazionale, Milan
Children Cancer Study Group
University of Athens
National Taiwan University Hospital
University of Pittsburgh
Memorial Sloan-Kettering Cancer Center
Pick et a1 [12] 9 18 58
Lombardi et al [ 151 20 15 55
Jenkin et al [ 101 119 30 51
Papavasiliou et al [9] 26 30 50
Shu-Chen [14] 119 30 45a
Deutsch et al [16] 7 18 19
Jereb et a1 [ 17) 16 17 14
Present series 17 30 14 Bohorquez [ 181 29 30 10"
Roval Marsden HosDital. London
aCrude survival.
All the tumors were lymphoepitheliomas or undiffer- entiated carcinomas which is in agreement with other studies [2, 7-91. Cervical nodal metastases were present in 94% of our patients. Eighty-eight percent of cases were stage IV at the initial presentation.
Table VI shows the results of the treatment of carci- noma of the nasopharynx in young patients taken from the medical literature. While most of the reports [8-151 suggest a more favorable prognosis in the young patient, other experiences [ 16-18], including ours, are disap- pointing. However, it is important to take into account the fact that the main cause of failure in our series was not the loco-regional disease, but the distant disease. Seventy-one percent of our patients developed distant metastasis.
REFERENCES Bala Krishnan V: An additional younger-age peak for cancer of the nasopharynx. Int J Cancer 15:651-657, 1975. Cammoun M, Hoerner Vogt G. Mourali W: Tumours of the nasopharynx in Tunisia. Cancer 33: 184-192, 1974. Greene MH, Fraumeni Jr. JF. Hoover R: Nasopharyngeal cancer among young people in the United States: Racial variations by cell type. J Natl Cancer lnst 58: 1267-1270. 1977. Kar-Kedar I, Chatchik S. Hercberg A: Nasopharyngeal carci-

Cancer of Nasopharynx in Young Patients 185
12. Pick T, Maurer HM, and McWilliams NB: Lymphoepithelioma in childhood. J Pediatr 84:96-100, 1974.
13. Castro-Vita H, Mendiondo OA, Shaw DL, Jelden G, Reiie JB, Frias Z, and Someren A: Nasopharyngeal carcinoma in the sec- ond decade of life. Radiology 148:253-256, 1983.
14. Shu-Chen H: Nasopharyngeal cancer: A review of 1605 patients treated radically with cobaltm. Int J Radiat Oncol Biol Phys
15. Lombardi F, Gasparini M, Gianni C, De Mari M, Molinari R, Pilotti S: Nasopharyngeal carcinoma in childhood. Med Pediatr Oncol 10:243-250, 1982.
16. Deutsch M, Mercado Jr. R, Parsons JA: Cancer of the nasophar ynx in children. Cancer 41:1128-1133, 1978.
17. Bohorquez J: Factors that modify the radio-response of cancer of the nasopharynx. Am. J. Roentgenol., Rad. Therapy & Nuclear Med. 126:863-875, 1976.
18. Jereb B, Huvos AG, Steinherz P, Unal A: Nasopharyngeal car- cinoma in children. Review of 16 cases. Int J Radiat Oncol Biol
19. Surveillance, Epidemiology, and End Results: Incidence and
6 :40 1-407, 1980.
Phys 6~487-491, 1980.
mortality data, 1973-1977. Natl Cancer Inst Monograph #57.
noma at the Tel-Hashomer Government Hospital, Israel. A 20 year survey (1951-1970). Clin Radio1 25:403-407, 1974.
5. Waterhourse 3: Cancer Handbook of Epidemiology and Prog- nosis. Edinburg: Churchill Livingstone, 1974.
6 . Lin TM, Chm KP, Lin CC. Hsu MM, Tu SM, Chang TC, Jung PF, Hirayama T: Retrospective study on nasopharyngeal carci- noma. J Natl Cancer Inst 51:1403-1408, 1973.
7. Ho JHC: An epidemiologic and clinical study of nasopharyngeal carcinoma. Int J Radiat Oncol Biol Phys 4:183-198, 1978.
8. Berry MP, !Smith ChR, Brown TC, Jenkin RDT. Rider WD: Nasopharyngeal carcinoma in the young. Int J Radiat Oncol Biol
9. Papavisiliou C, Paulatou M, Pappas J: Nasopharyngeal cancer in patients under the age of thirty years. Cancer 40:2312-2316, 1977.
10. Jenkin RDT, Anderson JR, Jereb B, Thompson JC, F'yesmany A, Wara WM, Hammond D: Nasopharyngeal carcinoma-A retro- spective review of patients less than thirty years of age: A report from Childrens Cancer Study Group. Cancer 47: 360-366, 1981.
11. Fernhdez CH, Cangir A, Samaan NA, and Rivera R: Nasophar- yngeal carcinoma in children. Cancer 37:2787-2791, 1976.
Phys 6:415-421, 1980.