Cancer Medicine Prices - WHO | World Health...
8
Cancer Medicine Prices IN LOW- AND MIDDLE- INCOME COUNTRIES
Transcript of Cancer Medicine Prices - WHO | World Health...

Cancer Medicine PricesIN LOW- AND MIDDLE- INCOME COUNTRIES
Global Task Force on Expanded Access to Cancer Care and Controlin Developing Countries (GTF.CCC)
Harvard Global Equity Initiative, Secretariat651 Huntington Avenue
FXB Building, Room 632Boston, MA 02115
gtfccc.harvard.edu [email protected]
About Management Sciences for Health Management Sciences for Health (MSH) is a global nonprofit health organization, using proven approaches developed over four decades to help leaders, health managers, and communities in developing nations build stronger health systems for greater health impact. We work to save lives by closing the gap between knowledge and action in public health Most of the leading causes of death and disability in developing countries can be prevented or treated with cost-effective medicines. Despite this fact, hundreds of millions of people do not have access to these medicines. Improving the way medicines are accessed and used is a powerful opportunity to create stronger health systems and achieve greater health impact. Management Sciences for Health’s Center for Pharmaceutical Management develops the capacity of both the public and private sectors to select, procure, and distribute quality medicines and health supplies and helps to ensure their proper dispensing and use–all in a cost-effective way.
About The Global Task Force on Expanded Accessto Cancer Care and Control in Developing Countries
The mandate of The Global Task Force on Expanded Access to Cancer Care and Control in Developing Countries (GTF.CCC) is to design, implement and evaluate innovative, multi-stakeholder strategies for expanding access to cancer prevention, detection and care. Through local partners, the GTF.CCC supports implementation of innovative service in delivery models that can provide evidence for scaling up access to cancer care and control, and strengthening health systems in developing countries.

Cancer Medicine Prices in Low- and MiddLe-inCoMe Countries

Rising BuRden of CanCeR and TReaTmenT needs
According to the World Health Organization (WHO), cancer is one of the leading causes of death worldwide; in 2008, it accounted for approximately 7.6 million deaths (13 percent of all causes of death).1 More than 70 percent of all cancer deaths occurred in low- and middle-income countries (LMICs). While it is estimated that more than 30 percent of deaths can be prevented through early detection and modifying or avoiding key risk factors, the demand for cancer treatment, especially in low-income countries, is not being adequately met. High cost and poor availability of cancer treatment are significant barriers to access in many LMICs. In Pakistan, which has a per capita income of 2,860 US dollars (USD), the cost of treating leukemia with chemotherapy and associated transfusion requirements is USD 20,000.2 Although the cost of medicines for palliative care at the supplier level does not represent a substantial barrier to access, retail prices can be a major deterrent to access as they can be prohibitive.3
Ensuring affordable access to quality cancer medicines, vaccines, and related health techno-logies depends not only on wise selection by national authorities, but also on price reduction and procurement strategies appropriate to each type of product. If essential medicines for cancer are listed in a country’s national essential medicines list (NEML) and linked to standard treatment guidelines, selection and procurement become easier and can contribute to lower prices. For example, antihypertensive medicines are cheaper in the public sector when listed in an NEML.4
Procurement officers often do not have easy access to available pricing information to make the best purchase decisions for public health programs. Transparent, web-based exchange of information on prices and sources of cancer medicines and vaccines should be expanded. Such information can achieve dramatic price reductions –especially on off-patent products– when used in competitively pooled procurement by reliable global, regional, or national procurement and supply organizations. For example, price information transparency for antiretrovirals through initiatives by Médecins Sans Frontières and WHO’s Global Price Reporting Mechanism contribute to informed purchasing decisions for HIV/AIDS programs. Likewise, the Global Fund to Fight AIDS, Tuberculosis and Malaria (Global Fund) requires that principal recipients submit prices paid for a range of procured medicines for AIDS, tuberculosis, and malaria that are then publicly posted through its Price and Quality Reporting System with country and region specific analyses.
WoRld maRkeT PRiCes of essenTial CanCeR mediCines and agenTs
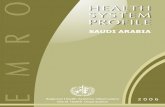
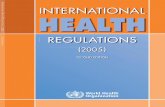
The table below lists antineoplastic, immunosuppressives, and medicines used in palliative care sourced from the WHO’s 17th edition of Model Essential Medicines List. Also listed are several chemotherapeutic agents deemed essential based on recommendations in the essential package of cancer services from the Global Task Force on Expanded Access to Cancer Care and Control in Developing Countries’ report, “Closing the Cancer Divide: The Global Equity Imperative of Expanding Access in Low and Middle Income Countries” (http://gtfccc.harvard.edu/icb/icb.do).
The pricing information for these chemotherapeutic agents is from the 2010 edition of the International Drug Price Indicator Guide (http://erc.msh.org/priceguide) published by Mana-gement Sciences for Health (MSH) and WHO. Pricing data are indicative of buyer prices – usually government agency international competitive bidding, or tender, prices from public sector sources. All prices from the MSH Drug Price Indicator Guide are from reputable suppliers who meet quality standards established by MSH and WHO.5
1

Ind
icat
ive
pric
es o
f es
sent
ial
canc
er m
edic
ines
and
age
nts
use
d i
n p
alli
ativ
e ca
re
from
the
MSH
-WH
O I
nter
nat
ion
al D
rug
Pri
ce I
ndic
ator
Gu
ide
dru
g (i
nte
rnat
ion
al
non
pro
pri
etar
y n
ames
)
MsH
dru
g P
rice
in
dic
ator
Gu
ide
- 201
0 e
dit
ion
stre
ngt
hd
osa
ge f
orm
un
it p
rice
Low
est
(us$
)M
edia
n
(us$
)H
igh
est
(us$
)n
o. o
f p
rice
sH
igh
/Low
r
atio
IMM
UN
OSU
PP
RE
SIV
E M
ED
ICIN
ES
Aza
thio
pri
ne
50
mg
tab-
cap
per
tab
0.09
0.15
0.25
5 2
.83
Cic
losp
orin
25 m
gta
b-ca
pp
er t
ab0.
450.
480.
973
2.17
CY
TO
TO
XIC
AN
D A
DJU
VA
NT
ME
DIC
INE
S
All
opu
rin
ol10
0 m
gta
b-ca
pp
er t
ab0.
020.
020.
064
3.5
Asp
arag
inas
e10
,00
0 IU
/ml
1 vi
al (
1 m
l)p
er v
ial
43.1
563
.73
84.3
22
1.95
Ble
omyc
in15
mg
vial
per
via
l12
.16
15.6
646
.75
93.
84
Cal
ciu
m F
olin
ate
15 m
g ta
b-ca
pp
er t
ab0.
211.
44
2.07
49.
7
Car
bopl
atin
150
mg
vial
per
via
l13
.09
14.0
618
.04
41.
39
Ch
lora
mbu
cil
2 m
gta
b-ca
pp
er t
ab0.
460.
962.
065
4.47
Cyc
loph
osph
amid
e50
0 m
g1
vial
per
via
l3.
686.
719.
904
2.69
50 m
gta
b-ca
pp
er t
ab0.
200.
220.
465
2.23
Cyt
arab
ine
100
mg
vial
per
via
l1.
753.
633.
834
2.19
Dac
tin
omyc
in0.
5 m
g1
vial
per
via
l11
.00
24.6
027
.68
32.
52
Dau
nor
ubi
cin
20 m
g1
vial
per
via
l5.
846.
00
92.0
53
15.7
7
Doc
etax
el80
mg
1 vi
alp
er v
ial
4211
3.51
346.
164
8.24
Dox
oru
bici
n50
mg
1 vi
alp
er v
ial
8.89
12.4
517
.93
62.
02
Eto
pos
ide
20 m
g/m
lvi
alp
er v
ial
0.49
0.84
1.48
63
Flu
orou
raci
l50
mg/
ml
vial
per
ml
0.17
0.19
0.22
31.
34
Hyd
rox
ycar
bam
ide
500
mg
tab-
cap
per
tab
0.08
0.31
0.50
46.
07
Ifos
fam
ide
1 gm
vial
per
via
l10
.36
14.7
446
.86
44.
52
Mer
cap
top
uri
ne
50 m
gta
b-ca
pp
er t
ab0.
581.
832.
744
4.69
Mes
na
100
mg/
ml
Am
pou
le (4
ml)
per
ml
0.37
0.72
1.08
22.
93
Met
hot
rexa
te25
mg/
ml
vial
per
ml
0.55
1.03
1.33
42.
41
2.5
mg
Tab-
cap
per
tab
0.05
0.10
0.15
63.
11
Pac
lita
xel
6 m
g/m
l1
vial
per
ml
1.88
2.61
8.48
54.
51
Th
iogu
anin
e40
mg
tab-
cap
per
tab
3.92
4.62
5.32
21.
36
Vin
blas
tin
e10
mg
1 vi
alp
er v
ial
7.94
14.7
517
.14
52.
16
Vin
cris
tin
e1
mg
1 vi
alp
er v
ial
1.09
2.33
2.69
42.
46
AD
DIT
ION
AL
ESS
EN
TIA
L A
GE
NT
S
An
astr
ozol
e1
mg
Tab-
cap
p
er t
ab0.
471.
012.
264
4.79
Cis
plat
in
1 m
g/m
lvi
alp
er m
l0.
160.
200.
252
1.6
Mel
phal
an2
mg
tab-
cap
per
tab
0.90
1.41
2.0
03
2.23
Rit
uxi
mab
10 m
g/m
lA
mp
oule
per
ml
35.6
341
.35
47.0
82
1.32
HO
RM
ON
ES
AN
D A
NT
I-H
OR
MO
NE
S
Dex
amet
has
one
4 m
g/m
lA
mp
oule
(1
ml)
per
ml
0.02
0.13
0.4
48
22.0
1
Hyd
roco
rtis
one
100
mg
vial
per
via
l0.
180.
291.
719
9.35
Met
hyl
pre
dn
isol
one
40 m
g/m
lvi
alp
er v
ial
1.65
2.47
3.30
22.
01
Pre
dn
isol
one
5 m
g/5
ml
oral
liqu
idp
er m
l0.
020.
050.
073
2.68
5 m
gta
b-ca
pp
er t
ab0.
005
0.01
0.08
916
.88
Tam
oxif
en20
mg
tab-
cap
per
tab
0.01
0.09
0.20
622
.67
ME
DIC
INE
S U
SED
IN
PA
LL
IAT
IVE
CA
RE
Am
itri
pty
lin
e10
mg
tab-
cap
per
tab
0.01
0.01
0.02
31.
9
25 m
gta
b-ca
pp
er t
ab0.
00
40.
010.
067
15.1
3
Dia
zep
am5
mg/
ml
vial
per
ml
0.0
40.
080.
258
6.77
10 m
gta
b-ca
pp
er t
ab0.
010.
020.
353
24.5
1
Flu
oxet
ine
20 m
gta
b-ca
pp
er t
ab0.
010.
020.
04
72.
79
Ibup
rofe
n10
0 m
g/5
ml
oral
liqu
idp
er m
l0.
003
0.01
0.01
54
200
mg
tab-
cap
per
tab
0.0
030.
010.
015
3.21
Lac
tulo
se3.
35 g
/5 m
lor
al li
quid
per
ml
0.01
0.02
0.02
21.
71
Mid
azol
am5
mg/
ml
amp
oule
per
ml
0.17
0.23
1.32
77.
75
Mor
phin
e10
mg/
ml
amp
oule
per
ml
0.16
0.37
1.90
512
.11
30 m
gSR
tab
-cap
per
tab
0.62
0.97
3.66
45.
93
On
dan
setr
on2
mg/
ml
amp
oule
per
ml
0.11
0.26
1.65
415
.33
4 m
gta
b-ca
pp
er t
ab0.
020.
190.
953
51.1
2
2

Not
es:
1. P
rici
ng
dat
a n
ot a
vail
able
for
th
e fo
llow
ing
med
icin
es/a
gen
ts -
cycl
izin
e, d
ocu
sate
sod
ium
, hyo
scin
e h
ydro
brom
ide
and
sen
na.
2. O
nly
on
e p
rice
in
form
atio
n s
ourc
e w
as a
vail
able
for
dac
arb
azin
e, p
roca
rbaz
ine,
im
atin
ib a
nd
tra
stu
zum
ab -
so t
hes
e ar
e n
ot i
ncl
ud
ed i
n t
his
tab
le.
dru
g (i
nte
rnat
ion
al
non
pro
pri
etar
y n
ames
)
MsH
dru
g P
rice
in
dic
ator
Gu
ide
- 201
0 e
dit
ion
stre
ngt
hd
osa
ge f
orm
un
it p
rice
Low
est
(us$
)M
edia
n
(us$
)H
igh
est
(us$
)n
o. o
f p
rice
sH
igh
/Low
r
atio
IMM
UN
OSU
PP
RE
SIV
E M
ED
ICIN
ES
Aza
thio
pri
ne
50
mg
tab-
cap
per
tab
0.09
0.15
0.25
5 2
.83
Cic
losp
orin
25 m
gta
b-ca
pp
er t
ab0.
450.
480.
973
2.17
CY
TO
TO
XIC
AN
D A
DJU
VA
NT
ME
DIC
INE
S
All
opu
rin
ol10
0 m
gta
b-ca
pp
er t
ab0.
020.
020.
064
3.5
Asp
arag
inas
e10
,00
0 IU
/ml
1 vi
al (
1 m
l)p
er v
ial
43.1
563
.73
84.3
22
1.95
Ble
omyc
in15
mg
vial
per
via
l12
.16
15.6
646
.75
93.
84
Cal
ciu
m F
olin
ate
15 m
g ta
b-ca
pp
er t
ab0.
211.
44
2.07
49.
7
Car
bopl
atin
150
mg
vial
per
via
l13
.09
14.0
618
.04
41.
39
Ch
lora
mbu
cil
2 m
gta
b-ca
pp
er t
ab0.
460.
962.
065
4.47
Cyc
loph
osph
amid
e50
0 m
g1
vial
per
via
l3.
686.
719.
904
2.69
50 m
gta
b-ca
pp
er t
ab0.
200.
220.
465
2.23
Cyt
arab
ine
100
mg
vial
per
via
l1.
753.
633.
834
2.19
Dac
tin
omyc
in0.
5 m
g1
vial
per
via
l11
.00
24.6
027
.68
32.
52
Dau
nor
ubi
cin
20 m
g1
vial
per
via
l5.
846.
00
92.0
53
15.7
7
Doc
etax
el80
mg
1 vi
alp
er v
ial
4211
3.51
346.
164
8.24
Dox
oru
bici
n50
mg
1 vi
alp
er v
ial
8.89
12.4
517
.93
62.
02
Eto
pos
ide
20 m
g/m
lvi
alp
er v
ial
0.49
0.84
1.48
63
Flu
orou
raci
l50
mg/
ml
vial
per
ml
0.17
0.19
0.22
31.
34
Hyd
rox
ycar
bam
ide
500
mg
tab-
cap
per
tab
0.08
0.31
0.50
46.
07
Ifos
fam
ide
1 gm
vial
per
via
l10
.36
14.7
446
.86
44.
52
Mer
cap
top
uri
ne
50 m
gta
b-ca
pp
er t
ab0.
581.
832.
744
4.69
Mes
na
100
mg/
ml
Am
pou
le (4
ml)
per
ml
0.37
0.72
1.08
22.
93
Met
hot
rexa
te25
mg/
ml
vial
per
ml
0.55
1.03
1.33
42.
41
2.5
mg
Tab-
cap
per
tab
0.05
0.10
0.15
63.
11
Pac
lita
xel
6 m
g/m
l1
vial
per
ml
1.88
2.61
8.48
54.
51
Th
iogu
anin
e40
mg
tab-
cap
per
tab
3.92
4.62
5.32
21.
36
Vin
blas
tin
e10
mg
1 vi
alp
er v
ial
7.94
14.7
517
.14
52.
16
Vin
cris
tin
e1
mg
1 vi
alp
er v
ial
1.09
2.33
2.69
42.
46
AD
DIT
ION
AL
ESS
EN
TIA
L A
GE
NT
S
An
astr
ozol
e1
mg
Tab-
cap
p
er t
ab0.
471.
012.
264
4.79
Cis
plat
in
1 m
g/m
lvi
alp
er m
l0.
160.
200.
252
1.6
Mel
phal
an2
mg
tab-
cap
per
tab
0.90
1.41
2.0
03
2.23
Rit
uxi
mab
10 m
g/m
lA
mp
oule
per
ml
35.6
341
.35
47.0
82
1.32
HO
RM
ON
ES
AN
D A
NT
I-H
OR
MO
NE
S
Dex
amet
has
one
4 m
g/m
lA
mp
oule
(1
ml)
per
ml
0.02
0.13
0.4
48
22.0
1
Hyd
roco
rtis
one
100
mg
vial
per
via
l0.
180.
291.
719
9.35
Met
hyl
pre
dn
isol
one
40 m
g/m
lvi
alp
er v
ial
1.65
2.47
3.30
22.
01
Pre
dn
isol
one
5 m
g/5
ml
oral
liqu
idp
er m
l0.
020.
050.
073
2.68
5 m
gta
b-ca
pp
er t
ab0.
005
0.01
0.08
916
.88
Tam
oxif
en20
mg
tab-
cap
per
tab
0.01
0.09
0.20
622
.67
ME
DIC
INE
S U
SED
IN
PA
LL
IAT
IVE
CA
RE
Am
itri
pty
lin
e10
mg
tab-
cap
per
tab
0.01
0.01
0.02
31.
9
25 m
gta
b-ca
pp
er t
ab0.
00
40.
010.
067
15.1
3
Dia
zep
am5
mg/
ml
vial
per
ml
0.0
40.
080.
258
6.77
10 m
gta
b-ca
pp
er t
ab0.
010.
020.
353
24.5
1
Flu
oxet
ine
20 m
gta
b-ca
pp
er t
ab0.
010.
020.
04
72.
79
Ibup
rofe
n10
0 m
g/5
ml
oral
liqu
idp
er m
l0.
003
0.01
0.01
54
200
mg
tab-
cap
per
tab
0.0
030.
010.
015
3.21
Lac
tulo
se3.
35 g
/5 m
lor
al li
quid
per
ml
0.01
0.02
0.02
21.
71
Mid
azol
am5
mg/
ml
amp
oule
per
ml
0.17
0.23
1.32
77.
75
Mor
phin
e10
mg/
ml
amp
oule
per
ml
0.16
0.37
1.90
512
.11
30 m
gSR
tab
-cap
per
tab
0.62
0.97
3.66
45.
93
On
dan
setr
on2
mg/
ml
amp
oule
per
ml
0.11
0.26
1.65
415
.33
4 m
gta
b-ca
pp
er t
ab0.
020.
190.
953
51.1
2
3

All prices are expressed in unit cost such as per tablet or per millileter. The high/low ratio compares the highest unit price with the lowest. For example, a high/low ratio of 6 means that the highest unit price is six times greater than the lowest unit price. Of the 42 agents listed in the table, 10 medicines have extreme price variations (high/low ratio) of over 10. For example, the highest unit price for dexamethasone is 22 times the lowest price. Seven medicines have a high/low ratio of over 5 but below 10. A large high/low ratio can indicate an opportunity for cost savings. If buyer A can see he is paying eight times as much for the same product as buyer B, he can use that information to negotiate for a lower price or find another source from which to purchase.
The inTeRnaTional dRug PRiCe indiCaToR guide
The International Drug Price Indicator Guide provides what the name implies – an indication of medicine prices on the international market. The Guide has been published by MSH since 1986, and in collaboration with WHO since 2000. It provides a spectrum of prices from nonprofit drug suppliers and commercial procurement agencies, based on their current catalogs or price lists. It also contains prices obtained from international development agencies and government agencies. MSH and WHO are working with partners to make existing medicine price information more widely available to improve procuring medicines of assured quality for the lowest possible price. This will contribute to equitable access to health services and commodities necessary for the prevention and treatment of prevalent diseases.
Because the cost of providing a full range of treatments for common diseases could potentially be high, prices and financing are inescapable factors in determining access to essential medicines. When price ranges can be reviewed and compared, lower prices can be obtained through bulk purchasing, competition, skillful negotiation, and sound supply management. Such information helps in price negotiations, in locating new supply sources, and in assessing the efficiency of local procurement systems.
4

The International Drug Price Indicator Guide helps supply officers determine the probable cost of pharmaceutical pro-ducts for their programs. It can be used as a reference list to compare current prices paid to prices for products available on the international market; it can also be used to assess the potential financial impact of changes to a pharmaceu-ticals list. The Guide is intended as a comparative reference only; it is not suitable for actually ordering products. Prices from buyers are listed for comparison purposes only. The 2010 edition includes more than 1,100 items and has prices from 26 sources.
RefeRenCes
1. World Health Organization. 2011. Fact Sheet No. 297 on Cancer. Geneva: WHO. http://www.who.int/mediacentre/factsheets/fs297/en/index.html accessed 17 October, 2011.
2. Aziz, Z. 2008. Across generations: cancer treatment in developing coun-tries. Journal of Clinical Oncology 26:4990-91.
3. Milani, B. and W. Scholten. 2011. Access to Controlled Medicines. The World Medicines Situation. Geneva: WHO.
4. Twagirumukiza, M., L. Annemans, J. G. Kips, et al. 2010 JG, 2010. Prices of antihypertensive medicines in sub-Saharan Africa and alignment to WHO’s model list of essential medicines. Tropical Medicine & Interna-tional Health 15:350-61.
5. Management Sciences for Health. 2010. International Drug Price Indi-cator Guide. Quality Standards. http://erc.msh.org/mainpage.cfm?file=2.4.cfm&id=5541&temptitle=Quality%20standards&module =DMP&language=English. accessed 17 October, 2011.

Cancer Medicine PricesIN LOW- AND MIDDLE- INCOME COUNTRIES
Global Task Force on Expanded Access to Cancer Care and Controlin Developing Countries (GTF.CCC)
Harvard Global Equity Initiative, Secretariat651 Huntington Avenue
FXB Building, Room 632Boston, MA 02115
gtfccc.harvard.edu [email protected]
About Management Sciences for Health Management Sciences for Health (MSH) is a global nonprofit health organization, using proven approaches developed over four decades to help leaders, health managers, and communities in developing nations build stronger health systems for greater health impact. We work to save lives by closing the gap between knowledge and action in public health Most of the leading causes of death and disability in developing countries can be prevented or treated with cost-effective medicines. Despite this fact, hundreds of millions of people do not have access to these medicines. Improving the way medicines are accessed and used is a powerful opportunity to create stronger health systems and achieve greater health impact. Management Sciences for Health’s Center for Pharmaceutical Management develops the capacity of both the public and private sectors to select, procure, and distribute quality medicines and health supplies and helps to ensure their proper dispensing and use–all in a cost-effective way.
About The Global Task Force on Expanded Accessto Cancer Care and Control in Developing Countries
The mandate of The Global Task Force on Expanded Access to Cancer Care and Control in Developing Countries (GTF.CCC) is to design, implement and evaluate innovative, multi-stakeholder strategies for expanding access to cancer prevention, detection and care. Through local partners, the GTF.CCC supports implementation of innovative service in delivery models that can provide evidence for scaling up access to cancer care and control, and strengthening health systems in developing countries.