Cancer Biomarkers Aspirin Use and Risk of Breast Cancer ... · included studies independently using...
11
Review Aspirin Use and Risk of Breast Cancer: Systematic Review and Meta-analysis of Observational Studies Shanliang Zhong 1 , Lin Chen 2 , Xiaohui Zhang 1 , Dandan Yu 3 , Jinhai Tang 3 , and Jianhua Zhao 1 Abstract Previous studies concerning the association between aspirin use and breast cancer risk yielded inconsistent results. We aimed to investigate the association by meta-analysis. PubMed and EMBASE were searched for relevant studies. We calculated the summary relative risks (RR) and 95% confidence intervals (CI) using random-effects models. Seventeen cohort studies and 15 case–control studies were included. The overall result showed that aspirin use decreased risk of breast cancer (RR, 0.90; 95% CI, 0.85–0.95). However, there was evidence of publication bias and heterogeneity and the association disap- peared after correction using the trim-and-fill method. When stratified by study design, a significant benefit for aspirin users was only found in population-based and hospital-based case– control studies but not in cohort or nest case–control studies. Further subgroup analyses showed that aspirin use could decrease risk of in situ breast tumors or hormone receptor– positive tumors and reduce risk of breast cancer in postmen- opausal women. Aspirin use may not affect overall risk of breast cancer, but decrease risk of in situ breast tumors or hormone receptor–positive tumors and reduce risk of breast cancer in postmenopausal women. Considering between-study signifi- cant heterogeneity and publication bias, confirmation in future studies is also essential. Cancer Epidemiol Biomarkers Prev; 24(11); 1645–55. Ó2015 AACR. Introduction Breast cancer, one of the most frequently diagnosed cancers among women of all racial and ethnic groups, leads to the second most common cancer-associated death among U.S. women (1). Despite many efforts, few modifiable risk factors for breast cancer have been identified. Recently, the potential anticancer properties of aspirin, commonly known as pain reliever, have attracted more interest (2). Aspirin display anticancer activity by inhibiting cyclooxygenase (COX; ref. 3), thus decreasing the formation of downstream tissue-specific signaling lipids known as prostanoids. Prostanoids play an important role in carcinogenesis by affecting cellular proliferation, apoptosis, and angiogenesis (4). Although protection of aspirin against cancer has been showed, the pro- tective effects are seen mainly in colorectal, esophageal, gastric, and endometrial cancers (3, 5). Previously, we have investigated the effect of aspirin intake on the mortality in breast cancer, but only found that aspirin use has a small effect on the survival of breast cancer patients (6). A number of observational studies have investigated the effect of aspirin use on the risk of breast cancer in the past three decades, but their results are conflicting rather than conclusive. A meta- analysis (7) including 33 studies has evaluated the association and found that a decreased risk of breast cancer for aspirin users was found in the pooled analysis of all studies [odds ratio (OR) ¼ 0.86; 95% confidence interval (CI) ¼ 0.81–0.92] but not in a randomized controlled trial (OR, 0.98; 95% CI, 0.87–1.09). The investigators concluded that regular use of aspirin may be asso- ciated with reduced risk of breast cancer. However, the subjects of two included articles (8, 9) were overlapped in another two included articles (10, 11). The duplicated data could bias the results. We also noted that two studies (12, 13) examining the association between aspirin use and mortality in breast cancer patients but not between aspirin use and breast cancer risk were also included in that meta-analysis. In addition, previous meta- analysis has not performed a subgroup analysis according to hormone receptor status, menopausal status, or cancer stage. Since the meta-analysis, seven large observational studies have published. Therefore, we performed a meta-analysis with all available studies to explore the association between aspirin use and risk of breast cancer. Besides, we also performed a dose– response analysis to further evaluate the potential dose–response relations. Materials and Methods Literature search We searched PubMed (from 1980 to present) and Embase (from 1977 to present) using the following terms: "aspirin" or 1 Center of Clinical Laboratory Science, Jiangsu Cancer Hospital Affil- iated to Nanjing Medical University, Nanjing, China. 2 Department of Oncology, Xuzhou Medical College, Xuzhou, China. 3 Department of General Surgery, Jiangsu Cancer Hospital Affiliated to Nanjing Medical University, Nanjing, China. Note: Supplementary data for this article are available at Cancer Epidemiology, Biomarkers & Prevention Online (http://cebp.aacrjournals.org/). Corresponding Author: Jianhua Zhao, Center of Clinical Laboratory Science, Jiangsu Cancer Hospital Affiliated to Nanjing Medical University, Baiziting 42, Nanjing 210009, China. Phone: 8625-8328-3334; Fax: 8625-8335-1406; E-mail: [email protected] doi: 10.1158/1055-9965.EPI-15-0452 Ó2015 American Association for Cancer Research. Cancer Epidemiology, Biomarkers & Prevention www.aacrjournals.org 1645 Cancer Research. by guest on August 28, 2020. Copyright 2015 American Association for https://bloodcancerdiscov.aacrjournals.org Downloaded from
Transcript of Cancer Biomarkers Aspirin Use and Risk of Breast Cancer ... · included studies independently using...

Review
Aspirin Use and Risk of Breast Cancer: SystematicReview and Meta-analysis of ObservationalStudiesShanliang Zhong1, Lin Chen2, Xiaohui Zhang1, Dandan Yu3, Jinhai Tang3, andJianhua Zhao1
Abstract
Previous studies concerning the association between aspirinuse and breast cancer risk yielded inconsistent results. Weaimed to investigate the association by meta-analysis. PubMedand EMBASE were searched for relevant studies. We calculatedthe summary relative risks (RR) and 95% confidence intervals(CI) using random-effects models. Seventeen cohort studiesand 15 case–control studies were included. The overall resultshowed that aspirin use decreased risk of breast cancer (RR,0.90; 95% CI, 0.85–0.95). However, there was evidence ofpublication bias and heterogeneity and the association disap-peared after correction using the trim-and-fill method. Whenstratified by study design, a significant benefit for aspirin users
was only found in population-based and hospital-based case–control studies but not in cohort or nest case–control studies.Further subgroup analyses showed that aspirin use coulddecrease risk of in situ breast tumors or hormone receptor–positive tumors and reduce risk of breast cancer in postmen-opausal women. Aspirin use may not affect overall risk of breastcancer, but decrease risk of in situ breast tumors or hormonereceptor–positive tumors and reduce risk of breast cancer inpostmenopausal women. Considering between-study signifi-cant heterogeneity and publication bias, confirmation in futurestudies is also essential. Cancer Epidemiol Biomarkers Prev; 24(11);1645–55. �2015 AACR.
IntroductionBreast cancer, one of the most frequently diagnosed cancers
among women of all racial and ethnic groups, leads to the secondmost common cancer-associated death among U.S. women (1).Despite many efforts, fewmodifiable risk factors for breast cancerhave been identified. Recently, the potential anticancer propertiesof aspirin, commonly known as pain reliever, have attractedmoreinterest (2). Aspirin display anticancer activity by inhibitingcyclooxygenase (COX; ref. 3), thus decreasing the formation ofdownstream tissue-specific signaling lipids knownasprostanoids.Prostanoids play an important role in carcinogenesis by affectingcellular proliferation, apoptosis, and angiogenesis (4). Althoughprotection of aspirin against cancer has been showed, the pro-tective effects are seen mainly in colorectal, esophageal, gastric,and endometrial cancers (3, 5). Previously, we have investigatedthe effect of aspirin intake on the mortality in breast cancer, but
only found that aspirin use has a small effect on the survival ofbreast cancer patients (6).
A number of observational studies have investigated the effectof aspirin use on the risk of breast cancer in the past three decades,but their results are conflicting rather than conclusive. A meta-analysis (7) including 33 studies has evaluated the associationand found that a decreased risk of breast cancer for aspirin userswas found in the pooled analysis of all studies [odds ratio (OR)¼0.86; 95% confidence interval (CI) ¼ 0.81–0.92] but not in arandomized controlled trial (OR, 0.98; 95% CI, 0.87–1.09). Theinvestigators concluded that regular use of aspirin may be asso-ciated with reduced risk of breast cancer. However, the subjects oftwo included articles (8, 9) were overlapped in another twoincluded articles (10, 11). The duplicated data could bias theresults. We also noted that two studies (12, 13) examining theassociation between aspirin use and mortality in breast cancerpatients but not between aspirin use and breast cancer risk werealso included in that meta-analysis. In addition, previous meta-analysis has not performed a subgroup analysis according tohormone receptor status, menopausal status, or cancer stage.Since the meta-analysis, seven large observational studies havepublished. Therefore, we performed a meta-analysis with allavailable studies to explore the association between aspirin useand risk of breast cancer. Besides, we also performed a dose–response analysis to further evaluate the potential dose–responserelations.
Materials and MethodsLiterature search
We searched PubMed (from 1980 to present) and Embase(from 1977 to present) using the following terms: "aspirin" or
1Center of Clinical Laboratory Science, Jiangsu Cancer Hospital Affil-iated to Nanjing Medical University, Nanjing, China. 2Department ofOncology, Xuzhou Medical College, Xuzhou, China. 3Department ofGeneral Surgery, JiangsuCancerHospital Affiliated toNanjingMedicalUniversity, Nanjing, China.
Note: Supplementary data for this article are available at Cancer Epidemiology,Biomarkers & Prevention Online (http://cebp.aacrjournals.org/).
Corresponding Author: Jianhua Zhao, Center of Clinical Laboratory Science,Jiangsu Cancer Hospital Affiliated to Nanjing Medical University, Baiziting 42,Nanjing 210009, China. Phone: 8625-8328-3334; Fax: 8625-8335-1406; E-mail:[email protected]
doi: 10.1158/1055-9965.EPI-15-0452
�2015 American Association for Cancer Research.
CancerEpidemiology,Biomarkers& Prevention
www.aacrjournals.org 1645
Cancer Research. by guest on August 28, 2020. Copyright 2015 American Association forhttps://bloodcancerdiscov.aacrjournals.orgDownloaded from

"acetylsalicylic acid" or "non-steroidal anti-inflammatory drug"or "non-steroidal anti-inflammatory drugs," and "breast cancer"and "risk" or "incidence". The latest date of this search was April2015. All cohort or case–control studies evaluating the relation-ship between aspirin use and risk of breast cancer were eligible,without language restriction. Reference lists from relevant articleswere examined manually to further identify potentially relevantstudies. All searches were conducted independently by tworeviewers; differences were checked by the two and resolved bydiscussion.When two ormore studies presented possible overlap,we included the one with largest populations.
Inclusion criteriaAll the studies were included in this meta-analysis if they met
the following criteria: (i) the exposure of interest was aspirin use;(ii) theoutcomeof interestwas breast cancer; (iii) the studydesignwas case–control or cohort; and (iv) risk estimates and 95% CIswere reported (or information to calculate them).
Data extractionTwo independent investigators extracted data from the eligible
articles. The extracted data included the last name of first author,year of publication, origin of the study, follow-up period, studydesign, sample size, aspirin use, risk estimates, and corresponding95%CIs, and covariates adjusted for in themultivariable analysis.For studies providedmore than one risk estimate, we extracted theone that was adjusted for the greatest number of confoundingfactors. Discrepancies were resolved by consensus, involving athird investigator.
Study quality assessmentTwo investigators assessed the methodological quality of
included studies independently using the nine-star NewcastleOttawa scale (NOS; ref. 14). Each study was evaluated based oneight items, categorized into three broad perspectives, includingselection, comparability, and outcome, for cohort studies orexposure for case–control studies. We considered studies with ascore of 7 or greater as high quality. Discrepancies were resolvedby discussion or through consultation with a third investigator.
Statistical analysisBecause outcomes were relatively rare, the ORs and HRs were
considered approximations of relative risks (RR). Summaryestimates of RRs and 95% CIs were obtained using a ran-dom-effects model where the restricted maximum likelihoodestimator was used to evaluate the interstudy heterogeneity (15,16). We calculated prediction interval (PI) of summary esti-mate for the random effects model to depict the uncertaintyaround the estimate (17). If studies did not report a summaryrisk estimate for aspirin use, a summary risk estimate wascalculated using risk estimates for each of the aspirin usecategories (18–33). Interstudy heterogeneity was estimatedusing a c2-based Q test (34), with a P value of <0.10 consideredstatistically significant (35). We also calculated the I2 quantity(34), which lies between 0% and 100%. A value of 0% indicatesno observed heterogeneity and larger values indicate increasingheterogeneity. Metaregression was conducted to further explorethe sources of heterogeneity. Sensitivity analyses were per-formed to reflect the influence of individual data on summaryHRs. Finally, the potential for publication bias was examined
using Begg and Egger regression test (36). Where publicationbias was found, the trim-and-fill method was used to estimatethe potential influence of this bias on pooled summary esti-mates (37).
A two-stage random-effects dose–response meta-analysis wasperformed to compute the trend from the correlated log RRestimates across levels of aspirin use into account the between-study heterogeneity (38). A potential nonlinear relation betweenaspirin use and risk ofdeathwas investigatedusing restricted cubicsplines with three knots at the 25th, 50th, and 75th percentiles ofthe exposure distribution. Then, the study-specific estimates werecombined using the restricted maximum likelihood method in amultivariate random-effects meta-analysis (39). A P value fornonlinearity was calculated by testing the null hypothesis thatthe coefficient of the second spline is equal to zero. For each study,we calculated the median level of aspirin use for each category byassigning the midpoint of upper and lower boundaries in eachcategory as the average aspirin use level. When the highestcategory was open-ended, we assigned the lower end value ofthe category multiplied by 1.5. Studies were not eligible if therequired data were not reported or could not be estimated. All ofthe statistical analyses were done with R software, version 3.1.1,using the packages metafor (40) and dosresmeta (41). All statis-tical tests were two-sided.
ResultsCharacteristics of the studies
Figure 1 presents the process of study selection. Two thousandsix hundred and ten abstracts and titles were identified andassessed, and 45 studies were evaluated in detail with regard totheir fulfillment of the inclusion criteria. Four articleswere exclud-ed as the exposure of interestwas not aspirin use, or nousable datawere reported (42–45). Nine studies were excluded because their
Figure 1.Flow chart of the selection of publications included in the meta-analysis.
Zhong et al.
Cancer Epidemiol Biomarkers Prev; 24(11) November 2015 Cancer Epidemiology, Biomarkers & Prevention1646
Cancer Research. by guest on August 28, 2020. Copyright 2015 American Association forhttps://bloodcancerdiscov.aacrjournals.orgDownloaded from

Table
1.Cha
racteristics
ofstud
iesinclud
edin
themeta-an
alysis
First
author
Yea
rCoun
try
Follo
w-upperiod
Stud
ydesign
Sample
size
Asp
irin
use
RR(95%
CI)
Cova
riatead
justmen
t
Brasky
2014
USA
1993–
2010
Coho
rt126,689
Nonu
ser
HR1.0
0Age,
observationa
lstud
yen
rollm
ent,
horm
one
therap
ytrialenrollm
ent,diet
modificationtrialenrollm
ent,calcium/
vitamin
Dtrialenrollm
ent,U.S.reg
ion,
education,
ethn
icity,
height,B
MI,
phy
sicalactivity,alco
holconsum
ption,
pack-ye
arsofsm
oking
,fruitan
dve
getab
leco
nsum
ption,
redmea
tco
nsum
ption,
family
histories
of:
breastcancer,cervicalcancer,
endometrial
cancer,a
ndco
lorectal
cancer;screen
ingfor:breastcancer,
coloncancer,and
cervicalcancer;age
atmen
arche,
ageat
men
opau
se,
gravidity,ag
eat
firstbirth,d
urationof
estrogen
therap
y,durationof
combined
postmen
opau
salho
rmone
therap
y,hy
sterectomystatus,
multivitamin
use,
useof
antihy
pertensivemed
ication,
history
ofco
rona
ryhe
artdisea
se,u
seof
cholesterol-loweringmed
ication,
history
ofa
rthritis,history
ofm
igraine,
history
ofulcer,an
dother
NSAID
use.
Med
ian9.7
years
Inco
nsistent
use
0.99(0.91–1.0
9)
Consistent
use
1.11(1.00–1.24)
Cui
2014
USA
2001–20
11PCC
5,078
Nonu
sers
OR1.0
0Persona
lhistory
ofben
ignbreast
disea
se,fi
rst-deg
reefamily
history
of
breastcancer,m
enopau
salstatus,
history
oflivebirth,a
geat
firstlive
birth,u
seofho
rmone
replacemen
ttherap
y,regular
exercise,a
lcoho
lco
nsum
ption,
andcigarette
smoking
status.
Eve
rusers
0.82(0.69–0
.99)
Hollestein
2014
The
Nethe
rlan
ds
1998–2010
Coho
rt55
,597
Nonu
sers
HR1.0
0Age,
sex,un
ique
number
ofdispen
sing
san
dun
ique
number
ofh
ospitalizations
intheye
arpriorto
startoffollo
w-up.
Med
ian9.7
years(IQR2–
7)Users
1.02(0.97–
1.08)
Lee
2012
China
2002–
2008
PCC
67,38
80–27cD
DD
OR1.0
0Urban
ization,
inco
me,
diabetes
mellitus,
metform
inusag
e,statin
usag
e,estrogen
usag
e,an
dprogesterone
usag
e.
28–3
64cD
DD
0.92(0.87–
0.99)
�365cD
DD
0.86(0.79–0
.93)
Zha
ng20
12USA
1980–2
008
Coho
rt84,602
Nonu
ser
RR1.0
0Age,ag
eat
men
arche,he
ight,B
MIatag
e18
years,weight
chan
gesinceag
e18
years,parityan
dag
eat
firstbirth,
history
ofbreastcancer
inparen
tor
sibling,h
istory
ofben
ignbreast
disea
se,alcoho
lconsum
ption,phy
sical
activity,a
ndpostmen
opau
sal
horm
one
use.
28ye
ars
Past
0.97(0.88–1.08)
Current
0.96(0.87–
1.05)
(Continue
donthefollowingpag
e)
Aspirin Use and Risk of Breast Cancer
www.aacrjournals.org Cancer Epidemiol Biomarkers Prev; 24(11) November 2015 1647
Cancer Research. by guest on August 28, 2020. Copyright 2015 American Association forhttps://bloodcancerdiscov.aacrjournals.orgDownloaded from

Table
1.Cha
racteristics
ofstud
iesinclud
edin
themeta-an
alysis
(Cont'd)
First
author
Yea
rCoun
try
Follo
w-upperiod
Stud
ydesign
Sample
size
Asp
irin
use
RR(95%
CI)
Cova
riatead
justmen
t
Bardia
2011
USA
1986–2
005
Coho
rt26
,580
Nev
erRR1.0
0Age,
education,
family
history
ofbreast
cancer,a
geat
men
arche,
ageat
men
opau
se,p
arity/ag
eat
firstlive
birth,use
ofo
ralcontraceptive
s,useof
horm
one
therap
y,BMIin
1992,
BMIat
age18
years,relative
weight
atag
e12,
history
ofosteo
arthritis,history
of
rheu
matoid
arthritis,sm
oking
,use
of
alco
hol,sm
oking
,and
phy
sicalactivity
leve
l.
13ye
ars
Eve
r0.80(0.71–0.90)
Bosco
2011
USA
1995–
2007
Coho
rt59
,000
Nonu
seRR1.0
Agean
dque
stionn
aire
cyclean
dad
justed
fored
ucation,
BMIat
age18,
vigorous
activity,fem
aleho
rmone
use,
andsm
oking
.Modelsforaspirin
adjusted
furthe
rforother
NSAIDs,
other
NSAIDsad
justed
foraspirin,and
acetam
inophe
nforaspirin
andother
NSAIDs.
Form
eruse
1.15(0.95–
1.38)
Current
use
0.79(0.66–0
.95)
Brasky
2010
USA
1996–2001
PCC
3,28
5Nonu
sers
OR1.0
0Age,
race,e
ducation,
ageat
men
arche,
ageat
men
opau
se,p
arity,
useof
horm
one
therap
y,ben
ignbreast
disea
se,fam
ilyhistory
ofbreast
cancer,a
ndother
NSAID
use.
Users
0.80(0.68–0
.94)
Cronin–
Fen
ton
2010
Den
mark
1991–20
06
NCC
90,14
5Nev
erOR1.0
0Use
ofho
rmone
replacemen
ttherap
y,rheu
matoid
arthritisan
dmigraine.
Eve
r0.98(0.90–1.07)
Eliassen
2009
USA
1989–2
003
Coho
rt112,29
2Nonu
sers
RR1.0
0Ageat
men
arche,
height,B
MIat
age18
years,weight
chan
gesinceag
e18
years,oralcontraceptive
use,
parity
andag
eat
firstbirth,a
lcoho
lco
nsum
ption,history
ofben
ignbreast
disea
se,fam
ilyhistory
ofbreast
cancer.
14ye
ars
Pastusers
1.21(1.03–
1.41)
Current
users
1.07(0.89–1.29)
Friis
2008
Den
mark
1993–
2003
Coho
rt28
,695
Nonu
sers
RR1.0
0Age,scho
oleducation,parity,nu
mber
of
births,useofHRTan
dhistory
of
ben
ignbreasttumour
surgery.
Ave
rage7.5ye
ars(Ran
ge
0.1–
10.1)
Users
1.31(1.12
–1.53)
Gierach
2008
USA
1995–
2003
Coho
rt126,12
4Nev
erRR1.0
0Age,
race,a
geat
firstbirth,h
orm
one
therap
yuse,
number
ofbreast
biopsies,a
lcoho
lintake,h
istory
of
hypertension,
family
history
ofbreast
cancer
infirst-deg
reerelative
and
freq
uencyofuseofopposite
NSAID
type.
Ave
rage3.43ye
arsforcases
(ran
ge,
1day
to7.13
years);
6.75ye
arsforno
ncases
(ran
ge,
1day
to7.17
years)
<1times/w
eek
0.95(0.89–1.03)
1–6times/w
eek
0.95(0.87–
1.04)
�1times/day
0.93(0.85–
1.01)
Rea
dy
2008
USA
2000–2004
Coho
rt35
,323
None
HR1.0
0Age,
race,B
MI,family
history
ofbreast
cancer,h
istory
ofbreastbiopsy,
mam
mogram
in2ye
arspriorto
baseline,ag
eat
men
arche,ag
eat
first
birth,a
geat
men
opau
se,h
istory
of
surgical
men
opau
se,y
ears
of
combined
estrogen
andprogesterone
horm
one
therap
y,multivitamin
use
andalco
holu
seas
wella
sad
justmen
tforuseofother
categories
ofNSAIDs.
Any
0.99(0.80–1.23)
(Continue
donthefollowingpag
e)
Zhong et al.
Cancer Epidemiol Biomarkers Prev; 24(11) November 2015 Cancer Epidemiology, Biomarkers & Prevention1648
Cancer Research. by guest on August 28, 2020. Copyright 2015 American Association forhttps://bloodcancerdiscov.aacrjournals.orgDownloaded from

Table
1.Cha
racteristics
ofstud
iesinclud
edin
themeta-an
alysis
(Cont'd)
First
author
Yea
rCoun
try
Follo
w-upperiod
Stud
ydesign
Sample
size
Asp
irin
use
RR(95%
CI)
Cova
riatead
justmen
t
Gallicchio
2007
USA
1989–2
006
Coho
rt15,651
Nonu
sers
RR1.0
0Age.
Users
0.90(0.70–1.16
)Gill
2007
USA
1993–
2002
Coho
rt98,920
Current
users
Age,
ethn
icity,
BMI,family
history
of
breastcancer,e
ducation,
mam
mography
screen
ing,a
lcoho
lintake,a
geat
men
arche,
ageat
first
liveb
irth,n
umber
ofchild
ren,
men
opau
salstatus,a
geat
men
opau
se,h
orm
one
replacemen
ttherap
y,an
dallp
ainmed
icationuse.
Nonu
sers
HR1.0
0�1
year
1.01(0.79–1.30)
2–5ye
ars
0.89(0.72–
1.09)
�6ye
ars
1.05(0.88–1.25)
Pastusers
Nonu
sers
HR1.0
0�1
year
1.07(0.87–
1.32)
2–5ye
ars
0.95(0.75–
1.22)
�6ye
ars
1.04(0.84–1.27)
Jaco
bs
2007
USA
1992–
2003
Coho
rt76
,303
Noreported
use
RR1.0
0Age,
race,e
ducation,
smoking
,BMI,
phy
sicalactivityleve
l,useofho
rmone
replacemen
ttherap
y,history
of
mam
mography
,history
ofco
lorectal
endoscopy,useofno
naspirin
NSAIDs,
andhistory
ofhe
artattack,d
iabetes,
andhy
pertension.
Less
than
daily,
low–d
ose,o
rpastuse
1.10(1.00–1.21)
Current
daily
use,
<5ye
ars
1.02(0.88–1.19
)
Current
daily
use,
�5ye
ars
0.83(0.63–
1.10)
Kirsh
2007
Can
ada
1996–1998
PCC
4,872
Nonu
sers
OR1.0
0Age,
arthritis,an
dben
ignbreastcysts.
Users
0.75(0.64–0
.88)
Slattery
2007
USA
1999–2004
PCC
4,850
No
OR1.0
0Age,
stud
ycenter,referen
tye
arBMI,
lifetim
ephy
sicala
ctivityscore,p
arity,
andpercentag
eNativeAmerican
ancestry.
Yes
0.92(0.74–1.15
)
Harris
2006
USA
2003–
2004
HCC
770
Nonu
sers
OR1.0
0Age,
bodymass,parity,
men
opau
sal
status,fam
ilyhistory,smoking
,and
alco
holintake.
Users
0.49(0.26–0
.94)
Marshall
2005
USA
1995–
2001
Coho
rt114,460
Noregular
use
RR1.0
0Race,
BMI,first-deg
reefamily
history
of
breastcancer,m
enopau
sala
ndho
rmone
therap
yusestatus,smoking
,alco
holintake,p
hysicala
ctivity,
mam
mography
history,b
reastbiopsy
history,p
aritystatus
before
age30
,an
dne
ighb
orhoodsocioecono
mic
status.
Reg
ular
use
1–6days/wee
k1.0
9(0.98–1.22)
Daily
0.98(0.86–1.13
)
Rah
me
2005
Can
ada
1998–2
002
NCC
46,080
Notexposed
OR1.0
0Age,mam
mography
inye
ars2or3prior
toindex
date,breastprocedurein
the
prior3ye
ars,ben
ignne
oplasm
ofthe
breastintheprior3
years,other
breast
disea
sein
theprior3ye
ars,estrogen
replacemen
ttherap
yin
thepriorye
ar,
andvisitto
agyn
ecologistin
theprior
year.
�100mg/day
0.91(0.71–1.16)
>100mg/day
0.75(0.64–0
.89
Swed
e20
05
USA
1982–
1998
HCC
4,861
Nev
erOR1.0
0Ageat
men
arche,
ageat
1stbirth,B
MI,
history
of1st-deg
reerelative
with
breastcancer,a
ndhistory
ofben
ign
breastdisea
se.
Occasiona
l0.80(0.67–
0.96)
Reg
ular
0.85(0.74–0
.97)
(Continue
donthefollowingpag
e)
Aspirin Use and Risk of Breast Cancer
www.aacrjournals.org Cancer Epidemiol Biomarkers Prev; 24(11) November 2015 1649
Cancer Research. by guest on August 28, 2020. Copyright 2015 American Association forhttps://bloodcancerdiscov.aacrjournals.orgDownloaded from

Table
1.Cha
racteristics
ofstud
iesinclud
edin
themeta-an
alysis
(Cont'd)
First
author
Yea
rCoun
try
Follo
w-upperiod
Stud
ydesign
Sample
size
Asp
irin
use
RR(95%
CI)
Cova
riatead
justmen
t
Zha
ng20
05
USA
1976
–2002
HCC
3,960
Nev
erused
OR1.0
0Age,ye
arofinterview
,studycenter,race,
yearsofed
ucation,
ben
ignbreast
disea
se,n
umber
ofphy
sician
visits
2ye
arsbefore
hospitalization,
duration
offemaleho
rmone
supplemen
tuse,
durationofo
ralcontraceptive
use,ag
eat
men
arche,
ageat
men
opau
se,a
ge
atfirstbirth,p
arity,
alco
hol
consum
ption,
family
history
ofbreast
cancer,p
racticeofbreastself-
exam
ination,
andBMI.
Reg
ular
use
0.86(0.64–1.16
)
GarciaRodrigue
z20
04
UK
1995–
2001
NCC
23,708
Nouse
OR1.0
0Age,
calend
arye
ar,B
MI,sm
oking
,alco
hol,priorben
ignbreastdisea
se,
NSAIDs,paracetam
ol,steroidan
dHRT
use.
Current
use
0.88(0.75–
1.04)
Pastuse
0.90(0.70–1.15
)
Terry
2004
USA
1996–1997
PCC
2,862
Nonu
sers
OR1.0
0Ageat
diagno
sis,migrainehe
adache
,BMI,an
dsimultane
ously
adjusted
for
theother
typeofmed
icationuse.
Eve
rusers
0.80(0.66–0
.97)
Harris
2003
USA
From
1992
Coho
rt80,741
0–11months
RR1.0
0Age.
Ave
rage43months
1–4ye
ars
0.90(0.72–
1.13)
�5ye
ars
0.81(0.66–0
.99)
Moorm
an20
03
USA
1996–2000
PCC
2,631
Nonu
sers
OR1.0
0Agean
drace.
Eve
rusers
0.4
(0.3–0
.7)
Harris
1999
USA
1991–1996
Coho
rt32
,505
0,<
1pill/w
eek
RR1.0
0Age.
Ave
rage4.7
years
1–3pills/wee
k0.57(0.40–0
.81)
�4pills/wee
k0.64(0.45–
0.90)
Neu
gut
1998
USA
1989–1992
HCC
428
Nonu
sers
OR1.0
0Age,
education,
parity,
men
opau
sal
status,a
ndfamily
history
ofbreast
cancer.
Users
0.80(0.35–
1.80)
Harris
1996
USA
Notstate
PCC
2,045
Nonu
sers
OR1.0
0Age,
parity,
men
opau
salstatus,a
ndfamily
history.
Users
0.69(0.46–0
.99)
Schreinem
ache
rs1994
USA
1971–1987
Coho
rt7,029
Nonu
sers
RR1.0
0Age.
Ave
rage12.4
years
Users
0.72(0.52–
1.00)
Pag
anini-Hill
1989
USA
1981–1988
Coho
rt7,439
Nonu
sers
RR1.0
0None
.Users
1.00(0.76–1.33)
Abbreviations:B
MI,bodymassindex;cDDD,cum
ulativedefi
neddailydose;C
I,co
nfiden
ceinterval;H
CC,hospital-based
case–controlstudy;NCC,nestcase–controlstudy;NSAID,nonsteroidalan
ti-infl
ammatory
drugs;PCC,
population-based
case–controlstudy.
Zhong et al.
Cancer Epidemiol Biomarkers Prev; 24(11) November 2015 Cancer Epidemiology, Biomarkers & Prevention1650
Cancer Research. by guest on August 28, 2020. Copyright 2015 American Association forhttps://bloodcancerdiscov.aacrjournals.orgDownloaded from

data duplicated or overlapped with other articles (8, 9, 46–52).Nevertheless, one of these studies (46) was included in thesubgroup analysis by hormone receptor status, and anotherstudy (48) was included in dose–response analysis. Finally, 17cohort studies (10, 18, 20–25, 29–31, 53–58) and 15 case–control studies (11, 19, 26–28, 32, 33, 59–66) involving1350,913 participants were selected for meta-analysis. Table 1shows the characteristics of the included studies. Supplemen-tary Tables S1 and S2 summarize the methodological quality ofall the included studies. The NOS results showed that theaverage score was 6.9 (range 4–9) for cohort studies and 6.3(range 4–9) for case–control studies. There were 18 studies witha score of 7 or more.
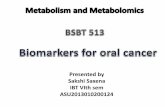
Evidence synthesisFigure 2 presents the pooled RR of the association between
aspirin use and risk of breast cancer. When the association ofaspirin use on breast cancer risk was analyzed as users versusnonusers, a RR of 0.90 (95% CI, 0.85–0.95, P < 0.01; 95% PI,0.68–1.19) was found. In stratified by study design, a significantbenefit for aspirin users was only found in population-basedcase–control (PCC) studies (RR, 0.80; 95% CI, 0.73–0.88, P <0.01; 95%PI, 0.65–0.98) and hospital-based case–control (HCC)studies (RR, 0.82; 95% CI, 0.75–0.91, P < 0.01; 95% PI, 0.75–0.91; Fig. 2). In the subgroup analysis by estrogen receptor (ER)or/and progesterone receptor (PR) status, a decreased breastcancer risk was found for aspirin users with ER-positive tumors(RR, 0.90; 95% CI, 0.81–0.99, P ¼ 0.04; 95% PI, 0.68–1.19), PR-positive tumors (RR, 0.87; 95% CI, 0.77–0.98, P ¼ 0.02; 95% PI,0.67–1.13), and ER- and PR-positive tumors (RR, 0.88; 95% CI,0.79–0.99, P¼ 0.04; 95% PI, 0.68–1.14; Fig. 3). When stratifyingby menopausal status, the results revealed that postmenopausalwomenwhoused aspirinhad aRRof 0.86 (95%CI, 0.80–0.93,P<0.01; 95% PI, 0.75–1.00) for breast cancer risk (Fig. 3). Furtheranalysis by cancer stage showed that aspirin use was only asso-ciated with decreased risk of in situ breast cancer (RR, 0.79; 95%CI, 0.71–0.88, P < 0.01; 95% PI, 0.71–0.88; Fig. 3).
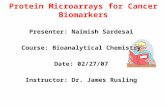
Dose–response meta-analysisThe dose–response effects of aspirin on breast cancer risk were
assessed with 14 studies (10, 11, 18, 20, 22, 24, 27–29, 48, 54, 55, 60, 63). Among these studies, exposure to aspirinwas expressed in duration of exposure (11, 18, 20, 24, 27–29, 55, 63) or frequency (e.g., pills/week; refs. 10, 22, 27, 48, 54,55, 60, 63). If exposure to aspirin was expressed in a times/week(or days/week) scale (10, 22, 55), we assumed the scale equals topills/week. A linear relationship was found for both duration (Pfor nonlinearity¼0.29) and frequency (P for nonlinearity¼0.88)of aspirin use (Fig. 4). A 1-year increment in duration of exposureto aspirin conferred aRRof 0.98 (95%CI, 0.97–1.00,P¼0.02) forbreast cancer risk (Fig. 4A). The risk of breast cancer was decreasedby 4% for every 3 pills/week increment in aspirin use (RR, 0.96;95% CI, 0.92–0.99, P ¼ 0.02; Fig. 4B).
Sensitivity analysis and publication biasFrom the results of the leave-one-out sensitivity analysis, the
summary RR was not materially altered (data not shown). Weexplored the source of heterogeneity by country (United Statesand others), study design (cohort, NCC, PCC, and HCC), pub-lication year, methodological quality (continuous variables), andsample size (�8,000 and <8,000 subjects) with metaregression.
The results revealed that noneof them contributed to the source ofheterogeneity (data not shown).
The results of Begg (P < 0.05) and Egger tests (P ¼ 0.01) haveshown the evidence of publication bias. Then, trim-and-fill meth-od was used to correct the result, and nine potential missingstudieswere required in the right side of the funnel plot in order tomake the plot symmetric (Supplementary Fig. S1). However, thecorrection achieved a nonsignificant reduction of breast cancerrisk for aspirin users (RR, 0.95; 95%CI, 0.88–1.02, P¼ 0.12; 95%PI, 0.65–1.38).
DiscussionThe current meta-analysis investigated the relationship
between aspirin use and risk of breast cancer involving1350,913 participants. The summary results, as derived from17 cohort studies and 15 case–control studies, indicated that theaverage effect of aspirin use was associated with decreased risk ofbreast cancer. However, there was evidence of publication biasand the association between aspirin use and breast cancer risk nolonger existed after correction using the trim-and-fill method. We
Figure 2.Pooled analyses and subgroup analyses by study design for theassociation between aspirin use and risk of breast cancer. The squares andhorizontal lines correspond to the study-specific relative risk and95%CIs. The area of the square is proportional to the inverse of the sumof thebetween studies variance and the study-specific variance. The diamondrepresents the pooledmultivariate relative risk and 95% CI. The dotted line ofthe diamond indicates the bounds of the 95% PI.
Aspirin Use and Risk of Breast Cancer
www.aacrjournals.org Cancer Epidemiol Biomarkers Prev; 24(11) November 2015 1651
Cancer Research. by guest on August 28, 2020. Copyright 2015 American Association forhttps://bloodcancerdiscov.aacrjournals.orgDownloaded from

Figure 3.Subgroup analyses by hormone receptor status, menopausal status, and cancer stage for the association between aspirin use and risk of breast cancer.The squares and horizontal lines correspond to the study-specific relative risk and 95% CIs. The area of the square is proportional to the inverse of the sum of thebetween studies variance and the study-specific variance. The diamond represents the pooled multivariate relative risk and 95% CI.
Zhong et al.
Cancer Epidemiol Biomarkers Prev; 24(11) November 2015 Cancer Epidemiology, Biomarkers & Prevention1652
Cancer Research. by guest on August 28, 2020. Copyright 2015 American Association forhttps://bloodcancerdiscov.aacrjournals.orgDownloaded from

also noted significant heterogeneity between included studies.Weexplored the source of heterogeneity using meta-regression andsubgroup analysis but failed to find convincing explanations forthe significant heterogeneity. When stratified by study design, asignificant benefit for aspirin users was only found in PCC andHCC studies but not in cohort and nest case–control (NCC)studies. PCC and HCC studies give a lower level of evidence thancohort and NCC studies and might provide spurious resultsbecause of selection bias and recall bias, which might havecontributed to the different results. Considering above men-tioned, we conclude that aspirin use may not be associated withdecreased risk of breast cancer overall.
In subgroup analysis by ER or/and PR status, a benefit foraspirin use on breast cancer risk was only found in hormonereceptor–positive tumors. Evidence suggested that endogenousestrogens are important risk factors for breast cancer (67). Post-menopausal women who are regular users of aspirin showedlower estrogen levels compared with nonusers, which couldpotentially lower the risk of breast cancer (68). As our resultindicated, the effect for ever use of aspirin was beneficial amongpostmenopausal women but not premenopausal women. The
different effect of aspirin may be due to postmenopausal womentend to have more hormone receptor–positive tumors (69).Further analysis by cancer stage showed that aspirin use was onlyassociated with decreased risk of in situ breast cancer. AlthoughCOX2 overexpression has been observed in both invasive and insitu breast tumors, a higher frequency of COX2 expression wasobserved in in situ tumors suggesting that the potential therapeuticimpact of COX2 inhibitionmay bemore relevant for in situ breastcancer than invasive tumors (70).
We further explored the dose–response relationship betweenaspirin use and risk of breast cancer. Our results indicated a linearand borderline significant relationship between aspirin use andbreast cancer risk. The risk of breast cancer was decreased by 2%for 1-year increment of aspirin use. There was a 4% breast cancerrisk reduction for every 3 pills/week increment in aspirin use.Considering the small effect, long-term or high-frequency aspirinuse is not recommended for prevention of breast cancer.
There is significant heterogeneity between included studies.However, we failed to find the source of heterogeneity. Severalreasons may account for the heterogeneity. First, seven cohortstudies reassessed exposure to aspirin during the course offollow-up, while ten cohort studies assessed the exposure onlyat baseline (Supplementary Table S1), which can lead to immor-tal time bias (71). Second, misclassification of aspirin use islikely to impact on the effect estimates of aspirin use. Moststudies assessed the exposure to aspirin based on self-reported,while some studies obtained exposure data from prescriptiondatabase or medical record. Self-reported data are not expectedto be accurately recalled. Third, studies conducted among popu-lations are varying in age and ethnicity. All of these may partlyexplain the significant heterogeneity between studies.
The potential limitations of our study should be consideredwhen interpreting the results. First, there was evidence of pub-lication bias and heterogeneity among included studies. Second,although included studies had adjusted for important riskfactors, unmeasured factors related to aspirin use may also haveinfluenced results of individual studies. Third, in the subgroupanalyses, the limited study number with relatively small samplesize in each subgroup may not have enough statistical power toexplore the real association. Fourth, the included studies weremajor conducted in Western countries, and hence the resultsshould be extrapolated to other populations with caution.
In conclusion, aspirin use may not affect overall risk of breastcancer, but decrease risk of in situ breast tumors or hormonereceptor–positive tumors and reduce breast cancer risk in post-menopausal women. Considering the heterogeneity and publi-cation bias, our results on the effect of aspirin use on risk of breastcancer overall or in the subgroups should be confirmed in futurestudies with well-controlled confounding factors, long enoughfollow-up time, and more accurate assessment of aspirin use,including quantity, frequency, and duration of use.
Disclosure of Potential Conflicts of InterestNo potential conflicts of interest were disclosed.
The costs of publication of this articlewere defrayed inpart by the payment ofpage charges. This article must therefore be hereby marked advertisement inaccordance with 18 U.S.C. Section 1734 solely to indicate this fact.
Received May 4, 2015; revised June 12, 2015; accepted August 4, 2015;published OnlineFirst August 27, 2015.
Figure 4.The dose–response analysis with restricted cubic splines in a multivariaterandom-effects dose–response model for the relationships of duration ofaspirin use and risk of breast cancer (A) and frequency of aspirin use and riskof breast cancer (B). The solid line and the short dash line represent theestimated relative risk and its 95% CI.
www.aacrjournals.org Cancer Epidemiol Biomarkers Prev; 24(11) November 2015 1653
Aspirin Use and Risk of Breast Cancer
Cancer Research. by guest on August 28, 2020. Copyright 2015 American Association forhttps://bloodcancerdiscov.aacrjournals.orgDownloaded from

References1. Siegel R, Ma J, Zou Z, Jemal A. Cancer statistics, 2014. CA Cancer J Clin
2014;64:9–29.2. Lazzeroni M, Petrera M, Marra D, Decensi A. Aspirin and breast cancer
prevention. Curr Breast Cancer Rep 2013;5:202–7.3. Thorat MA, Cuzick J. Role of aspirin in cancer prevention. Curr Oncol Rep
2013;15:533–40.4. ThunMJ, Jacobs EJ, Patrono C. The role of aspirin in cancer prevention. Nat
Rev Clin Oncol 2012;9:259–67.5. Neill AS, Nagle CM, Protani MM, Obermair A, Spurdle AB, Webb PM, et al.
Aspirin, nonsteroidal anti-inflammatory drugs, paracetamol and risk ofendometrial cancer: a case-control study, systematic review and meta-analysis. Int J Cancer 2013;132:1146–55.
6. Zhong S, ZhangX,ChenL,MaT, Tang J, Zhao J. Associationbetween aspirinuse andmortality in breast cancer patients: ameta-analysis of observationalstudies. Breast Cancer Res Treat 2015;150:199–207.
7. Luo T, Yan HM, He P, Luo Y, Yang YF, Zheng H. Aspirin use andbreast cancer risk: a meta-analysis. Breast Cancer Res Treat 2012;131:581–7.
8. Johnson TW, Anderson KE, Lazovich D, Folsom AR. Association of aspirinand nonsteroidal anti-inflammatory drug use with breast cancer. CancerEpidemiol Biomarkers Prev 2002;11:1586–91.
9. Coogan PF, Rao SR, Rosenberg L, Palmer JR, StromBL, Zauber AG, et al. Therelationship of nonsteroidal anti-inflammatory drug use to the risk ofbreast cancer. Prev Med 1999;29:72–6.
10. Bardia A, Olson JE, Vachon CM, Lazovich D, Vierkant RA, Wang AH, et al.Effect of aspirin and other NSAIDs on postmenopausal breast cancerincidence by hormone receptor status: results from a prospective cohortstudy. Breast Cancer Res Treat 2011;126:149–55.
11. Zhang Y, Coogan PF, Palmer JR, Strom BL, Rosenberg L. Use ofnonsteroidal antiinflammatory drugs and risk of breast cancer: theCase-Control Surveillance Study revisited. Am J Epidemiol 2005;162:165–70.
12. ThunMJ, Namboodiri MM, Calle EE, FlandersWD, Heath CW. Aspirin useand risk of fatal cancer. Cancer Res 1993;53:1322–7.
13. Ratnasinghe LD, Graubard BI, Kahle L, Tangrea JA, Taylor PR, Hawk E.Aspirin use and mortality from cancer in a prospective cohort study.Anticancer Res 2004;24:3177–84.
14. Wells G, Shea B, O'Connell D, Robertson J, Peterson J, Welch V, et al. TheNewcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomisedstudies in meta-analyses. www.ohri.ca/programs/clinical_epidemiology/oxford_web.ppt. 2010.
15. Viechtbauer W. Bias and efficiency of meta-analytic variance estimators inthe random-effects model. J Educ Behav Stat 2005;30:261–93.
16. Raudenbush SW. Analyzing effect sizes: random-effects models. In:Cooper H, Hedges LV, Valentine JC, editors. The Handbook of ResearchSynthesis and Meta-analysis. New York: Russell Sage Foundation; 2009.p. 295–316.
17. Riley RD, Higgins JP, Deeks JJ. Interpretation of random effects meta-analyses. BMJ 2011;342:d549.
18. Brasky TM, Liu J,White E, PetersU, Potter JD,Walter RB, et al.Non-steroidalanti-inflammatory drugs and cancer risk in women: Results from theWomen's Health Initiative. Int J Cancer 2014;135:1869–83.
19. Lee HH, Tsan YT, Ho WC, Lin MH, Lee CH, Tseng CD, et al. Angiotensin-converting enzyme inhibitors enhance the effect of cyclooxygenase inhi-bitors on breast cancer: a nationwide case-control study. J Hypertens2012;30:2432–9.
20. Bosco JL, Palmer JR, Boggs DA, Hatch EE, Rosenberg L. Regular aspirin useand breast cancer risk in US Black women. Cancer Causes Control 2011;22:1553–61.
21. Eliassen AH, Chen WY, Spiegelman D, Willett WC, Hunter DJ, HankinsonSE. Use of aspirin, other nonsteroidal anti-inflammatory drugs, and acet-aminophen and risk of breast cancer among premenopausal women in theNurses' Health Study II. Arch Intern Med 2009;169:115–21.
22. Gierach GL, Lacey JV Jr, Schatzkin A, Leitzmann MF, Richesson D, Hol-lenbeck AR, et al. Nonsteroidal anti-inflammatory drugs and breast cancerrisk in the National Institutes of Health-AARP Diet and Health Study.Breast Cancer Res 2008;10:R38.
23. Gill JK, Maskarinec G, Wilkens LR, Pike MC, Henderson BE, Kolonel LN.Nonsteroidal antiinflammatory drugs and breast cancer risk: the multi-ethnic cohort. Am J Epidemiol 2007;166:1150–8.
24. Jacobs EJ, Thun MJ, Bain EB, Rodriguez C, Henley SJ, Calle EE. A largecohort study of long-term daily use of adult-strength aspirin and cancerincidence. J Natl Cancer Inst 2007;99:608–15.
25. Marshall SF, Bernstein L, Anton-Culver H, Deapen D, Horn-Ross PL,Mohrenweiser H, et al. Nonsteroidal anti-inflammatory drug use andbreast cancer risk by stage and hormone receptor status. J Natl CancerInst 2005;97:805–12.
26. Rahme E, Ghosn J, Dasgupta K, Rajan R, Hudson M. Association betweenfrequent use of nonsteroidal anti-inflammatory drugs and breast cancer.BMC Cancer 2005;5:159.
27. Swede H, Mirand AL, Menezes RJ, Moysich KB. Association of regularaspirin use and breast cancer risk. Oncology 2005;68:40–7.
28. Garcia Rodriguez LA, Gonzalez-Perez A. Risk of breast cancer among usersof aspirin and other anti-inflammatory drugs. Br J Cancer 2004;91:525–9.
29. Harris RE, Chlebowski RT, Jackson RD, Frid DJ, Ascenseo JL, Anderson G,et al. Breast cancer and nonsteroidal anti-inflammatory drugs: prospectiveresults from the Women's Health Initiative. Cancer Res 2003;63:6096–101.
30. Harris RE, Kasbari S, Farrar WB. Prospective study of nonsteroidal anti-inflammatory drugs and breast cancer. Oncol Rep 1999;6:71–3.
31. Zhang X, Smith-Warner SA, Collins LC, Rosner B, Willett WC, HankinsonSE. Use of aspirin, other nonsteroidal anti-inflammatory drugs, and acet-aminophen and postmenopausal breast cancer incidence. J Clin Oncol2012;30:3468–77.
32. Kirsh VA, Kreiger N, Cotterchio M, Sloan M, Theis B. Nonsteroidal anti-inflammatory drug use and breast cancer risk: subgroup findings. Am JEpidemiol 2007;166:709–16.
33. Slattery ML, Curtin K, Baumgartner R, Sweeney C, Byers T, Giuliano AR,et al. IL6, aspirin, nonsteroidal anti-inflammatory drugs, and breast cancerrisk in women living in the southwestern United States. Cancer EpidemiolBiomarkers Prev 2007;16:747–55.
34. Higgins JP, Thompson SG. Quantifying heterogeneity in a meta-analysis.Stat Med 2002;21:1539–58.
35. Hedges LV, Pigott TD. The power of statistical tests in meta-analysis.Psychol Methods 2001;6:203–17.
36. Egger M, Davey Smith G, Schneider M, Minder C. Bias in meta-analysisdetected by a simple, graphical test. BMJ 1997;315:629–34.
37. Duval S, Tweedie R. Trim and fill: a simple funnel-plot-based method oftesting and adjusting for publication bias in meta-analysis. Biometrics2000;56:455–63.
38. Orsini N, Li R, Wolk A, Khudyakov P, Spiegelman D. Meta-analysis forlinear and nonlinear dose-response relations: examples, an evaluation ofapproximations, and software. Am J Epidemiol 2012;175:66–73.
39. Jackson D, White IR, Thompson SG. Extending DerSimonian and Laird'smethodology to perform multivariate random effects meta-analyses. StatMed 2010;29:1282–97.
40. ViechtbauerW. Conductingmeta-analyses in R with themetafor package. JStat Softw 2010;36:1–48.
41. Crippa A, Orsini N. Dosresmeta: Performing multivariate dose-responsemeta-analysis. Vienna, Austria: R Foundation for Statistical Computing;2013.
42. Poynter JN, Inoue-Choi M, Ross JA, Jacobs DR Jr, Robien K. Reproductive,lifestyle, and anthropometric risk factors for cancer in elderly women.Cancer Epidemiol Biomarkers Prev 2013;22:681–7.
43. Davis S, Mirick DK. Medication use and the risk of breast cancer. Eur JEpidemiol 2007;22:319–25.
44. Harris R, Namboodiri K, Farrar W. Epidemiologic-study of nonsteroidalantiinflammatory drugs and breast-cancer. Oncol Rep 1995;2:591–2.
45. Friedman GD, Ury HK. Initial screening for carcinogenicity of commonlyused drugs. J Natl Cancer Inst 1980;65:723–33.
46. Brasky TM, Bonner MR, Moysich KB, Ambrosone CB, Nie J, Tao MH,et al. Non-steroidal anti-inflammatory drugs (NSAIDs) and breastcancer risk: differences by molecular subtype. Cancer Causes Control2011;22:965–75.
47. Shen J, Gammon MD, Terry MB, Teitelbaum SL, Neugut AI, Santella RM.Genetic polymorphisms in the cyclooxygenase-2 gene, use of nonsteroidalanti-inflammatory drugs, and breast cancer risk. Breast Cancer Res 2006;8:R71.
48. Jacobs EJ, ThunMJ, Connell CJ, Rodriguez C,Henley SJ, FeigelsonHS, et al.Aspirin and other nonsteroidal anti-inflammatory drugs and breast cancer
Zhong et al.
Cancer Epidemiol Biomarkers Prev; 24(11) November 2015 Cancer Epidemiology, Biomarkers & Prevention1654
Cancer Research. by guest on August 28, 2020. Copyright 2015 American Association forhttps://bloodcancerdiscov.aacrjournals.orgDownloaded from

incidence in a large U.S. cohort. Cancer Epidemiol Biomarkers Prev2005;14:261–4.
49. Cotterchio M, Kreiger N, Sloan M, Steingart A. Nonsteroidal anti-inflam-matory drug use and breast cancer risk. Cancer Epidemiol Biomarkers Prev2001;10:1213–7.
50. Egan KM, StampferMJ, Giovannucci E, Rosner BA, Colditz GA. Prospectivestudy of regular aspirin use and the risk of breast cancer. J Natl Cancer Inst1996;88:988–93.
51. Lee HH, Tsan YT, Ho WC, Lin MH, Lee CH, Tseng CD, et al. Angiotensin-converting enzyme inhibitors enhance the effect of cyclooxygenase inhi-bitors on breast cancer : a nationwide casecontrol study. Value in Health2012;15:A654.
52. Lee HH, Tsan YT, Ho WC, Lin MH, Lee CH, Tseng CD, et al. Angiotensin-converting enzyme inhibitors enhance the effect of cyclooxygenase inhi-bitors on breast cancer : aa nationwide case-control study. Epidemiology2012;23:S590.
53. Hollestein LM, Van Herk-Sukel MPP, Ruiter R, De Vries E, Mathijssen RHJ,Wiemer EAC, et al. Incident cancer risk after the start of aspirin use: resultsfromaDutch population-based cohort study of lowdose aspirin users. Int JCancer 2014;135:157–65.
54. Friis S, Thomassen L, Sorensen HT, Tjonneland A, Overvad K,Cronin-Fenton DP, et al. Nonsteroidal anti-inflammatory drug useand breast cancer risk: a Danish cohort study. Eur J Cancer Prev2008;17:88–96.
55. Ready A, Velicer CM, McTiernan A, White E. NSAID use and breastcancer risk in the VITAL cohort. Breast Cancer Res Treat 2008;109:533–43.
56. Gallicchio L, Visvanathan K, Burke A, Hoffman SC, Helzlsouer KJ. Non-steroidal anti-inflammatory drugs and the risk of developing breast cancerin a population-based prospective cohort study in Washington County,MD. Int J Cancer 2007;121:211–5.
57. Schreinemachers DM, Everson RB. Aspirin use and lung, colon, andbreast cancer incidence in a prospective study. Epidemiology 1994;5:138–46.
58. Paganini-Hill A, Chao A, Ross RK, Henderson BE. Aspirin use and chronicdiseases: a cohort study of the elderly. BMJ 1989;299:1247.
59. Cui Y, Deming-Halverson SL, Shrubsole MJ, Beeghly-Fadiel A, Cai H, FairAM, et al. Use of nonsteroidal anti-inflammatory drugs and reduced breastcancer risk among overweight women. Breast Cancer Res Treat 2014;146:439–46.
60. Brasky TM, Bonner MR, Moysich KB, Ambrosone CB, Nie J, Tao MH, et al.Non-steroidal anti-inflammatory drug (NSAID) use and breast cancer riskin theWesternNewYorkExposures andBreastCancer (WEB) Study. CancerCauses Control 2010;21:1503–12.
61. Cronin-Fenton DP, Pedersen L, Lash TL, Friis S, Baron JA, SorensenHT. Prescriptions for selective cyclooxygenase-2 inhibitors, non-selec-tive non-steroidal anti-inflammatory drugs, and risk of breast cancerin a population-based case-control study. Breast Cancer Res 2010;12:R15.
62. Harris RE, Beebe-Donk J, Alshafie GA. Reduction in the risk of humanbreast cancer by selective cyclooxygenase-2 (COX-2) inhibitors. BMCCancer 2006;6:27.
63. Terry MB, Gammon MD, Zhang FF, Tawfik H, Teitelbaum SL, BrittonJA, et al. Association of frequency and duration of aspirin use andhormone receptor status with breast cancer risk. JAMA 2004;291:2433–40.
64. Moorman PG, Grubber JM, Millikan RC, Newman B. Association betweennon-steroidal anti-inflammatory drugs (NSAIDs) and invasive breast can-cer and carcinoma in situ of the breast. Cancer Causes Control 2003;14:915–22.
65. Harris RE, Namboodiri KK, Farrar WB. Nonsteroidal antiinflammatorydrugs and breast cancer. Epidemiology 1996;7:203–5.
66. Neugut AI, Rosenberg DJ, Ahsan H, Jacobson JS, Wahid N, Hagan M,et al. Association between coronary heart disease and cancers of thebreast, prostate, and colon. Cancer Epidemiol Biomarkers Prev 1998;7:869–73.
67. Hankinson SE, Colditz GA, Willett WC. Towards an integrated model forbreast cancer etiology: the lifelong interplay of genes, lifestyle, and hor-mones. Breast Cancer Res 2004;6:213–8.
68. GatesMA, Tworoger SS, Eliassen AH,Missmer SA,Hankinson SE. Analgesicuse and sex steroid hormone concentrations in postmenopausal women.Cancer Epidemiol Biomarkers Prev 2010;19:1033–41.
69. Anderson WF, Chu KC, Chatterjee N, Brawley O, Brinton LA. Tumorvariants by hormone receptor expression in white patients with node-negative breast cancer from the surveillance, epidemiology, and end resultsdatabase. J Clin Oncol 2001;19:18–27.
70. Howe LR. Inflammation and breast cancer. Cyclooxygenase/prostaglandinsignaling and breast cancer. Breast Cancer Res 2007;9:210.
71. Suissa S. Immortal time bias in pharmaco-epidemiology. Am J Epidemiol2008;167:492–9.
www.aacrjournals.org Cancer Epidemiol Biomarkers Prev; 24(11) November 2015 1655
Aspirin Use and Risk of Breast Cancer
Cancer Research. by guest on August 28, 2020. Copyright 2015 American Association forhttps://bloodcancerdiscov.aacrjournals.orgDownloaded from