
Cancer Biology Course Tuesdays, 12 noon, Farrell Teacher Center, Holden Auditorium, All students,...
35
Cancer Biology Course Tuesdays, 12 noon, Farrell Teacher Center, Holden Auditorium, All students, Postdocs, faculty, staff welcome Schedule for 2010 Course Jan 19 - Lee Ratner – Intro Jan 26 – Len Maggi - Translational Regulation of Cancer Feb 2 - Laura Beirut - Genetics of Lung Cancer Prevention Feb 9 - Dennis Hallahan – Radiosensitizers Feb 16 – Tom Ellenberger - Molecular Logic of DNA Repair Feb 23 – David Linehan - Immune Dysregulation of Pancreatic Ca Mar2 – Will Gilanders - Breast Ca Vaccine Mar 9 –Elaine Mardis – Genomics of Breast Ca Mar 16 – To be scheduled Mar 23 - You - ATM, DNA Damage Signaling and Cancer *Mar 30 - Lihong Wang - Photoacoustic Imaging *Apr 6 – Fehniger - microRNAs and hematologic malignancies Apr 13 - Mills - Metaplasia and the Mists of change: the molecular basis of gastric cancer Apr 20 - ? Visiting Speaker Apr 27 - ? Visiting Speaker Attendance of all sessions & active discussion esp during presentation classic paper WebSite:http://www.siteman.wustl.edu/physician/ prof_education/courses_online.shtml Format: 45 min didactic/30 min discussion
-
Upload
lilian-walton -
Category
Documents
-
view
213 -
download
0
Transcript of Cancer Biology Course Tuesdays, 12 noon, Farrell Teacher Center, Holden Auditorium, All students,...

Cancer Biology CourseTuesdays, 12 noon, Farrell Teacher Center, Holden Auditorium, All students,Postdocs, faculty, staff welcome
Schedule for 2010 CourseJan 19 - Lee Ratner – IntroJan 26 – Len Maggi - Translational Regulation of CancerFeb 2 - Laura Beirut - Genetics of Lung Cancer PreventionFeb 9 - Dennis Hallahan – RadiosensitizersFeb 16 – Tom Ellenberger - Molecular Logic of DNA RepairFeb 23 – David Linehan - Immune Dysregulation of Pancreatic CaMar2 – Will Gilanders - Breast Ca VaccineMar 9 –Elaine Mardis – Genomics of Breast CaMar 16 – To be scheduledMar 23 - You - ATM, DNA Damage Signaling and Cancer*Mar 30 - Lihong Wang - Photoacoustic Imaging*Apr 6 – Fehniger - microRNAs and hematologic malignanciesApr 13 - Mills - Metaplasia and the Mists of change: the molecular basis of gastric cancerApr 20 - ? Visiting Speaker Apr 27 - ? Visiting SpeakerAttendance of all sessions & active discussion esp during presentation classic paper
WebSite:http://www.siteman.wustl.edu/physician/prof_education/courses_online.shtmlFormat: 45 min didactic/30 min discussion

Introduction
• History• Epidemiology• Biology• Diagnosis• Treatment• Prevention• Social Issues
See Perspectives in Nature Reviews in Cancer
JCO Dec 10 2009, Advances in Cancer

Cancer – Historical Perspective1600 BC Egyptian physician record 1st description of breast cancer
460 BC Hippocrates uses “carcinos” to describe tumors (Greek – crab)
129 AD Galen attributes cancer to black bile
1660 Mastectomy for breast cancer
1713 Ramazzini notes absence of cervical but increased breast ca in nuns
1775 Pott describes scrotal cancer in chimney sweeps
1838 Muller describes cancer as abnormalities of cells
1896 Grubbe administers xrays to cancer patient

Cancer – 20th Century1903 Radium isolated by Curies used for tumor treatment
1913 American Cancer Society founded
1928 Papanicolau provides basis for PAP smears
1937 Roosevelt creates NCI
1941 Huggins used hormones to treat prostate Ca
1948 Hitchings uses 6MP for childhood leukemia
1955 MTX used for solid tumor
1957 IFN and FU introduced
1966 NCI testing for cancer-causing chemicals
1970 DeVita develops MOPP for Hodgkin

Cell-cycle checkpoints (Hemmungseinrichtung: inhibitory mechanism) that would allow cell division only when a specific external stimulus is experienced by the cell.
The clonal origin of tumours.
Genetic mosaicism.
Tumour-suppressor genes (Teilungshemmende Chromosomen), the effects of which can be overcome by external signals, and which are physically lost in progressively growing tumours.
Oncogenes (Teilungsfoerdernde Chromosomen) that become amplified (im permanenten Übergewicht) during tumour development.
Tumour progression from benign to malignant, involving sequential changes of increased growth-stimulatory chromosomes and loss of growth-inhibitory chromosomes.
Cancer predisposition through inheritance of chromosomes (genes) that are less able to suppress malignancy.
Cancer predisposition through inheritance of genes that cause aberrant mitoses.
Inheritance of the same 'weak chromosome' from both parents leads to homozygosity for the defective chromosome and, consequently, to high-penetrance cancer syndromes — for example, xeroderma pigmentosum.
The role of wounding and inflammation in tumour promotion.
Loss of cell adhesion in metastasis.
Sensitivity of malignant cells to radiation therapy.
Boveri’s Predictions (1902)

Acquired Capabilities of Cancer
Genetic and epigenetic instability
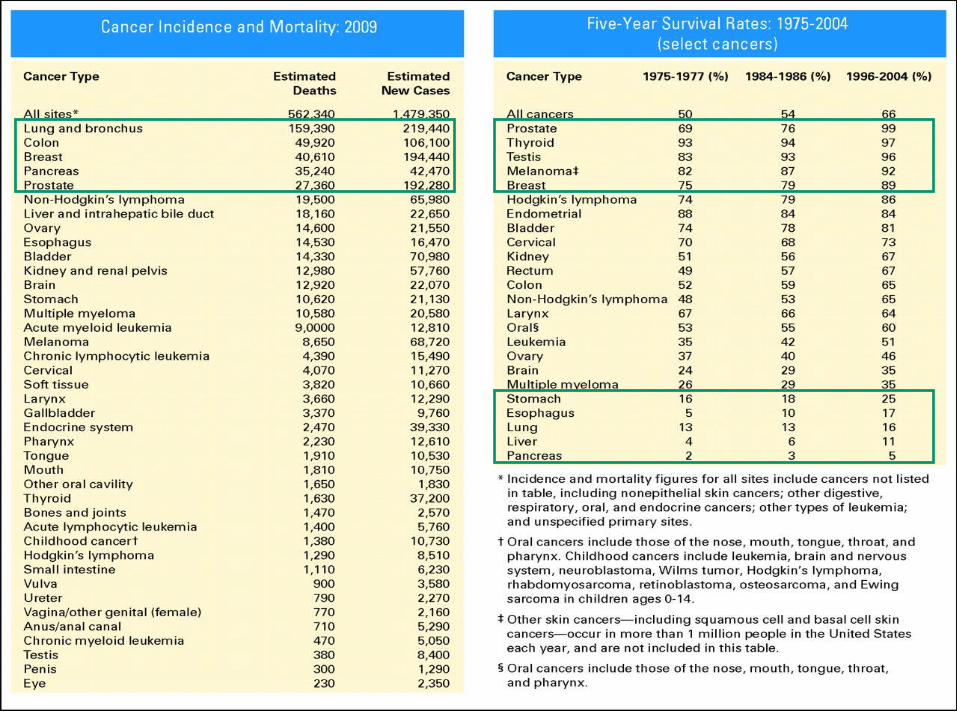


Estimated proportion of cancer in US that could have been avoided by changes in
each category of non-genetic cancer causes – Risk
– Structured-data summaries
– Meta-analysis
– Pooled analysis
– Prospective studies
– Retrospective studies
– Bias
– Confounding
– Randomized controlled trials
– Statistical power

Multiple Steps to Cancer
Reversibility?

Cancer Genome Atlas - Glioblastoma
Mardis

ChromosomalTranslocations in CML and Solid
Tumors1961-Nowell & Hungerford – Ph chromosome
1972 Rowley t9;22 CML
t8;14 Burkitt, t15;17 APL,
t11;22 Ewings
1984 – BCR-ABL fusion
1988 – Huang – ATRA
1998 – Druker – Imatinib, Gleevec
2009 – EML4-ALK in Lung Cancer

Cancer Stem Cells
Stem cells in adult somatic tissues, Scenarios involving cancer stem cells

Metastasis
Paget, 1889 “seed and soil”

Bevacizmab slows disease progression of metastatic renal cell
carcinoma

Signal Transduc-
tion by HER
family

Trastuzumab improves survival for patients with HER2+ gastric cancer
Fig. 1. Her-2 IHC (A) and HE (B) in intestinal-type gastric cancer (magnification ×100). FISH analysis shows homogenous amplification of HER-2 (C) and TOP2A (D) in gastric carcinoma (clusters of red signals). Green signals represent centromere 17. Cell nuclei are counterstained with blue dye.
International, phase III trail found 26% reduction in deaths with addition of trastuzumab to standard chemo
Mills

Platinum-Based Chemotherapy plus Cetuximab in Head and Neck
CancerNEJM Sep 08
Improved survival with cetuximab

The molecular circuitry
of cancer.*
**


Maggi
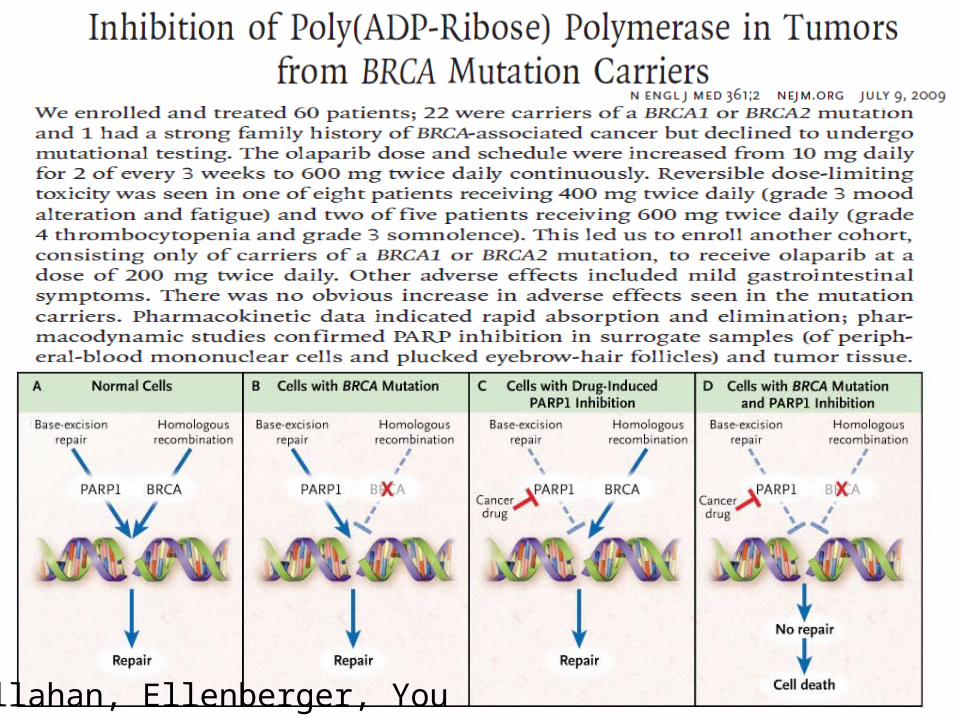
Hallahan, Ellenberger, You

Fostamatinib, Syk inhibitor, shrinks CLL
Fehniger

Old, 1996

Lancet. 2009 Jun.Safety, immunogenicity, and efficacy of
quadrivalent human papillomavirus (types 6, 11, 16, 18) recombinant vaccine in women aged 24-45 years: a randomised, double-blind trial.

New Linkages in ImagingNew Linkages in Imaging
MolecularMolecularBiologyBiology
RadiologyRadiology
MolecularMolecularImagingImaging
XRT
Surgery
Nanotechnology; BLI Wong

Phase I, II, III
CR, PR, stable, progressive
QoL, DFS, OS, surrogate markers – cancer Ag, PET
NCI, FDA, IRB


Oncotype Dx for stage II colon cancer4 studies (total n=1,851; 761 candidate genes) identified 48 genes associated with recurrence risk and 66 genes predictive of 5FU/LV benefit
Multivariate analysis, in the context of stage, grade, nodes examined, and MSI status, yielded 18 genes (7 prognostic genes, 6 predictive genes, 5 reference genes) and separate prognostic recurrence score (RS) and predictive treatment score (TS) algorithms.
In validation study, tumor blocks of 1,490 pts with blocks had stage II colon cancer and RT-PCR was successful in 1,436 eligible pts (711 Sx, 725 Sx+5FU/LV)
Median FU=6.6 yrs.
In the primary analysis pts following Sx, the RS predicted recurrence risk (HR/25 units=1.58, 95% CI 1.15-2.15; p=0.004).
The RS also predicted DFS (p=0.01) and OS (p=0.04).
Recurrence risk increased monotonically with increasing RS.
In multivariate analyses, RS retained prognostic significance (p=0.008) independent of mismatch repair (MMR), T stage, nodes examined, grade, and lymphovascular invasion. MMR deficiency (HR=0.31, 95% CI 0.15-0.63; p<0.001) and T4 stage (HR=1.94, 95% CI 1.35-2.79; p=0.005), together ~25% of pts, also were independently prognostic.
5FU/LV benefit was significant (p<0.001).
However, TS was not validated as a predictor of 5FU/LV benefit (interaction p=0.19).

J Natl Cancer Inst. 2009 January; Meta-analysis of Risk Reduction Estimates Associated With Risk-Reducing Salpingo-
oophorectomy in BRCA1 or BRCA2 Mutation Carriers
RRSO was also associated with a statistically significant reduction in the risk of BRCA1/2-
associated ovarian or fallopian tube cancer (HR = 0.21; 95% CI = 0.12 to 0.39).

Animal models & safety

Quality of Life & Prevention Advances
US cancer screening rates are low or decliningPSA screening has limited benefit
Survivors of childhood cancer are not receiving recommended cancer screening testsAndrogen receptor inhibitor reduces prostate cancer riskSupplements (vit E, minerals) ineffective False positive screening tests increase number of f/u testsStudies identify determinants of and effects of end-of-life care


ASCO Recommendations
Strengthen nation’s clinical research
funding, support, insurers, regulatory barriers
High quality cancer care for all

Acquired Capabilities of Cancer
Genetic & epigenetic instability
Hanahan & Weinberg
Cell 100:57-70, 2000
Discussion Paper


















