
CANADIAN STROKE BEST PRACTICE …€¦ · · 2017-11-21Mood, Cognition and Fatigue Following...
38
Mood, Cognition and Fatigue Following Stroke Evidence Tables Vascular Cognitive Impairment: Screening and Assessment Eskes G and Lanctot K (Writing Group Chairs) on Behalf of the Canadian Stroke Best Practice Recommendations Mood, Cognition and Fatigue Writing Group © 2015 Heart and Stroke Foundation CANADIAN STROKE BEST PRACTICE RECOMMENDATIONS
Transcript of CANADIAN STROKE BEST PRACTICE …€¦ · · 2017-11-21Mood, Cognition and Fatigue Following...

Mood, Cognition and Fatigue Following Stroke Evidence Tables
Vascular Cognitive Impairment: Screening and Assessment
Eskes G and Lanctot K (Writing Group Chairs) on Behalf of the Canadian Stroke Best Practice Recommendations
Mood, Cognition and Fatigue Writing Group
© 2015 Heart and Stroke Foundation
CANADIAN STROKE BEST PRACTICE RECOMMENDATIONS

Heart and Stroke Foundation Mood, Cognition and Fatigue Following Stroke Canadian Stroke Best Practice Recommendations Evidence Tables
VCI: Screening and Assessment 2015 2
Table of Contents Search Strategy………………………………………………………………….……………………………………………………………………….…. 3
Published Guidelines…………………………………………………………….……………………………………….………………………………… 4
What is the prevalence of cognitive impairment after stroke?............................................................................................................................ 9
What is the impact of neuropsychological/neurocognitive deficits on stroke outcome?..................................................................................... 15
What tools are used to assess VCI?.................................................................................................................................................................. 21
Imaging………………………………………………………………………………………………………………………………………………………. 22
Cognitive Tests……………………………………………………………………………………………………………………………………………… 25
What are the differences between the tools used to assess VCI?..................................................................................................................... 29
Does treatment of vascular risk factors reduce the risk of cognitive decline?................................................................................................... 31
Reference List……………………………………………………………………………………………………………………………………………….. 35

Heart and Stroke Foundation Mood, Cognition and Fatigue Following Stroke Canadian Stroke Best Practice Recommendations Evidence Tables
VCI: Screening and Assessment 2015 3
Search Strategy
The Medline, Embase, PsycInfo, and Cochrane databases were searched using the terms [stroke OR cerebrovascular disorders] and [cognition OR neuropsychology OR mild cognitive impairment OR cognitive training OR cognitive rehabilitation]. The title and abstract of each article was reviewed for relevance. Bibliographies were reviewed to find additional relevant articles. Articles were excluded if they were: non-English, commentaries, case-studies, narrative, book chapters, editorials, non-systematic review, or conference abstracts. Additional searches for relevant best practice guidelines were completed and included in a separate section of the review. A total of 67 articles and 6 guidelines were included and were separated into categories designed to answer specific questions.
Included
Eligibility
Screening
Identification Cochrane, Medline, and Embase were searched
Titles and Abstracts of each study were reviewed. Bibliographies of major reviews or meta-analyses were searched for additional relevant articles
Excluded articles: Non-English, Commentaries, Case-Studies, Narratives, Book Chapters, Editorials, Non-systematic Reviews (scoping reviews), and conference abstracts.
Included Articles: English language articles, Cochrane reviews, RCTs.
A total of 67 Articles and 6 guidelines

Heart and Stroke Foundation Mood, Cognition and Fatigue Following Stroke Canadian Stroke Best Practice Recommendations Evidence Tables
VCI: Screening and Assessment 2015 4
Published Guidelines Guideline Recommendations National Stroke Foundation. Clinical Guidelines for Stroke Management 2010 Recommendations. Melbourne Australia.
Assessment of Cognition 1. All patients should be screened for cognitive and perceptual deficits using validated and reliable screening tools
(GPP). 2. Patients identified during screening as having cognitive deficits should be referred for comprehensive clinical
neuropsychological investigations (GPP). Attention and Concentration
1. Cognitive rehabilitation can be used in stroke survivors with attention and concentration deficits (C). Memory
1. Any patient found to have memory impairment causing difficulties in rehabilitation or adaptive functioning should: • Be referred for a more comprehensive assessment of their memory abilities (GPP) • Have their nursing and therapy sessions tailored to use techniques which capitalize on preserved memory
abilities (GPP) • Be assessed to see if compensatory techniques to reduce their disabilities, such as notebooks, diaries,
audiotapes, electronic organizers and audio alarms, are useful (D) • Be taught approaches aimed at directly improving their memory (GPP) • Have therapy delivered in an environment as like the patient’s usual environment as possible to
encourage generalization (GPP) Executive functions
1. Patients considered to have problems associated with executive functioning deficits should be formally assessed using reliable and valid tools that include measures of behavioural symptoms (GPP).
2. External cues, such as a pager, can be used to initiate everyday activities in stroke survivors (C). In stroke survivors with impaired executive functioning, the way in which information is provided should be considered (C).
Intercollegiate Stroke Working Party. National clinical guideline for stroke, 4th edition. London: Royal College of Physicians, 2012.
Cognitive impairments 1. Interventions or patient management should be organised so that people with cognitive difficulties can participate in
the treatments and are regularly reviewed and evaluated. 2. Every patient seen after a stroke should be considered to have at least some cognitive losses in the early phase.
Routine screening should be undertaken to identify the patient’s broad level of functioning, using simple standardised measures (eg Montreal Cognitive Assessment (MOCA)).
3. Any patient not progressing as expected in rehabilitation should have a more detailed cognitive assessment to determine whether cognitive losses are causing specific problems or hindering progress.
4. Care should be taken when assessing patients who have a communication impairment. The advice from a speech and language therapist should be sought where there is any uncertainty about these individuals’ cognitive test results (see section 6.20).
5. The patient’s cognitive status should be taken into account by all members of the multidisciplinary team when planning and delivering treatment.
6. Planning for discharge from hospital should include an assessment of any safety risks from persisting cognitive

Heart and Stroke Foundation Mood, Cognition and Fatigue Following Stroke Canadian Stroke Best Practice Recommendations Evidence Tables
VCI: Screening and Assessment 2015 5
Guideline Recommendations impairments.
7. Patients returning to cognitively demanding activities (eg some work, driving) should have their cognition assessed formally beforehand.
Attention and concentration
1. Any person after stroke who appears easily distracted or unable to concentrate should have their attentional abilities (eg focused, sustained and divided) formally assessed.
2. Any person with impaired attention should have cognitive demands reduced through: • having shorter treatment sessions • taking planned rests • reducing background distractions • avoiding work when tired.
3. Any person with impaired attention should: • be offered an attentional intervention (eg Time Pressure Management, Attention Process Training,
environmental manipulation), ideally in the context of a clinical trial • receive repeated practice of activities they are learning.
Memory
1. Patients who complain of memory problems and those clinically considered to have difficulty in learning and remembering should have their memory assessed using a standardised measure such as the Rivermead Behavioural Memory Test (RBMT).
2. Any patient found to have memory impairment causing difficulties in rehabilitation or undertaking activities should: • be assessed medically to check that there is not another treatable cause or contributing factor (eg delirium,
hypothyroidism) • have their profile of impaired and preserved memory abilities determined (as well as the impact of any other
cognitive deficits on memory performance, for example attentional impairment) • have nursing and therapy sessions altered to capitalise on preserved abilities • be taught approaches that help them to encode, store and retrieve new information, for example, spaced
retrieval (increasing time intervals between review of information) or deep encoding of material (emphasising semantic features)
• be taught compensatory techniques to reduce their prospective memory problems, such as using notebooks, diaries, electronic organisers, pager systems and audio alarms
• have therapy delivered in an environment that is as similar to the usual environment for that patient as possible.
Executive Functioning
1. Any person who appears to have adequate skills to perform complex activities but who fails to organise the tasks needed should be formally assessed for the dysexecutive syndrome, for example using the Behavioural Assessment of the Dysexecutive Syndrome (BADS).
2. Any person with an executive disorder and activity limitation should be taught compensatory techniques. This may include internal strategies (eg self-awareness and goal setting) and/or external strategies (eg use of electronic organisers or pagers, or use of written checklists) ideally in the context of a clinical trial.
3. When a patient’s activities are affected by an executive disorder, the nature and effects of the impairment and ways of supporting and helping the patient should be discussed with others involved (eg family, staff).

Heart and Stroke Foundation Mood, Cognition and Fatigue Following Stroke Canadian Stroke Best Practice Recommendations Evidence Tables
VCI: Screening and Assessment 2015 6
Guideline Recommendations Psychological Care
1. Interventions for individual disorders of mood or cognition should be applied within the framework of a stepped care and comprehensive model.
2. Patients with continuing disorders should be considered for comprehensive interventions tailored towards developing compensatory behaviours and the learning of adaptive skills.
3. Within Step 1 care all patients after stroke should be screened within 6 weeks of diagnosis, using a validated tool, to identify mood disturbance and cognitive impairment.
4. Any patient assessed as having a cognitive impairment should be considered for referral to a specialist in cognitive aspects of stroke. Patients identified as having cognitive impairment or mood disorder should be reassessed before discharge decisions are taken.
Scottish Intercollegiate Guidelines Network (SIGN). Management of patients with stroke: Rehabilitation, prevention and management of complications, and discharge planning: A national clinical guideline, 2010. Edinburgh, Scotland.
• A full understanding of the patient’s cognitive strengths and weaknesses should be an integral part of the rehabilitation plan (GPP).
• Stroke patients should have a full assessment of their cognitive strengths and weaknesses when undergoing rehabilitation or when returning to cognitively demanding activities such as driving or work (GPP).
• Cognitive assessment may be carried out by occupational therapists with expertise in neurological care, although some patients with more complex needs will require access to specialist neuropsychological expertise (GPP).
Cognitive rehabilitation: “There is not yet sufficient evidence to support or refute the benefits of cognitive rehabilitation for patients with problems of attention or memory. When cognitive problems are suspected and relatives report personality change, the patient can be referred to a clinical psychologist to provide assessment and where appropriate, psychological intervention which may include carer education and support” (page 22)
VA/DoD clinical practice guideline for the management of stroke rehabilitation 2010.
Assessment of cognitive function 1. Assessment of arousal, cognition, and attention should address the following areas:
a. Arousal b. Attention deficits c. Visual neglect d. Learning and Memory deficits e. Executive function and problem-solving difficulties
2. There is insufficient evidence to recommend for the use of any specific tools to assess cognition. Several screening and assessment tools exist. (See Appendix B for standard screening instruments for cognitive assessment.)
Use of standardized assessments
1. Recommend that all patients should be screened for depression and motor, sensory, cognitive, communication, and swallowing deficits by appropriately trained clinicians, using standardized and valid screening tools. [C]
2. If depression, or motor, sensory, cognitive, communication, or swallowing deficits are found on initial screening assessment, patients should be formally assessed by the appropriate clinician from the coordinated rehabilitation team. [C]
Non-drug therapies for cognitive impairment
1. Recommend that patients be given cognitive re-training, if any of the following conditions are present:

Heart and Stroke Foundation Mood, Cognition and Fatigue Following Stroke Canadian Stroke Best Practice Recommendations Evidence Tables
VCI: Screening and Assessment 2015 7
Guideline Recommendations a. Attention deficits [A] b. Visual neglect [B] c. Memory deficits [B] d. Executive function and problem-solving difficulties [C]
2. Patients with multiple areas of cognitive impairment may benefit from a variety of cognitive re-training approaches that may involve multiple disciplines. [C]
3. Recommend the use of training to develop compensatory strategies for memory deficits in post-stroke patients who have mild short term memory deficits. [B]
Use of drugs to improve cognitive impairment
1. Consider using acetylcholinesterase inhibitors (AChEIs), specifically galantamine, donepezil, and rivastigmine, in patients with vascular dementia or vascular cognitive impairment in the doses and frequency used for Alzheimer’s disease.
2. Consider using the NMDA receptor inhibitor memantine (Namenda) for patients with vascular dementia (VaD) or vascular cognitive impairment (VCI). [B]
3. The use of conventional or atypical antipsychotics for dementia-related psychosis or behavioral disturbance should be used with caution for short term, acute changes.
4. Recommend against centrally acting a2-adrenergic receptor agonists (such as clonidine and others) and a1-receptor antagonists (such as prazosin and others) as antihypertensive medications for stroke patients because of their potential to impair recovery. [D]
Recommend against the use of amphetamines to enhance motor recovery following stroke. [D]
Duncan PW, Zorowitz R, Bates B, et al. Management of adult stroke rehabilitation care: a clinical practice guideline. Stroke 2005;36:e100-e143.
Assessment of Cognition and Communication 1. Recommend that assessment of cognition, arousal, and attention address the following areas: learning and
memory, visual neglect, attention, apraxia, and problem solving. 2. The Working Group does not recommend for or against the use of any specific tools to assess cognition. Several
screening and assessment tools exist. Appendix D includes standard instruments for assessment of cognition. The use of standardized assessment tools
1. Recommend that all patients be screened for depression and motor, sensory, cognitive, communication, and swallowing deficits by appropriately trained clinicians, using standardized and valid screening tools.
2. Recommend that if depression and motor, sensory, cognitive, communication, and swallowing deficits are found, all patients should be formally assessed by the appropriate clinician from the coordinated rehabilitation team.
Cognitive Remediation 2. Recommend that patients be assessed for cognitive deficits and be given cognitive retraining, if any of the following
conditions are present: Attention deficits, Visual neglect, Memory deficits, or Executive function and problem-solving difficulties
3. Patients with multiple areas of cognitive impairment may benefit from a variety of cognitive retraining approaches that may involve multiple disciplines. Recommend the use of training to develop compensatory strategies for memory deficits in poststroke patients who have mild short-term memory deficits.
Gorelick PB, Scuteri A, Black SE, et al. Vascular contributions to cognitive impairment and dementia: a statement for
Pharmacological therapy: 1. Donepezil can be useful for cognitive enhancement in patients with VaD (Class IIa; Level of Evidence A). 2. Administration of galantamine can be beneficial for patients with mixed Alzheimer disease/VaD (Class IIa; Level of
Heart and Stroke Foundation Mood, Cognition and Fatigue Following Stroke Canadian Stroke Best Practice Recommendations Evidence Tables
VCI: Screening and Assessment 2015 8
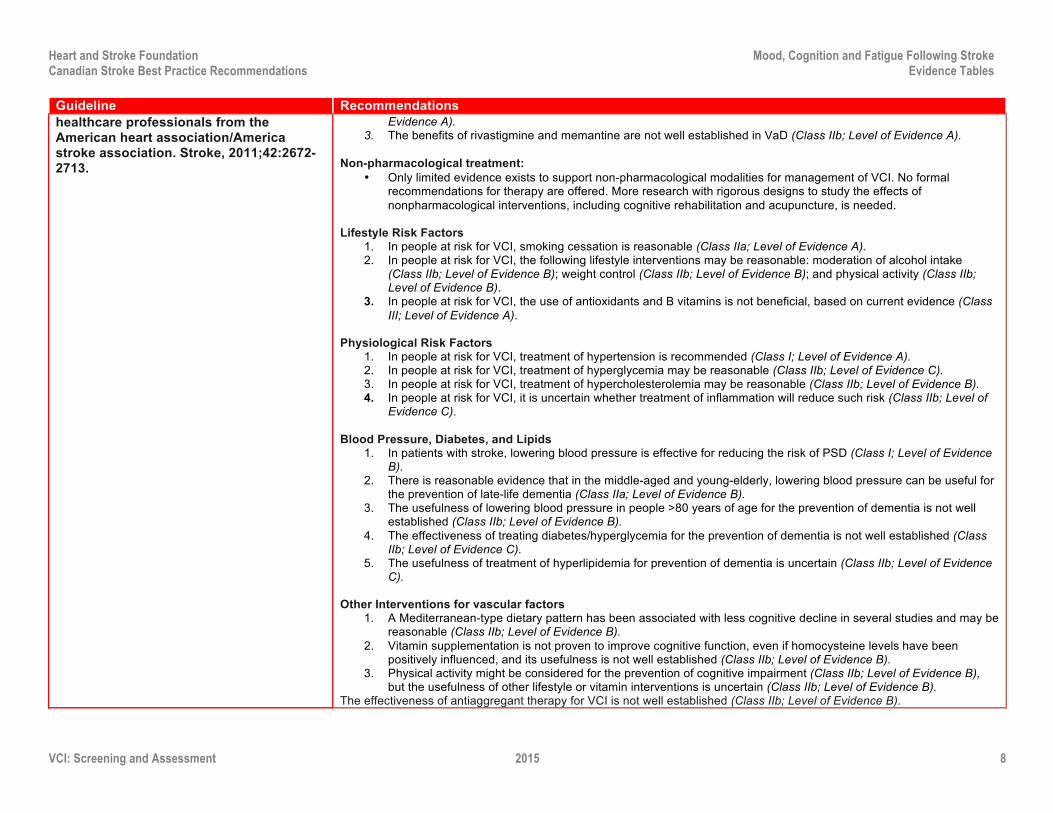
Guideline Recommendations healthcare professionals from the American heart association/America stroke association. Stroke, 2011;42:2672-2713.
Evidence A). 3. The benefits of rivastigmine and memantine are not well established in VaD (Class IIb; Level of Evidence A).
Non-pharmacological treatment:
• Only limited evidence exists to support non-pharmacological modalities for management of VCI. No formal recommendations for therapy are offered. More research with rigorous designs to study the effects of nonpharmacological interventions, including cognitive rehabilitation and acupuncture, is needed.
Lifestyle Risk Factors
1. In people at risk for VCI, smoking cessation is reasonable (Class IIa; Level of Evidence A). 2. In people at risk for VCI, the following lifestyle interventions may be reasonable: moderation of alcohol intake
(Class IIb; Level of Evidence B); weight control (Class IIb; Level of Evidence B); and physical activity (Class IIb; Level of Evidence B).
3. In people at risk for VCI, the use of antioxidants and B vitamins is not beneficial, based on current evidence (Class III; Level of Evidence A).
Physiological Risk Factors
1. In people at risk for VCI, treatment of hypertension is recommended (Class I; Level of Evidence A). 2. In people at risk for VCI, treatment of hyperglycemia may be reasonable (Class IIb; Level of Evidence C). 3. In people at risk for VCI, treatment of hypercholesterolemia may be reasonable (Class IIb; Level of Evidence B). 4. In people at risk for VCI, it is uncertain whether treatment of inflammation will reduce such risk (Class IIb; Level of
Evidence C). Blood Pressure, Diabetes, and Lipids
1. In patients with stroke, lowering blood pressure is effective for reducing the risk of PSD (Class I; Level of Evidence B).
2. There is reasonable evidence that in the middle-aged and young-elderly, lowering blood pressure can be useful for the prevention of late-life dementia (Class IIa; Level of Evidence B).
3. The usefulness of lowering blood pressure in people >80 years of age for the prevention of dementia is not well established (Class IIb; Level of Evidence B).
4. The effectiveness of treating diabetes/hyperglycemia for the prevention of dementia is not well established (Class IIb; Level of Evidence C).
5. The usefulness of treatment of hyperlipidemia for prevention of dementia is uncertain (Class IIb; Level of Evidence C).
Other Interventions for vascular factors
1. A Mediterranean-type dietary pattern has been associated with less cognitive decline in several studies and may be reasonable (Class IIb; Level of Evidence B).
2. Vitamin supplementation is not proven to improve cognitive function, even if homocysteine levels have been positively influenced, and its usefulness is not well established (Class IIb; Level of Evidence B).
3. Physical activity might be considered for the prevention of cognitive impairment (Class IIb; Level of Evidence B), but the usefulness of other lifestyle or vitamin interventions is uncertain (Class IIb; Level of Evidence B).
The effectiveness of antiaggregant therapy for VCI is not well established (Class IIb; Level of Evidence B).

Heart and Stroke Foundation Mood, Cognition and Fatigue Following Stroke Canadian Stroke Best Practice Recommendations Evidence Tables
VCI: Screening and Assessment 2015 9
Evidence Tables What is the prevalence of cognitive impairment after stroke?
Study/Type Quality Rating Sample Description Method Outcomes Key Findings and Recommendations
Douiri et al. 2013 UK Cohort Study
n/a 4,212 patients with first ever stroke or TIA.
As part of the South London Stroke Register study, participants underwent cognitive screening in the acute phase of stroke, 3 months post-stroke onset, and annually thereafter.
Mini Mental State Exam (MMSE) or the Abbreviated Mental Test (AMT): the MMSE was used for the 1st five years and the AMT for thereafter.
Of the 4,212 participants, 1,618 completed a cognitive assessment and 1,229 completed the 3 month follow-up. The prevalence of cognitive impairment was 22% (95% CI 21.2 to 27.8) at 3 months, 22% (95% CI 17.4 to 26.8) and 5 years, and 21% (95% CI 3.6 to 63.6) at 14 years. The prevalence of post-stroke cognitive impairment was significantly associated with older age, black ethnicity, and low SES.
Yu et al. 2013 Korea Observational
n/a 620 ischemic stroke patients. Patients with severe medical conditions, neurological conditions, or aphasia were excluded. 69% of those screened for eligibility were included in the study.
Participants were enrolled in the study within 2 weeks of the index stroke event and underwent comprehensive cognitive evaluation 3 months post-stroke.
The Korean Vascular Cognitive Impairment Harmonization Standards Neuropsychological (K-VCIHS-NP) protocol, the Mini-Mental Status Exam (MMSE), and the Informant Questionnaire of Cognitive Decline in the Elderly (IQCODE).
According to results from the VCIHS-NP protocol, vascular cognitive impairment (VCI) without dementia was detected in 49.9% (n=176) of participants, whereas vascular dementia was detected in 12.7% (n=45) of participants. 37.4% (n=132) of participants demonstrated normal cognition. According to results from the MMSE, VCI without dementia and vascular dementia were detected in 9.9% (n=35) and 16.4% (n=58) of participants. Lost to follow-up: 18.4%, with 43.1% not completing the follow-up VCIHS.
Bejot et al. 2011 France Cohort study
n/a 3948 patients with first-ever strokes.
As part of the Dijon Stroke Registry, cognitive function was evaluated by a neurologist within the first month of stroke. Dementia was diagnosed according to DSM III or IV criteria.
Prevalence of dementia. Of the 3,201 participants, 3201 (81%) completed a cognitive assessment. Of those assessed, 20.4% were diagnosed with post-stroke dementia. The prevalence of dementia varied from 23.7% (95% CI 20 to 27) in 1985-1990 to 19.3% (95% CI 16 to 22) in 1991-1996, 19% (95% CI 16 to 22) in 1997-2002, and 20.2% (95% CI 18 to 23) in 2003-2008. Significant temporal changes in the prevalence of dementia were identified in multivariate analysis, with both the 2nd and 4th time periods significantly differing from the 1st (p<0.05).
Racic et al. 2011 Bosnia and
n/a 251 stroke patients admitted to hospital.
Participants completed neuropsychological testing 3 months post-
Prevalence of dementia 3-months post-stroke.
At 3-months post-stroke, 19.5% (n=49) of participants met criteria for vascular dementia. Participants with dementia were significantly

Heart and Stroke Foundation Mood, Cognition and Fatigue Following Stroke Canadian Stroke Best Practice Recommendations Evidence Tables
VCI: Screening and Assessment 2015 10
Study/Type Quality Rating Sample Description Method Outcomes Key Findings and Recommendations
Herzegovina Observational
Patients with pre-stroke dementia or severe aphasia were excluded.
stroke. Diagnosis of dementia was defined using the NINDS-AIREN criteria.
more likely to have atrial fibrillation (p<0.01), ventricular arrhythmias (p<0.01), and previous stroke (p<0.05). Diagnosis with dementia at 3-months post-stroke was also significantly associated with greater cognitive and functional impairment at the time of stroke (p<0.05).
Wadley et al. 2011 REGARDS US Cohort
n/a 23,913 individuals 45 years of age or older residing in the US “stroke belt” (56%) or other US states (44%). Individuals with a history of stroke or cognitive impairment at baseline were excluded. 33% of those invited to participate were included in the study.
Baseline data was collected via telephone interview and home visit. Participants completed follow-up interviews by telephone twice per year, with the cognitive screen administered once per year. A cognitive battery was introduced in the 3rd study year and was administered once every 2 years.
Incidence cognitive impairment, defined as a score <5 on the Six-Item Screener (SIS).
8.1% (n=1,937) of participants were identified as being cognitively impaired at their most recent assessment (mean follow-up = 4.1 years). As compared to those who resided in other US states, participants living within the “stroke belt” (Alabama, Arkansas, Georgia, Louisiana, Mississippi, North Carolina, South Carolina, and Tennessee) had significantly increased odds of incident cognitive impairment (OR 1.18, 95% CI 1.07 to 1.30). Participants who were older, men, of African (vs. European) descent, and less educated were also at significantly increased odds of incident cognitive impairment.
Wolfe et al. 2011 UK Cohort study
n/a 3,373 patients with first ever stroke or TIA.
As part of the South London Stroke Register study, participants underwent cognitive screening in the acute phase of stroke, 3 months post-stroke onset, and annually thereafter.
Mini Mental State Exam (MMSE) or the Abbreviated Mental Test (AMT): the MMSE was used for the 1st five years and the AMT for thereafter.
Of the 3,373 participants, 223 completed the 10 year follow-up. The authors state that the rate of cognitive impairment declined during the first year post-stroke, fluctuated year-by-year until the eighth year, than increased to the tenth year. For 15-year outcomes from the South London Stroke Register Study, see Douiri et al. 2013 (above).
Delgado et al. 2010 Chile Observational
n/a 164 consecutively admitted stroke patients 60 years of age or older. Exclusion criteria: TIA, subarachnoid or juxtadural hematoma, other disorders of the central nervous system, and sever impairment (mRS>3). 46% of those assessed for eligibility were included.
Participants completed a cognitive assessment administered by a neuropsychologist at 3 and 12 months post-stroke.
Neuropsychological evaluation including the Mini-Mental State Exam (MMSE), the Mattis Dementia Rating Scale (MDR), and the Frontal Assessment Battery (FAB).
122 (74%) participants completed the 3 month follow-up. Of these, 81 (66%) were determined to have post-stroke cognitive impairment. 101 (52%) participants completed the 1 year follow-up. Of these, 39 (39%) were determined to have post-stroke cognitive impairment whereas 22 (22%) were diagnosed with dementia.

Heart and Stroke Foundation Mood, Cognition and Fatigue Following Stroke Canadian Stroke Best Practice Recommendations Evidence Tables
VCI: Screening and Assessment 2015 11
Study/Type Quality Rating Sample Description Method Outcomes Key Findings and Recommendations
Savva et al. 2010 UK Systematic review
n/a 16 articles reporting the incidence of all-cause dementia following symptomatic stroke.
Studies were identified through an electronic search strategy. Findings were summarized using a narrative approach.
Incidence of dementia. As compared to individuals who are stroke free, the authors report that history of stroke is associated with a doubling in the incidence of dementia in those 65 years of age or older. This increase in incident dementia is reported to be greatest in the period immediately following the index stroke event and decreases over time. For individuals >85 years of age, no difference was reported in terms of the incidence of dementia between those with and without a history of stroke.
Pendlebury et al. 2009 Systematic Review and Meta-analysis
n/a 73 articles (n=7511; 22 hospital-based cohorts and 8 population-based cohorts) reporting on consecutive patients with symptomatic stroke followed for at least 3 months.
Studies were identified through the use of electronic and manual search techniques. Pooled estimates of prevalence were calculated using the Mantel-Haenszel method. Cumulative incidence was estimated using logistic regression. Data pertaining to risk factors were pooled using fixed effects methods and reported as odds ratios. Random effects models were used if evidence of heterogeneity was observed.
Prevalence, incidence, and factors associated with pre-stroke and post-stroke dementia.
The prevalence of pre-stroke dementia at the time of stroke was estimated to be 14.4% (95% CI 12.0 to 16.8) in hospital based studies and 9.1 (95% CI 6.9 to 11.3) in population based studies. The prevalence of post-stroke dementia was estimated to be 41.3% (95% CI 29.6 to 53.1) for patients with recurrent stroke and 26.5% (95% CI 24.3 to 28.7) for patients with first or recurrent stroke in hospital-based studies (including patients with pre-stroke dementia) and 7.4% (95% CI 4.8 to 10.0) in population based studies (including patients with first-ever stroke but excluding those with pre-stroke dementia). The pooled cumulative incidence of post-stroke dementia was estimated to increase linearly at a rate of 3.0% (95% CI 1.3 to 4.7) per year. Some of the factors that were identified as being associated with significantly increased risk of post-stroke dementia include female sex (OR 1.3, 95% CI 1.1-1.6), low education (OR 2.5, 95% CI 1.8 to 3.4), diabetes (OR 1.4, 95% CI 1.2 to 1.7), atrial fibrillation (OR 2.0, 95% CI 1.4 to 2.8), and previous stroke (OR 1.9, 95% CI 1.5 to 2.3), as well as a number of other stroke factors, complications, and brain imaging factors.
Pendlebury 2009 Review
n/a This article presents a review of stroke-related dementia.
The author considers published literature pertaining to the rate of
Prevalence and incidence of stroke-related dementia and factors associated with
The author reports that pooled estimates of the prevalence of pre-stroke dementia at the time of stroke is 14.4% (95% CI 12.0 to 16.8) in

Heart and Stroke Foundation Mood, Cognition and Fatigue Following Stroke Canadian Stroke Best Practice Recommendations Evidence Tables
VCI: Screening and Assessment 2015 12
Study/Type Quality Rating Sample Description Method Outcomes Key Findings and Recommendations
pre-and post—dementia as well as associated risk factors.
pre- and post-stroke dementia.
hospital-based studies and 9.1% (95% CI 6.9 to 11.3) in population-based studies. The pooled estimate of the prevalence of post-stroke dementia is reported to be 41.3% (95% CI 29.6 to 53.1) in studies in which individuals with pre-stroke dementia are included and 7.4% (95% CI 4.8 to 10.0) in studies in which such individuals are excluded. The incidence of post-stroke dementia is reported to increase linearly at a rate of 3.0% (95% CI 1.3 to 4.7) per year. Some of the factors that are associated with post-stroke dementia include female sex, low education, recurrent stroke, incontinence, early seizures, acute confusion, abnormal EEG, hypoxic ischemic episodes, diabetes, atrial fibrillation, and dysphasia (all at p<0.05).
Yip et al. 2006 UK Case-control
n/a 4,075 individuals’ ≥65 years of age.
A two-phase sampling approach was used in which all participants completed a screening interview and select participants completed an assessment interview. The study was conducted in three waves, with participants screened but not assessed in the previous wave invited to participant in the next wave. The second and third waves were conducted 2 and 6 years following the first study wave.
Associations between risk factors and incident dementia.
Dementia was diagnosed in 277 participants at the second and third study waves. Incident dementia was significantly associated with older age (>90 vs 65-69: OR 25.6, 95% CI 11.6 to 56.9), female sex (OR 1.6, 95% CI 1.1 to 2.4), history of stroke (OR 2.1, 95% CI 1.1 to 4.2 or Parkinson’s Disease (OR 3.5%, 95% CI 1.3 to 9.3), and poor self-perceived health (OR 3.9, 95% CI 2.2 to 6.9). A significant trend was also observed between incident dementia and fewer years of education (p=0.02).
Mok et al. 2004 China Observational
n/a 75 patients with stroke associated with small vessel disease. Exclusion criteria: intracerebral hemorrhage, cortical or large subcortical
Participants completed a cognitive assessment 3-months post-stroke. Severity of cognitive symptoms were rated using the Clinical Dementia Rating Scale
Semi-structured clinical interview, Mini-Mental State Exam (MMSE), Alzheimer’s Disease Assessment Scale Cognition subscale (ADAS-cog), and the Mattis Dementia Rating Scale.
43% (n=32) of participants reported post-stroke cognitive decline. Reported cognitive symptoms included being memory problems (92.3%), slow thinking (74.4%), disorientation (17.9%), aphasia (17.9%), and disinhibition (2.6%). Pre-stroke cognitive impairment (OR 95.5, 95% CI 7.4 to 1248) and previous stroke (OR 11.35, 95% CI

Heart and Stroke Foundation Mood, Cognition and Fatigue Following Stroke Canadian Stroke Best Practice Recommendations Evidence Tables
VCI: Screening and Assessment 2015 13
Study/Type Quality Rating Sample Description Method Outcomes Key Findings and Recommendations
(>2 cm) infarcts, non-ischemic lesions, pre-stroke dementing illness not due to Alzheimer’s disease or vascular dementia, major depression, and communication problems precluding cognitive assessment.
(CDR). 1.6 to 79.7) were both associated with significantly increased odds of post-stroke cognitive decline. Stroke severity and executive dysfunction were each significantly associated with impaired functioning in instrumental activities of daily living (both at p<0.001).
Patel et al. 2003 UK Cohort Study
n/a 163 individuals with first-ever stroke. Patients with severe dysphasia were excluded.
As part of the South London Stroke Register, participants completed a cognitive assessment at 3 months and 1, 2, and 3 years post-stroke. Disability indices were also administered at the 1 year follow-up. Cognitive impairment was defined as an MMSE score <24.
The Mini Mental State Examination (MMSE), the Barthel Index, the Frenchay Activities Index (FAI), survival, and institutionalization.
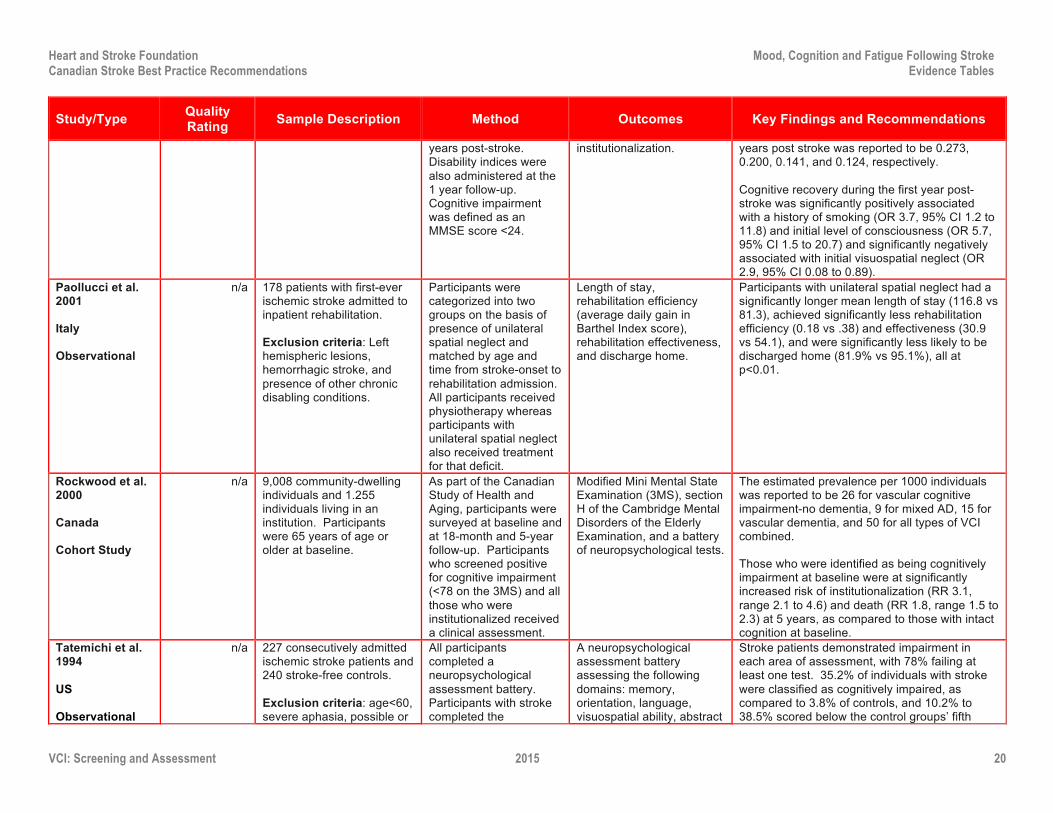
At 3 months post-stroke, 39.3% of participants were identified as being cognitively impaired, as compared to 35.3% at 1 year, 30.3% at 2 years, and 31.9% at 3 years. The prevalence rate per 1000 individuals at 3 months and at 1, 2, and 3 years post stroke was reported to be 0.273, 0.200, 0.141, and 0.124, respectively. Cognitive recovery during the first year post-stroke was significantly positively associated with a history of smoking (OR 3.7, 95% CI 1.2 to 11.8) and initial level of consciousness (OR 5.7, 95% CI 1.5 to 20.7) and significantly negatively associated with initial visuospatial neglect (OR 2.9, 95% CI 0.08 to 0.89).
Tham et al. 2002 Singapore Observational
n/a 252 patients with TIA or non-disabling stroke. Exclusion criteria: disabling stroke (Rankin >2), severe apraxia, and major affective or psychotic disorder.
Participants completed cognitive assessments at baseline (within 6-months post-stroke) and at a 1-year follow-up. Dementia was diagnosed according to the DSM-IV criteria.
The Vascular Dementia Battery (VDB) and the Mini-Mental State Exam (MMSE).
During the baseline assessment, 4% (n=10) of participants were diagnosed with dementia, whereas 40% (n=102) demonstrated cognitive impairment without dementia. 155 (62%) participants completed the 1-year follow-up assessment. Of those who were cognitively intact at baseline, 10% (n=9) were identified as cognitively impaired at follow-up. Of those who were cognitively impaired at baseline, 30% (n=19) demonstrated intact cognition and 11% (n=7) were diagnosed with dementia at follow-up. All participants diagnosed with dementia at baseline (n=7) met diagnostic criteria for dementia at follow-up.
Hoffmann et al. 2001
n/a 1000 consecutively admitted stroke patients. Participants who were not alert (n=5)
As part of the Durban Stroke Data Bank, “higher cortical function
Semi-quantitative bedside cognitive function screening.
Higher cortical functional deficits were detected in 60.7% (n=607) of participants, including 25.2% with aphasia, 14.5% with apraxia, 11.6%

Heart and Stroke Foundation Mood, Cognition and Fatigue Following Stroke Canadian Stroke Best Practice Recommendations Evidence Tables
VCI: Screening and Assessment 2015 14
Study/Type Quality Rating Sample Description Method Outcomes Key Findings and Recommendations
South Africa Observational
were excluded. deficit” screening was administered within 2 weeks of stroke
with amnesia, and 9.2% with frontal network symptoms. Cognitive impairment was identified in 22.5% of participants without apparent elementary neurologic deficits.
Madureira et al. 2001 Portugal Observational
n/a 237 patients with a supratentorial ischemic or hemorrhagic stroke. Patients with subarachnoid hemorrhage, TIA, cerebral venous thrombosis, and pre-stroke dependency were excluded.
Participants completed a neuropsychological evaluation 3 months post-stroke.
A neuropsychological battery that included the Mini-Mental State Examination (MMSE), a complementary cognitive battery, the Hamilton Rating Scale for Depression, and the Blessed Dementia Scale (BDS).
55.3% (n=131) of participants demonstrated impaired cognitive functioning in at least one cognitive domain. Of these participants, 27% demonstrated non-memory deficits, 7% demonstrated focal memory deficits, 9% demonstrated memory and other deficits, and 6% were diagnosed with dementia.
Rockwood et al. 2000 Canada Cohort Study
n/a 9,008 community-dwelling individuals and 1.255 individuals living in an institution. Participants were 65 years of age or older at baseline.
As part of the Canadian Study of Health and Aging, participants were surveyed at baseline and at 18-month and 5-year follow-up. Participants who screened positive for cognitive impairment (<78 on the 3MS) and all those who were institutionalized received a clinical assessment.
Modified Mini Mental State Examination (3MS), section H of the Cambridge Mental Disorders of the Elderly Examination, and a battery of neuropsychological tests.
The estimated prevalence per 1000 individuals was reported to be 26 for vascular cognitive impairment-no dementia, 9 for mixed AD, 15 for vascular dementia, and 50 for all types of VCI combined. Those who were identified as being cognitively impairment at baseline were at significantly increased risk of institutionalization (RR 3.1, range 2.1 to 4.6) and death (RR 1.8, range 1.5 to 2.3) at 5 years, as compared to those with intact cognition at baseline.
Hochstenbach et al. 1998 Netherlands Observational
n/a 229 consecutively admitted stroke patients and 33 stroke-free controls. Exclusion criteria: age <18 or >70, major physical illness (other than stroke), and mental disorder treated within the past 10 years.
Participants completed a neurological assessment. Results from stroke patients were compared to those obtained from control participants.
Neuropsychological assessment of each of the following domains: orientation, memory, attention / concentration, visuospatial / constructive, language, and arithmetic.
The authors report that approximately 70% of the participants demonstrated reduced information processing speed. 40% of participants demonstrated deficits in the domains of visuospatial/constructive, language, and arithmetic whereas 30% demonstrated memory deficits. The authors also report male stroke patients performed better than female patients on visuospatial tasks but worse on memory tasks. With a few exceptions, patients with left-sided lesions, hemorrhages, and aphasia tended to perform worse than those with right-sided lesions, infarcts, and no aphasia, respectively.
Tatemichi et al. 1994
n/a 227 consecutively admitted ischemic stroke patients and 240 stroke-free controls.
All participants completed a neuropsychological
A neuropsychological assessment battery assessing the following
Stroke patients demonstrated impairment in each area of assessment, with 78% failing at least one test. 35.2% of individuals with stroke

Heart and Stroke Foundation Mood, Cognition and Fatigue Following Stroke Canadian Stroke Best Practice Recommendations Evidence Tables
VCI: Screening and Assessment 2015 15
Study/Type Quality Rating Sample Description Method Outcomes Key Findings and Recommendations
US Observational
Exclusion criteria: age<60, severe aphasia, possible or probable Alzheimer’s disease.
assessment battery. Participants with stroke completed the assessment within 3 months of stroke onset.
domains: memory, orientation, language, visuospatial ability, abstract reasoning, and attention.
were classified as cognitively impaired, as compared to 3.8% of controls, and 10.2% to 38.5% scored below the control groups’ fifth percentile. The domains in which stroke patients showed the most impairment were memory, orientation, language, and attention. Cognitive impairment was significantly associated with dependent living (OR 2.4, 95% CI 1.3 to 4.4), controlling for age and physical impairment.
Ferro et al. 1988 Portugal Observational
n/a 254 stroke patients between the ages of 15 and 50 years.
Participants underwent a neuropsychological evaluation within 6 months of stroke onset.
A neuropsychological battery including 4 subtests for aphasia, the Token Test, and tests of alexia, agraphia, buccofacial limb, apraxia, and hemispatial neglect.
65% (n=166) of participants were reported to have aphasia. Broca’s aphasia was significantly more common than Wernicke’s aphasia (54 vs. 13, p<0.001). The authors reported that younger stroke patients are more likely to experience non-fluent aphasias than older stroke patients.
Note: CA: Concealed Allocation; ITT: Intention-to-treat
What is the impact of neuropsychology/neurocognitive deficits on stroke outcome?
Study/Type Quality Rating Sample Description Method Outcomes Key Findings and Recommendations
Rist et al. 2013 International Cohort Study
n/a 6,080 patients with stroke or TIA within 5 years of study enrollment. Patients with dementia or subarachnoid hemorrhage were excluded as were those with a clear indication or contraindication for treatment with a angiotensin-converting enzyme inhibitor.
As part of the PROGRESS trial, participants were assessed at baseline, 6 months, 12 months, and annually thereafter. Patients who scored <24 of the MMSE during any assessment were referred to a specialist experienced in diagnosing dementia.
Mini Mental State Exam (MMSE).
At baseline, 41% of participants obtained a score of 30 on the MMSE, whereas 29.1% had a score of 27-29, 22.5% had a score24-26, and 7.4% had a score <24. Participants were followed for a mean of 3.8 years, during which time 407 cases of dementia were diagnosed and 709 recurrent strokes occurred. As compared to those with a baseline MMSE of 30, those with lower baseline MMSE scores were at significantly greater risk of dementia:
• MMSE <24: RR 26.8, 95% CI 18.08 to 39.76
• MMSE 24-27: RR 6.59 (95% CI 4.54 to 9.55 • MMSE 28-29: RR 2.15 (95% CI 1.43 to 3.24

Heart and Stroke Foundation Mood, Cognition and Fatigue Following Stroke Canadian Stroke Best Practice Recommendations Evidence Tables
VCI: Screening and Assessment 2015 16
Study/Type Quality Rating Sample Description Method Outcomes Key Findings and Recommendations
The authors also reported that risk of dementia was more strongly associated with baseline MMSE scores in the absence of recurrent stroke.
Racic et al. 2011 Bosnia and Herzegovina Observational
n/a 251 stroke patients admitted to hospital. Patients with pre-stroke dementia or severe aphasia were excluded.
Participants completed neuropsychological testing 3 months post-stroke. Diagnosis of dementia was defined using the NINDS-AIREN criteria.
Prevalence of dementia 3-months post-stroke.
At 3-months post-stroke, 19.5% (n=49) of participants met criteria for vascular dementia. Participants with dementia were significantly more likely to have atrial fibrillation (p<0.01), ventricular arrhythmias (p<0.01), and previous stroke (p<0.05). Diagnosis with dementia at 3-months post-stroke was also significantly associated with greater cognitive and functional impairment at the time of stroke (p<0.05).
Toglia et al. 2011 US Observational
n/a 72 stroke patients admitted to an inpatient rehabilitation unit. Patients with incomplete intake assessments or impaired language comprehension were excluded. 31% of patients assessed for eligibility were included.
Participants completed the Mini-Mental State Exam (MMSE; administered by a physiatrist) and the Montreal Cognitive Assessment (MoCA; administered by an occupational therapist). All assessments were completed within 48 hours of admission.
The Mini-Mental State Exam (MMSE), the Montreal Cognitive Assessment (MoCA), the National Institutes of Health Stroke Scale (NIHSS), and the Functional Independence Measure (FIM).
MMSE and MoCA scores were significantly correlated with each other (r=0.79, p<0.001), although mean scores were significantly lower on the MoCA than on the MMSE (17.8 vs. 24.4, p<0.01). Using a cutoff score of 26 on the MoCA and 27 on the MMSE, 89% vs. 63% of participants were detected as having cognitive impairment, respectively. The authors also note that, as compared to the MMSE, the MoCA demonstrated a less pronounced ceiling effect and greater internal reliability. In a linear regression, the MoCA visuo-executive subtest was significantly associated with discharge motor FIM score, controlling for NIHSS, age, and motor FIM score at admission (p<0.05). In similar regression models neither the MoCA nor the MMSE total scores were significantly predictive of functional motor gain.
Viscogliosi et al. 2011 Canada Observational
n/a 197 stroke patients discharged home from hospital. Exclusion criteria: age<65 years, neurodegenerative disease, including Alzheimer’s disease and Parkinson’s disease.
Participants completed measures to assess participation and cognitive status. Participation level was compared between those with and without cognitive impairment.
Assessment of Life Habits (Life-H) and a neuropsychological assessment battery.
Participants with memory deficits had reduced participation in the communication (p=0.006) and leisure (p=0.03) domains, whereas visual perceptual deficits were associated with reduced participation in the nutrition (p=0.02), communication (p=0.004), and responsibilities (p<0.001) domains. Language deficits were associated with reduced participation in the communication (p<0.001), responsibilities (p<0.001), community life (p=0.001), and leisure (p=0.02) domains.

Heart and Stroke Foundation Mood, Cognition and Fatigue Following Stroke Canadian Stroke Best Practice Recommendations Evidence Tables
VCI: Screening and Assessment 2015 17
Study/Type Quality Rating Sample Description Method Outcomes Key Findings and Recommendations
Barker-Collo et al. 2010 New Zealand Observational
n/a 307 stroke patients. As part of the Auckland Stroke Outcomes study, participants completed cognitive and physical functioning assessments 5-years following the onset of stroke.
A neuropsychological test battery, the modified Rankin Scale, and the Geriatric Depression Scale.
Overall, the majority of participants demonstrated cognitive abilities within the average range, whereas 30-50% demonstrated decreased cognitive functioning on most measures, with the most common deficits being in the executive functioning and information processing speed domains.
Brodaty et al. 2010 Australia Observational
n/a 202 consecutive patients admitted to hospital with ischemic stroke and 97 matched community-residing controls. Exclusion criteria: previous stroke, pre-stroke dementia, age>85, hemorrhagic stroke, TIC, and presence of severe aphasia.
Participants with stroke completed study assessments at 3-7 days post-stroke, 3-6 months later, and again at 1, 3, and 5 years following stroke. Matched control participants completed study assessments at baseline and at 1, 3, 5 year follow-up. All stroke participants and 86 control participants underwent neuroimaging during the 3-month/baseline assessment. Participants were followed to capture mortality and institutionalization for a total of 10-years.
Mortality, institutionalization, Mini-Mental State Exam (MMSE), National Adult Reading Test-Revised (NART-R), European Stroke Scale (ESS), Activities of Daily Living (ADLs), and Instrumental ADLs.
74 (36.6%) stroke participants survived and completed the 5-year follow-up, as compared to 76 (78.4%) control participants. The cumulative survival rate for stroke as compared to control participants was 97% vs. 99% at 1-year, 84% vs. 99% at 3-years, 73% vs. 96% at 5-years, and 18% vs. 90% at 10 years (8.9 years for controls). Mean survival time was significantly shorter for stroke as compared to control participants (p<0.001). Significant predictors of mortality included cognitive impairment, older age, functional dependence, and lower education. Whereas none of the control participants were institutionalized during the study period, 5% of stroke participants was institutionalized at 1 year, 12% at 3 years, 24% at 5 years, and 32% at 10 years. Significant predictors of institutionalization were older age and functional dependence.
Cederfeldt et al. 2010 Sweden Observational
n/a 45 stroke patients. Exclusion criteria: age <65 years, low consciousness, severe medical conditions, severe aphasia, and severe dementia.
Participants completed assessments of physical and cognitive functioning during hospitalization for stroke and at 6- and 12-month follow-ups.
The Barthel Index, the Cognitive Impairment Questionnaire, The National Institute of Health Stroke Scale, Mini-Mental State Exam, and a neuropsychological test battery.
The authors report that participants with post-stroke cognitive impairment at baseline (n=6) did not demonstrate improvement in personal ADLs or cognitive functioning at the 1-year follow-up, whereas significant improvement was observed for participants free of cognitive impairment (n=39) in terms of personal ADLs and most of the cognitive domains assessed.
Narasimhalu et al. 2011 Singapore
n/a 419 patients with non-disabling stroke or TIA who were free of dementia at baseline.
As part of the ESPIRIT study, participants completed a neuropsychological assessment at 3-months
A neuropsychological test battery.
Of the 419 participants, 212 (51%) had no cognitive impairment, 109 (26%) had mild cognitive impairment without dementia (CIND), and 98 (23%) had moderate CIND. In multivariate analyses, mild and moderate CIND

Heart and Stroke Foundation Mood, Cognition and Fatigue Following Stroke Canadian Stroke Best Practice Recommendations Evidence Tables
VCI: Screening and Assessment 2015 18
Study/Type Quality Rating Sample Description Method Outcomes Key Findings and Recommendations
Cohort study post-stroke and annually for 5 years.
were each significantly associated with increased risk of dependency (HR 7.22 and 8.32, respectively), whereas moderate CIND was significantly associated with increased risk of death (HR 3.81).
Narasimhalu et al. 2009 Singapore Cohort study
n/a 362 patients with non-disabling stroke or TIA who were free of dementia at baseline.
As part of the ESPIRIT study, participants completed a neuropsychological assessment at 3-months post-stroke and annually for 5 years.
A neuropsychological test battery.
During the mean 3.4 year follow-up, 24 (6.6%) participants developed incident dementia. Presence of cognitive impairment without dementia and multiple domain mild cognitive impairment with a amnestic component were each significantly associated with increased risk of incident dementia in both univariate (HR 22.5, 95% CI 5.2 to 97.2, and HR 6.43, 95% CI 1.3 to 31.7, respectively) and multivariable analyses (HR 19.3, 95% CI 4.5 to 83.4, and HR 5.77, 95% CI 1.2 to 28.0, respectively).
Barker-Collo and Feigin 2006 New Zealand Review
n/a This article reviews published literature examining the impact of neuropsychological deficits on post-stroke functional outcomes.
The author considers evidence regarding the association between post-stroke neuropsychological functioning and functional outcomes.
n/a The author presents evidence that neuropsychological functioning predicts future functional outcomes within individuals post-stroke. Nevertheless, the author concludes that the existing literature base is limited in several respects and that long-term, large scale research is need to further explore the predictive ability of neuropsychological functioning.
Cristea et al. 2006 Canada RCT
CA: ý
Blinding: Patient þ
Assessorþ
ITT: ý
37 stroke patients with chronic hemiparesis. Exclusion criteria: unable to reach with the impaired arm, stroke in the non-dominate hemisphere, occipital, cerebellar, or brain stem lesions, multiple strokes, major perceptual deficits or other neurological disorders. 10% of those assessed for eligibility were included in the study.
Participants were randomized to one of three study arms: Knowledge of Results (KR, n=14), Knowledge of Performance (KP, n=14), or control (n=9). Associations between kinetic gains and cognitive functioning were investigated.
Cognitive functioning was assessed across 5 domains: verbal memory, visuospatial memory, attention, mental flexibility, and planning/ problem solving. Arm motor impairment was assessed using the arm section of the Fugl-Meyer Scale, the Composite Spasticity Index, and the Upper Extremity Performance Test for the Elderly
Baseline arm function was significantly correlated with cognitive scores. For those in the KP study arm, improvement in segmentation and precision were significantly associated with verbal memory, mental flexibility, and planning ability, whereas those with impaired memory and planning abilities made less clinical improvement in arm function (all at p<0.05). For participants in the control group, mental flexibility was significantly associated with increased retention of decreased velocity variability (p<0.05). The authors concluded that cognitive deficits are “important factors for choosing motor rehabilitation interventions after stroke”.
Van Zandvoort et al. 2005
n/a 57 consecutively admitted ischemic stroke patients.
Participants completed neuropsychological
A neuropsychological test battery, the Barthel Index,
51 (88%) participants completed the follow-up interview. Neuropsychological test scores at

Heart and Stroke Foundation Mood, Cognition and Fatigue Following Stroke Canadian Stroke Best Practice Recommendations Evidence Tables
VCI: Screening and Assessment 2015 19
Study/Type Quality Rating Sample Description Method Outcomes Key Findings and Recommendations
Netherlands Observational
Exclusion criteria: age >18 and <81, previous stroke, modified Rankin <2 or >4, and pre-stroke dependence.
assessments within 4-20 days of stroke onset. At 12-24 months post-stroke, a follow-up interview was conducted that included both neuropsychological and functional assessment.
the modified Rankin Scale, and the Short-Form Medical Outcome Study Questionnaire (SF-36).
baseline were significantly associated with scores at follow-up, with linear regression coefficients ranging from 0.60 to 0.95 for the majority of tests. Cognitive functioning at baseline was also significantly associated with functional outcome at follow-up (p<0.001), but not quality of life.
Mok et al. 2004 China Observational
n/a 75 patients with stroke associated with small vessel disease. Exclusion criteria: intracerebral hemorrhage, cortical or large subcortical (>2 cm) infarcts, non-ischemic lesions, pre-stroke dementing illness not due to Alzheimer’s disease or vascular dementia, major depression, and communication problems precluding cognitive assessment.
Participants completed a cognitive assessment 3-months post-stroke. Severity of cognitive symptoms were rated using the Clinical Dementia Rating Scale (CDR).
Semi-structured clinical interview, Mini-Mental State Exam (MMSE), Alzheimer’s Disease Assessment Scale Cognition subscale (ADAS-cog), and the Mattis Dementia Rating Scale.
43% (n=32) of participants reported post-stroke cognitive decline. Reported cognitive symptoms included being memory problems (92.3%), slow thinking (74.4%), disorientation (17.9%), aphasia (17.9%), and disinhibition (2.6%). Pre-stroke cognitive impairment (OR 95.5, 95% CI 7.4 to 1248) and previous stroke (OR 11.35, 95% CI 1.6 to 79.7) were both associated with significantly increased odds of post-stroke cognitive decline. Stroke severity and executive dysfunction were each significantly associated with impaired functioning in instrumental activities of daily living (both at p<0.001).
Zinn et al. 2004 US Cohort study
n/a 272 acute stroke patients. Exclusion criteria: pre-stroke institutionalization, admission >10 days post-stroke onset, age>40 and <90 years of age, and life-expectancy <6 months. 21% of participants screened for eligibility were included in the study.
A retrospective chart review was completed for each participant to determine eligibility and collect baseline data. At 6-months post-stroke participants were contacted by telephone to complete a follow-up interview.
Quality, timing and receipt of specific rehabilitation services and functional outcomes at 6-months post-stroke.
185 (n=68%) participants were identified as having cognitive impairment. Participants with cognitive impairment reported significantly less independence in instrumental activities of daily living (18.2 vs 21.0, p<0.01). Participants with cognitive impairment were also significantly more likely to currently be receiving rehabilitation services 6-months post-stroke (25% vs 12.7%, p<0.05). No differences were found between participants with and without cognitive deficits in terms of quality, timing, or receipt of rehabilitation services or performance on activities of daily living.
Patel et al. 2003 UK Cohort Study
n/a 163 individuals with first-ever stroke. Patients with severe dysphasia were excluded.
As part of the South London Stroke Register, participants completed a cognitive assessment at 3 months and 1, 2, and 3
The Mini Mental State Examination (MMSE), the Barthel Index, the Frenchay Activities Index (FAI), survival, and
At 3 months post-stroke, 39.3% of participants were identified as being cognitively impaired, as compared to 35.3% at 1 year, 30.3% at 2 years, and 31.9% at 3 years. The prevalence rate per 1000 individuals at 3 months and at 1, 2, and 3
Heart and Stroke Foundation Mood, Cognition and Fatigue Following Stroke Canadian Stroke Best Practice Recommendations Evidence Tables
VCI: Screening and Assessment 2015 20
Study/Type Quality Rating Sample Description Method Outcomes Key Findings and Recommendations
years post-stroke. Disability indices were also administered at the 1 year follow-up. Cognitive impairment was defined as an MMSE score <24.
institutionalization. years post stroke was reported to be 0.273, 0.200, 0.141, and 0.124, respectively. Cognitive recovery during the first year post-stroke was significantly positively associated with a history of smoking (OR 3.7, 95% CI 1.2 to 11.8) and initial level of consciousness (OR 5.7, 95% CI 1.5 to 20.7) and significantly negatively associated with initial visuospatial neglect (OR 2.9, 95% CI 0.08 to 0.89).
Paollucci et al. 2001 Italy Observational
n/a 178 patients with first-ever ischemic stroke admitted to inpatient rehabilitation. Exclusion criteria: Left hemispheric lesions, hemorrhagic stroke, and presence of other chronic disabling conditions.
Participants were categorized into two groups on the basis of presence of unilateral spatial neglect and matched by age and time from stroke-onset to rehabilitation admission. All participants received physiotherapy whereas participants with unilateral spatial neglect also received treatment for that deficit.
Length of stay, rehabilitation efficiency (average daily gain in Barthel Index score), rehabilitation effectiveness, and discharge home.
Participants with unilateral spatial neglect had a significantly longer mean length of stay (116.8 vs 81.3), achieved significantly less rehabilitation efficiency (0.18 vs .38) and effectiveness (30.9 vs 54.1), and were significantly less likely to be discharged home (81.9% vs 95.1%), all at p<0.01.
Rockwood et al. 2000 Canada Cohort Study
n/a 9,008 community-dwelling individuals and 1.255 individuals living in an institution. Participants were 65 years of age or older at baseline.
As part of the Canadian Study of Health and Aging, participants were surveyed at baseline and at 18-month and 5-year follow-up. Participants who screened positive for cognitive impairment (<78 on the 3MS) and all those who were institutionalized received a clinical assessment.
Modified Mini Mental State Examination (3MS), section H of the Cambridge Mental Disorders of the Elderly Examination, and a battery of neuropsychological tests.
The estimated prevalence per 1000 individuals was reported to be 26 for vascular cognitive impairment-no dementia, 9 for mixed AD, 15 for vascular dementia, and 50 for all types of VCI combined. Those who were identified as being cognitively impairment at baseline were at significantly increased risk of institutionalization (RR 3.1, range 2.1 to 4.6) and death (RR 1.8, range 1.5 to 2.3) at 5 years, as compared to those with intact cognition at baseline.
Tatemichi et al. 1994 US Observational
n/a 227 consecutively admitted ischemic stroke patients and 240 stroke-free controls. Exclusion criteria: age<60, severe aphasia, possible or
All participants completed a neuropsychological assessment battery. Participants with stroke completed the
A neuropsychological assessment battery assessing the following domains: memory, orientation, language, visuospatial ability, abstract
Stroke patients demonstrated impairment in each area of assessment, with 78% failing at least one test. 35.2% of individuals with stroke were classified as cognitively impaired, as compared to 3.8% of controls, and 10.2% to 38.5% scored below the control groups’ fifth

Heart and Stroke Foundation Mood, Cognition and Fatigue Following Stroke Canadian Stroke Best Practice Recommendations Evidence Tables
VCI: Screening and Assessment 2015 21
Study/Type Quality Rating Sample Description Method Outcomes Key Findings and Recommendations
probable Alzheimer’s disease.
assessment within 3 months of the index event.
reasoning, and attention. percentile. The domains in which stroke patients showed the most impairment were memory, orientation, language, and attention. Cognitive impairment was significantly associated with dependent living (OR 2.4, 95% CI 1.3 to 4.4), controlling for age and physical impairment.
Note: CA: Concealed Allocation; ITT: Intention-to-treat
What tools are used to assess VCI?
Study/Type Quality Rating Sample Description Method Outcomes Key Findings and Recommendations
Braun et al. 2012 US Review
n/a This article presents a review of neuropsychological assessment.
The authors discuss the benefits of neuropsychological assessment across several diagnostic categories.
n/a The authors state that neuropsychological assessment is beneficial in the diagnosis, prognosis, and management of “nearly all neurocognitive and psychiatric disorders”. With respect to stroke specifically, the authors state that neuropsychological assessment enhances post-stroke rehabilitation intervention planning and the prediction of functional outcomes.
Gottesman et al. 2010 US Observational
n/a 200 patients with acute non-dominant hemispheric stroke. Exclusion criteria: history or neurological disease, hearing loss, or blindness, hemorrhage on admission CT, and left hemispheric or infratentorial acute infarcts on diffusion-weighted imaging (DWI) MRI.
Participants completed a neglect battery and neuroimaging within 24 hours of hospital admission and within 5 days of stroke onset. Infarct volume was determined with the aid of ImageJ software.
A neglect battery including oral reading, copying the “Ogden scene”, clock draw, line bisection, line cancellation, visual extinction, and tactile extinction.
Median infarct volume was 8.1 (range 0.03-258.3) cc. Infarct volume was most strongly correlated with the scene copy (r=0.48), line cancellation (r=0.43), and visual perception (r=0.44). In a multivariate model, log-transformed line cancellation and visual perception were each significantly associated with log-transformed infarct volume (p=0.02 and p=0.004, respectively). A modified version of the National Institutes of Health Stroke Scale, the NIHSS-Plus, was developed through the addition of line cancellation and visual perception scores. The resultant NIHSS-Plus was reported to have a slightly stronger correlation with infarct volume than the standard NIHSS (r=0.54 vs. r=0.49).
Nyenhuis and Gorelick 2007 Review
n/a This article presents a review of topics related to the diagnosis and management of vascular
The authors consider published literature relating to the diagnosis of VCI as well as VCI
n/a The authors state that prevalence estimates of VCI widely vary between studies because of the use of different diagnostic criteria. The authors identify and summarize the most common VCI

Heart and Stroke Foundation Mood, Cognition and Fatigue Following Stroke Canadian Stroke Best Practice Recommendations Evidence Tables
VCI: Screening and Assessment 2015 22
Study/Type Quality Rating Sample Description Method Outcomes Key Findings and Recommendations
cognitive impairment (VCI). risk factors and pharmacological agents that have been examined for the management of VCI.
diagnostic systems, including the Diagnostic and Statistical Manual (DSM-IV), the Hachinski Ischemia Score, the National Institute of Neurological Disorders and Stroke – Association Internationale pour la Recherche et l’Enseignement un Neurosciences (NINDS-AIREN), the State of California Alzheimer’s Disease Diagnostic and Treatment Centers (ADDTC) criteria for ischemic VaD, and the Vascular CIND criteria. The authors conclude that the recently proposed Vascular Cognitive Impairment Harmonization Standards (Hachinshi et al. 2006, below) will likely help to improve the diagnostic process.
Hachinski et al. 2006 Consensus Statement
n/a This article presents results from the “Vascular Cognitive Impairment: Harmonization Criteria” workshop held in 2005.
Workshop participants were tasked with defining data sets that would be recommended for use in future studies.
Recommendations regarding screening questions, a minimum dataset, and an ideal dataset were proposed.
The working group proposed 60-minute, 30, minute, and 5-minute neuropsychological test protocols, MRI and CT measures for neuroimaging, neuropathology data to be collected, and recommendations for research in the areas of experimental models, biomarkers, and genetics. Please see the full Vascular Cognitive Impairment Harmonization Standards document for specific recommendations.
Note: CA: Concealed Allocation; ITT: Intention-to-treat
Imaging
Study/Type Quality Rating Sample Description Method Outcomes Key Findings and Recommendations
Gorelick et al. 2011 AHA/ASA Scientific Statement
n/a This article presents a statement regarding the vascular contribution to cognitive impairment and dementia.
Writing group members used systematic literature reviews, published guidelines, and expert opinion to summarize the current evidence and develop recommendations. Recommendations are
n/a The term vascular cognitive impairment refers to all forms of cognitive deficits, ranging from vascular mild cognitive impairment to vascular dementia. Vascular and degenerative pathologies often coexist and each increases risk of cognitive impairment and dementia. With respect to pharmacological therapy, the working group recommends that donepezil “can

Heart and Stroke Foundation Mood, Cognition and Fatigue Following Stroke Canadian Stroke Best Practice Recommendations Evidence Tables
VCI: Screening and Assessment 2015 23
Study/Type Quality Rating Sample Description Method Outcomes Key Findings and Recommendations
graded according to a classification scheme that considers both the size and estimated certainty of the treatment effect.
be useful for cognitive enhancement in patients with vascular dementia, that galantamine “can be beneficial for patients with mixed Alzheimer disease/vascular dementia, and that the benefits of rivastigmine and memantine “are not well established in vascular dementia”. In terms of non-pharmacological management, the working group concluded that no formal recommends could be offed due to the limited evidence available.
Debette et al. 2010 US Cohort study
n/a 2,229 participants. As part of the Framingham Offspring Study, participants underwent volumetric MRI and neuropsychological assessment. 1,664 participants completed a second neuropsychological assessment approximately 5 years later.
Neuropsychological assessment.
White matter hyperintensities volume (WMHV; HR 2.22, 95% CI 1.3 to 3.7), extensive WMHV (HR 3.97, 95% CI 1.1 to 14.3), and MRI-detected brain infarcts (HR 6.12, 95% CI 1.8 to 20.5) were each significantly associated with increased risk of incident dementia.
Black et al. 2009 Review
n/a This article presents a review of white matter disease
The author includes a discussion of the relationship between stroke and Alzheimer’s disease, Challenges in measuring small vessel disease in Vivo, and clinical-pathological correlates of small vessel disease.
n/a The author reports that the interrelationship between CVD and AD suggests that ischemia may drive pathophysiology in sporadic AD and that even small strokes may lower the threshold for dementia when combined with AD. Although overall cognitive ability is best predicted by brain atrophy, the burden of small vessel disease has been found to independently predict memory, language, and some executive functions. Ischemia from arterial and capillary pathology and venous insufficiency from periventricular venular collagenosis are both implicated in cerebral white matter disease. The author concludes that further research is needed to understand and treat subcortical vascular disease.
Hachinski et al. 2006
n/a This article presents results from the “Vascular Cognitive Impairment: Harmonization
Workshop participants were tasked with defining data sets that
Recommendations regarding screening questions, a minimum
The working group proposed 60-minute, 30, minute, and 5-minute neuropsychological test protocols, MRI and CT measures for

Heart and Stroke Foundation Mood, Cognition and Fatigue Following Stroke Canadian Stroke Best Practice Recommendations Evidence Tables
VCI: Screening and Assessment 2015 24
Study/Type Quality Rating Sample Description Method Outcomes Key Findings and Recommendations
Consensus Statement
Criteria” workshop held in 2005.
would be recommended for use in future studies.
dataset, and an ideal dataset were proposed.
neuroimaging, neuropathology data to be collected, and recommendations for research in the areas of experimental models, biomarkers, and genetics. Please see the full Vascular Cognitive Impairment Harmonization Standards document for specific recommendations.
Rasquin et al. 2004 Netherlands Observational
n/a 176 patients with first-ever ischemic stroke. Exclusion criteria: age <40 years, severe cognitive impairment (MMSE<15), pre-stroke dementia, other neurological or psychiatric disorders.
Participants underwent neuropsychological assessment within 1-month of stroke and at 6- and 12-month follow-up. CT scanning was completed at baseline.
Neuropsychological test battery assessing memory, mental speed, interference susceptibility, orientation, language, praxis, and abstract thinking.
Older age (OR 6.2), less education (OR 4.1), territorial stroke type (OR 4.5), presence of silent infarcts (OR 5.6), and pre-stroke cerebrovascular damage (OR 5.6) were all significantly associated with increased odds of dementia at 12-months post-stroke, as compared to those with intact cognition (all at p<0.05). Older age (OR 3.5), female sex (OR 2.7), less education (OR 2.6), presence of white matter lesions (OR 3.4), atrophy (OR 2.5), and pre-stroke cerebrovascular damage (OR 2.5)were all significantly associated with increased odds of vascular cognitive impairment at 12-months, as compared to those with intact cognition (all at p<0.05) .
Vermeer et al. 2003 Netherlands Cohort Study
n/a 1015 participants, aged 60-90 years, free of dementia and stroke at baseline.
As part of the Rotterdam Scan Study, participants completed a neurological assessment and underwent MRI at baseline and again approximately 4-years later.
The Mini-Mental State Exam, the 15-word verbal learning test, the Stroop test, the Paper-and-Pencil Memory Scanning Task, and the Letter-Digit Substitution Task.
739 participants completed the 2nd neuropsychological assessment whereas 629 underwent a 2nd MRI. 619 participants remained stroke-free and 30 (3%) developed dementia during the study period. The risk of developing dementia was significantly greater for participants with than without silent brain infarcts at baseline (HR 2.26, 95% CI 1.09 to 4.7).
Note: CA: Concealed Allocation; ITT: Intention-to-treat

Heart and Stroke Foundation Mood, Cognition and Fatigue Following Stroke Canadian Stroke Best Practice Recommendations Evidence Tables
VCI: Screening and Assessment 2015 25
Cognitive Tests
Study/Type Quality Rating Sample Description Method Outcomes Key Findings and Recommendations
McClure et al. 2012 Canada Chart Audit
n/a 123 stroke patients consecutively admitted to inpatient stroke rehabilitation.
A retrospective chart audit was conducted to collect information pertaining to screening and assessment of cognitive impairment.
Proportion of patients formally screened and assessed for cognitive impairment.
In total, 82.9% (n=102) of patients were screened for cognitive impairment using a formal screening instrument. The MoCA was the most commonly used screening instrument (67%), followed by the MMSE (33%). Cognitive impairment was detected in 77.5% (n=79) of those screened. Evidence of referral for comprehensive cognitive assessment was detected for 3.7% (n=3) of patients.
Cumming et al. 2011 Australia Observational
n/a 294 stroke patients admitted to hospital. Exclusion criteria: age <18 years, presentation >24 hours post-stroke onset, premorbid disability, and rapid deterioration, among others.
As part of the Very Early Rehabilitation Trial (AVERT), participants completed cognitive screening as part of the 3-month post-stroke assessment.
The Montreal Cognitive Assessment (MoCA).
220 (75%) participants completed the MoCA at the 3-month follow-up. For these participants, the mean MoCA score was 21.1 (SD 7.5) with a range of 0 to 31. Using a cut-off of ≥26, 35% (n=78) of participants were classified as having intact cognitive functioning. The authors concluded that the MoCA is a “feasible global cognitive screening toll in stroke trials”.
Korner-Bitensky et al. 2011 Canada Survey
n/a 663 occupational therapists (OTs) that provide services to stroke rehabilitation patients in acute care, inpatient rehabilitation, or community-based services.
A telephone survey was conducted to identify clinician practices through a series of patient vignettes.
Type and frequency of cognitive issues identified, assessment methods, and use of interventions.
Of the 183 OTs working in acute Care, 69% identified cognitive impairment as a potential issue, 70% reported they would use a standardized cognitive assessment tool, and 81% reported they would employ a cognitive intervention. Of the 253 OTs working in an inpatient rehabilitation facility, 83% identified cognitive impairment as a potential issue, 77% reported they would use a standardized cognitive assessment tool, and 83% reported they would employ a cognitive intervention. Of the 227 OTs working in a community-based setting, 31% identified cognitive impairment as a potential issue, 58% reported they would use a standardized cognitive assessment tool, and 50% reported they would employ a cognitive intervention.

Heart and Stroke Foundation Mood, Cognition and Fatigue Following Stroke Canadian Stroke Best Practice Recommendations Evidence Tables
VCI: Screening and Assessment 2015 26
Study/Type Quality Rating Sample Description Method Outcomes Key Findings and Recommendations
Racic et al. 2011 Bosnia and Herzegovina Observational
n/a 251 stroke patients admitted to hospital. Patients with pre-stroke dementia or severe aphasia were excluded.
Participants completed neuropsychological testing 3 months post-stroke. Diagnosis of dementia was defined using the NINDS-AIREN criteria.
Prevalence of dementia 3-months post-stroke.
At 3-months post-stroke, 19.5% (n=49) of participants met criteria for vascular dementia. Participants with dementia were significantly more likely to have atrial fibrillation (p<0.01), ventricular arrhythmias (p<0.01), and previous stroke (p<0.05). Diagnosis with dementia at 3-months post-stroke was also significantly associated with greater cognitive and functional impairment at the time of stroke (p<0.05).
Toglia et al. 2011 US Observational
n/a 72 stroke patients admitted to an inpatient rehabilitation unit. Patients with incomplete intake assessments or impaired language comprehension were excluded. 31% of patients assessed for eligibility were included.
Participants completed the Mini-Mental State Exam (MMSE; administered by a physiatrist) and the Montreal Cognitive Assessment (MoCA; administered by an occupational therapist). All assessments were completed within 48 hours of admission.
The Mini-Mental State Exam (MMSE), the Montreal Cognitive Assessment (MoCA), the National Institutes of Health Stroke Scale (NIHSS), and the Functional Independence Measure (FIM).
MMSE and MoCA scores were significantly correlated with each other (r=0.79, p<0.001), although mean scores were significantly lower on the MoCA than on the MMSE (17.8 vs. 24.4, p<0.01). Using a cutoff score of 26 on the MoCA and 27 on the MMSE, 89% vs. 63% of participants were detected as having cognitive impairment, respectively. The authors also note that, as compared to the MMSE, the MoCA demonstrated a less pronounced ceiling effect and greater internal reliability. In a linear regression, the MoCA visuoexecutive subtest was significantly associated with discharge motor FIM score, controlling for NIHSS, age, and motor FIM score at admission (p<0.05). In similar regression models neither the MoCA nor the MMSE total scores were significantly predictive of functional motor gain.
Verhoeven et al. 2011 Netherlands Observational
n/a 209 stroke patients with a one-sided supratentorial lesion admitted to inpatient rehabilitation. Exclusion criteria: age <18 years, previous stroke, disabling comorbidity, and communication deficits.
Participants completed a cognitive assessment during hospitalization. Follow-up assessments were conducted at 1 and 3 years post-stroke and included assessment of both cognitive and physical functioning.
The CAMCOG, the Stroke-Adapted Sickness Impact Profile (SA-SIP30), the Motricity Index (MI), and the Barthel Index.
134 participants completed both the 1 and 3 year follow-up assessments. Baseline scores on the CAMCOG perception subscale were significantly correlated with the physical dimension of the SA-SIP30 at both 1 year (r=-0.20, p<0.05) and 3 years (r=-0.30, p<0.01) post-stroke. Controlling for age, sex, education, MI score, and side and type of stroke, baseline scores on the CAMCOG significantly predicted SA-SIP30 scores at 1 at 3 years, explaining 6.9% and 6.5% of SA-SIP30 scores, respectively.
Bour et al. 2010 Netherlands
n/a 194 consecutively admitted patients with supratentorial stroke.
Participants completed neuropsychological assessments
The MMSE and a neuropsychological test battery, including the
MMSE score at 1 month was significantly correlated with the number of impaired cognitive domains at 1 (r=-0.68), 6 (r=-0.70), 12 months

Heart and Stroke Foundation Mood, Cognition and Fatigue Following Stroke Canadian Stroke Best Practice Recommendations Evidence Tables
VCI: Screening and Assessment 2015 27
Study/Type Quality Rating Sample Description Method Outcomes Key Findings and Recommendations
Observational
Exclusion criteria: age <40 years, previous stroke, severe cognitive impairment (MMSE<15), severe aphasia, and pre-stroke dementia.
administered by a neuropsychologist at 1, 6, 12, and 24 months post-stroke onset.
CAMCOG, Concept Shifting Test, Stroop Coloyr Wort Test, Auditory Verbal Learning Test, and the Groninger Intelligence Test.
(r=-0.62), and 24 months (r=-0.69), all at p<0.001. Baseline MMSE remained a significant predictor of the number of impaired cognitive domains at each follow-up after controlling for age, sex, and level of education. MMSE at baseline was also a significant predictor of presence of dementia (p<0.05). However, the authors reported that MMSE score at 1-month did not significantly predict cognitive improvement or further deterioration in either univariate or multivariate analyses.
Gottesman et al. 2010 US Observational
n/a 200 patients with acute non-dominant hemispheric stroke. Exclusion criteria: history or neurological disease, hearing loss, or blindness, hemorrhage on admission CT, and left hemispheric or infratentorial acute infarcts on diffusion-weighted imaging (DWI) MRI.
Participants completed a neglect battery and neuroimaging within 24 hours of hospital admission and within 5 days of stroke onset. Infarct volume was determined with the aid of ImageJ software.
A neglect battery including oral reading, copying the “Ogden scene”, clock draw, line bisection, line cancellation, visual extinction, and tactile extinction.
Median infarct volume was 8.1 (range 0.03-258.3) cc. Infarct volume was most strongly correlated with the scene copy (r=0.48), line cancellation (r=0.43), and visual perception (r=0.44). In a multivariate model, log-transformed line cancellation and visual perception were each significantly associated with log-transformed infarct volume (p=0.02 and p=0.004, respectively). A modified version of the National Institutes of Health Stroke Scale, the NIHSS-Plus, was developed through the addition of line cancellation and visual perception scores. The resultant NIHSS-Plus was reported to have a slightly stronger correlation with infarct volume than the standard NIHSS (r=0.54 vs. r=0.49).
Stricker et al. 2010 US Observational
n/a 42 patients >6 months post-stroke and 36 stroke-free controls. Exclusion criteria: bilateral stroke, left-handed, neurological disorder other than stroke and history of psychiatric disorder, among others.
A standardized neurological assessment battery, Global Deficit Score (GDS), and a motor composite score (including Finger Tapping, Grip Strength, and Grooved Pegboard).
As compared to stroke-free controls, participants with stroke demonstrated less cognitive ability in all five cognitive domains. The authors concluded that “the neuropsychological assessment battery is a useful clinical tool for detection of cognitive deficits in individuals with chronic unilateral stroke”.
Douglas et al. 2007 Canada Survey
n/a 247 currently practicing occupational therapists The survey response rate was 24.5%.
Participants completed a web-based questionnaire.
Measures used by occupational therapists to assess cognition and the purposes for which the assessments are used.
Respondents reported using a total of 75 assessment measures, of which 65 were standardized. The most commonly used standardized measures were the Mini Mental State Exam and the Cognitive Competency Test. Respondents reported using assessment

Heart and Stroke Foundation Mood, Cognition and Fatigue Following Stroke Canadian Stroke Best Practice Recommendations Evidence Tables
VCI: Screening and Assessment 2015 28
Study/Type Quality Rating Sample Description Method Outcomes Key Findings and Recommendations
measures to identify deficits (47%), for prediction (32%), and to measure change (20%).
Van Zandvoort et al. 2005 Netherlands Observational
n/a 57 consecutively admitted ischemic stroke patients. Exclusion criteria: age >18 and <81, previous stroke, modified Rankin <2 or >4, and pre-stroke dependence.
Participants completed neuropsychological assessments within 4-20 days of stroke onset. At 12-24 months post-stroke, a follow-up interview was conducted that included both neuropsychological and functional assessment.
A neuropsychological test battery, the Barthel Index, the modified Rankin Scale, and the Short-Form Medical Outcome Study Questionnaire (SF-36).
51 (88%) participants completed the follow-up interview. Neuropsychological test scores at baseline were significantly associated with scores at follow-up, with linear regression coefficients ranging from 0.60 to 0.95 for the majority of tests. Cognitive functioning at baseline was also significantly associated with functional outcome at follow-up (p<0.001), but not quality of life.
Stephens et al. 2004 UK Observational
n/a 381 stroke patients and 66 age matched stroke-free controls.
Participants completed neurological assessments 3 months post-stroke onset.
A neuropsychological test battery, including section B of the revised Cambridge Assessment Mental Disorders in the Elderly (CAMCOG) and the Cognitive Drug Research Battery.
259 (68%) participants were classified as not cognitively impaired, 92 (24%) were classified as having vascular cognitive impairment without dementia (VCIND), and 33 (9%) were diagnosed with post-stroke dementia. Stroke patients meeting criteria for VCIND and dementia were significantly impaired in all cognitive domains. Stroke patients with dementia demonstrated significantly more impairment in the orientation and memory domains, as compared to those with VCIND (both at p<0.001).
Ingles et al. 2002 Canada Cohort study
n/a 10 263 community and institution residing individuals 65 years of age or older.
As part of the Canadian Study of Health and Aging, participants completed the Modified Mini-Mental Status Exam (3MS). Those who scored <78 on the 3MS underwent a clinical assessment and follow-up assessment 5-years later.
A Neuropsychological test battery.
149 participants were classified as having vascular cognitive impairment no dementia (VCIND). Of these, 125 completed the neuropsychological assessment and follow-up cognitive diagnoses were available for 102. 45 (44%) patients who had VCIND at baseline were diagnosed with dementia at the 5-year follow-up. Development of dementia was significantly associated with memory and category fluency impairment at baseline.
Note: CA: Concealed Allocation; ITT: Intention-to-treat

Heart and Stroke Foundation Mood, Cognition and Fatigue Following Stroke Canadian Stroke Best Practice Recommendations Evidence Tables
VCI: Screening and Assessment 2015 29
What are the differences between the tools used to assess VCI?
Study/Type Quality Rating Sample Description Method Outcomes Key Findings and Recommendations
Cumming et al. 2013 Australia Observational
n/a 60 stroke patients 18 years of age or older. Patients who unconscious at admission to hospital and those with major visual, hearing, or language impairments were excluded.
Trained research assistants administered the two screening tools in the participant’s place of residence 3 months post-stroke. A second session was completed one week later in which a full neuropsychological testing battery was administered.
The Montreal Cognitive Assessment (MoCA), the Mini Mental State Exam (MMSE), and a neuropsychological battery (Rey Complex Figure, WAIS-R, digit span and digit symbol, Hopkins Verbal Learning Test-Revised, Trail-Making Test, letter and animal fluency, Star Cancellation, Token Test, and the Boston Naming Test).
Median scores on the MoCA and MMSE were 21 (IQR 17-24) and 26 (IQR 22-27), respectively. Area under the curve in ROC analysis did not differ significantly between the two tools (p>0.05). 37 (62%) and 43 (72%) of participants were classified as cognitively impaired according to scores on the MMSE and MoCA, respectively. 12 participants were misclassified by the MMSE, whereas 10 were misclassified by the MoCA. As optimized cutpoints, the positive and negative predictive values were 0.86 and 0.70 for the MMSE and 0.84 and 0.82 for the MoCA, respectively. The authors concluded that both tools demonstrate acceptable validity for detecting cognitive impairment among stroke patients.
Pendlebury et al. 2012 UK Observational
n/a 100 individuals >1 year following stroke or TIA. Individuals residing in a nursing and those with acute illness or deficits that could interfere with testing were excluded.
As part of the OXVASC study, participants underwent additional cognitive assessment as part of their 1 or 5 year follow-up.
The Montreal Cognitive Assessment (MoCA), Mini Mental State Exam (MMSE), Addenbrooke’s Cognitive Examination-Revised (ACE-R), and a neuropsychological battery (Train Test A and B, Symbol Digit Modalities Test, Boston Naming Test, Rey-Osterrieth Complex Figure copy, Hopkins Verbal Learning Test-Revised, and letter and category fluency).
Of the 91 participants who completed all assessments, 39 (43%) were found to have mild cognitive impairment, of which 51% were impaired in a single domain. In ROC analysis, the area under the curve was 0.85 (95% CI 0.78 to 0.93) for the MoCA, 0.83 (95% CI 0.75 to 0.92) for the MMSE, and 0.90 (95% CI 0.83 to 0.96) for the ACE-R. At optimized cutpoints the sensitivity and specificity were 77% and 83% for the MoCA, 77% and 81% for the MMSE, and 83% and 73% for the ACE-R. The authors concluded that the MoCA and the ACE-R demonstrated good sensitivity and specificity in detecting MCI but that the MMSE achieved poorer sensitivity due to a “relative insensitivity to single-domain impairment.”
Dong et al. 2012 Observational Cohort Study
n/a 300 patients with ischemic stroke or TIA. Exclusion criteria: age<21 years, a major psychiatric
Cognitive screening measures (MMSE and MoCA) were administered within 14 days of the index stroke
The Montreal Cognitive Assessment (MoCA), the Mini Mental State Exam (MMSE), and a neuropsychological battery
239 (80%) of participants completed the cognitive assessments. 42.3% of participants’ demonstrated no or mild cognitive impairment, 32.6% had mild and 22.2% had moderate cognitive impairment without dementia, and

Heart and Stroke Foundation Mood, Cognition and Fatigue Following Stroke Canadian Stroke Best Practice Recommendations Evidence Tables
VCI: Screening and Assessment 2015 30
Study/Type Quality Rating Sample Description Method Outcomes Key Findings and Recommendations
illness, pre-existing dementia, and major disability (mRS>4), aphasia or dysarthria.
event. Participants were assessed with a formal neuropsychological battery at a 3-6 month follow-up.
(including measures of attention, language, visuomotor speed, executive functioning, and memory).
2.9% had dementia. Areas under the curve in ROC analysis did not differ significantly between the MoCA (0.85, 95% CI 0.79 to 0.90) and the MMSE (0.83, 95% CI 0.77 to 0.89) in detecting moderate to severe cognitive impairment at 3-6 month follow-up (p>0.05). No differences were found in between the two tools in terms of their ability to predict domain-specific cognitive impairments 3-6 months post-stroke.
Godefroy et al. 2011 France Observational
n/a 95 acute stroke patients Participants completed cognitive assessments during hospitalization for acute stroke.
The Montreal Cognitive Assessment (MoCA), the Mini Mental State Exam (MMSE), and a neuropsychological test battery.
Significantly fewer participants were classified as having cognitive impairment according to results from the MMSE than the MoCA (45% vs 82%, p<0.001). Sensitively and specificity were 0.66 and 0.97 for the MMSE and 0.94 and 0.42 for the MoCA, respectively. The area under the curve in ROC analysis was 0.88 (95% CI 0.82 to 0.95) for the MMSE and 0.89 (95% CI 0.83 to 0.96) for the MoCA.
Toglia et al. 2011 US Observational
n/a 72 stroke patients admitted to an inpatient rehabilitation unit. Patients with incomplete intake assessments or impaired language comprehension were excluded. 31% of patients assessed for eligibility were included.
Participants completed the Mini-Mental State Exam (MMSE; administered by a physiatrist) and the Montreal Cognitive Assessment (MoCA; administered by an occupational therapist). All assessments were completed within 48 hours of admission.
The Mini-Mental State Exam (MMSE), the Montreal Cognitive Assessment (MoCA), the National Institutes of Health Stroke Scale (NIHSS), and the Functional Independence Measure (FIM).
MMSE and MoCA scores were significantly correlated with each other (r=0.79, p<0.001), although mean scores were significantly lower on the MoCA than on the MMSE (17.8 vs. 24.4, p<0.01). Using a cutoff score of 26 on the MoCA and 27 on the MMSE, 89% vs. 63% of participants were detected as having cognitive impairment, respectively. The authors also note that, as compared to the MMSE, the MoCA demonstrated a less pronounced ceiling effect and greater internal reliability. In a linear regression, the MoCA visuoexecutive subtest was significantly associated with discharge motor FIM score, controlling for NIHSS, age, and motor FIM score at admission (p<0.05). In similar regression models neither the MoCA nor the MMSE total scores were significantly predictive of functional motor gain.
Dong et al. 2010 Singapore
n/a 100 patients with ischemic stroke or TIA within 14 days or study enrollment.
Participants completed cognitive and physical assessments while in hospital.
The Montreal Cognitive Assessment (MoCA), the Mini-Mental State Exam (MMSE), the modified
Using cut-offs of ≤24 for the MMSE and ≤21 for the MoCA, a total of 43 and 59 participants were classified as being cognitively impaired according to the MMSE and MoCA, respectively.

Heart and Stroke Foundation Mood, Cognition and Fatigue Following Stroke Canadian Stroke Best Practice Recommendations Evidence Tables
VCI: Screening and Assessment 2015 31
Study/Type Quality Rating Sample Description Method Outcomes Key Findings and Recommendations
Observational Exclusion criteria: age <21 years, severe physical disability, severe aphasia or dysarthria, pre-existing dementia, or major psychiatric illness.
Rankin Scale (mRS), and the National Institutes of Health Stroke Scale (NIHSS).
18 participants classified as cognitively intact according to the MMSE were identified as being cognitively impaired on the MoCA, whereas only 2 participants were found to be cognitively intact on the MoCA and impaired on the MMSE. The authors concluded that the MoCA is “more sensitive than the MMSE in screening for cognitive impairment after acute stroke”.
Pendlebury et al. 2010 UK Observational
n/a 493 individuals following stroke or TIA.
As part of the OXVASC study, participants underwent additional cognitive assessment as part of their 6-month or 5-year follow-up. Cognitive impairment was defined as a score <27 on the MMSE and <26 on the MoCA.
The Montreal Cognitive Assessment (MoCA) and the Mini Mental State Exam (MMSE).
413 (84%) participants completed the cognitive assessments. Median scores (and interquartile range) were 28 (26-29) on the MMSE and 23 (20-26) on the MoCA. According to results on the MoCA, 291 (70%) patients were cognitively impaired. Of these 291 participants, 162 (56%) scored in the normal range on the MMSE. The authors concluded that the MMSE demonstrated deficits in detecting impairment in executive function, attention, and delayed recall and thus provides an underestimation of cognitive impairment among patients with stroke and TIA.
Note: CA: Concealed Allocation; ITT: Intention-to-treat Does treatment of vascular risk factors reduce the risk of cognitive decline?
Study/Type Quality Rating Sample Description Method Outcomes Key Findings and Recommendations
McGuinness et al. 2009(a) Cochrane Review and Meta-analysis Update to review
published in 2006.
n/a 4 RCTs (n=15,936) investigating an intervention to lower blood pressure in participants with hypertension and no history of cerebrovascular disease. Study duration was at least 6 months.
Pooled analyses used fixed-effects models unless significant heterogeneity was detected, in which case a random effects model was used. Results are reported as weighted mean difference, standardized mean difference, or odds ratio, as appropriate.
Primary outcome: Incident dementia, cognitive change. Secondary outcome: Blood pressure, quality of life, adverse events.
Trials meeting inclusion criteria include HYVET (2008), SCOPE (2003), SHEP (1991), and Syst EUR (1997). Mean baseline blood pressure across the included trials was 171/86 mmHG. 4 trials reported incident dementia: no significant effect of treatment was observed (OR 0.89, 95% CI 0.74 to 1.07; p>0.05). 3 trials reported cognitive change from baseline: pooled analysis revealed a significant benefit of treatment (WMD 0.42, 95% CI 0.30 to 0.53). Nevertheless, the authors concluded that there is no convincing evidence that blood pressure interventions

Heart and Stroke Foundation Mood, Cognition and Fatigue Following Stroke Canadian Stroke Best Practice Recommendations Evidence Tables
VCI: Screening and Assessment 2015 32
Study/Type Quality Rating Sample Description Method Outcomes Key Findings and Recommendations
Methodological quality was assessed using the Cochrane approach.
prevent the development of dementia or cognitive impairment.
McGuinness et al. 2009(b) Cochrane Review and Meta-analysis
n/a 2 RCTs (n=26,340) comparing statins to placebo for the prevention of dementia in individuals at risk for Alzheimer’s disease (including those with history of stroke).
Methodological quality was assessed using the Cochrane approach. Results from individual studies are reported. Data was not pooled because included trials used different outcomes at different time points.
Incident dementia, Alzheimer’s disease, vascular dementia, and cognitive change.
Trials meeting inclusion criteria include HPS (2002) and PROSPER (2002). No significant effect of treatment was reported in terms of either incident dementia or change in cognitive functioning. The authors concluded that there is good evidence that statins are not effective in preventing Alzheimer’s disease or dementia.
Evans and Sastre, 2009 Cochrane Review and Meta-analysis
n/a RCTs investigating the effect of treatment for Type II diabetes on cognitive functioning.
Trials were identified through a combination of electronic and manual search strategies. Methodological quality was assessed using the Cochrane approach. Meta-analysis was not performed.
Change in cognition functioning.
No studies were identified for inclusion. The authors concluded that there is no evidence that diabetic treatment is beneficial for the prevention or management of cognitive impairment in patients with Type II diabetes.
Sofi et al. 2011 Italy Systematic Review and Meta-analysis
n/a 15 prospective cohort studies (n=33,816) examining the association between physical activity and cognitive function in non-demented adults. Intervention studies were excluded.
Studies were identified using electronic and manual searching techniques. Data was pooled using random-effects models and reported as hazard ratios. Statistical heterogeneity was assessed using the I2 statistic.
Cognitive decline or cognitive impairment. Timing of assessment: Cognition was assessed at baseline and at the end of the study, whereas physical activity level was assessed at baseline only.
Follow-up in each study ranged from 1 to 12 years, during which 3210 cases of incident cognitive decline were reported. As compared to those who reported being sedentary, participants who reported a high level of physical activity at baseline were at significantly reduced risk of cognitive decline (HR 0.62, 95% CI 0.54 to 0.70, p<0.001), as were those who reported low-to-moderate levels of physical activity (HR 0.65, 95% CI 0.57 to 0.75, p<0.001).
Tangney et al. 2011 CHAP US Observational
n/a 3,790 community-residing individuals >56 years of age.
As part of the Chicago Health and Aging Project (CHAP), participants completed assessments of cognitive functioning and dietary pattern to assess the association between Mediterranean-type diet and cognitive decline.
A composite measure of global cognition, the Harvard Food-Frequency Questionnaire (FFQ), the MedDiet, and the Healthy Eating Indes-2005 (HEI-2005). Timing of assessment: Baseline and every 3 years.
Participants completed a mean of 7.6 years of follow-up. The mean MedDIet score was 28.1 (SD 0.1). The overall rate of change in global cognition was 0.06 units per year. Greater adherence to a Mediterranean diet was significantly associated with a reduced decline in cognitive functioning (p<0.001), as based on MedDiet score, adjusting for age, sex, race, education, total energy intake, and participation in cognitive activies. Scores on the HEI-2005
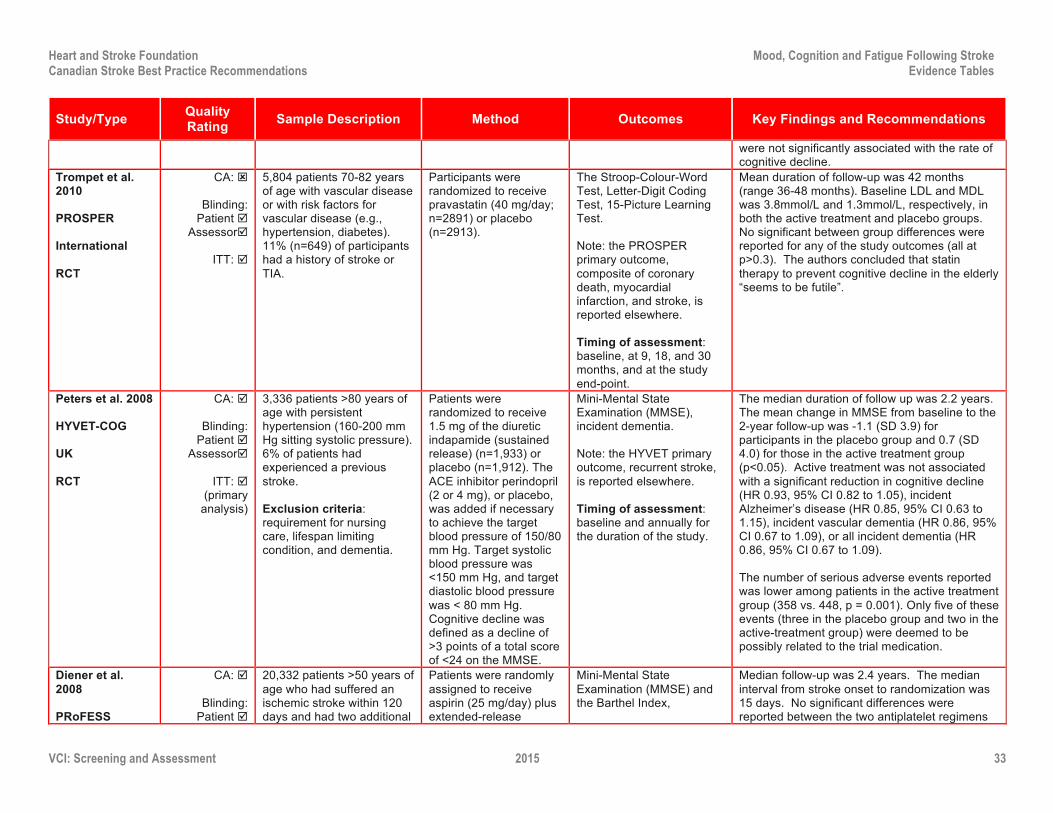
Heart and Stroke Foundation Mood, Cognition and Fatigue Following Stroke Canadian Stroke Best Practice Recommendations Evidence Tables
VCI: Screening and Assessment 2015 33
Study/Type Quality Rating Sample Description Method Outcomes Key Findings and Recommendations
were not significantly associated with the rate of cognitive decline.
Trompet et al. 2010 PROSPER International RCT
CA: ý
Blinding: Patient þ
Assessorþ
ITT: þ
5,804 patients 70-82 years of age with vascular disease or with risk factors for vascular disease (e.g., hypertension, diabetes). 11% (n=649) of participants had a history of stroke or TIA.
Participants were randomized to receive pravastatin (40 mg/day; n=2891) or placebo (n=2913).
The Stroop-Colour-Word Test, Letter-Digit Coding Test, 15-Picture Learning Test. Note: the PROSPER primary outcome, composite of coronary death, myocardial infarction, and stroke, is reported elsewhere. Timing of assessment: baseline, at 9, 18, and 30 months, and at the study end-point.
Mean duration of follow-up was 42 months (range 36-48 months). Baseline LDL and MDL was 3.8mmol/L and 1.3mmol/L, respectively, in both the active treatment and placebo groups. No significant between group differences were reported for any of the study outcomes (all at p>0.3). The authors concluded that statin therapy to prevent cognitive decline in the elderly “seems to be futile”.
Peters et al. 2008 HYVET-COG UK RCT
CA: þ
Blinding: Patient þ
Assessorþ
ITT: þ (primary
analysis)
3,336 patients >80 years of age with persistent hypertension (160-200 mm Hg sitting systolic pressure). 6% of patients had experienced a previous stroke. Exclusion criteria: requirement for nursing care, lifespan limiting condition, and dementia.
Patients were randomized to receive 1.5 mg of the diuretic indapamide (sustained release) (n=1,933) or placebo (n=1,912). The ACE inhibitor perindopril (2 or 4 mg), or placebo, was added if necessary to achieve the target blood pressure of 150/80 mm Hg. Target systolic blood pressure was <150 mm Hg, and target diastolic blood pressure was < 80 mm Hg. Cognitive decline was defined as a decline of >3 points of a total score of <24 on the MMSE.
Mini-Mental State Examination (MMSE), incident dementia. Note: the HYVET primary outcome, recurrent stroke, is reported elsewhere. Timing of assessment: baseline and annually for the duration of the study.
The median duration of follow up was 2.2 years. The mean change in MMSE from baseline to the 2-year follow-up was -1.1 (SD 3.9) for participants in the placebo group and 0.7 (SD 4.0) for those in the active treatment group (p<0.05). Active treatment was not associated with a significant reduction in cognitive decline (HR 0.93, 95% CI 0.82 to 1.05), incident Alzheimer’s disease (HR 0.85, 95% CI 0.63 to 1.15), incident vascular dementia (HR 0.86, 95% CI 0.67 to 1.09), or all incident dementia (HR 0.86, 95% CI 0.67 to 1.09). The number of serious adverse events reported was lower among patients in the active treatment group (358 vs. 448, p = 0.001). Only five of these events (three in the placebo group and two in the active-treatment group) were deemed to be possibly related to the trial medication.
Diener et al. 2008 PRoFESS
CA: þ
Blinding: Patient þ
20,332 patients >50 years of age who had suffered an ischemic stroke within 120 days and had two additional
Patients were randomly assigned to receive aspirin (25 mg/day) plus extended-release
Mini-Mental State Examination (MMSE) and the Barthel Index,
Median follow-up was 2.4 years. The median interval from stroke onset to randomization was 15 days. No significant differences were reported between the two antiplatelet regimens

Heart and Stroke Foundation Mood, Cognition and Fatigue Following Stroke Canadian Stroke Best Practice Recommendations Evidence Tables
VCI: Screening and Assessment 2015 34
Study/Type Quality Rating Sample Description Method Outcomes Key Findings and Recommendations
International RCT (factorial)
Assessorþ
ITT: þ
risk factors (e.g. diabetes, hypertention, obesity, etc.). Exclusion criteria: primary hemorrhagic stroke, severe disability, and contraindications to one of the study agents.
dipyridamole (400 mg/day) or clopidogrel (75 mg/day) and either telmisartan (80 mg/day) or placebo. Thus, there were 4 study arms, with 5060-5095 participants in each arm.
Note: The PRoFESS primary outcome, recurrent stroke, is reported elsewhere. Timing of assessment: Congintion was assessed at 1 month and 2 years post-stroke and at the end of the study period.
(RR 1.02, 95% CI 0.94 to 1.10)) or between the telmisartan and placebo groups (RR 1.01, 95% CI 0.94 to 1.09) in terms of the number of patients with MMSE scores ≤24 at the end of the study period. Likewise, no significant between group differences were reported with respect to the number of participants who had a decrease of >2 points on the MMSE only the duration of the study (dipyridamole vs. clopidogrel: RR 0.91, 95% CI 0.83 to 1.00; telmisartan vs. placebo: RR 0.95, 95% CI 0.87 to 1.05). A total of 125 patients (0.6%) were lost to follow up.
The PROGRESS Collaborative Group, 2003 PROGRESS International RCT
CA: þ
Blinding: Patient þ
Assessorþ
ITT: þ
6,105 patients with a history of stroke (ischemic or hemorrhagic) or TIA within the previous 5 years. No blood pressure criteria was used for study eligibility.
Patients who adhered to, and tolerated, the run-in treatment were randomly assigned to continued active therapy (n=3,051) or matching placebo (n=3,054). Patients in the active treatment group received a flexible regimen based on perindopril (4 mg daily) with the addition of indapamide (2.5 mg daily) in patients for whom the responsible physician judged there to be no specific indication for or contraindication to treatment with a diuretic. Cognitive decline was defined as a decline of >2 points from baseline on the MMSE.
Mini-Mental State Exam (MMSE), incident dementia. The PROGRSS primary outcome, recurrent stroke, in reported elsewhere. Timing of assessment: Baseline, 6- and 12-months, and annually for the duration of follow-up.
Mean duration of follow-up was 3.9 years. 22% of patients had discontinued medication by end of study follow-up. Cognitive decline, defined as a decrease of 3 or more points on the MMSE over the study period, was reported in 9.1% of participants in the active treatment group and 11% of participants in the placebo group. Active treatment was associated with a significant reduction in the risk of cognitive decline (risk reduction =19%, 95% CI 4% to 32%) and the composite outcome of cognitive decline and recurrent stroke (risk reduction =45%, 95% CI 21% to 61%). Dementia was diagnosed in 6.4% and 7.1% of participants in the active treatment and placebo groups, respectively. Active treatment was associated with a non-significant reduction in risk of dementia (risk reduction =12%, 95% CI -8% to 28%; p>0.05) and a significant reduction in the composite outcome of dementia and recurrent stroke (risk reduction =34%, 95% CI 3% to 55%).
Note: CA: Concealed Allocation; ITT: Intention-to-treat

Heart and Stroke Foundation Mood, Cognition and Fatigue Following Stroke Canadian Stroke Best Practice Recommendations Evidence Tables
VCI: Screening and Assessment 2015 35
Reference List Barker-Collo S, Feigin VL, Parag C, et al. Auckland stroke outcomes study: part 2: cognition and functional outcomes 5 years poststroke. Neurology,
2010;75:1608-1616. Barker-Collo S, Feigin V. The impact of neuropsychological deficits on functional stroke outcomes. Neuropsychol Rev, 2006;16:53-64. Bejot Y, Aboa-Eboule C, Durier J, Rouaud O, Jacquin A, Ponavoy E, Richard D, Moreau T, Giroud M. Prevalence of early dementia after first-ever stroke: a 24
year population-based study. Stroke, 2011;42:607-612. Black S, Gao F, Bilbao J. Understanding white matter disease: imaging-pathological correlations in vascular cognitive impairment. Stroke, 2009;40(suppl 1): S48-
S52. Bour A, Rasquin S, Boreas A, Limburg M, Verhey F. How predictive is the MMSE for cognitive performance after stroke? J Neurol, 2010;257:630-637. Braun M, Tupper D, Kaufman P, McCrea M, Postal K, Westerveld M, Wills K, Deer T. Neuropsychological assessment: a valuable tool in the diagnosis and
management of neurological, neurodevelopmental, medical, and psychiatric disorders. Cog Behav Neurol, 2011;24:107-114. Brodaty H, Altendorf A, Withall A, Sachdev PS. Mortality and institutionalization in early survivors of stroke: the effects of cognition, vascular mild cognitive
impairment, and vascular dementia. Journal of Stroke and Cerebrovascular Diseases, 2010;19(6): 485-493. Cederfeldt M, Gosman-Hedstrom G, Guitierrez Perez C, Savborg M, Tarkowski E. Recovery in personal care related to cognitive impairment before and after
stroke- a 1-year follow-up. Acta Neurol Scand, 2010;122:430-437. Cristea CM, Ptito A, Levin MF. Feedback and cognition in arm motor skill reacquisition after stroke. Stroke, 2006;37:1237-1242. Cumming TB, Bernhardt J, Linden T. The Montreal cognitive assessment short cognitive evaluation in a large stroke trial. Stroke, 2011;42:2642-2644. Cumming TB, Churilov L, Linden T, Bernhardt J. Montreal Cognitive Assessment and Mini-Mental State Examination are both valid cognitive tools in stroke. Acta
Neurol Scand 2013;128:122-29. Debette S, Beiser A, DeCarli C, Au R, Himali JJ, Kelly-Hayes M, Romero JR, Kase CS, Wolf PA, Seshadri S. Association of MRI markers of vascular brain injury
with incident stroke, mild cognitive impairment, dementia, and mortality: the Framingham offspring study. Stroke, 2010;41:600-606. Delgdo C, Donoso A, Orellana P, Vasquez C, Diaz V, Behrens MI. Frequency and determinants of poststroke cognitive impairment at three and twelve months in
Chile. Dement Geriatr Cogn Disord, 2010;29:397-405. Diener HC, Sacco RL, Yusuf S, et al. Effects of aspirin plus extended-release dipyridamole versus clopidogrel and telmisartan on disability and cognitive function
after recurrent stroke in patients with ischaemic stroke in the Prevention Regimen for Effectively Avoiding Second Strokes (PRoFESS) trial: a double-blind, active and placebo-controlled study. Lancet Neurol 2008;7:875-884.
Dong YH, Venketasubramanian N, Chan BPL, et al. Brief screening tests during acute admission in patients with mild stroke are predictive of vascular cognitive impairment 3-6 months after stroke. J Neurol Neurosurg Psychiatry 2012;83:580-85.
Dong Y, Sharma VK, Chan-BP-L, Venketasubramanian N, Teoh HL, Seet RCS, Tanicala S, Chan YH, Chen C. The Montreal cognitive assessment (MoCA) is superior to the mini-mental state examination (MMSE) for the detection of vascular cognitive impairment after acute stroke. Journal of Neurological Sciences, 2010;299:15-18.
Douglas A, Liu L, Warren S, Hopper T. Cognitive assessments for older adults: which ones are used by Canadian therapists and why. Canadian J Occupational Therapy, 2007;74(5):371-81.
Douiri A, Rudd AG, Wolfe CDA. Prevalence of poststroke cognitive impairment: South London Stroke Register 1995-2010. Stroke 2013;44:138-45.

Heart and Stroke Foundation Mood, Cognition and Fatigue Following Stroke Canadian Stroke Best Practice Recommendations Evidence Tables
VCI: Screening and Assessment 2015 36
Evans GJ, Sastre AA. Effect of the treatment of Type II diabetes mellitus on the development of cognitive impairment and dementia. Cochrane Database of Systematic Reviews 2009;1:CD003804.
Ferro JM, Crespo M. Young adult stroke: neuropsychological dysfunction and recovery. Stroke, 2988;19:982-986. Godefroy O, Fickl A, Roussel M, Auribault C, Bugnicourt JM, Lamy C, Canaple S, Petitnicolas G. Is the Montreal cognitive assessment superior to the mini-mental
state examination to detect poststroke cognitive impairment? Stroke, 2011;42:1712-1716. Gorelick PB, Scuteri A, Black SE, et al. Vascular contributions to cognitive impairment and dementia: a statement for healthcare professionals from the American
heart association/America stroke association. Stroke, 2011;42:2672-2713. Gottesman RF, Kleinman JT, Davis C, Heidler-Gary J, Newhart M, Hillis AE. The NIHSS-Plus: improving cognitive assessment with the NIHSS. Behav Neurol,
2010;22(1-2): 11-15. Gottesman RF, Hillis AE. Predictors and assessment of cognitive dysfunction resulting from ischaemic stroke. Lancet Neurology, 2010;9:895-905. Hachinski V, Iadecola C, Petersen RC, et al. National institute of neurological disorders and stroke- Canadian stroke network vascular cognitive impairment
harmonization standards. Stroke, 2006;37:2220-2241. Hochstenbach J, Mulder T, van Limbeek J, Donders R, Schoonderwaldt H. Cognitive decline following stroke: a comprehensive study of cognitive decline following
stroke. Journal of Clinical and Experimental Neuropsychology, 1998;20(4):504-517. Hoffman, M. Higher cortical function deficits after stroke: an analysis of 1,000 patients from a dedicated cognitive stroke registry. Neurorehabilitation and Neural
Repair, 2001;15:113-127. Ingles JL, Wentzel C, Fisk JD, Rockwood K. Neuropsychological predictors of incident dementia in patients with vascular cognitive impairment, without dementa.
Stroke, 2002;33:1999-2002. Korner-Bitensky N, Barrett-Bernstein S, Bibas G, Poulin V. National survey of Canadian occupational therapists assessment and treatment of cognitive impairment
post-stroke. Australian Occupational Therapy Journal 2011;58:241-50. Madureira S, Guerreiro M, Ferro JM. Dementia and cognitive impairment three months after stroke. European Journal of Neurology, 2001;8:621-627. McClure JA, Salter K, Foley N, Mahon H, Teasell R. Adherence to Canadian Best Practice Recommendations for Stroke Care: vascular cognitive impairment
screening and assessment practices in an Ontario inpatient stroke rehabilitation facility. Top Stroke Rehabil 2012;19:141-48. McGuinness B, Craig D, Bullock R, Passmore P. Statins for the prevention of dementia. Cochrane Database of Systematic Reviews 2009(b);2:CD003160. McGuinness B, Todd S, Passmore P, Bullock R. Blood pressure lowering in patients without prior cerebrovascular disease for prevention of cognitive impairment
and dementia. Cochrane Database of Systematic Reviews 2009(a);4:CD004034. Mok VCT, Wong A, Lam WWM, Fan YH, Tang WK, Kwok T, Hui ACF, Wong KS. Cognitive impairment and functional outcome after stroke associated with small
vessel disease. J Neurol Neurosurg Psychiatry, 2004;75:560-566. Narasimhalu K, Ang S, De Silva A, et al. Severity of CIND and MCI predict incidence of dementia in an ischemic stroke cohort. Neurology, 2009;73:1866-1872. Narasimhalu K, Ang S, De Silva A, Wong M-C, Chang H-M, Chia K-S, Auchus AP, Chen CP. The prognostic effects of poststroke cognitive impairment no
dementia and domain-specific cognitive impairments in nondisabled ischemic stroke patients. Stroke, 2011;42:883-888. Nyenhuis DL, Gorelick PB. Diagnosis and management of vascular cognitive impairment. Current Atheroschlerosis Reports, 2007;9:326-332. Paolucci S, Antonucci G, Grasso MG, Pizzamiglio L. The role of unilateral spatial neglect in rehabilitation of right-brain damaged ischemic stroke patients: a
matched comparison. Arch Phys Med Rehabil, 2001;82:743-749.

Heart and Stroke Foundation Mood, Cognition and Fatigue Following Stroke Canadian Stroke Best Practice Recommendations Evidence Tables
VCI: Screening and Assessment 2015 37
Patel M, Coshall C, Rudd AG, Wolfe CA. Natural history of cognitive impairment after stroke and factors associated with its recovery. Clinical Rehabilitation, 2003;17:158-166.
Pendlebury ST, Mariz J, Bull L, Mehta Z, Rothwell PM. MoCA, ACE-R, and MMSE versus the National Institute of Neurological Disorders and Stroke-Canadian Stroke Network Vascular Cognitive Impairment Harmonization Standards Neuropsychological Battery after TIA and stroke. Stroke 2012;43:464-69.
Pendlebury ST, Cuthbertson FC, Welch SJV, Mehta Z, Rothwell PM. Underestimation of cognitive impairment by Mini-Mental State Examination versus the Montreal Cognitive Assessment in patients with transient ischemic attack and stroke: a population-based study. Stroke 2010;41:1290-93.
Pendlebury S, Rothwell PM. Prevalence, incidence, and factors associated with pre-stroke and post-stroke dementia: a systematic review and meta-analysis. Lancet Neurology, 2009;8:1006-1018.
Pendlebury ST. Stroke-related dementia: rates, risk factors and implications for future research. Maturitas, 2009;64:165-171. Peters R, Beckett N, Forette F, et al. Incident dementia and blood pressure lowering in the Hypertension in the Very Elderly Trial cognitive function assessment
(HYVET-COG): a double-blind, placebo controlled trial. Lancet Neurol 2008;7:683-689. Progress Collaborative Group. Effects of blood pressure lowering with perindopril and indapamide therapy on dementia and cognitive decline in patients with
cerebrovascular disease. Arch Intern Med 2003;163:1069-1075. Racic D, Slankamenac P, Vujkovic Z, Miljkovic S, Dajic V, Dominovic Kovacevic A. Vascular dementia: clinical and neuroradiological correlation. Med Pregl,
2011;LXIC(3-4):152-156. Rasquin SMC, Verhey FRJ, van Oostenbrugge RJ, Lousberg R, Lodder J. Demographic and CT scan features related to cognitive impairment in the first year after
stroke. J Neurol Neurosurg Psychiatry, 2004;75:1562-1567. Rist PM, Chalmers J, Arima H, et al. Baseline cognitive function, recurrent stroke, and risk of dementia in patients with stroke. Stroke 2013;44:1790-95. Rockwood K, Wentzel C, Hachinski V, et al. Prevalence and outcomes of vascular cognitive impairment. Neurology, 2000;54:447-451. Savva GM, Stephan BCM, and the Alzheimer’s Society Vascular Dementia Systematic Review Group. Epidemiological studies of the effect of stroke on incident
dementia: a systematic review. Stroke, 2010;41:e41-e46. Sofi F, Valecchi D, Bacci D, et al. Physical activity and risk of cognitive decline: a meta-analysis of prospective studies. J Intern Med 2011;269:107-117. Stephens S, Kenny RA, Rowan E, Allan L, Kalaria RN, Bradbury M, Ballard CG. Neuropsychological characteristics of mild vascular cognitive impairment and
dementia after stroke. International Journal of Geriatric Psychiatry, 2004;19:1053-1057. Stricker NK, Tybur JM, Sadek JR, Haaland KY. Utility of the neuropsychological assessment battery in detecting cognitive impairment after unilateral stroke.
Journal of the International Neuropsychological Society, 2010;16:813-821. Tangney CC, Kwasny KJ, Li H, Wilson RS, Evans DA, Morris MC. Adherence to a Mediterranean-type dietary pattern and cognitive decline in a community
population. Am J Clin Nutr 2011;93:601-607. Tatemichi TK, Desmond DW, Stern Y, Paik M, Sano M, Bagiella E. Cognitive impairment after stroke: frequency, patterns, and relationship to functional abilities.
Journal of Neurology, Neurosurgery, and Psychiatry, 1994;57:202-207. Tham W, Auchus AP, Thong M, Goh M-L, Chang H-M, Wong M-C, Chen CPL-H. Progression of cognitive impairment after stroke: one year results from a
longitudinal study of Singaporean stroke patients. Journal of the Neurological Sciences, 2002;203-204:49-52. Toglia J, Fitzgerlad KA, O’Dell MW, Mastrogiovanni AR, Lin CD. The mini-mental state exam and Montreal cognitive assessment in persons with mild subacute
stroke: relationship to functional outcome. Arch Phys Med Rehabil, 2011;92:792-798,

Heart and Stroke Foundation Mood, Cognition and Fatigue Following Stroke Canadian Stroke Best Practice Recommendations Evidence Tables
VCI: Screening and Assessment 2015 38
Trompet S, van Vliet P, de Craen AJM, et al. Pravastatin and cognitive function in the elderly. Results of the PROSPER study. J Neurol 2010;257:85-90. Van Zandvoort MJE, Kessels RPC, Nys GMS, de Haan EHF, Kappelle LJ. Early neuropsychological evaluation in patients with ischaemic stroke provides valid
information. Clinical Neurology and Neurosurgery, 2005;107:385-392. Verhoeven CL, Schepers VP, Post MW, van Heugten CM. The predictive value of cognitive impairments measured at the start of clinical rehabilitation for health
status 1 year and 3 years poststroke. International Journal of Rehabilitation Research, 2011;34:38-43. Vermeer SE, Prins ND, den Heiher T, Hofman A, Koudstaal PJ, Breteler MMB. Silent brain infarcts and the risk of dementia and cognitive decline. New England
Journal of Medicine, 2003;348:1215-1222. Viscogliosi C, Desrodiers J, Belleville S, Caron CD, Ska B, BRAD Group. Differences in participation according to specific cognitive deficits following a stroke.
Applied Neuropsychology, 2011;18:117-126. Wadley VG, Unverzagt FW, McGuidre LC, Moy CS, Go R, Kissela B, McClure LA, Crowe M, Howard VJ, Howard G. Incident cognitive impairment is elevated in
the stroke belt: the REGARDS study. Ann Neurol, 2011;70:229-236. Wolfe CDA, Crichton SL, Heuschmann PU, McKevitt CJ, Toschke AM, Grieve AP, Rudd AG. Estimates of outcomes up to ten years after stroke: analysis from the
prospective south London stroke register. PLoS Medicine, 2011;8(5):e1001033. Yip AG, Brayne C, Matthews FE. Risk factors for incident dementia in England and Wales: the medical research council cognitive function and ageing study. A
population-based nested case-control study. Age and Ageing, 2006;35:154-160. Yu KH, Cho SJ, Oh MS, et al. Cognitive impairment evaluated with Vascular Impairment Harmonization Standards in a multicenter prospective stroke cohort in
Korea. Stroke 2013;44:786-88. Zinn S, Dudley TK, Bosworth HB, Hoenig HM, Duncan PW, Horner RD. The effect of poststroke cognitive impairment on rehabilitation process and functional
outcome. Arch Phys Med Rehabil, 2004;85:1084-1090.


















