
Canadian Institutes of Health Research, University of Toronto Comparative Program on Health and...
61
Canadian Institutes of Health Research, University of Toronto Comparative Program on Health and Society and Care- Peru Workshop on Rights- Based Policy Options for Accessing Medicines in Peru Hotel Jose Antonio
-
Upload
florence-rose -
Category
Documents
-
view
214 -
download
0
Transcript of Canadian Institutes of Health Research, University of Toronto Comparative Program on Health and...

Canadian Institutes of Health Research, University of Toronto Comparative Program on Health and Society
and Care-Peru
Workshop on Rights-Based Policy Options for Accessing
Medicines in Peru
Hotel Jose AntonioLima, Peru
20-21 July 2009

Objective
Advance knowledge of the right to health in international and national law
Advance knowledge about trade related intellectual property rights and the ways these can be used to ensure access
Explore case-studies from Thailand and Brazil of social and legal strategies
Advance strategies and policy tools which use rth standards to assess and reform trade-related intellectual property rights under TRIPS and free trade agreements, and otherwise use rights to ensure greater access to medicines

Aims to Advance
1) Knowledge
2) Application
3) Consensus
33

2 billion people—1/3 global population—lack regular access
Similar figures in Peru 1/3 population lack access to essential
medicines, including for diabetes, hypertension, schizophrenia, AIDS and cancer
1. The Problem: Limited Access to Medicines

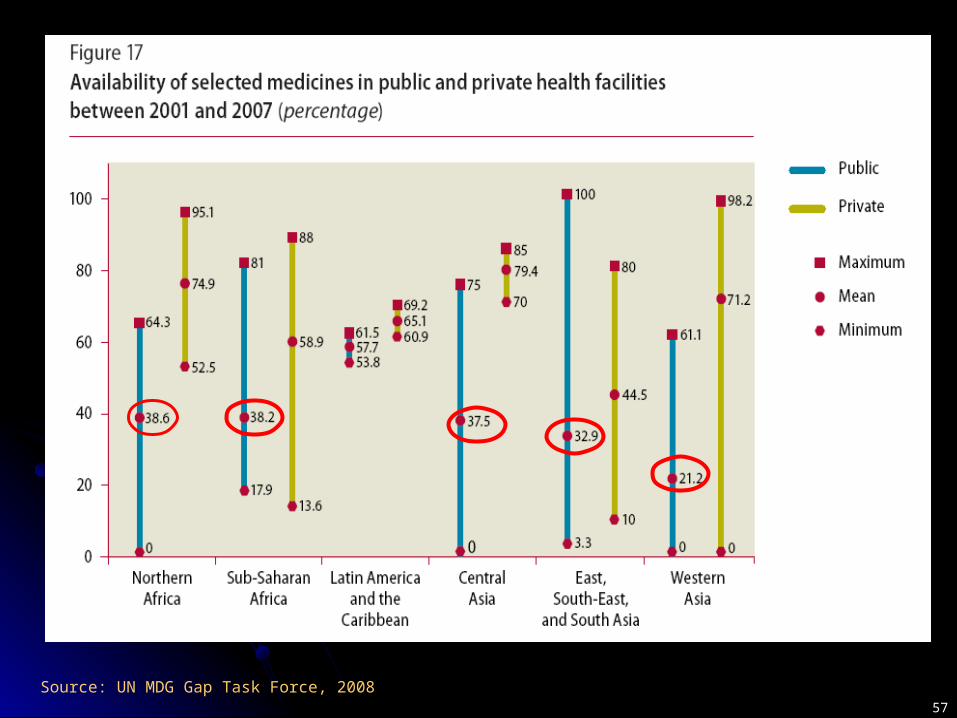
55
Factors Affecting Access
Public procurement in Peru depends on price (HAI, 2007)
Some treatments are unaffordable
Less availability of originator brands, more generics
Source: WHO (2004)

20 year exclusive patents for pharmaceuticals Exceptions and limitations
compulsory licensing (article 31) parallel imports (article 6)exclude inventions to protect life or health (article
27.1) limited exceptions (article 30)anti-competitive measures (article 40)
Agreement on Trade-Related Aspects of Intellectual Property Rights (TRIPS)

77
TRIPS-Plus Pressures and Rules Unilateral Trade Sanctions
Korea, Mexico, Chile, Thailand, Indonesia, Bolivia, Columbia, Ecuador, Peru, Venezuela, India, Argentina, Brazil, Taiwan
Corporate Litigation Kenya, Uganda, Ghana, Thailand, Brazil, China,
South Africa
Free Trade Agreements Extend monopoly periods Limit TRIPS flexibilities

Public Health Impact of FTA
Extend monopoly periods beyond twenty years
Limit market entry for genericsLimit compulsory licensingProhibit parallel importsRaise prices (Peru’s assessment of FTA)

Peru’s FTA with TRIPS-plus
99
US-FTA European Free Trade Association Impacts price, generic availability

1010
2. The right to health
The right to health requires priority to accessibility of medicines
What are implications for access and trade rules?

1111
1946 – Constitution of the World Health Organization1948 – Universal Declaration of Human Rights1961 – European Social Charter1965 – Convention on Elimination of Racial Discrimination1966 – Covenant on Economic Social and Cultural Rights1979 – Convention on Elimination of Discrimination against
Women1981 – African Charter of Human and People’s Rights1988 – American Protocol of San Salvador1989 – Convention on the Rights of the Child1990 – Cairo Declaration on Human Rights in Islam 2002 – Convention on the Protection of the Rights of Migrants
Workers
International and Regional Instruments with Right to Health

1212
1965 – Convention on Elimination of Racial Discrimination1966 – Covenant on Economic Social and Cultural Rights1979 – Convention on Elimination of Discrimination against
Women
1988 – American Protocol of San Salvador1989 – Convention on the Rights of the Child
2002 – Convention on the Protection of the Rights of Migrants Workers
– Constitution of Peru (articles 7, 9,11) – Universal Health Insurance Law (articles 4.1 and 5) – General Health Law
Peru’s International, Regional and National Commitments to the Right to Health

1313
193 185 173 160
Global ratifications of treaties with right to health
Economic and Social Rights Covenant
Racial Discrimination Covenant
Women's Covenant
Children's Covenant
Source: Forman, from UN OHCHR (2008)Source: Information drawn from UN OHCHR (2008)

1414
Domestic Force of the Right
2/3 of domestic constitutions protect health (Kinney & Clark, 2004)
Growing human rights jurisprudence on health and medicines
Consistent variables are ratification of Social Rights Covenant and constitutional entrenchment of health right (Hogerzeil et al, 2006)
ICESCR, Article 12
1. State parties recognize everyone’s right to the enjoyment of the highest attainable standard of physical and mental health
2. Steps to be taken include a. reducing still birth and infant mortality and for
children’s healthy developmentb. improving environmental and industrial hygienec. preventing, treating and controlling epidemic,
endemic, occupational and other diseased. creating conditions to assure to all medical services
and attention in sickness

General Comment 14 – Scope, Content and Duties
Right to health includes adequate health care and underlying determinants of health
Inclusive right interdependent with other rights
1616

Essential Elements of the Right to Health
Availability - sufficient quantities
Accessibility - non-discriminatory, physical, economic and informational
Acceptability - medically, ethically and culturally appropriate
Quality - Good quality goods and services

Relevance of AAAQ to Medicines
= Duty to realize access to available, accessible, acceptable and good quality medicines

Right to Health Obligations
Minimum core obligations not subject to resource constraints
Duty to progressively realize right to health
Duties to respect (don’t obstruct)protect (regulate corporations)fulfil (provide)

Duties relevant to medicines
Minimum core obligation to provide essential medicines
Duty to progressively realize access to available, accessible and good quality medicines

Duties relevant to trade
Take right to health obligations into account when entering bilateral or multilateral agreements
Ensure international agreements don’t adversely impact right to health
2222
Access to medicines as a human right
April 2001 Commission on Human Rights, Access to Medication in the Context of Pandemics
such as HIV/AIDS
June 2001 Intellectual Property Rights and Human Rights: Report of the Secretary-General
The Impact of TRIPS on Human Rights–Report of High Commissioner
August 2001 Intellectual Property Rights and Human Rights
Dec 2001 Committee on Economic, Social and Rights, Human Rights and Intellectual Property
July 2002 OHCHR and UNAIDS, Revised Guideline 6 on Access to Prevention, Treatment, Care
and Support

Commission on Human Rights, 2001
Access to medication in the context of pandemics such as HIV/AIDS is one fundamental element for achieving progressively the full realization of the right of everyone to the enjoyment of the highest attainable standard of physical and mental health

Commission on Human Rights (2001) continued
Calls on states to refrain from taking measures that would deny or limit equal access to pharmaceuticals to treat pandemics such as HIV/AIDS
Calls on states to ensure that their actions as members of international organizations take due account of the [right to health] and support public health policies which promote broad access to safe, effective and affordable pharmaceuticals

General Comment 17 (2005)
State parties should ensure that intellectual property rights do not impede core obligations under rights to food, health and education
State parties have a duty to prevent unreasonably high costs for access to essential medicines

Implications of right to health for trade
States should use TRIPS flexibilities to realize the right to health
States imposing/implementing TRIPS-plus rules in FTA may be violating the right to health
2626

Concern about impact of TRIPS-plus rules on right to health
Committee on Economic Social and Cultural Rights Concluding Observations Ecuador, 2004 Peru, 2006
Committee on the Rights of the Child Concluding Observations Thailand, 2006 Nicaragua, 2005 Philippines, 2005 El Salvador, 2004
What does this mean for social
and political actors in Peru?

3) Rights-based strategies to access medicines
Litigation Rights-based law & policy Participatory advocacy Impact assessment

1. Rights-based Litigation
Growing cases globally challenging government and companies
South Africa- NGOs sue Minister of Health, results in national MTCT policy
Thailand – NGOs successfully challenge AIDS patent
2. Rights-based policy approach
Policy based on participation, non-discrimination and accountability
Adopts right to health standards Essential elements (AAAQ)State duties (core, respect, protect, fulfil)
3131

Conceptual Framework AppliedAAAQ Access to Medicines
Availability Is the trade policy likely to enhance or jeopardize the availability of medicines in the State?
Accessibility Is the policy likely to enhance or jeopardize the physical and economic accessibility of medicines?
Acceptability Is the policy likely to enhance or jeopardize the ethical and/or cultural acceptability of medicines?
Quality Is the likely to enhance or jeopardize the quality of medicines?
3232Adapted from Hunt and MacNaughton, 2006

Applying Duties to PolicyGovernment Obligation Medicines
1. Minimum core duties •To provide accessible, available, acceptable, quality essential medicines (GC14)
2. Duty to respect •To prevent unreasonably high medicine prices (GC17)•Not to obstruct access to accessible, available, acceptable, quality essential medicines (GC14, CHR Resolutions)
3. Duty to protect • To prevent third parties from obstructing access (GC14)• To ensure international agreements do not adversely impact right to medicine (GC14, CHR Resolutions)
4. Duty to fulfill •State guarantees free access to health benefits and pensions, through public, private or mixed entities (Peru Constitution, article 11)•State guarantees universal health insurance for all Peru residents without discrimination (Universal Health Insurance Law, article 4.1)
3333

Rights-based medicines policy
MoH, DIGIMED duties to ensure available, affordable, accessible and good quality medicines
Implications for financingprocurementdistributionregistrationmarketing
Rights-based policy beyond the health sector
Trade, financing and patent departmentsHealth care financingTRIPS flexibilitiesFTA negotiations Patent law and policy
3535
3. Participatory Advocacy
Care Peru and Forasalud’s Health Rights ProgramTrainingCapacity buildingPolicy dialogue
Results: policy input, governmental representation, Ministry of Health mobilization on health rights and responsibilities
(Frisancho (2008), Frisancho and Goulden (2008)
3636

4. Impact assessment
Right to health standards used to reform trade-related patent law and policy
Ensure greater use of TRIPS flexibilitiesPeru’s impact assessment is keyMethod will be presented tomorrow

3838
AcknowledgementsResearch funded by
Canadian Institutes of Health Research
Comparative Program on Health and Society,
University of Toronto
Research Assistance – Jennifer Simpson
For further informationEmail: [email protected]

Profits before the Poor? Drugs giant offers an answer to the toxic question facing a ‘heartless’ industry
Sarah Boseley, 14 February 2009Andrew Witty, CEO of GlaxoSmithKline“Its been obvious for a while, I think, that efforts have to be made to really reassert and strengthen that contract with society.”
On the risk of re-importation of cheap drugs:
“Its not a reason not to do it. Of course it creates risk but now it’s our job to work with the Europeans and the Americans and whoever else is involved to try and get them to understand why it is important it doesn’t all get reimported, why it’s important that you don’t benchmark the price in New York to the price in Ethiopia, because it’s just wrong to do that. It’s almost as wrong to do that as it would be not to do it in the first place.”

Doha Ministerial Declaration on TRIPS and Public Health (November 2001)
TRIPS can and should be interpreted and implemented in a manner supportive of WTO Member’s right to protect public health and, in particular, to promote access to medicines for all.
We affirm the right of WTO Members to use, to the full, the provisions in the TRIPS Agreement, which provide flexibility for this purpose
Subsequent revision of requirement that license be predominantly for supply of domestic market (August 30 decision)

WHO Global Strategy on Public Health, Innovation and Intellectual Property
Reinforces use of specified and general flexibilities Doesn’t mention FTA or TRIPS-plus Does recommend that countries take public health
impact into account when considering more extensive intellectual property protection than in TRIPS (5.2.b) Specific flexibilities
research exceptions export to countries w/o manufacturing capacity ‘regulatory exception’ prevent abuse of intellectual property rights
General flexibilities adapt national legislation to use TRIPS flexibilities to the full policies to improve access to affordable products (6.3.b)

4242
Reports on Corporate Responsibility
1- Oxfam et al (2002) 2 - Core Ratings (2003) 3 - Henderson Global Investors (2003) 4 - Pharmaceutical Shareowners Group (2004) 5 - Pharma Futures (2004) 6 - Ethical Investment Research Services
(2005) 7 - WHO CIPIH (2006)8 - Access to Medicines Foundation I (2007)9 - Access to Medicines Foundation II (2007)
10 - DFID (2005)
4343
Investor and Shareholder Reports
Core Ratings (2003) Henderson Global Investors (2003) Pharmaceutical Shareowners Group (2004) Pharma Futures (2004) Ethical Investment Research Services (2005)
Reports conclude that failing to act responsibly threatens industry’s business model based on patents
Reports propose best practices to rebuild public trust and strengthen corporate license to operate
4444
Growing Consensus on Priorities & Best Practices
Pricing (1, 2, 6, 7, 8, 9)
Patents & Licencing (1, 2, 3, 6, 7, 8, 9)
Research and Development (1, 3, 6, 7, 8, 9)
Joint Public/Private Partnerships(1, 2, 3, 6, 7)
Donations (2, 3, 8, 9)
Responsible influence on public policy (4, 8, 9)
Transparent reporting (3, 4, 6, 8)
Philanthropic Activities (8, 9)
Board level leadership (4, 8)
Ethical Promotion & Marketing (8)
Drug Manufacturing, Distribution and Capability Advancement (9)
Ethical performance (3, 8)
Responsibility in governance (3)
Leadership in global health (3)

WHO and HAI, 2008, 175

Deletions on TRIPS-plus Rules
Deletes caution against adopting TRIPS-plus rules in bilateral free trade agreements
Deletes specified flexibilities and TRIPS-plus corrections parallel imports exploitation of expired or invalid patents restricting data-exclusivity
Recommends that countries take public health impact into account when considering more extensive intellectual property protection than in TRIPS (5.2.b)
4646

WHO and HAI, 2008, 176

No Innovation for Neglected Diseases
Troiller et al: Between 1975-1999, 0.1% of new chemical entities were for tropical diseases and tuberculosis
WHO identifies 14 neglected diseases but Moran et al suggest there are 30 neglected diseases and 127 neglected disease-product areas (Moran et al, 2009)
4848

Actions of the Global StrategyElement 1- Prioritize R&D Needs (13 sub-actions)
1.1 map global R&D
1.2 prioritize strategies for R&D
1.3 encourage R&D in traditional medicines
Element 2- promote R&D (22 sub-actions) 2.1 promote private and public sector cooperation on R&D
2.2 promote upstream R&D in developing countries
2.3 improve cooperation of R&D
2.4 promote greater access to knowledge and technology
2.5 establish and strengthen national R&D coordinating bodies
Element 3- Build and improve innovative capacity (18 sub-actions)3.1 build R&D capacity of developing countries
3.2 promote capacities for health innovation
3.3 support innovative capacity for developing country needs
3.4 promote innovation based on traditional medicine
3.5 develop and implement possible incentive schemes for innovation
4949

Actions of the Global Strategy contElement 4- Transfer of Technology (9 sub-actions)
4.1 promote tech transfer and production in developing countries
4.2 support collaboration and coordination of technology transfer
4.3 develop new mechanisms to promote transfer and access to key technologies
Element 5- Application & Management of Intellectual Property (15 sub-actions)
5.1 support information sharing and capacity building
5.2 provide technical support to use TRIPS, including flexibilities
5.3 promote incentive schemes for R&D
Element 6- Improve Delivery and Access (21 sub-actions)
6.1 encourage investment in infrastructure and financing of health products
6.2 strengthen ethical review and regulate quality, safety and efficacy
6.3 promote competition to improve availability and affordability
Element 7- Promote Sustainable Financing Mechanisms (6 sub-actions)
7.1 secure financing for R&D
7.2 facilitate use of existing financing
Element 8- Establish Monitoring and Reporting Systems
8.1 measure performance and progress towards GSPA objectives5050

AIDS Access Foundation et al v Bristol Myers-Squibb & Department of Intellectual
Property (Thailand, 2002)
Patent on AIDS drug challenged in IP and trade court
Court partially invalidated patent to permit domestic production and distribution of generic

FTA signed andapproved by US Congress
FTA signed, but not yet approved by US Congress
FTA currently being negotiated
Vietnam (2001) DR-CAFTA (Dominican Republic, Costa Rica, El Salvador, Guatemala, Honduras, Nicaragua)
Andean countries (Colombia, Ecuador, Peru)
Jordan (2001) Bahrain Thailand
Singapore (2003) Panama
Chile (2003) Southern African Customs Union (South Africa, Botswana, Lesotho, Namibia and Swaziland)
Morocco (2004) Free Trade Area of the Americas (Antigua and Barbuda,Argentina, Bahamas, Barbados, Belize, Bolivia, Brazil, Canada, Chile, Colombia, Costa Rica, Dominica, Dominican Republic,Ecuador, El Salvador, Grenada, Guatemala, Guyana, Haiti, Honduras, Jamaica, Mexico, Nicaragua, Panama, Paraguay, Peru, St. Vincent and the Grenadines, St. Lucia, St. Kitts and Nevis, Suriname, Trinidad and Tobago, Uruguay, and Venezuela)
Australia (2004) United Arab Emirates
Oman
Fink and Reichenmuller, 2005, USTR Website
US Free Trade Agreements

IGWG Process
First Session (4-8 December 2006) Second Session (5-10 November 2007) Resumed Second Session (28 April-3 May 2008)
1st Web-Based Hearing (1-14 November 2006) Country and Regional Consultations (August,
September & October 2007) 2nd Web-Based Hearing (15 August-30 September 2007)
61st World Health Assembly (May 2008)

5454
6.1 WHO should develop a Global Plan of action to secure enhanced and sustainable funding for developing and making accessible products to address diseases that disproportionately affect developing countries.

Snowballing Norms Cascade from AIDS Medicines to All Medicines?
1995-2001: Global refusal to fund AIDS treatment 2001: South African litigation 2001: Doha Declaration on Public Health 2001: UN human rights declarations on medicines 2002: Commission on Intellectual Property Rights 2002: Global Fund to Fight HIV/AIDS, TB and Malaria 2002: WHO and UNAIDS adopt “3x5” 2005: WHO, UNAIDS, UN General Assembly, G8 adopt
‘Universal access by 2010’ 2004-6: Commission on Intellectual Property, Innovation
and Health 2006-8: Intergovernmental Working Group on Public
Health, Innovation and Intellectual property 5555

5656
ARV Access Shoots Up
5757
Source: UN MDG Gap Task Force, 2008

World Time and the Right to Health
1976: ICESCR, article 12.1 (33 years ago)
1978: Declaration of Alma Ata
1985: Creation of Committee on Economic, Social and Cultural Rights (24 yrs ago)
2000: General Comment 14 on the Right to Health
2002: Special Rapporteur on the Right to Health
2005: General Comment 17 on Right to Benefit from Scientific Progress
2008: UNGA adopts Optional Protocol on ICESCR

Peru’s National Right to Health Commitments
Constitution of Peru, articles 7,9, 11Universal Health Insurance Law, article 4.1
and 5.General Health Law, introduction, articles
2, 3

Constitution of Peru
Article 7: Everyone has the right to the protection of their health, the health of their family and of the community, as well as the duty to contribute to its protection and defense. Persons incapacitated, either physically or mentally, have the right to respect of their dignity and to a legal regime of protection, attention, re-adaption and security
Article 9: The State determines national health policy. The Executive Power makes rules and supervises its application, and is responsible for designing and administering the plan in a decentralized and plural manner in order to assure equal access to health services for all
Article 11: The State guarantees free access to health benefits and pensions, through public, private or mixed entities.

Universal Health Insurance Law No. 29344
Article 4: The principles of universal health insurance are universality, solidarity, unity, integrality, equity and irreversibility
1. Universality - Health is a fundamental right enshrined in the Constitution of Peru and other documents and agreements signed by Peru and other laws of lower hierarchy; thus, universal health insurance is the guarantee of the protection of health for all Resident in Peru, without any discrimination, in all stages of life.
5. Equity – The health system provides health services of quality to the entire Peruvian population, giving priority to those most vulnerable and with fewer resources. To avoid discrimination based on ability to pay or financial risk, the system provides subsidized funding for the poorest and most vulnerable and mechanisms to avoid adverse selection.


















