
Campylobacterpylori and Gastroduodenal Disease · beenfound to be associated with ulcer...
12
CLINICAL MICROBIOLOGY REVIEWS, Jan. 1990, p. 1-12 Vol. 3, No. 1 0893-8512/90/010001-12$02.00/0 Copyright C 1990, American Society for Microbiology Campylobacter pylori and Gastroduodenal Disease GEORGE E. BUCK Department of Microbiology, Norton Hospital and Kosair Children's Hospital, Louisville, Kentucky 40232 INTRODUCTION .......................................1 GASTRIC DISEASES .......................................1 DISCOVERY OF C. PYLORI .......................................2 CHARACTERISTICS OF C. PYLORI .......................................2 TAXONOMY .......................................3 PATHOGENICITY .......................................4 Gastritis .......................................4 Pediatric Patients .......................................4 Epidemic Hypochlorhydria .......................................5 NUD .......................................5 Peptic Ulcers .......................................5 Other Gastric Conditions .......................................6 PRESENCE IN ASYMPTOMATIC PATIENTS .......................................6 MODE OF TRANSMISSION .......................................7 POSSIBLE MECHANISMS OF PATHOGENESIS .......................................7 LABORATORY DIAGNOSIS .......................................7 CONCLUSION .......................................9 ACKNOWLEDGMENTS .......................................9 LITERATURE CITED .......................................9 INTRODUCTION One of the fascinating aspects of medical microbiology is the periodic discovery of new organisms. In recent years, the human immunodeficiency virus, Legionella species, Bor- relia burgdorferi, and other new pathogens have been dis- covered. Campylobacter pylori is the latest addition to this group. Since its discovery in 1982 (80; J. R. Warren and B. J. Marshall, Letter, Lancet i:1273-1275, 1983), information has accumulated at a rapid rate. Although several recent publi- cations have reviewed various aspects of this organism and the diseases with which it has been associated (22, 35, 83), additional information has since accumulated and there has been no comprehensive review. The purpose of this review is to present a detailed discussion of this organism from the point of view of the microbiologist and to summarize current thinking regarding its role in disease. GASTRIC DISEASES Microbiologists generally have not dealt with diseases of the stomach; therefore, it may be useful to summarize several terms and concepts before proceeding further. Gas- tritis, as the name implies, refers to inflammation of the stomach. This is a heterogeneous condition, however, with a number of varieties defined by the area of the stomach affected, the suspected etiology, and the type of tissue damage. In addition, different authors have used different terms to describe the same conditions, thus adding to the confusion. Nevertheless, two major forms of gastritis have been defined, type A and type B. Type A seems to affect primarily the body of the stomach and involves destruction of the parietal (acid-producing) cells. This type seems likely to be an autoimmune disease, since antibodies to parietal cells can be found in the patient's serum. It is found frequently in patients with pernicious anemia (72, 120, 124). On the other hand, type B primarily involves the antrum (the portion just above the pylorus) but may also extend into the body of the stomach and affects the mucus-secreting cells. Both types are termed chronic gastritis, because they are generally long-term conditions and mononuclear cells are found in histological sections of the affected tissue. White- head et al. (133) introduced a system for subclassification of chronic gastritis which has been used by most subsequent investigators. According to their terminology, when poly- morphonuclear leukocytes are present in tissue sections in addition to mononuclear cells, the gastritis is called chronic active gastritis. This terminology is slightly different from the traditional terminology of inflammation, in which an infiltrate composed predominantly of polymorphonuclear cells is called acute inflammation and one composed pre- dominantly of mononuclear cells is called chronic inflamma- tion, but it has nevertheless been adopted by gastroenterol- ogists. Another term commonly used in the literature is atrophic gastritis. This was defined by Whitehead et al. (133) as inflammation extending to the glandular layer of the epithelial tissue, whereas superficial gastritis is defined as inflammation confined to the superficial epithelial cells, gastric pits, and related lamina propria. Since peptic ulcers are so common, many people are familiar with currently accepted concepts. It is worthwhile to point out that there are two types of peptic ulcers: gastric and duodenal. Over the years several factors, including genetic predisposition, smoking, and acid secretion, have been found to be associated with ulcer development. It has also been known for some years that patients with ulcers have gastritis (32, 52, 116), a fact that has taken on new significance with reports of bacteria being present. Nonulcer dyspepsia (NUD) is a term that may not be readily recognized by microbiologists. This is a condition in which patients have symptoms of peptic ulcer, such as epigastric pain, bloating, nausea, and vomiting, but no ulceration can be found. Little is known about the etiology of 1 on January 6, 2020 by guest http://cmr.asm.org/ Downloaded from
Transcript of Campylobacterpylori and Gastroduodenal Disease · beenfound to be associated with ulcer...

CLINICAL MICROBIOLOGY REVIEWS, Jan. 1990, p. 1-12 Vol. 3, No. 10893-8512/90/010001-12$02.00/0Copyright C 1990, American Society for Microbiology
Campylobacter pylori and Gastroduodenal DiseaseGEORGE E. BUCK
Department of Microbiology, Norton Hospital and Kosair Children's Hospital, Louisville, Kentucky 40232
INTRODUCTION.......................................1GASTRIC DISEASES.......................................1DISCOVERY OF C. PYLORI.......................................2CHARACTERISTICS OF C. PYLORI.......................................2TAXONOMY.......................................3PATHOGENICITY.......................................4
Gastritis.......................................4Pediatric Patients.......................................4Epidemic Hypochlorhydria.......................................5NUD.......................................5Peptic Ulcers.......................................5Other Gastric Conditions.......................................6
PRESENCE IN ASYMPTOMATIC PATIENTS .......................................6MODE OF TRANSMISSION.......................................7POSSIBLE MECHANISMS OF PATHOGENESIS.......................................7LABORATORY DIAGNOSIS.......................................7CONCLUSION.......................................9ACKNOWLEDGMENTS.......................................9LITERATURE CITED.......................................9
INTRODUCTION
One of the fascinating aspects of medical microbiology isthe periodic discovery of new organisms. In recent years,the human immunodeficiency virus, Legionella species, Bor-relia burgdorferi, and other new pathogens have been dis-covered. Campylobacter pylori is the latest addition to thisgroup. Since its discovery in 1982 (80; J. R. Warren and B. J.Marshall, Letter, Lancet i:1273-1275, 1983), information hasaccumulated at a rapid rate. Although several recent publi-cations have reviewed various aspects of this organism andthe diseases with which it has been associated (22, 35, 83),additional information has since accumulated and there hasbeen no comprehensive review. The purpose of this reviewis to present a detailed discussion of this organism from thepoint of view of the microbiologist and to summarize currentthinking regarding its role in disease.
GASTRIC DISEASES
Microbiologists generally have not dealt with diseases ofthe stomach; therefore, it may be useful to summarizeseveral terms and concepts before proceeding further. Gas-tritis, as the name implies, refers to inflammation of thestomach. This is a heterogeneous condition, however, with anumber of varieties defined by the area of the stomachaffected, the suspected etiology, and the type of tissuedamage. In addition, different authors have used differentterms to describe the same conditions, thus adding to theconfusion. Nevertheless, two major forms of gastritis havebeen defined, type A and type B. Type A seems to affectprimarily the body of the stomach and involves destructionof the parietal (acid-producing) cells. This type seems likelyto be an autoimmune disease, since antibodies to parietalcells can be found in the patient's serum. It is foundfrequently in patients with pernicious anemia (72, 120, 124).On the other hand, type B primarily involves the antrum
(the portion just above the pylorus) but may also extend intothe body of the stomach and affects the mucus-secretingcells. Both types are termed chronic gastritis, because theyare generally long-term conditions and mononuclear cells arefound in histological sections of the affected tissue. White-head et al. (133) introduced a system for subclassification ofchronic gastritis which has been used by most subsequentinvestigators. According to their terminology, when poly-morphonuclear leukocytes are present in tissue sections inaddition to mononuclear cells, the gastritis is called chronicactive gastritis. This terminology is slightly different fromthe traditional terminology of inflammation, in which aninfiltrate composed predominantly of polymorphonuclearcells is called acute inflammation and one composed pre-dominantly of mononuclear cells is called chronic inflamma-tion, but it has nevertheless been adopted by gastroenterol-ogists. Another term commonly used in the literature isatrophic gastritis. This was defined by Whitehead et al. (133)as inflammation extending to the glandular layer of theepithelial tissue, whereas superficial gastritis is defined asinflammation confined to the superficial epithelial cells,gastric pits, and related lamina propria.
Since peptic ulcers are so common, many people arefamiliar with currently accepted concepts. It is worthwhileto point out that there are two types of peptic ulcers: gastricand duodenal. Over the years several factors, includinggenetic predisposition, smoking, and acid secretion, havebeen found to be associated with ulcer development. It hasalso been known for some years that patients with ulcershave gastritis (32, 52, 116), a fact that has taken on newsignificance with reports of bacteria being present.Nonulcer dyspepsia (NUD) is a term that may not be
readily recognized by microbiologists. This is a condition inwhich patients have symptoms of peptic ulcer, such asepigastric pain, bloating, nausea, and vomiting, but noulceration can be found. Little is known about the etiology of
1
on January 6, 2020 by guesthttp://cm
r.asm.org/
Dow
nloaded from

CLIN. MICROBIOL. REV.
this condition (126), and therapy is usually not helpful (121).It may well be a heterogeneous entity, i.e., a group of relatedconditions with closely related symptoms but different etiol-ogies (122).
DISCOVERY OF C. PYLORI
Spiral bacteria were first described in gastric tissue ofhumans early in this century (62), following similar observa-tions made in other animals (5, 114). Subsequent investiga-tors confirmed this finding and attempted to correlate thepresence of these organisms with various pathological con-ditions, with various degrees of success (12, 20, 21, 29, 69).One of the difficulties with most of these studies was that thegastric tissue was obtained at autopsy; thus, invasion of theorganisms after the death of the patient could not be ruledout (29). Palmer (97) attempted to resolve this question byobtaining tissue from living subjects with a vacuum tubetechnique but failed to observe any bacteria. Consequently,interest in this subject waned for almost 30 years. During thistime, reports relating bacteria to gastric ulcers (119) andchronic gastritis (30) appeared, but this work received littleattention.A major breakthrough came in 1983, when Warren and
Marshall published their observations (Warren and Mar-shall, Letter). Warren, a pathologist, had previously ob-served in gastric tissue spiral bacteria that seemed to beassociated with active chronic gastritis, and he and Marshallconducted studies to confirm this association. Since thebacteria they saw in the biopsy material were morphologi-cally similar to Campylobacter species, they reasoned thatmicroaerophilic conditions might be required for growth andwere able to recover an organism in vitro. They examinedantral biopsies from 100 patients with gastric symptoms andfound a striking relationship between the bacteria and gas-tritis and peptic ulcers (80), especially duodenal ulcers. Theorganism, which was found to be a new species, wasoriginally called pyloric Campylobacter-like organism, orgastric Campylobacter-like organism, and then named Cam-pylobacter pyloridis (78). Because this name violated theinternational rules of nomenclature, it was subsequentlyamended to Campylobacter pyrlori (75).
CHARACTERISTICS OF C. PYLORI
C. pylori is a gram-negative, curved or spiral bacterium(10, 57, 80, 104). Unique "oxbow" shapes have been de-scribed (10, 87), and these are often especially prominentwhen the organism is grown in vitro (10). The cells areusually 2.5 to 3.5 pum long and 0.5 to 1.0 pLm in diameter (39,54, 78, 104, 111), although longer forms are occasionallyseen (39, 111), and they have a wavelength of about 0.9 to 1.2pum (111; A. D. Phillips, K. R. Hine, G. K. T. Holmes, andD. F. Woodings, Letter, Lancet ii:100, 1984). They usuallypossess one to six polar flagella (39, 54, 78, 80, 104, 123),which are covered with a membrane sheath (Fig. 1) andappear to have a terminal bulb (39; Warren and Marshall,Letter). The cells have smooth surfaces and rounded ends.This contrasts with cells of other Campylobacter species,which have ruffled surfaces, pointed ends, and depressionsin the end (Fig. 2) (39, 54).The organism has been grown on blood agar, chocolate
agar, Skirrow medium, and Thayer-Martin medium (10, 78,97). It grows slightly on GC agar base and Mueller-Hintonagar without additional supplementation but grows muchbetter when these media are supplemented with serum,
FIG. 1. Transmission electron micrograph showing the sheathedstructure of flagella from C. pylori. Magnification, x 150,000.
activated charcoal, or soluble starch (10, 11). It fails to growon other common laboratory media, such as brucella agarand brain heart infusion agar, unless supplemented withblood, serum, or one of the other supplements mentionedabove (11). Broth culture media must also be supplemented(11, 57, 87). Morgan et al. reported that growth in broth wasenhanced by using a large surface area and agitation (90).Early publications reported a requirement for hemin (49),but this has not been substantiated (11, 78).One of the basic characteristics of C. pylori is its mi-
croaerophilic nature. Although some isolates grow in 5 to10% CO2 or under anaerobic conditions, these conditionsseem less satisfactory (10, 78). It grows at 370C but not at 25to 30'C, and different workers have obtained different resultsfor growth at 420C (1, 10, 57, 78, 80, 104). On appropriatemedia, colonies usually develop after about 3 days of incu-bation, although up to 7 days of incubation are sometimesrequired for recovery of the organism in primary culture.They are greyish and reach a maximum size of approxi-mately 0.5 to 1.0 mm (10, 57, 78, 80).The biochemical characteristics include positive oxidase
and catalase tests (10, 78, 80, 123). A striking feature is theabundant production of urease, which has been implicated asa possible pathogenic mechanism and forms the basis forrapid detection systems (see below). The urease enzyme hasbeen characterized and appears to be different from theenzymes of other common urease-producing bacteria (88).Other biochemical characteristics include production of hy-drogen sulfide (when detected with lead acetate paper),
2 BUCK
on January 6, 2020 by guesthttp://cm
r.asm.org/
Dow
nloaded from

C. PYLORI AND GASTRODUODENAL DISEASE 3
.e jjjej
-3__
_:,_'P
AFIG. 2. Transmission electron micrographs showing the ultrastructure of C. jejuni (A) and C. pylon (B); magnification, x 57,000. C. jejuni
has a ruffled surface, tapered ends with a depression in the end, and single polar flagellum. C. pylori is slightly larger, with rounded ends anda smooth surface.
alkaline phosphatase, -y-glutamyl aminopeptidase, leucineaminopeptidase, and DNase (84, 87). It does not fermentcarbohydrates and does not produce indole or grow in 1%bile salts, 1% glycine, or 3.5% sodium chloride; it is nitrateand hippurate negative (10, 78, 80, 84, 87, 123).
C. pylori is susceptible to amoxicillin, ampicillin, carben-icillin, cefamandole, cefoxitin, cephalothin, cephradine,chloramphenicol, ciprofloxacin, clindamycin, clorobiocin,CP 62993, doxycycline, erythromycin, gentamicin, imi-penem, kanamycin, minocycline, nifuroxazide, nitrofuran-toin, norfloxacin, ofloxacin, oxolinic acid, rifampin,roxithromycin, tetracycline, and tobramycin (2, 10, 16, 36,57, 78, 80, 86, 117, 123, 128). Most isolates are resistant tocolistin, nalidixic acid, trimethoprim, sulfonamides, vanco-mycin, and polymyxin B (10, 57, 78, 80, 117, 123), and someare resistant to cefaclor, metronidazole, and penicillin (78,86, 128). Since drugs such as cimetidine and bismuth com-pounds have been used for treating gastric disease for anumber of years, there has been significant interest inexamining the in vitro activity of these agents against C.pylori. The results show that it is susceptible to bismuthcompounds but resistant to cimetidine, ranitidine, famoti-dine, and sucralfate (2, 3, 36, 86, 119). Armstrong et al. (3)investigated the ultrastructural effects of several antibioticsand acid-reducing agents. They found that structural defectsdeveloped when the organism was treated with amoxicillin,penicillin, or cephalexin. No structural changes were notedwith bismuth subcitrate treatment, but particulate bismuth
complexes appeared to accumulate inside the cells. VanCaekenberghe and Breyssens (128) investigate the synergis-tic effect of bismuth subcitrate with several different antibi-otics and found that oxolinic acid produced a synergisticeffect with all strains tested and several other antibioticsacted synergistically with some isolates. One of the diffi-culties with in vitro susceptibility testing is that resultsobtained at pH 7.4 may bear little relation to the gastricenvironment, which may have a pH of 4, 5, or 6 (44).
TAXONOMY
On the basis of spiral morphology, microaerophilic nature,and early data showing a G+C ratio of 35.8 to 37.1 mol%(78), the organism was initially placed in the genus Campylo-bacter. However, as more information has accumulated,significant differences have become apparent. The mostobvious are the morphological differences between thisorganism and other Campylobacter species mentioned ear-lier. Other differences include the fatty acid composition ofthe cell wall (39) and whole-cell protein profiles examined bypolyacrylamide gel electrophoresis (55, 93, 101).
Definitive taxonomic data have been provided by recentanalyses of partial 16S rRNA sequences. These studies (64,99, 112) show that C. pylori is more closely related toWolinella succinogenes than to other species of Campylo-bacter. Thompson et al. (125) reported that "C. cinaedi,""C. fennelliae," W. succinogenes, and C. pylori form a
VOL. 3, 1990
,.A ;%'," -gff 4z1 O 01A'r NW,
'Nr. 1,
on January 6, 2020 by guesthttp://cm
r.asm.org/
Dow
nloaded from

CLIN. MICROBIOL. REV.
closely related taxonomic group and proposed that the nameWolinella be retained for the group, because W. succino-genes is the type species for this genus. Whether this will beaccepted is not yet known.
PATHOGENICITY
The reports by Marshall and Warren (80; Warren andMarshall, Letter) triggered the interest of other investigatorsaround the world, and numerous publications soon appearedconfirming the existence of C. pylori and its association withgastric disease. The cardinal question then became whetherthis organism actually causes disease or merely inhabitsdamaged tissue. The evidence related to this question will bediscussed for each type of disease.
Gastritis
Recent studies have shown a highly significant relation-ship between C. pylori and gastritis (1, 7, 10, 13, 18, 24, 31,57, 59, 71, 94, 100, 104, 111, 113, 123, 132). There has beensome disagreement about the type of gastritis with which it isassociated; i.e., in studies in which the type of gastritis wasspecified, some investigators found that the bacteria wereassociated mostly with chronic active gastritis (1, 13, 59, 80,113), while others noted association with both chronic andchronic active gastritis (18, 57, 107). There is also disagree-ment about the relationship between the quantity of bacteriapresent and the severity of inflammation (1, 7, 57, 80, 107,132). Nevertheless, it appears that some type of inflamma-tion is virtually always found when the organism is present.On the other hand, studies of the organism in subjects withnormal gastric tissue have generally reported a prevalence of<10% (1, 31, 45, 57, 80, 123, 132), although a few studieshave reported slightly higher rates (10, 13, 111). Therefore,the organism seems to be uncommon in individuals withnormal gastric mucosa. In addition, it is not associated withdrug-induced gastritis (45), autoimmune gastritis (H. J.O'Connor, A. T. R. Axon, and M. F. Dixon, Letter, Lancetii:1091, 1984; D. Gonzalez Juan, F. J. Sancho, S. Sainz, J.Such, M. Fernandez, and J. Mones Xiol, Letter, Lancet i:57,1988), or gastritis in children when another cause can beidentified (23, 24), suggesting that it does not merely colonizedamaged tissue.Other evidence supporting a causative role for the organ-
ism in gastritis is that serum (7, 37, 55, 57, 58, 108, 132) andlocal (108, 135) antibodies are produced by the host and thebacteria appear to attract and be ingested by polymorpho-nuclear leukocytes (S. Shousha, T. B. Bull, and R. A.Parkins, Letter, Lancet ii:101, 1984). Also, ultrastructuralexamination of tissue from patients with C. pylori and gastricinflammation (13) has shown interruption of intercellulartight junctions and other ultrastructural damage to gastricepithelial cells.More substantial evidence for a causative role comes from
treatment studies. Treatment of patients with either colloidalbismuth subcitrate (De-Nol) or bismuth subsalicylate (Pepto-Bismol) reduces the number of campylobacters and pro-duces a parallel resolution of the inflammation (53, 73, 85).Since bismuth compounds may have antisecretory and othereffects besides antibacterial activity, however, treatmentstudies with antibiotics probably provide better evidence.Studies with furazolidone, nitrofurantoin (R. Gilman, R.Leon-Barua, A. Ramirez-Ramos, D. Morgan, S. Recavar-ron, W. Spira, P. Watanabe, W. Kraft, and A. Pearson,Gastroenterology 92[Part 2]:1405, 1987), and amoxicillin (34,
109) have shown clearance of organisms and resolution ofthe inflammation.One of the problems with most of these treatment studies,
however, has been a high relapse rate when the antibacterialagents were discontinued. Recent studies have suggestedthat more permanent clearance may be provided by using acombination of agents. Marshall et al. (73) reported that acombination of bismuth subcitrate and amoxicillin or tinida-zole provided more long-lasting clearance, and Borsch et al.(G. Borsch, U. Mai, and W. Opferkuch, Gastroenterology94[Part 2]:A44, 1988), using bismuth subsalicylate plusamoxicillin and metronidazole, were able to eradicate theorganism in 90% of patients for at least 4 weeks. Althougherythromycin inhibits the organism when tested in vitro, ithas not been effective when used to treat patients (85).The best evidence that the organism causes gastritis has
been obtained through volunteer studies. Marshall et al. (74)described an experiment in which a subject ingested about109 C. pylori. A biopsy of the gastric antrum before theexperiment started showed normal gastric epithelial cells. Aweek after ingesting the bacteria the subject noted mildgastric symptoms, and a biopsy of the epithelium taken 10days after ingestion showed abnormal epithelial cells, deple-tion of mucus, and accumulation of polymorphonuclearleukocytes. Another biopsy taken at day 14 showed that theinfection was spontaneously resolving by that time. Morrisand Nicholson (91) published a similar experiment. In theircase, the subject developed epigastric pain and vomiting 2 to4 days after ingestion of a C. pylori culture. A biopsy takenat day 5 showed acute antral gastritis and gram-negativespiral bacilli in the tissue, and C. pylori was recovered onculture. The gastric pH was elevated on day 8 of theexperiment and remained elevated until treatment wasstarted. Treatment with doxycycline was begun on day 25but proved ineffective and was changed to bismuth subsalic-ylate. After 28 days of this treatment, no organisms could berecovered, and only mild residual chronic gastritis remained.When considered together, these data provide substantialevidence that C. pylori is indeed a cause of gastritis. Whilemost of the studies have examined gastritis in the antrum,there is evidence that the body and fundus of the stomachcan also be affected (47; R. Leon-Barua, W. M. Spira, A.Ramirez-Ramos, R. H. Gilman, S. Recavarren, J. Wata-nabe, and J. Cok, Gastroenterology 92[Part 2]:1501, 1987;J. T. Bickel, M. Brophy, R. S. Gitan, and R. W. Madson,Gastroenterology 94[Part 2]:A25, 1988). However, the exactmechanism by which the organism produces this inflamma-tion has yet to be elucidated.
Pediatric Patients
Although most information about the association of C.pylori with gastric disease has been obtained from adultpatients, several investigators have recently published ob-servations on the role of the organism in gastric disease ofchildren. In a 1-year survey, De Giacomo et al. (C. DeGiacomo, G. Maggiore, and R. Fiocca, Letter, Am. J.Gastroenterol. 83:202, 1988) diagnosed chronic gastritis in 18Italian children and found evidence of spiral bacteria in 8.Czinn et al. (18) reported five patients between the ages of 10and 16 with spiral bacteria resembling C. pylori in theirgastric tissues. All five had abdominal pain and three of thefive had hematemesis. All of the patients had chronic gastri-tis with nodules in the gastric antrum, but there was noevidence of acute inflammation. Drumm and co-workersperformed both retrospective (23) and prospective (24) stud-
4 BUCK
on January 6, 2020 by guesthttp://cm
r.asm.org/
Dow
nloaded from

C. PYLORI AND GASTRODUODENAL DISEASE 5
ies and found evidence of C. pylori in the antrum of patientswith active gastritis, but not in patients with normal gastricmucosa or in patients with gastritis resulting from otherknown conditions. Eastham et al. (25) found the organism inassociation with antral gastritis. The patients had circulatingantibody to the bacterium, and treatment eradicated theorganism and resulted in resolution of inflammation andsymptoms. Hill et al. (50) reported three children withprotein-losing enteropathy associated with acute gastritisand infection with C. pylori. Two of the patients were treatedwith erythromycin and the third was treated with antacids.In all three, the gastric mucosa returned to normal, theorganism disappeared, and the serum protein returned tonormal. These studies require additional confirmation beforefirm conclusions can be established.
Epidemic HypochlorhydriaIn 1979, an outbreak of hypochlorhydria was described
among volunteers enrolled in a study of gastric physiology(106). A similar outbreak was reported some years later (33).In both instances the affected subjects exhibited mild gastricsymptoms, including nausea, vomiting, and abdominal pain,several days before hypochlorhydria was detected, andbiopsies of gastric tissue revealed the presence of gastritis.These illnesses were termed epidemic hypochlorhydria, andan unknown pathogenic agent was suspected in both in-stances. In retrospect, the illness described resembles cam-pylobacter-associated gastritis. Gastric tissue and sera fromthe volunteers in one of the studies was saved and examinedrecently for evidence of C. pylori. Spiral bacteria were seenwith approximately equal frequency in subjects with andwithout hypochlorhydria. However, subjects with gastritisand hypochlorhydria had significantly higher titers of anti-body to C. pylori than did asymptomatic subjects (W.Peterson, E. Lee, and M. Skoglund, Abstr. Int. Campylo-bacter Workshop 1987, Keystone, Colo.). An isolated casewas reported recently (40) in which C. pylori was shown tobe absent prior to the onset of illness and present after theillness began. In light of data from human volunteers show-ing that increased gastric pH accompanies infection with C.pylori (91) and the fact that the organism has been shown toadhere to endoscopes (C. R. Fricker, Letter, Lancet i:800,1984), it seems likely that these outbreaks were cases ofacute gastritis caused by this organism and the bacteria weretransmitted by equipment during examination of the sub-jects.
NUD
The prevalence of C. pylori in patients with NUD is 45 to70% and the prevalence of gastritis is similar (68, 77, 109,110, 126, 127), suggesting possible involvement of the organ-ism in the disease. One of the problems with assessing thesedata is that there is an age-related increase in the prevalenceof the organism (43, 50, 92), and, thus, C. pylori is found inabout 50% of asymptomatic individuals 50 to 60 years old.Graham and Klein (41) have argued that, because many ofthe individuals with NUD are in this age group, the statisticalrelationship with NUD may be a coincidence. A recent studyby Rokkas et al. (110), however, showed that, whereas theorganism could be found in a significant proportion ofage-matched asymptomatic control subjects, the prevalencewas significantly higher in NUD patients. The best evidencefor involvement of C. pylori in NUD would be in animalmodel or human volunteer studies, but no animal model has
been described as yet. Although the two subjects in thepublished human volunteer studies (74, 91) developed symp-toms, it is questionable whether their symptoms were anal-ogous to those in a typical case of NUD, since they devel-oped acute symptoms and NUD is a chronic illness.At present, then, treatment studies may be the only means
for assessing the role of C. pylon in NUD. McNulty et al.(85) found no significant difference in improvement of symp-toms between patients in whom C. pylori had been clearedand patients in whom the organism persisted. On the otherhand, Lambert et al. (J. R. Lambert, M. Borromeo, M. G.Korman, and J. Hansky, Gastroenterology 92[Part 2]:1488,1987) reported that treatment with bismuth subcitrate de-creased abdominal pain, but had little or no effect on othersymptoms. Borody and colleagues (T. Borody, W. Hennes-sey, G. Daskalopoulos, J. Carrick, and S. Hazell, Gastroen-terology 92[Part 2]:1324, 1987) treated patients with a com-bination of bismuth subcitrate, tinidazole, and amoxicillin,erythromycin, or tetracycline and reported a significantdecrease in epigastric pain or burning, abdominal distention,and nausea. These reports need additional confirmation,however. Even if additional evidence can be obtained,statistical significance may not mean clincial significance;i.e., the relief from symptoms may not be appreciableenough to warrant routine treatment.
Furthermore, if C. pylori participates in NUD develop-ment, why is the organism present in only 50 to 70% of thepatients? One possibility is that the same set of diseasesymptoms may have more than one cause and patientswithout the organism may have symptoms resulting fromanother cause. Currently, then, only meager information isavailable regarding the role of C. pylori in NUD, and theconclusions are controversial. A great deal more work isnecessary to define this association clearly.
Peptic Ulcers
One of the striking aspects of the original work by Mar-shall and Warren (80) was the association found between C.pylori and peptic ulcers. They found the organism in 100% ofduodenal ulcer patients and 77% of gastric ulcer patientsthey examined. Although some investigators subsequentlyfailed to confirm these findings (10, 111, 123), others foundsimilar results (7, 53, 94, 104, 109). The discrepanciesbetween studies probably reflect sampling error, which isone of the major difficulties of this type of study.Why there is a weaker association with gastric ulcers than
with duodenal ulcers is not clear. A possible explanation wasproposed by O'Connor and colleagues (95, 96). They foundthat C. pylori seemed to be absent in patients with highduodenogastric reflux and suggested that reflux gastritisrepresents a distinct entity. Thus, gastric ulcer patientswithout this organism might have disease due to reflux of bileand acid from the duodenum. While this is an attractivehypothesis, it has been challenged (T. Karttunen and S.Niemela, Letter, Lancet i:118, 1988) and remains to befirmly established. On the other hand, Rauws et al. (109)reported that, with careful exclusion of other known causesof gastric ulcer, such as the use of analgesics, the prevalenceof C. pylori in gastric ulcer patients approaches 100%.Even before the recognition of C. pylori, it was known that
gastritis occurred in peptic ulcer patients (116) and remainedafter conventional treatment with H2 blockers, suggestingthat the "healing" was not complete (H. Fullman, G. VanDeventer, D. Schneidman, J. Walsh, J. Elashoff, and W.Weinstein, Gastroenterology 88[Part 21:1390, 1985). More-
VOL. 3, 1990
on January 6, 2020 by guesthttp://cm
r.asm.org/
Dow
nloaded from

CLIN. MICROBIOL. REV.
over, the relapse rate for ulcers had been shown to be lowerin patients treated with bismuth compounds than in thosetreated with H2 blockers (66, 129). The discovery of C. pyloriprovided a plausible explanation for these observations. Areliable animal model or the ability to reproduce the diseasein human volunteers would provide definitive proof forinvolvement of the organism. Such proof is not availablenow and, for ethical or technical reasons, may be difficult toobtain. Therefore, the only evidence that C. pylori is in-volved in peptic ulcers has come from treatment studies.Humphreys et al. (53) showed that healing of ulcers with
bismuth subcitrate correlated with the clearance of C. pylori.Lambert et al. (J. R. Lambert, M. Borromeo, M. G. Kor-man, J. Hansky, and E. R. Eaves, Gastroenterology 92[Part21:1489, 1987) treated 45 patients with bismuth subcitrate for8 weeks. Ulcer relapse occurred more frequently in patientsin whom the bacteria persisted than in those in whom thebacteria were eradicated. Borody and colleagues (T.Borody, P. Cole, S. Noonan, A. Morgan, G. Ossip, J.Maysey, and S. Brandl, Gastroenterology 94[Part 2]:A43,1988) treated patients with a combination of bismuth subci-trate, metronidazole, and either tetracycline or amoxicillin.Eight weeks after treatment, 94% of the patients were stillnegative for the organism by histological stain and directurease testing; 93% had a reduced number of polymorpho-nuclear leukocytes, and 76% had a reduced number oflymphocytes. Fifty patients who were successfully treatedwere followed for more than 18 months. Twenty-one of theseoriginally had duodenal ulcers; all but three remained free ofulcers and negative for C. pylori for 18 months or longer. Thethree subjects in whom ulcers recurred also became positiveagain for the organism.
Although the latter two reports seem to suggest a role forthe organism in ulcers, the studies did not include groupstreated with H2 blockers or placebo for comparison, thusleaving some question. More convincing evidence has beenprovided by two other studies. Coghlan et al. (14) treatedgroups of duodenal ulcer patients with bismuth subcitrate orcimetidine and then followed the relapse rate in patientswhose ulcers healed. Relapse occurred more often in pa-tients who were positive for C. pylori (by culture or histol-ogy) at the end of treatment than in patients who werenegative. In addition, no patient who remained negative forthe organism had gastritis, whereas all patients in whom theorganism recurred developed gastritis. This finding suggeststhat the organism is a factor in recurrence of ulcers. Marshalland colleagues (76) randomized duodenal ulcer patients tofour treatment groups: cimetidine plus placebo or tinidazoleand bismuth subcitrate plus placebo or tinidazole. C. pyloripersisted in all patients in the cimetidine-placebo group and95% of patients in the cimetidine-tinidazole group. It waseradicated in 27% of the bismuth-placebo group and 70% ofthe bismuth-tinidazole group. When C. pylori persisted, 61%of the ulcers healed and 84% relapsed. When C. pylori waseradicated, 92% of the ulcers healed and only 21% relapsed.On the other hand, Graham et al. (D. Y. Graham, P. H.Jordan, A. R. Opekun, I. A. David, and P. D. Klein,Gastroenterology 94[Part 2]:A152, 1988) reported evidencethat C. pylori may not be the only factor involved in ulcerproduction. They studied patients who had previously un-dergone highly selective vagotomy to cure their ulcers. Eventhough 77% of these patients were infected with C. pylori,only 13% experienced ulcer relapse. Therefore, the presenceof the organism alone is not sufficient for development ofulcers, and they concluded that, while infection with the
organism may contribute to ulcer production, it is not theabsolute cause.
In conclusion, then, evidence for a role of C. pylori inpeptic ulcers is relatively meager. Available data suggestthat the organism is involved in some way in the develop-ment of ulcers but is probably not the only factor involved.If the process of ulcerogenesis is thought of as a sequence ofsteps leading to the final outcome of tissue destruction,infection with the organism may be one of the steps. Whileconventional ulcer therapy, such as H2 receptor antagonistsor vagotomy, can affect the final outcome of the process,these treatments have little or no effect on the presence ofthe organism. On the other hand, treatment of C. pylori mayinterrupt the process at an earlier stage or simply eliminateone additional factor favoring development of ulcers.
Other Gastric Conditions
C. pylori has been reported in about 75% of patients withalcohol-induced hemorrhagic and erosive gastritis (L. Laine,M. Marin-Sorensen, and W. M. Weinstein, Gastroenterol-ogy 94[Part 2]:A246, 1988), but these observations have notbeen confirmed and their significance is not clear. There areunconfirmed reports of an association with gastric carcinoma(J. R. Lambert, K. L. Dunn, E. R. Eaves, M. G. Korman,and J. Hansky, Gastroenterology 90[Part 2]:1509, 1986) andgastric mucosal dysplasia (R. Leon-Barua, S. Recavarren-Arce, A. Ramirez-Ramos, R. H. Gilman, W. M. Spira, C.Rodriguez, G. Garrido-Klinge, and F. Atanassio, Gastoren-terology 94[Part 2]:A256, 1988), but the significance of theseobservations is also not clear.Three reports have described the presence of the organism
in the esophagus. Hazell et al. (S. L. Hazell, J. Carrick, andA. Lee, Gastroenterology 94[Part 2]:A178, 1988) found it inassociation with chronic inflammation, but only in areaswhere gastric metaplasia, i.e., a change to gastric-typeepithelial tissue, had developed. On the other hand, otherinvestigators found the organism in only the lower portion ofthe esophagus in the absence of inflammation and concludedthat it was present there because of gastro-esophageal refluxor concomitant carriage in the antrum (E. H. Zimbalist,E. B. Dreznick, and G. S. Gettenberg, Gastroenterology94[Part 2]:A517, 1988; R. W. McCallum, V. Deluca, andB. J. Marshall, Gastroenterology 92[Part 2]:1524, 1987).Therefore, its significance at this site is not clear.A recent report described C. pylori in the rectum of a
patient where it occurred in association with a chronicinflammatory reaction in gastric-type epithelial cells thatapparently developed in the rectum (D. J. Pambianco, K. R.Dye, B. J. Marshall, H. F. Frierson, R. H. MacMillan, D.Franquemont, and R. W. McCallum, Gastroenterology94[Part 2]:A340, 1988). The significance of this observationis also unknown, however.While these reports suggest that C. pylori may be associ-
ated with gastric-type epithelium that develops in the intes-tinal tract or esophagus, the organism does not appear tocolonize intestinal epithelium that develops in the stomach(i.e., intestinal metaplasia [31]). These findings suggest apossible predilection for gastric-type epithelium, but nodirect evidence is available to support this.
PRESENCE IN ASYMPTOMATIC PATIENTS
As mentioned previously, several studies have shown anincrease in the prevalence of C. pylori with age (43, 55, 92),reaching a level of 50% or more in asymptomatic people over
6 BUCK
on January 6, 2020 by guesthttp://cm
r.asm.org/
Dow
nloaded from

C. PYLORI AND GASTRODUODENAL DISEASE 7
the age of 50. How, then, can the organism be a pathogenwhen it is found in so many asymptomatic individuals?Dooley et al. (C. P. Dooley, P. Fitzgibbons, H. Cohen,M. D. Appleman, G. P. Perez, and M. J. Blaser, Gastroen-terology 94[Part 2]:A102, 1988) examined the prevalence inasymptomatic individuals and found that all persons with C.pylori also had gastritis. Thus, it is virtually always found inassociation with inflammation, though not necessarily withovert symptoms.Lee and Hazell (65), discussing the organism from an
ecological perspective, suggested that it is highly adapted tothe gastric environment and proposed that it be considered"almost" normal flora, i.e., an organism that occurs com-monly in the population but which causes disease in only a
few individuals. Expressing this another way, one could saythat C. pylon is a pathogen, but one that most often causesasymptomatic infection. At certain times or in certain indi-viduals it may cause, or participate in the production of,symptomatic disease, but the full extent of its participation isstill being defined. Certainly other known pathogens may
cause asymptomatic disease. C. pylon may have a lowerlevel of virulence than traditional pathogens and, therefore,produce a larger production of asymptomatic infections.
MODE OF TRANSMISSION
Since its discovery, one of the puzzles about C. pylon hasbeen where it comes from and how it is transmitted. Thiscannot be answered conclusively yet, but information hasbecome available that permits some speculation. Since othercampylobacters can be acquired from animals (6), an animalreservoir initially seemed like a good possibility. However,C. pylori has not been reported from animals, except non-human primates (4, 9), and these are unlikely to be a
significant source for most people.Attempts to isolate the organism from the periodontal
pockets of patients with gastritis have been negative (L. E.Rosenthal, D. Smoot, and H. L. T. Mobley, Letter, Am. J.Gastroenterol. 83:202, 1988), but highly sensitive methods,such as DNA probes, have not yet been used to address thisquestion. The age-related increase in prevalence suggeststhat the organism is acquired as people become older,although the actual prevalence may depend on ethnic or
geographic differences (109). Murphy et al. reported datasuggesting that the infection can last for at least 4 years (R.Murphy, E. M. Behler, H. D. Appelman, J. L. Barnett, andG. H. Elta, Gastroenterology 94[Part 21:A317, 1988).Berkowicz and Lee (J. Berkowicz and A. Lee, Letter,Lancet ii:681, 1987) found serological evidence of a higherprevalence in institutionalized persons, suggesting person-
to-person transmission. However, studies examining anti-body to the organism in family members of patients with C.pylori infection (56; H. M. Mitchell, T D. Bohane, J.Berkowicz, S. L. Hazell, and A. Lee, Letter, Lancet ii:681-682, 1987) produced conflicting results. A study ofantibody in endoscopy room personnel (J. W. Rawles, M. L.Harris, G. Paull, J. Dick, J. H. Yardley, D. R. Kafonek,T. R. Hendrix, and W. J. Ravich, Gastroenterology 92[Part2]:1589, 1987) failed to show increased risk for acquiring theinfection.
POSSIBLE MECHANISMS OF PATHOGENESIS
The actual steps leading to the establishment of C. pyloriin the gastric environment and production of inflammationhave not been defined. The profuse production of urease
could create an alkaline microenvironment that protects theorganism from gastric acid (D. S. Tompkins and A. P. West,Letter, J. Clin. Pathol. 40:1387, 1987) until it becomesestablished under the layer of mucus. The bacteria appear toattach to the surface of the epithelial cells (13, 35, 49, 50, 65),possibly by a hemagglutinin on the surface of the bacteria(31, 125). Goodwin et al. (35) described attachment pedestalssimilar to those seen in infections with enteropathogenicEscherichia coli. Microvilli on the epithelial cells appear tobecome depleted (35), and the organism seems to congregateespecially at intercellular junctions (35, 49, 65) and causedisruption of the junctions (13, 50). A cytotoxin has beendescribed that causes nonlethal effects on various mamma-lian cells (67). This cytotoxin is produced only by approxi-mately half of C. pylori isolates, however, and thus seems ofquestionable significance. By whatever mechanism it isproduced, the mild tissue damage may elicit a leukocyteresponse, thus producing gastritis.Although the evidence for involvement in peptic ulcers is
only circumstantial, the following data provide an idea abouthow the organism might be involved. Wyatt et al. (134) foundthat 88% of patients with duodenitis had both C. pylon andgastric metaplasia (i.e., development of gastric-type epithe-lial cells) in the duodenum. Metaplasia was present only inpatients with a gastric pH of <2.5, and the bacteria wereconfined to the areas of the duodenum with the gastric-typetissue. Based on these findings, the investigators suggestedthe following sequence of events. Patients with high gastricacid output may develop gastric metaplasia in the duode-num, which could become colonized by C. pylori originatingfrom the antrum. Colonization by the organism would thenproduce inflammation, which could ultimately lead to devel-opment of an ulcer. This model preserves the traditionalconcept of acid involvement and, at the same time, recon-ciles data implicating C. pylori.
Hazell and Lee (48) have proposed another mechanism bywhich ulcers could be produced. They suggested that thegastric environment is altered by C. pylori due to rapid ureahydrolysis at intercellular junctions. This may prevent thenormal passage of H' ions and cause back diffusion, result-ing in hypochlorhydria and tissue damage.Slomiany and co-workers (118) found that the organism
has a proteolytic activity that degrades mucin. They hypoth-esized that this activity could weaken the protective mucusbarrier and allow acid to damage underlying epithelial cells.There is not yet sufficient support for any of these proposals,however, to know whether any, or all, of them are operativein patients.
LABORATORY DIAGNOSIS
The methods for laboratory diagnosis of C. pylori infectionare only now beginning to be defined. Up to this point, mostinvestigators have examined tissue by culture and histolog-ical stains, but other, more rapid techniques have recentlybeen investigated.The best type of specimen to be used for diagnosis has not
yet been established. One recent study (31) reported thatspecimens taken by brushing the gastric epithelium were asadequate as tissue specimens, but either of these were betterthan gastric fluid. The optimal procedure for transportingspecimens also has not been established. Goodwin et al. (38)found that specimens could be held in 0.5 ml of sterile 20%glucose at 40C for up to 5 h without loss of organismviability, and C.pylon has also been recovered from tissueheld in sterile 0.85% saline at4°C for 5 h (unpublished
VOL. 3, 1990
on January 6, 2020 by guesthttp://cm
r.asm.org/
Dow
nloaded from

CLIN. MICROBIOL. REV.
observation), but systematic studies of holding conditionshave not been conducted.The first tissue stain used was the hematoxylin and eosin
stain used early in the century (5, 20, 21, 62, 114), but theorganism is barely discernible with this procedure. Freed-berg and Barron (29) introduced the use of silver staining,which allows the organism to be seen in histological sectionsmuch more readily. The Warthin-Starry procedure was usedin the landmark work of Marshall and Warren (80) and inmost studies since then. The Dieterle method has also beenused successfully (10) and is easier to perform than theWarthin-Starry method, but is still relatively complicated.Other simpler stains have been suggested recently. Theseinclude the Giemsa (103), Gimenez (82), cresyl fast violet(R. A. Burnet, I. L. Brown, and J. Findlay, Letter, J. Clin.Pathol. 40:353, 1987), partial Gram (J. E. Trowell, A. K. H.Yoong, K. J. Saul, P. W. Gant, and G. D. Bell, Letter, J.Clin. Pathol. 40:702, 1987), and acridine orange (L. L.Walters, R. E. Budin, and G. Paull, Letter, Lancet i:42,1986) stains. In addition, phase-contrast microscopy hasbeen advocated (102). Madan et al. (70) compared Giemsa,hematoxylin and eosin, Warthin-Starry, and a tissue Gramstain and concluded that the Giemsa stain provided the bestcombination of simplicity and accuracy. Another recentreport (B. Aymard, B. Labouyrie, J. D. Korwin, R. Ferry,and A. Duprez, Gastroenterology 94[Part 2]:A16, 1988)compared Giemsa, hematoxylin and eosin, Warthin-Starry,and acridine orange stains and reached the same conclusion.There has been no systematic comparison of all of thevarious stain procedures, however.A number of different media have been used for recover-
ing C. pylori, including 5 to 10% horse blood agar (24, 38, 98,104), 5 to 10% sheep blood agar (61, 68, 123, 132), chocolateagar (10, 14, 60, 77, 80, 109), Skirrow medium (24, 104, 110),and Thayer-Martin medium (10, 34, 98). A number of inves-tigators found that using antibiotics in the medium to sup-press contaminating bacteria was advantageous (19, 24, 38,61, 98, 132). Queiroz et al. (105) proposed a new medium,called Belo Horizonte medium, composed of brain heartinfusion agar supplemented with 10% sheep blood, 2,3,5-triphenyltetrazolium chloride, and selective antibiotics. Onthis medium, C. pylori exhibits tiny, convex colonies withgolden yellow pigment, and other bacteria are either inhib-ited or do not exhibit this distinctive morphology. Dent andMcNulty (19) proposed another new medium, called Cam-pylobacter pylori selective medium, which contains 7%horse blood, cefsulodin, vancomycin, trimethoprim, andamphotericin B. The colonies are larger on this medium thanon chocolate agar.Only minimal work has been conducted to establish which
of these media is best for isolating the organism. Krajden etal. (61) compared the performances of Skirrow medium andsheep blood agar in two different laboratories. In one insti-tution, Skirrow medium performed better, but in the otherinstitution the performances of the two media were equal, sothere was no clear evidence of superiority. Parsonnet et al.(98) compared the performance of modified Thayer-Martinmedium with brucella agar containing 5% horse blood andconcluded that modified Thayer-Martin medium recoveredmore isolates. Dent and McNulty (19) recovered moreisolates with Campylobacter pylori selective medium thanwith Skirrow medium or chocolate agar. Grinding biopsyspecimens before inoculating culture media has been re-ported to increase the number of colonies recovered (38).Due to the microaerophilic nature of the organism, the
inoculated plates should be incubated in an environment
containing 5% oxygen, 10% carbon dioxide, and 85% nitro-gen. This can be generated in several ways, includingevacuation-replacement or the use of commercial gas gener-ation systems. The Bacti-Gas bag system (Scott Laborato-ries, Fiskeville, R.I.) requires special precautions to performproperly. The plates either must be double bagged or a moistpaper towel must be placed in the bag to preserve moisture(Scott Laboratories, personal communication).Once the atmosphere has been established, the cultures
should be incubated at 37TC. Because C. pylon growsrelatively slowly, cultures should be incubated for a total of7 days, although many isolates can be recovered aftershorter incubation periods. When colonies develop, theyshould be Gram stained and tested with the oxidase, cata-lase, and urease tests. The isolate can be identified as C.pylori if it is a curved, gram-negative bacillus with some cellsexhibiting "horseshoe" or oxbow shapes and is positive foroxidase, catalase, and urease. Further confirmation can beobtained, if desired, by using a system to detect preformedenzymes (84, 87).
Since cultures need prolonged incubation and many of thehistological methods are cumbersome and time-consuming,more rapid methods have recently been investigated. Anobvious approach is the examination of biopsy tissue bydirect Gram stain. Several studies have shown that theexamination of a single antral biopsy by this technique has 65to 85% sensitivity (89, 98; L. J. Barrett, B. J. Marshall, K.Dye, J. Sarazin, R. MCallum, and R. L. Guerrant, Abstr.Annu. Meet. Am. Soc. Microbiol. 1988, C101, p. 348). Iftissue from both the antrum and fundus is examined, thesensitivity appears to increase to 92 to 100% (89, 98).Parsonnet et al. (98) reported better results with the Gramstain when a rinse-imprint technique, rather than groundmaterial, was used to prepare the smears, but this has notbeen confirmed.The abundant production of urease provides an indirect
means of detecting the organism in a rapid manner. This typeof test was first described by McNulty and Wise (C. A. M.McNulty and R. Wise, Letter, Lancet i:1443-1444, 1985),using Christensen urea broth incubated for up to 24 h. Morerecent modifications include Stuart urease test broth (17) anda solution with a high concentration of urea and a pHindicator (46). One of the most widely used methods is a gelpellet containing urea and pH indicator (CLO-test; DeltaWest, Ltd., Canning Vale, Western Australia) (8, 81). Thesenewer tests have 90 to 100% sensitivity and 97 to 100%specificity, and approximately 75 to 85% of the tests arepositive within 1 h (8, 17, 46, 81). Studies evaluating them,however, have been conducted by immediately inoculatingthe urease test; the accuracy may be less when specimensare transported to the laboratory before testing (C. A. M.McNulty and R. Wise, Letter, Lancet i:387, 1986). Anotherpromising modification is a urease test in which the specimenis incubated in 1 ml of 10% urea containing 2 drops of 1%phenol red (A. S. Arvind, R. S. Cook, S. Tabaqchali, andM. J. G. Farthing, Letter, Lancet i:704, 1988). This test isincubated for 1 min and reportedly has a sensitivity of 91%and specificity of 100%.An extension of the urease test is the urea breath test. In
this test, the patient ingests labeled urea and after a period oftime the level of labeled CO2 is determined in a breathsample. Two forms of this test have been described: one inwhich the urea is labeled with "3C and is detected with amass spectrometer (42, 43), and one in which the urea islabeled with "4C and detected with a scintillation counter(79). The obvious advantage of this type of test is that it is
8 BUCK
on January 6, 2020 by guesthttp://cm
r.asm.org/
Dow
nloaded from

C. PYLORI AND GASTRODUODENAL DISEASE 9
both rapid and noninvasive. The disadvantage is that spe-cialized equipment is necessary.Serum antibody to the organism provides the basis for
another indirect means of detecting the presence of theorganism. As mentioned previously, several investigatorshave documented the presence of immunoglobulins G and Aantibody in individuals with C. pylori and, conversely, littleor no antibody in individuals with normal gastric mucosa (7,15, 37, 55, 57, 58, 92, 108, 131, 132). Although severaldifferent immunological techniques have been used, themajority of workers have utilized an enzyme-linked immuno-sorbent assay. Various antigen preparations have been used,including whole cells (15, 92, 108), sonicated cells (7, 55),glycine-acid extract (37, 130), and a high-molecular-weightcell-bound protein thought to be urease (26-28). None ofthese preparations has been standardized or is commerciallyavailable. Depending on the antigen preparation, the sensi-tivity of serological assays has been reported to be 81 to100% (15, 27, 37, 92). Hirschl et al. (51) concluded thatsonicated whole cells or sonicated whole cells subjected toultracentrifugation provide more accurate results than gly-cine-acid extracts. Additional work to standardize the anti-gen preparation and establish commercially available re-
agents is necessary before this approach will be routinelyavailable.
Additional possible rapid detection methods include im-munofluorescence staining of the bacteria in tissue, usingmonoclonal antibody (L. Engstrand, Letter, Lancet ii:1403,1986), and a DNA probe (A. W. Trofa, B. Jones, L.Rosenthal, D. Green, G. Chippendale, and H. Mobley,Abstr. Annu. Meet. Am. Soc. Microbiol. 1988, D60, p. 81).Which of these methods should be used routinely in the
laboratory? Histological staining was the first method usedto detect this organism and is still a useful and accuratemethod. The particular stain used is probably a matter ofpreference, although silver stains clearly require more timeand effort. Most investigators have found that culture per-forms about as well as histology in detecting C. pylori (19,24, 45, 47, 57, 63, 89, 98, 104), but culture is the mosttime-consuming and expensive method and is probably notnecessary unless a laboratory has research interest in thisorganism. As discussed above, a direct Gram stain can berelatively reliable, but only when specimens from severalsites are examined (89, 98). The newer modifications of rapidurea tests appear to be both sensitive and specific, whencompared with culture and histology (8, 46, 81, 115), andhave the advantage of providing results rapidly. While ureabreath tests are also rapid and accurate and have theadvantage of being noninvasive, the equipment necessary toperform these tests limits their usefulness. Serological testsalso appear to be highly accurate and are noninvasive, butare not yet standardized or commercially available. Basedon these considerations, the best approach to use at thepresent time would probably be a histological stain plus arapid urease test. As immunological methods become moredeveloped, they will probably find a prominent place indetecting C. pylori.For two reasons it can be argued that it is premature to
implement any procedures for detecting C. pylori on aroutine basis. First, the role of the organism is still beingdefined in the many conditions with which it is associated.Second, effective treatment regimens have yet to be fullyestablished. Therefore, at present, if a gastroenterologistserved by the laboratory has a particular interest in C. pylorior if there is a research interest, establishment of detection
procedures may be justified. If not, it may be best to waituntil more questions have been answered.
CONCLUSION
Rapid progress has been made in the 8 years since thediscovery of C. pylori, and a significant amount of informa-tion has come to light. The morphology and characteristicsof the organism have been extensively investigated, and ithas become established as a cause of gastritis. Evidence ismounting for a role in the development of duodenal ulcersand symptomatic gastritis in children. Additional work isnecessary to clarify its role in gastric ulcers and NUD. Morework is also needed to settle the question of its taxonomyand establish its mode of transmission and mechanism ofpathogenesis. With the current level of interest, however,answers to these questions should be available soon. Theseanswers may very well provide a revolutionary advance inthe diagnosis and treatment of gastric disease.
ACKNOWLEDGMENTS
Sincere appreciation is extended to Andrea Spalding for typingthe manuscript. Electron micrographs were provided by MichaelEisenback, Electron Microscopy Laboratory, Norton and KosairChildren's hospitals.
LITERATURE CITED1. Andersen, L. P., S. Holck, C. 0. Poulsen, L. Elsborg, and T.
Justensen. 1987. Campylobacter pyloridis in peptic ulcer dis-ease. I. Gastric and duodenal infection cause by C. pyloridishistopathologic and microbiologic findings. Scand. J. Gastro-enterol. 22:219-224.
2. Andreasen, J. J., and L. P. Andersen. 1987. In vitro suscepti-bility of Campylobacter pyloridis to cimetidine, sucralfate,bismuth and sixteen antibiotics. Acta Pathol. Microbiol. Im-munol. Scand. Sect. B 95:147-149.
3. Armstrong, J. A., S. H. Wee, C. S. Goodwin, and D. H. Wilson.1987. Response of Campylobacter pyloridis to antibiotics,bismuth and an acid-reducing agent in vitro-an ultrastructuralstudy. J. Med. Microbiol. 24:343-350.
4. Baskerville, A., and D. G. Newell. 1988. Naturally occurringchronic gastritis and C. pylori infection in the rhesus monkey:a potential model for gastritis in man. Gut 29:465-472.
5. Bizzozero, G. 1893. Ueber die schlauchfoermigen Drusen desMagendarmakanals und die Beziehungen ihres Epithels zu demOberfachenepithel der Schleimhaut. Arch. Mikrob. Anat. 42:82-152.
6. Blaser, M. J., D. N. Taylor, and R. A. Feldman. 1984. Epidemi-ology of Campylobacter infections, p. 142-161. In J. P. Butzler(ed.), Campylobacter infection in man and animals. CRCPress, Boca Raton, Fla.
7. Booth, L., G. Holdstock, H. MacBride, P. Hawtin, J. R. Gibson,A. Ireland, J. Bamforth, C. E. DuBoulay, R. S. Lloyd, and A. D.Pearson. 1986. Clinical importance of Campylobacter pyloridisand associated serum IgG and IgA endoscopy. J. Clin. Pathol.39:215-219.
8. Borromeo, M., J. R. Lambert, and K. J. Pinkard. 1987.Evaluation of "CLO-test" to detect Campylobacter pyloridisin gastric mucosa. J. Clin. Pathol. 40:462-468.
9. Bronsdon, M. A., and F. D. Schoenknecht. 1988. Campylobac-ter pylori isolated from the stomach of the monkey, Macacanemestrina. J. Clin. Microbiol. 26:1725-1728.
10. Buck, G. E., W. K. Gourley, W. K. Lee, K. Subramanyam,J. M. Latimer, and A. R. DiNuzzo. 1986. Relation of Campylo-bacter pyloridis to gastritis and peptic ulcer. J. Infect. Dis.153:664-669.
11. Buck, G. E., and J. S. Smith. 1987. Medium supplementationfor growth of Campylobacter pyloridis. J. Clin. Microbiol.25:597-599.
12. Celler, H. L., and W. Thalheimer. 1916. Bacteriological and
VOL. 3, 1990
on January 6, 2020 by guesthttp://cm
r.asm.org/
Dow
nloaded from

CLIN. MICROBIOL. REV.
experimental studies on gastric ulcer. J. Exp. Med. 23:791.13. Chen, X. G., P. Correa, J. Offerhaus, E. Rodriguez, F. Janney,
E. Hoffman, J. Fox, F. Hunter, and S. Diavolitsis. 1986.Ultrastructure of the gastric mucosa harboring campylobacter-like organisms. Am. J. Clin. Pathol. 86:575-582.
14. Coghlan, J. G., D. Gilligan, H. Humphries, D. McKenna, C.Dooley, E. Sweeney, C. Keane, and C. O'Morain. 1987. Cam-pylobacter pylori and recurrence of duodenal ulcers-a 12-month follow-up study. Lancet ii:1109-1111.
15. Cohen, H., M. Gramisu, P. Fitzgibbons, M. Appleman, M.Skoglund, and J. E. Valenzuela. 1989. Campylobacter pylon:associations with antral and fundic mucosal histology anddiagnosis by serology in patients with upper gastrointestinalsymptoms. Am. J. Gastroenterol. 84:367-71.
16. Czinn, S., H. Carr, and S. Aronoff. 1986. Susceptibility ofCampylobacter pylori to three macrolide antibiotics (erythro-mycin, roxithromycin [RU 2895], and CP 62,993) and rifampin.Antimicrob. Agents Chemother. 30:328-329.
17. Czinn, S. J., and H. Carr. 1987. Rapid diagnosis of Campylo-bacter pyloridis-associated gastritis. J. Pediatr. 110:569-570.
18. Czinn, S. J., B. B. Dahms, G. H. Jacobs, B. Kaplan, and F. C.Rothstein. 1986. Campylobacter-like organisms in associationwith symptomatic gastritis in children. J. Pediatr. 109:80-83.
19. Dent, J. C., and C. A. M. McNulty. 1988. Evaluation of a newselective medium for Campylobacter pylori. Eur. J. Clin.Microbiol. Infect. Dis. 7:555-558.
20. Doenges, J. L. 1938. Spirochetes in gastric glands of Macacusrhesus and humans without definite history of related disease.Proc. Soc. Exp. Biol. Med. 38:536-538.
21. Doenges, J. L. 1939. Spirochetes in the gastric glands ofMacacus rhesus and of man without related disease. Arch.Pathol. 27:469-477.
22. Dooley, C. P., and H. Cohen. 1988. The clinical significance ofCampylobacter pylori. Ann. Intern. Med. 108:70-79.
23. Drumm, B., A. O'Brien, E. Cutz, and P. Sherman. 1987.Campylobacter pyloridis-associated primary gastritis in chil-dren. Pediatrics 80:192-195.
24. Drumm, B., P. Sherman, E. Cutz, and M. Karmali. 1987.Association of Campylobacter pylori on the gastric mucosawith antral gastritis in children. N. Engl. J. Med. 316:1557-1561.
25. Eastham, E. J., T. S. J. Elliott, D. Berkley, and D. M. Jones.1987. Campylobacter pylori infection in children. J. Infect.16:77-79.
26. Evans, D. G., D. J. Evans, Jr., J. J. Moulds, and D. Y. Graham.1988. N-Acetylneuraminyllactose-binding fibrillar hemaggluti-nin of Campylobacter pylori: a putative colonization factorantigen. Infect. Immun. 56:2896-2906.
27. Evans, D. J., Jr., D. G. Evans, D. Y. Graham, and P. D. Klein.1989. A sensitive and specific serologic test for detection ofCampylobacter pylori infection. Gastroenterology 96:1004-1008.
28. Evans, D. J., Jr., D. G. Evans, K. E. Smith, and D. Y. Graham.1989. Serum antibody responses to the N-acetylneuraminyllac-tose-binding hemagglutinin of Campylobacter pylori. Infect.Immun. 57:664-667.
29. Freedberg, A. S., and L. E. Barron. 1940. The presence ofspirochetes in human gastric mucosa. Am. J. Dig. Dis. 7:443-445.
30. Fung, W. P., J. M. Papadimitriou, and L. R. Matz. 1979.Endoscopic, histological and ultrastructural correlations inchronic gastritis. Am. J. Gastroenterol. 71:269-279.
31. Gastrointestinal Physiology Working Group. 1986. Rapid iden-tification of pyloric Campylobacter in Peruvians with gastritis.Dig. Dis. Sci. 31:1089-1094.
32. Gear, M. W. L., S. C. Truelove, and R. Whitehead. 1971.Gastric ulcer and gastritis. Gut 12:639-645.
33. Gledhill, T., R. J. Leicester, B. Addis, N. Lightfoot, J. Barnard,N. Viney, D. Darkin, and R. H. Hunt. 1985. Epidemic hypo-chlorhydria. Br. Med. J. 290:1383-1386.
34. Glupczynski, Y., A. Burette, M. Labbe, C. Deprez, M.DeReuck, and M. Deltenre. 1988. Campylobacter pylori-asso-ciated gastritis: a double-blind placebo-controlled trial withamoxycillin. Am. J. Gastroenterol. 83:365-372.
35. Goodwin, C. S., J. A. Armstrong, and B. J. Marshall. 1986.Campylobacter pyloridis gastritis, and peptic ulceration. J.Clin. Pathol. 39:252-365.
36. Goodwin, C. S., P. Blake, and E. Blincow. 1986. The minimuminhibitory and bactericidal concentrations of antibiotics andanti-ulcer agents against Campylobacter pyloridis. J. Antimi-crob. Chemother. 17:309-314.
37. Goodwin, C. S., E. Blincow, G. Peterson, C. Sanderson, W.Cheng, B. Marshall, J. R. Warren, and R. McCulloch. 1987.Enzyme-linked immunosorbent assay for Campylobacter py-loridis: correlation with presence of C. pyloridis in the gastricmucosa. J. Infect. Dis. 155:488-484.
38. Goodwin, C. S., E. D. Blincow, J. R. Warren, T. E. Waters,C. R. Sanderson, and L. Easton. 1985. Evaluation of culturaltechniques for isolating Campylobacter pyloridis from endo-scopic biopsies of gastric mucosa. J. Clin. Pathol. 38:1127-1131.
39. Goodwin, C. S., R. K. McCulloch, J. A. Armstrong, and S. H.Wee. 1985. Unusual cellular fatty acids and distinctive ultra-structure in a new spiral bacterium (Campylobacter pyloridis)from the human gastric mucosa. J. Med. Microbiol. 19:257-267.
40. Graham, D. Y., L. C. Alpert, J. L. Smith, and H. H. Yoshi-mura. 1988. latrogenic Campylobacter pylori infection is acause of epidemic achlorhydria. Gastroenterology 83:974-980.
41. Graham, D. Y., and P. D. Klein. 1987. Campylobacterpyloridisgastritis: the past, the present, and speculations about thefuture. Am. J. Gastroenterol. 82:283-286.
42. Graham, D. Y., P. D. Klein, D. J. Evans, Jr., D. G. Evans,L. C. Alpert, A. R. Opekun, and T. W. Boutton. 1987.Campylobacter pylori detected noninvasively by the '3C-ureabreath test. Lancet i:1174-1177.
43. Graham, D. Y., P. D. Klein, A. R. Opekun, and T. W. Bouton.1988. Effect of age on the frequency of active Campylobacterpylori infection diagnosed by the ['3C]urea breath test innormal subjects and patients with peptic ulcer disease. J.Infect. Dis. 157:777-780.
44. Graham, D. Y., P. D. Klein, A. R. Opekun, K. E. Smith, R. R.Polasani, D. J. Evans, D. G. Evans, L. C. Alpert, P. A.Michaletz, H. H. Yoshimura, and E. Adam. 1989. In vivosusceptibility of Campylobacter pylori. Am. J. Gastroenterol.84:233-238.
45. Gustavsson, S., S. F. Phillips, J. R. Malagelada, and J. E.Rosenblatt. 1987. Assessment of Campylobacter-like organ-isms in the postoperative stomach, iatrogenic gastritis, andchronic gastroduodenal diseases: preliminary observations.Mayo Clin. Proc. 62:265-268.
46. Hazell, S. L., T. J. Borody, A. Gal, and A. Lee. 1987.Campylobacter pyloridis gastritis. I. Detection of urease as amarker of bacterial colonization and gastritis. Am. J. Gastro-enterol. 82:292-295.
47. Hazell, S. L., W. B. Hennessy, T. J. Borody, J. Carrick, M.Ralston, L. Brady, and A. Lee. 1987. Campylobacter pyloridisgastritis. II. Distribution of bacteria and associated inflamma-tion in the gastroduodenal environment. Am. J. Gastroenterol.82:297-301.
48. Hazell, S. L., and A. Lee. 1986. Campylobacter pyloridis,urease, hydrogen ion back diffusion, and gastric ulcers. Lancetii:15-17.
49. Hazell, S. L., A. Lee, L. Brady, and W. Hennessey. 1986.Campylobacter pyloridis and gastritis: association with inter-cellular spaces and adaptation to an environment of mucus asimportant factors in colonization of the gastric epithelium. J.Infect. Dis. 153:658-663.
50. Hill, I. D., C. Sinclair-Smith, A. J. Lastovica, M. D. Bowie, andM. Emms. 1987. Transient protein losing enteropathy associ-ated with acute gastritis and Campylobacter pylori. Arch. Dis.Child. 62:1215-1219.
51. Hirschl, A. M., M. Pleschette, M. H. Hirschl, J. Berger, G.Stanek, and M. L. Rotter. 1988. Comparison of differentantigen preparations in an evaluation of the immune responseto Campylobacter pylori. Eur. J. Clin. Microbiol. Infect. Dis.7:570-75.
52. Hui, W. M., S. K. Lam, P. Y. Chau, J. Ho, I. Lui, C. H. Lai,
10 BUCK
on January 6, 2020 by guesthttp://cm
r.asm.org/
Dow
nloaded from

C. PYLORI AND GASTRODUODENAL DISEASE 11
A. S. F. Lok, and M. M. T. Ng. 1987. Persistence of Campylo-bacter pyloridis despite healing of duodenal ulcer and improve-ment of accompanying duodenitis and gastritis. Dig. Dis. Sci.32:1255-1260.
53. Humphreys, H., S. Bourke, C. Dooley, D. McKenna, B. Power,C. T. Keane, E. C. Sweeney, and C. O'Morain. 1988. Effect oftreatment on Campylobacter pylori in peptic ulcer disease: arandomized prospective trial. Gut 29:279-283.
54. Jones, D. M., A. Curry, and A. J. Fox. 1985. An ultrastructuralstudy of the gastric campylobacter-like organism 'Campylo-bacter pyloridis.' J. Gen. Microbiol. 131:2335-2341.
55. Jones, D. M., J. Eldridge, A. J. Fox, P. Sethi, and P. J.Whorwell. 1986. Antibody to the gastric campylobacter-likeorganism ("Campylobacter pyloridis"')-clinical correlationsand distribution in the normal population. J. Med. Microbiol.22:57-62.
56. Jones, D. M., J. Eldridge, and P. J. Whorwell. 1987. Antibodiesto Campylobacter pyloridis in household contacts of infectedpatients. Br. Med. J. 294:615.
57. Jones, D. M., A. M. Lessels, and J. Eldridge. 1984. Campylo-bacter like organisms on the gastric mucosa: culture, histolog-ical, and serological studies. J. Clin. Pathol. 37:1002-1006.
58. Kaldor, J., W. Tee, C. Nicolacopolous, K. Demirtzoglou, D.Noonan, and B. Dwyer. 1986. Immunoblot confirmation ofimmune response to Campylobacter pyloridis in patients withduodenal ulcers. Med. J. Aust. 145:133-135.
59. Karttunen, T., S. Niemela, J. Lehtola, and J. Heikkila. 1987.Campylobacter-like organisms and gastritis: histopathology,bile reflux, and gastric fluid composition. Scand. J. Gastroen-terol. 22:478-486.
60. Kasper, G., and N. Dickgiesser. 1984. Isolation of Campylobac-ter-like bacteria from gastric epithelium. Infection 12:179-180.
61. Krajden, S., J. Bohnen, J. Anderson, J. Kempston, M. Fuksa,A. Matlow, N. Marcon, G. Haber, P. Kortan, M. Karmali, P.Corey, C. Petrea, C. Babida, and S. Hayman. 1987. Compari-son of selective and nonselective media for recovery of Cam-pylobacter pylori from antral biopsies. J. Clin. Microbiol.25:1117-1118.
62. Krienitz, W. 1906. Ueber das Auftreten von Spirochaetenverschiedener Form im Mageninhalt bei Carcinoma Ventriculi.Deutsch. Med. Wochenschr. 22:872.
63. Lamouliatte, H., F. Megraud, A. DeMascarel, D. Roux, and A.Quinton. 1987. "Campylobacterpyloridis" and epigastric pain:endoscopic, histological, and bacteriological correlations. Gas-troenterol. Clin. Biol. 11:212-216.
64. Lau, P. P., B. Debrunner-Vossbrinek, B. Dunn, K. Miotto,M. T. MacDonnell, D. M. Rollins, C. J. Pillidge, R. B. Hespell,R. R. Colwell, M. L. Sogin, and G. E. Fox. 1987. Phylogeneticdiversity and position of the genus Campylobacter. Syst. Appl.Microbiol. 9:231-238.
65. Lee, A., and S. L. Hazell. 1988. Campylobacter pylori in healthand disease: an ecological perspective. Microb. Ecol. HealthDis. 1:1-16.
66. Lee, F. I., I. M. Samloff, and M. Hardman. 1985. Comparisonof tri-potassium di-citrato bismuthate tablets with ranitidine inhealing and relapse of duodenal ulcers. Lancet i:1299-1302.
67. Leunk, R. D., P. T. Johnson, B. C. David, W. G. Kraft, andD. R. Morgan. 1988. Cytotoxic activity in broth-culture fil-trates of Campylobacter pylori. J. Med. Microbiol. 26:93-9.
68. Loffeld, R. J. L., H. V. P. J. Potters, J. W. Arends, E.Stobberingh, J. A. Flendrig, and J. P. Van Spreuwel. 1988.Campylobacter associated gastritis in patients with non-ulcerdyspepsia. J. Clin. Pathol. 41:85-88.
69. Luger, A., and H. Neuberger. 1921. Uber Spirochaetenbefundeim Magensaft und deven diagnostische Bedeutung fur dasCarcinoma Ventriculi. Z. Klin. Med. 92:54.
70. Madan, E., J. Kemp, T. U. Westblom, M. Subik, S. Sexton, andJ. Cook. 1988. Evaluation of staining methods for identifyingCampylobacter pylori. Am. J. Clin. Pathol. 90:450-453.
71. Marcheggiano, A., C. Jannoni, M. Agnello, P. Pauluzi, and F.Pallone. 1987. Campylobacter-like organisms on the humangastric mucosa. Relation to type and extent of gastritis indifferent clinical groups. Gastroenterol. Clin. Biol. 11:376-381.
72. Marshall, B. J. 1986. Campylobacter pyloridis and gastritis. J.
Infect. Dis. 153:650-657.73. Marshall, B. J., J. A. Armstrong, G. J. Francis, N. T. Nokes,
and S. H. Wee. 1987. Antibacterial action of bismuth in relationto Campylobacter pyloridis colonization and gastritis. Diges-tion 37(Suppl. 2):16-30.
74. Marshall, B. J., J. A. Armstrong, D. B. McGechie, and R. J.Glancy. 1985. Attempt to fulfill Koch's postulates for pyloriccampylobacter. Med. J. Aust. 142:436-439.
75. Marshall, B. J., and C. S. Goodwin. 1987. Revised nomencla-ture of Campylobacter pyloridis. Int. J. Syst. Bacteriol. 37:68.
76. Marshall, B. J., C. S. Goodwin, J. R. Warren, R. Murray, E. D.Blincow, S. J. Blackbourn, M. Phillips, T. E. Waters, and C. R.Sanderson. 1988. Prospective double-blind study of duodenalulcer relapse after eradication of Campylobacter pylori. Lancetii:1437-1442.
77. Marshall, B. J., D. B. McGechie, P. A. Rogers, and R. J.Glancy. 1985. Pyloric campylobacter infection and gastroduo-denal disease. Med. J. Aust. 142:439-444.
78. Marshall, B. J., H. Royce, D. I. Annear, C. S. Goodwin, J. W.Pearman, J. R. Warren, and J. A. Armstrong. 1984. Originalisolation of Campylobacter pyloridis from human gastric mu-cosa. Microbios Lett. 25:83-88.
79. Marshall, B. J., and I. Surveyor. 1988. Carbon-14 urea breathtest for the diagnosis of Campylobacter pylori associatedgastritis. J. Nucl. Med. 29:11-16.
80. Marshall, B. J., and J. R. Warren. 1984. Unidentified curvedbacilli in the stomach of patients with gastritis and pepticulceration. Lancet i:1311-1314.
81. Marshall, B. J., J. R. Warren, G. J. Francis, C. S. Goodwin,and E. Blincow. 1987. Rapid urease test in the management ofCampylobacter pyloridis-associated gastritis. Am. J. Gastro-enterol. 82:200-210.
82. McMullen, L., M. M. Walker, L. A. Bain, Q. N. Karim, andJ. H. Baron. 1987. Histological identification of Campylobacterusing Gimenez technique in gastric antral mucosa. J. Clin.Pathol. 40:464.
83. McNulty, C. A. M. 1986. Campylobacter pyloridis-associatedgastritis. J. Infect. 13:107-113.
84. McNulty, C. A. M., and J. Dent. 1987. Rapid identification ofCampylobacter pylori (C. pyloridis) by preformed enzymes. J.Clin. Microbiol. 25:1683-1686.
85. McNulty, C. A. M., J. C. Gearty, B. Crump, M. Davis, I. A.Donovan, V. Melikian, D. M. Lister, and R. Wise. 1986.Campylobacter pyloridis and associated gastritis: investigatorblind, placebo controlled trial of bismuth salicylate and eryth-romycin ethylsuccinate. Br. Med. J. 293:645-649.
86. McNulty, C. A. M., and R. Wise. 1985. Susceptibility of clinicalisolates of Campylobacter pyloridis to 11 antimicrobial agents.Antimicrob. Agents Chemother. 28:837-838.
87. Megraud, F., F. Bonnet, M. Garnier, and H. Lamouliatte. 1985.Characterization of Campylobacter pyloridis by culture, enzy-matic profile, and protein content. J. Clin. Microbiol. 22:1007-1010.
88. Mobley, L. T., M. J. Cortesia, L. E. Rosenthal, and B. D. Jones.1988. Characterization of urease from Campylobacter pylori. J.Clin. Microbiol. 26:831-836.
89. Montgomery, E. A., D. F. Martin, and D. A. Peura. 1988. Rapiddiagnosis of Campylobacter pylori by Gram's stain. Am. J.Clin. Pathol. 90:606-609.
90. Morgan, D. R., R. Freedman, C. E. Depew, and W. G. Kraft.1987. Growth of Campylobacter pylori in liquid media. J. Clin.Microbiol. 25:2123-2125.
91. Morris, A., and G. Nicholson. 1987. Ingestion of Campylobac-ter pyloridis causes gastritis and raised fasting gastric pH. Am.J. Gastroenterol. 82:192-199.
92. Morris, A., G. Nicholson, G. Lloyd, D. Haines, A. Rogers, andD. Taylor. 1986. Seroepidemiology of Campylobacter pylori-dis. N. Z. Med. J. 99:657-659.
93. Newell, D. G. 1987. Identification of the outer membraneproteins of Campylobacter pyloridis and antigenic cross-reac-tivity between C. pyloridis and C. jejuni. J. Gen. Microbiol.133:163-170.
94. Niemela, S., T. Kartunen, and J. Lehtola. 1987. Campylobac-ter-like organisms in patients with gastric ulcer. Scand. J.
VOL. 3, 1990
on January 6, 2020 by guesthttp://cm
r.asm.org/
Dow
nloaded from

CLIN. MICROBIOL. REV.
Gastroenterol. 22:487-490.95. O'Connor, H. J., M. F. Dixon, J. I. Wyatt, A. T. R. Axon, D. C.
Ward, E. P. Dewar, and D. Johnston. 1986. Effect of duodenalulcer surgery and enterogastric reflux on Campylobacter py-loridis. Lancet ii:1178-1181.
96. O'Connor, H. J., J. I. Wyatt, M. F. Dixon, and A. T. R. Axon.1986. Campylobacter like organisms and reflux gastritis. J.Clin. Pathol. 39:531-534.
97. Palmer, E. D. 1954. Investigation of the gastric mucosa spiro-chetes of the human. Gastroenterology 27:218-220.
98. Parsonnet, J., K. Welch, C. Compton, R. Strauss, T. Wang, P.Kelsey, and M. J. Ferraro. 1988. Simple microbiologic detec-tion of Campylobacter pylori. J. Clin. Microbiol. 26:948-949.
99. Paster, B. J., and F. E. Dewhirst. 1988. Phylogeny of campylo-bacters, wolinellas, Bacteroides gracilis, and Bacteroides ureo-lyticus by 16S ribosomal ribonucleic acid sequencing. Int. J.Syst. Bacteriol. 38:56-62.
100. Pearson, A. D., M. B. Skirrow, H. Lior, and B. Rose (ed.). 1985.Campylobacter III: Proceedings of the Third InternationalWorkshop on Campylobacter Infections. Public Health Labo-ratory Service, London.
101. Perez-Perez, G. I., and M. J. Blaser. 1987. Conservation anddiversity of Campylobacter pyloridis major antigens. Infect.Immun. 5:1256-1263.
102. Pinkard, K. J., B. Harrison, J. A. Capstick, G. Medley, andJ. R. Lambert. 1986. Detection of Campylobacter pyloridis ingastric mucosa by phase contrast microscopy. J. Clin. Pathol.39:112-113.
103. Potters, H. V. P. J., R. J. L. F. Loffeld, E. Stobberingh, J. P.van Spreeuwel, and J. W. Arends. 1987. Rapid staining ofCampylobacter pyloridis. Histopathology 11:1223.
104. Price, A. B., J. Levi, J. M. Dolby, P. L. Dunscombe, A. Smith,J. Clark, and M. L. Stephenson. 1985. Campylobacterpyloridisin peptic ulcer disease: microbiology, pathology, and scanningelectron microscopy. Gut 26:1183-1188.
105. Queiroz, D., E. Mendez, and G. A. Rocha. 1987. Indicatormedium for isolation of Campylobacter pylori. J. Clin. Micro-biol. 25:2378-2379.
106. Ramsey, E. J., K. V. Carey, W. L. Peterson, J. J. Jackson,F. K. Murphy, N. W. Read, K. B. Taylor, J. S. Trier, and J. S.Fordtran. 1979. Epidemic gastritis with hypochlorhydria. Gas-troenterology 76:1449-1457.
107. Raskov, H., C. Lanng, K. Gaarslev, B. Fischer, and 0. Hauch.1987. Screening for Campylobacter pyloridis in patients withupper dyspepsia and the relation to inflammation of the humangastric antrum. Scand. J. Gastroenterol. 22:568-572.
108. Rathbone, B. J., J. I. Wyatt, B. W. Worsley, S. E. Shires, L. K.Trejdosiewicz, R. V. Heatley, and M. S. Losowsky. 1986.Systemic and local antibody responses to gastric Campylobac-ter pyloridis in non-ulcer dyspepsia. Gut 27:642-647.
109. Rauws, E. A. J., W. Langenberg, H. J. Houthoff, H. C. Zanen,and G. N. J. Tytgat. 1988. Campylobacter pyloridis-associatedchronic active antral gastritis. Gastroenterology 94:33-40.
110. Rokkas, T., C. Pursey, E. Uzoechina, L. Dorrington, N. A.Simmons, M. I. Filipe, and G. E. Sladen. 1987. Campylobacterpylori and non-ulcer dyspepsia. Am. J. Gastroenterol. 82:1149-1152.
111. Rollason, T. P., J. Stone, and J. M. Rhodes. 1984. Spiralorganisms in endoscopic biopsies of the human stomach. J.Clin. Pathol. 37:23-26.
112. Romaniuk, P. J., B. Zoltowska, T. J. Trust, D. J. Lane, G. J.Olsen, N. R. Pace, and D. A. Stahl. 1987. Campylobacterpylori, the spiral bacterium associated with human gastritis, isnot a true Campylobacter sp. J. Bacteriol. 169:2137-2141.
113. Rouvroy, D., J. Bogaerts, 0. Nsengiumwa, M. Omar, L.Versailles, and J. Haot. 1987. Campylobacter pylori, gastritis,and peptic ulcer disease in central Africa. Br. Med. J. 295:1174.
114. Salomon, H. 1896. Ueber das Spirillum des Saugetiermagensund sein Verhalten zu den Belegzellen. Zentralbl. Bakteriol.Mikrobiol. Hyg. 19:433-442.
115. Schnell, G. A., and T. T. Schubert. 1989. Usefulness of culture,
histology, and urease testing in the detection of Campylobacterpylori. Am. J. Gastroenterol. 84:133-137.
116. Schrager, J., R. Spink, and S. Mitra. 1967. The antrum inpatients with duodenal and gastric ulcers. Gut 8:497-508.
117. Shungu, D. L., D. R. Nalin, R. H. Gilman, H. H. Gadebusch,A. L. Cerami, C. Gill, and B. Weissberger. 1987. Comparativesusceptibilities of Campylobacter pylon to norfloxacin andother agents. Antimicrob. Agents Chemother. 31:949-950.
118. Slomiany, B. L., J. Bilski, J. Sarosiek, V. L. N. Murty, B.Dworkin, K. VanHorn, J. Zielenski, and A. Slomiany. 1987.Campylobacter pyloridis degrades mucin and undermines gas-tric mucosal integrity. Biochem. Biophys. Res. Commun.14:307-314.
119. Steer, H. W., and D. G. Colin-Jones. 1975. Mucosal changes ingastric ulceration and their response to carbenoxolone sodium.Gut 16:590-597.
120. Strickland, R. G., and I. R. Mackay. 1973. A reappraisal of thenature and significance of chronic atrophic gastritis. Am. J.Dig. Dis. 18:426-437.
121. Talley, N. J., D. McNeil, A. Hayden, and D. W. Piper. 1986.Randomized, double-blind, placebo-controlled crossover trialof cimetidine and pirenzepine in non-ulcer dyspepsia. Gastro-enterology 91:149-156.
122. Talley, N. J., and D. W. Piper. 1985. The association betweennon-ulcer dyspepsia and other gastrointestinal disorders.Scand. J. Gastroenterol. 20:896-900.
123. Taylor, D. E., J. A. Hargreaves, L.-K. Ng, R. W. Sherbaniuk,and L. D. Jewell. 1987. Isolation and characterization ofCampylobacter pyloridis from gastric biopsies. Am. J. Clin.Pathol. 87:49-54.
124. Taylor, K. B. 1976. Immune aspects of pernicious anemia andatrophic gastritis. Clin. Haematol. 5:497-519.
125. Thompson, L. M., III, R. M. Smibert, J. L. Johnson, and N. R.Krieg. 1988. Phylogenetic study of the genus Campylobacter.Int. J. Syst. Bacteriol. 38:190-200.
126. Thompson, W. G. 1984. Nonulcer dyspepsia. Can. Med. J.Assoc. 130:565-569.
127. Toukan, A. U., M. F. Kamal, S. S. Amr, M. A. Arnaout, andA. S. Abu-Romiyeh. 1985. Gastroduodenal inflammation inpatients with nonulcer dyspepsia: a controlled endoscopic andmorphometric study. Dig. Dis. Sci. 30:313-320.
128. Van Caekenberghe, D. L., and J. Breyssens. 1987. In vitrosynergistic activity between bismuth subcitrate and variousantimicrobial agents against Campylobacter pyloridis (C. py-lori). Antimicrob. Agents Chemother. 31:1429-1430.
129. Vantrappen, G., P. Rutgeerts, L. Broeckaert, and J. Janssens.1980. Randomized open controlled trial of colloidal bismuthsubcitrate tablets and cimetidine in the treatment of duodenalulcer. Gut 21:329-333.
130. Von Wulffen, H., and H. J. Grote. 1988. Enzyme-linkedimmunosorbent assay for detection of immunoglobulin A andG antibodies to Campylobacter pylori. Eur. J. Clin. Microbiol.Infect. Dis. 7:559-565.
131. Von Wulffen, H., H. J. Grote, S. Gatermann, T. Loning, B.Berger, and C. Buhl. 1988. Immunoblot analysis of immuneresponse to Campylobacter pylori and its clinical associations.J. Clin. Pathol. 41:653-659.
132. Von Wulffen, H., J. Heesemann, G. H. Butzow, T. Loning, andR. Laufs. 1986. Detection of Campylobacter pyloridis in pa-tients with antrum gastritis and peptic ulcers by culture,complement fixation test, and immunoblot. J. Clin. Microbiol.24:716-720.
133. Whitehead, R., S. C. Truelove, and M. W. L. Gear. 1972. Thehistological diagnosis of chronic gastritis in fibreoptic gastro-scope biopsy specimens. J. Clin. Pathol. 25:1-11.
134. Wyatt, J. I., B. J. Rathbone, M. F. Dixon, and R. V. Heatley.1987. Campylobacter pyloridis and acid induced gastric meta-plasia in the pathogenesis of duodenitis. J. Clin. Pathol.40:841-848.
135. Wyatt, J. I., B. J. Rathbone, and R. V. Heatley. 1986. Localimmune response to gastric Campylobacter in non-ulcer dys-pepsia. J. Clin. Pathol. 39:863-870.
12 BUCK
on January 6, 2020 by guesthttp://cm
r.asm.org/
Dow
nloaded from











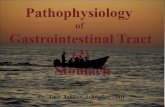
![Gastritis [Compatibility Mode]](https://static.fdocuments.in/doc/165x107/577d39881a28ab3a6b99f9d2/gastritis-compatibility-mode.jpg)




