
CalmingAnxiousBrain Oct 2013
87
© 2013 WJ Sieber Buddha “To tame this mind of ours” “We are what we think. All that we are arises with our thoughts.” “With our thoughts we make the world.” “Speak or act with an impure mind and trouble will follow you. Speak or act with a pure mind and happiness will follow you.”
description
act
Transcript of CalmingAnxiousBrain Oct 2013

© 2013 WJ Sieber
Buddha
“To tame this mind of ours”
“We are what we think. All that we are arises with our thoughts.”
“With our thoughts we make the world.”
“Speak or act with an impure mind and trouble will follow you. Speak or act with a pure mind and happiness will follow you.”
© 2013 WJ Sieber
Calming an Overactive Brain
William J. Sieber, Ph.D.
Inner Solutions for Success
Clinical ProfessorDepartment of Family & Preventive Medicine
Department of PsychiatryUC San Diego
© 2013 WJ Sieber
What to expect
Learn how stress and anxiety-related disorders affect your brain
Understand how stress affects your sleep, your eating habits, and your overall energy levels
Evidence-based strategies to manage anxiety-related disorders
Meditation, contemplative practices and their impact on our health

© 2013 WJ Sieber
Alphabet soupHPA = hypothylamic pituitary adrenal
PNI = psychoneuroimmunology
CPAP = continuous positive airway pressure
CRF = corticotropin releasing factor
BNST= Bed Nucleus of the Stria Terminalis
OR = Odds Ratio
ACT = Acceptance and Commitment Therapy
MBSR = Mindfulness Based Stress Reduction
rCBF = regional cerebral blood flow

© 2013 WJ Sieber
Stress in America 22% of Americans report stress at 8 or higher on 10-point scale
32% of adults say it is very important to talk with their health care provider about stress; less than 18% do
92 % believe stress negatively impacts health; only 31% believe stress negatively affects their health
Nearly half state they’re poor at preventing or managing stress
Top symptoms of stress: irritability (42%), anxious (39%), and fatigue (37%), feeling sad (37%), and low energy (35%)

© 2013 WJ Sieber
32% of adults report not getting enough sleep
Importance to well-being? Good family/friend relationships (76%), managing stress (61%), getting enough sleep (60%), eating well & exercising (54%)
Westerners report using meditation & yoga more to manage stress, while Easterners drink more alcohol.
Midwesterners are more likely to turn to family/friends than other regions. Midwesterners are also more likely to state “willpower” and lack of confidence as factors that prevent healthy behaviors.
Stress in America (StressinAmerica.org)

© 2013 WJ Sieber
How do you feel?
Dread
Fretful
Nervous
Panicked
Restless
Anxious
Apprehensive
Worried
Tense
Angst
Concerned
Uneasy
Fidgety

© 2013 WJ Sieber
What models do we use? Symptoms as pathology – DSM-IV criteria for ‘over-active brain’ disorders (GAD, OCD, PTSD, Social Phobia)
Dualism or integration?Psychological or physicalHolistic, multi-factorial model of inter-connectivity (e.g., allostatic load, childhood trauma, neuroplasticity)
Direct mind-body connection (HPA axis)
Behavioral response to stress/anxiety that perpetuates over-activity of the brain (caffeine/ nutrition, social isolation & rumination, physical inactivity)
© 2013 WJ Sieber
Self-assessment, self awareness, and emotional intelligence
Avoidance (cognitive, affective, and behavioral) leads to lowered tolerance
Many effective techniques are based on reflection and awareness
Self-care, and balancing action with acceptance are critical

© 2013 WJ Sieber
The mind-body connectionMaladaptive thought patterns & controlling the frontal lobe (social/emotional intelligence) → lowers anxiety
rCBF studies show ↓amygdala response when affect was labeled (intellectualized) vs. when affect stayed ‘perceptual’ – self-awareness/self-assessment IS executive functioning (i.e., building descending inhibitory circuitry)
Hypothalamus → CRF → pituitary → beta-endorphins & adrenocorticotropin hormone (ACTH) → adrenal → cortisol, gluccocorticoids, and pro-inflammatory cytokines → down regulate system elements upstream

+
+
Adrenal Glandsadrenaline
glucocorticoids
Hypothalamic Pituitary Adrenal (HPA)
Anterior Pituitary
Hypothalamus

© 2013 WJ Sieber
Corticotropin-releasing factor (CRF) in the Hypothalamus, Medulla, and Amygdala
1. Hypothalamus a. Activation of endocrine (hormonal) stress
response stimulates release of ACTH from pituitary b. ACTH in turn stimulates release of
glucocorticoids from adrenal gland c. Glucocorticoids increase blood sugar,
suppress immune function, and break down fats
Neurobiology of Stress Response
© 2013 WJ Sieber
Neurobiology of Stress ResponseCorticotropin-releasing factor (CRF) in the Hypothalamus, Medulla, and Amygdala
2. Medulla a. Activation of sympathetic nervous system-
release of norepinephrine (noradrenaline) b. Stimulates nerves leading to adrenal
medulla- release of epinephrine (adrenaline) c. Norepinephrine and epinephrine increase
heart rate, increase blood pressure, and produce bronchial dilation
© 2013 WJ Sieber
Neurobiology of Stress Response
Corticotropin-releasing factor (CRF) in the Hypothalamus, Medulla, and Amygdala
3. Amygdala a. Coordination of behavioral responses to
stress b. Associated with fear and survival/threat
response
© 2013 WJ Sieber
The amygdalaDecision-making in unpredictable and ambiguous situations.
Neuroimaging shows induced negative emotion leads to greater amygdala activation than positive emotions.
Patients with bilateral amygdala damage judge unfamiliar individuals to be more approachable and trustworthy suggesting their ‘fear-trigger’ is muted, as the amygdala is important in the recognition of cues of threats or danger.
Amygdala is crucial for learning new stimulus-threat contingencies and in the expression of cue-specific fear. The amygdala and BNST are where memories are ‘burned’ into memory, because fear-associated events need to be remembered for our survival.
© 2013 WJ Sieber
The amygdalaThe amygdala is not necessary for the expression of already acquired individual differences in temperament or affective style. Generally the initial reactivity of amygdala is unrelated to trait anxiety, though recovery time is.
The Bed Nucleus Stria Terminalis (BNST), the ‘extended anygdala’, is more implicated in chronic anxiety per se.
PET / fMRI studies show amygdala activation when anxiety-disordered patients are exposed to their specific anxiety-provoking stimuli compared to control stimuli. However there is rapid habituation of the amygdala response, suggesting the time-limited function of the amygdala in the stream of affective information processing.

© 2013 WJ Sieber
The mind-body connectionThe prefrontal cortex is related to affective chronometry
Right-sided prefrontal and orbitofrontal cortex activation: withdrawal-related negative emotions.
Left-sided prefrontal cortex activation: experience of positive affect (damage results in depressed mood /anhedonia).
PET scan studies show that negative affect activates anterior orbital, inferior frontal, middle and superior frontal gyri; positive affect is associated with left-sided metabolic changes. For example, when social phobics anticipate making a public speech, they show a large increase in right-sided anterior activation, including right-sided prefrontal cortex.

© 2013 WJ Sieber
The mind-body connection
Asymmetric activation of these brains regions are associated with specific ‘reactive’ emotions when a person is confronted with an environmental challenge, not in differences in mood without such stressors (i.e., temperament, personality).

© 2013 WJ Sieber
Overactive Brain: Fatigue and sleep
Prolonged HPA activation, often the result of hyper-vigilance secondary to a traumatic event, impairs sleep and reduces sleep quality.
Chronic stress can result in hormonal imbalances and impact thyroid function. A low thyroid level can cause fatigue, weakness, lethargy, weight gain, and depression; high thyroid levels can cause fatigue, and/or anxiety.
Poor sleep quality & fatigue leads to over-reactive amygdala.

© 2013 WJ Sieber
Chronic fatigue syndromeDefinition / criteria (CDC); Women account for 65-80% of CFS.
A. Chronic fatigue for >6 months that doesn’t resolve with bedrest & impairs function by 50% or more
B. Exhaustion after completion of simple tasks.
C. 7 or more of the following: (main symptom having abrupt onset)1. Mild fever and chills
2. Sore throat
3. Painful lymph nodes
4. Generalized muscle weakness
5. Myalgias
6. Post-exertional fatigue/malaise
7. Headaches
8. Joint aches
9. Neuropsych complaints
10. Sleep disturbances
11. Non-productive congestion
© 2013 WJ Sieber
CFS – Stress syndromeMetabolism of CFS patients is normal so symptoms are due to psychological factors, with mental fatigue considered a lack of motivation (brain is major consumer of resting cellular energy!)
Parental physical abuse, childhood GI symptoms, and parental reports of many colds each had ORs > 1.6 for patients with CFS.
Outcomes are predicted by ê in ‘perceived problems with activity’ and an é in sense of control over fatigue. Patients with CFS tend to perceive problems with activity independent of their own objective performance and see CFS as uncontrollable, itself resulting in chronic anxiety and fatigue.
When gluccocorticoids are released as part of short term stress they destroy weaker/older lymphocytes; prolonged stress leads to indiscriminate destruction of lymphocytes. Prolonged stress elevations and compromised compensatory recovery systems can result in autoimmunity.
© 2013 WJ Sieber
CFS – Immune dysfunctionFindings have consistently shown adrenal insufficiency/low cortisol especially during typical morning surge. CFS also have been shown to have low heart rate variability.
Pro-inflammatory cytokines act on the brain to cause sickness behavior. When inflammation continues unabated, such as during systemic infections, cancer or autoimmune disorders, the ensuing immune signaling to the brain can lead to exacerbation of depression. This may be why depressive symptoms such as fatigue, reduced interest, and low mood is more prevalent with immune dysfunction.

© 2013 WJ Sieber
CFS – Immune dysfunctionAs compared to non-CFS patients, CFS patients with post-infective (mononucleosis) fatigue had gene expression profiles of “altered host response”, with most of these genes affecting mitochondrial functions. It remains unclear whether this fatigue reflects chronic effects of persistent Epstein Barr Virus (EBV) or if the EBV triggers a chronically altered host response to various viruses.
When the digestive system is operating properly glucose and lipids are fed into the blood stream, and with erythrocytes (red blood cells) are transported to every cell in blood. GI disturbance can thus lead to insufficient energy production and fatigue.

© 2013 WJ Sieber
Chronic fatigue syndrome“While immune dysfunction is associated with CFS we do not know if this plays an etiological role or is simply confounded with low cortisol levels or sleep dysfunction, both of which are common in CFS and both of which are associated with immune activation. Cross sectional studies that compare CFS to other medical conditions have shown that the proportion of these patients with co-morbid psychological disorders is too high to simply be a reaction to having the illness but is compatible with the idea that this co-morbidity might reflect a shared underlying CNS dysfunction.” – Simon Wessely, CFS expert

© 2013 WJ Sieber
Chronic fatigue syndrome“CFS has multiple causes and to call it a single disease greatly underestimates the complexity of the problem. Thus to look for “the cause” of CFS is a self-defeating exercise. There is accumulating evidence for a wide variety of abnormalities in CFS, including altered adaptive immunity, disordered pain perception, endocrine abnormalities, sleep disorders, and cardiovascular dysfunction. However, one is left with a strong sense that post-viral events are a common trigger in CFS, but how they lead to chronic disease remains unresolved.” – Stephen Hilgate, CFS expert

© 2013 WJ Sieber
Chronic fatigue syndrome
“Even when they sleep, their stress-responsive neural systems are on high alert, signaling that it is not safe to relax. I think this condition may be understood by analogy to PTSD, just that in CFS the original trauma is most likely a physiological, internal one, such as a severe infection.” – Ute Vollmer-Conna, CFS expert
© 2013 WJ Sieber
Self-assessment - sleep
Sleep diary è Sleep efficiency
Sleep restriction, sleep hygiene, and stimulus control
What will be different next week?
© 2013 WJ Sieber
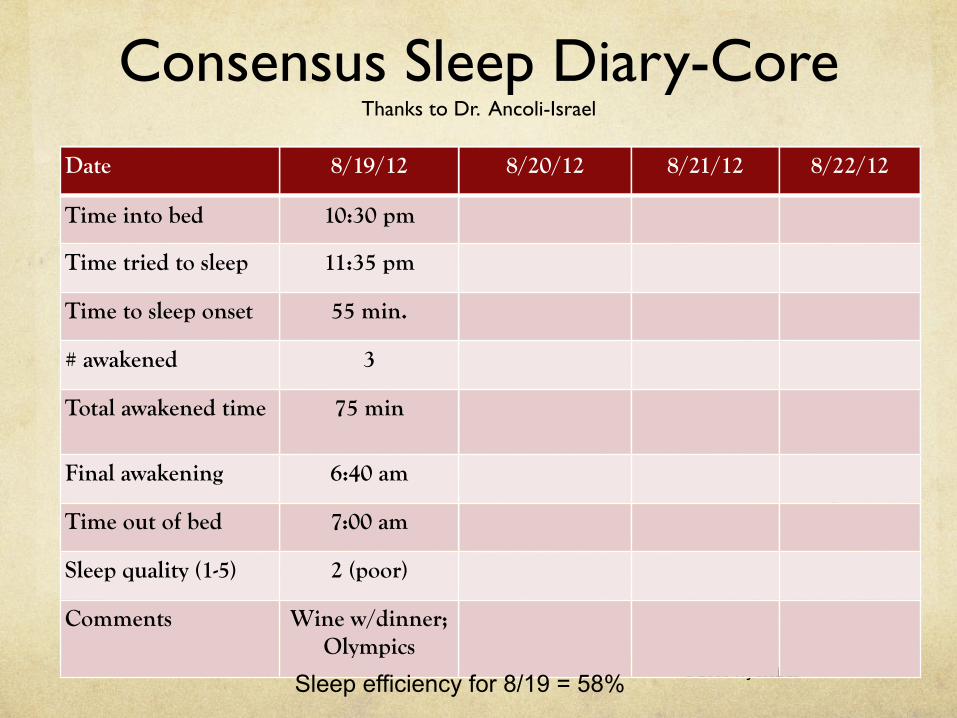
Consensus Sleep Diary-CoreThanks to Dr. Ancoli-Israel
Date 8/19/12 8/20/12 8/21/12 8/22/12
Time into bed 10:30 pm
Time tried to sleep 11:35 pm
Time to sleep onset 55 min.
# awakened 3
Total awakened time 75 min
Final awakening 6:40 am
Time out of bed 7:00 am
Sleep quality (1-5) 2 (poor)
Comments Wine w/dinner; Olympics
Sleep efficiency for 8/19 = 58%
© 2013 WJ Sieber
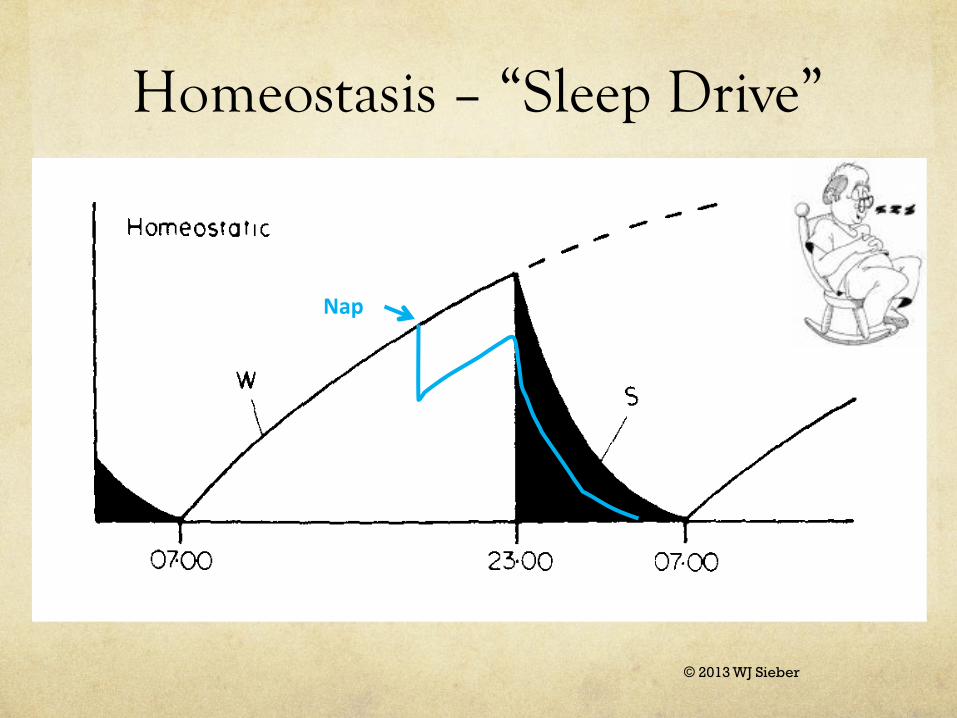
Homeostasis – “Sleep Drive”
Nap
© 2013 WJ Sieber
Effects of sleep deprivationTwo studies using fMRI showed sleep restriction
ñamygdala activation (and subjective emotional intensity) and lessens connectivity between amygdala and medial-prefrontal cortex (controller of amygdala) when exposed to 150 ‘affective’ pictures. (van der Helm E, Yao J, et
al, (2011) Current Biology; Yoo SS, Gujar N, Hu P, Jolesz FA, Walker MP (2011) Current Biology)
Cross sectional survey in Japan showed < 6 hours sleep had OR 1.42 for diabetes than those with 8+ hours average (Kobayashi, Takahashi et al, 2010, Internal Medicine)
Improved sleep for 3 months (via CPAP crossover design) in patients with metabolic syndrome results in lower blood pressure, cholesterol, and A1c (Sharma, Agrawal et
al 2011, NEJM)

© 2013 WJ Sieber
Sleep problemsConsequences of impaired sleep
Daytime sleepiness, depression, cognitive impairment, anxiety, emotional reactivity
Inflammation: Cardiovascular & immunologic effects
Cohen, 2009, < 6 hrs/night more susceptible to flu
Heffner, 2012 & Haack and Mullington, 2007, sleep deprived
ñinterleukin-6/pain sensitivity
Extending sleep ñpain tolerance by 25%, more than 60 mg of codeine (Sleep, 2012)
< 6 hours/night = higher breast cancer recurrence, post-menopausal only
Prostate cancer (OR 1.6 – 2.0) for sleep problems in > 65 age (Cancer Epi, 2013)
Mortality (OR 1.97)
© 2013 WJ Sieber
Sleep restriction
NIH Consensus Panel concluded sleep restriction, sleep hygiene and stimulus control are most effective treatment for Onset insomnia; terminal insomnia (SSRIs)
Physical activity (vigorous, no closer than 3 hours)
Set wake time
No naps
Bed when sleepy; 30 minute maximum per attempt
© 2013 WJ Sieber
Sleep hygiene and stimulus controlAll activity outside bedroom
darkness/no electronics 60 minutes prior to bedtime
cool temperature to mimic lowered body temp at night
no clock visible
list of concerns outside bedroom (60 min pre, night-stand)
pets in their place (53% of pet owners report disrupted sleep every night)
Caffeine, alcohol, tryptophan
What will be different next week?

© 2013 WJ Sieber
Cathy H.56 y.o. female, entertainment publisher, unknown work hours
Adult son & family ‘in transition’
GAD-7 = 16, sleep diary, cognitive log (re: work)
Intervention: bed only for sleep, no alcohol past 7 pm, sleep restriction, worry pad, 60 minute pre-bed routine, mid-day walk, daily planner, assertiveness training, plan for dedicated work space at home, unifying principles to guide work decisions, biofeedback (MyCalmBeat.com)

© 2013 WJ Sieber
“Gut Brain” - Ghrelin
Adiposity hormones, leptin and ghrelin, regulate short-term food intake to achieve long-term energy balance.
Leptin signals satiety, down regulates food intake
Ghrelin increase appetite and peaks during first bites
Decreased sleep ↑ ghrelin levels and ê leptin levels
Ghrelin : circulating levels surge shortly before meals, and secondary to stress.
Ghrelin is most quickly suppressed by ingestion of carbohydrates. Proteins and then fats suppress ghrelin to a lesser degree. Crude fiber also lowers ghrelin production.

© 2013 WJ Sieber
The “Gut Brain” - caffeineo Most often used psychoactive substance on earth; improves
attention and concentration yet impairs short-term memory when eliminated
o Caffeine intensifies dopamine receptors, resulting in stimulation of the cardiovascular system. May lower risk of Alzheimer disease.
o Chronic use increases risk of dehydration, and poor sleep quality, leading to fatigue and susceptibility to anxiety.
o Long-term caffeine consumption has been linked to fibrocystic breast disease &cardiovascular disease (DBP 3 pts.).
o Now often combined with sweeteners which increases dopamine (addictive substance?).
© 2013 WJ Sieber
Acquired dopamine deficiency
• Repeated exposure to drugs of abuse or fatty foods leads to down-regulation of dopamine receptors
• Dopamine-deficient animals show compulsive drug or food seeking (i.e. will seek out junk food or drugs despite punishment)
• Mindful eating ?

© 2013 WJ Sieber
Managing cravings with increased dopamine?
When dopamine is low in the limbic system then immediate rewards (simple decision) wins out. When sufficient dopamine is present, then prefrontal cortex (complexity, delayed gratification) will win out.
Memory, based in hippocampus, tends to lower firing of dopamine neurons with expectation of a familiar non-gratifying activity, more firing of dopamine neurons with a familiar pleasurable activity, whereas greater firing of dopamine neurons occur when ‘opportunity’ for pleasure is novel (encouraging exploration).
Gratitude journal, self-care, massage, dance, play, novelty
© 2013 WJ Sieber
Generalized Anxiety Disorderuncontrollable, excessive worry across variety of issues, restlessness, fatigue, poor concentration, muscle tension, and sleep disturbance.
Lifetime prevalence in U.S. of 8.3% with one-year prevalence of 3.1%
Only 13% of patients with GAD present to their PCP with a chief complaint of anxiety; common presentations include vague somatic symptoms, pain, sleep disturbance, and depression.

© 2013 WJ Sieber
Generalized Anxiety Disorder
The neurobiology of the disorder is thought to involve a wide cortical and subcortical network that includes but is not limited to the amygdala and the bed nucleus of the stria terminalis (BNST). These two regions have been hypothesized to play different roles in stress and anxiety; the amygdala regulates responses to brief emotional stimuli, while the BNST is involved in regulation of sustained anxiety.

© 2013 WJ Sieber
Generalized Anxiety Disorder
Trait anxiety associated with decreased connectivity between amygdala and anterior cingulate.
fMRI scans show that GAD patients have decreased activity in the amygdala and increased activity in the BNST, supporting advocates of SSRIs/SNRIs versus short-acting benzodiazepines. GAD patients disengage the amygdala and its response to acute stress earlier than non-anxious controls, making way for the BNST to maintain a more sustained state of anxiety. (Bishop, 2009).

© 2013 WJ Sieber
PTSD• Lifetime Prevalence
• 8% of general population• 15-30% of Vietnam veterans• 21-48% of sexual abuse survivors• 18-32% of firefighters• 7-11% of inhabitants of NYC after 9/11
• Females 2x as likely to develop PTSD post-trauma
© 2013 WJ Sieber
Post Traumatic Stress DisorderDSM-IV-R Criteria
Traumatic event
SymptomsRe-experiencing
Persistent avoidance
Hyper-arousal
Impairment in functioning, one month or more duration
Neuropsychological mechanisms (e.g., hippocampus) that are affected and the reciprocal loop of memory, arousal, and avoidance (Ravindran, Stein, 2009). Consolidation of memories is when reminders are associated with hyper-arousal (intrusion, nightmares, startle response).
Low levels of cortisol increase risk for PTSS

© 2013 WJ Sieber
An intact hippocampus is necessary for the consolidation of information from short-term memory to long-term memory (all explicit memories).
Hippocampus is necessary for the consciously recalled details of events associated with fear memories (again explicit memories)
An intact amygdala is necessary for the production of implicit memory reflected in conditioned fear (reflexive, visceral symptoms).
Peri-traumatic dissociation impairs consolidation (explicit memories) yet fear and arousal (implicit memories) remain.
Role of the hippocampus and amygdala in fear memory processing?
© 2013 WJ Sieber
Obsessive Compulsive Disorderobsessions or compulsions : time-consuming & unreasonable
obsessions: recurrent thoughts/images experienced as intrusive and not worries about real-life problems
compulsions: repetitive behaviors or mental acts aimed at preventing a dreaded event.
Actions associated (brain connected) with decreased anxiety are going to be repeated (i.e., compulsions), yet always be connected with anxiety
Thought-action fusion: Individuals assume that thoughts imply the immorality of their character or increase the likelihood of catastrophic events (superstition); this may not be specific to OCD, but more general to anxiety.

© 2013 WJ Sieber
Panic Disorder
Unexpected Panic attacks (pounding heart, sweating, choking, dizzy, depersonalization, shaking, numbness, fear of dying), experienced repeatedly or chronic fear of having another
Lifetime Prevalence of 4.7%
Only 11% of patients receive SSRIs, similar for CBT
Increased risk of Coronary Artery Disease
© 2013 WJ Sieber
Social Anxiety and Phobias
Social Anxiety Disorder: persistent fear of scrutiny or humiliation in social situations ; fear to display anxiety symptoms or act in way (e.g., stuttering) that will be embarrassing or potentially lower social status or acceptance.
Annual prevalence of up to 7% in U.S.Hyperactivity of amygdala (also in specific phobias and PTSD)
Specific phobia: excessive, persistent, and unreasonable fear cued by object or situation
© 2013 WJ Sieber
Other resources
NCCAM.NIH.GOV
Googlescholar
© 2012 WJ Sieber

© 2013 WJ Sieber
“There is nothing either good or bad,
but thinking makes it so.” - Hamlet
“The mind is its own place, and in itself
Can make a Heaven of Hell, a Hell of Heaven.”
- Milton
© 2013 WJ Sieber
Common cognitive distortions in anxiety
‘Shoulds’/ perfectionism
Catastrophizing
Mind reading
Forecasting
Feelings are Facts

CBT: Thought Record
Situation Mood Automatic Thoughts Impact on
What happened? The event.
How did you feel in this situation?
What are you telling yourself about the event?
Mood-5 to +5
Late for work AngryUpsetStupidAnxious
1. I can’t do anything right.2. I’m an idiot.3. I should have left earlier.
4. I’m going to get fired.Replacement thoughts5. This is the first time I’ve been late this year.6. I will stay 20 minutes later to make up the time.
-3-4-2
-4
+1
+2
© 2013 WJ Sieber
Attributional style
Personal? (internal ……….……….. external)
Pervasive? (global …………………. specific)
Permanent? (stable ………..……….... temporary)

© 2013 WJ Sieber
Essential concepts in mood management
Awareness: hard to change what you’re not aware of.
Control:
Central to anger and depression
Illusion and perceived controlEysenck’s Attentional Control Theory: Anxiety impairs efficient functioning of the goal-directed attentional system and increases the extent to which the processing is influenced by the stimulus-driven attentional system.
Inhibition and Shifting
The AAA model.

© 2013 WJ Sieber
Control Over a Stressor• vPFC turns off the stress response
• Control activates the ventral prefrontal cortex (vPFC) (trait anxiety lowers top-down control over threat-related distractors)
• Perceived control eliminates the effects of stress; after experiencing control, extrapolate to other stressors
• PTSD patients don’t activate this region under stress
• Top (dorsal) portion of anterior cingulate involved in cognitive processing, whereas bottom/rear of anterior cingulate is involved in emotional processing and is most associated with anxiety.

© 2013 WJ Sieber
Interventions for anxiety
Coping skills training (Donald Meichenbaum) for panic disorder: This evidence-based strategy teaches skills for de-escalation for several of the patient’s physiological and cognitive symptoms of panic. Important to its success is brief cycling of skills with refocus away from “success”.
A highly similar approach is described as Interoceptive exposure by (Boswell and Barlow, 2013). A patient re-imagines the physiological sensations during a panic episode in order to apply learned relaxation skills.

© 2013 WJ Sieber
Interventions for PTSD• Emotional regulation and prolonged exposure (Foa)
• Eye Movement Desensitization Reprocessing (Shapiro):Using a 3-pronged approach: past (trauma), present (symptom and recent experiences), and the future (prepare a template for the future). Identify negative cognitions about the traumatic event and “install” positive cognitions via “bilateral sets”.
Recent neuro-imaging studies show outcome of EMDR is increased thalamic activity (involved in integration of perceptual, somatosensory, memorial, and cognitive processes). Proposed mechanism of benefits of EMDR are that bilateral stimulation increase thalamic activation, during which time there is repair/integration. (Bergmann, 2008).

© 2013 WJ Sieber
Behavioral interventions - exposure
• Flooding therapy:
• Studies have shown little evidence that cortisol
increases during naturally occurring panic
attacks.
• Cortisol levels are higher in those with Panic
Disorder than controls.
• Lower cortisol release during exposure predicted
poorer response to exposure-based therapies
including virtual reality studies.

© 2013 WJ Sieber
Behavioral interventions - Journaling• Emotional disclosure /diary-keeping (J. Pennebaker):
When 3 elements are present in describing previous traumatic events experienced personally, most studies show emotional and immunological benefit, though only after a given period of time (usually 3 - 6 months). The 3 elements are: initial disclosure, ‘heartfelt’, and ‘new meaning’ achieved from processing.• Story-telling increases integration between hemispheres as
stories are both linear and emotive
• Increased somatic illnesses if right hemisphere activation is inadequately transferred to left hemisphere for verbal expression

© 2013 WJ Sieber
.
“Action trumps anxiety”
– W. J. Sieber

© 2013 WJ Sieber
Unified Protocol for the Transdiagnostic Treatment of Emotional Disorders (Barlow et al, 2011)
An emotion-focused CBT treatment that distills and incorporates common evidence-based treatment strategies (identifying &modifying maladaptive appraisals, changing maladaptive action tendencies/experiential prevention of avoidance/exposure), and is designed to be applied to anxiety and unipolar mood disorders.
These modules are preceded by motivation enhancement and psycho-education on the nature of emotions.
Final sessions focus on relapse prevention techniques.

© 2013 WJ Sieber
Acceptance & Commitment Therapy (Hayes, 1999)
A contextually focused therapy that uses mindfulness and behavioral activation to increase psychological flexibility, engagement in values-based positive behaviors while experiencing difficult thoughts and emotions
Experiential AvoidanceThe tendency to avoid making direct contact with distressing thoughts or images, unpleasant emotions, painful memories, distressing physical sensations, and the situations that trigger them
Cognitive FusionTendency of human beings to get caught up in the content of what they are thinking so that it dominates over other useful sources of behavioral regulation.

© 2013 WJ Sieber
Acceptance & Commitment Therapy
F.E.A.R.:Fusion with your thoughts
Evaluation of experience
Avoidance of your experience
Reason giving for your behavior
D.A.R.E.:Disengagement from unhelpful thinking
Acceptance that at times you will feel discomfort
Realistic goals
Embracing values

© 2013 WJ Sieber
A C TAccept your reactions and be present
Choose a valued direction
Take actionDescribe client’s change agenda and how it hasn’t worked
Undermine attachment to change agenda
Maybe the solutions make things worse because the whole thing is a setup
Maybe these so-called solutions are actually part of the problem
The point isn’t to get to a “relaxed state,” the point is to be aware of whatever is going on for you without avoidance or fusion
© 2013 WJ Sieber
Now what?

© 2013 WJ Sieber
Final ideas on ‘over—active’ brain & emotional management
20 minutes in 20 seconds
Framing CBT (tolerance and reduction, full tool box)
“He who fears he shall suffer already suffers what he fears.” – Michel de Montaigne
Thought-stopping/attention grabbing tasksWorry box/compartmentalizing

© 2013 WJ Sieber
Average effect size estimates (Hedges’ g) and corresponding 95% confidence intervals of the acute treatment efficacy of CBT as compared to placebo on the various anxiety disorders for the primary continuous anxiety measures (red bars) and depression measures (green bars)
© 2013 WJ Sieber
Foundational concepts
Intolerance for Uncertainty (Alan Watts)
Sense of coherenceHedonic pleasure (e.g., good meal, plasma TV)Eudaimonic (i.e., meaning, noble purpose) is associated with significant decrease in stress-related gene expression profile

© 2013 WJ Sieber
Control over oneself
• Anxiety = aberrant ANS cardiac control. • A range of HRV indices converge to implicate low
vagal and elevated sympathetic activity in anxiety. • These findings fit a theoretical model that views
anxiety as a systemic inflexibility grounded in poor inhibition.
• This is compatible with systems models of biological stability that stress the importance of a wide range of responsiveness for maximal adaptation and resiliency.

© 2013 WJ Sieber
© 2013 WJ Sieber
Factors in effective treatment
Exposure to trauma scripts produces:Increased activity (as measured by blood flow) in:
Right medial orbital frontal cortex, insula, and amygdalaDecreased activity in:
Left anterior prefrontal cortex- especially Broca’s area (expressive speech)
Increased HR and decreased HRV occurs in Panic Disorder patients; CBT treatment increases HRV by correcting dysregulated breathing.
Adding HRV biofeedback may enhance treatment effects for panic.
© 2013 WJ Sieber
Mindfulness Meditation is not a means to an end. It is both means and the end. - J. Krishnamurti
• What lies behind us and before us are tiny matters compared to what lies within us. - Oliver W. Holmes
• “All of man’s difficulties are caused by his inability to sit, quietly, in a room by himself.” – Pascal
• Our intent is not to feel better, but to get better at feeling. – Michael Brown
• Live vertically, not horizontally. – W. Sieber
• Cognitive flexibility & non-judgmental focus on the present.

© 2013 WJ Sieber
Mindfulness(Fraser et al, Healing Power of Meditation)
Mistakenly we identify with thoughts and emotions and take them to be all that we are. So if we have a positive thought we conclude that we are good; if we have a mean thought we condemn ourselves as terrible and unworthy.
Where are all the thoughts you had this morning…… they don’t exist. They were fleeting and impermanent and constantly changing. And does anyone see these thoughts of yours? Do you? They just come and they go. But we attach such huge importance to them.
Thoughts settle on their own, quite naturally just like the waves that arise and then settle back into the ocean.

© 2013 WJ Sieber
Mindfulness • Thoughts and emotions are not really our mind. They just go
drifting by like the clouds. Its all a question of our perspective.
Whether we view the thoughts and emotions the way the sky
views the clouds, or we view them like someone down on the
ground looking up and unable even to believe there is a sky
up there beyond the clouds.
• We’re plagued by restlessness, speed & aggression. We don’t know how to settle in ourselves, come in touch with ourselves, and find our ground.
© 2013 WJ Sieber
Mindfulness
We also have the capacity to hear and articulate sounds, yet
the habit of hearing sounds may create in us a stubborn
attitude of always blaming sounds as external.
“good sounds” and “bad sounds”?
If there were no notion of good sounds or bad sounds, we
would not have feelings of aversion or attachment toward the
things we hear (e.g., neurolinguistic programming).

© 2013 WJ Sieber
Mindfulness It is the same with our senses of taste, touch, and smell. Most importantly this attachment and aversion applies to our mind which comes up with all kinds of different thoughts. Its a wonderful potential that we are all naturally gifted with, yet that gift becomes intertwined with two things: stubbornness and impatience. Since we are always impatient and we are going to be stubborn we have to find quick answers to everything. The quickest answer seems to be to segregate everything into things we like and things we don’t like. So we have developed a habit of always saying “this is what I like, and this is what I don’t like”. What you do not like is blamed for a number of negative emotional experiences that we go through in life. What you do like you can never get enough of. Half of your life is spent chasing after that, and the other half is spent running away from what you do not want to encounter.

© 2013 WJ Sieber
Mindfulness
Allow yourself to be still for at least 15 minutes.
Be patient as you are actually reversing the current (e.g., 52 years of action-engaged body versus 15 minutes of stillness). Which one is going to win? which one will I be more familiar with? You need to know what your habit is and what you are reversing.
Each day try to find stillness. Sit still.
© 2013 WJ Sieber
Meditation
o Meditation is not the same as relaxation
o All meditation is not the same
o Major subtypes:o Focused attention (concentrative ) meditationo Open awareness (receptive/mindfulness) meditationo Meditative techniques that focus on a specific feeling
tone or relational stance (compassion, loving kindness)

© 2013 WJ Sieber
Meditationo Focused attention
o Directing and sustaining attention on a selected object (e.g., breath sensation)
o Detecting mind wandering and distractors (e.g., thoughts)o Disengagement of attention from distractors and shifting
attention back to the selected objecto Cognitive reappraisal of distractor (e.g., ‘just a thought’, ‘it is
OK to be distracted’)
o Open monitoringo No explicit focus on objectso Non-reactive meta-cognitive monitoringo Non-reactive awareness of automatic cognitive & emotional
interpretations of sensory and perceptual stimuli

© 2013 WJ Sieber
Vipassanao Open Monitoring practice leads one to a more acute, but less emotionally
reactive, awareness of autobiographical sense of identity
o Open Monitoring involves cultivation of awareness and its emotional tone without judgment; it engages processes involved in interoception/somatic awareness
o Apprehend how our feelings and attitudes change. For example, pain is pain, but as you focus on your bodily sensations you begin to realize that what you thought was pain is just a concept, and if you can peer beyond the concept you perceive a cluster of sensations – tingling in your feet, pressure in your knees, burning in your calf muscles.
o The whole gestalt adds up to pain, but if you focus on its constituents, it is no longer painful – the sensations are still there, but the way we attend to them has changed. The strategy of labeling aspects of your experience (e.g., “this is distressing”) is central to MBSR.
o The new process is : That is my feet tingling (or knees burning), but the mind learns not to conceptualize this set of sensations as the aversive, unpleasant thing labeled ‘pain’.

© 2013 WJ Sieber
Meditationo So the discipline is to keep bringing your mind back to the breath. If
you are distracted, then the instant you remember, you simply bring your mind back to the breath. Nothing less is necessary. Even asking yourself “How on earth did I get so distracted?” is only another distraction. “I’m not doing this right; I’m not good enough.”
o Mind is the same as a restless child being put to bed. At first it may be very jumpy. But however agitated it gets, keep bringing it back, time and time again, to the simplicity of breathing. Gradually mind will settle, in the mind.
o “Water, if you don’t stir it, will become clear”
o “Calm Abiding” is not to fixate. It is recommended that only 25 % of your attention should be on your breath, another 25% to watchful awareness ( of your thoughts/attention), and the remaining 50% of your attention is left abiding, spaciously.”
© 2013 WJ Sieber
Meditation
o Neuroplasticity: creating new connections and associationso The brain is not static, it is constantly changing,
regenerating and rewiringo Thousands of new neurons are generated daily in the
hippocampus and ventricleso For example, scanning studies show with vipassana there is
enhanced frontal brain activity and enhanced gamma activation of the posterior cortex
o The brain changes function and structure based on what is attended to

© 2013 WJ Sieber
Meditation & neuroplasticity
o Focused attention activates (results in higher CBF) the prefrontal cortex, anterior cingulate, and other executive function areas of brain, whereas‘open monitoring’ decreases activation (Manna, Raffone, 2010).
o Neurofeedback/neurotherapy helps patients change brain waves in ways that activate some regions while lower in activation in others (e.g., ADHD)
o Mindful meditation > relaxation training for anterior cingulate (Tang, Lu, Fan Yang, Posner, 2012, Proc Natl Acad Sci; Xue, Tang, Posner, 2011, Neuroreprot)
o Compassion changes the anterior cingulate (Richard Davidson: www.investigatinghealthyminds.org)
© 2013 WJ Sieber
Meditation reduces activity and size of the amygdala.
Meditators increase size of their hippocampus, the posterior cingulate, and the temporal-parietal junction (playing a central role in empathy and compassion)
Meditation boosts telomerase.
Studies by Sara Lazar and others, using imaging techniques show that certain zones of the cortex thicken with meditation. Because our cerebral cortex thins as we get older, thickening of the cortex can have anti-aging effects.
Meditation & neuroplasticity
© 2013 WJ Sieber
Meditation increases activity in the ‘paralimbic cortex’.The limbic system is the emotional center of the brain, whereas the cortical regions are engaged during thinking and problem-solving.
The paralimbic cortex connects these regions, and so can be seen as the “mind-body connection”. The paralimbic cortex has been implicated in numerous psychological phenomena including anxiety, depression, and bipolar disorders.
Meditators had expansion of their paralimbic regions, an area involved in the integration of senses, emotions, and thoughts.
Meditation & neuroplasticity

© 2013 WJ Sieber
Resilience (too fast or slow to recover?): To speed up recovery from stress change your environment, change your cognitions, practice mindful meditation; to slow down recovery spend more time focusing on negative emotional experiences, develop greater empathy.
Outlook (pessimistic or optimistic): To be more optimistic write down 3 positive characteristics of you and 3 of another each day, express gratitude regularly, compliment others regularly. Depressive realism is achieved by sitting with negative life events.
Social Intuition (‘other’ focused): To increase social intuition focus on strangers and detect subtle social cues, predict their feelings. To
Richard Davidson’s Six Emotional styles
© 2013 WJ Sieber
Self-Awareness: To boost self-awareness practice mindful meditation, decrease distractions and chose quiet environments; to decrease self-awareness multitask more or have more external stimuli present.
Sensitivity to Context (myopic or big picture): To become more sensitive to context try exposure therapy with a focus on discriminating important from unimportant details. To become less sensitive, engage in more self-reflection and complete activities that increase self-awareness.
Attention (focused concentration): To improve focus try mindful meditation and/or body scan. To reduce over-focused attention scatter books, photos and objects to distract you.
Richard Davidson’s Six Emotional styles
© 2013 WJ Sieber
Where’s your motivation?Often people attempt to live their lives backwards: they try to have more things or more money, in order to do more of what they want, so they will be happier. The way it actually works is the reverse. You must first be who you really are, then do what you need to do, in order to have what you want – Margaret Young
What is your goal, what would change if your brain were less over-active? What is the benefit?
List 3 behaviors that you can place on next week’s calendar. What will be different next week?


















