Calcium channel blockers and coronary atherosclerosis: From the rabbit to the real world
8
Calcium channel blockers and coronary atherosclerosis: From the rabbit to the real world Many calcium channel blockers have been shown to retard the development of atherosclerosis in cholesterol-fed rabbits. The mechanisms that may contribute to this effect include Stimulation of choiesteryi ester hydroiase activity in smooth muscle ceils, ameiiii of hypercholesteroiemic- induced endotheiiai dysfunction, or inhibition of smooth muscle ceil proliferation and migration. The effect of calcium channel blockers on the evolution of coronary atherosclerosis in humans has been assessed in three clinical trials. in the Montreal Heart institute trial, nicardipine did not influence the overall rate of progression and regression; however, patients treated with nicardipine experienced significantly less progression of minimal lesions, deftned as stenoses of less than or equal to 20% severity. in the international Niiedipine Trial on Antiatherosclerotic Therapy (INTACT), nifedipine had no effect on overall progression and regression but, by one method of analysis, reduced the rate of appearance of new coronary iesions. in a prefiminary report, diitiazem prevented the development of coronary atherosclerosis in heart tmnsplant recipients. These studies indicate that calcium channel blockers retard the development of early atherosclerosis not only in animal models but also in human coronary arteries. Other studies recently completed or now under way will help to clarify the clinical role of calcium channel blockers in antiatherosclerotic therapy. (AM HEART J 1994;128:1309-16.) David Waters, MD,” and Jacques Lesperance, MDb Hartford, Conn., and Montreal, Quebec, Canada Progression of coronary atherosclerosis leads to un- stable angina, myocardial infarction, congestive heart failure, and sudden coronary death. Treatments di- rected at preventing these consequences of coronary disease progression have led to reduced rates of mor- bidity and mortality; however, a more direct ap- proach would be preferable. Interventions that could prevent the appearance of the atherosclerotic plaque, slow its progression, stabilize its fibrous cap to reduce the risk of plaque fissure, or induce regression of es- tablished lesions would obviously have a major im- pact on the incidence of coronary events. To date, lipid-lowering therapy has appeared to be the most promising intervention to accomplish these objectives. l-6 However, favorable modifications of lipid levels do not solve the problem entirely. For ex- ample, in the Familial Atherosclerosis Treatment From the aDivision of Cardiology, Hartford Hospital and the University of Connecticut School of Medicine, and the “Department of Radiology, Mon- treal Heart Institute and the University of Montreal Medicel School, Reprint requests: David Waters, MD, Division of Cardiology, Hartford Hospital, 80 Seymour St., Hartford, CT 06102-5037. Copyright !L 1994 by Mosby-Year Book, Inc. 000%8703/94/$3.00 + 0 4/O/59821 Study (FATS),i one quarter of patients treated with colestipol plus niacin experienced coronary progres- sion in only 2.5 years, despite a reduction of 32% in low-density lipoprotein (LDL) cholesterol and an in- crease of 43 % in high-density lipoprotein cholesterol. Other approaches need to be explored. This paper reviews a large body of experimental evidence and three completed clinical trials suggesting that cal- cium channel blockers exert a favorable effect on the development of coronary atherosclerosis. CALCIUM CHANNEL BLOCKERS IN ANIMAL MODELS OF ATHEROSCLEROStS The model that has been used most extensively to investigate the antiatherosclerotic effects of calcium channel blockers is the cholesterol-fed rabbit. Rab- bits fed a 1% to 2 % cholesterol diet for 8 to 12 weeks develop total serum cholesterol levels in the range of 2000 mg/dl, massive hepatic lipid accumulation, and diffuse aortic atherosclerosis. Histologically, this ath- erosclerosis is characterized by an abundance of lip- id-laden foam cells and is quite dissimilar to ad- vanced human atherosclerotic plaques. A further limitation of this experimental model is that the de- velopment of atherosclerosis is variable and is influ- 1309
-
Upload
david-waters -
Category
Documents
-
view
213 -
download
0
Transcript of Calcium channel blockers and coronary atherosclerosis: From the rabbit to the real world

Calcium channel blockers and coronary atherosclerosis: From the rabbit to the real world
Many calcium channel blockers have been shown to retard the development of atherosclerosis in cholesterol-fed rabbits. The mechanisms that may contribute to this effect include Stimulation of choiesteryi ester hydroiase activity in smooth muscle ceils, ameiiii of hypercholesteroiemic- induced endotheiiai dysfunction, or inhibition of smooth muscle ceil proliferation and migration. The effect of calcium channel blockers on the evolution of coronary atherosclerosis in humans has been assessed in three clinical trials. in the Montreal Heart institute trial, nicardipine did not influence the overall rate of progression and regression; however, patients treated with nicardipine experienced significantly less progression of minimal lesions, deftned as stenoses of less than or equal to 20% severity. in the international Niiedipine Trial on Antiatherosclerotic Therapy (INTACT), nifedipine had no effect on overall progression and regression but, by one method of analysis, reduced the rate of appearance of new coronary iesions. in a prefiminary report, diitiazem prevented the development of coronary atherosclerosis in heart tmnsplant recipients. These studies indicate that calcium channel blockers retard the development of early atherosclerosis not only in animal models but also in human coronary arteries. Other studies recently completed or now under way will help to clarify the clinical role of calcium channel blockers in antiatherosclerotic therapy. (AM HEART J 1994;128:1309-16.)
David Waters, MD,” and Jacques Lesperance, MDb Hartford, Conn., and Montreal, Quebec, Canada
Progression of coronary atherosclerosis leads to un- stable angina, myocardial infarction, congestive heart failure, and sudden coronary death. Treatments di- rected at preventing these consequences of coronary disease progression have led to reduced rates of mor- bidity and mortality; however, a more direct ap- proach would be preferable. Interventions that could prevent the appearance of the atherosclerotic plaque, slow its progression, stabilize its fibrous cap to reduce the risk of plaque fissure, or induce regression of es- tablished lesions would obviously have a major im- pact on the incidence of coronary events.
To date, lipid-lowering therapy has appeared to be the most promising intervention to accomplish these objectives. l-6 However, favorable modifications of lipid levels do not solve the problem entirely. For ex- ample, in the Familial Atherosclerosis Treatment
From the aDivision of Cardiology, Hartford Hospital and the University of Connecticut School of Medicine, and the “Department of Radiology, Mon- treal Heart Institute and the University of Montreal Medicel School,
Reprint requests: David Waters, MD, Division of Cardiology, Hartford Hospital, 80 Seymour St., Hartford, CT 06102-5037.
Copyright !L 1994 by Mosby-Year Book, Inc. 000%8703/94/$3.00 + 0 4/O/59821
Study (FATS),i one quarter of patients treated with colestipol plus niacin experienced coronary progres- sion in only 2.5 years, despite a reduction of 32% in low-density lipoprotein (LDL) cholesterol and an in- crease of 43 % in high-density lipoprotein cholesterol. Other approaches need to be explored. This paper reviews a large body of experimental evidence and three completed clinical trials suggesting that cal- cium channel blockers exert a favorable effect on the development of coronary atherosclerosis.
CALCIUM CHANNEL BLOCKERS IN ANIMAL MODELS
OF ATHEROSCLEROStS
The model that has been used most extensively to investigate the antiatherosclerotic effects of calcium channel blockers is the cholesterol-fed rabbit. Rab- bits fed a 1% to 2 % cholesterol diet for 8 to 12 weeks develop total serum cholesterol levels in the range of 2000 mg/dl, massive hepatic lipid accumulation, and diffuse aortic atherosclerosis. Histologically, this ath- erosclerosis is characterized by an abundance of lip- id-laden foam cells and is quite dissimilar to ad- vanced human atherosclerotic plaques. A further limitation of this experimental model is that the de- velopment of atherosclerosis is variable and is influ-
1309

1310 Waters an& Lespirance December 1994
American Heart Journal
Table I. Potential explanations for the antiatherogenic effect of calcium channel blockers
Reduction of arterial pressurelg Antithrombotic and antiplatelet activity20, 21 Preservation of endothelial functionQ Antioxidant activityis, 2g Reduction of intracellular lipid accumulation by stimulating
cholesteryl ester hydrolase activitysQ-32 Inhibition of SMC proliferation in response to growth
factors22-24 Inhibition of SMC migration33s 34 Promotion of cholesterol efIlux26 and preventing cholesteryl
ester deposition in macrophages25
enced by many factors, including the season of the year.
Kramsch et al7 reported in the early 1980s that the calcium channel blocker lanthanum suppressed ex- perimental atherosclerosis. A beneficial effect on the development of atherosclerosis in the cholesterol- fed rabbit was subsequently demonstrated with the dihydropyridines nifedipine,8 isradipine,g nisol- dipine,lO nilvadipine,ll and nicardipine,i2 as well as with diltiazem13 and verapamil.14 The study of Henry and Bentley8 that used nifedipine is typical of these reports. For 8 weeks a 2 % cholesterol diet was fed to 13 rabbits given a placebo and 13 rabbits treated with nifedipine 10 mg twice daily. The aortic intimal sur- face covered with lipid-stainable lesions averaged 40% of: 5% in placebo-treated rabbits and 17 % f 3 % in nifedipine-treated rabbits @ < O.OOl), in spite of similar high serum cholesterol levels in both groups.
However, several studies have failed to demon- strate a beneficial effect of calcium channel blockers on experimental atherosclerosis. Potential reasons for this discrepancy include an inadequate sample size, given the wide variability in atherosclerosis de- velopment among rabbits, and poor drug bioavail- ability.15 Felodipine has recently been reported to retard aortic atherosclerosis in the cholesterol-fed rat.i6 Nifedipine17 and amlodipine la have also been shown to suppress atherogenesis in monkeys, a model more analogous to human atherosclerosis.
MECHANISM OF ACTlON
of the animal experiments, and the benefit could thus be explained by a lowering of arterial pressure. How- ever, Habib et a1.g used low doses of isradipine, within the range used in humans, and demonstrated that the antiatherogenic effect was still present even in the absence of changes in arterial pressure. On the other hand, in the clinical trial with nicardipine (discus- sion to follow), lowering of arterial systolic pressure and lower systolic pressure at baseline were signi- ficant predictors of prevention of minimal lesion progression.ig
Increased platelet aggregation is associated with coronary progression and a higher risk of coronary eventszO Calcium channel blockers exert only a weak antiaggregatory effect on platelets; however, recent data indicate that verapamil inhibits platelet throm- bus formation in humans.21 Platelet-derived growth factor (and other growth factors) plays a key role in atherogenesis by stimulating smooth muscle cell (SMC) proliferation. Nifedipine,22 isradipine,23 and verapami124 have been shown to block this response. The antiatherosclerotic effect of calcium channel blockers could therefore be related to their antiplate- let activities.
Macrophages and endothelial cells do not contain voltage-dependent calcium channels; however, cal- cium channel blockers inhibit cholesteryl ester depo- sition and promote cholesterol ef?lux from macro- phages. 26 The calcium channel blocker isradipine has been shown to partially reverse the endothelial dys- function associated with hypercholesterolemia in rabbits9 In patients with risk factors including hypercholesterolemia but without angiographic evi- dence of coronary atherosclerosis, endothelial func- tion is already abnormal, as indicated by its vasocon- strictive response to acetylcholine.27 The antiathero- genie effects of calcium channel blockers may be related to their beneficial effects on endothelial function.
Oxidation of LDL cholesterol greatly increases its atherogenic potential. 28 The process of LDL oxida- tion can probably occur in the subendothelial microenvironment where antioxidant levels may be 10w.s~ Several recent reports indicate that some cal- cium channel blockers behave as weak antioxidants in membrane systems. 2g They could thus shift the balance away from LDL oxidation and block the
The antiatherogenic effects of calcium channel generation of foam cells. In a recent preliminary re- blockers are important because they act indepen- p0rt,18 amlodipine-treated hypercholesterolemic dently of serum lipid lowering and thus provide an monkeys had less circulating oxidized LDL choles- alternate approach to influencing the evolution of terol and less coronary and aortic atherosclerosis human coronary atherosclerosis. Various mecha- than did control animals with comparable plasma nisms of action advanced to account for this benefit levels of total and LDL cholesterol. are listed in Table I. High doses were used in many Intracellular lipid accumulation is an important

Volume 126, Number 6, Par! 2
American Heart Journal Waters and Lrspkrance 1311
feature of the atherosclerotic plaque that can be fa- vorably influenced by nifedipine30 or verapamiL31 As shown by Etingin and Hajjar,30 nifedipine increases cholesteryl ester hydrolase activity and thus reduces cholesterol and cholesteryl ester levels in lipid-laden, cultured SMCs from rabbits. This mechanism has been proven to be relevant to human atherosclero- sis32: in 35 patients undergoing coronary bypass sur- gery, aortic tissue samples were obtained and stripped of endothelium and adventitia. In the 23 patients who had been treated for several months with cal- cium channel blockers, cholesteryl ester hydrolase activity was significantly higher in the tissue samples and cholesterol and cholesteryl ester levels were sig- nificantly lower compared with the 12 patients who did not receive pretreatment with a calcium channel blocker. These differences were independent of serum cholesterol levels, age, and other medica- tions. The mechanism by which calcium channel blockers stimulate cholesteryl ester hydrolase activ- ity is by increasing intracellular cyclic adenosine monophosphate.2g
In addition to SMC proliferation, migration of SMCs from the media to the intima is another com- ponent of atherogenesis that is favorably influenced by calcium channel blockers. Nakao et a1.33 demon- strated that nicardipine can block SMC migration. In a recent preliminary report,34 amlodipine, nitren- dipine, and verapamil each inhibited SMC migration induced by platelet-derived growth factor, with am- lodipine being somewhat superior to the other two drugs. A possible explanation for this superiority has been provided by the work of Mason.35 The charged dihydropyridine amlodipine remains in contact with the calcium channel longer and has almost no loss of activity when the cholesterol content of the cell membrane is increased, as has been shown to occur with increasing blood cholesterol levels. In contrast, the membrane concentrations of uncharged dihydro- pyridines such as nimodipine or isradipine may decrease up to fourfold in the presence of an in- creased membrane cholesterol content.
CLINICAL TRIALS OF CALCIUM CHANNEL BLOCKERS
AND CORONARY ATHEROSCLEROSIS
The results of three randomized, placebo-con- trolled clinical trials assessing the effect of calcium channel blockers on the evolution of coronary ath- erosclerosis have been reported.lgp 36, 37
The Montreal Heart Institute Nicardipine Trial. The purpose of this study was to determine whether chronic treatment with nicardipine could influence the progression of coronary atherosclerosis.ig Pa- tients 65 years of age or younger with less than 75%
stenoses in at least four coronary artery segments were randomized within 1 month of baseline coro- nary arteriography to double-blind therapy with placebo or nicardipine, 30 mg three times per day. The following patients were excluded: those with previous or planned bypass surgery or angioplasty; those with an ejection fraction less than 0.40, severe triple vessel disease, or left main stenosis; and those with a heart condition requiring treatment with a calcium channel blocker. Of the 383 patients en- rolled, 335 (87 % ) underwent repeat coronary arteri- ography at 24 months, with coronary lesions mea- sured quantitatively.
Coronary events (five deaths, 22 myocardial in- farctions, and 28 episodes of unstable angina) oc- curred in 28 of 192 patients treated with nicardipine and 23 of 191 patients who received placebo (p = 0.21). Progression, defined as a worsening of minimum diameter by at least 0.4 mm, was detected in 44 % of patients receiving nicardipine and 43 % of patients receiving placebo; 23% of patients treated with nicardipine and 19% of placebo recipients experienced regression of one or more lesions. None of these differences approached statistical significance.
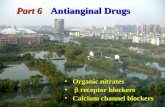
Among the 217 patients with 411 stenoses of less than or equal to 20% at the first arteriogram, such minimal lesions progressed in only 15 of 99 patients treated with nicardipine compared with 32 of 118 patients who received a placebo (15% vs 27 % , p = 0.046). In this subgroup, 16 of 178 minimal lesions in patients treated with nicardipine and 38 of 233 minimal lesions in patients who received a placebo progressed (p = 0.038). Progression of a minimal lesion is illustrated in Fig. 1. By stepwise lo- gistic regression analysis, baseline systolic blood pressure (p = 0.04) and the change in systolic blood pressure between baseline and 6 months (p = 0.002) correlated with progression of minimal lesions. This finding suggests that blood pressure reduction might account for the beneficial effect of nicardipine on minimal lesions.
Overall, the results of this trial indicate that nicardipine has no effect on advanced coronary ath- erosclerosis but may retard the progression of mini- mal lesions, defined as those less than 20 % in steno- sis diameter on the first arteriogram. This effect of the drug is compatible with the experimental animal data discussed previously. Although “new” lesions, or minimal lesions that progress, are rarely severe enough to cause myocardial ischemia, they are dan- gerous because they increase the risk of a coronary event. Coronary lesions that rupture and cause my- ocardial infarction are usually in the range of 30% to

1312 Waters and Lespbrance December 1994
American Heart Journal
Fig. 1. Development of a new coronary lesion. A, This segment of the left anterior descending coronary artery contains only minimal irregularities (arrows). B, The quantitative measurement system calculates a diameter stenosis of 13.5 % . Stenoses within this range can be classified as measurement noise. C, Repeat arteriography 2 years later reveals a mild but definite lesion (arrows) at the same site. D, The minimum lumen diameter has decreased from 2.41 to 1.55 mm and the diameter stenosis is now 36 % . Although this lesion is not severe enough to causeischemia, the patient is at risk for occlusion and myocardial infarction.
70% diameter stenosis,38 and new lesions in this range are more likely to be at higher risk than older, more fibrotic stenoses.
The International Nifedipine Trial on Antiatheroscle- rotic Therapy (INTACT). The purpose of INTACT was to assess whether treatment with nifedipine retarded the angiographic progression of coronary atheroscle- rosis.36 In nine European centers, 425 patients with “mild” coronary artery disease were randomly allo- cated to double-blind therapy with placebo or nifed- ipine, 80 mg per day in divided doses. Inclusion cri- teria included age of less than 65 years and the pres- ence of at least one coronary risk factor. Patients previously treated with calcium channel blockers for at least 6 months, those with diffuse or severe coro- nary disease, and patients requiring extensive revas- cularization procedures were excluded. A second coronary arteriography was planned after 3 years and all films were interpreted quantitatively.
The two groups were well matched for clinical variables, and 282 (82 % ) of the patients had a second arteriography. Progression and regression were de- fined as a change of greater than or equal to 20% in diameter stenosis or of greater than or equal to 0.4 mm in minimum diameter. Progression, using the latter criterion, was seen in 35% of patients who re- ceived a placebo and 29% of patients treated with nifedipine; 21% of patients in the placebo group and 16% of patients in the nifedipine group had re- gression. These differences were not statistically significant.
New coronary lesions, defined as stenoses of less than 20% on the first arteriogram and greater than 20 % on the second arteriogram, developed in 49 % of patients receiving placebo and 40% of patients treated with nifedipine. This difference, which rep- resents the statistically more appropriate method for evaluating a treatment effect, was not statistically

Volume 126, Number 6, Part 2
American Heart Journal Waters and Lesptkance 1313
significant. However, the authors also reported new lesions on a per-patient basis: 0.82 new lesions per patient in the placebo group and 0.59 in the nifed- ipine group. Expressed this way, as a 28% reduction in new lesions per patient with active treatment, the difference was statistically significant (p = 0.034).
Although clinical events were not an endpoint of the trial, it is disturbing to note that mortality was higher in the nifedipine group. Two patients who re- ceived placebo and eight patients treated with nifed- ipine died from cardiac causes, and four additional noncardiac-related deaths were reported in the nifed- ipine group. No differences between treatment groups were seen for new myocardial infarctions or unstable angina. The pattern of mortality in INTACT is con- sistent with two other studies in survivors of myo- cardial infarction, in which more deaths were re- ported in patients treated with nifedipine compared with those receiving placebo.3gy 4o Some dihydropyri- dine calcium channel blockers have occasionally shown “proischemic” effects41; how long-term treat- ment with these drugs will influence coronary events and overall mortality is not certain.
Coronary atherosclerosis after heart transplantation. A form of accelerated coronary atherosclerosis de- velops after heart transplantation that limits the long-term prognosis of these patients. This process is manifest angiographically as progressive distal vessel obliteration associated with more typical proximal atherosclerotic lesions. 42 Intracoronary ultrasonog- raphy shows that by 1 year after transplantation all patients have developed at least some degree of intimal thickening, the initial atherosclerotic abnormality.43
Preliminary results from an ongoing study indicate that diltiazem may prevent this type of atherosclero- sis. 37 Coronary arteriograms were obtained soon after heart transplantation and at 1 and 2 years after transplantation in 57 of 104 consecutive eligible pa- tients who were randomized to unblinded treatment with or without diltiazem. The average coronary ar- terial diameter decreased in the control group (p < 0.001) but remained unchanged in patients treated with diltiazem. Coronary stenoses greater than 50% of luminal diameter have developed in seven untreated and two diltiazem-treated patients. Coronary death or retransplantation has occurred in five patients, none of whom was in the diltiazem group. Further follow-up will reveal whether the small improvements seen within 2 years in coronary dimensions will presage a reduction in future coro- nary events in these patients.
The importance of immunologic mechanisms in the pathogenesis of atherosclerosis after heart trans-
plantation and its similarity to ordinary atheroscle- rosis in terms of etiology have not been well defined. The mechanism by which diltiazem appears to pre- vent atherosclerosis after heart transplantation and the mechanism by which dihydropyridines appear t,o prevent the development of new lesions may be sim- ilar but are as yet undefined.
Other trials. A small study that was neither ran- domized nor blinded reported that patients treated with nifedipine had less coronary progression and more regression than did patients treated with iso- sorbide dinitrate or propranoloi.44 These results with nifedipine were not confirmed by the much larger INTACT study.
A salutary effect of nifedipine on the development of atherosclerosis in coronary bypass grafts, as as- sessed in a randomized, double-biind, placebo-con- trolled trial, was reported in preliminary form in 1989.45 In another study of the effect of drug therapy on the evolution of atherosclerosis in bypass grafts and native vessels, the Frankfurt Isoptin Progression Study (FIPS) randomized patients after coronary bypass surgery to verapamil or placebo. The trial was hampered by avery high dropout rate, and the results have not yet been published.
The effect of isradipine on the development of ca- rotid atherosclerosis has been assessed with use of ultrasonography in the recently completed Multi- center Isradipine Diuretic Atherosclerosis Study (MIDAS). This trial did not observe an antiathero- genie effect of isradipine (Curt D. Furberg, personal communication, August 1994). The Prospective Ran- domized Evaluation of the Vascular Effects of Nor- vast Trial (PREVENT) is currently randomizing 720
patients with mild coronary atherosclerosis to amlo- dipine or placebo. Patients will undergo a second coronary arteriography after 3 years; a subset of pa- tients will also be assessed by carotid ultrasonogra- phy. The results of these two trials will help clarify what clinical role calcium channel blockers will have as antiatherosclerotic therapy.
FUTURE DIRECTIONS
A major limitation of angiographic trials is that coronary arteriography provides limited informa- tion. Although quantitative techniques can more ac- curately assess changes in the severity of arterial narrowings than could older methods,46 the arterial wall and its pathology are not directly visualized. Newer techniques, specifically angioscopy47 and in- travascular ultrasonography,48 circumvent this limi- tation and will eventually yield data on lesion changes to complement coronary arteriography. Although both of these techniques are now in their infancy, in-

1314 Waters and Lespkrance December 1994
American Heart Journal
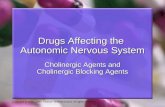
Fig. 2. In this segment that appeared normal on coronary arteriography, intracoronary ultrasonography (A) demonstrates extensive intramural disease. The white arrow denotes a large echo-dense plaque that was not apparent on any of the angiographic views. The underlying junction of plaque and intima is clearly seen (black arrow). The corresponding pathology cross-section (B) reveals a large, lipid-rich plaque (ar- row). This case illustrates that intracoronary ultrasonography is capable of defining intramural atheroscle- rosis that is not appreciated by arteriography.
travascular ultrasonography is superior to angios- copy because it does not require a blood-free field of vision and displays the entire thickness of the vessel wall, not just the surface. Intracoronary ultrasonog- raphy is likely to be more useful than coronary arte- riography, particularly in the assessment of early coronary lesions. As illustrated by Fig. 2, intramural coronary atherosclerosis can be detected by intra- coronary ultrasonography early in its evolution, be- fore a lesion is seen on coronary arteriography.
In spite of their limitations, the clinical trials com- pleted to date demonstrate that calcium channel blockers do not influence the evolution of established coronary atherosclerosis but appear to prevent the progression of early lesions. This conclusion is tenta-
tive, pending completion of ongoing clinical trials. Whether this beneficial effect is a feature of all cal- cium channel blockers or whether some of these drugs are more potent than others in this regard is as yet not known.
The combined effect of lipid-lowering therapy and a calcium channel blocker on human coronary ath- erosclerosis has yet to be investigated. In the recently published Canadian Coronary Atherosclerosis Inter- vention Trial (CCAIT),6 lovastatin significantly re- duced the appearance of new coronary lesions. Add- ing a calcium channel blocker to a 3-hydroxy-3- methylglutaryl coenzyme A reductase inhibitor might add no additional benefit with respect to the devel- opment of new lesions, or the combination might

Volume 128, Number 6, ParI2
American Heeti Journal
produce an additive or synergistic effect because the mechanisms of action of the two classes of drugs dif- fer. Further studies can be expected to yield an array of drugs that exert a favorable influence on the evo- lution of coronary atherosclerosis by acting on dif- ferent components of the atherosclerotic process.
REFERENCES
1.
2.
3.
4.
5.
6.
I.
8.
9.
10.
11.
12.
13.
14.
15.
16.
11.
18.
Brown G, Albers JJ, Fisher LD, Schaffer SM, Lin JT, Kaplan C, Zhao XQ, Bisson BD, Fitzpatrick VF, Dodge HT. Regression of coronary ar- tery disease as a result of intensive lipid-lowering therapy in men with high levels of epolipoprotein B. N Engl J Med 1990;323:1289-98. Buchwald H, Varco RL, Matts JP, Long JM, Fitch LL, Campbell GS, Pearce MB, Yellin AE, Edmiston WA, Smink RD, Sawin HS, Campos CT, Hansen BJ, Tuna N, Karnegis JN, Sanmarco ME, Amplatx K, Castaneda-Zuniga WR, Hunter DW, Bissett JK, Weber FJ, Stevenson JW, Leon AS, Chalmers TC, and the POSCH Group. Effect of partial ileal bypass surgery on mortality and morbidity from coronary heart disease in patients with hypercholesterolemia. N Engl J Med 1990; 323:946-55. Cashin-Hemphill L, Mack WJ, Pagoda JM, Sanmarco ME, Asen SP, Blankenborn DH. Beneficial effects of colestipol-niacin on coronary atherosclerosis. JAMA 1990,264:3013-7. Kane JP, Malloy MJ, Ports TA, Phillips NR, Diehl JC, Have1 RJ. Re- gression of coronary atherosclerosis during treatment of familial hyper- cholesterolemia with combined drug regimens. JAMA 1990;264:3067- 12. Watts GF. Lewis B, Brunt JNH, Lewis ES, Coltart DJ, Smith LDR, Mann JI, Swan AV. Effects on coronary artery disease of lipid-lowering diet, or diet plus cholestyrsmine, in the St Thomas’ Atherosclerosis Re- gression Study (STARS). Lancet 1992;339:563-9. Waters D, Higginson L, Gladstone P, Kimball B, Le May M, Boccuzsi SJ, Lesperance J, the CCAIT Study Group. Effects of monotherapy with an HMG-CoA reductase inhibitor on the progression of coronary ath- erosclerosis as assessed by serial quantitative arteriography: the Cana- dian Coronary Atherosclerosis Intervention Trial. Circulation 1994;89: 959-68. Kramsch DM, Aspen AJ, Rozler LJ. Atherosclerosis prevention by agents not affecting abnormal levels of blood lipids. Science 1981;213: 1511-2. Henry PD, Bentley KI. Suppression of atherogenesis in cholesterol-fed rabbit treated with nifedipine. J Clin Invest 1981;68:1366-9. Habib JB, Bossaller C, Wells S, Williams C, Morrisett JD, Henry PD. Preservation of endothelium-dependent vascular relaxation in choles- terol-fed rabbit by treatment with the calcium blocker PN 29tlllO. Circ Res 1986;58:305-9. Fronek K. Effect of nisoldipine on diet-induced atherosclerosis in rab- bits. Ann NY Acad Sci 1988;522:525-6. Nomoto A, Hirosumi J, Sekiguchi C, Mutoh S, Yamaguchi I, Aoki H. Antiatherogenic activity of FE34235 (Nilvadipine), a new potent calcium antagonist: effect on cuff-induced intimal thickening of rabbit carotid artery. Atherosclerosis 1987;64:255-61. Willis AL, Nagel B, Churchill V, Whyte MA, Smith DL, Mahmud I, Puppione DL. Antiatherosclerotic effects of nicardipine and nifedipine in cholesterol-fed rabbits. Atherosclerosis 1985;5:250-5. Sugano M, Nakashima Y, Tasaki H, Takasugi M, Kuroiwa A, Koide 0. Effects of diltissem on suppression and regression of experimental ath- erosclerosis. Br J Exp Pathol 1988;69:515-23. Rouleau JL, Parmley WW, Stevens J, W&mar-Coffelt J, Sievers R, Mahley RW, Have1 RJ. Verapamil suppresses atherosclerosis in choles- terol-fed rabbits. J Am Co11 Cardiol 1983;1:1453-60. Henry PD. Calcium antagonists as anti-atherosclerotic agents. Arterio- sclerosis 1990;10:963-5. Nunnari JJ, White SDT, Cuenoud HF. The effect of felodipine on lipid deposition in the rat aorta (abstract). Circulation 1993;88(supplI):I522. Lichtor T, Davis HR, Vesselinovitch D, Wissler RW, Mullan S. Suppression of atherogenesis by nifedipine in the cholesterol-fed rhesus monkey. Appl Pathol 1989;7:8-18. Kramsch DM. Sharma RC, Hodis HN. Amlodipine suppresses in viva
low-density lipoprotein oxidation, hyperinsulinemia and atherosclero- sis in primates (abstract). Circulation 1993;88(suppl IhI562.
19. Waters D, Lesperance J, Francetich M, Causey D, Theroux P, Chiang YK, Hudon G, Lemarbre L, Reitman M, Joyal M, Gosselin G, Dyrda I, Mater J, Have1 RJ. A controlled clinical trial to assess the effect of a calcium channel blocker on the progression of coronary atherosclerosis. Circulation 1990;82:1940-53.
20. Lam JYT, L&our JG, Lesperance J, Waters D. Platelet aggregation, coronary artery disease progression, and future coronary events. Am J Cardiol 1994;73:333-8.
21. Lacoste LL, Lam JYT, Hung J, Waters D. Oral verapamil inhibits platelet thrombus formation in men. Circulation 1994;89:630-4.
22. Jackson LJ, Bush RC, Bowyer DE. Inhibitory effect of calcium antag- onists on balloon catheter-induced arterial smooth muscle cell prolif- eration and lesion size. Atherosclerosis 1988:69:115-22.
23. Handley DA, Van Valen RG, Melden MK, Saunders RN. Suppression of rat carotid lesion development by the calcium channel blocker PN 200-110. Am J Path01 1986;124:88-93.
24. Yang Z, No11 G, Luscher TF. Calcium antagonists differently inhibit proliferation of human coronary smooth muscle cells in response to pulsatile stretch and platelet-derived growth factor. Circulation 1993; 88:832-6.
25. Daugherty A, Rateri DL, Schonfeld G, Sobel BE. Inhibition of cho- lesteryl ester deposition in macrophages by calcium entry blockers: an effect dissociable from calcium entry blockade. Rr d Pharmacol 1987; 91:113-8.
26. Schmitz G, Robenek H, Beuck M. Ca++ antagonists and ACAT inhib- itors promote cholesterol etawt from macrophages by different mecha- nisms. Arteriosclerosis 1988,8:46-56.
27. VitaJA,TreasureCB,NabelEG,McLenachanJM,FishRD,YeungAC, Vekshtein VI, Selwyn AP, Ganz P. Coronary vasomotor response to acetylcholine relates to risk factors for coronary artery disease. Circu- lation 1990;81:491-7.
28. Steinberg D, Parthasarathy S, Carew TE, Khoo JC, Witztum JL. Be- yond cholesterol modifications of low-density lipoprotein that increase its atherogenicity. N Engl J Med 1989;320:915-24.
29. Henry PD. Antiperoxidative actions of calcium antagonists and athero- genesis. J Cardiovasc Pharmacol 1991;18(suppl l):S6-10.
30. Etingin OR, Hajjar DP. Nifedipine increases cholesteryl ester hydro- lytic activity in lipid-laden rabbit arterial smooth muscle cells. J Clin Invest 19%$75:1554-E.
31. Stender S, Ravn H, Haugegaard M, Kjeldson K. Etfect of verapemil on accumulation of free and esteriied cholesterol in the thoracic aorta of cholesterol-fed rabbits. Atherosclerosis 1986;61:15-23.
32. Etingin OR, Hajjar DP. Calcium channel blockers enhance cholesteryl ester hydrolysis and decrease total cholesterol accumulation in human aortic tissue. Circ Res 1990;66:185-90.
33. Nakao J, Ito H, Ooyama T, Chang WC, Murota S. Calcium dependency of aortic smooth muscle cell migration induced by 12-L-hydroxy- 5,8,10,14-eico-satetraenoic acid. Atherosclerosis 1983;46:399-19.
34. McMurray HF, Chahwala SB. Amlodipine exerts a potent antimigra- tory effect on aortic smooth muscle cells in culture (abstract). d Am Co11 Cardiol 1991;17:194A.
35. Mason RP. Differential effect of cholesterol on membrane interaction of charged versus uncharged 1,4-dihydropyridine calcium channel an- tagonists: a biophysical analysis. Cardiovasc Drug Ther (in press).
36. Lichtlen PR, Hugenholtz PG, Rafhenbeul W, Hecker H. Jost S, Deck- em JW, on behalf of the INTACT group investigators. Retardation of angiographic progression of coronary artery disease by nifedipine. Lan- cet 1990;335:1109-13.
37. Schroeder JS, Gao SZ, Alderman EL, Hunt SA, Johnstone I, Boothroyd DB, Wiederhold V, Stinson E. A preliminary study of diltiazem in the prevention of coronary artery disease in heart transplant recipients. N Engl J Med 1993;328:164-70.
38. Taeymans Y, Theroux P, Lesperance J, Waters D. Quantitative angio- graphic morphology of the coronary artery lesions at risk for thrombotic occlusion. Circulation 1992;85:78-85.
39. Muller JE, Morrison J, Stone PH, Rude RE, Roser B, Roberts R, Pearle I, Turi ZG, Schneider JF, Serfas DH, Tate C, Scheiner E, Sobel BE, Henneken CH, Braunwald E. Nifedipine therapy for patients with threatened and acute myocardial infarction: a randomized. double- blind, placebo-controlled comparison. Circulation 1984;69:740-‘7

Kaplan and Manuck December 1994
American Heart Journal
40. The SPRINT Study Group. The Secondary Prevention Re-infarction Israeli Nifedipine Trial (SPRINT) II: results (abstract). Eur Heart J 1988;V(suppl 1):1350.
41. Waters D. Proischemic complications of dihydropyridine calcium channel blockers. Circulation 1991;84:2598-600.
42. Gao SZ, Alderman EL, Schroeder JS, Silverman JF, Hunt SA. Acceler- ated coronary vascular disease in the heart transplant patient: coronary arteriographic findings. J Am Co11 Cardiol 1988;12:334-40.
43. St. Gear FG, Pinto FJ, Alderman EL, Valantine HA, Schroeder JS, Gao SZ, Stinson EB, Popp RL. Intracoronary ultrasound in cardiac trans- plant recipients: in viva evidence of “angiographically silent” intimal thickening. Circulation 1992;85:979-87.
44. Loaldi A, Polese A, Montorsi P, De Cesare N, Fabbiocchi F, Ravagnani P, Guassi MD. Comparison of nifedipine, propranolol and isosorbide dinitrate on angiographic progression and regression of coronary arte- rial narrowings in angina pectoris. Am J Cardiol 1989$4:433-V.
45. Gottlieb SO, Brinker JA, Mellits ED, Achuff SC, Baughman KL, Trail1 TA, Weiss JL, Reits BA, Weisfeldt ML, Gerstenblith G. Effect of nifed- ipine on the development of coronary bypass graft stenoses in high-risk patients: a randomized, double-blind, placebo-controlled trial (ab- stract). Circulation 1989;84l(suppI Il):II228.
46. Waters D, Lesperance J, Craven TE, Hudon G, Gillam LD. Advantages and limitations of serial coronary arteriography for the assessment of progression and regression of coronary atherosclerosis: implications for clinical trials. Circulation 1993;87(suppl II):II38-47.
47. Misuno K, Miyamoto A, Satomura K, Kurita A, Arai T, Sakurada M, Yanagida S, Nakamura H. Angioscopic coronary macromorphology in patients with acute coronary disorders. Lancet 1991;337:809-12.
48. Potkin BN, Bartorelli AL, Gessert JM, Neville RF, Almagor Y, Roberts WC, Leon MB. Coronary artery imaging with intravascular higb- frequency ultrasound. Circulation 1990;81:1575-85.
Antiatherogenic effects of ,8-adrenergic blocking agents: Theoretical9 experimental, and epidemiologic considerations
Theoretical considerations and results from experimental studies in animal models suggest that long-term P-adrenergic blockade should be antiatherogenic. Some of these experimental results indicate that &blockers could inhibit atherogenesfs and thus prevent clinical events independently of any effects on blood pressure through concomitant reductions in heart rate, blood velocity and energy, endothelial permeability to lipoproteins, and the likelihood of plaque rupture. Any such independent inhibition of atherogenesis implies, in turn, that &blockers might be more desirable than alternative antihypertensive therapies in persons at high risk for atherosclerotic diseases. Results of the three major trials directly comparing &blockers to diuretics in the primary prevention of coronary heart disease among patients with hypertension were largely inconclusive. However, ancillary data from these and other trials are consistent in demonstrating that &adrenergic blockade is associated with anti-coronary heart disease effects and, thus, is perhaps antiatherogenic. A definitive evaluation of the antiatherogenic effects of ,&blockers is not forthcoming because no large clinical trials directly assessing the effect of these drugs on atherosclerosis have been done or are planned. (AM HEART J 1994;128:1316-28.)
Jay R. Kaplan, PhDF and Stephen B. Manuck, PhDar b Winston-Salem, N.C., and
Pittsburgh, Pa.
From the BDepartment of Comparative Medicine, Bowman Gray School of Medicine of Wake Forest University, and the bDepartment of Psychology,
&Adrenergic blocking agents (@-blockers) are widely
University of Pittsburgh. prescribed after myocardial infarction (MI) and for
Supported in part by grant Nos. MH-47234, HL-45666, and HL-40962 from the treatment of hypertension, angina pectoris, and the National Institutes of Health. arrhythmia.l Hypertension, which affects at least Reprint requests: Jay R. Kaplan, PhD, Department of Comparative Med- 25 % of adult Americans,2 is the most prevalent of the mine, Bowman Gray School of Medicine of Wake Forest University, Med- ical Center Blvd., Winston-Salem, NC 27X7-1040.
disorders for which @-blockers are indicated.3 How-
Copyright @ 1994 by Mosby-Year Book, Inc. ever, ,&blockers comprise only one of several classes OOOZ-8703/94/$3.00 + 0 4lOf89822 of drugs that are useful in treating hypertension;
1316