Caesarean Section - DiVA portaluu.diva-portal.org/smash/get/diva2:1134412/FULLTEXT01.pdf ·...
62
ACTA UNIVERSITATIS UPSALIENSIS UPPSALA 2017 Digital Comprehensive Summaries of Uppsala Dissertations from the Faculty of Medicine 1358 Caesarean Section Short- and long-term maternal complications SUSANNE HESSELMAN ISSN 1651-6206 ISBN 978-91-513-0041-2 urn:nbn:se:uu:diva-327934
Transcript of Caesarean Section - DiVA portaluu.diva-portal.org/smash/get/diva2:1134412/FULLTEXT01.pdf ·...
ACTAUNIVERSITATIS
UPSALIENSISUPPSALA
2017
Digital Comprehensive Summaries of Uppsala Dissertationsfrom the Faculty of Medicine 1358
Caesarean Section
Short- and long-term maternal complications
SUSANNE HESSELMAN
ISSN 1651-6206ISBN 978-91-513-0041-2urn:nbn:se:uu:diva-327934

Dissertation presented at Uppsala University to be publicly examined in FöreläsningssalenBiblioteket, Falu Lasarett, Falun, Friday, 6 October 2017 at 13:00 for the degree of Doctor ofPhilosophy (Faculty of Medicine). The examination will be conducted in Swedish. Facultyexaminer: Associate professor Jens Langhoff-Roos (Rigshospitalet Köpenhamn, Danmark).
AbstractHesselman, S. 2017. Caesarean Section. Short- and long-term maternal complications. DigitalComprehensive Summaries of Uppsala Dissertations from the Faculty of Medicine 1358.61 pp. Uppsala: Acta Universitatis Upsaliensis. ISBN 978-91-513-0041-2.
Caesarean section is a common major surgical procedure and long-term complications have notbeen fully investigated. By longitudinal population based register studies, based on Nationalhealth registers and medical data records, maternal complications after caesarean deliveryat subsequent labour (N=7 683), among extremely preterm births (N=406), and at remotegynaecologic surgery (N=25 354) were explored.
In Paper I, uterine closure was investigated in respect to uterine rupture in a subsequentdelivery after caesarean section. Uterine rupture occurred in 1.3 % of women with a previouscaesarean section. There was no increased risk of uterine rupture with single compared withdouble layers for closure of the uterus (adjusted Odds Ratio 1.17, 95 % CI 0.78-1.70). Modifiablerisk factors of uterine rupture in a trial of labour after caesarean section included induction oflabour and use of epidural analgesia.
In Paper II, maternal outcomes and surgical aspects of caesarean section in the extremelypreterm period were assessed. Maternal complications were more frequently reported inextremely preterm- compared with term caesarean delivery. No increase in short-term morbiditywas observed at 22-24 compared with 25-27 gestational weeks, but uterine corporal incisionswere performed more frequently (18.1 % vs. 9.6 %, p=0.02).
Furthermore, risk factors for abdominal adhesions after caesarean section and organ injuryin remote gynaecologic surgery were analysed (Paper III and IV). Numbers of prior caesareansections were the most important factor for formation of adhesions. Advanced maternal age,obesity, infection and delivery year 1997-2013 were factors associated with adhesions inconjunction with caesarean section. Organ injury occurred in 2.2 % of women undergoingbenign hysterectomy. A history of caesarean section increased the risk (adjusted Odds Ratio1.74, 95 % CI 1.41-2.15), but was only partly explained by the presence of adhesions. Theorgan affected depended on medical history; prior caesarean predisposed for bladder injury,prior bowel/pelvic surgery for bowel injury and endometriosis was associated with ureterinjury at time of hysterectomy. In conclusion; data from National health registers indicates thatcaesarean delivery is associated with long-term complications, although the absolute risk ofsevere complications for the woman is low.
Keywords: adhesion, caesarean section, extremely preterm birth, gynaecologic surgery, organinjury, uterine rupture, trial of labour
Susanne Hesselman, Department of Women's and Children's Health, Obstetrics andGynaecology, Akademiska sjukhuset, Uppsala University, SE-75185 Uppsala, Sweden.
© Susanne Hesselman 2017
ISSN 1651-6206ISBN 978-91-513-0041-2urn:nbn:se:uu:diva-327934 (http://urn.kb.se/resolve?urn=urn:nbn:se:uu:diva-327934)

Den mätta dagen, den är aldrig störst. Den bästa dagen är en dag av törst.
Karin Boye. I rörelse, Härdarna.


List of Papers
This thesis is based on the following papers, which are referred to in the text by their Roman numerals.
I Hesselman S, Högberg U, Ekholm-Selling K, Råssjö EB, Jons-
son M. (2015). The risk of uterine rupture is not increased with single- compared with double-layer closure: a Swedish cohort study. BJOG. Oct; 122 (11): 1535-41.
II Hesselman S, Jonsson M, Råssjö EB, Windling M, Högberg U. (2017) Maternal complications in settings where two-thirds of extremely preterm births are delivered by cesarean section. J Perinat Med. Jan 1; 45(1): 121-127.
III Hesselman S, Högberg U, Råssjö EB, Schytt E, Löfgren M, Jonsson M. (2017). Abdominal adhesions in gynaecologic sur-gery after caesarean section: a longitudinal population based register study. BJOG. June 17th. Epub before print.
IV Hesselman S, Högberg U, Jonsson M. (2017). Effect of remote cesarean delivery on complications during hysterectomy: a co-hort study. Am J Obstet Gynecol. Accepted manuscript 17 July. Epub before print.
Reprints were made with permission from the respective publishers.


Contents
Preface ........................................................................................................... 11
Introduction ................................................................................................... 12Caesarean Section ..................................................................................... 12
Historical notes, techniques and rates .................................................. 12Short-term complications of Caesarean Section ....................................... 14
Surgical techniques and complications ................................................ 15Preterm caesarean section ......................................................................... 15Long-term complications of Caesarean Section ....................................... 16
Abnormal location and invasion of placenta ....................................... 16Uterine rupture ..................................................................................... 17Adhesions ............................................................................................. 19
Rationale ........................................................................................................ 22
Aims .............................................................................................................. 23
Methods ......................................................................................................... 24Data sources .............................................................................................. 24
National Registers ................................................................................ 24Medical records .................................................................................... 25
Study populations and designs ................................................................. 25Paper I .................................................................................................. 25Paper II ................................................................................................. 26Papers III-IV ........................................................................................ 26
Main outcome measures ........................................................................... 27Paper I .................................................................................................. 27Paper II ................................................................................................. 27Paper III ............................................................................................... 27Paper IV ............................................................................................... 28
Statistical methods .................................................................................... 28Ethical considerations ............................................................................... 29
Summary of results ....................................................................................... 31Uterine closure and risk of uterine rupture (Paper I) ................................ 31Maternal complications after CS in the extremely preterm period (Paper II) ................................................................................................... 32Abdominal adhesions at gynaecological surgery following CS (Paper III) ................................................................................................. 33CS and risk of complications at subsequent hysterectomy (Paper IV) ..... 35
Discussion ..................................................................................................... 37General conclusions .................................................................................. 37Incidence of maternal complications ........................................................ 37Risk factors for maternal complications ................................................... 38
Surgical techniques .............................................................................. 38Maternal characteristics ....................................................................... 39Pregnancy and labour characteristics ................................................... 40Post-operative infection ....................................................................... 40Adhesions and complications .............................................................. 41
Methodological considerations ................................................................. 41Systematic errors .................................................................................. 42Random errors ...................................................................................... 43Strengths .............................................................................................. 44
Clinical implications ................................................................................. 44Future research ......................................................................................... 46
Summary in Swedish ..................................................................................... 47
Acknowledgements ....................................................................................... 49
References ..................................................................................................... 51
Abbreviations
AIP Abnormally Invasive Placentation AOR Adjusted Odds Ratio BMI Body Mass Index CI Confidence Interval CS Caesarean section CTG Cardiotocography GSEM Generalised Structural Equation Modelling ICD International Classification of Disease ICU Intensive Care Unit IUGR Intrauterine Growth Restriction MBR Swedish Medical Birth Register OR Odds Ratio PAR Swedish Patient Register RCT Randomised Controlled Trial TOL Trial Of Labour VBAC Vaginal Birth After Caesarean WHO World Health Organization


11
Preface
The word Caesarean section reflects more than a surgical procedure. For the resident on call, it is the first major intervention performed independently, but a caesarean section could also be a challenging surgical procedure for the experienced clinician. For the pregnant woman, caesarean delivery may be associated with relief or with sense of failure. It can be a life saving proce-dure, but at the same time it is associated with short- and long-term maternal morbidity. As a result, conflicting information about risks and benefits of caesarean delivery may be given in antenatal care, during labour and after labour. The risks and benefits are appreciated differentially between caregiv-ers and mothers but also between caregivers. The increased rate of ab-dominal deliveries worldwide during the last few decades have resulted in programmes aiming to reduce the rate of caesarean section. A particular situation is women in labour after caesarean. These are high risks deliveries, and most clinicians agree that efforts to avoid a first caesarean section are beneficial for future reproductive health. However, knowledge of adverse effects of caesarean delivery occurring re-mote years after childbirth is limited. The following papers aim to investi-gate maternal complications after caesarean section, with emphasis on long-term.

12
Introduction
Caesarean Section Historical notes, techniques and rates Caesarean section (CS) is the most common abdominal surgery performed in women at present. The rate of caesarean deliveries varies substantially be-tween nations and healthcare facilities but continues to rise worldwide [1, 2].
Historically, CS was performed post-mortem, according to lex regia, a Roman law forbidding burial of an undelivered woman. Caesarean delivery as a surgical procedure is described in the 15-16th century, but some scepti-cism might be appropriate when successful stories of women undergoing multiple caesarean deliveries are mentioned. In the 19th century, the mortali-ty rate after abdominal delivery was around 75 %. The introduction of clos-ing the uterus, advocated by Max Sanger in 1882, and the use of aseptic technique around 1870, were both important factors to reduce maternal mor-tality [3]. Different CS techniques have been used and described over the years. In a classical CS, midline vertical incisions of the skin and the cor-poral part of the uterus are performed. In 1926, Munro Kerr proposed a transverse incision of the lower uterine segment, which proved to be superior to a corporal incision, with reduced maternal mortality and lower risk of uterine rupture in a subsequent pregnancy [4]. The transverse incision of the uterus did not gain acceptance until 1949 and was either combined with a midline incision of the skin or a low transverse incision- the Pfannenstiel-Kerr method. In these techniques, both visceral and parietal peritoneum lay-ers were closed, but later clinical studies suggested that closure was not mandatory for peritoneal healing [5, 6]. In 1995, Stark and colleagues at the hospital Misgav-Ladach introduced a new CS technique, described in the paper by Holmgren et al. [7]. A transverse skin incision 5 cm above the symphysis, proposed by Joel-Cohen, was combined with blunt division of tissues, single layer closure of the uterus and non-closure of the peritoneal layers. The new CS technique, concomitantly referred to as Stark, Misgav-Ladach or Joel-Cohen technique, was further modified with a lower skin incision level and was introduced in Sweden from 1996-1999 [7-9]. The optimal surgical technique and the optimal rate of CS are still debated. The previously advocated optimal rate of CS of 10-15 % [10] was replaced
13
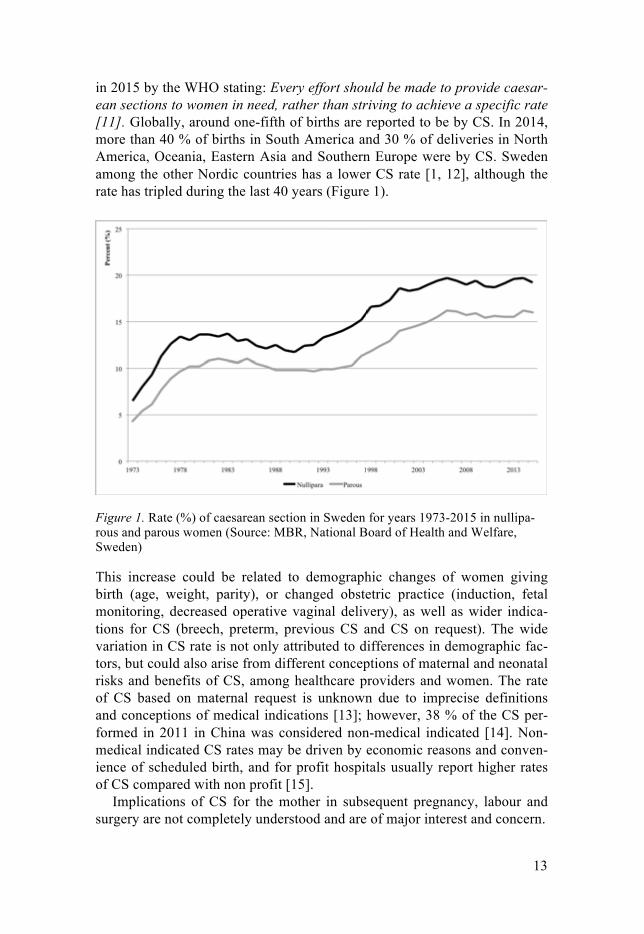
in 2015 by the WHO stating: Every effort should be made to provide caesar-ean sections to women in need, rather than striving to achieve a specific rate [11]. Globally, around one-fifth of births are reported to be by CS. In 2014, more than 40 % of births in South America and 30 % of deliveries in North America, Oceania, Eastern Asia and Southern Europe were by CS. Sweden among the other Nordic countries has a lower CS rate [1, 12], although the rate has tripled during the last 40 years (Figure 1).
Figure 1. Rate (%) of caesarean section in Sweden for years 1973-2015 in nullipa-rous and parous women (Source: MBR, National Board of Health and Welfare, Sweden)
This increase could be related to demographic changes of women giving birth (age, weight, parity), or changed obstetric practice (induction, fetal monitoring, decreased operative vaginal delivery), as well as wider indica-tions for CS (breech, preterm, previous CS and CS on request). The wide variation in CS rate is not only attributed to differences in demographic fac-tors, but could also arise from different conceptions of maternal and neonatal risks and benefits of CS, among healthcare providers and women. The rate of CS based on maternal request is unknown due to imprecise definitions and conceptions of medical indications [13]; however, 38 % of the CS per-formed in 2011 in China was considered non-medical indicated [14]. Non-medical indicated CS rates may be driven by economic reasons and conven-ience of scheduled birth, and for profit hospitals usually report higher rates of CS compared with non profit [15].
Implications of CS for the mother in subsequent pregnancy, labour and surgery are not completely understood and are of major interest and concern.

14
Short-term complications of Caesarean Section The reported incidence of complications after CS varies by method of col-lecting data: time to follow-up, population studied and definitions of compli-cations used. A limited number of randomised controlled trials (RCT) have been performed for breech presentation and report a small increased risk of short-term maternal morbidity with planned CS compared with planned vag-inal birth [16]. However, evidence of maternal complications related to CS is mostly based on observational studies, investigating the effect of the actual mode of delivery and not the intended mode. The overall complication rate after CS has been estimated to occur in one-third of patients and suggests that emergency CS carries the highest risk [17, 18]. In a population based register study, risk of severe obstetric haemorrhage, defined as blood loss >1000 ml, was two-fold after elective CS and three-fold following emergen-cy CS compared with vaginal delivery [19]. In a prospective cohort of 106,546 deliveries, severe maternal morbidity was assessed to be two-fold with CS compared with vaginal delivery and with four-fold increased risk of hysterectomy. In this publication, emergency CS compared with elective CS was not associated with higher maternal morbidity [20]. Post-operative in-fection following CS, including febrile morbidity requiring antibiotic treat-ment, has been reported in 7-17 % in retrospective and prospective studies [17, 21-23], but is reduced by 60 % with prophylactic antibiotics [24]. Post-partum thromboembolism is a major complication with five-fold increased risk after CS compared with vaginal delivery and affects at least 0.23 % [23, 25].
The interpretation of observational studies of complications is confound-ed by the indication for CS. Complications recorded after CS may result from underlying maternal conditions resulting in a CS, and not from the procedure per se. Preeclampsia increases the risk of haemorrhage and thromboembolism [17, 25]. Chronic hypertension, diabetes and multiple births are all risk factors for severe sepsis [26]. Dystocia and high birth weight are related to uterine atony and blood loss [27]. According to a pro-spective observational study of 2,751 caesarean deliveries, intra-operative complications including lacerations of cervix, vagina and bladder increased with advanced cervical dilatation [27, 28], and a second stage CS has been associated with higher risk of intensive care unit (ICU) admission, blood transfusion and infectious morbidity [29-31]. Increased maternal morbidity is seen with repeated CS [32] and preterm CS [17, 33], which could be relat-ed to the indication of CS or the technical difficulties encountered in these cases.
CS performed before labour is usually regarded as elective but includes both CS with emergent obstetric indications such as placental abruption and severe preeclampsia. CS after onset of labour includes emergent procedures, with different indications and maternal conditions, which make risk esti-

15
mates between different categories of CS imprecise [13]. Moreover, the lack of strict definitions of maternal outcomes limits interpretations and compari-sons between studies.
Surgical techniques and complications Observational studies of the Joel-Cohen based technique demonstrate re-duced risk of per- and post-operative complications, with less post-operative pain and infection and faster maternal recovery [34, 35]. Decreased blood loss, shorter duration of surgery and time to deliver the baby has been re-ported in randomised controlled trials, whereas the effect on infectious mor-bidity diverges [8, 9, 36, 37]. A Cochrane report from 2014 concluded that single layer closure of the uterus compared with double layer closure de-creases blood loss but not febrile morbidity [38]. Another Cochrane review, investigating the effect of peritoneal closure, concluded that non-peritoneal closure compared with closure of both peritoneal layers reduces duration of surgery and hospital stay but does not affect the rate of post-operative infec-tion [39]. The CORONIS trial (N=15,935) found no difference in comparing sharp vs. blunt division of tissues, single or double-layer closure of the uter-us, suture material or peritoneal closure and non-closure in respect to mater-nal infection, re-operation or blood transfusion [40]. The Caesar trial (N=3,033) investigated maternal infection in respect to uterine closure, peri-toneal closure and use of subrectus drain and found no technique to be supe-rior to the other, but duration of surgery was shorter with non-peritoneal closure (mean 2.4 minutes, 95 % CI 1.3-3.6 minutes) [21].
Preterm caesarean section The rate of preterm births, defined as birth before 37 completed gestational weeks, is estimated to 5 % in northern Europe and to 12 % in North America and constitutes of both spontaneous and iatrogenic births [41]. Extreme pre-term birth (gestational age 22-27 weeks) constitutes around 5 % of all pre-term births and is associated with risk of adverse maternal complications, independent of the mode of delivery [42].
Preterm, compared to term, CS has been associated with higher propor-tion of maternal complications, such as increased blood loss, hysterectomy, sepsis, thrombosis and post-operative hematoma [17, 27, 33], but low rates of serious maternal complications have also been reported in selected popu-lations [42, 43]. In a retrospective cohort of 540 extremely preterm deliver-ies, adverse maternal outcome defined as maternal death, admission to ICU, sepsis, hysterectomy, transfusion, postpartum haemorrhage, surgical injury, reoperation, endometritis or re-admission to hospital, occurred in one-fifth of delivered women, but CS did not increase the risk (aOR 0.67, 95 % CI 0.40-

16
1.12) [42]. An underdeveloped lower segment of the uterus or malpresenta-tion of the fetus may lead to a corporal uterine incision, which is performed in 20-56 % of the extremely preterm CS, and has been associated with in-creased blood loss and infection [33, 42-45]. In subsequent pregnancy, inci-sions extending into the corpus increase the risk of uterine rupture [46], and data also suggest an increased risk of rupture after a low transverse CS per-formed at 20-26 weeks of gestation [47, 48].
Sweden, with about 400 extremely preterm births annually, has a high rate of perinatal interventions, including delivery by CS at gestational age 22-26 [49]. According to a guideline proposed by an expert group from the Swedish Neonatal Society and Swedish Society of Obstetrics and Gynaecol-ogy 2015, caesarean delivery on fetal indication is recommended at 24 weeks of gestation and should be considered at 23 gestational weeks [50]. The American College of Obstetricians and Gynecologists and the Society for Maternal Fetal Medicine recommend CS on fetal indication from 25 ges-tational weeks and that decision of CS on fetal indication should be individ-ualised at lower gestational weeks [51].
The restricted number of prospective trials comparing planned CS and planned vaginal delivery for preterm births limits conclusions about maternal and neonatal risks and benefits of CS to observational studies [52]. Results are conflicting and prone to selection bias, but CS may be beneficial for the growth restricted infant and breech presentations [53-55].
Increased survival rates among infants who are delivered extremely pre-term [49, 53, 56], and a potential benefit of CS for the neonate raise the question about maternal complications of abdominal deliveries performed extremely preterm.
Long-term complications of Caesarean Section In a subsequent pregnancy and delivery, abnormal placentation [32, 57], uterine rupture [46, 58] and adhesions associated with intra-operative diffi-culties [59] are all feared complications of previous CS, with major impact on maternal health.
Abnormal location and invasion of placenta Placenta previa and abnormally invasive placentation (AIP) are strongly associated with prior CS and increase risks of haemorrhage, peripartum hys-terectomy and maternal mortality [32, 57]. Placenta previa, when the placen-ta is at the margin or covers the cervix inlet, occurs in 10 % of women with a history of four or more CS compared with 0.23 % of women without prior CS. AIP results from deficient decidua formation, when the placenta villi morbidly attach or invade the myometrium. In a Nordic population based

17
study, the prevalence of AIP was estimated to 1 out of 720 women with prior CS, and the seven-fold risk after one prior CS rose dramatically to a 56-fold increased risk of AIP after three or more CS [57]. The risk of placenta accre-ta and peripartum hysterectomy have been thoroughly investigated by Silver et al., and rates increases with each repeat CS [32]. Corporal incision and pre-labour CS have been associated with increased risk of AIP [60, 61], whereas single compared with double layer closure of the uterus, according to a case-control study, did not influence the risk [62].
Myometrium disruption after CS may also result in implantation of the conceptus in the scar, resulting in a scar pregnancy.
Uterine rupture Uterine rupture, which is full disruption of the uterine wall in labour, is an obstetric emergency associated with high maternal and neonatal morbidity, and the main risk factor in developed countries is a previous caesarean de-livery [46, 58].
Incidence of uterine rupture The incidence of uterine rupture depends on definition, population and study method used, and there is great variation of reported rates [63]. The rate is influenced by the validity of diagnosis in national registers, and both over- and underreporting is observed [64, 65].
In the Nordic countries, uterine rupture has been reported to occur in 0.06 % of all deliveries [66, 67]. Rupture of an unscarred uterus is a rare event, affecting 0.005 % [67]. The main risk factor for uterine rupture is a previous CS, and uterine rupture occurs mainly after onset of labour [63]. The rate of uterine rupture in women attempting a trial of labour (TOL) after previous low transverse CS has been estimated from 0.21-1.5 %; the variation may reflect that selection of patients and management of TOL differ between settings [46, 63, 68-72]. Apart from population studied, different definitions of uterine rupture will have an effect on reported rates [63]. Usually, uterine rupture refers to a full thickness disruption of the uterine wall [73], but cases with any separation of the uterine wall associated with clinical symptoms could also be included [74]. Associated symptoms help to distinguish rupture from asymptomatic dehiscence of the uterine scar, which has little impact on maternal and neonatal outcome [46, 75].
Risk factors of uterine rupture Risk of rupture of the uterine scar might depend on the integrity and strength of the scar and the strain on the scar during labour. The risk of uterine rup-ture in TOL is closely associated with previous modes of births. In a trial of labour, the risk is three-fold in women with ≥ 2 prior CS compared with one prior CS, whereas a prior vaginal delivery lowers the risk of uterine rupture

18
substantially [71, 76, 77]. Induction of labour, especially with the use of oxytocin and prostaglandins, has been identified as a risk factor for uterine rupture in women with a uterine scar [46, 71]. Prostaglandins have been associated with a two- to six-fold increased risk of rupture compared with spontaneous onset of labour [46, 69, 72, 75, 78], but these findings have been suggested to be confounded by its indication with an unripe cervix and thus longer duration of labour [79]. Advanced maternal age both at index CS and subsequent labour, high birth weight, postpartum fever and short deliv-ery interval are also reported risk factors for uterine rupture in a subsequent TOL [70, 71, 75, 80-83].
Surgical techniques and risk of uterine rupture The strength of the scar may be result of the surgical technique used for uter-ine closure, and single and double layer have been studied in respect to uter-ine rupture. Results from retrospective observational studies are conflicting. Bujold et al. have reported a four-fold increased risk of rupture after single layer closure compared to double layer closure, but a meta-analysis from 2011 including nine studies (one RCT, six cohort and two case control stud-ies) found no increased risk [73, 84]. The largest RCT, investigating effects of CS technique is the CORONIS trial [40]. In the recently published 3-year follow-up, the risk of uterine rupture according to single or double layer closure of the hysterotomy did not differ. However, there was a lack of pow-er to detect differences due to the low incidence of subsequent pregnancies (n=4,992). Further, two-thirds were delivered with a pre labour CS; conse-quently, the risk of rupture was low [85].
In attempt to overcome the methodological problems, measurement with ultrasonography of lower uterine thickness after CS has been investigated. Disruption of the anterior wall and a visible scar defect increases with num-ber of caesarean deliveries, but the incidence proportion is high, ranging from 61 % after one CS to 100 % after > 3 CS [86], which limits the clinical utility. Myometrium thickness has been used in follow-up studies of uterine closure with conflicting results [87] [88]. To set cut-off values of antenatal myometrium thickness for predicting uterine rupture has proved to be hard [89]. The lower uterine segment thickness decreases with gestational length and has been measured to 2.3 mm at term, in women without a prior CS [90]. A meta-analysis, including 21 studies, concluded that there was a strong negative predictive value of myometrium thickness 2.1-4.0 mm and a strong positive predictive value of 0.6-2.0 mm for diagnosing defects of the uterine wall in CS.
Due to the rare outcome and presumably multifactorial cause of uterine rup-ture, long-term follow-up studies of uterine closure and risk of uterine rup-ture has posed methodological problems, and the optimal surgical technique is still debated.

19
Clinical signs and symptoms of uterine rupture Efforts to improve safety of vaginal delivery after CS have focused on the identification of risk factors for uterine rupture, and few studies have exam-ined the actual course of labour or aspects of intrapartum management in cases of rupture [91, 92]. Recognition of clinical signs of uterine rupture is challenging due to the lack of specific symptoms; moreover, most signs do not precede but follow uterine rupture. Clinical signs include fetal heart rate abnormalities, abdominal pain, vaginal bleeding, haematuria, loss of en-gagement of the presenting fetal part and maternal cardiovascular collapse [93-96]. In a case control study, pathological CTG occurred in 77 % of cases with uterine rupture but was also present in 53 % of labours without rupture [95]. The most common CTG patterns in uterine rupture were severe varia-ble decelerations and terminal fetal bradycardia indicating overt rupture. Arrest of labour is commonly reported in cases with uterine rupture [92], and augmentation with oxytocin poses a risk [72, 78, 91, 97], but these features can also be present in labours without rupture. Despite the high-risk proce-dure, there are no specific protocols of augmentation of labour or surveil-lance of women undergoing TOL after caesarean in Sweden.
Adhesions Incidence and clinical burden of adhesions Intra-abdominal adhesions are fibrous structures formed between abdominal organs, peritoneum and the abdominal wall after inflammation caused by surgery, infection or chemical irritation and may develop in more than 90 % after laparotomy [98, 99]. In epidemiologic studies, burden of adhesions after different types of surgery has been evaluated by rates of re-admissions, diagnosis or surgical procedures that could be attributed to adhesions [100, 101]. Abdominal adhesions are associated with small bowel obstruction and accounts for 65-75 % of cases requiring surgery [99, 102]. Morbidity from post-surgical adhesions is closely related to type of index surgery; small bowel obstruction has been reported in only 0.5/1000 after CS compared with 15.6/1000 after abdominal hysterectomy [103]. In a Swedish register and populations based study, Andolf et al. reported a higher incidence of bowel obstruction and symptomatic adhesions, affecting 2.2/1000 women with previous CS [101]. Adhesions have also been related to subfertility and pelvic pain and were formerly an indication of gynaecologic adhesiolysis [59, 104]. Following CS, subfertility has been reported in 3 % and chronic pain in 6 % of women [85].
Even if severe morbidity after CS occurs infrequently, adhesions may in-crease intra-operative complications in subsequent surgery. Pelvic adhesions are estimated to develop in one- to two-thirds of women who delivered by CS, and may contribute to bladder- bowel and ureter injuries, longer operat-

20
ing times, blood loss and delayed delivery in repeat CS [105-107]. At time of subsequent gynaecologic surgery, prior caesarean delivery has been associ-ated with increased risk of surgical complications [108-110] such as bladder injury, haemorrhage and conversion from minimal invasive routes to lapa-rotomy, but studies are restricted in number and participants.
Risk factors for adhesions Number of previous surgeries influences the adhesion formation. Repeat CS is associated with more and dense pelvic adhesions and requires adhesiolysis more often [106, 111, 112]. In a prospective study of 1,000 laparoscopic procedures, a low rate of adhesions following laparoscopy was observed, but intestinal adhesions increased for each number of surgery.
Closure of the peritoneum after CS has been studied with respect to adhe-sion formation, and results are conflicting. In a systematic review of obser-vational studies, Shi et al. concluded that a modified Joel Cohen CS with peritoneum closure was associated with fewer adhesions than non-closure [113]. However, in a RCT with 97 women followed up with second look at a repeat CS, no difference in adhesion rate according to peritoneal closure was observed [114]. The large CORONIS study found no evidence of an effect of peritoneal closure on adhesion related symptoms [85].
In a secondary analysis from a prospective cohort, Blumenfeld et al. ob-served that bladder adhesions occurred more frequently after single com-pared with double layer closure of the uterus [115].
Apart from surgical history and technique, predisposing factors for post-operative adhesions may be related to medical history and individual suscep-tibility [116-119]. Pelvic inflammatory disease caused by infections and/or endometriosis is strongly associated with the occurrence of adhesions [118]. The gold standard for diagnosis of endometriosis is laparoscopy with direct visualisation of abdominal lesions followed by histopathology examination. [120]. Endometriosis has been reported in one-fifth of women undergoing hysterectomy because of chronic pelvic pain [120]. Knowledge of obstetric factors for post-operative adhesions after CS is lim-ited. In a retrospective study of 160 patients, gestational weeks, pregnancy complications, emergency vs. elective CS or infection at first CS did not differ between women with and without adhesions at repeat CS [116]. Moro et al. investigated 308 women with a history of CS, prospectively with ab-dominal and transvaginal ultrasonography and after exclusion of women with prior pelvic surgery other than CS, 40 % of women had adhesions. Post-operative infection after CS posed over ten-fold risk of abdominal wall adhesions [121]. As a repeat surgical procedure is required, there are methodological difficul-ties to assess the rate of adhesions resulting from different types of surgeries

21
and techniques. As a result, study populations are often restricted to small number or to symptomatic women.

22
Rationale
Randomised controlled trials that investigate surgical techniques and rare outcomes requiring long-term follow-up are hard to perform, and observa-tional studies must contribute to evidence. The Swedish National registers, kept by the National Board of Health and Welfare, are valuable resources for large-scale register-based studies [122], and by combining registers a variety of research questions could be addressed. Uterine rupture is a rare but severe complication, and the main risk factor is a previous CS. The high number of CS surgeries performed worldwide puts many women at risk, and identification of potential modifiable risk factors, such as surgical technique, is of importance. Long-term follow-up studies of uterine closure and risk of uterine rupture have posed methodological prob-lems due to both limited number of participants and outcome, and the ques-tion remains unanswered. The optimal mode of delivery at extreme preterm birth is complex, and the risk and benefit for the mother and the infant might diverge. The restricted number of participants and recruitment failure of prospective trials compar-ing planned CS and planned vaginal delivery for preterm birth limits draw-ing conclusions about maternal and neonatal risks to observational trials. Increased survival rates among neonates delivered extremely preterm and a potential benefit of CS for the infant raise the question about complications for the mother. Another knowledge gap that requires long time to follow up is formation of abdominal adhesions after CS, and studies are limited in number and partici-pants. National health registers combined with National quality registers, which contain detailed data of gynaecologic surgery, give an opportunity to investigate the association between obstetric risk factors and adhesions as well as complications in gynaecologic surgery on large scale.

23
Aims
The overall aim with this thesis is to explore maternal complications follow-ing caesarean section, with focus on long-term complications. The specific objectives of the studies are: • To compare single with double layer closure of the uterus at caesarean
section, for the risk of uterine rupture in a subsequent trial of labour (Pa-per I)
• To describe the maternal short-term outcomes after CS in the extremely preterm period (Paper II)
• To assess the incidence of abdominal adhesions at gynaecological sur-gery, according to previous mode of delivery and to investigate obstetric factors associated with development of adhesions (Paper III)
• To investigate associations between history of caesarean delivery and
complications at time of hysterectomy (Paper IV)
24
Methods
Table 1. Study populations and designs
Data sources National Registers The Swedish Medical Birth Register (MBR) was founded in 1973 and pro-vides information about pregnancy, labour and perinatal outcome. The regis-ter is validated and covers more than 98 % of all deliveries in Sweden [123, 124]. Information is prospectively collected from standardised prenatal, ob-stetrical and neonatal medical records. It includes demographic data of the mother, previous pregnancies and modes of delivery, medical conditions and medication before and during pregnancy, onset and mode of delivery, fetal presentation, blood loss, analgesia and anaesthesia used and maternal diag-nosis according to the International Classification of Diseases (ICD) [125]. Information provided from the neonatal care includes birth weight, body length and head circumference of the infant, single or multiple birth, gesta-tional week, Apgar score and diagnoses of the neonate by ICD codes. The Swedish Patient Register (PAR) [126] was launched in 1964, but com-plete coverage did not begin until 1987. The register includes nearly all in-patient diagnoses and surgical procedures by codes from ICD and Classifica-tion of Surgical Procedures. The proportion of valid diagnoses in the PAR is considered high in patients with severe disease and among patients with iatrogenic complications [127].
Study
Design Subjects Study period
Source
I Cohort 7,683 in a trial of labour after a previous caesarean section
2001-2009
National health registers and medical records
II Case-Referent
647 deliveries in 22-27 weeks of gestation 2001-2012
Medical records
III Cohort 15,479 women undergoing benign pelvic surgery with prior delivery 1973-2013
2000-2014
National health and quali-ty registers
IV Cohort 25,354 women undergoing hysterectomy with prior delivery 1973-2013
2000-2014
National health and quali-ty registers

25
The Quality register of gynaecologic surgery has collected information of indication, surgical technique, results and complication rates in gynaecologi-cal surgery since 1997. Information in this register is retrieved from two different sources (Gynop and GKR register) and covers 75 % of all clinics offering gynaecologic surgery in Sweden.
Data are collected by patient questionnaires (pre operatively, at eight weeks and one year after the surgery) [128]. Information of the surgical pro-cedure and per- and post-operative complications is retrieved from standard-ised tick boxes filled in by the surgeon and the attending physician.
Medical records Obstetrix® (Siemens AB, Healthcare) is a medical data record system for antepartum care, labour and postpartum period, used in more than 90 % of maternity wards in Sweden today. A standardised surgical template of CS was introduced in 2001, and a detailed surgical report is constructed from check-boxes, with information about station of fetal presenting part, extrac-tion of fetus and placenta, suture material and techniques of uterine-, perito-neal and fascia closure. Cosmic® (Cambio Healthcare Systems) is the medical data record system at Uppsala University Hospital, which provided information for part of the study population in Paper II. Data were retrieved with a predefined protocol including information about the woman’s medical and obstetric history and the actual pregnancy.
Study populations and designs Paper I A cohort study including 19,604 nulliparous women who delivered by CS at 23 maternity units in Sweden was conducted. Centres of recruitment were all units that were users of the data record system Obstetrix® during the time period (23 out of 46). In the second pregnancy, 7,683 women attempted a trial of labour at 42 different maternity units in Sweden and defined the study population.
Data in the Obstetrix® database were linked to the MBR and PAR by each woman’s unique personal identity number. The research database contained information about the women´s first delivery during the years 2001 to 2007 and second delivery between 2001 and 2009.
The MBR provided maternal, pregnancy, labour and neonatal data from first and second delivery based on standardised check boxes and diagnosis

26
according to ICD-10. The Obstetrix® database provided information about uterine closure dichotomized into single or double layers.
Paper II In this observational study, data were collected from medical charts of ex-tremely preterm deliveries at Uppsala University Hospital and Umeå Univer-sity Hospital (n=647) for the years 2001-2012. The hospitals support a pro-active management of extremely preterm births in Sweden, including obstet-ric and neonatal interventions from 22 weeks of gestation. CS procedures < 24 weeks of gestation were restricted to maternal indications at Uppsala during the study period. Detailed information about the CS was collected, and indication of CS was regarded as fetal (breech or transverse presenta-tion, fetal distress and IUGR) or maternal (preeclampsia, abnormal placenta-tion and abruption). If coexisting maternal and fetal conditions prevailed, indication was regarded maternal. Gestational length was divided into two strata, 22-24 (n=105) and 25-27 (n=301) completed gestational weeks for extremely preterm CS. A referent group was retrieved from the cohort of nulliparous women from study I with CS performed at term (n=16,907).
Papers III-IV A cohort of 44,455 women undergoing benign hysterectomy and/or adnexal surgery at 46 different units in Sweden during the years 2000-2014, with a previous delivery during 1973-2013, was identified in the Gynop register. Data retrieved from the register were aggregated with MBR and PAR through the woman’s personal identification number.
In Paper III, women with any history of other abdominal surgeries than CS, bowel or pelvic inflammatory disease and endometriosis were excluded. Twelve units reporting in GKR did not provide information about adhesions (n= 5,584). The study population consisted of 15,479 women undergoing hysterectomy and/or adnexal surgery. Data from Gynop included demo-graphic variables at surgery and details of the surgical procedure. From MBR, information regarding prior mode of delivery, number of CS, maternal pregnancy and labour characteristics were retrieved. Year of first CS was divided into before and after 1997 to reflect the introduction of the modified Joel-Cohen technique and transition in Sweden [7-9]. Indications of caesare-an section and information about post partum complications, retrieved from diagnosis according to the ICD codes, were restricted to deliveries from 1987. A composite variable “postpartum infection” included intra partum fever, puerperal sepsis or post-operative uterine or wound infection, diag-nosed in the MBR or PAR until six weeks after delivery.
27
The study population in Paper IV included all women, regardless of prior medical and surgical history, undergoing hysterectomy (N= 25,354). A per-sonal history of: CS (n=5,152), other bowel/pelvic surgery (n=11,376) and/or endometriosis (n=2,116) visualised or diagnosed at time of the gynae-cologic surgery were considered as main conditions predisposing for adhe-sions. Route of hysterectomy was divided into abdominal or minimally inva-sive which included laparoscopic and vaginal approaches.
Main outcome measures Paper I Cases with uterine rupture in the second delivery were identified in the MBR by the diagnosis codes: O71.0 or O71.1, according to ICD 10.
For identified cases with uterine rupture, full surgical reports were ob-tained from the maternity departments. Uterine rupture during labour was defined as a full thickness separation of the uterine wall or when a separation covered by the visceral or bladder peritoneum presented with clinical symp-toms such as excessive vaginal bleeding, fetal heart rate abnormalities, ab-dominal pain or palpable fetal part through the abdominal wall. The diagno-sis was confirmed during caesarean section or during laparotomy performed immediately after delivery and, in one case, by abdominal ultrasound that revealed an abdominal haemorrhage and a scar defect of the uterus.
Paper II Multiple maternal outcomes were assessed: the composite ‘post-operative’ infection included sepsis, wound-, uterine- and urinary tract infection. A major maternal complication was defined as blood loss ≥2000 ml, sepsis, deep hematoma, re-operation or thromboembolism. Type of uterine incision was divided into low transverse and other types (classic-, T or J shaped- or low vertical incision).
Paper III The main outcome was adhesions in the surgical field. Presence of adhesions was assessed and filled in by the surgeon as yes, no, mild, moderate or ex-tensive by standardised check boxes at time of the gynaecologic procedure. Occurrence of adhesions was dichotomised into yes or no.

28
Paper IV The main outcome was organ injury at hysterectomy. Organ injuries includ-ed mild and severe bladder-; vascular-, bowel- and ureter injuries identified per-operatively or during the hospital stay and detected ureter injuries within eight weeks post-operatively. Information was retrieved from Gynop, by standardised check boxes, which information of blood loss, duration of sur-gery and post-operative infection and hematoma reported by the caregiver either at discharge or at eight weeks follow-up.
Statistical methods
Measures of disease occurrence The average risk for a group of people of a diseases or health event to occur could be referred to as an incidence proportion.
Descriptive measures in the studies included absolute and relative fre-quencies (Papers I-IV). Continuous data were checked for normal distribu-tion by normality plots and presented as means ± standard deviation (SD) and medians with 10th-90th percentiles when appropriate. In Paper III, differ-ences were tested with Welch’s t-test because of unequal sample sizes and variances and by non-parametric test in Paper IV.
Continuous variables were further categorised, and differences in propor-tions between groups were investigated with Pearson´s Chi2 test (Papers I-IV). A p-value <0.05 was considered statistically significant.
Logistic regression and point estimates In the following papers, the term risk and risk factor refers to an increased incidence of the outcome after exposure. To control for potential confound-ers, associations were investigated using logistic regression and presented as crude and adjusted risk estimates, Odds Ratios (OR) with 95 % Confidence Intervals (CI). In Paper I, factors from the first and second deliveries and uterine rupture were analysed, and significant factors retrieved from bivari-ate analysis and logistic regression were included in the models. In Paper III, factors from the time point of caesarean delivery and presence of adhesions at subsequent gynaecologic surgery were adjusted for number of CS. Paper IV investigated associations of prior CS, other abdominal surgery and endo-metriosis with complications at hysterectomy. In the multiple logistic regres-sion model, factors with plausible biologic associations with the outcome were included.
29
Heterogeneity and clustering As more than one individual was recruited from the same unit (hospital), observations for different variables might cluster. The independence assump-tion of observations in regression analysis is then violated, hence necessitat-ing multilevel regression to be conducted. Multi-level logistic regression with mixed-effect models were performed in order to rule out heterogeneity in Paper I and control for observed heteroge-neity between hospitals in Papers III-IV.
Generalised structural equation modelling (GSEM) and mediation effects In Paper III, a GSEM was performed to explore the causal pathways leading to formation of adhesions and to estimate size effects of mediation between explanatory variables. Factors, selected with the means of logistic regression and with plausible biologic associations with adhesions, were used in the model.
In Paper IV, the direct effect of prior CS, other abdominal surgery and endometriosis on occurrence of organ injury in subsequent hysterectomy and the proportion mediated by presence of adhesions was investigated by GSEM.
Ethical considerations Risk and benefit of the importance of the research question and the integrity of individuals in the research databases were assessed and regarded as being balanced. The Regional Ethical Board at Umeå University approved study I. The Re-gional Ethical Board at Uppsala University approved studies II-IV. Data for studies I, III and IV were aggregated and delivered from the Swe-dish National Board of Health and Welfare without personal identification numbers. The Swedish National Board of Health and Welfare keep the key of personal identification number for three years. Patients included in the quality register of gynaecologic surgery Gynop are informed about the regis-ter and have the right to decline participation. Paper II required access to medical records by personal identification num-bers. Data from the medical records were kept in a database without personal identification, and the key of personal identification number was kept sepa-rately in a key-locked computer.

30
Personal identification was not possible, neither during data analysis or fol-lowing publication of data.

31
Summary of results
Uterine closure and risk of uterine rupture (Paper I) Uterine rupture during labour occurred in 103 (1.3%) of the women with a previous CS. There were 70 anatomically complete ruptures and 33 incom-plete ruptures. There was no significant difference in the rate of uterine rup-tures when single layer closure was compared with double layer closure of the uterus. Non-modifiable risk factors from the first delivery for uterine rupture in a subsequent labour included maternal age ≥ 35 years and mater-nal height ≤ 160 cm. No effect was seen of BMI, short delivery interval or type or indication of first CS. Delivery of an infant large for gestational age and infectious morbidity from the first CS increased the risk of uterine rup-ture about two-fold in a subsequent labour.
In the trial of labour after caesarean, vaginal delivery succeeded in 71 % of cases. The majority had a spontaneous onset of labour, and 1,242 (16 %) women were induced. Modifiable risk factors for uterine rupture in the se-cond delivery included induction of labour and use of epidural analgesia. Gestational diabetes and birth weight ≥ 4500 g increased the risk.
Table 2. Factors from first and second delivery associated with uterine rupture.
Exposure Outcome (uterine rupture)
N=7,683 n=103 aOR’ 95 % CI First delivery Single layer closure 2,589 38 1.17 0.78-1.76 Age ≥35 (years) 672 15 2.08 1.19-3.63 Maternal height ≤160 (cm) 1,595 32 1.69 1.11-2.58 Large for gestational age 214 7 2.46 1.12-5.40 Infection 326 9 2.03 1.01-4.08 Second delivery (TOL) Induction 1,242 27 1.71 1.09-2.68 Epidural analgesia 3,698 68 1.99 1.31-3.02 Birth weight ≥ 4500 g 314 9 2.11 1.05-4.26
* adjusted for explanatory variables at first or second delivery

32
A secondary analysis with review of labour records including partograms and CTG tracings for cases with uterine rupture (N=103) identified in study I was performed [129]. The aim was to describe clinical signs preceding uter-ine rupture, and maternal as well as neonatal outcomes in relation to the stage of labour at which rupture was diagnosed. The most frequent clinical signs anticipating uterine rupture were fetal dis-tress (65 %), abdominal pain (56 %) and protracted labour (54 %). Vaginal bleeding, palpable scar defect or contraction ring were less frequently re-ported. When uterine rupture was diagnosed at the second stage of labour, loss of station of the fetal head and cessation of contractions were more common, indicating overt rupture. CTG tracings were available in half of the cases. The most common pathological CTG pattern before diagnosis was prolonged decelerations and bradycardia. All women with uterine rupture had operative deliveries. Operative vaginal delivery failed in 10 out of 16 cases. There were no maternal deaths. Eight women had blood loss > 2000 ml and two underwent peripartum hysterectomy. Bladder injury occurred in 7 out of 103 women with uterine rupture. Diagnosis at later stages of labour increased the risk of maternal complications.
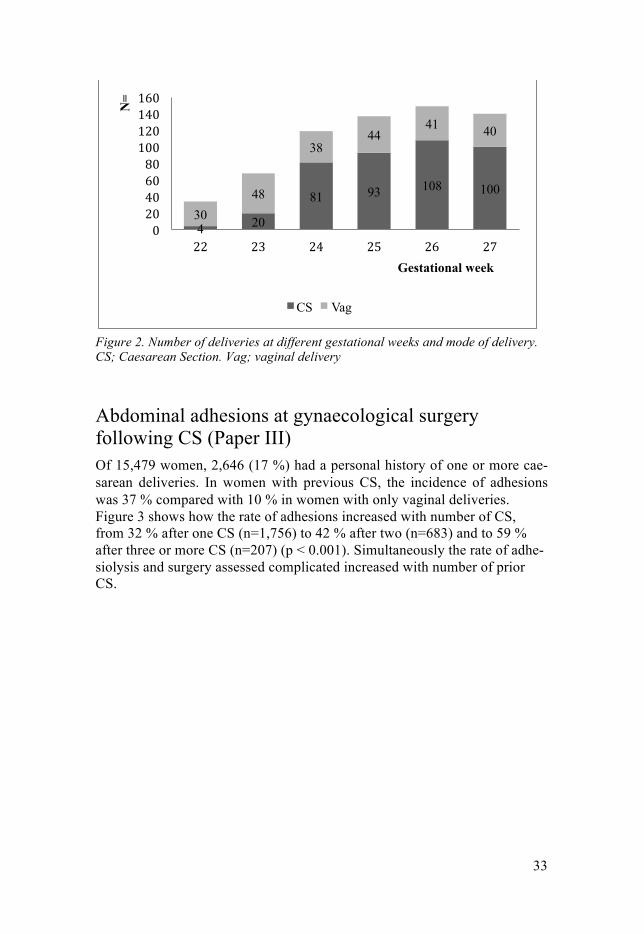
Maternal complications after CS in the extremely preterm period (Paper II) Two-thirds of women with extremely preterm births had a CS, and the pro-portion increased with gestational length (Figure 2). Breech, cord prolapse, abnormal placentation and preeclampsia were more common among deliver-ies by CS, whereas premature rupture of membranes and spontaneous pre-term contractions were associated with vaginal delivery. The majority of CS was performed due to fetal indication. Maternal indications of CS were asso-ciated with increased risk of complications. The most common complication recorded after an extremely preterm CS was infection (19 %). Major maternal complications occurred in 7 % of the ex-tremely preterm compared with 2 % of term births (p < 0.01). No increased blood loss was found among extremely preterm compared with term CS. Uterine incisions extending into corpus were required more often at 22-24 (18 %) than at 25-27 gestational weeks (10 %). Surgery and fetal extraction were assessed as being more difficult at gestational week 22-24, but there was no increased blood loss, infections or other complication rates compared with gestational week 25-27.
33
Figure 2. Number of deliveries at different gestational weeks and mode of delivery. CS; Caesarean Section. Vag; vaginal delivery
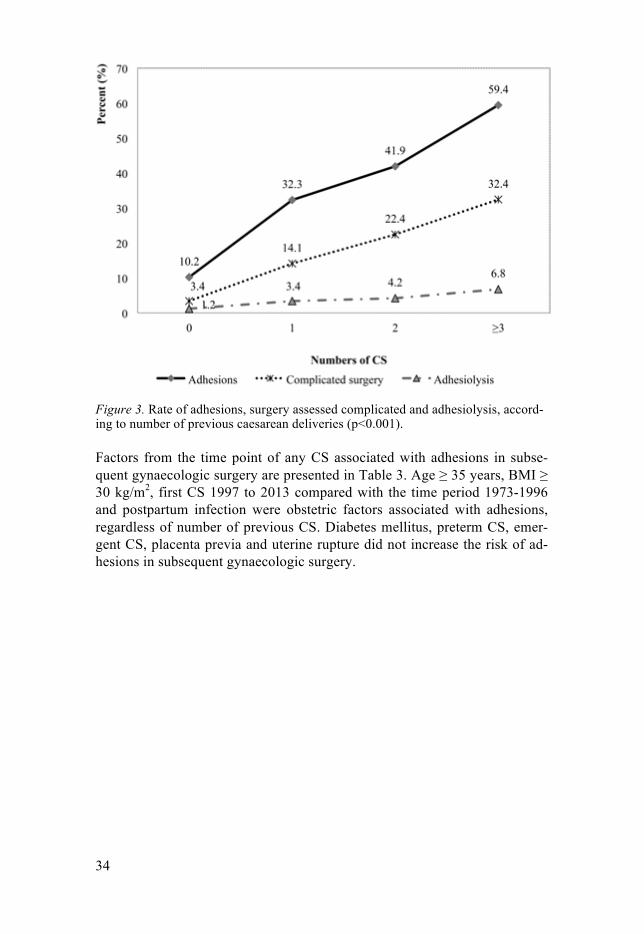
Abdominal adhesions at gynaecological surgery following CS (Paper III) Of 15,479 women, 2,646 (17 %) had a personal history of one or more cae-sarean deliveries. In women with previous CS, the incidence of adhesions was 37 % compared with 10 % in women with only vaginal deliveries. Figure 3 shows how the rate of adhesions increased with number of CS, from 32 % after one CS (n=1,756) to 42 % after two (n=683) and to 59 % after three or more CS (n=207) (p < 0.001). Simultaneously the rate of adhe-siolysis and surgery assessed complicated increased with number of prior CS.
4 20
81 93 108 100
30 48
38 44
41 40 N
=
Gestational week
CS Vag
34
Figure 3. Rate of adhesions, surgery assessed complicated and adhesiolysis, accord-ing to number of previous caesarean deliveries (p<0.001).
Factors from the time point of any CS associated with adhesions in subse-quent gynaecologic surgery are presented in Table 3. Age ≥ 35 years, BMI ≥ 30 kg/m2, first CS 1997 to 2013 compared with the time period 1973-1996 and postpartum infection were obstetric factors associated with adhesions, regardless of number of previous CS. Diabetes mellitus, preterm CS, emer-gent CS, placenta previa and uterine rupture did not increase the risk of ad-hesions in subsequent gynaecologic surgery.
35
Table 3. Factors from the caesarean section (CS) associated with adhesions in subsequent surgery (N=2,646)
Exposure Outcome (adhesions)
n= n (%)= aOR* 95 % CI Number of CS 1 1,756 568 (32) Ref 2 683 286 (42) 1.51 1.26-1.82 ≥3 207 123 (59) 3.16 2.34-4.26 Maternal age ≥35 (years)
577 246 (43) 1.28 1.05-1.55
BMI ≥30 (kg/m2) 264 143 (54) 1.91 1.49-2.45 Extremely preterm 34 15 (44) 1.43 0.71-2.87 Preterm 533 197 (37) 0.93 0.76-1.15 Year of CS 1997-2013 901 379 (42) 1.47 1.24-1.75 CS with labour 1,840 704 (38) 1.10 0.92-1.32 Postpartum infection 113 56 (50) 1.55 1.05-2.30 * Number of CS presented as crude OR. All other explanatory variables adjusted for number of CS and hospital unit at second level.
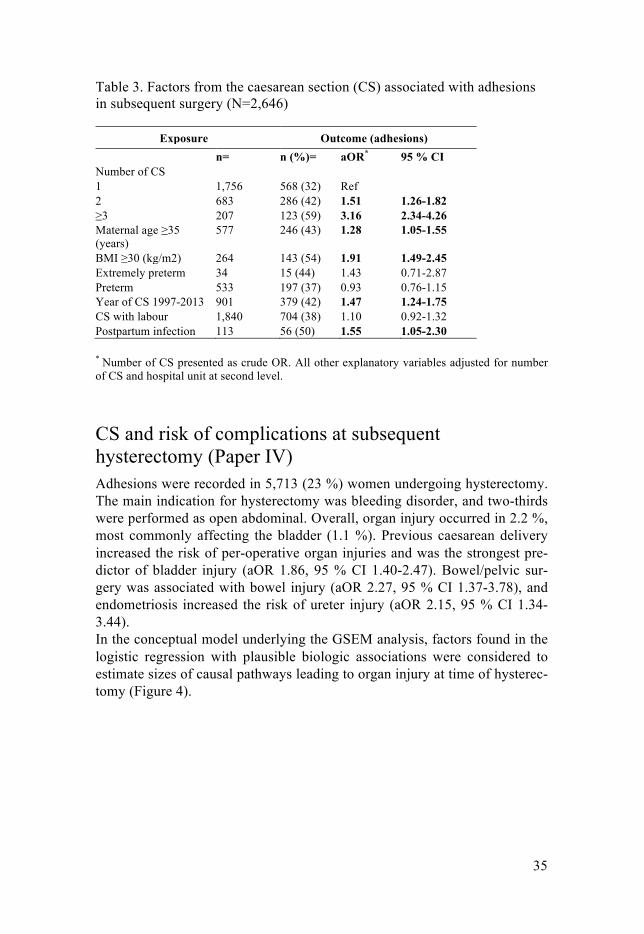
CS and risk of complications at subsequent hysterectomy (Paper IV) Adhesions were recorded in 5,713 (23 %) women undergoing hysterectomy. The main indication for hysterectomy was bleeding disorder, and two-thirds were performed as open abdominal. Overall, organ injury occurred in 2.2 %, most commonly affecting the bladder (1.1 %). Previous caesarean delivery increased the risk of per-operative organ injuries and was the strongest pre-dictor of bladder injury (aOR 1.86, 95 % CI 1.40-2.47). Bowel/pelvic sur-gery was associated with bowel injury (aOR 2.27, 95 % CI 1.37-3.78), and endometriosis increased the risk of ureter injury (aOR 2.15, 95 % CI 1.34-3.44). In the conceptual model underlying the GSEM analysis, factors found in the logistic regression with plausible biologic associations were considered to estimate sizes of causal pathways leading to organ injury at time of hysterec-tomy (Figure 4).
36
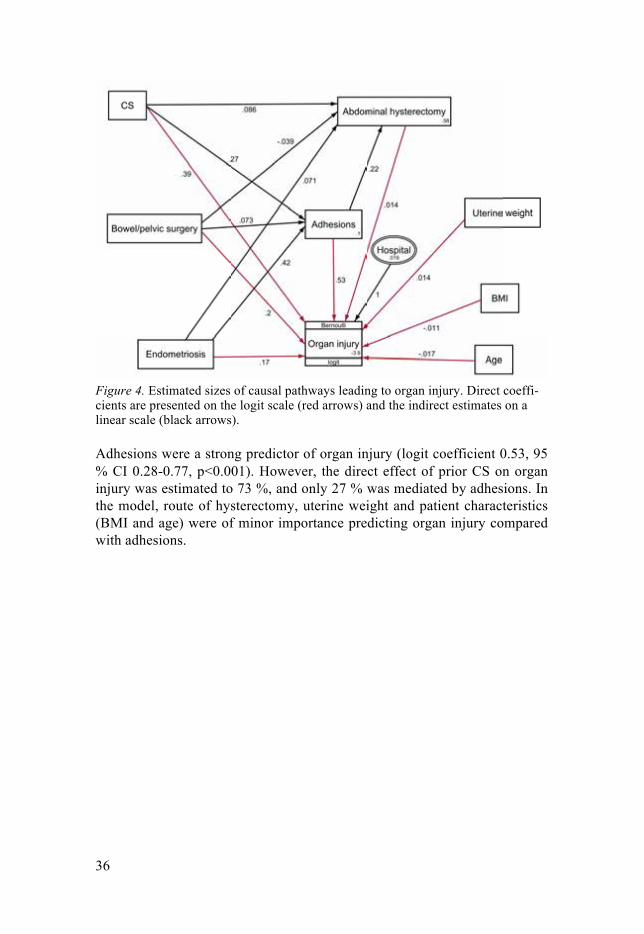
Figure 4. Estimated sizes of causal pathways leading to organ injury. Direct coeffi-cients are presented on the logit scale (red arrows) and the indirect estimates on a linear scale (black arrows).
Adhesions were a strong predictor of organ injury (logit coefficient 0.53, 95 % CI 0.28-0.77, p<0.001). However, the direct effect of prior CS on organ injury was estimated to 73 %, and only 27 % was mediated by adhesions. In the model, route of hysterectomy, uterine weight and patient characteristics (BMI and age) were of minor importance predicting organ injury compared with adhesions.
37
Discussion
The rate of CS is increasing, resulting in increasing number of women who are exposed to potential complications at short- and long-term. In labour and surgery following CS, factors that can be modified such as surgical tech-nique, management of labour and postpartum care are important to investi-gate in relation to complications to prevent future maternal morbidity.
General conclusions The risk of uterine rupture in a subsequent trial of labour did not differ be-tween single and double layer closure of the uterus.
Major maternal complications occurred more frequently in extremely pre-term compared with term CS, but there was no increased blood loss. In the extremely preterm period, maternal complications could not be attributed to the gestational week and the surgical procedure per se but were more related to the indication of the CS.
Number of CS was the most important obstetric factor for formation of adhesions after caesarean delivery. A history of CS was associated with in-creased risk of per- and post-operative complications in hysterectomy. The risk of bladder injury during hysterectomy after previous CS was almost doubled, regardless of route of hysterectomy, maternal characteristics and uterine weight but was not always attributed to presence of adhesions.
Incidence of maternal complications Uterine rupture occurred in 1.3 % of women attempting a TOL, which is a higher rate compared with 0.6 % in a retrospective cohort by Lydon-Rochelle but similar to the 1.5 % reported in a prospective study from the Netherlands [72]. The rate of uterine rupture is influenced by selection of patients for TOL and obstetric management. In the study by Kwee et al., TOL was attempted in 72 % compared to 62 % in this Swedish setting.
Major maternal complications were assessed in 7 % of extremely preterm CS. Interestingly, blood loss was not increased in extremely preterm com-pared to term, and there was a low rate of corporal incisions (12 %) com-pared with other settings [33, 42].

38
The incidence proportion of adhesions after CS in gynaecologic surgery depended on exclusion criteria. In a non-selected group of women undergo-ing hysterectomy, adhesions were recorded in 23 % (45 % of women with prior CS and 17 % in women with no prior CS). In women with no other prior surgery in the abdomen except CS, adhesions were reported in 32-59 %, depending on prior numbers of caesarean deliveries. A similar increase in rates of adhesions according to numbers of CS has been reported at time of repeat caesarean delivery [105, 106].
Risk factors for maternal complications Surgical techniques Caesarean Section The conclusion from study I that single, as opposed to double, layer closure of the uterus does not increase the risk of uterine rupture in subsequent la-bour is in concordance with results from the largest RCT (CORONIS) that has investigated short- and long-term effects of different CS techniques. In the trial, risk of uterine rupture did not differ between single and double clo-sure, although it was underpowered to detect modest differences [85]. This reflects the methodological difficulties encountered when studying rare out-comes. In both the CORONIS trial and the Caesar trial, none of the different parts of the Joel-Cohen technique was proven superior to the other, in re-spect to short-term complications [21, 40].
The role of peritoneal closure for development of adhesion-related com-plications was also investigated in CORONIS. They found no difference in rates of pelvic pain, bowel obstruction, infertility or ectopic pregnancy fol-lowing a CS with peritoneal closure or non-closure. A clear advantage in Papers III and IV is that assessment of adhesions was by direct visualisation and not restricted to symptoms associated with adhesions. In Paper III, women with a first CS during 1997-2013 had 47 % increased odds of adhe-sions present at gynaecologic surgery compared with women with prior CS 1973-1996. This finding might be interpreted as indication of an association with the introduction of the new surgical technique of CS and adhesions. This is in accordance with results from two systematic reviews from 2009 and 2011, suggesting a benefit of peritoneal closure at CS in respect to for-mation of adhesions [113, 130]. Presence of adhesions after preterm CS was investigated in Paper III. As extremely preterm CS could be technically dif-ficult and requires a corporal incision more often, we anticipated the inci-dence of adhesions to be increased compared with CS at term. This could not be confirmed, probably due to the small number (n=34) of extremely pre-term CS in the material.

39
Hysterectomy A personal history of CS increased the risk of organ injury, independent if hysterectomy was abdominal or by minimally invasive route. In a case con-trol study, rates of incidental cystotomy according to type of hysterectomy were 0.76 % in abdominal, 1.3 % with vaginal and 1.8 % with laparoscopic assisted vaginal hysterectomy; a previous CS doubled the risk [108]. In-creased risk of bladder injury at surgery is well documented in women with prior CS [107-110], but results have been inconclusive and sparse regarding ureter and bowel injuries. In a review of 307 women with prior laparotomy undergoing laparoscopic surgery, there was no increased risk of organ injury or conversion to laparotomy after CS, but prior myomectomy posed an al-most five-fold risk [131]. During vaginal hysterectomy (n=741), bowel inju-ry was reported in 1.4 % of women with prior CS compared with 0.14 % of women with no history of CS [109]. However, the risk of organ injury in minimally invasive techniques is closely related to volume of surgical pro-cedures and experience of the surgeon [132]. In the survey from Finland, the proportion of vaginal hysterectomy increased from 18 % to 44 % from 1996-2006; simultaneously, there was a significant decrease of bowel injury from 0.5 % to 0.1 % in vaginal approaches. In the same time period, ureter com-plications decreased from 1.1 % to 0.3 % following laparoscopic hysterec-tomy [132].
Maternal characteristics Advanced maternal age in conjunction with CS was associated with both uterine ruptures in subsequent labour and development of adhesions. Ad-vanced maternal age increases the risk of complications during pregnancy and labour such as hypertensive disorders, diabetes, dystocia and high birth weight, but the effect of age remained after adjusting for these factors in Paper I. The results are in agreement with a Norwegian population based register study where maternal age ≥40 years doubled the risk of rupture [75]. This could be attributed to increased risk of advanced maternal age of im-paired healing at first CS, or more augmented labours at subsequent deliver-ies with age. The impact of age at time of surgery on adhesion formation remains unclear. There are no previous studies investigating the effect of age on development of adhesions after CS, but appendectomy at 20-39 years has been associated with lower risk of subsequent small bowel obstruction com-pared with appendectomy at all other age categories [133].
Obesity is associated with increased risk of surgical morbidity including infection and suboptimal wound healing [134], and obesity could also de-crease fibrinolysis, leading to more adhesions [119]. In concordance, we found that BMI ≥30 at CS, regardless of number of CS, almost doubled the rate of adhesions at subsequent gynaecologic surgery. Age and obesity are

40
factors to consider when counselling women, and the risks of a trial of la-bour must be balanced against risk of repeat CS and the development of adhesions.
In Paper IV, age and BMI were not associated with increased risk of or-gan injury at time of hysterectomy. Obesity at hysterectomy and caesarean section is a known risk factor of post-operative complications such as thrombosis, wound dehiscence and infection [135], whereas the risk for or-gan injury in fact might be decreased [136, 137]. In a study by Lee et al., neither age nor BMI were predictors of re-admission to hospital after hyster-ectomy.
Pregnancy and labour characteristics Modifiable risk factors for uterine rupture included induction of labour and epidural analgesia. Results from a population based study concluded that an increasing trend of uterine rupture in Norway from 1967 to 2008 could be attributed to induction with prostaglandins and more labours augmented with oxytocin in women with a scarred uterus [67]. In protracted labour, epidural analgesia is more frequently used [138], and repeated epidural dosing has been suggested as a warning sign for uterine rupture [139].
In Paper III, number of CS was the main obstetric risk factor for adhe-sions in subsequent gynaecological surgery. Number of CS can to some ex-tent be modified by avoiding CS in the first delivery and by encouraging a trial of labour after CS.
The high maternal morbidity observed after an extremely preterm CS could be result of the indication for delivery that often is related to maternal complications such as hypertensive disorders, abruption and sepsis. In Paper II, maternal complication rates did not differ between gestational weeks 22-24 and 25-27, but a maternal indication of delivery carried a higher risk of complications compared with fetal indication of an extremely preterm CS. Reddy et al. analysed women with placental conditions (previa, accreta and abruption) separately, and a serious maternal complication was recorded in 26 % (GW 23-27), 31 % (GW 28-31) and 35 % (GW 32-33) [33]. The over-all rate of incisions extending into the corpus of 12 % was low compared to 25-56 % reported in prior studies [33, 42], but rates might be influenced by different definitions of incisions and populations studied. A previous preterm CS was not associated with increased rate of abdominal adhesions at gynae-cological surgery.
Post-operative infection The incidence of a post-operative infection reported in MBR and PAR after CS was 4 % (Paper I, referents Paper II and Paper III). Infectious morbidity was much higher after extremely preterm CS (18 %) (Paper II). Complica-

41
tion rates vary by method of collecting data and post-operative infection following CS, including all febrile morbidity requiring antibiotic treatment, was estimated to 17 % in the Caesar trial with prospectively collected data [21]. As a milder postpartum infection is likely to be treated in an outpatient clinic, diagnosis will not be provided by PAR; hence, register based rates will be underestimated and comparison between study groups biased. How-ever, results indicate that extremely preterm CS is a high-risk procedure in terms of infectious morbidity, which may result from the fact that infection is an important cause of preterm birth. Post-operative infection was a risk factor for both uterine rupture and adhesions, making measures to prevent the occurrence of post-operative infections important also for complications occurring in the long-term. The majority of women had received prophylac-tic antibiotics in the cohort of study I (67 %) and among extremely preterm (84 %). According to a review of Smaill et al. 2014, prophylactic antibiotics halves rates of wound- uterine infections following both elective and emer-gent CS [24].
Adhesions and complications Results from Paper IV suggest that history of CS poses risk for complica-tions at remote hysterectomy, but the risk is only partly attributable to pres-ence of adhesions. Previous caesarean delivery and endometriosis were ma-jor predisposing factors for organ injury at time of hysterectomy, whereas patient and operation characteristics were of minor importance. Results from Paper IV demonstrate that prior CS poses a higher risk of organ injuries at hysterectomy (aOR 1.74, 95 % CI 1.41-2.15) compared with history of other bowel/pelvic surgery or endometriosis. The organ affected depended on medical history; prior CS predisposed for bladder injury, prior bowel/pelvic surgery for bowel injury, and endometriosis was associated with ureter inju-ry at time of hysterectomy. Endometriosis is a well-recognised strong predic-tor of intra-operative complications and ureter injury at pelvic surgery [131, 140].
Methodological considerations Observational studies are subject of two types of errors: random error and systematic error. With sufficiently large data the impact of random errors decreases but systematic errors remain, causing bias.
42
Systematic errors Selection Bias The population-based designs in Papers I, III and IV decrease the likelihood of selection bias. Adhesions after CS have been associated with pelvic pain, infertility and dyspareunia [59]; as a result, these indications of surgery might influence the reported rates of adhesions of the study group in Papers III and IV. Pelvic pain was reported as the main indication of hysterectomy in only 5 % in Paper IV; consequently, this selection bias is of minor con-cern.
In Paper III, the study population consisted of women who delivered ex-tremely preterm at two University clinics with proactive management, and results may not be attributable to other settings.
Type of surgery depends on a woman’s medical history; even if prior CS is not a contraindication for vaginal approach, a lower proportion of women with prior CS planned for this route (Papers III-IV). Type of surgery influ-ences the rate of adhesions reported by the surgeon; adhesions are less re-ported in vaginal hysterectomy compared with the abdominal route, which might reflect restricted inspection of the abdomen or reflect the true status of adhesions present in this group.
Information Bias Misclassification of information can be differential and non differential. Non-differential misclassification occurs at random of either exposed/non exposed and independently of the outcome. In contrast, differential misclas-sification occurs if information of exposure differs between cases and con-trols, for example caused by recall bias. It is plausible that misclassification occurred in the reporting of diagnosis and checking of boxes by different physicians. In Paper I, closure of the uterus may have been reported as single when double layers were sutured, or the opposite (exposure). We believe that misclassification did not differ be-tween women with uterine rupture or no uterine rupture (outcome), and it was considered non-differential. Non-differential misclassification can bias an effect towards the null effect. Differential misclassification may have occurred in Papers III and IV, as encountered difficulties in surgery might affect reporting of adhesions, giv-ing an overestimated association between adhesions and obesity, as well as overestimation of adhesions and risk of complications.
In Paper II, various methods of collecting data potentially overestimated the risks of extremely preterm CS compared with term CS.

43
Confounding and mediation A confounder is a cause for both the exposure and the outcome resulting in a confusion of effect. In contrast, a mediator is on the causal pathway from exposure to outcome. In Paper III, potential confounding between CS and adhesions, depending on prior medical history, was addressed by excluding patients with diagnosis of pelvic/bowel surgery and or inflammatory disease of the abdomen preceding the gynaecological surgery. In Papers I and IV, covariates included in the models were based on the framework of associa-tions found in prior studies and by the results of bivariate analysis. Multi-level logistic regression analysis was performed to adjust for potential con-founding at the individual and contextual level (hospitals). However, un-measured and unknown confounders may still be a problem. The results of the GSEM analysis of Paper IV suggest presence of an unrecognised media-tor associated with both CS and organ injury. The effect of organ injury at surgery following a CS could only be attributed to adhesions in less than one-third.
Random errors Question of power and erroneous statistical inference In observational studies, power calculation could be considered as being irrelevant, but reflections about size of study population and statistical infer-ence are appropriate.
Power calculation of Paper I was designed to detect a two-fold increased risk of uterine rupture with respect to uterine closure. The study was under-powered to detect smaller differences and potentially subject to a type 2 er-ror (false negative). However a small risk difference would have no clinical significance since the baseline risk of uterine rupture is low. Statistical pow-er in between group comparisons in Paper II was restricted by stratification of the extremely preterm and could contribute to non-detected differences between the gestational age strata. One should remember, ‘Absence of evi-dence is not evidence of absence’ (Altman).
Table 4. Types of statistical errors Null hypothesis True False Null hypothesis rejected Type 1 error Correct inference Null hypothesis not rejected Correct inference Type 2 error In all studies, multiple testing increased the risk of a type 1 error (false posi-tive), and some of the associations may be by chance. To reduce this error, all testing was based on a conceptual framework of plausible biological ac-
44
tions. The confidence intervals around the estimates reported in Papers III and IV were all narrow, indicating a high precision.
Another problem resulting from large study populations (Paper I, III and IV) may be the interpretation of statistical significance at group level to clin-ical significance at the individual level. In Paper IV, the absolute risk of organ injury was 2.2 %. Although statistically significant, a small risk in-crease may not have a strong impact for the individual, and the development and use of predictive models may be limited.
Strengths The aggregation of National health registers and medical records have per-mitted for conclusions to be drawn for long-term complications of CS. Ran-domised controlled trials investigating long-term effects of surgical tech-niques, as well as optimal mode of delivery of the extremely preterm, have been hard to perform, due to the time span required and recruitment prob-lems.
Strengths of Studies I, III and IV include population-based settings, large study samples and reliable data for exposure and outcome. Standardised operation template with check boxes provided information for suture layers in 99 % (Paper I), was complete for presence of adhesions (Paper III) and included information about organ injury in 89 % of patients (Paper IV). Re-call bias was not a concern since all exposure and outcome information was recorded prospectively and independently. Selection bias was minimised since the cohorts were well defined. In the cohort studies, potential hetero-geneity and clustering between hospitals were controlled for by multi-level logistic regression.
The observational study II provided detailed information of the rare con-dition of extremely preterm CS.
Clinical implications The results are in agreement with evidence from well designed RCT and meta analysis concluding that one compared with two layer closure of the hysterotomy at CS, neither improves short-term morbidity or increases the risk of uterine rupture in subsequent labour [21, 40, 73]. As a result, either technique can be used. Locked sutures of the hysterotomy have been associ-ated with defect healing and increased risk of uterine rupture [73, 88]. Babu has proposed a technique with a continuous modified mattress suture, which stresses the importance of correct approximation of cut margins, i.e. decidua to decidua and myometrium to myometrium [141].

45
Figure 5. Suture technique for closing the hysterotomy proposed by Babu..
In pre labour counselling after CS, adverse effects of repeat CS should be balanced against risk of uterine rupture. Predictive models of uterine rupture have proved to be difficult to develop [76, 142], but a validated model to predict failed vaginal birth after caesarean has been proposed by Smiths et al. [143]. Prior indication of CS influences the chance of vaginal birth in a trial of labour. Index indication of multiple births, breech and placenta previa are associated with CS rate of 17-18 %, whereas prior indication of macro-somia or complications during labour increases CS rates in TOL to 40 % [144]. Maternal characteristics such as age and height as well as diabetes are important factors to consider in pre labour counselling for a trial of labour after CS. Induction of labour after CS increases the risk of uterine rupture, and should be used cautiously in women with a scarred uterus. These factors are closely related to an emergency CS during a trial of labour [143], which, in turn, carries the highest risk of adverse maternal outcome [46].
On the other hand, encouragement of VBAC will decrease complications caused by multiple caesarean deliveries; number of CS is the most important factor for development of adhesions, and adhesions are closely related to organ injury in subsequent surgery.
There was a high rate of postpartum infection after an extremely preterm CS, and type and dose of prophylactic antibiotics needs to be explored fur-ther in this group. The low rate of corporal incisions, with reproductive con-sequences for the mother in the long-term, indicates that centralisation of extremely preterm deliveries may also benefit the mothers.
Clinicians acknowledge that surgery in women with endometriosis is high-risk procedure, but a personal history of CS carried higher risks for organ injury and post-operative complications at time of hysterectomy com-pared with previous bowel/pelvic surgery or endometriosis. As medical his-tory and prior CS indicates which organ is most affected, preventive measures including operation techniques [145], patient information and fol-low-up is essential and should be individualised. As route of hysterectomy was of minor importance for organ injury, prior CS should not be regarded as a contraindication for the vaginal approach. Vaginal hysterectomy is asso-ciated with faster recovery and less haemorrhage, whereas laparoscopic sur-

46
gery requires longer operating times and might increase the risk of urinary tract injuries compared with abdominal route [146].
Future research Large studies are needed to evaluate important but rare outcomes, and RCTs are often proved to be underpowered.
The main drawback with observational studies is the risk of uncontrolled confounding, which can result in false associations and confusion of effects. Epidemiologic studies restrict interpretation of causality and biological ac-tions between exposures and outcomes. The recently established network in Sweden called SNAKS (Svenskt nätverk för Nationella Kliniska Studier inom OB/Gyn) gives an excellent opportunity to conduct well-designed pro-spective multicentre studies with the possibility of randomisation. By com-bining National quality registers, allocation to certain interventions and treatments and follow-up is feasible in respect to recruitment and costs. Short- and long-term morbidity can be assessed by evaluating a bundle of peri-operative processes of CS, including choice of surgical technique.
The low rate of adhesions following a CS compared with other gynaeco-logical procedures such as myomectomy is puzzling and contradicts the fact that fibrinolysis is decreased during pregnancy. Basic biochemical research and animal models might be beneficial to investigate effects of pregnancy, for example, the role of amniotic fluid on adhesion formation.
The lack of standardised outcome measures concerning adverse outcomes restricts interpretation and comparison between studies and often leads to contradictory results. The initiated work of core outcomes for evaluations of interventions preventing preterm birth [147], should inspire to elaborate standardised maternal outcomes in obstetric clinical trials.
An important issue that requires follow-up is the implementation of team-led hospital based care, which has been associated with reduced rates of CS in nulliparous women without increased risk of neonatal complications [148]. The pregnancy register, with detailed information regarding labour management and maternal and neonatal outcomes, could be a valuable re-source to investigate and evaluate specific procedures of these programmes.
47
Summary in Swedish
Kejsarsnitt är den vanligaste större gynekologiska operationen som utförs i världen idag. I hög och mellaninkomstländer sker mellan 15-40 % av för-lossningar med kejsarsnitt. Andel kejsarsnitt vid extrem för tidig födsel (<28 graviditetsveckor) har också ökat globalt och nationellt men med stora glob-ala och regionala skillnader. Ärr i livmodern medför ökade risker för kom-plikationer vid efterföljande graviditeter och förlossningar och sam-manväxningar i buken efter kejsarsnitt kan innebära försvårade opera-tionsförhållanden vid kirurgi. Kunskapsläget om den mest fördelaktiga oper-ationstekniken vid kejsarsnitt för långsiktiga komplikationer är begränsat på grund av metodologiska svårigheter att studera dessa. Målsättningen med avhandlingen var att studera komplikationer för modern efter kejsarsnitt.
I arbete I studerades om risken för uterusruptur efter ett kejsarsnitt påverkades av suturering av livmoderväggen i ett jämfört med två suturlager. Genom länkning av datajournalsystem, med data om operationsteknik, och Medicinska födelseregistret identifierades en kohort av 19 604 förstföder-skor som förlöstes med kejsarsnitt 2001-2007. Under andra graviditeten gjorde 7 683 ett vaginalt förlossningsförsök, varav 103 kvinnor (1, 3 %) fick en livmoderbristning. Ingen skillnad för livmoderbristning, avseende ett och två lager suturering av livmodern kunde påvisas, däremot medförde högre ålder hos modern, kortvuxenhet, infektion efter första kejsarsnitt, igångsättning av den andra förlossningen samt barn med större födelsevikt en ökad risk.
I studie II undersöktes komplikationer efter kejsarsnitt vid extrem under-burenhet hos kvinnor förlösta i Uppsala eller Umeå 2001-2012 i gravidi-tetsvecka 22-27. Det var fler komplikationer i denna grupp jämfört med kvinnor förlösta med kejsarsnitt i fullgången tid, men ingen skillnad mellan 22-24 jämfört med 25-27 graviditetsveckor. Om kejsarsnittet utfördes p.g.a. moders sjuklighet ökade komplikationerna jämfört med då kejsarsnitt utfördes på barnindikation.
I arbete III och IV används en kohort av kvinnor som genomgått gyne-kologisk buk kirurgi, 2000-2014, och som var registrerade i ett nationellt kvalitetsregister (Gynop). Data från kvinnans tidigare graviditeter, förloss-ningar, bukoperationer och diagnoser från Nationella hälsoregister sam-manlänkades med Gynop. I samband med den gynekologiska operationen registrerade operatören förekomst av sammanväxningar. I studie III exklude-rades kvinnor med tidigare bukoperationer frånsett kejsarsnitt och 15 479
48
kvinnor undersöktes med avseende på sammanväxningar. Andel med sam-manväxningar ökade med antal kejsarsnitt från 32 % efter ett kejsarsnitt till 42 % efter två och 59 % efter tre eller fler kejsarsnitt. Faktorer i samband med kejsarsnitt kopplade till sammanväxningar var ålder ≥35 år, BMI ≥30 och infektion. I arbete IV studerades komplikationsrisk vid bortopererande av livmodern utifrån tidigare kejsarsnitt, övrig bukoperation och endometri-os, och hur stor andel av organskada som drivs av sammanväxningar i buken. Tidigare kejsarsnitt var en stark riskfaktor för komplikationer vid och efter bortopererande av livmodern och var kopplat till skada på inre organ, men endast en del av dessa komplikationer förklarades av sam-manväxningar.
Sammanfattningsvis har länkning av data av Svenska Nationella kvalitetsregister möjliggjort studier av långsiktiga komplikationer för mod-ern av kejsarsnitt. Även om de absoluta riskerna för allvarliga komplikation-er såsom uterusruptur och organskada kan tyckas små, så är den relativa riskökningen av kejsarsnitt av stor betydelse. Med kartläggning av risk-faktorer kan vård för förlossning och operationer av kvinnor med tidigare kejsarsnitt optimeras.
49
Acknowledgements
This journey would not have been possible without tremendous support. First of all, my supervisors: Maria Jonsson, Associate professor at the Department of Women´s and Chil-dren´s Health Uppsala University and main supervisor, for your combined clinical- and evidence- based approach to obstetrics. Your rapid clear-cut thoughts and words have been invaluable for these works and have inspired me both as a clinician and for future research questions.
Ulf Högberg, Senior professor at the Department of Women´s and Chil-dren´s Health Uppsala University and co-supervisor, for your patience and generous sharing of your outstanding knowledge in medical science, always combined with a visionary and humanistic approach.
Eva-Britta Råssjö, PhD and co-supervisor, I am so grateful that you intro-duced me to research and always kept an eye on the clinical relevance of ques-tions. Tomas Riman, former head and Agneta Romin, head of the department of Ob-stetrics and Gynaecology Falu Lasarett, for providing an opportunity for re-search. Centre of clinical Research Dalarna (CKF): Erica Schytt, co-worker and head of the department, for contribution and wise counselling. Maria Pilawa, for always being helpful and for your contribution to a welcoming atmosphere at CKF. Katarina Ekholm-Selling, IMCH and Erik Lampa, UCR for the introduction and outstanding help in statistics combined with inspiring discussions. Dear friends and colleagues at the department of Obstetrics and Gynaecology:
Lina Bergman, colleague and friend both at the clinic and in research, for your endless energy and sharp observations. You helped me through this!
Cecilia Anagrius, for your friendship and support. Ingela Lundin, for discussions and reflections concerning gynaecological
surgery. At last, with all my love to my family.

50
51
References
1. Declercq E, Young R, Cabral H, Ecker J: Is a rising cesarean delivery rate inevitable? Trends in industrialized countries, 1987 to 2007. Birth 2011, 38(2):99-104.
2. Betran AP, Ye J, Moller AB, Zhang J, Gulmezoglu AM, Torloni MR: The Increasing Trend in Caesarean Section Rates: Global, Regional and National Estimates: 1990-2014. PloS one 2016, 11(2):e0148343.
3. Lurie S: Spencer Wells and uterine sutures at caesarean section. The Lancet 2012, 380(9853):1558.
4. Kerr JM: Technique of Lower Segment Caesarean Section, More Especially in "Suspect" and Infected Cases: (Section of Obstetrics and Gynaecology). Proceedings of the Royal Society of Medicine 1936, 29(12):1645-1647.
5. Tulandi T, Hum HS, Gelfand MM: Closure of laparotomy incisions with or without peritoneal suturing and second-look laparoscopy. American journal of obstetrics and gynecology 1988, 158(3 Pt 1):536-537.
6. Irion O, Luzuy F, Beguin F: Nonclosure of the visceral and parietal peritoneum at caesarean section: a randomised controlled trial. British journal of obstetrics and gynaecology 1996, 103(7):690-694.
7. Holmgren G, Sjoholm L, Stark M: The Misgav Ladach method for cesarean section: method description. Acta obstetricia et gynecologica Scandinavica 1999, 78(7):615-621.
8. Wallin G, Fall O: Modified Joel-Cohen technique for caesarean delivery. British journal of obstetrics and gynaecology 1999, 106(3):221-226.
9. Darj E, Nordstrom ML: The Misgav Ladach method for cesarean section compared to the Pfannenstiel method. Acta obstetricia et gynecologica Scandinavica 1999, 78(1):37-41.
10. Appropriate technology for birth. Lancet 1985, 2(8452):436-437. 11. Betran AP, Torloni MR, Zhang JJ, Gulmezoglu AM, Section WHOWGoC:
WHO Statement on Caesarean Section Rates. BJOG : an international journal of obstetrics and gynaecology 2016, 123(5):667-670.
12. European Perinatal Health Report: Health and care of pregnant women and babies in Europe in 2010. (www.europeristat.com/ reports/european-perinatal-health-report-2010.html)
13. Lavender T, Hofmeyr GJ, Neilson JP, Kingdon C, Gyte GM: Caesarean section for non-medical reasons at term. The Cochrane database of systematic reviews 2012(3):CD004660.
14. Wang X, Hellerstein S, Hou L, Zou L, Ruan Y, Zhang W: Caesarean deliveries in China. BMC pregnancy and childbirth 2017, 17(1):54.
15. Hoxha I, Syrogiannouli L, Luta X, Tal K, Goodman DC, da Costa BR, Juni P: Caesarean sections and for-profit status of hospitals: systematic review and meta-analysis. BMJ open 2017, 7(2):e013670.
52
16. Hofmeyr GJ, Hannah M, Lawrie TA: Planned caesarean section for term breech delivery. The Cochrane database of systematic reviews 2015(7):CD000166.
17. Pallasmaa N, Ekblad U, Aitokallio-Tallberg A, Uotila J, Raudaskoski T, Ulander VM, Hurme S: Cesarean delivery in Finland: maternal complications and obstetric risk factors. Acta obstetricia et gynecologica Scandinavica 2010, 89(7):896-902.
18. van Ham MA, van Dongen PW, Mulder J: Maternal consequences of caesarean section. A retrospective study of intra-operative and postoperative maternal complications of caesarean section during a 10-year period. European journal of obstetrics, gynecology, and reproductive biology 1997, 74(1):1-6.
19. Al-Zirqi I, Vangen S, Forsen L, Stray-Pedersen B: Prevalence and risk factors of severe obstetric haemorrhage. BJOG : an international journal of obstetrics and gynaecology 2008, 115(10):1265-1272.
20. Villar J, Carroli G, Zavaleta N, Donner A, Wojdyla D, Faundes A, Velazco A, Bataglia V, Langer A, Narvaez A et al: Maternal and neonatal individual risks and benefits associated with caesarean delivery: multicentre prospective study. Bmj 2007, 335(7628):1025.
21. CAESAR study collaborative group: Caesarean section surgical techniques: a randomised factorial trial (CAESAR). BJOG : an international journal of obstetrics and gynaecology 2010, 117(11):1366-1376.
22. Leth RA, Moller JK, Thomsen RW, Uldbjerg N, Norgaard M: Risk of selected postpartum infections after cesarean section compared with vaginal birth: a five-year cohort study of 32,468 women. Acta obstetricia et gynecologica Scandinavica 2009, 88(9):976-983.
23. Burrows LJ, Meyn LA, Weber AM: Maternal morbidity associated with vaginal versus cesarean delivery. Obstetrics and gynecology 2004, 103(5 Pt 1):907-912.
24. Smaill FM, Grivell RM: Antibiotic prophylaxis versus no prophylaxis for preventing infection after cesarean section. The Cochrane database of systematic reviews 2014, 10:CD007482.
25. Lindqvist P, Dahlback B, Marsal K: Thrombotic risk during pregnancy: a population study. Obstetrics and gynecology 1999, 94(4):595-599.
26. Acosta CD, Knight M, Lee HC, Kurinczuk JJ, Gould JB, Lyndon A: The continuum of maternal sepsis severity: incidence and risk factors in a population-based cohort study. PloS one 2013, 8(7):e67175.
27. Hager RM, Daltveit AK, Hofoss D, Nilsen ST, Kolaas T, Oian P, Henriksen T: Complications of cesarean deliveries: rates and risk factors. American journal of obstetrics and gynecology 2004, 190(2):428-434.
28. Lurie S, Raz N, Boaz M, Sadan O, Golan A: Comparison of maternal outcomes from primary cesarean section during the second compared with first stage of labor by indication for the operation. European journal of obstetrics, gynecology, and reproductive biology 2014, 182:43-47.
29. Alexander JM, Leveno KJ, Rouse DJ, Landon MB, Gilbert S, Spong CY, Varner MW, Moawad AH, Caritis SN, Harper M et al: Comparison of maternal and infant outcomes from primary cesarean delivery during the second compared with first stage of labor. Obstetrics and gynecology 2007, 109(4):917-921.
53
30. Tuuli MG, Liu L, Longman RE, Odibo AO, Macones GA, Cahill AG: Infectious morbidity is higher after second-stage compared with first-stage cesareans. American journal of obstetrics and gynecology 2014, 211(4):410 e411-416.
31. Pergialiotis V, Vlachos DG, Rodolakis A, Haidopoulos D, Thomakos N, Vlachos GD: First versus second stage C/S maternal and neonatal morbidity: a systematic review and meta-analysis. European journal of obstetrics, gynecology, and reproductive biology 2014, 175:15-24.
32. Silver RM, Landon MB, Rouse DJ, Leveno KJ, Spong CY, Thom EA, Moawad AH, Caritis SN, Harper M, Wapner RJ et al: Maternal morbidity associated with multiple repeat cesarean deliveries. Obstetrics and gynecology 2006, 107(6):1226-1232.
33. Reddy UM, Rice MM, Grobman WA, Bailit JL, Wapner RJ, Varner MW, Thorp JM, Jr., Leveno KJ, Caritis SN, Prasad M et al: Serious maternal complications after early preterm delivery (24-33 weeks' gestation). American journal of obstetrics and gynecology 2015, 213(4):538 e531-539.
34. Stark M, Finkel AR: Comparison between the Joel-Cohen and Pfannenstiel incisions in cesarean section. European journal of obstetrics, gynecology, and reproductive biology 1994, 53(2):121-122.
35. Hudic I, Bujold E, Fatusic Z, Skokic F, Latifagic A, Kapidzic M, Fatusic J: The Misgav-Ladach method of cesarean section: a step forward in operative technique in obstetrics. Archives of gynecology and obstetrics 2012, 286(5):1141-1146.
36. Hofmeyr GJ, Mathai M, Shah A, Novikova N: Techniques for caesarean section. The Cochrane database of systematic reviews 2008(1):CD004662.
37. Xavier P, Ayres-De-Campos D, Reynolds A, Guimaraes M, Costa-Santos C, Patricio B: The modified Misgav-Ladach versus the Pfannenstiel-Kerr technique for cesarean section: a randomized trial. Acta obstetricia et gynecologica Scandinavica 2005, 84(9):878-882.
38. Dodd JM, Anderson ER, Gates S, Grivell RM: Surgical techniques for uterine incision and uterine closure at the time of caesarean section. The Cochrane database of systematic reviews 2014(7):CD004732.
39. Bamigboye AA, Hofmeyr GJ: Closure versus non-closure of the peritoneum at caesarean section: short- and long-term outcomes. The Cochrane database of systematic reviews 2014(8):CD000163.
40. Group CC, Abalos E, Addo V, Brocklehurst P, El Sheikh M, Farrell B, Gray S, Hardy P, Juszczak E, Mathews JE et al: Caesarean section surgical techniques (CORONIS): a fractional, factorial, unmasked, randomised controlled trial. Lancet 2013, 382(9888):234-248.
41. Blencowe H, Cousens S, Oestergaard MZ, Chou D, Moller AB, Narwal R, Adler A, Vera Garcia C, Rohde S, Say L et al: National, regional, and worldwide estimates of preterm birth rates in the year 2010 with time trends since 1990 for selected countries: a systematic analysis and implications. Lancet 2012, 379(9832):2162-2172.
42. Thomas PE, Petersen SG, Gibbons K: The influence of mode of birth on neonatal survival and maternal outcomes at extreme prematurity: A retrospective cohort study. The Australian & New Zealand journal of obstetrics & gynaecology 2015.
43. Hogberg U, Hakansson S, Serenius F, Holmgren PA: Extremely preterm cesarean delivery: a clinical study. Acta obstetricia et gynecologica Scandinavica 2006, 85(12):1442-1447.
54
44. Boyle JG, Gabbe SG: T and J vertical extensions in low transverse cesarean births. Obstetrics and gynecology 1996, 87(2):238-243.
45. Luthra G, Gawade P, Starikov R, Markenson G: Uterine incision-to-delivery interval and perinatal outcomes in transverse versus vertical incisions in preterm cesarean deliveries. The journal of maternal-fetal & neonatal medicine : the official journal of the European Association of Perinatal Medicine, the Federation of Asia and Oceania Perinatal Societies, the International Society of Perinatal Obstet 2013, 26(18):1788-1791.
46. Landon MB, Hauth JC, Leveno KJ, Spong CY, Leindecker S, Varner MW, Moawad AH, Caritis SN, Harper M, Wapner RJ et al: Maternal and perinatal outcomes associated with a trial of labor after prior cesarean delivery. The New England journal of medicine 2004, 351(25):2581-2589.
47. Chauhan SP, Magann EF, Wiggs CD, Barrilleaux PS, Martin JN, Jr.: Pregnancy after classic cesarean delivery. Obstetrics and gynecology 2002, 100(5 Pt 1):946-950.
48. Lannon SM, Guthrie KA, Vanderhoeven JP, Gammill HS: Uterine rupture risk after periviable cesarean delivery. Obstetrics and gynecology 2015, 125(5):1095-1100.
49. Express group, Fellman V, Hellstrom-Westas L, Norman M, Westgren M, Kallen K, Lagercrantz H, Marsal K, Serenius F, Wennergren M: One-year survival of extremely preterm infants after active perinatal care in Sweden. Jama 2009, 301(21):2225-2233.
50. Domellof M PK: Riktlinjer vid hotande förtidsbörd ska ge bättre och mer jämlik vård. Läkartidningen 2017, 114(EEYI).
51. American College of O, Gynecologists, Society for Maternal-Fetal M: ACOG Obstetric Care Consensus No. 3: Periviable Birth. Obstetrics and gynecology 2015, 126(5):e82-94.
52. Alfirevic Z, Milan SJ, Livio S: Caesarean section versus vaginal delivery for preterm birth in singletons. The Cochrane database of systematic reviews 2013, 9:CD000078.
53. Kallen K, Serenius F, Westgren M, Marsal K, Group E: Impact of obstetric factors on outcome of extremely preterm births in Sweden: prospective population-based observational study (EXPRESS). Acta obstetricia et gynecologica Scandinavica 2015, 94(11):1203-1214.
54. Mercer BM: Mode of delivery for periviable birth. Seminars in perinatology 2013, 37(6):417-421.
55. Herbst A, Kallen K: Influence of mode of delivery on neonatal mortality and morbidity in spontaneous preterm breech delivery. European journal of obstetrics, gynecology, and reproductive biology 2007, 133(1):25-29.
56. Stoll BJ, Hansen NI, Bell EF, Walsh MC, Carlo WA, Shankaran S, Laptook AR, Sanchez PJ, Van Meurs KP, Wyckoff M et al: Trends in Care Practices, Morbidity, and Mortality of Extremely Preterm Neonates, 1993-2012. Jama 2015, 314(10):1039-1051.
57. Thurn L, Lindqvist PG, Jakobsson M, Colmorn LB, Klungsoyr K, Bjarnadottir RI, Tapper AM, Bordahl PE, Gottvall K, Petersen KB et al: Abnormally invasive placenta-prevalence, risk factors and antenatal suspicion: results from a large population-based pregnancy cohort study in the Nordic countries. BJOG : an international journal of obstetrics and gynaecology 2015.
55
58. Hofmeyr GJ, Say L, Gulmezoglu AM: WHO systematic review of maternal mortality and morbidity: the prevalence of uterine rupture. BJOG : an international journal of obstetrics and gynaecology 2005, 112(9):1221-1228.
59. Lyell DJ: Adhesions and perioperative complications of repeat cesarean delivery. American journal of obstetrics and gynecology 2011, 205(6 Suppl):S11-18.
60. Kamara M, Henderson JJ, Doherty DA, Dickinson JE, Pennell CE: The risk of placenta accreta following primary elective caesarean delivery: a case-control study. BJOG : an international journal of obstetrics and gynaecology 2013, 120(7):879-886.
61. Gyamfi-Bannerman C, Gilbert S, Landon MB, Spong CY, Rouse DJ, Varner MW, Caritis SN, Meis PJ, Wapner RJ, Sorokin Y et al: Risk of uterine rupture and placenta accreta with prior uterine surgery outside of the lower segment. Obstetrics and gynecology 2012, 120(6):1332-1337.
62. Sumigama S, Sugiyama C, Kotani T, Hayakawa H, Inoue A, Mano Y, Tsuda H, Furuhashi M, Yamamuro O, Kinoshita Y et al: Uterine sutures at prior caesarean section and placenta accreta in subsequent pregnancy: a case-control study. BJOG : an international journal of obstetrics and gynaecology 2014, 121(7):866-874; discussion 875.
63. Guise JM, McDonagh MS, Osterweil P, Nygren P, Chan BK, Helfand M: Systematic review of the incidence and consequences of uterine rupture in women with previous caesarean section. Bmj 2004, 329(7456):19-25.
64. Al-Zirqi I, Stray-Pedersen B, Forsen L, Kjersti Daltveit A, Vangen S, group NUR: Validation study of uterine rupture registration in the Medical Birth Registry of Norway. Acta obstetricia et gynecologica Scandinavica 2013, 92(9):1086-1093.
65. Thisted DL, Mortensen LH, Hvidman L, Rasmussen SC, Larsen T, Krebs L: Use of ICD-10 codes to monitor uterine rupture: validation of a national birth registry. European journal of obstetrics, gynecology, and reproductive biology 2014, 173:23-28.
66. Colmorn LB, Petersen KB, Jakobsson M, Lindqvist PG, Klungsoyr K, Kallen K, Bjarnadottir RI, Tapper AM, Bordahl PE, Gottvall K et al: The Nordic Obstetric Surveillance Study: a study of complete uterine rupture, abnormally invasive placenta, peripartum hysterectomy, and severe blood loss at delivery. Acta obstetricia et gynecologica Scandinavica 2015, 94(7):734-744.
67. Al-Zirqi I, Stray-Pedersen B, Forsen L, Daltveit AK, Vangen S: Uterine rupture: trends over 40 years. BJOG : an international journal of obstetrics and gynaecology 2015.
68. Kaczmarczyk M, Sparen P, Terry P, Cnattingius S: Risk factors for uterine rupture and neonatal consequences of uterine rupture: a population-based study of successive pregnancies in Sweden. BJOG : an international journal of obstetrics and gynaecology 2007, 114(10):1208-1214.
69. Lydon-Rochelle M, Holt VL, Easterling TR, Martin DP: Risk of uterine rupture during labor among women with a prior cesarean delivery. The New England journal of medicine 2001, 345(1):3-8.
70. Studsgaard A, Skorstengaard M, Glavind J, Hvidman L, Uldbjerg N: Trial of labor compared to repeat cesarean section in women with no other risk factors than a prior cesarean delivery. Acta obstetricia et gynecologica Scandinavica 2013, 92(11):1256-1263.
56
71. Fitzpatrick KE, Kurinczuk JJ, Alfirevic Z, Spark P, Brocklehurst P, Knight M: Uterine rupture by intended mode of delivery in the UK: a national case-control study. PLoS medicine 2012, 9(3):e1001184.
72. Kwee A, Bots ML, Visser GH, Bruinse HW: Obstetric management and outcome of pregnancy in women with a history of caesarean section in the Netherlands. European journal of obstetrics, gynecology, and reproductive biology 2007, 132(2):171-176.
73. Roberge S, Chaillet N, Boutin A, Moore L, Jastrow N, Brassard N, Gauthier RJ, Hudic I, Shipp TD, Weimar CH et al: Single- versus double-layer closure of the hysterotomy incision during cesarean delivery and risk of uterine rupture. International journal of gynaecology and obstetrics: the official organ of the International Federation of Gynaecology and Obstetrics 2011, 115(1):5-10.
74. Weimar CH, Lim AC, Bots ML, Bruinse HW, Kwee A: Risk factors for uterine rupture during a vaginal birth after one previous caesarean section: a case-control study. European journal of obstetrics, gynecology, and reproductive biology 2010, 151(1):41-45.
75. Al-Zirqi I, Stray-Pedersen B, Forsen L, Vangen S: Uterine rupture after previous caesarean section. BJOG : an international journal of obstetrics and gynaecology 2010, 117(7):809-820.
76. Grobman WA, Lai Y, Landon MB, Spong CY, Leveno KJ, Rouse DJ, Varner MW, Moawad AH, Caritis SN, Harper M et al: Prediction of uterine rupture associated with attempted vaginal birth after cesarean delivery. American journal of obstetrics and gynecology 2008, 199(1):30 e31-35.
77. Zelop CM, Shipp TD, Repke JT, Cohen A, Lieberman E: Effect of previous vaginal delivery on the risk of uterine rupture during a subsequent trial of labor. American journal of obstetrics and gynecology 2000, 183(5):1184-1186.
78. Dekker GA, Chan A, Luke CG, Priest K, Riley M, Halliday J, King JF, Gee V, O'Neill M, Snell M et al: Risk of uterine rupture in Australian women attempting vaginal birth after one prior caesarean section: a retrospective population-based cohort study. BJOG : an international journal of obstetrics and gynaecology 2010, 117(11):1358-1365.
79. Harper LM, Cahill AG, Boslaugh S, Odibo AO, Stamilio DM, Roehl KA, Macones GA: Association of induction of labor and uterine rupture in women attempting vaginal birth after cesarean: a survival analysis. American journal of obstetrics and gynecology 2012, 206(1):51 e51-55.
80. Bujold E, Goyet M, Marcoux S, Brassard N, Cormier B, Hamilton E, Abdous B, Sidi EA, Kinch R, Miner L et al: The role of uterine closure in the risk of uterine rupture. Obstetrics and gynecology 2010, 116(1):43-50.
81. Jastrow N, Roberge S, Gauthier RJ, Laroche L, Duperron L, Brassard N, Bujold E: Effect of birth weight on adverse obstetric outcomes in vaginal birth after cesarean delivery. Obstetrics and gynecology 2010, 115(2 Pt 1):338-343.
82. Stamilio DM, DeFranco E, Pare E, Odibo AO, Peipert JF, Allsworth JE, Stevens E, Macones GA: Short interpregnancy interval: risk of uterine rupture and complications of vaginal birth after cesarean delivery. Obstetrics and gynecology 2007, 110(5):1075-1082.
83. Shipp TD, Zelop C, Cohen A, Repke JT, Lieberman E: Post-cesarean delivery fever and uterine rupture in a subsequent trial of labor. Obstetrics and gynecology 2003, 101(1):136-139.
57
84. Bujold E, Bujold C, Hamilton EF, Harel F, Gauthier RJ: The impact of a single-layer or double-layer closure on uterine rupture. American journal of obstetrics and gynecology 2002, 186(6):1326-1330.
85. Group CC, Abalos E, Addo V, Brocklehurst P, El Sheikh M, Farrell B, Gray S, Hardy P, Juszczak E, Mathews JE et al: Caesarean section surgical techniques: 3 year follow-up of the CORONIS fractional, factorial, unmasked, randomised controlled trial. Lancet 2016, 388(10039):62-72.
86. Osser OV, Jokubkiene L, Valentin L: High prevalence of defects in Cesarean section scars at transvaginal ultrasound examination. Ultrasound in obstetrics & gynecology : the official journal of the International Society of Ultrasound in Obstetrics and Gynecology 2009, 34(1):90-97.
87. Bennich G, Rudnicki M, Wilken-Jensen C, Lousen T, Lassen PD, Wojdemann K: Impact of adding a second layer to a single unlocked closure of a Cesarean uterine incision: randomized controlled trial. Ultrasound in obstetrics & gynecology : the official journal of the International Society of Ultrasound in Obstetrics and Gynecology 2016, 47(4):417-422.
88. Roberge S, Demers S, Girard M, Vikhareva O, Markey S, Chaillet N, Moore L, Paris G, Bujold E: Impact of uterine closure on residual myometrial thickness after cesarean: a randomized controlled trial. American journal of obstetrics and gynecology 2016, 214(4):507 e501-506.
89. Valentin L: Prediction of scar integrity and vaginal birth after caesarean delivery. Best practice & research Clinical obstetrics & gynaecology 2013, 27(2):285-295.
90. Fukuda M, Fukuda K, Shimizu T, Bujold E: Ultrasound Assessment of Lower Uterine Segment Thickness During Pregnancy, Labour, and the Postpartum Period. Journal of obstetrics and gynaecology Canada : JOGC = Journal d'obstetrique et gynecologie du Canada : JOGC 2016, 38(2):134-140.
91. Harper LM, Cahill AG, Roehl KA, Odibo AO, Stamilio DM, Macones GA: The pattern of labor preceding uterine rupture. American journal of obstetrics and gynecology 2012, 207(3):210 e211-216.
92. Hamilton EF, Bujold E, McNamara H, Gauthier R, Platt RW: Dystocia among women with symptomatic uterine rupture. American journal of obstetrics and gynecology 2001, 184(4):620-624.
93. Ouzounian JG, Quist-Nelson J, Miller DA, Korst LM: Maternal and fetal signs and symptoms associated with uterine rupture in women with prior cesarean delivery. The journal of maternal-fetal & neonatal medicine : the official journal of the European Association of Perinatal Medicine, the Federation of Asia and Oceania Perinatal Societies, the International Society of Perinatal Obstet 2014:1-8.
94. Ayres AW, Johnson TR, Hayashi R: Characteristics of fetal heart rate tracings prior to uterine rupture. International journal of gynaecology and obstetrics: the official organ of the International Federation of Gynaecology and Obstetrics 2001, 74(3):235-240.
95. Andersen MM, Thisted DL, Amer-Wahlin I, Krebs L, Danish CTGMdVsg: Can Intrapartum Cardiotocography Predict Uterine Rupture among Women with Prior Caesarean Delivery?: A Population Based Case-Control Study. PloS one 2016, 11(2):e0146347.
58
96. Sheiner E, Levy A, Ofir K, Hadar A, Shoham-Vardi I, Hallak M, Katz M, Mazor M: Changes in fetal heart rate and uterine patterns associated with uterine rupture. The Journal of reproductive medicine 2004, 49(5):373-378.
97. Vachon-Marceau C, Demers S, Goyet M, Gauthier R, Roberge S, Chaillet N, Laroche J, Bujold E: Labor Dystocia and the Risk of Uterine Rupture in Women with Prior Cesarean. American journal of perinatology 2016, 33(6):577-583.
98. Practice Committee of the American Society for Reproductive M, Society of Reproductive S: Pathogenesis, consequences, and control of peritoneal adhesions in gynecologic surgery. Fertility and sterility 2007, 88(1):21-26.
99. Menzies D: Postoperative adhesions: their treatment and relevance in clinical practice. Annals of the Royal College of Surgeons of England 1993, 75(3):147-153.
100. Lower AM, Hawthorn RJ, Ellis H, O'Brien F, Buchan S, Crowe AM: The impact of adhesions on hospital readmissions over ten years after 8849 open gynaecological operations: an assessment from the Surgical and Clinical Adhesions Research Study. BJOG : an international journal of obstetrics and gynaecology 2000, 107(7):855-862.
101. Andolf E, Thorsell M, Kallen K: Cesarean delivery and risk for postoperative adhesions and intestinal obstruction: a nested case-control study of the Swedish Medical Birth Registry. American journal of obstetrics and gynecology 2010, 203(4):406 e401-406.
102. Ellis CN, Boggs HW, Jr., Slagle GW, Cole PA: Small bowel obstruction after colon resection for benign and malignant diseases. Diseases of the colon and rectum 1991, 34(5):367-371.
103. Al-Took S, Platt R, Tulandi T: Adhesion-related small-bowel obstruction after gynecologic operations. American journal of obstetrics and gynecology 1999, 180(2 Pt 1):313-315.
104. Moore J, Kennedy S: Causes of chronic pelvic pain. Bailliere's best practice & research Clinical obstetrics & gynaecology 2000, 14(3):389-402.
105. Nisenblat V, Barak S, Griness OB, Degani S, Ohel G, Gonen R: Maternal complications associated with multiple cesarean deliveries. Obstetrics and gynecology 2006, 108(1):21-26.
106. Tulandi T, Agdi M, Zarei A, Miner L, Sikirica V: Adhesion development and morbidity after repeat cesarean delivery. American journal of obstetrics and gynecology 2009, 201(1):56 e51-56.
107. Phipps MG, Watabe B, Clemons JL, Weitzen S, Myers DL: Risk factors for bladder injury during cesarean delivery. Obstetrics and gynecology 2005, 105(1):156-160.
108. Rooney CM, Crawford AT, Vassallo BJ, Kleeman SD, Karram MM: Is previous cesarean section a risk for incidental cystotomy at the time of hysterectomy? A case-controlled study. American journal of obstetrics and gynecology 2005, 193(6):2041-2044.
109. Boukerrou M, Lambaudie E, Collinet P, Crepin G, Cosson M: A history of cesareans is a risk factor in vaginal hysterectomies. Acta obstetricia et gynecologica Scandinavica 2003, 82(12):1135-1139.
110. Wang L, Merkur H, Hardas G, Soo S, Lujic S: Laparoscopic hysterectomy in the presence of previous caesarean section: a review of one hundred forty-one cases in the Sydney West Advanced Pelvic Surgery Unit. Journal of minimally invasive gynecology 2010, 17(2):186-191.
59
111. Uygur D, Gun O, Kelekci S, Ozturk A, Ugur M, Mungan T: Multiple repeat caesarean section: is it safe? European journal of obstetrics, gynecology, and reproductive biology 2005, 119(2):171-175.
112. Sikirica V, Broder MS, Chang E, Hinoul P, Robinson D, Wilson M: Clinical and economic impact of adhesiolysis during repeat cesarean delivery. Acta obstetricia et gynecologica Scandinavica 2012, 91(6):719-725.
113. Shi Z, Ma L, Yang Y, Wang H, Schreiber A, Li X, Tai S, Zhao X, Teng J, Zhang L et al: Adhesion formation after previous caesarean section-a meta-analysis and systematic review. BJOG : an international journal of obstetrics and gynaecology 2011, 118(4):410-422.
114. Kapustian V, Anteby EY, Gdalevich M, Shenhav S, Lavie O, Gemer O: Effect of closure versus nonclosure of peritoneum at cesarean section on adhesions: a prospective randomized study. American journal of obstetrics and gynecology 2012, 206(1):56 e51-54.
115. Blumenfeld YJ, Caughey AB, El-Sayed YY, Daniels K, Lyell DJ: Single- versus double-layer hysterotomy closure at primary caesarean delivery and bladder adhesions. BJOG : an international journal of obstetrics and gynaecology 2010, 117(6):690-694.
116. Herzberger EH, Alon H, Hershko-Klement A, Ganor-Paz Y, Fejgin MD, Biron-Shental T: Adhesions at repeat cesarean delivery: is there a personal impact? Archives of gynecology and obstetrics 2015, 292(4):813-818.
117. Salim R, Kadan Y, Nachum Z, Edelstein S, Shalev E: Abdominal scar characteristics as a predictor of intra-abdominal adhesions at repeat cesarean delivery. Fertility and sterility 2008, 90(6):2324-2327.
118. Lundorff P, Brolmann H, Koninckx PR, Mara M, Wattiez A, Wallwiener M, Trew G, Crowe AM, De Wilde RL, Anti-Adhesions in Gynaecology Expert P: Predicting formation of adhesions after gynaecological surgery: development of a risk score. Archives of gynecology and obstetrics 2015, 292(4):931-938.
119. Fortin CN, Saed GM, Diamond MP: Predisposing factors to post-operative adhesion development. Human reproduction update 2015, 21(4):536-551.
120. Mowers EL, Lim CS, Skinner B, Mahnert N, Kamdar N, Morgan DM, As-Sanie S: Prevalence of Endometriosis During Abdominal or Laparoscopic Hysterectomy for Chronic Pelvic Pain. Obstetrics and gynecology 2016, 127(6):1045-1053.
121. Moro F, Mavrelos D, Pateman K, Holland T, Hoo WL, Jurkovic D: Prevalence of pelvic adhesions on ultrasound examination in women with a history of Cesarean section. Ultrasound in obstetrics & gynecology : the official journal of the International Society of Ultrasound in Obstetrics and Gynecology 2015, 45(2):223-228.
122. Register [http://www.socialstyrelsen.se/register] 123. Center for Epidemiology, National Board of Health and Welfare: Evaluation
of the Swedish Medical Birth Register. Stockholm, Sweden; 2002. 124. Cnattingius S, Ericson A, Gunnarskog J, Kallen B: A quality study of a
medical birth registry. Scandinavian journal of social medicine 1990, 18(2):143-148.
125. Center for Epidemiology, National Board of Health and Welfare: The Swedish Version of 10th Revision of WHO International classification of Diseases.Stockholm, Sweden;1997.
60
126. Centre for Epidemiology, National Board of Health and Welfare: The National Patient Register. (Article no 2003-42-8). Stockholm, Sweden;2003.
127. Ludvigsson JF, Andersson E, Ekbom A, Feychting M, Kim JL, Reuterwall C, Heurgren M, Olausson PO: External review and validation of the Swedish national inpatient register. BMC public health 2011, 11:450.
128. Ladfors MB, Lofgren ME, Gabriel B, Olsson JH: Patient accept questionnaires integrated in clinical routine: a study by the Swedish National Register for Gynecological Surgery. Acta obstetricia et gynecologica Scandinavica 2002, 81(5):437-442.
129. Hesselman S HU, Råssjö E-B, Jonsson M: Warning signs of uterine rupture after previous caesarean section:a case review. COGRM 2016, 2(3):170-174.
130. Cheong YC, Premkumar G, Metwally M, Peacock JL, Li TC: To close or not to close? A systematic review and a meta-analysis of peritoneal non-closure and adhesion formation after caesarean section. European journal of obstetrics, gynecology, and reproductive biology 2009, 147(1):3-8.
131. Kumakiri J, Kikuchi I, Kitade M, Kuroda K, Matsuoka S, Tokita S, Takeda S: Incidence of complications during gynecologic laparoscopic surgery in patients after previous laparotomy. Journal of minimally invasive gynecology 2010, 17(4):480-486.
132. Makinen J, Brummer T, Jalkanen J, Heikkinen AM, Fraser J, Tomas E, Harkki P, Sjoberg J: Ten years of progress--improved hysterectomy outcomes in Finland 1996-2006: a longitudinal observation study. BMJ open 2013, 3(10):e003169.
133. Andersson RE: Small bowel obstruction after appendicectomy. The British journal of surgery 2001, 88(10):1387-1391.
134. Wilson JA, Clark JJ: Obesity: impediment to postsurgical wound healing. Advances in skin & wound care 2004, 17(8):426-435.
135. Stamilio DM, Scifres CM: Extreme obesity and postcesarean maternal complications. Obstetrics and gynecology 2014, 124(2 Pt 1):227-232.
136. Bohlin KS, Ankardal M, Stjerndahl JH, Lindkvist H, Milsom I: Influence of the modifiable life-style factors body mass index and smoking on the outcome of hysterectomy. Acta obstetricia et gynecologica Scandinavica 2016, 95(1):65-73.
137. Smid MC, Vladutiu CJ, Dotters-Katz SK, Boggess KA, Manuck TA, Stamilio DM: Maternal obesity and major intraoperative complications during cesarean delivery. American journal of obstetrics and gynecology 2017, 216(6):614 e611-614 e617.
138. Kjaergaard H, Olsen J, Ottesen B, Nyberg P, Dykes AK: Obstetric risk indicators for labour dystocia in nulliparous women: a multi-centre cohort study. BMC pregnancy and childbirth 2008, 8:45.
139. Cahill AG, Odibo AO, Allsworth JE, Macones GA: Frequent epidural dosing as a marker for impending uterine rupture in patients who attempt vaginal birth after cesarean delivery. American journal of obstetrics and gynecology 2010, 202(4):355 e351-355.
140. Wallis CJ, Cheung DC, Garbens A, Kroft J, Carr L, Nathens AB, Po L, Nam RK, Liu G, Gien L et al: Occurrence of and Risk Factors for Urological Intervention During Benign Hysterectomy: Analysis of the National Surgical Quality Improvement Program Database. Urology 2016, 97:66-72.
61
141. Babu K, Magon N: Uterine closure in cesarean delivery: a new technique. North American journal of medical sciences 2012, 4(8):358-361.
142. Macones GA, Cahill AG, Stamilio DM, Odibo A, Peipert J, Stevens EJ: Can uterine rupture in patients attempting vaginal birth after cesarean delivery be predicted? American journal of obstetrics and gynecology 2006, 195(4):1148-1152.
143. Smith GC, White IR, Pell JP, Dobbie R: Predicting cesarean section and uterine rupture among women attempting vaginal birth after prior cesarean section. PLoS medicine 2005, 2(9):e252.
144. Fagerberg MC, Marsal K, Ekstrom P, Kallen K: Indications for first caesarean and delivery mode in subsequent trial of labour. Paediatric and perinatal epidemiology 2013, 27(1):72-80.
145. Chang WC, Hsu WC, Sheu BC, Huang SC, Torng PL, Chang DY: Minimizing bladder injury in laparoscopically assisted vaginal hysterectomy among women with previous cesarean sections. Surgical endoscopy 2008, 22(1):171-176.
146. Aarts JW, Nieboer TE, Johnson N, Tavender E, Garry R, Mol BW, Kluivers KB: Surgical approach to hysterectomy for benign gynaecological disease. The Cochrane database of systematic reviews 2015(8):CD003677.
147. van 't Hooft J, Duffy JM, Daly M, Williamson PR, Meher S, Thom E, Saade GR, Alfirevic Z, Mol BW, Khan KS et al: A Core Outcome Set for Evaluation of Interventions to Prevent Preterm Birth. Obstetrics and gynecology 2016, 127(1):49-58.
148. Blomberg M: Avoiding the first cesarean section--results of structured organizational and cultural changes. Acta obstetricia et gynecologica Scandinavica 2016, 95(5):580-586.

Acta Universitatis UpsaliensisDigital Comprehensive Summaries of Uppsala Dissertationsfrom the Faculty of Medicine 1358
Editor: The Dean of the Faculty of Medicine
A doctoral dissertation from the Faculty of Medicine, UppsalaUniversity, is usually a summary of a number of papers. A fewcopies of the complete dissertation are kept at major Swedishresearch libraries, while the summary alone is distributedinternationally through the series Digital ComprehensiveSummaries of Uppsala Dissertations from the Faculty ofMedicine. (Prior to January, 2005, the series was publishedunder the title “Comprehensive Summaries of UppsalaDissertations from the Faculty of Medicine”.)
Distribution: publications.uu.seurn:nbn:se:uu:diva-327934
ACTAUNIVERSITATIS
UPSALIENSISUPPSALA
2017