Cad 3
45
Copyright © 2013, 2010, 2006, 2002 by Saunders, an imprint of Elsevier Inc. Chapter 40 Care of Patients with Acute Coronary Syndromes
-
Upload
claudia-sanchez -
Category
Documents
-
view
57 -
download
2
description
t
Transcript of Cad 3

Copyright © 2013, 2010, 2006, 2002 by Saunders, an imprint of Elsevier Inc.
Chapter 40
Care of Patients
with Acute Coronary Syndromes

2Copyright © 2013, 2010, 2006, 2002 by Saunders, an imprint of Elsevier Inc.
Learning Outcomes
Compare and contrast the clinical manifestations of stable angina and unstable angina.
Prioritize nursing care for patients with chest pain. Describe the etiology, pathophysiology, clinical
manifestations, diagnostic findings, complications,
collaborative care, and nursing management for patients with coronary artery disease (CAD) and chronic stable angina.
Develop a plan of care for the patient who has a
percutaneous coronary angioplasty (PTCA). Develop a teaching plan for patients at risk for CAD
regarding cardiovascular risk modification programs and lifestyle changes.

3Copyright © 2013, 2010, 2006, 2002 by Saunders, an imprint of Elsevier Inc.
Coronary Artery Disease
Includes stable angina, acute coronary syndromes
Ischemia—insufficient oxygen supply to meet requirements of myocardium
Infarction—necrosis or cell death that occurs when severe ischemia is prolonged and decreased perfusion causes irreversible damage to tissue

4Copyright © 2013, 2010, 2006, 2002 by Saunders, an imprint of Elsevier Inc.
Chronic Stable Angina (CSA) Pectoris
“Strangling of the chest” Temporary imbalance between coronary
artery’s ability to supply oxygen and cardiac muscle’s demand for oxygen
5Copyright © 2013, 2010, 2006, 2002 by Saunders, an imprint of Elsevier Inc.
Chronic Stable Angina (CSA) Pectoris (cont’d)
Ischemia limited in duration and does not cause permanent damage to myocardial tissue
Chronic stable angina Unstable angina

6Copyright © 2013, 2010, 2006, 2002 by Saunders, an imprint of Elsevier Inc.
Acute Coronary Syndrome (ACS)
Patients who present with either unstable angina or acute myocardial infarction
Believed that atherosclerotic plaque in coronary artery ruptures, resulting in platelet aggregation, thrombus formation or vasoconstriction
7Copyright © 2013, 2010, 2006, 2002 by Saunders, an imprint of Elsevier Inc.
Unstable Angina Pectoris
New-onset angina Variant (Prinzmetal’s) angina Pre-infarction angina Patients present with ST changes on 12-lead
ECG, but will not have changes in troponin or CK levels

8Copyright © 2013, 2010, 2006, 2002 by Saunders, an imprint of Elsevier Inc.
Nonmodifiable Risk Factors
Age Gender Family history Ethnic background

9Copyright © 2013, 2010, 2006, 2002 by Saunders, an imprint of Elsevier Inc.
Modifiable Risk Factors
Elevated serum cholesterol Cigarette smoking Hypertension Impaired glucose tolerance/DM Obesity Excessive alcohol Limited physical activity Stress
10Copyright © 2013, 2010, 2006, 2002 by Saunders, an imprint of Elsevier Inc.
Laboratory Assessment
Troponin T and troponin I Creatine kinase-MB (CK-MB) Myoglobin Imaging assessment 12-lead electrocardiograms Cardiac catheterization

11Copyright © 2013, 2010, 2006, 2002 by Saunders, an imprint of Elsevier Inc.
Pathophysiology of Atherosclerosis

12Copyright © 2013, 2010, 2006, 2002 by Saunders, an imprint of Elsevier Inc.
Progression of Atherosclerosis
Fig. 34-2Fig. 34-2

13Copyright © 2013, 2010, 2006, 2002 by Saunders, an imprint of Elsevier Inc.
Clinical Manifestations
• Symptoms are due to myocardial ischemia• Symptoms and complications are related to the
location and degree of vessel obstruction• Angina pectoris • Myocardial infarction• Heart failure• Sudden cardiac death

14Copyright © 2013, 2010, 2006, 2002 by Saunders, an imprint of Elsevier Inc.
The most common symptom of myocardial ischemia is chest pain; however, some individuals may be asymptomatic or have atypical symptoms such as weakness, dyspnea, and nausea.Atypical symptoms are more common in women and in persons who are older, or who have a history of heart failure or diabetes.

15Copyright © 2013, 2010, 2006, 2002 by Saunders, an imprint of Elsevier Inc.
Angina Pectoris
• A syndrome characterized by episodes or paroxysmal pain or pressure in the anterior chest caused by insufficient coronary blood flow.
• Physical exertion or emotional stress increases myocardial oxygen demand and the coronary vessels are unable to supply sufficient blood flow to meet the oxygen demand.

16Copyright © 2013, 2010, 2006, 2002 by Saunders, an imprint of Elsevier Inc.
Angina pain varies from mild to severe
• May be described as tightness, choking, or a heavy sensation.
• Frequently retrosternal and may radiate to neck, jaw, shoulders, back or arms (usually left).
• Anxiety frequently accompanies the pain.
• Other symptoms may occur: dyspnea/shortness of breath, dizziness, nausea, and vomiting.

17Copyright © 2013, 2010, 2006, 2002 by Saunders, an imprint of Elsevier Inc.
Location of Chest Pain (Angina)
Fig. 34-7

18Copyright © 2013, 2010, 2006, 2002 by Saunders, an imprint of Elsevier Inc.
Nursing Process: The Care of the Patient with Angina Pectoris—Assessment
Symptoms and activities, especially those that precede and precipitate attacks
Risk factors, lifestyle, and health promotion activities
Patient and family knowledge Adherence to the plan of care

19Copyright © 2013, 2010, 2006, 2002 by Saunders, an imprint of Elsevier Inc.
Nursing Process: The Care of the Patient with Angina Pectoris—Diagnoses
Ineffective cardiac tissue perfusion Death anxiety Deficient knowledge Noncompliance, ineffective management of
therapeutic regimen

20Copyright © 2013, 2010, 2006, 2002 by Saunders, an imprint of Elsevier Inc.
Collaborative Problems Acute pulmonary edema Heart failure Cardiogenic shock Dysrhythmias and cardiac arrest Myocardial infarction

21Copyright © 2013, 2010, 2006, 2002 by Saunders, an imprint of Elsevier Inc.
Nursing Process: The Care of the Patient with Angina Pectoris—Planning
Goals include immediate and appropriate treatment of angina prevention of angina reduction of anxiety awareness of the disease process understanding of prescribed care adherence to the self-care program absence of complications.

22Copyright © 2013, 2010, 2006, 2002 by Saunders, an imprint of Elsevier Inc.
Treatment
Treatment seeks to decrease myocardial oxygen demand and increase oxygen supply Medications Oxygen
Reduce and control risk factors Reperfusion therapy may also be done

23Copyright © 2013, 2010, 2006, 2002 by Saunders, an imprint of Elsevier Inc.
Treatment of Angina Pain Treatment of angina pain is a priority nursing concern. Patient is to stop all activity and sit or rest in bed. Assess the patient while performing other necessary
interventions. Assessment includes VS, and observation for respiratory distress, and assessment of pain. In the hospital setting, the ECG is assessed or obtained.
Administer oxygen. Administer medications as ordered or by protocol,
usually NTG. MONA

24Copyright © 2013, 2010, 2006, 2002 by Saunders, an imprint of Elsevier Inc.
Pain Management
Nitroglycerin Morphine sulfate Oxygen Position of comfort; semi-Fowler’s position Quiet and calm environment

25Copyright © 2013, 2010, 2006, 2002 by Saunders, an imprint of Elsevier Inc.
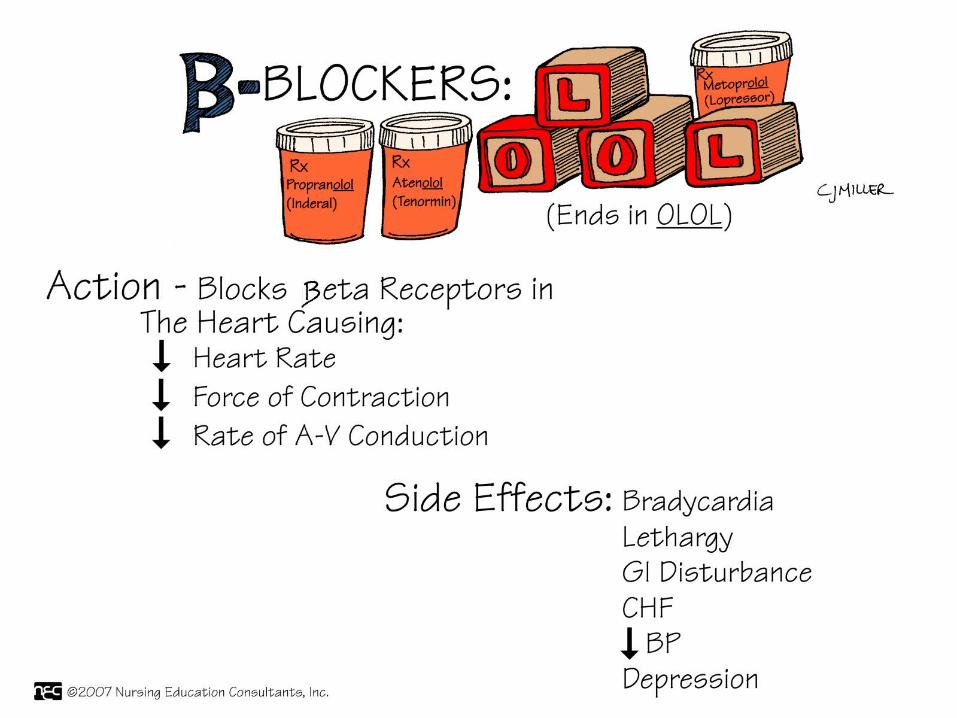
Medications
• Nitroglycerin• Beta-adrenergic blocking agents• Calcium channel blocking agents• Antiplatelet and anticoagulant medications
• Aspirin• Clopidogrel and ticlopidine• HeparinKNOW THE PHYSIOLOGIC ACTION OF THESE
MEDICATIONS, THE MOST COMMON SIDE EFFECTS, AND THE NURSING IMPLICATIONS

26Copyright © 2013, 2010, 2006, 2002 by Saunders, an imprint of Elsevier Inc.
27Copyright © 2013, 2010, 2006, 2002 by Saunders, an imprint of Elsevier Inc.

28Copyright © 2013, 2010, 2006, 2002 by Saunders, an imprint of Elsevier Inc.
Ineffective Tissue Perfusion (Cardiopulmonary)
Interventions: Drug therapy (aspirin, thrombolytic agents) Restoration of perfusion to injured area limits
amount of extension, improves left ventricular function
Complete sustained reperfusion of coronary arteries in first few hours after MI has decreased mortality

29Copyright © 2013, 2010, 2006, 2002 by Saunders, an imprint of Elsevier Inc.
Thrombolytic Therapy
Fibrinolytics dissolve thrombi in coronary arteries, restore myocardial blood flow Tissue plasminogen activator Reteplase Tenecteplase

30Copyright © 2013, 2010, 2006, 2002 by Saunders, an imprint of Elsevier Inc.
Other Drug Therapies
Glycoprotein (GP) IIB/IIIa inhibitors Once-a-day beta blockers ACE inhibitors or angiotensin receptor
blockers Calcium channel blockers Ranolazine (Ranexa)

31Copyright © 2013, 2010, 2006, 2002 by Saunders, an imprint of Elsevier Inc.
Reperfusion Therapy
Myocardial tissue can become increasingly ischemic and necrotic
Thrombolytic therapy using fibrinolytics dissolves thrombi in the coronary arteries and restores myocardial blood flow

32Copyright © 2013, 2010, 2006, 2002 by Saunders, an imprint of Elsevier Inc.
Percutaneous Transluminal Coronary Angioplasty
Clopidogrel before procedure IV heparin after procedure IV or intracoronary nitroglycerin or diltiazem Possible IV GP IIb/IIIa inhibitors Long-term therapy, antiplatelet therapy, beta
blocker, ACE inhibitor, or ARB

33Copyright © 2013, 2010, 2006, 2002 by Saunders, an imprint of Elsevier Inc.
Percutaneous Transluminal Coronary Angioplasty (cont’d)

34Copyright © 2013, 2010, 2006, 2002 by Saunders, an imprint of Elsevier Inc.
Other Procedures
Arthrectomy Stents Rheolytic thrombectomy

35Copyright © 2013, 2010, 2006, 2002 by Saunders, an imprint of Elsevier Inc.
Coronary Stent
http://www.youtube.com/watch?v=N7nghr9TpSU

36Copyright © 2013, 2010, 2006, 2002 by Saunders, an imprint of Elsevier Inc.
Coronary Artery Bypass Graft Surgery

37Copyright © 2013, 2010, 2006, 2002 by Saunders, an imprint of Elsevier Inc.
Community-Based Care
Home care management Teaching for self-management Health care resources

38Copyright © 2013, 2010, 2006, 2002 by Saunders, an imprint of Elsevier Inc.
Patient Teaching
• Lifestyle changes and reduction of risk factors • Explore, recognize, and adapt behaviors to
avoid to reduce the incidence of episodes of ischemia
• Teaching regarding disease process• Medications• Stress reduction• When to seek emergency care

39Copyright © 2013, 2010, 2006, 2002 by Saunders, an imprint of Elsevier Inc.
Paramedics arrive at the ED with a 78-year-old man who presents with severe chest pains. In triage, he reports that he experienced chest pains for several hours before calling 911. He reports that he takes “heart medications” but he does not know their names. He describes his chest pain as a 9 on a 0-to-10 scale. Patient history includes an MI 6 years ago that resulted in stent placement for severe CAD. One stent was placed in the LAD and another in his circumflex artery. He states that his health care provider told him he also has heart failure.
What laboratory tests do you anticipate the provider will order for this patient?

40Copyright © 2013, 2010, 2006, 2002 by Saunders, an imprint of Elsevier Inc.
(cont’d)
Two hours later, the patient is admitted to the cardiac stepdown unit with orders for a saline lock, cardiac diet, and oxygen at 2 L per nasal cannula with follow-up cardiac enzymes, and 12-lead ECG in 6 hours. One hour later, the patient reports severe shortness of breath. His oxygen saturation has dropped to 88%, BP is 96/54, and his monitor shows sinus tachycardia with a rate of 114. He reports mild chest pain.
1.What do you suspect is happening to the patient at this time?
2.The patient’s laboratory values include troponin T 0.6 mg/mL. What is your best interpretation of this finding?

41Copyright © 2013, 2010, 2006, 2002 by Saunders, an imprint of Elsevier Inc.
You immediately notify the provider and within 45 minutes, the patient is transferred to the CCU for close monitoring. He is in serious condition and has developed crackles bilaterally, and his chest pain level has increased.
What medications do you anticipate will be ordered for this patient? (Select all that apply.)
A.Furosemide (Lasix)
B.Atenolol (Tenormin)
C.Acetaminophen (Tylenol)
D.Morphine
E.Prednisone (Deltasone)
(cont’d)

42Copyright © 2013, 2010, 2006, 2002 by Saunders, an imprint of Elsevier Inc.
The next morning, the patient is taken to the cardiac catheterization laboratory. The cardiologist finds that there is an 80% blockage in the proximal LAD coronary artery.
Which procedure is most likely to be performed to correct this condition?
A.Coronary artery bypass graft surgery
B.Coronary atherectomy
C.Percutaneous transluminal coronary angioplasty (PTCA)
D.PTCA with coronary artery stent placement
(cont’d)

43Copyright © 2013, 2010, 2006, 2002 by Saunders, an imprint of Elsevier Inc.
The patient’s condition improves and he is returned to the cardiac stepdown unit. He is to be discharged after 6 days in the hospital.
What should you teach him before he is discharged from the hospital?
(cont’d)

44Copyright © 2013, 2010, 2006, 2002 by Saunders, an imprint of Elsevier Inc.
PREGUNTAS???

45Copyright © 2013, 2010, 2006, 2002 by Saunders, an imprint of Elsevier Inc.
If there are no questions . . . .
Let’s have . . . .