Ca thyroid
58
THYROID CARCINOMA BY- SAMPURNA DAS
-
Upload
sampurna-das -
Category
Health & Medicine
-
view
86 -
download
0
Transcript of Ca thyroid

THYROID CARCINOMA
BY- SAMPURNA DAS
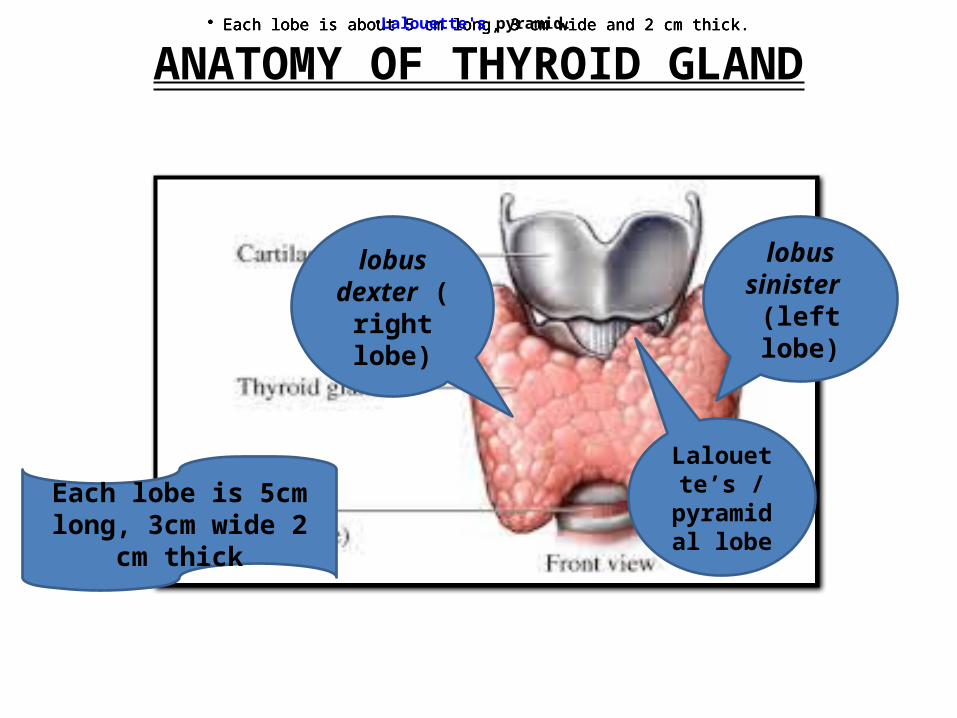
ANATOMY OF THYROID GLAND
lobus dexter (rig
ht lobe)
lobus sinister (le
ft lobe)
Each lobe is 5cm long, 3cm wide 2 cm thick
• Each lobe is about 5 cm long, 3 cm wide and 2 cm thick.• Each lobe is about 5 cm long, 3 cm wide and 2 cm thick.• Each lobe is about 5 cm long, 3 cm wide and 2 cm thick.• Each lobe is about 5 cm long, 3 cm wide and 2 cm thick.
Lalouette’s /
pyramidal lobe
•Lalouette's pyramid.
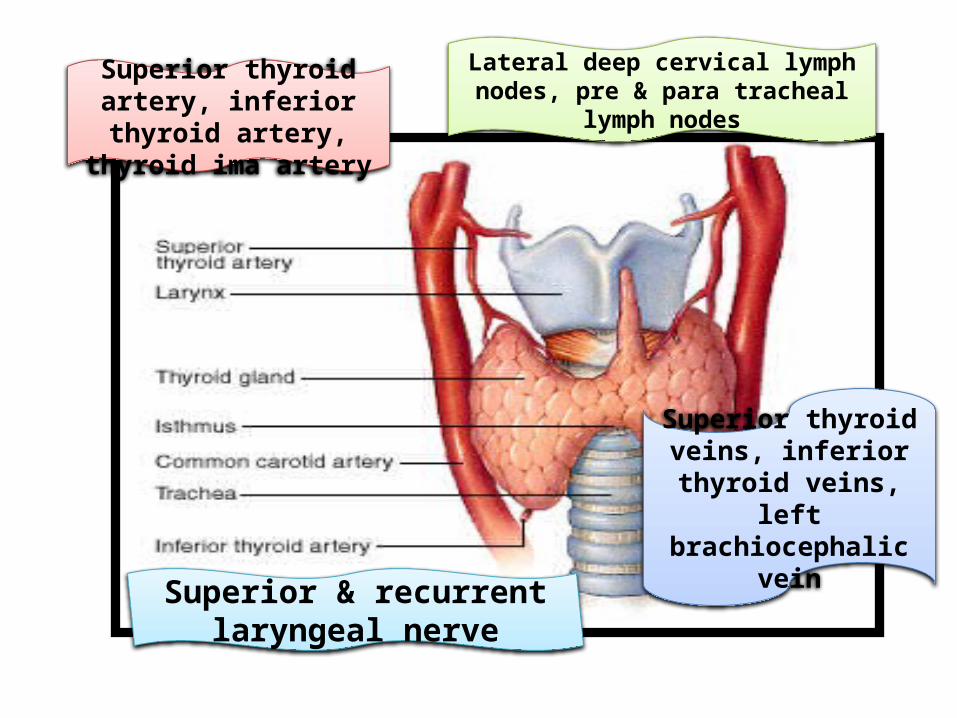
Superior & recurrent laryngeal nerve
Superior thyroid artery, inferior thyroid artery,
thyroid ima artery
Lateral deep cervical lymph nodes, pre & para tracheal lymph nodes
Superior thyroid veins, inferior thyroid veins,
left brachiocephalic vein
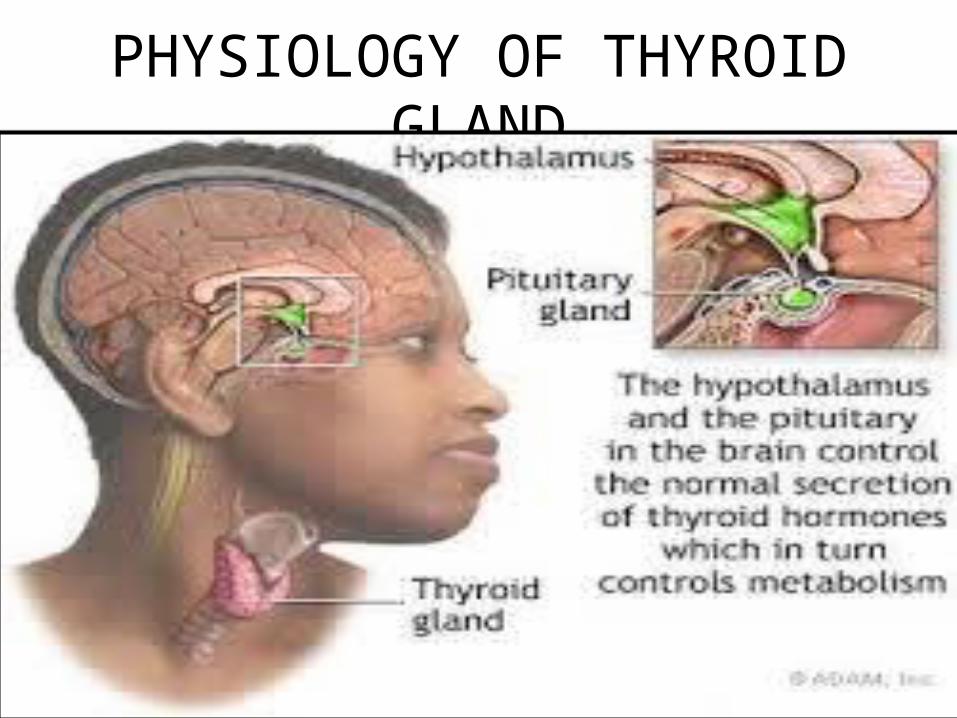
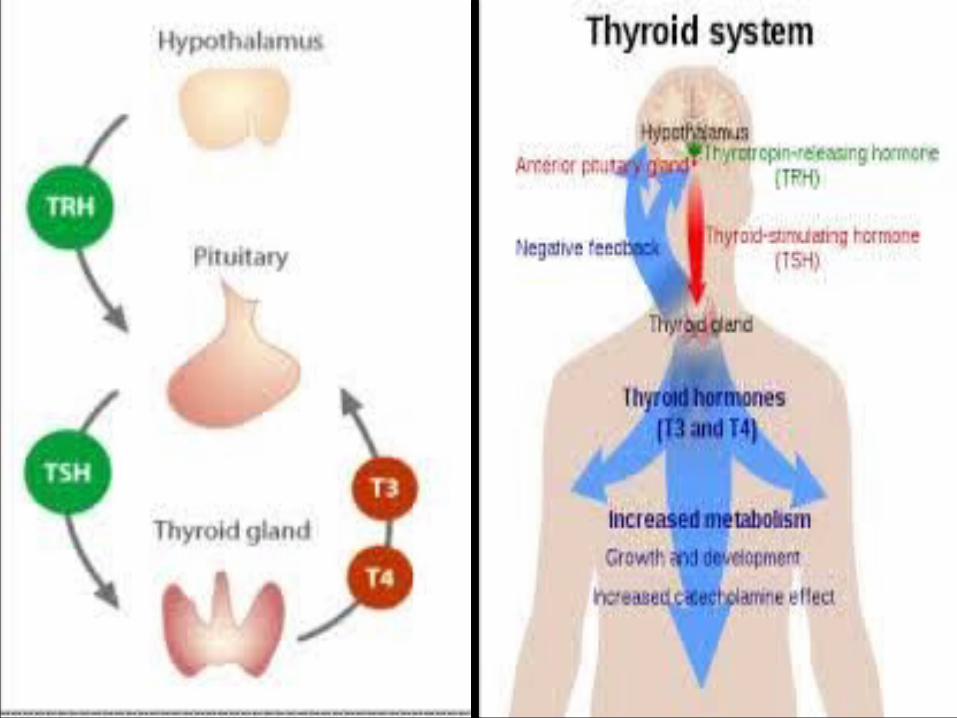
PHYSIOLOGY OF THYROID GLAND
Feature Description
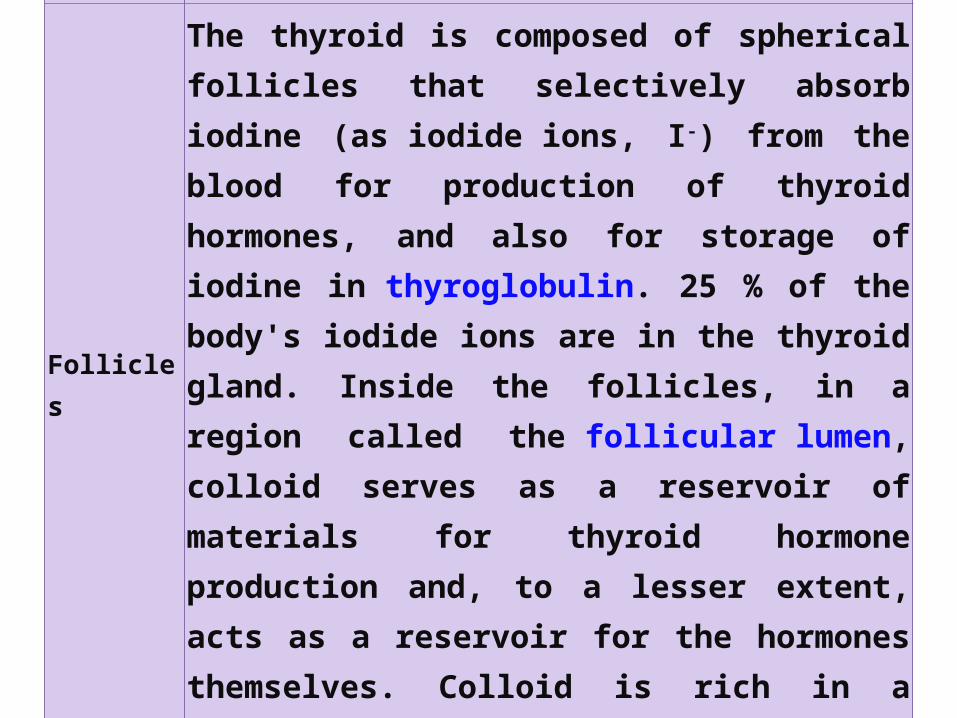
Follicles
The thyroid is composed of spherical follicles that selectively absorb iodine (as iodide ions, I-) from the blood for production of thyroid hormones, and also for storage of iodine in thyroglobulin. 25 % of the body's iodide ions are in the thyroid gland. Inside the follicles, in a region called the follicular lumen, colloid serves as a reservoir of materials for thyroid hormone production and, to a lesser extent, acts as a reservoir for the hormones themselves. Colloid is rich in a protein called thyroglobulin.
Thyroid epithelial cells
(or "follicular cells")
The follicles are surrounded by a single layer of thyroid epithelial cells, which secrete T3 and T4. When the gland is not secreting T3 and T4 (inactive), the epithelial cells range from low columnar to cuboidal cells. When active, the epithelial cells become tall columnar cells.
Parafollicular cells(or "C cells")
Scattered among follicular cells and in spaces between the spherical follicles are another type of thyroid cell, parafollicular cells, which secrete calcitonin.

HISTOLOGY OF THYROID GLAND

CAUSES OF THYROID CANCER
• Environmental exposure to ionizing radiation
• Thyroiditis and other thyroid disease
• Genetic causes include Multiple endocrine neoplasia type 2

PATHOPHYSIOLOGY
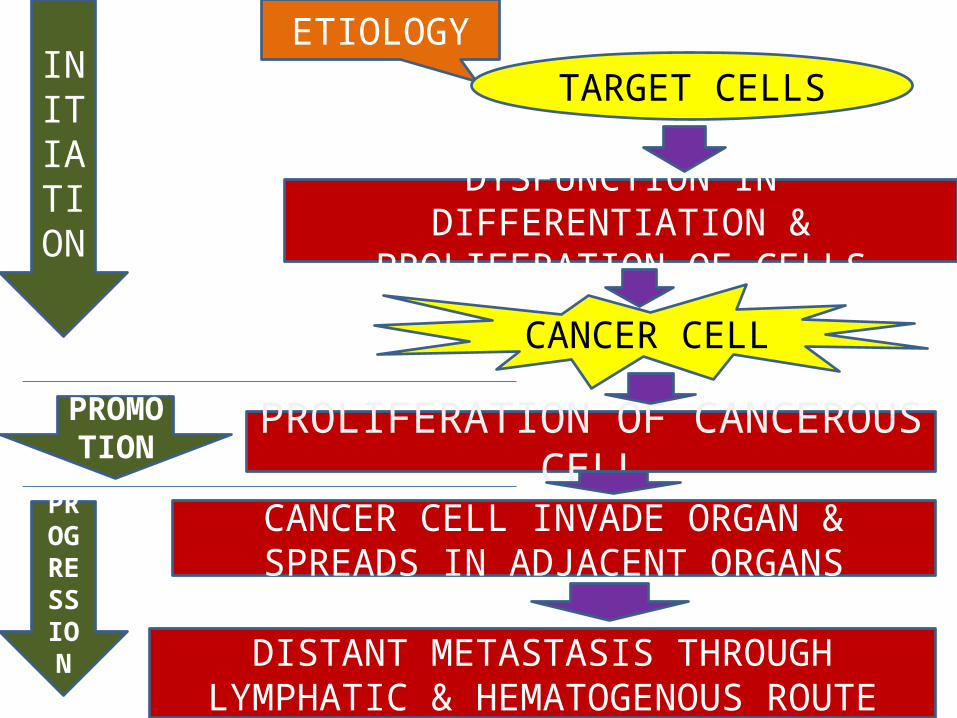
ETIOLOGYTARGET CELLS
DYSFUNCTION IN DIFFERENTIATION & PROLIFERATION OF CELLS
CANCER CELL
PROLIFERATION OF CANCEROUS CELL
CANCER CELL INVADE ORGAN & SPREADS IN ADJACENT ORGANS
DISTANT METASTASIS THROUGH LYMPHATIC & HEMATOGENOUS ROUTE
INITIATION
PROMOTION
PROGRESSION

TNM STAGING
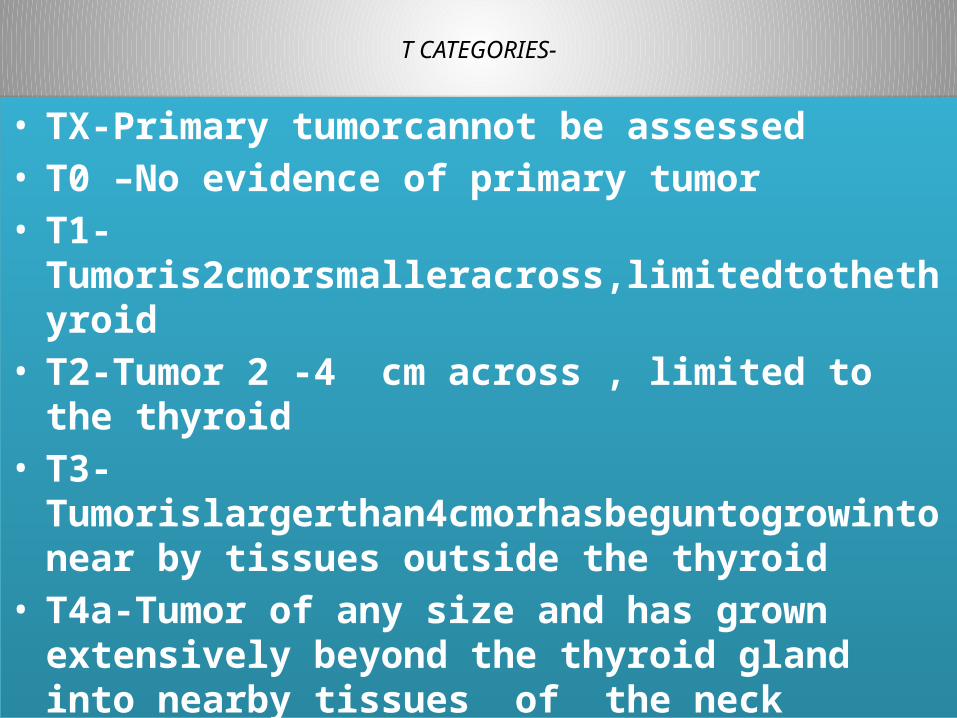
T CATEGORIES-
• TX-Primary tumorcannot be assessed• T0 –No evidence of primary tumor• T1-Tumoris2cmorsmalleracross,limitedtothethyroid• T2-Tumor 2 -4 cm across , limited to the thyroid• T3-Tumorislargerthan4cmorhasbeguntogrowintonear by
tissues outside the thyroid• T4a-Tumor of any size and has grown extensively beyond
the thyroid gland into nearby tissues of the neck• T4b-Tumor has grown either back toward the spine or into
nearby large blood vessels
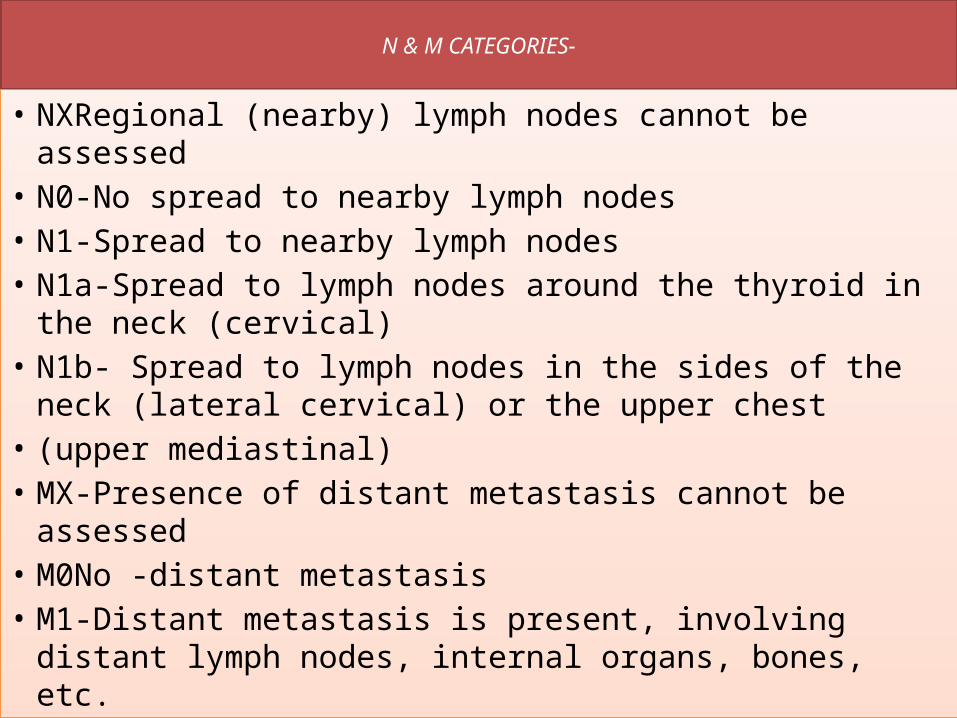
N & M CATEGORIES-
• NXRegional (nearby) lymph nodes cannot be assessed • N0-No spread to nearby lymph nodes • N1-Spread to nearby lymph nodes • N1a-Spread to lymph nodes around the thyroid in the neck (cervical)
• N1b- Spread to lymph nodes in the sides of the neck (lateral cervical) or the upper chest
• (upper mediastinal) • MX-Presence of distant metastasis cannot be assessed • M0No -distant metastasis • M1-Distant metastasis is present, involving distant lymph nodes, internal organs, bones, etc.
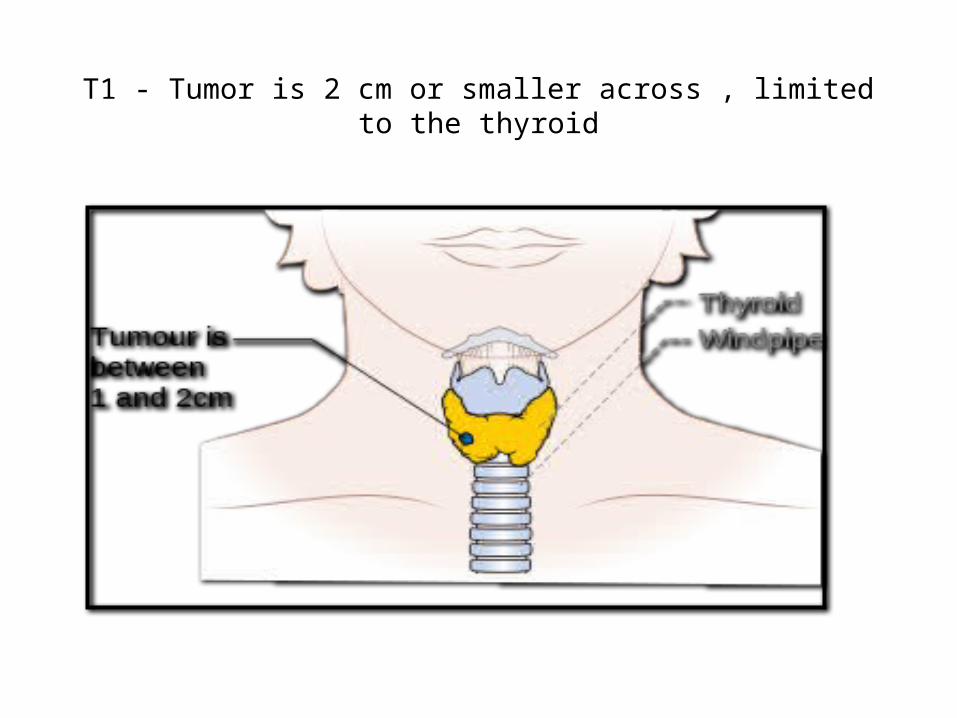
T1 - Tumor is 2 cm or smaller across , limited to the thyroid
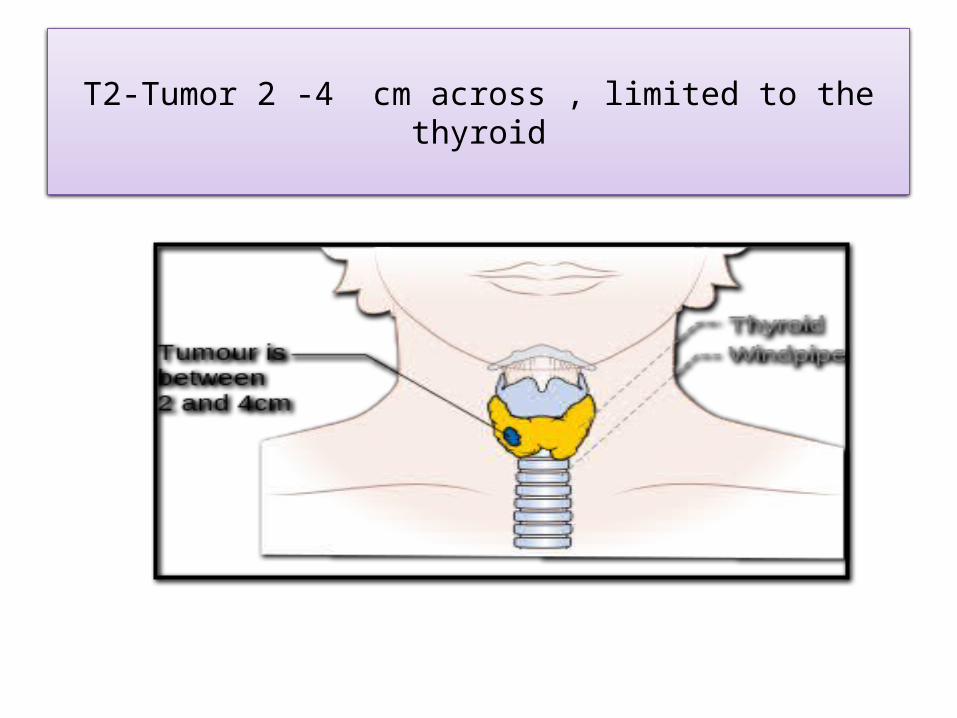
T2-Tumor 2 -4 cm across , limited to the thyroid

T3-Tumor is larger than 4 cm or has begun to grow into near by tissues outside the thyroid

T4a-Tumor of any size and has grown extensively beyond the thyroid gland into nearby tissues of the neck
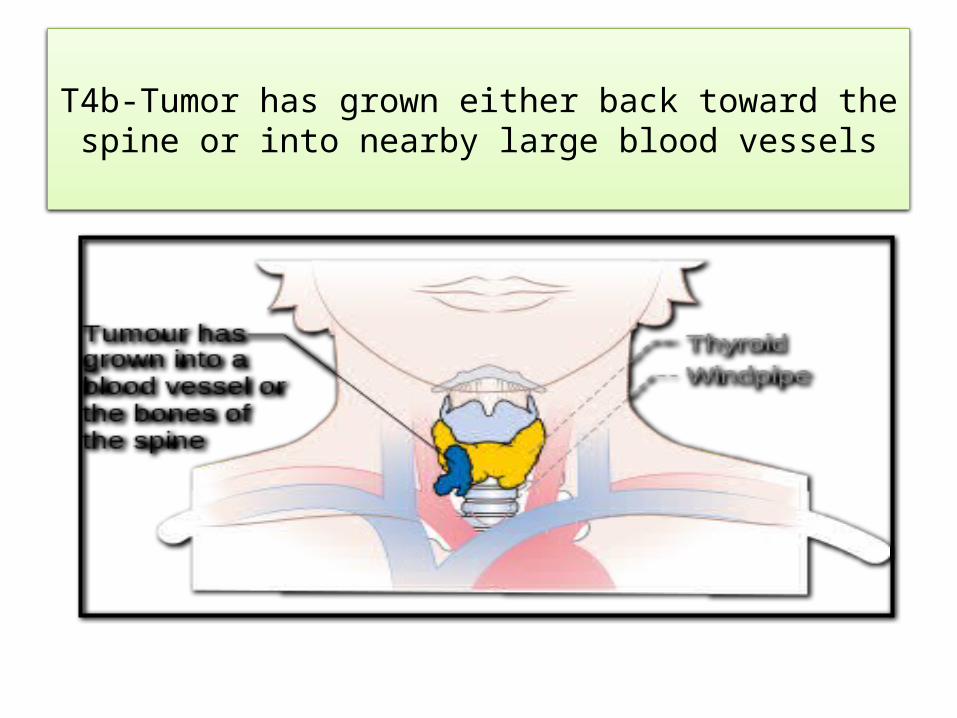
T4b-Tumor has grown either back toward the spine or into nearby large blood vessels
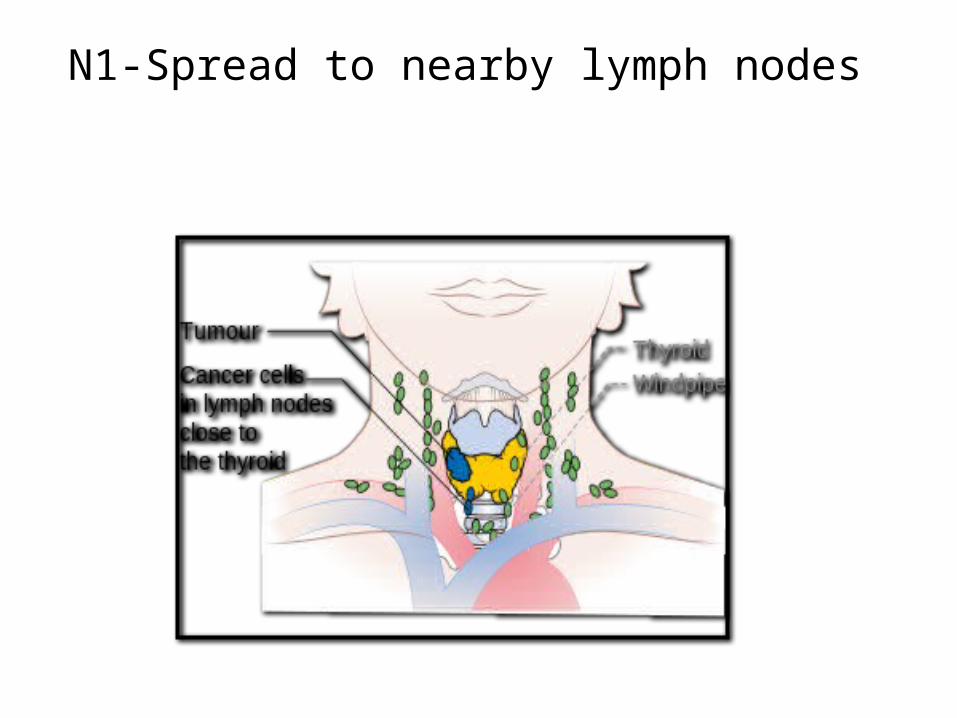
N1-Spread to nearby lymph nodes
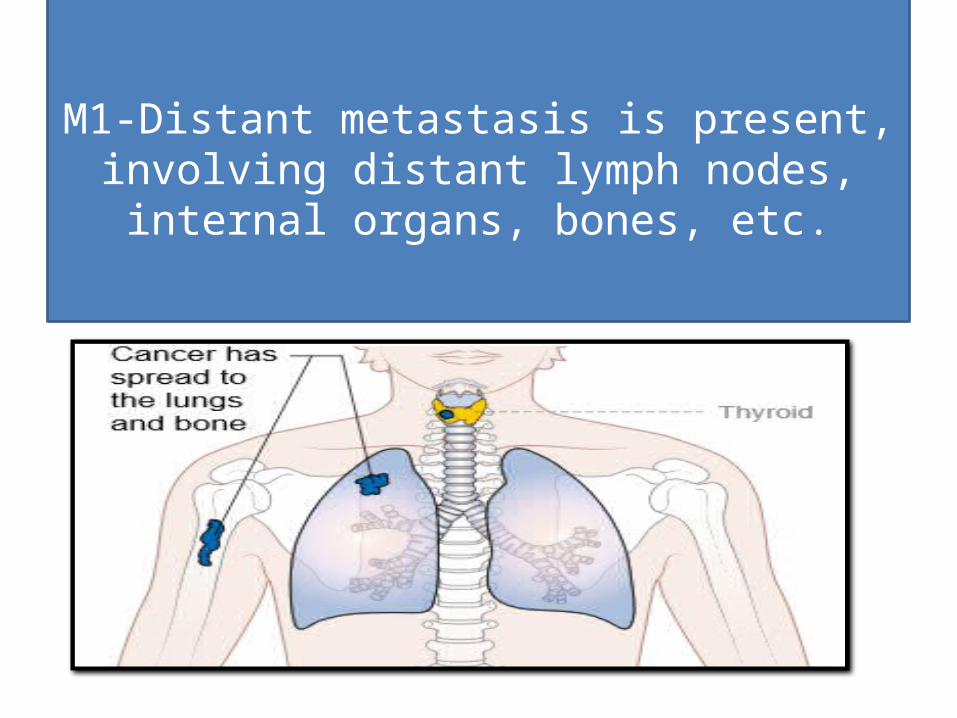
M1-Distant metastasis is present, involving distant lymph nodes, internal
organs, bones, etc.

DIFFERENT TYPES OF THYROID CANCER

TYPE CAUSE CELL OF ORIGIN
MEDULLARY Caused by mutation in the RET proto-oncogene
Parafollicular
FOLLICULAR Tumors tend carry either a RAS mutation or a PAX8-PPARγ1 fusion,
Follicular
ANAPLASTIC p53 gene mutations Follicular
PAPILLARY RET(rearranged during transfection)/ PTC (for papillary thyroid carcinoma) oncogene
Follicular
SIGNS & SYMPTOMS-

• Thyroid nodule• Enlarged lymph node• Pain in the anterior region of the neck• Changes in voice due to an involvement of the recurrent laryngeal
nerve.• Thyroid cancer is usually found in a euthyroid patient, but
symptoms of hyperthyroidism or hypothyroidism may be associated with a large or metastatic well-differentiated tumour.
• Thyroid nodules are of particular concern when they are found in those under the age of 20. The presentation of benign nodules at this age is less likely, and thus the potential for malignancy is far greater.
• The flushing and diarrhea observed in carcinoid syndrome is caused by elevated levels of circulating serotonin.
• flushing, diarrhea, and itching (pruritis) are all caused by elevated levels of calcitonin.
• Enlarged cervical lymph nodes.
DIAGNOSTIC STUDIES-
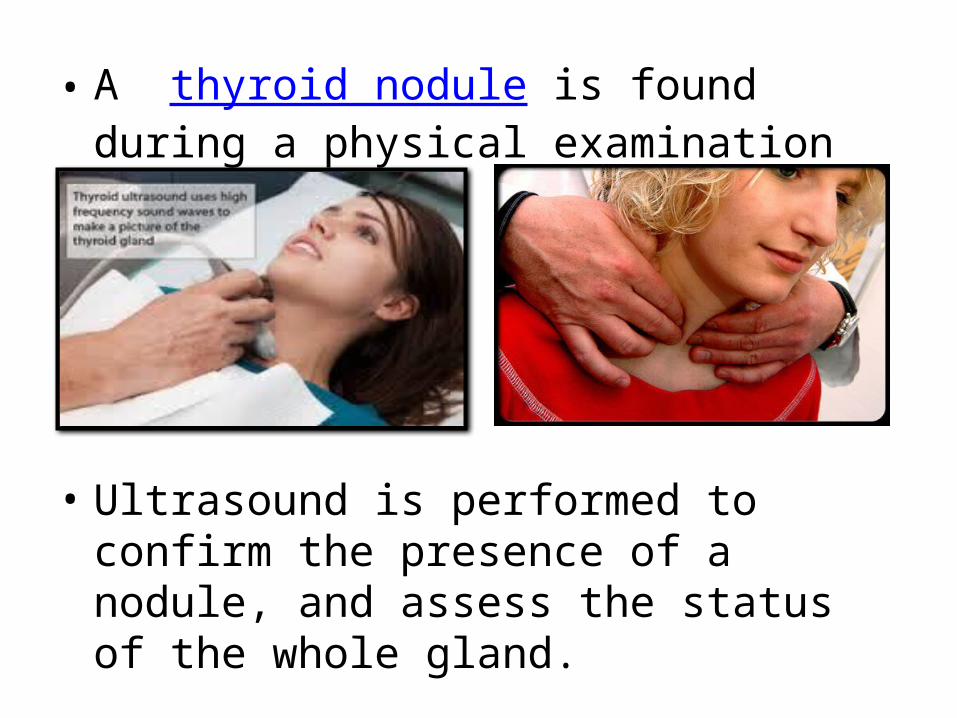
• A thyroid nodule is found during a physical examination
• Ultrasound is performed to confirm the presence of a nodule, and assess the status of the whole gland.
• Measurement of thyroid stimulating hormone and anti-thyroid antibodies will help decide if there is a functional thyroid disease.
• Measurement of calcitonin is necessary to exclude the presence of medullary thyroid cancer
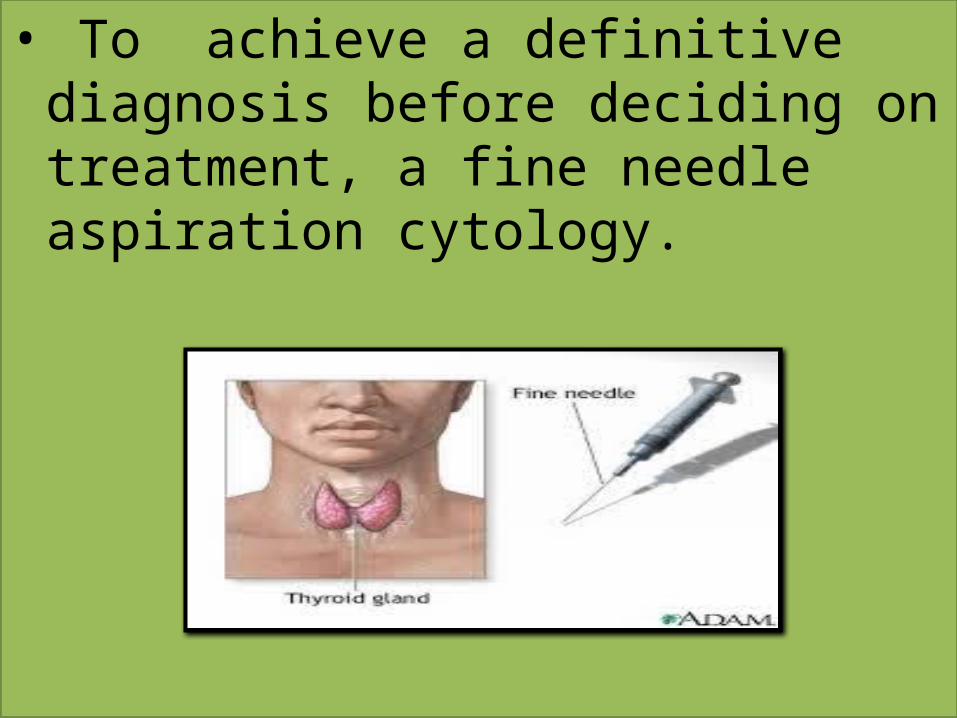
• To achieve a definitive diagnosis before deciding on treatment, a fine needle aspiration cytology.

Detection of any metastases of thyroid cancer can be performed with a full body scanning using iodine-131.

• CT scan or MRI thyroid scan shows this growth to be "cold," meaning it does not absorb a radioactive substance.

TREATMENT-

SURGICAL MANAGEMENT
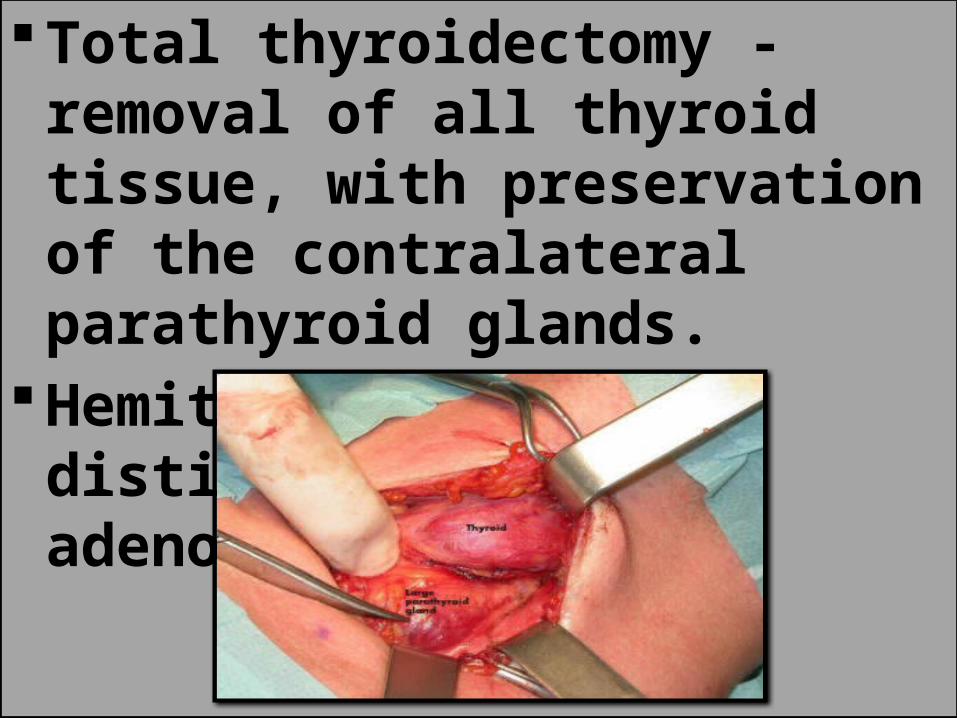
Total thyroidectomy -removal of all thyroid tissue, with preservation of the contralateral parathyroid glands.
Hemithyroidectomy to distinguish between adenoma & carcinoma
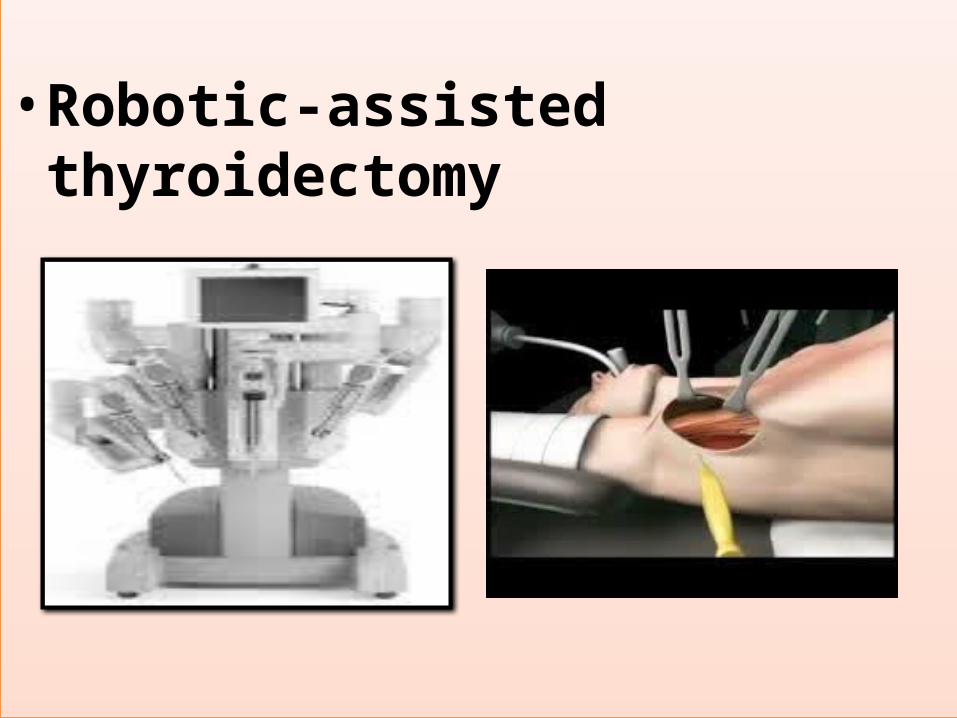
• Robotic-assisted thyroidectomy
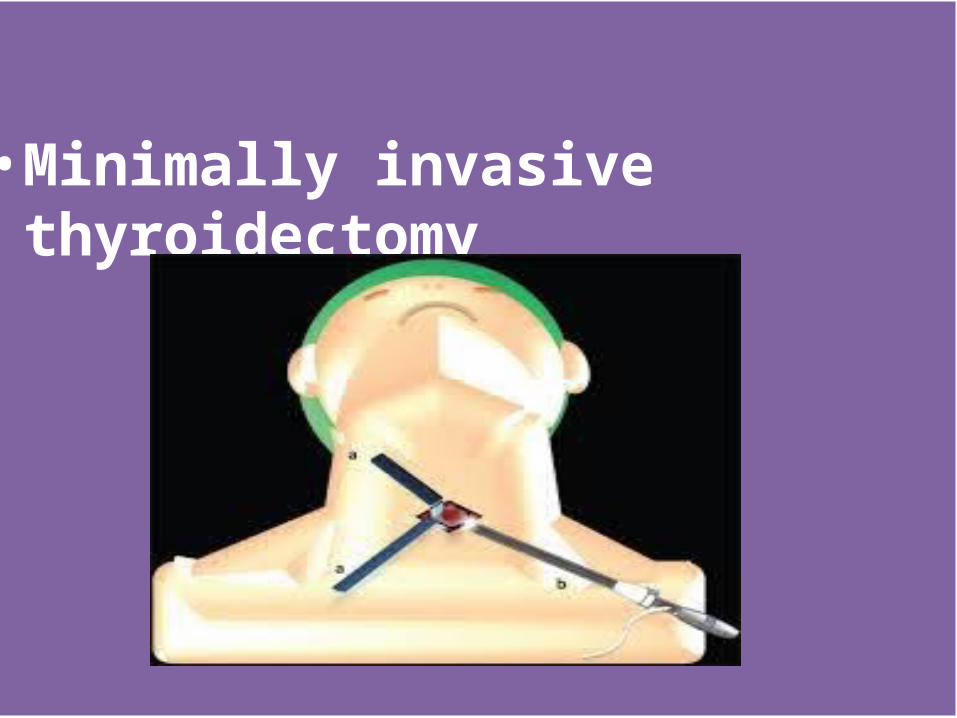
• Minimally invasive thyroidectomy

RADIATION
RADIO ACTIVE IODINE THERAPY

CHEMOTHERAPY
Carboplatin – Eprubicin Protocol
• CARBOPLATIN – 300mg/msq. (IV) – D1 (over 30 mins.)• EPIRUBICIN - 75 mg/ msq.
(4 hours after Carboplatin) [Administration repeat cycle after 4 to 6 weeks]

CVD PROTOCOL• INDICATION: Advanced Medullary
Thyroid Carcinoma• CYCLOPHOSPHAMIDE – 750mg/m.sq. –
D1• VINCRISTINE – 1.4mg/m.sq. – D1• DACARBAZINE – 600mg/m.sq. – D1,D2• CYCLE- to be repeated every 3-4 weeks
depending on tolerance

DACARBAZINE – 5FU
• INDICATION: Advanced Medullary Thyroid Cancer• Dacarbazine – 250mg/m.sq.- IV- (5Day
intraveously)• 5FU- 450mg/m.sq. – (12 hour infusion) • cycle to be repeated every 4 weeks

TARGETED THERAPY

SORAFENIB—-400 mg- PO –BD- DailyIndication – metastatic , iodine refractory carcinoma
MOTESANIB—-125mg- PO - DailyIndication – Progressive advanced
(metastatic , radio iodine resistant differentiated carcinoma

NURSING MANAGEMENT

• Acute PainRelated to:• pressure / swelling of the tumor nodule• Surgical interruption/manipulation of tissues/muscles• Postoperative edemaPossible evidenced by:• The existence of the neck pain may spread to the orbital area.• Pain scale of 0-10• Looks withstand pain• There is pain in swallowing, and difficulty swallowing• Narrowed focus; guarding behavior; restlessness• Autonomic responses
• Ineffective airway clearance Related to:• Tracheal obstruction due to tumor mass pressure• Laryngeal spasm• Accumulation of secretionsPossible evidenced by:• Difficulty breathing• Difficulty of removing secret• Complained of shortness of breath• Above normal respiration
• .Impaired verbal CommunicationRelated to:
• Injury to vocal cords• Laryngeal nerve damage• Tissue oedema
Possible evidenced by:• Talk husky / can not speak
• Injury, risk for [tetany]Related to• Risk factors may include• Chemical imbalance: excessive CNS
stimulation

• .Knowledge deficient [Learning Need] regarding condition, prognosis, treatment, self-care, and discharge needs
Related to• Lack of exposure/recall, misinterpretation• Unfamiliarity with information resourcesAs evidenced by• Questions; request for information; statement of
misconception• Inaccurate follow-through of instructions/development
of preventable complications

CAN YOU ANSWER??
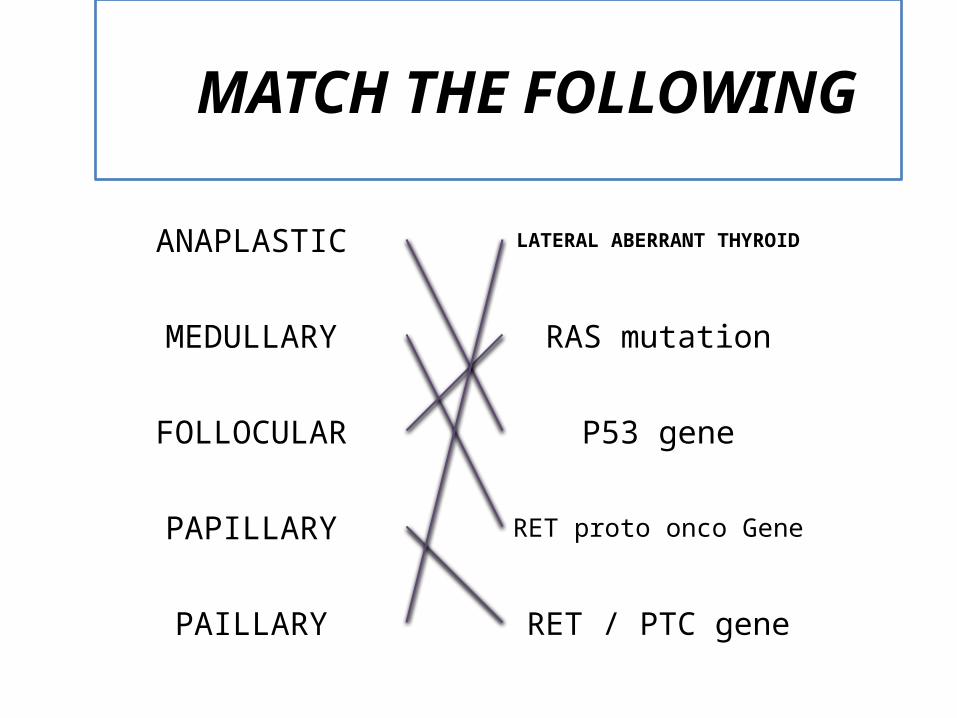
ANAPLASTIC
FOLLOCULAR
PAPILLARY
PAILLARY
LATERAL ABERRANT THYROID
RAS mutation
P53 gene
RET proto onco Gene
RET / PTC gene
MATCH THE FOLLOWING
MEDULLARY

T1 - Tumor is 2 cm or smaller across , limited to the thyroid
NAME 2 CHEMOTHERAPY DRUGS USED FOR TREATMENT OF CHEMOTHERAPY?
NAME 1 DRUG USED AS TARGETED THERAPY?
TELL ANY 2 ETIOLOGY OF THYROID CANCER?
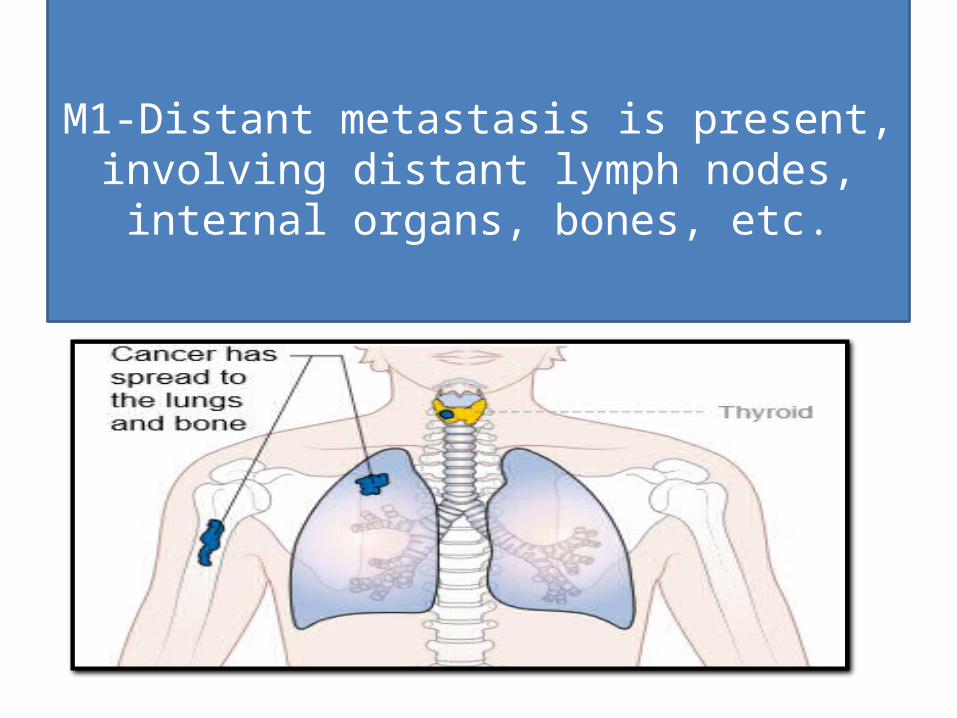
M1-Distant metastasis is present, involving distant lymph nodes, internal
organs, bones, etc.

![Thyroid Cancer and Thyroid Nodules.ppt [Read-Only] · Thyroid CaThyroid Ca 20012001. Newer Exceptions Unfortunately recent Studies have shown exceptions: *** *** In one study of papillary](https://static.fdocuments.in/doc/165x107/5d4794b388c9931b4f8b7654/thyroid-cancer-and-thyroid-read-only-thyroid-cathyroid-ca-20012001-newer.jpg)