
Ca breast management (according to NCCN guidelines)
44
-
Upload
pirah-azadi -
Category
Documents
-
view
53 -
download
4
Transcript of Ca breast management (according to NCCN guidelines)


CA BREAST MANAGEMENT
(RECENT GUIDELINES)
BYDR. PIRAH KORAI
fcps-ii traineeg. surgery
cmc larkana

Outlines
• Epidemiology of CA Breast
• Clinical manifestations
• Management according to NCCN guidelines
(Stage-wise)

BREAST CANCER IN THE WORLD
Breast cancer is second only to lung cancer as a cause of cancer deaths
1.15 million new cases
470 000 deaths
Half of the global burden in low- and medium-resourced countries

CLINICAL MANIFESTATIONS
5
Most common: lump or thickening in breast. Often painless
Change in color or appearance of areola
Redness or pitting of skin over the breast, like the skin of an orange
Discharge or bleeding
Change in size or contours of breast

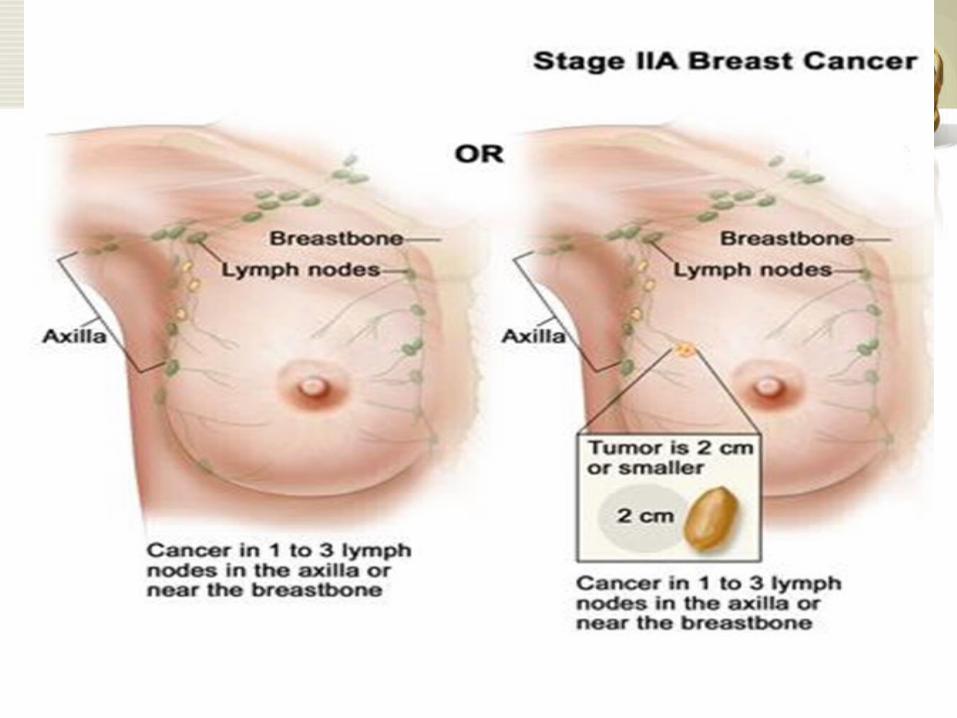
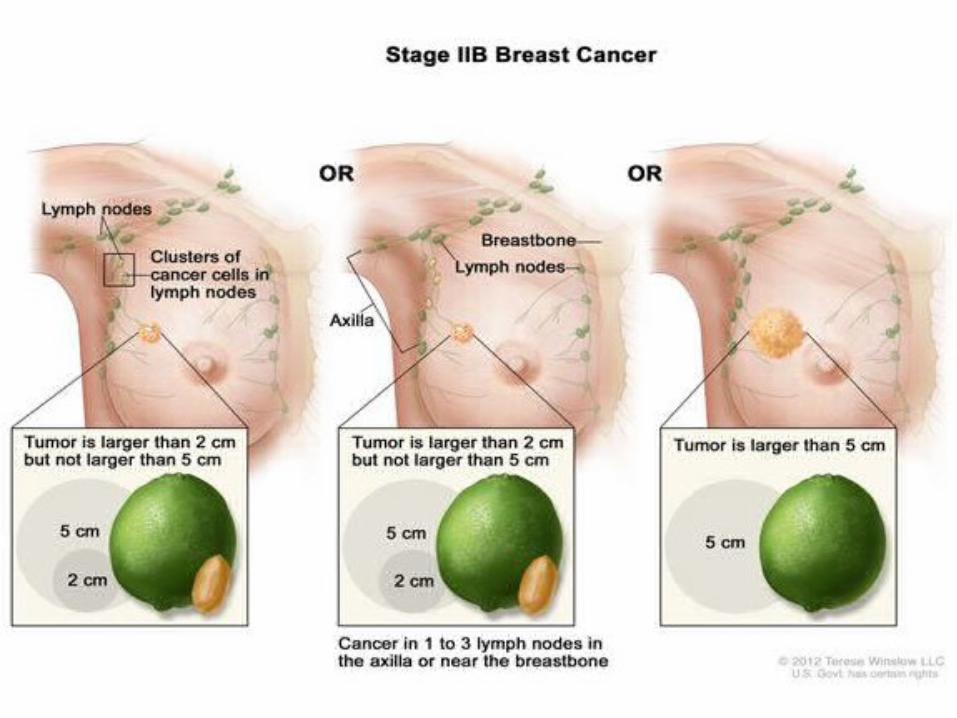
MANAGEMENT

American Joint Committee on Cancer
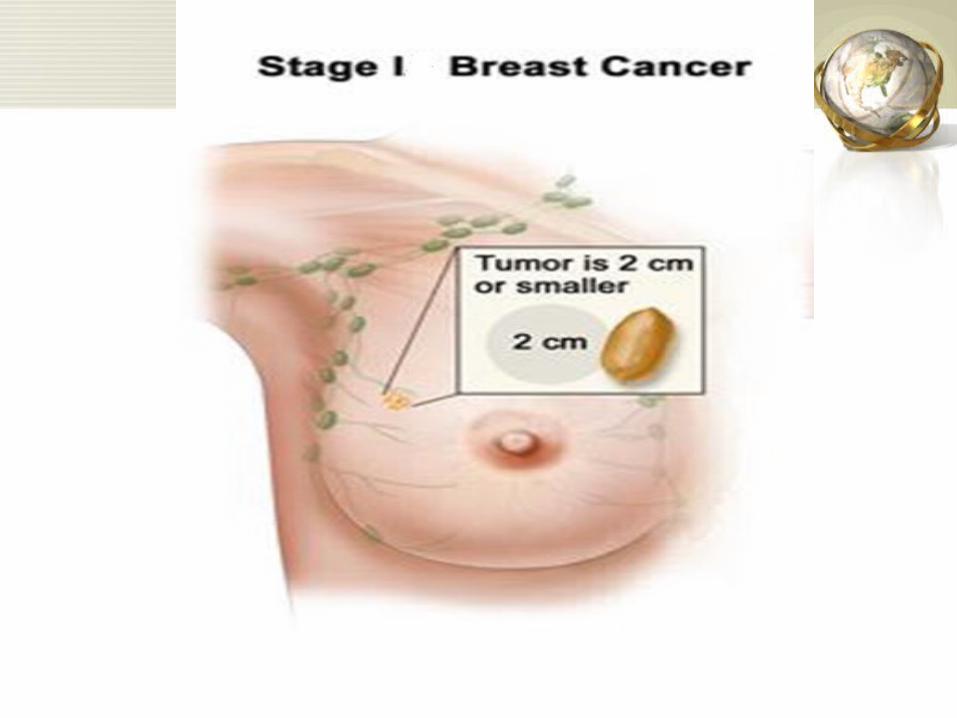
t< 2 cm,no nodes
t 2 to 5 cm, +/-nodes
matted lymph nodes,variable tumor size
distant metastases

STAGE-WISE MANAGEMENT ( ACCORDING TO NCCN GUIDELINES)


MANAGEMENT OF LCIS
BIOPSY:• FNA• Core Biopsy• Incisional biopsy• Excisional biopsy (Tumor + surgical margins)
ADVISES For RISK REDUCTION:
• Modify life style• Hormonal Therapy: Anti-estrogen• Surgery• Follow-up care

SURGERIES
B/L Simple Mastectomy with reconstruction surgery
Indication:
•Family history of CA Breast•Relatives having mutations in BRCA1 and BRCA2•Ovarian cancer
FOLLOW-UP
•Mammography: every year after age of 50
•CBE: every 6 to 12 months
•Self examination awareness
•Breast MRI
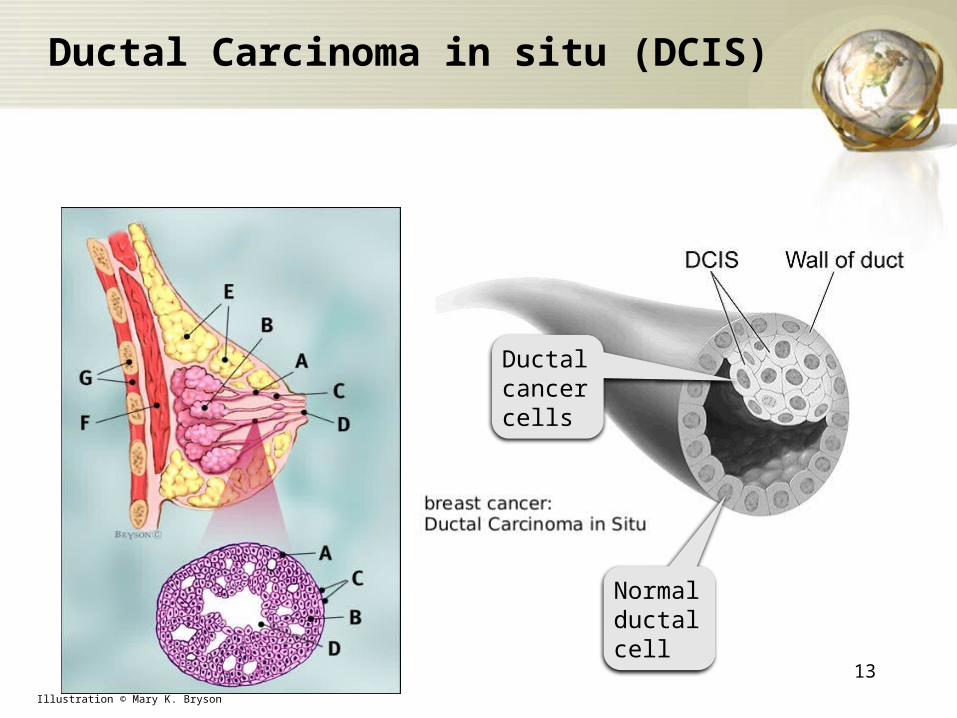
Ductal Carcinoma in situ (DCIS)
13Illustration © Mary K. Bryson
Ductal cancer cells
Normal ductal cell

• Medical history
• Physical examination
• Diagnostic mammography
• Biopsy
• Hormone receptor test
• Genetic counseling

Management
• Lumpectomy alone
• Lumpectomy with radiotherapy (EBRT)– (Breast conserving therapy)
• Total Mastectomy – (with or without breast reconstruction)
• Sentinel lymph node biopsy

BREAST RECONSTRUCTION
BREAST RECONSTRUCTION
• After Lumpectomy– Volume displacement
• After mastectomy– Skin sparing mastectomy– Time for reconstruction

Types of reconstruction
• Implants
• Flaps
• Both

Nipple Replacement
• Remade nipple:– From surrounding tissue– Vulva– Thigh– Other nipple
• fake nipple

Choice between
Breast conserving surgery
/ Breast reconstruction

Breast conserving surgery
–Pros• Skin’s natural look is kept• Quicker healing• Intact sensation so better
psychological satisfaction
–Cons• Asymmetry• Radiation required• May need second surgery
Breast reconstruction
–Pros• Reconstruct whole breast• Less worry about recurrence• Less likely to need radiation
–Cons• Loss of breast• Longer healing• Serious side effects e.g: edema

RISK REDUCTION
Modify life style
Hormonal therapy
Follow-up• Mammography (every 6months)• CBE• Self examination• Breast MRI

STAGE i & STAGE ii
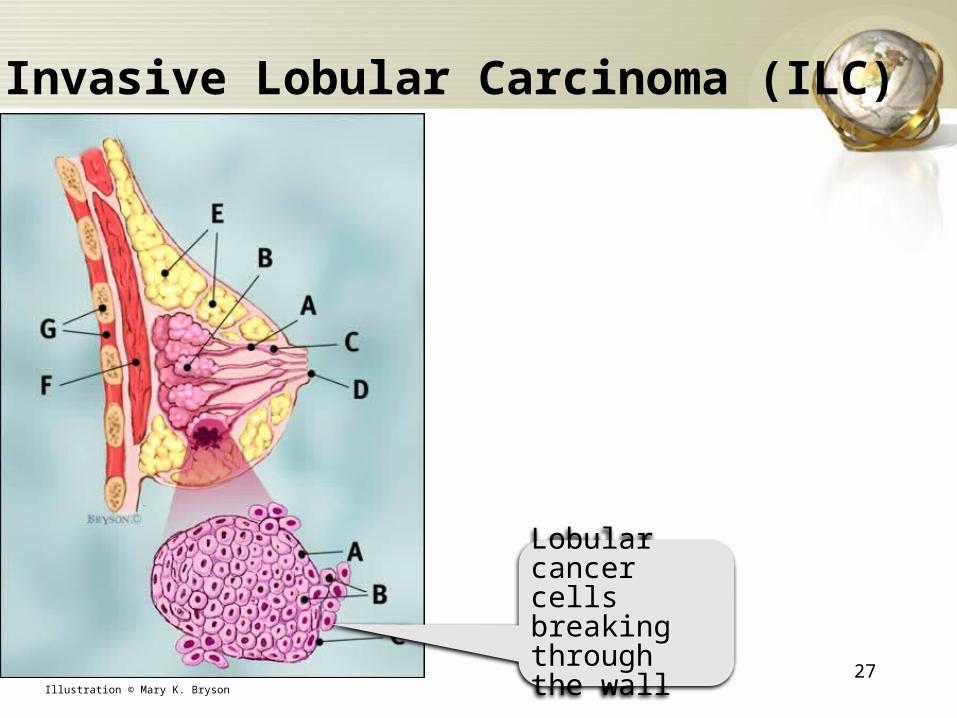
Invasive Lobular Carcinoma (ILC)
27Illustration © Mary K. Bryson
Lobular cancer cells breaking through the wall

WORK-UP• Medical history
• Physical examination
• Blood test: CBC, LFTs
• Imaging: – mammography, – u/s,– MRI,– bone scan,– CT Chest, – Abdominal/pelvic CT scans

• C.A cell tests: – Hormone receptor tests– HER2 receptor test
• Lymph node biopsy
• Genetic counseling
• Fertility counseling
SURGERIES
• Breast conservative surgery: Lumpectomy
• Total mastectomy
(With or without breast reconstruction)
• Surgeries for Lymph node– Sentinel lymph node dissection– Axillary dissection

NEOADJUVANT THERAPY
• Chemotherapy
• Radiotherapy
-In whole breast
-Partial breast
• Hormonal therapy

STAGE iii




• INVESTIGATIONS
• SURGERIES
– BCT: Lumpectomy with radiation
– Total mastectomy (with or without breast reconstruction)
– Lymph nodes dissection


TREATMENT OPTIONS
• Hormonal therapy
• Chemotherapy
• Targeted therapy
HORMONAL THERAPY
• Anti-estrogen: Tamoxifen and Toremifene
• Aromatase inhibitors:
• Hormones: high dose megestrol acetate, flurymesterone, ethinyl estradiol
• Ovarian ablation (through B/L oophrectomy or radiation)
• Ovarian suppression: LNRH agonist e.g: Goserelin, Leuprolide

CHEMOTHERAPY
• Alkylating agents:– carboplatin, cisplatin, cyclophosphamide
• Anthracyclins: – Doxorubicin, epirubicin
• Antimetabolites: – flurouracil, methotraxate, gematabine etc
• Microtubule inhibitors: – Docetexal, emtansine, eribulin, paclitaxel
TARGETED THERAPY
• Trastuzumab and pertuzumab
• Ado-transluzmab
• Lapatinib
• Bevicizumab
• everolimus

SUPPORTIVE TREATMENT
• Bisphosphonates
• Vitamin D
• Calcium etc


QUESTIONS


















