C3: Collaborating to Conquer Cancer
11
Sendipity by design ANSCHUTZ MEDICAL CAMPUS COLLABORATING TO CONQUER CANCER 12: DON’T CALL HIM SUPERMAN 16: SCREENING WARRIORS 10: Q&A WITH JONATHAN GUTMAN, MD 11: C3 MD LIA GORE 18: SUPPORTER FOCUS ON GARY REECE WINTER 2011
-
Upload
university-of-colorado-cancer-center -
Category
Documents
-
view
218 -
download
1
description
The University of Colorado Cancer Center's magazine - C3: Collaborating to Conquer Cancer, Fall 2011 edition.
Transcript of C3: Collaborating to Conquer Cancer

Serendipity by design
A N S C H U T Z M E D I C A L C A M P U S
C O L L A B O R A T I N G T O C O N Q U E R C A N C E R
12: DoN’T CALL HIM
Superman
16: SCrEENINg
WarriorS
10: Q&A wITH
Jonathan Gutman, mD
11: C3 MD Lia Gore
18: SUPPorTEr FoCUS oN
Gary reece
W I N T E R 2011

www.coloradocancercenter.org
2C3: Winter 2011
3
The University of Colorado Cancer Center’s lead cancer care partners have been ranked among the top
hospitals for cancer care in the 2011-2012 U.S. News & World Report Best Hospitals and Best Children’s
Hospitals surveys. University of Colorado Hospital was ranked 34th for adult cancer care and Children’s
Hospital Colorado was ranked 10th for pediatric cancer care among hospitals nationwide. Both hospitals
are part of the CU Cancer Center consortium, a National Cancer Institute-designated comprehensive
cancer center. Both hospitals are the top-ranked cancer care facilities in Colorado.
University of Colorado Hospital was also ranked as the top-performing academic hospital in the
United States for delivery of quality heath care by University HealthSystem Consortium, the 114-member
alliance of the nation’s leading nonprofit academic medical centers. The award is based solely on patient
experience data.
cu cancer reSearcherS are firSt to Sequence bLaDDer cancer,
tarGet mutationS for therapy
common cLaSS of pain DruGS reDuceS Severity of poStpartum
breaSt cancerS
feWer Women GettinG mammoGramS
after 2009 GuiDeLine reviSion
A University of Colorado Cancer Center team, led by director Dan Theodorescu, MD, PhD, is the first
to sequence the most prevalent type of bladder cancer.
The gene sequencing project, done in partnership with universities in China and Denmark, allows
researchers to recognize genetic mutations that make bladder cancer cells different from their healthy
neighbors. That information may allow early genetic screenings for bladder cancer and new therapies
for cells with these mutations.
“when we talk about ‘causes’ of cancer, there’s a black box between a healthy cell and the emergence
of cancerous ones,” Theodorescu says. “By exploring the genetic changes that take place inside this
box, we can look at the links of the chain of events that lead to cancer and, hopefully speaking, target
specific links for therapy.”
About 69,250 people in the United States are predicted to be diagnosed with bladder cancer this year,
and 14,990 will die, according to the National Cancer Institute. It’s the fourth most common type of cancer
in men and ninth most common type in women. Smoking is a leading cause of the disease.
The study was reported online in the Aug. 7, 2011 issue of Nature Genetics.
uch, chiLDren’S amonG nation’S beSt for cancer care
University of Colorado Cancer Center
director Dan Theodorescu, MD, PhD,
and center investigators Scott Lucia, MD,
and Jeff Kieft, PhD, have been awarded
a $9.55 million, five-year grant to define
the molecular changes that occur
as prostate cancer progresses to
a therapy-resistant state.
The Colorado researchers share
the National Cancer Institute grant
with a multidisciplinary team from
University of Virginia, led by Bryce M.
Paschal, PhD.
when caught in its early stages,
prostate cancer is treatable in most
cases. But once it reaches a critical
threshold, the disease transforms to
become largely resistant to current
treatments. These changes include
alterations in how the cancer cells
respond to signals and what genes
are expressed, researchers say.
In 2003, CU Cancer Center
investigators Fred Hirsch, MD,
PhD, and wilbur Franklin, MD,
created a test that identifies
key biomarkers in advanced
lung cancer.
Now, a European clinical trial
shows that patients identified with
this test as having high levels of
the biomarker, called epidermal growth factor
receptor, have 36 percent better survival rates
when treated with the drug cetuximab and chemo-
therapy. Cetuximab, or Erbitux, is primarily used to
fight colorectal and head and neck cancers.
“with this personalized medicine we can
identify subgroups of patients that can get better
effects from certain drugs,” Hirsch says. “In some
cases there is a potential for a cure. right now
the cure rate for advanced lung cancer is 2 to 3
percent at best. This is a huge improvement but
everything is based on the selection criteria.”
About 30 percent of people with non-small
cell lung cancer have elevated levels of EgFr.
Head and neck cancer patients in Colorado
have access to the nation’s first cancer stem cell
clinical trial, aimed at giving the cells a “one-two
punch” of drugs, according to CU Cancer Center
investigator Antonio Jimeno, MD, PhD.
while cancer stem cells may form roughly
1 to 2 percent of a tumor’s mass, they are
especially resistant to traditional chemotherapies
and many researchers believe they contribute to
relapse by repopulating a tumor post-therapy.
The phase I clinical trial is based on preclinical
animal studies that Jimeno calls “striking.”
It combines the drug cetuximab with the anti-
cancer-stem-cell agent IPI-926, developed by
Infinity Pharmaceuticals. The first agent targets
the tumor’s mass and the second disrupts the
“hedgehog” signaling pathway that tells cancer
stem cells to regenerate killed cancer tissues.
The National Institutes of Health grant awards
the project $500,000 over two years, during
which Jimeno, director of the Cancer Stem
Cell-Directed Clinical Trials Program, hopes to
enroll 18 to 24 people with relapsed head and
neck cancer.
coLoraDo cancer reSearcherS Share $9.55 miLLion Grant to Learn hoW
proState cancer reSiStS treatment
tWo cu cancer center ScientiStS
LauDeD aS boettcher inveStiGatorS
bemiS, SpiLLman aim to DeveLop accurate, eaSy teSt
to Detect ovarian cancer recurrence
N3wS
HirscH
scHedin, Borges
Lucia , K ieft, tHeodorescu
Get more cu cancer center news on our blog: www.coloradocancerblogs.org
read the stories here in full and sign up for our bimonthly email, Colorado Cancer News.
A 2009 recommendation to stop screening
women between the ages of 40 and 49 for
breast cancer using mammograms has begun
to negatively affect the number of yearly
mammograms performed in this age group.
The recommendation from the United States
Preventive Services Task Force may also
interfere with the possibility of the early
detection of breast cancer.
Since the November 2009 recommendation,
University of Colorado Hospital performed
screening mammograms for 205 fewer women
in the 40-49 age range than in the previous
year, according to a study by CU Cancer
Center investigator Lara Hardesty, MD, chief
of breast imaging at University of Colorado
Hospital and associate professor of radiology
at the CU medical school.
In a separate study, Hardesty also found
referring physicians are beginning to follow the
revised recommendations. Hardesty says,
“If the trend continues, we may miss the oppor-
tunity to diagnose breast cancer in its early
stages, and early detection is crucial.”
205f e w e r wo m e n
s c r e e n e d
The ibuprofen found in most household
medicine cabinets could prove to be
an effective treatment for postpartum
breast cancers if animal model research,
published in August in Nature Medicine
by Colorado cancer researchers, holds
true in humans.
Pepper Schedin, PhD, and Virginia
Borges, MD, MMSc, co-directors of
the University of Colorado Cancer
Center Young women’s Breast Cancer
Translational Program, have been work-
ing on the hypothesis that the process
responsible for killing milk-producing
cells in the breast after pregnancy, called
involution, contributes to a 30 percent
increase in breast cancer in women who
have children after age 35. Postpartum
breast cancers tend to be more aggres-
sive, with increased risk of spreading
to other organs, and have much lower
five-year survival rates.
The team, which includes trainees
Traci Lyons and Jenean o’Brien, discovered
that breast involution increases production of an
enzyme called CoX-2, which non-steroidal anti-
inflammatory drugs (NSAIDs) like ibuprofen and its
more targeted cousin, celecoxib, inhibit.
The team tested the treatment in postpartum
mice with breast cancer, and found that ibuprofen
and celecoxib treatment reduced mammary tumor
size, collagen architecture, CoX-2 expression and
breast tumor cells spreading into the lung.
“we caution patients and providers that
because a mother’s body is undergoing radical
changes during this time, we can’t yet speak to the
safety of these drugs for women diagnosed with or
at risk for postpartum breast cancer, and thus can’t
yet recommend NSAIDs as a preventative therapy
or cancer treatment,” cautions Schedin, professor
of medical oncology at the CU medical school.
c o lo r a d o t e st h e l p s b o o st su rv i va l r at e s f o r lu n g ca n c e r pat i e n t s
f i r st ca n c e r st e m c e l l c l i n i ca l t r i a l o p e n s at c u ca n c e r c e n t e r
CU Cancer Center investigators robert Doebele,
MD, PhD, who studies drug resistance in
oncogene-driven lung cancer, and Jing wang, PhD,
who studies antibody production and genomic
instability in B lymphocytes, have been named to
the 2011 Class of Boettcher Investigators in the
webb-waring research Program.
The Boettcher Investigators Program, in its
second year, supports early-career scientists in
their work toward making discoveries that improve
human health. Last year, CU Cancer Center
researcher Paul Jedlicka, MD, PhD, received
the award.
doeBeLe
Wang
CU Cancer Center investigators Lynne Bemis, PhD, and Monique Spillman,
MD, PhD, have received a grant from the HErA women’s Cancer Foundation
to design a test that returns quick, accurate results about whether ovarian
cancer has returned. Bemis, a basic researcher and associate professor of
medical oncology at the CU medical school, and Spillman, a gynecological
oncologist, surgeon and assistant professor of obstetrics and gynecology
at the CU medical school, will develop a urine-based test that looks for
small molecules called microrNAs that are either over- or under-expressed
as an indicator of recurrence. The pair aim to define the “signature” for the
microrNAs that are the most predictive of ovarian cancer, and then to
develop a test that could be administered in any doctor’s office.
The current test for ovarian cancer recurrence after treatment requires
a blood draw and can return false positives created by a variety of factors.
Most ovarian cancer is diagnosed when it is no longer curable. This
research project is one step toward the goal of developing a test that detects
cancer when it is treatable—and still confined to the ovaries.
Lyn
n c
Lar
K
gLe
nn
as
aK
aW
a

www.coloradocancercenter.org
4C3: Winter 2011
5
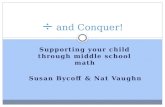
imagine a chromosome as an inchwormwhen the inchworm is stretched out, the pattern of its feet forms the blueprints of the body’s proteins. now imagine this inchworm, inching—bringing its feet up to just behind its head. this is what chromosome no. 2 does in 3 percent of non-small-cell lung cancer patients. instead of making a healthy alK protein from the worm’s front half and a healthy eml4 protein from its back half, the bunched worm makes an alK-fusion protein from the squished-together bits of tip and tail. this alK-fusion protein causes lung cancer in about 45,000 people each year. lung cancer in general remains the leading cause of cancer deaths worldwide.
in the world of cancer research $10,000 is a tiny drop in a mighty ocean, but it was this drop, dripped in just the right place, that allowed garcia to develop a specific test for these alK-fusion proteins in lung cancer patients.
“it’s a tricky test because the two partners are on the same chromosome and not far apart, and when they fuse they’re on the same gene not so far apart,” bunn says.
relying on her experience, her expert research team, and the center’s cytogenetics shared resource, which she directs, by the end of november 2007, garcia had her test.
meanwhile, lung cancer patients were fighting for their liveselsewhere at the cu cancer center, ross camidge, md, phd, clinical director of the thoracic oncology program, was chugging away on a drug trial for pfizer. patients in the study were tested for a different mutation, one in the met gene, and the drug camidge’s patients were taking through the center’s developmental therapeutics clinic was supposed to nix the function of this faulty gene.
the phase i safety trial of this drug was taking place at a number of hospitals around the country, notably also at the juggernaut of massachusetts general hospital in boston, but because the cu cancer center was the only site in the west, “we got patients from california, washington, las vegas,” garcia recalls.
in this large trial, little cu was a close second to mass general in patient enrollment. as can be the case with these safety studies, some patients responded while others
didn’t, and overall the drug was showing only middling results. the goal isn’t to find out if the drug works, but rather what side effects happen at different dosages or schedules. but then the news of this new cancer-causing gene, alK, broke in the journal Nature—and pfizer quickly changed the tune of its clinical trial.
the drug that camidge and others were testing didn’t just nix the first target, met, but also nixed the function of this newly described alK-fusion gene.
maybe it wasn’t that pfizer’s drug didn’t work, but rather that they were giving it to the wrong patients? it’s like offering macaroni and cheese to a food critic and a 5-year-old: the same meal makes one salivate and the other cringe. pfizer decided to see how its drug worked with the patients who salivated, the ones with alK-fusion genes.
pfizer asked who among its participating centers could test for this alK-fusion gene.
garcia raised her handthere were only two places in the country with the ability to test for this gene: mass general and, due to garcia and bunn’s foresight, the cu cancer center.
“because we could do the molecular test here, we became a partner and not an outpost,” garcia says.
in 2008, pfizer hired mass general and the cu cancer center to run these genetic tests and enroll alK-positive patients into a phase i clinical trial of their drug. “camidge got patients, he would send their samples to me, and in three days he knew if they were alK-positive,” says garcia.
this alK-fusion protein
causes lung cancer in about
45,000 people each year. lung
cancer in general remains
the leading cause of cancer
deaths worldwide.
b y G a r t h S u N d e m
In the university of Colorado
Cancer Center’s fight against
lung cancer, what looks like
luck on an ordinary day is
the product of forethought,
experience, and a willingness
to ride the winds of change.
Serendipityb y d e s i g n
alK positive
alK positive “split”
alK negativein august 2007, marileila varella-garcia went to paul bunn’s office to ask for $10,000. research grants take months and garcia’s intuition told her not to wait—the pres-tigious scientific journal Nature had just linked a type of lung cancer to a specific
genetic mutation, and garcia, phd, renowned international expert on cancer cell genet-ics, wanted to know which patients had it. she needed $10,000 to develop the test.
bunn is no slouch himself. at a 2010 conference of the american association for cancer research and the international association for the study of lung cancer, bunn was honored for his leadership in lung cancer research, with the conference chair call-ing him an “inspiration to physicians and scientists working in the field of lung cancer.”
over the years, the handsome, grey-haired bunn has built a world-class lung cancer treatment and research team at the cu cancer center, and was instrumental in bring-ing garcia onboard in 1993. and because paul bunn holds an endowed chair—the James dudley chair in cancer research—he doesn’t live grant-to-grant, but instead has his own yearly research endowment to spend as he sees fit. by 2007, bunn and garcia had worked together for 14 years, and so when garcia asked, bunn trusted garcia’s hunch and gave her $10,000 from his discretionary research account.
garcia took it to the lab.
veer
ima
ges
co
ur
tes
y o
f tH
e g
ar
cia
La
B
Listen to Dr. Garcia explain the ALK images.

www.coloradocancercenter.org
6C3: Winter 2011
7
“you spend all your time planning things and then stuff just happens and you have to run with it,” camidge says.
because the cu cancer center is comparatively nimble, it was able to sprint. the center soon started testing patients with garcia’s molecular spyglass and enrolling them on a refocused trial of pfizer’s drug. the results were dramatic.
“when one patient shows a benefit, it might be a fluke,” bunn says. “but when the number gets to ten, you know you have something special.”
one of these patients was ellen smithafter being diagnosed with lung cancer in 2008, smith had undergone a spring and summer of chemotherapy followed by surgery to remove her left lung and then radiation through the fall. finally, “the doctor came in and the news was spread all over his face,” smith says. “my lung cancer had spread to five places in my abdominal cavity. he was a great doctor, but basically he said, ‘i don’t know what else i can do for you.’ ”
her doctor was right; there was nothing more he could do. in fact, there was nothing that standard medical science could do.
but ellen smith says, “my family and i weren’t ready for that.” smith has three grown children, five grandchildren and was in a relationship with a man she called her “longtime gentleman friend.” it wasn’t a convenient time to die.
in another serendipitous turn, smith had retired from her job as a public school teacher and was working as a nanny for a mother who is a thyroid cancer researcher at the cu cancer center.
“she said, ‘ellen, you have to go to the cu cancer center.’ she twisted my arm until i went there for a second opinion,” says smith.
and there at the cu cancer center, ellen smith stumbled into camidge, garcia, bunn, and a melting pot of scientists and doctors who had spent years preparing for her arrival. she signed a consent form to have her tumor specimen tested, and then she went to scotland with her gentleman friend to retrace her family roots. it was something she had always wanted to do, and with cancer shutting down her body, it seemed like now or never. she almost didn’t survive the trip. in scotland, her
remaining cancer-blackened lung started bleeding, and she was rushed to the emergency room.
“i was in a foreign country, and i was so frightened,” smith says. then, on what she thought was her deathbed in a foreign emergency room, ellen got a long-distance call from her son. she was a match for the cu cancer center clinical trial. ellen smith was among the alK-positive 3 percent. she flew home to camidge.
by this time pfizer’s drug had a name—crizotinib—and it ripped ellen smith back from the precipice on which she had been standing. crizotinib works by starving alK-positive tumor cells of their energy source, and as ellen’s tumors starved, they shrank by more than 40 percent.
of the 82 alK-positive patients enrolled in what was supposed to be a trial assess-ing only the drug’s safety—a test of the medicine in patients beyond hope who had little to lose if the drug proved unexpectedly dangerous—90 percent saw their tumors stabilize or shrink, and 57 percent saw their tumors shrink by more than a third.
“it was as if their tumors melted away,” bunn says.
life after happily ever aftermost fairytales end here, but creating remission is only a step on the path to a cure.
“dr. camidge told me that a day would come when the alK inhibitor wouldn’t work,” ellen smith says. “that day came about a year and a half later.”
“what do you do when the honeymoon ends, when these people who responded fantastically start to become resistant?” camidge asks. cancer is insidious—the same mechanism that allows healthy cells to mutate into cancer cells also helps cancer cells mutate around the barricades of treatments.
first, just as we’ve seen that two lung cancers might not be created equal, so too can pockets of cancer within a patient’s body evolve differences over time. in ellen smith, when a follow-up scan showed that just one of her tumor deposits had become resis-tant to crizotinib, cu cancer center radiation oncologist brian Kavanagh, md, mph, was able to blast just this tiny part with stereotactic body radiation. in fact, Kavanagh literally wrote the textbook on stereotactic radiation, which was published in 2004— just another world expert who was fortunately part of ellen smith’s treatment team.
“this radiation just deletes one little bit of your body,” camidge says. “it’s very good for weeding the garden. you don’t throw the baby out with the bath water, just zap the resistant part of the tumor and keep the drug going.”
eventually all of ellen’s lung cancer became resistant, and the crizotinib honeymoon was officially over. at that point, most oncologists would’ve been back to the drawing board, guessing at a treatment that could put another barrier in lung cancer’s way.
the cu cancer center did better than guess.
Knowing your patients leads to patterns“one thing that comes from getting to know your patients is learning to listen to them when they tell you about what worked well or what didn’t,” camidge says. “for exam-ple, a 35-year-old man on crizotinib told me he had a new girlfriend, but wasn’t finding her as attractive as he should.” sure enough when they checked this man, his testos-terone was low. in fact, when he checked, 100 percent of camidge’s male patients on crizotinib developed low testosterone, which, once discovered, was easy to replace.
“we now check testosterone on all our crizotinib patients, and i think this will change the way the drug will safely be given in the future. the only way you get to find out this sort of thing is if you know your patients as people so that they’re comfort-able telling you about the intimacies of their lives,” camidge says. “with a big center, there are more patients, but they may be spread around across multiple doctors and it becomes harder to spot these subtle patterns.”
of the 82 alK-positive patients enrolled
in what was supposed to be a trial
assessing only the drug’s safety,
90 percent saw their tumors stabilize
or shrinK, and 57 percent saw their
tumors shrinK by more than a third.
because the cu cancer center is
comparatively nimble, it was able
to sprint. the center soon started
testing patients with marileila
varella-garcia’s molecular spy-
glass and enrolling them on a
refocused trial of pfizer’s drug.
the results were dramatic.
because of crizotinib and the cu cancer center treatment team that has consistently stayed a step ahead of her cancer, ellen smith is walking with her family instead of walking in their memories.
gLe
nn
as
aK
aW
a
Lyn
n c
Lar
Kmarileila varella-garcia, phd, with her lab staff.

www.coloradocancercenter.org
8C3: Winter 2011
9
working with camidge, new australian senior fellow andrew weickhardt, md, was the first to pull together the testosterone data from camidge’s original observation. recently weickhardt submitted the important findings for publication. “returning a young man’s testosterone to normal is something he is pretty grateful for. it gives them an important piece of their life back,” weickhardt says.
spotting another lucky pattern helped camidge save ellen smith’s life a second time. because these alK-positive patients had been treated with crizotinib as a therapy of
last resort, they’d commonly tried upwards of five other drugs before starting the crizotinib trial. camidge noticed that before their cancer had developed resistance, many of these alK-positive lung cancer patients had done surprisingly well on a drug called alimta.
“there’s nothing quite like that feeling—like you’re in school and everybody’s doing a math calculation and they all get different answers, but you have this little voice that says maybe they’re all wrong and you’re right and you just stick to your guns,” says camidge.
he was right about this: if a patient hadn’t seen alimta before moving down the line to crizotinib, then when lung cancer developed resistance to crizotinib, this alimta was a spectacular next line of defense. when ellen smith’s crizotinib honeymoon ended, as she had never seen alimta before, camidge immediately started her on it.
“confirming the earlier pattern seen with other patients, ellen had almost as dramatic a response on the alimta as she did on the crizotinib,” camidge says. “she’s been on the alimta for nine months (in sept. 2011) and i can’t see any sign of active cancer on her scans.”
staying a step aheadbut lung cancer never rests, and so cu cancer center doctors are already laying the groundwork for ellen smith’s next step.
for example, pathologists wilbur franklin, md, and dara aisner, md, whom the cu cancer center recently enticed away from the university of pennsylvania, are growing samples of patients’ tumors in the lab to discover how they evolve around drugs like crizotinib and alimta. franklin created the colorado molecular correlates laboratory, perhaps the nation’s most accomplished facility for testing for genes that drive tumors. in this lab, franklin grew a large culture of cells from a small sample of ellen smith’s tumor. and aisner developed tests that can tell exactly how these tumor cells develop resistance to drugs.
still another cook in this crowded kitchen, robert doebele, md, phd, connects the dots from the tumors of patients like ellen smith through franklin’s cells, using aisner’s test, to recommendations for the next line of drugs that will hit smith’s evolving tumor from an angle it hasn’t yet learned to protect, if and when needed.
this flock of therapies developed by a gaggle of scientists and administered by a covey of doctors has kept ellen smith alive.
“i’m three years out now,” ellen smith says. in that time—that extra time—ellen married the person she calls her “wonderful gentleman friend.” and then on July 12, 2011, her sixth grandchild was born. “her name is lucy and i’m just so completely in love,” smith says. “i see her twice a week. i go for walks with my daughter and see my granddaughter.” because of crizotinib and the cu cancer center treatment team that has consistently stayed a step ahead of her cancer, ellen smith is walking with her family instead of walking in their memories.
charles goodyear invented vulcanized rubber when he spilled a mixture of rubber, sulfur and lead onto a hot stove. wilson greatbatch invented the pacemaker when his attempt to monitor heart activity regulated its rhythm. dupont chemist roy pluckett invented teflon when the gas he was working with cooled into flakes. and on august 26, 2011, vaulting past the usual steps of phase ii and iii trials, the fda approved pfizer’s drug crizotinib, which serendipity in the form of garcia’s test of camidge’s patients had plucked from the trash bin of a struggling trial.
paul bunn, md, holds an endowed chair— the James dudley chair in cancer research.
ross camidge, md, phd, clinical director of the thoracic oncology program, was chugging away on a drug trial for pfizer.
Every cell in your body holds the 20,000-or-so
genes it needs to do things like grow fingernails
and solve the New York Times crossword. But
not every cell needs to do all these things, and
so your body turns these genes on and off as
needed. For example, your body only needs the
gene that makes the protein ALK in the early
stages of your developing nervous system. After
you form your brain and other nervous good-
ies, the gene that codes for this ALK protein just
sits there silently on inchworm-like chromosome
No. 2, opposite another idle gene called EML4,
twiddling its genetic thumbs and thinking deep
thoughts about the weather.
That is, unless the gene is reactivated.
When you do unkind things to your body like
age, sunbathe, or let the car door bang closed
on your shins while unloading groceries, your
cells die. And so you need new cells. Your body
creates them by duplicating old cells. Only,
sometimes your body’s copy machine goes awry,
allowing mutations to sneak into the genetic
codes of these new cells.
Most of these mutations do everything
or nothing—killing the new cell or making no
difference whatsoever. A very few of these
mutations lead to cancer.
One of these oncogenic mutations is the
ALK-fusion gene.
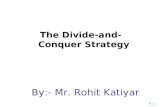
th e sc i e nc e of c r i zoti n i b
Unfortunately, in a very special 3-to-5 percent
of lung cancers, chromosome No. 2 folds back on
itself, like an inchworm bringing its back feet up
to just behind its front.
Now instead of exposing the code of its entire
belly, it shows a new code made from the gene on
its head (ALK) and the gene on its tail (EML4).
This squished-together code is the blueprint
for an ALK-fusion protein—called a “kinase”—
which sends signals telling cells to grow, split,
and survive in an out-of-control, cancerous way.
Crizotinib is an ALK inhibitor.
Like a kindergartner at a state fair, this
ALK-fusion protein needs to eat sugar in
order to function, in this case the sugar-like
molecule ATP.
But it can’t eat ATP if its mouth is plugged.
Crizotinib competes with ATP for space in the
ALK-fusion protein’s mouth—outcompetes,
actually—and if its mouth is plugged when
ATP comes along, then the ALK-fusion protein
can’t transmit its signal and the cell doesn’t
replicate out of control.
The gist is this: by blocking its energy,
crizotinib stops ALK-positive lung cancer cold
while leaving healthy tissues unharmed. Trials
at the University of Colorado Cancer Center and
elsewhere show that crizotinib halts the growth
of 90 percent of ALK-positive, non-small-cell
lung cancer patients. —Garth Sundem
but was it serendipity? louis pasteur said, “chance favors the prepared mind,” and in this case, the cu cancer center as a whole was that prepared mind. it was ripe for serendipity because paul bunn, marileila varella-garcia, ross camidge, andrew weikhardt, brian Kavanagh, dara aisner, wilbur franklin, robert doebele and all the other doctors and researchers—small in number but world-class in expertise, creativity and motivation—had built it that way.
“we’re small enough that i could walk down the corridor and knock on leila’s door and knock on bob’s door,” says camidge. and this melting pot of researchers, just big enough to have everything ellen smith needed but small enough to remain mixed and nimble, spawned a treatment with the potential to save 45,000 lives a year—that’s two-thirds of the average crowd at a denver broncos game.
imagine sitting in a nearly empty stadium. now imagine sitting in a full one. that is the difference of the drug crizotinib.
andrew weickhardt says, “no one thinks we’re going to pack up our bags and go home tomorrow, but the future seems brighter than it has for a long time in fighting lung cancer.”
Visit www.coloradocancerblogs.org to
• Watch a video about this story
• read related news articles
• make a donation to support lung
cancer research
• tell your story
chromoSome kink cauSeS cancer, iS perhapS aLSo itS cure
ALK
ALK
ALKA T P
A T P
AT
P
A T P
EML4
EML4
EML4
ALK-fusion protein
A T P ALK-fusion protein
ALK-fusion protein
DEC DINgcancerg
Len
n a
sa
Ka
Wa
Lyn
n c
Lar
K

www.coloradocancercenter.org
10C3: Winter 2011
11
A CoNVErSATIoN wITH Jonathan Gutman, mD
md C L I N I C A L C A R E
c3: first, how is your patient?
Gutman: She’s doing great. we infused her with
2.7 billion stem cells grown from donated umbilical
cord blood, and instead of the average hospital
discharge at 30 or 40 days after treatment, she was
able to go home to her large family and new baby
11 days after her stem cell transplant.
c3: is this stem cell transplant the same
as a bone marrow transplant?
Gutman: Yes and no. In a bone marrow transplant,
for a blood cancer like leukemia, you first knock
down a patient’s blood system with chemotherapy
and radiation, and then use a bone marrow trans-
plant from a matched donor to regrow it. In fact, it’s
the stem cells in the marrow that regrow a patient’s
blood system. But in this case we removed the
stem cells from banked umbilical cord blood and
grew them in the lab first before infusing them.
assistant professor, medical oncology, program for hematological malignancies and stem cell transplant, university of colorado school of medicineco-medical director, university of colorado cord blood bankB Y GA RT H S U N D E M
c3: if it’s the job of stem cells to grow more
cells, why was it important to grow them in
the lab first? Why couldn’t you just inject
these umbilical cord stem cells into the
patient and let them do their thing?
Gutman: we have in the past—doctors inject
patients with umbilical cord stem cells and eventu-
ally these stem cells repopulate the blood system,
as we’ve seen. But the key there is “eventually.”
In a typical unit of cord blood, there just aren’t
enough cells to quickly restart the immune system,
and in this time between blood systems, patients
are at desperate risk of infection.
c3: Does this new treatment help close the
window of danger?
Gutman: Yes, or at least it seems that way so far.
I trained at the Fred Hutchinson Cancer research
Center, where this stem cell treatment was devel-
oped. The Hutch treated 11 patients in Seattle
and this was our first patient in Colorado, the 12th
patient in the world to undergo this procedure. So
far, it looks as if growing these stem cells before
infusing them makes enough new blood to create
a functioning immune system in less than half the
time it takes the standard cord blood transplant.
c3: is this an improvement even for people
who can find a matched donor?
gutman: with a matched donor, you have the
opposite problem—you can infuse enough bone
marrow stem cells to cut down on the time a
patient spends without an immune system, but
because you need such a high degree of match
between the new blood and the patient’s old blood,
the new blood may not recognize traces of the
on the morning of aug. 19, 2011, young researcher Jonathan Gutman, mD, and the stem
cell transplant team infused a patient at the university of colorado cancer center with
stem cells grown from donated umbilical cord blood. in this phase i clinical trial, the
recently pregnant patient was fighting for her life, having delayed treatment for leukemia
so that her child could develop long enough to live. here we talk to Dr. Gutman about his
work and about this fascinating new treatment.
patient’s original, leukemic blood as foreign and
so may not eradicate it entirely. Unless you use a
high level of chemotherapy, patients may relapse.
Then again, some patients might not be able to
withstand that degree of chemo. It looks as if this
trial with expanded cord blood stem cells may
solve both problems—you grow enough to restart
the immune system but you also leave a degree
of mismatch that allows the new blood system to
wipe out traces of the old.
c3: it seems strange that nobody thought
of this before.
Gutman: It wasn’t that they didn’t think of it—the
idea of using donated cord blood to grow more
cord blood has been around for quite some time.
only, it’s not as easy as it sounds. In the past,
we’ve been able to grow more cord blood, but
not more cord blood stem cells. You treat them to
grow, but they mature and lose their “stemminess.”
This trial uses a brand new technique, growing this
cord blood in the presence of a special protein that
makes the umbilical cord stem cells create more
stem cells, not just more blood. Before this system,
getting a 10- or 20-fold expansion of stem cells
was considered a success, and now we’re getting
a 500-fold expansion of these cells.
c3: that’s how you got the 2.7 billion stem
cells you infused into your patient?
Gutman: Yes, exactly.
c3: Where does it go from here?
Gutman: well, this procedure is still in a phase
I clinical trial, but it definitely shows promise. we
hope to see success with more patients. And then,
in general, we’d like at the CU Cancer Center to
use this springboard to develop more of our own
science, our own trials, in addition to continuing to
test promising therapies developed at Fred Hutch
and elsewhere. This is an up-and-coming program
with the potential to become a national leader.
For an in-depth look at this clinical trial, Dr. gutman’s work and his patient,
see an accompanying article (and video) in the target: cancer section
of the CU Cancer Center news site, www.coloradocancerblogs.org.
the last-ditch doctorlia gore gives Kids and adults with cancer one more chance against all odds
Lia Gore’S Life haS been about
borroWeD time.
Before gore was born, her mother beat breast
cancer. “Everything I do feels like the bonus round,”
says the pediatric oncologist and head of the
Children’s Hospital Colorado Experimental
Therapeutics Program.
That feeling of extra time, she says, drives her
work in finding the next best treatment for every
patient she meets. “I love the fact that there are
kids alive today who had the odds against them.
And of all those kids who ultimately didn’t survive,
a lot of them lived with very high qual-
ity for longer than anyone expected.
we’re not just conducting research
for the greater good, but for the
very realistic chance that children
can benefit from research going
on today.”
gore, a CU Cancer Center inves-
tigator, knew at the age of 12 that
she wanted to take care of kids with cancer, and
she pursued the dream, landing at Children’s and
the University of Colorado School of Medicine for
her pediatric residency in 1996 and stayed for
her pediatric oncology training. In 2001 her post-
doctoral research training was over, and she didn’t
know what to do next.
“I needed a job, and I wanted to stay in Denver,”
she recalls. “I had two very good mentors who said,
‘Let’s think about what’s missing here. You’re not
afraid of people who are really sick, and you have
a good research mind.’”
That missing piece: an early clinical trials pro-
gram for kids with cancer. In fact, at the time kids
with the types of cancers most common to the
age group—leukemia and brain tumors—were
excluded from clinical trials.
one mentor, pediatric oncologist Steve Hunger,
MD, suggested gore apply for a training grant from
the National Institutes of Health called the Paul
Calabresi Fellowship, a prestigious training program
that teaches clinicians how to conduct basic and
translational research. gore got that training grant,
and also a mini-fellowship in drug development at
the National Institutes of Health.
She used the first year of her Calabresi
funding—and critical protected time away from
the clinic—to create a business plan for what
would become the Children’s Experimental
Therapeutics Program. Then she sold the idea to
Children’s leadership. “It’s a very expensive enter-
prise that Children’s supported well,” she says.
In a few, short years the program would
become one of the most prestigious phase I
pediatric clinical trials programs in the country,
leading the way to allow children with leukemia
and brain tumors to participate.
In 1999 the CU medical school
had recruited a clinical trials
expert—colon cancer physician
and drug development guru gail
Eckhardt, MD. gore reached out to
Eckhardt, who was building a phase
I clinical trials program at University
of Colorado Hospital. In August
2001, she started working in the
adult phase I clinic with Eckhardt, “because in order
to do it well in kids, I needed to learn how to do it
well in adults.”
In the years since, gore has directed more than
100 clinical trials for children and adults. She sits
on advisory panels to the National Cancer Institute
and the executive committee on acute lympho-
blastic leukemia for the Children’s oncology group,
a national clinical research consortium. She also
cofounded the Pediatric oncology Experimental
Therapeutics Program, a network of 11 large aca-
demic medical centers that promotes development
of new, promising therapies for kids, adolescents
and young adults with cancer.
She still cares for adult phase I patients at the
CU Cancer Center. But working with kids with
cancer is still her first love. Her office at Children’s
is filled with photos and notes from patients and
their families reporting in on life.
“Parents are afraid we’ll forget their kids,” she
says. “They may underestimate the impact these
kids have on us. Every kid is inspirational because
they keep walking through the door every day,
no matter what happens to them.”
She remembers one of her first patients,
a teenage girl from Highlands ranch, who asked
her why she was a doctor.
“I told her, ‘Because I want to cure cancer.’
She looked at me and said, as only a teenager
could, ‘Um … you already have.’ Meaning I had
already cured her cancer. I think about that a lot
because for that one kid, it’s true. Sometimes
I feel completely inadequate because some kids,
I haven’t saved. But my Mom’s story taught me
that I’m not smart enough to predict the future.
we don’t know who can be cured and who can’t.
The fact that there are kids who are alive because
of the things we’ve done keeps me coming back
to work.”
A patient comes to the phase I clinical trials
program because standard therapy failed. gore
says people consider her the “last-ditch doctor.”
“That may be true, but my goal is to help
my patients live the life they want to live, for as
long as they can,” she says. “Ultimately, I want
to cure everyone who walks in the door, but
I also know 7-year-olds who have lived better
than 90-year-olds. It’s how you live your life that
really matters.”
ABoUT LIA gorE, MD
director, experimental therapeutics program, children’s hospital coloradoassociate professor of pediatrics and medicine, university of colorado school of medicineco-founder and co-director, pediatric experimental therapeutics investigators consortium
b y l y N N C l a r k
my goal is to help my patients live
the life they want to live, for as long
as they can.
Bed
ro
ca
n/f
Lic
Kr
Lyn
n c
Lar
K

www.coloradocancercenter.org
12C3: Winter 2011
13Joel wanted to live long enough for daughter emerson to remember him. he has had melanoma for her whole life.
“your entire life is taken into consideration when you have this disease,” Joel says. “we decided to say yes to getting preg-nant and having a child. my regret is that we missed our window of opportunity to have more children.
in 1997, Joel and a pregnant danette moved from minnesota to longmont, colo., for Joel’s job as a technology company engineer. several months after arriving, he noted something on his abdomen. an X-ray revealed something in his lung. his family practitioner sent him to rene gonzalez, md, director of cutaneous oncology at the cu cancer center and university of colorado hospital. a couple of cts later, gonzalez delivered Joel’s second death sentence: the spot on his lung was melanoma.
Joel’s question to gonzalez: “what are we going to do next?”the answer: two-and-a-half years on a clinical trial that held
his disease at bay but didn’t shrink the tumors, followed by nine months of chemotherapy that had the same effect but made Joel so sick he had to stop. the tumors started growing again. in a last-ditch effort, Joel began biochemotherapy. the treatment is so poisonous that patients are admitted to the hospital rather than getting treatment in an outpatient infusion center. he endured two complete cycles. his tumors kept growing.
Joel doesn’t remember details about his hospitalization, but does remember his wife’s stalwart support, despite having
super survivorit’s august 2011, and about a dozen doctors, nurses, and clini-cal trials specialists mingle on the second floor of the anschutz cancer pavilion. as sunlight spills in from the high windows, they laugh and look at the sheet cake, decorated with a cartoon of superman while they wait for the guest of honor: Joel.
clinic scheduler christine miller coined his superman nickname. “we’ve never had a patient like Joel before,” she says. “i don’t
know if it’s his faith, or his amazing positive attitude. he’s a super-survivor, and to us, that makes him superman.”
a guest, scott holden, md, has come in from california, where he is senior medical director at the pharmaceutical giant genentech. in 2001, holden was wrapping up his oncology fellow-ship in the center’s phase i clinical trials clinic, where he found the drug trial that is holding Joel’s cancer in check.
“Joel is a reminder of what we’re trying to do, and a reminder of what got me into this line of work,” holden says. “one of the things about phase i clinical trials: you don’t expect things like this—for patients to survive for a decade. there is no way you let something like this go unnoticed.”
Joel arrives with wife danette and 13-year-old daughter emerson in tow. he’s tall, with an athletic build. you’d never guess he’s a cancer patient.
with graying red hair and green eyes, he’s the poster child for melanoma risk. add to his genetics his youth spent as a lifeguard and outdoor tennis champion with nothing but a zinc-oxided nose to protect him—today’s sunscreen did not exist, nor did public awareness of the link between sun exposure and skin cancer—and his risk escalated.
he says he doesn’t blame god for his illness. he laughs and says, “i blame adam.”
Joel is quick to laugh. at the party, he accepts a piece of cake, hugs his wife, and hugs the individuals who have supported his care over the years. later, he says he’s not interested in the spotlight.
“the celebration was really for the people who worked with me for 10 years,” he says. “all i had to do was live.”
no stranger to clinical trialswhen Joel received his first six-month death sentence in 1988, he and danette scoured the country for a treatment. they found it at duke university, where a doctor harvested melanoma cells, irradiated them, then re-injected them to build up immunity. Joel traveled from minnesota to durham seven times in six months for the experimental treatment.
“the doctor said, ‘i probably bought you 10 years,’” Joel recalls. he was right. Joel lived cancer free for almost a decade.
all along, the groebners struggled with the decision to raise a family in the face of Joel’s cancer diagnosis. nine years after treatment at duke, danette became pregnant with their daughter emerson.
a toddler at home and a full-time job to manage. danette was by her husband’s side, praying for his recovery. not every family can survive cancer treatment. the emotional, financial, physical, and relationship stress can be as devastating as the disease.
“danette’s support is unbelievable,” Joel says, tearing up. “i can’t imagine doing it alone.”
when biochemo failed in 2001, Joel received his third six-month expiration date. gonzalez referred him to the center’s early clinical trials program, where he met holden.
enter pi -88finding an appropriate clinical trial for people who have failed all standard treatment or other experimental therapies often means “phase i”—or “first in man.” these drug trials are not expected to find something that works, but rather are meant to discover the correct drug dosage and how it works in a human body after it’s been tested in animal models.
most phase i chemotherapy clinical trials require blood trans-fusions. because Joel and his family are Jehovah’s witnesses,
Joel Groebner is a livinG testament to the power of phase i clinical trials, faith, and a positive attitude
b y l y N N C l a r k
d o n ’ t c a l l h i m
Superman
three times doctors have given Joel groebner just six months to live. and three times, experimental treatments have stopped the cancer.
Joel has melanoma. the cancer that started as a deep purple mole on the back of his right thigh in 1988 is now in his lungs and liver. today the disease is stable, thanks to an experimental drug he administers himself.
when he found the mole, surgeons at the hutchinson, minn. community hospital removed it and told him that most people—80 percent—with his size of tumor were alive five years later. three months later, during a yearly physical, doctors found a suspicious lymph node in his right groin. pathology showed melanoma cells. the cancer had spread.
that was the first time doctors told him to prepare for death. in terms of outcomes for melanoma, doing nothing and treating with chemotherapy has the same poor result. the best hope for patients with melanoma that has spread beyond the initial tumor site is a clinical trial.
perhaps doctors underestimated the perseverance and good fortune of the man known to college buddies as “super J,” because Joel didn’t prepare for death, and 23 years later, he is alive and thriving.
“the celebration was really for the people who worked with me for 10 years,” he says. “all i had to do was live.”
Lyn
n c
Lar
K
nic
oLe
Ko
foed
nic
oLe
Ko
foed

www.coloradocancercenter.org
14C3: Winter 2011
15
and therefore choose not to take blood transfusions, finding an appropriate trial wasn’t easy.
“we’ve always looked for what new treatments might be available,” danette says. “we scoured the country for a trial, as did dr. holden. because we didn’t want the blood transfusion, it was disqualified, disqualified, disqualified.”
in august 2001, holden called and said, “i think i have some-thing for you.” melanoma tumors are highly reliant on blood vessels to deliver the energy they need to grow and spread. the experimental drug pi-88, manufactured by progen pharmaceuticals, inhibits blood vessel formation by targeting a vegf protein, cutting off its function and therefore starving the tumor.
as Joel started his first treatment week of pi-88, he and danette understood it was not likely to work, but they believed doing something was better than nothing.
the next month, Joel, danette and 3-year-old em traveled to minnesota for a family reunion. danette remembers it as awful.
“everybody knew what was going on—that we were there to say goodbye,” she recalls. “but no one said goodbye.”
Joel remembers it as a beautiful time of year.“Joel’s always been a glass-half-full guy,” his wife says, laughing.
“his amazing spirit is what has gotten him through this.”after just two cycles of four bi-weekly pi-88 shots, Joel’s tumors
shrunk by half, and then by half again during the next three years. his disease has been stable since.
saving Joel groebnerpeople who go on phase i cancer clinical trials are pioneers. they have almost always exhausted all other standard therapies. and they enroll in the trial with eyes open and no guarantees.
by participating, they help scientists gather information that may help future patients because, unfortunately, most people on phase i clinical trials do not survive as long as Joel. the average life expectancy for someone with metastatic melanoma is months, not years, and certainly not decades.
ask Joel about the broader purpose for his participation in a clinical trial, and he’ll be blunt. “it’s fantastic that they’ve found something that will work for others, but in the beginning, i was not thinking about the greater good. all i cared about was saving Joel groebner.”
Julie banahan, an oncology nurse, has been on Joel’s care team for a decade. “he is the definition of superman,” she says. “his attitude is inspiring. he has great karma. you just feel it.”
lia gore, md, who took over Joel’s care when holden moved on, says, “Joel is defying the odds. he’s at the intersection of sci-ence and technology and a few lucky guesses. who ever thought that he’d live to see his kid go to kindergarten? he’s a vibrant, contributing member to our society.”
Joel says he’s been motivated to fight his disease by the desire to have em remember him. the couple learned that long-term memory kicks in around age 4 or 5. “we weren’t thinking about 10 years,” danette says. “we just wanted em to remember her dad.”
“now i just want to survive her adolescence,” Joel jokes.the groebners say living with Joel’s illness for their entire
marriage has taught them, “you can be happy in the most awful circumstances.”
“your priorities change,” danette says. “we find ourselves asking, ‘is this worth arguing over?’”
today, Joel is more concerned with developing a secondary cancer from radiation exposure he’s had over the years from ct scans than dying from melanoma. he jokes about worrying about his weight and cholesterol—health concerns the average advanced cancer patient doesn’t have.
he says he is grateful for the experimental drug that holden found for him, which has allowed em not only to remember him, but to know him. he’s grateful for the extraordinary team at the cu cancer center who have supported him and become his friends. he is grateful for his health insurance, saying, “i must be the $6 million man by now”—referring to the cost of his treat-ment to date.
most of all, he is grateful for his wife, and for his daughter, and for his life.
“some people get cancer and say, ‘i’m done,’” he says. “i don’t get it. if this stops working, i know i have other options. i don’t care what kind of treatment comes next. i have to do something. i can’t give up. i have too much to live for.”
make a donation to support cancer clinical trials at the CU
Cancer Center at www.coloradocancerblogs.org/give.
patients like Joel Groebner (page 12) and ellen Smith (page 4)
are examples of people living at the cutting edge of medical
science. both are taking “experimental” cancer drugs, and
the therapies are keeping their diseases in check. cancer clinical trials—the highly regulated and monitored
system that tests new drugs, new combinations of drugs and other treatments that are not approved for use by the food and drug administration—are part of standard care at academic cancer centers like the university of colorado cancer center.
today, nearly every patient at the center’s lead care partners— university of colorado hospital and children’s hospital colorado—are evaluated to see if can be offered the option of a clinical trial. evaluation often includes testing each patient’s tumor to see if the genes, proteins or other biologic factors the experimental drug targets are present. patients are also evaluated for a host of other factors, including their general health status and the treatments they’ve been on before.
not all cancer patients are on a phase i clinical trial. in fact, those trials are usually reserved for patients for whom standard treatments have failed. the experimental drug may be their best remaining chance for a response.
f irst in mannew therapies are tested extensively in animal models to see if they work—kill cancer in the way they are designed to—before they are brought to people. often the drugs are created by pharmaceutical companies, and the companies come to academic cancer centers to “translate” the successful lab discoveries into human patients via a phase i clinical trial.
these so-called first in man trials aren’t looking for whether the drug kills the cancer. instead, the goal is to determine how it behaves in a human. the clinical trialists—physicians and nurses trained to specifically conduct clinical trials—are looking for dose-limiting toxicities to characterize the body’s general tolerance of the agent. the first group of patients gets the lowest dose, and then the amount of the drug or frequency is increased until patients get intolerable side effects. when that dosage is determined, the drug can move on to phase ii testing, where further efficacy testing comes into play.
sometimes, a small percentage of patients will see their tumors shrink or disappear with an experimental agent. in the past, when trial data was collected on paper and analyzed months after all patients had completed the protocol, these patients were often overlooked. but today, data goes back to the trial sponsors within days or even hours of the patient visit thanks to electronic medical records and databases.
real-time access to what’s happening in that patient allows doctors to notice trends when they can be taken advantage of. time is money, and time is life for these patients.
if a small number of patients respond to the drug, clinical researchers can usually figure out what the commonalities are and open a secondary arm of the trial that enrolls only patients with those features. that’s what happened with crizotinib and patients with the alK fusion protein in lung cancer, and as a result, the drug is now approved by the fda for treating those patients just three years after it entered phase i trials. —lynn Clark
phaSe i cancer triaL
Only cancer patients can enroll
Patients with limited treatment options
Patients do not receive monetary compensation
Standard care procedures are billed to insurance or the patient
All study treatments and procedures are covered
Patients undergo extensive monitoring
Goal is to determine correct dosing schedule and toxicity
Also looking at specific characteristics of this patient and this tumor
other phaSe i triaL
Normal population can enroll
Patients aren’t being treated for a particular disease
Patients often receive monetary compensation
There is no standard care to compare the new drug to
All costs are covered by the trial
Patients undergo extensive monitoring
Goal is to determine levels of toxicity
Not targeted
c a n c e r t r i a l s v s o t h e r t r i a l sall drugs, regardless of disease, have to be extensively and carefully tested before the fDa will approve them for regular use in humans.
but cancer clinical trials are different from the trials you might hear advertised on the radio. here’s how, using phase i trials as the example.
ST rYinSiDe
above: lia gore, md, here with Joel and scott holden, says Joel is defying the odds. right: pi-88.
To search for a cancer clinical trial, visit
www.uch.edu/conditions/cancer/research/research_trials/
p h a S e I C l I n I C a l T r I a l S p u t c a n c e r p at i e n t s o n t h e c u t t i n G e d G e
Lyn
n c
Lar
Kn
ico
Le K
ofo
ed

www.coloradocancercenter.org
16C3: Winter 2011
17
the prostate, lung, colorectal and ovarian cancer (plco) screening trial has been the energizer bunny of cancer trials—going and going and going. after 19 years of research on 13,166 coloradans, the university of colorado cancer center’s plco screening center is closing shop at the end of 2011.
“conducting a study for 19 years is a long time,” says e. david crawford, md, principal investigator of colorado’s plco trial and cu cancer center investigator. “we’ve really developed a family and have been able to retain phenomenal employees. i’m certainly going to miss everyone.”
started in 1992, the plco screening trial—a national cancer institute-funded randomized controlled trial—sought to deter-mine if certain cancer screening tests could reduce prostate, lung, colorectal and ovarian cancer deaths. according to the nci, these cancers are estimated to account for nearly 40 percent of all diagnosed cancers in the united states and 45 percent of cancer deaths in 2009.
the nci competitively selected 10 screening centers to recruit 55- to 74-year-old men and women with no plco cancer history. ultimately, the centers recruited nearly 155,000 par-ticipants across the country. patients were randomized into two arms: one that received annual cancer screenings and a second that received information about screenings.
“after all of these years, this study has been a huge learning experience,” says sheryl ogden, rn, bsn, plco project man-ager. “when i took this position in 1993, our goal was to get 20,000 people to enroll in the study in colorado, but none of us had any idea how we were going to recruit that many people.”
rECrUITMENT, oLD-SCHooL STYLEin a world of facebook, twitter and flash mobs, direct mail may be viewed as an outdated marketing approach, but in the 1990s it was a valuable recruitment tool.
printed in turquoise and red and with “we need you to make a difference” on the cover, plco mailed brochures to tens of thousands of colorado households from 1993 to 2000, when the last participant was recruited. at the time, obtaining a list of eligible coloradans was easy.
“since this was before hipaa, we were able to ask university of colorado hospital for a list of every patient aged 65 to 74 who had never been diagnosed with cancer,” says ogden. “this gave us enough names for our first mailing, but we needed to find other ways to get names.”
after the first recruitment phase, the nci added ten years to the trial and allowed 55- to 64-year-olds to participate. this change opened the doors to new names and addresses. plco staff hit the jackpot through the colorado department of motor vehicles with a list of thousands of coloradans that met trial criteria. yet enrollment numbers still came up short. the staff resorted to purchasing mailing lists for residents of colorado springs, southern wyoming, grand Junction and northern colorado. in the end, colorado enrolled 13,166 participants.
rECrUITINg HISPANICS wITH DIFFErENT TACTICSin 1998, colorado’s population was approximately 12.9 percent hispanic, but plco enrollment was only 3.9 percent. to recruit more minorities, the nci decided to grant additional funding to plco sites interested in recruiting hispanics and african americans. colorado launched a 16-month hispanic recruitment campaign, “por nosotros y nuestros hijos,” which translates to “for ourselves and our children,” with input from hispanic community members.
direct mail did not work with this population, says sally tenorio, rn, bsn, plco hispanic retention coordinator. through speaking at churches, recruitment seminars and one-on-one community health clinic visits, the plco team recruited 1,062 hispanic participants—more than any other study site.
“we really had to connect with people at the community level in churches and clinics and explain the study to them,” she says. “[recruitment] took more face time. the hispanic community was very interested in how the outcomes of the study could be used to educate their family and children about their health. participants brought their entire families to the screenings so that they could also be informed and educated.”
HUMor, CrEATIVITY AIDED rETENTIoNwith 13,166 participants, plco staff were challenged to keep everyone engaged with the study over the long haul.
from bookmarks and pocket calendars to newsletters and birthday cards, the participants received six to seven communica-tion pieces per year. at first, colorado plco staff sent traditional cards to each participant, but then they decided to get creative. the card covers evolved into funny photos of plco staff riding go-carts, wearing western attire and hitting piñatas. at the end of the trial, a satisfaction survey revealed how much participants enjoyed the birthday and holiday cards, ogden says.
“we wanted participants to know the staff they were talking to on the phone and getting mail from,” ogden says. “they really enjoyed those cards and often wanted to know where they could get more pocket calendars.”
the colorado plco site became known for its high retention rates, and many of their techniques were put into practice across the country. about 90 percent of the people recruited were still engaged at the end of the colorado study, and about 67 percent will continue participating as the trial moves to a central adminis-tration in 2012.
FIrST SCIENTIFICALLY VErIFIED LUNg CANCEr SCrEENINg TESTbecause plco screening sites had experience with enormous randomized population trials, the the nci asked the sites to take on a new study in 2002. the national lung screening trial compared lung cancer screening with low-dose helical computed tomography, or ct, and standard chest X-ray.
from 2002 to 2004, more than 53,000 current or former heavy smokers aged 55 to 74 enrolled in nlst, including 3,743 coloradans. in 2011, nlst published ground-breaking results: participants screened by low-dose helical ct scans had a 20 percent lower risk of dying from lung cancer than participants screened by standard chest X-rays. it is the first scientifically verified lung cancer screening test, and its impact will be felt for generations.
though plco screening results published so far haven’t shown a reduction in prostate or ovarian cancer mortality from screening—results for lung and colon screenings are yet unpub-lished—the study collected significant amounts of data and biologic samples about people who have and have not gone on to get cancer. approximately 2.7 million biologic specimens, including blood and cell samples, are available to researchers for studies on a vast array of health questions.
“the study will impact future research for years to come,” ogden says.
THE END, BUT NoT THE ENDparticipants who agreed to continue in the study will be trans-ferred to a central center and followed for an additional five years. plco screening results will be updated and published in coming years.
as the study comes to a close, crawford says, the plco will be remembered as the study that “brought a lot of patients to the [university of colorado hospital], raised awareness of the cu cancer center and school of medicine, and contributed significant research dollars to this campus.”
by december, dust will disappear from office shelves, archives will be shipped across the country, and goodbyes between co-workers and friends will be endless. although the plco trial couldn’t outlive the energizer bunny, its results—and massive data set—will benefit cancer patients long into the future.
pLco Staff Share their GreateSt SucceSSeS throuGhout 19 yearS of reSearch on 13,166 coLoraDanS
b y k I m C h r I S C a d e N
Warriorsscreening
from bookmarks and pocket calendars to newsletters and birthday
cards, the participants received six to seven
communication pieces per year.
p l co
pLco at a GLance
155,000+ US PArTICIPANTS
13,116 CoLorADo PArTICIPANTS
19 yearS oF DATA CoLLECTIoN
2.7 miLLion BIoLogIC SAMPLES CoLLECTED
wITH rELATED oUTCoMES INForMATIoN
ima
ges
co
ur
tes
y o
f P
Lco
See a slideshow of more PLCo cards on our blog.

www.coloradocancercenter.org
18C3: Winter 2011
19
C O M M U N I T Y N E W SS U P P O R T E R
GoLferS aGainSt cancer, amc cancer funD Donate $200,000 for piLot proJectS
cancer LeaGue of coLoraDo commitS $2 miLLion toWarD enDoWeD chair
behind the curtain raises $115,000 for
the anschutz cancer pavilion
Behind the Curtain, a women’s-only event about
prostate cancer, raised $115,000 for the expan-
sion of the Anschutz Cancer Pavilion at the
University of Colorado Hospital. Entertainment
was provided by the creators of “girls only.”
Dinner in White raises the bar and $20,000
Modeled after the Diner en Blanc in Paris,
the 2nd annual Dinner in white, hosted by the
AMC Cancer Fund, raised $20,000 for cancer
research at the CU Cancer Center.
golfers Against Cancer and AMC Cancer Fund
have awarded $200,000 in seed grants to four
groups of CU Cancer Center investigators.
The grants will be used to investigate new
cancer solutions.
Through an annual summer golf tournament and
auction, golfers Against Cancer raised $91,000
for the CU Cancer Center. An anonymous donor
stepped in with an additional $9,000 to fund both
projects at $50,000 each. The group’s board
selected two projects to fund:
heather feigelson, phD and
Dara aisner, mD, phD: Feasibility Study
for Large-scale, Population-based Validation
of a Molecular Staging
David barton, phD and Jay hesselberth,
phD: Hepatitis C Virus Infections, Inflammation
and Liver Cancer
Since 2009, golfers Against Cancer has given more
than $200,000, which has resulted in an additional
$2 million in grants or matching funds.
Cancer League of Colorado has filled a unique niche for 43 years, providing seed grants for promising yet
untested cancer research projects to scores of CU Cancer Center researchers.
In September, Cancer League announced a $2 million
pledge toward a Cancer League of Colorado endowed
chair at the CU Cancer Center, a step further in advancing
world-class cancer research here in Colorado, says center
director Dan Theodorescu, MD, PhD.
Join AMC Cancer Fund on March 8, 2012,
for an evening of cocktails and hors d’oeuvres
celebrating Colorado women and supporting
the continued research and treatment of
women’s cancers at the CU Cancer Center.
Featuring guest bartenders from some of
Denver’s top establishments, Cocktails for
a Cure is an opportunity for women to have
a girls’ night out while participating in a silent
auction and sipping on signature drinks.
This year’s honorary chairs include Sue Allon,
Stacy Carpenter, Keri Christiansen, Evalinda
Urman and Libby weaver. Tickets are $150
and include heavy hors d’oeuvres, signature
cocktails, wine and beer. Purchase tickets at
www.amc.org/events.
Save the Date: march 8
cocktaiLS for a cure
“We know that collaboration is essential to the advancement of cancer research and supporting these grants is our opportunity to be a part of it.”
—alice norton, amc cancer fund ceo
read about cancer League’s president,
Gary reece, on page 18.
F CUS
gary reece is no stranger to philanthropy. Barbara,
his wife of 37 years, spent her career as a profes-
sional philanthropist for many Denver nonprofits.
His former boss also donated to multiple causes
and encouraged his employees to do the same.
while gary got behind his wife’s causes,
attending multiple local benefits and galas, he didn’t
directly involve himself in the fundraising until 2008.
That year, after 20 years of service as a financial
executive at M.D.C. Holdings, Inc., gary retired
and quickly found his cause—cancer research.
“I guess you can say I’ve learned from the
best when it comes to getting behind great
causes,” gary says.
Since cancer has claimed the lives of several
members of the reece family, including gary’s
father and Barb’s grandmother, it was natural for
the couple to join Cancer League of Colorado,
an all-volunteer nonprofit organization that raises
money to support cancer research in Colorado.
“Cancer League of Colorado is made up of
people who have been touched by cancer and
want to do something to keep the ones they love
alive,” gary says.
At the time of gary’s retirement, Barbara was
already serving as president of the organization.
Naturally, gary found himself assuming a leadership
role; and in 2009 he was elected to take over as
president. He is serving his second term.
“I enjoy working with people who are passionate
about what they do,” says gary. “It’s most reward-
ing when we’re able to pull the dollars together to
fund projects that make a difference and eventually
gain the attention and additional funding from the
National Institutes of Health.”
Filling a unique niche, Cancer League provides
seed grants for promising yet untested cancer
research projects—the types of grants no other
funder offers on a systematic basis in the rocky
Mountain region.
Scores of University of Colorado Cancer Center
researchers have earned these grants and parlayed
them into far larger grants from federal funders
such as the National Institutes of Health when these
early research investigations proved to be fruitful
lines of inquiry.
In September 2011, Cancer League made
its largest pledge to the CU Cancer Center when
it announced it would commit $2 million toward
an endowed chair, a step further in advancing
world-class cancer research here in Colorado,
says Dan Theodorescu, MD, PhD, center director
and professor of surgery and pharmacology at
the CU School of Medicine.
“Cancer League of Colorado has helped the
Cancer Center fund innovative science in the
pursuit of our goal of relieving suffering from
cancer,” Theodorescu says. “we may use this
chair to recruit an eminent cancer scientist who
will lead and pursue innovative cancer research
in areas of strategic importance to our center.”
In discussions with Cancer Center leaders,
gary asked, “How can we have the greatest
impact in the fight against cancer in the state
of Colorado?”
“It became very clear that, to be one of the
best cancer centers in the country, we need the
best doctors,” he says. “Some of these doctors
cannot be recruited without the benefit of an
endowed chair.”
This year, Cancer League didn’t stop
its funding with an endowed chair. In July, it
distributed an additional $600,000 in seed
grants to 18 CU Cancer Center investigators,
totaling more than $10 million in grants to the
Cancer Center since 1985.
By funding innovative cancer research projects,
Cancer League has played a key early-stage role
in treatments and tests that directly benefit cancer
patients around the world, including sputum testing
that aids noninvasive diagnosis of lung cancers.
Many of these grants, which are selected by a
scientific advisory committee that includes Cancer
Center members and other researchers, wind up
generating $20 in federal research funding for every
dollar they grant to a researcher in seed funding.
“we want to make sure all researchers in
Colorado know that we are here to help fund their
research projects and we hope to continue to grow
our research grant program to fund even more
great projects in Colorado,” gary says.
while gary may have planned to spend his
retirement on the golf course, he now spends his
time meeting with cancer researchers, managing
Cancer League’s day-to-day operations, and help-
ing his family further their careers and devotions.
“If being a part of the Cancer League wasn’t fun
and I wasn’t enjoying it, I wouldn’t be a part of it,”
he says.
putting stake in untested researchgary reece, pres ident cancer league of colorado
left: gary and barbara reece trade in the golf course for a more fulfilling retirement plan.above: gary rappels down a denver skyscraper at the cancer league ‘over the edge’ fundraiser.
Learn more about Cancer League of
Colorado at www.cancerleague.org.
b y k I m C h r I S C a d e N
“one of the first projects we funded—a gastro-
intestinal cancer tumor bank focused on colorectal
and pancreas cancer—has received a $1 million
grant from the National Institutes of Health,” says
Scott Pearson, golfers Against Cancer’s president.
“The project for acute myeloid leukemia has
already received an additional $660,000 and is
seeking an additional $5 million grant. These are
great examples of how a little donation can go
a long way.”
AMC Cancer Fund, one of CU Cancer Center’s
fundraising partners, also stepped in to fund two
additional projects at $50,000 each:
mair churchill, phD and heide ford, phD:
Pharmacologically Targeting Histone
Chaperones for Breast Cancer Treatment
michael Graner, phD, natalie Serkova,
phD and allen Waziri, mD: Metabolomics
of glioblastomas and Tumor Tissues in a Novel
organotype Tumor Slice Culture Model—
Stress responses and the Dynamic Tumor
Metabolome
ro
na
Ld W
Hit
e
ro
na
Ld W
Hit
e
ste
ve Z
PH
oto
gr
aP
Hy

www.coloradocancercenter.org
20
W I N T E R 2011
www.coloradocancercenter.org
c3: collaborating to conquer cancerPublished twice a year by University of Colorado Denver for friends, members and the community of the University of Colorado Cancer Center. (No research money has been used for this publication.)
editor: Lynn g. Clark | 303-724-3160 | [email protected] Writers: Kim Chriscaden, garth Sundemphotos: Lynn Clark, glenn Asakawa, Nicole Kofoed, ronald whiteDesign: EnZed Design
the cu cancer center consortium membersUniversitiesColorado State UniversityUniversity of Colorado BoulderUniversity of Colorado DenverinstitUtionsUniversity of Colorado HospitalChildren’s Hospital ColoradoNational Jewish HealthDenver Health Medical CenterDenver Veterans Affairs Medical CenterKaiser Permanente Colorado
visit us on the web: www.coloradocancercenter.orgThe CU Cancer Center is dedicated to equal opportunityand access in all aspects of employment and patient care.
univerSity of coLoraDo Denver
13001 eaSt 17th pLace, mSf434
aurora, co 80045-0511
r e t u r N S e r V I C e r e Q u e S t e d
40 years after the war on cancer began, i feel more hopeful than ever for my patients
T H E M E S S A G E
FroM THE DIrECTor Dan theoDoreScu,
mD, phD
as a cancer surgeon, I know how critical it is to remove
every last bit of cancer from my patient’s body. The more
that is left behind, the more likely it is that the cancer will
return. As a cancer biologist, I also know how critical it is to know
exactly what errant genes or proteins are causing the tumors to
grow and spread so they can be targeted with drugs that stop
those errant actions.
I also know that there is a fine balance between too much
healthy tissue removed, or too many healthy
cells dying, in the race to cure the patient.
we often throw around the term person-
alized medicine, and yet we assume that
everyone knows what we’re talking about.
The obvious definition in cancer is finding the
treatment that takes advantage of an individ-
ual patient’s tumor characteristics, including
the genes and proteins, the tumor environ-
ment and other mechanisms at play, to kill the
cancer. Integral to this success also requires
a fundamental understanding of the host—
the normal organism that harbors the cancer. This knowledge is
important in such aspects as harnessing the immune system to kill
the cancer as well as understanding how anticancer drugs may be
metabolized (broken down) by the patient.
Forty years ago when the National Cancer Institute was
formed, cancer treatment was in an era of cut it all out, give the
highest doses of chemotherapies possible or almost killing the
patient to save the patient. Four decades later, we now have
fine-tuned knowledge and technology that allows us to be more
precise, to do less harm in saving a patient’s life. If we could
see and understand the moon back in 1971, today we can see
and understand the planets in orion’s belt. Concepts that were
once just specs of light in a far mysterious distance are now real,
understandable and world-changing.
I believe we are in a perfect storm of technology, knowledge
and communication. As you’ll read in this issue of Collaborating
to Conquer Cancer, in Colorado we are making specific and
giant leaps forward through discoveries that only come from this
storm, and from leveraging the enormous pool of talent, experi-
ence and knowledge assembled in our 442 cancer
center members across the state. our cancer
center represents the majority of the state’s effort
in cancer research.
Standing behind them: our generous donors,
such as Cancer League of Colorado, whose vol-
unteer-driven organization has provided millions of
dollars in funding for start-up science projects, and
which has just committed to raising $2 million for a
new endowed chair in cancer research that will help
us recruit an outstanding cancer researcher. Also
standing behind them are the remarkable patients
and families who are on this journey with them.
Today, we are becoming more precise in our understanding
of the seemingly never-ending mechanisms of cancer as hun-
dreds of individual diseases. we are becoming more precise in
how we use that knowledge to personalize treatment for every
patient. And we are becoming more precise in how we test for
disease in the first place.
Forty years after cancer became a war, I feel more hope than
ever for my patients and for cancer patients all around the world
that we will prevail in this fight in our lifetimes.
“We now have fine-tuned knowledge
and technology that allows us to be more precise, to do less harm in saving
a patient’s life.”