C H E S T T U B E S ORIENTATION 2005. A Little History Chest tubes has a history as far back as 460...
11
C H E S T T U B E S ORIENTATION 2005
-
Upload
mark-rogers -
Category
Documents
-
view
212 -
download
0
Transcript of C H E S T T U B E S ORIENTATION 2005. A Little History Chest tubes has a history as far back as 460...

C H E S T T U B E S
ORIENTATION
2005

A Little History
• Chest tubes has a history as far back as 460 -377 B.C. to drain pus from the pleural sac surrounding the lungs.
• In 1876, a system was developed for continuous drainage into a jar filled with anti septic.
• It was not until the Korean war that chest tubes were used routinely.

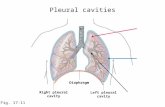
Importance & Purpose
• Used to drain blood, fluid, or air
• Prevents collapsing
• Enables the lung to re-inflate
• Relieves pain
• Used to manage life threatening situations

Incidence & Cause
• Air pressure build up in chest --- the lung collapsed
• Air build up in chest cavity --- the heart moves to opposite side of chest cavity
• Blood build up in chest cavity
• Air & blood build up in chest cavity with no improvement
• Chest wound with sucking
• Pus in chest cavity
• Fluid build up w/ s&s of bacteria, high acid content, low sugar content or high enzyme content

• Fatty white fluid present (Chyle)
• Clot busting drugs needed to remove clots from lungs.

Insertion / Placement
• Pain / comfort measures to the patient
• A small incision between 4th & 5th ribs.
• Small semi rigid tube is inserted and stitched into place
• Tube is placed to a drainage system
• Occlusive dressing is applied to insertion site
• An X ray is taken to confirm placement

COMPLICATIONS
• Infection of surgical site (tube removed and antibiotic begin)
• Bleeding ( replace tube)
• Blood Clots from trauma
• Re-expansion pulmonary edema (can be fatal)
• Tube kinking
• Improper placement
• Tube plugging

Care of Patient with Chest Tube
Pre-Insertion– Assess pt breath sounds, HR, BP, RR and
rhythm, and O2 Sat– Assure O2 and suction at bedside– Pain & comfort measures

Post Insertion, Maintenance
Assess patient breath sounds, HR, BP, T, RR and rhythm, O2 Sat, and comfort
Obtain X ray for placement confirmation
Assess insertion site, location and tube size
Check for fluctuations in air leak indicator
Check for air bubbles
Check for correct suction set level as ordered

Check drainage for amount, color, consistency
Check dressing for occlusiveness and drainage
Check chest wall at insertion site for subcutaneous emphysema
Must keep the drainage system upright
Secure the tubing as not to pull or tug and drainage is gravital

Reposition infant as tolerated and per policy
Change dressing as ordered
When clamping the tube, a padded hemostat is used