C Engaging the Dan River Region to Reduce Obesity fileEngaging the Dan River Region to Reduce...
13
Fam Community Health Vol. 35, No. 1, pp. 44–56 Copyright C 2012 Wolters Kluwer Health | Lippincott Williams & Wilkins Engaging the Dan River Region to Reduce Obesity Application of the Comprehensive Participatory Planning and Evaluation Process Jamie Zoellner, PhD, RD; Monica Motley, MSED; Margie E. Wilkinson, MS; Barbara Jackman, MHA; Morgan L. Barlow, MPH; Jennie L. Hill, PhD Despite ongoing recommendations to engage health-disparate populations in the initiation and execution of community-based research, few studies report on the process of community engage- ment. The action-oriented Comprehensive Participatory Planning and Evaluation (CPPE) process is designed to guide community health planning and evaluation. This article describes how the CPPE process was utilized within a community-based participatory research initiative aimed at ad- dressing obesity in the health-disparate Dan River Region. Encouraging community engagement in formulating research agendas and promoting ownership of health solutions will be key to improv- ing obesity risk factors among Dan River Region residents, and similar vulnerable communities. Key words: community-based participatory research, health status disparities, obesity, process assessment C OMMUNITY-BASED participatory res- earch (CBPR) is a recognized appro- ach to identify and address social and public health issues in health-disparate popula- tions. 1-3 Effective CBPR initiatives utilize the collective knowledge, expertise, and Author Affiliations: Virginia Tech, Human Nutrition, Foods, and Exercise, Blacksburg, Virginia (Drs Zoellner and Hill); Virginia Tech, Biomedical and Veterinary Sciences-Population Health Sciences, Blacksburg,Virginia (Ms Motley); Danville Regional Foundation, (Ms Wilkinson), and Get Fit Dan River Region, Danville, Virginia (Ms Jackman); and Duke Global Health Institute, Durham, North Carolina (Ms Barlow). The authors thank all members of the Dan River Region Obesity Task Force for their continued commitment to advance the mission of the community-academic part- nership. This study was funded by Virginia Tech’s Insti- tute for Society, Culture, and Environment, as well as funds from the Virginia Foundation for Healthy Youth. The authors declare no conflict of interest. Correspondence: Jamie Zoellner, PhD, RD, Virginia Tech, Human Nutrition, Foods, and Exercise, Integrated Life Sciences Bldg, 23, Room 1034 (0913), 1981 Kraft Dr, Blacksburg, VA 24061 ([email protected]). DOI: 10.1097/FCH.0b013e3182385cd9 resources gained through community- academic partnerships to develop and execute culturally effective interventions as prioritized by the community. 4-6 The initial 3 phases of CBPR include form- ing a partnership, assessing community strengths/dynamics, and identifying priority public health issues/research questions. These 3 phases are considered to be among the most critical. 1-2 These phases influence how prepared and engaged the community is to develop action-oriented plans, and how effectively the partnership can execute plans to produce desired outcomes and sustain their efforts. Central components in each phase are equitable and active participation of all partners, ideally from initial engagement, as well as sustainability and advancement of the partnership. 1-4,6-10 Various planning models have been de- veloped to engage community participa- tion in these phases; however, published studies documenting the extent of commu- nity member involvement through each of the core phases varies greatly. 6,11,12 Despite Copyright © 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited. 44
Transcript of C Engaging the Dan River Region to Reduce Obesity fileEngaging the Dan River Region to Reduce...

Fam Community HealthVol. 35, No. 1, pp. 44–56Copyright C© 2012 Wolters Kluwer Health | Lippincott Williams & Wilkins
Engaging the Dan River Regionto Reduce ObesityApplication of the ComprehensiveParticipatory Planning and Evaluation Process
Jamie Zoellner, PhD, RD; Monica Motley, MSED;Margie E. Wilkinson, MS; Barbara Jackman, MHA;Morgan L. Barlow, MPH; Jennie L. Hill, PhD
Despite ongoing recommendations to engage health-disparate populations in the initiation andexecution of community-based research, few studies report on the process of community engage-ment. The action-oriented Comprehensive Participatory Planning and Evaluation (CPPE) processis designed to guide community health planning and evaluation. This article describes how theCPPE process was utilized within a community-based participatory research initiative aimed at ad-dressing obesity in the health-disparate Dan River Region. Encouraging community engagement informulating research agendas and promoting ownership of health solutions will be key to improv-ing obesity risk factors among Dan River Region residents, and similar vulnerable communities.Key words: community-based participatory research, health status disparities, obesity, processassessment
COMMUNITY-BASED participatory res-earch (CBPR) is a recognized appro-
ach to identify and address social and publichealth issues in health-disparate popula-tions.1-3 Effective CBPR initiatives utilizethe collective knowledge, expertise, and
Author Affiliations: Virginia Tech, Human Nutrition,Foods, and Exercise, Blacksburg, Virginia (DrsZoellner and Hill); Virginia Tech, Biomedical andVeterinary Sciences-Population Health Sciences,Blacksburg,Virginia (Ms Motley); Danville RegionalFoundation, (Ms Wilkinson), and Get Fit Dan RiverRegion, Danville, Virginia (Ms Jackman); and DukeGlobal Health Institute, Durham, North Carolina(Ms Barlow).
The authors thank all members of the Dan River RegionObesity Task Force for their continued commitment toadvance the mission of the community-academic part-nership. This study was funded by Virginia Tech’s Insti-tute for Society, Culture, and Environment, as well asfunds from the Virginia Foundation for Healthy Youth.
The authors declare no conflict of interest.
Correspondence: Jamie Zoellner, PhD, RD, VirginiaTech, Human Nutrition, Foods, and Exercise, IntegratedLife Sciences Bldg, 23, Room 1034 (0913), 1981 KraftDr, Blacksburg, VA 24061 ([email protected]).
DOI: 10.1097/FCH.0b013e3182385cd9
resources gained through community-academic partnerships to develop andexecute culturally effective interventionsas prioritized by the community.4-6 Theinitial 3 phases of CBPR include form-ing a partnership, assessing communitystrengths/dynamics, and identifying prioritypublic health issues/research questions.These 3 phases are considered to be amongthe most critical.1-2 These phases influencehow prepared and engaged the communityis to develop action-oriented plans, and howeffectively the partnership can execute plansto produce desired outcomes and sustaintheir efforts. Central components in eachphase are equitable and active participation ofall partners, ideally from initial engagement,as well as sustainability and advancement ofthe partnership.1-4,6-10
Various planning models have been de-veloped to engage community participa-tion in these phases; however, publishedstudies documenting the extent of commu-nity member involvement through each ofthe core phases varies greatly.6,11,12 Despite
Copyright © 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
44

Engaging the Dan River Region to Reduce Obesity 45
ongoing recommendations to engage com-munity participation,6,11,13 a seminal CBPRreview by Viswanathan and colleagues6 re-veals that less than half of the studies reportedinvolvement of community members to helpto set priorities and generate hypotheses. Con-sequently, it is important to understand theprocess and utility of community planningmodels that actively engage community mem-bers in formulating and implementing health-related research agendas.
The Comprehensive Participatory Planningand Evaluation (CPPE) process is an action-oriented approach designed to guide projectplanning and evaluation in communities andconsists of 5 steps including: (1) problemassessments, (2) identification and selectionof potential interventions, (3) planning, (4)intervention proposal development, and (5)monitoring and evaluation.14 Each step in theapproach is flexible and may be adapted tomatch the current stage of the community inthe project development and execution pro-cesses. Many aspects of the CPPE process arecomplementary to CBPR.1-2,14 For example,the involvement of the community in all plan-ning phases aims to increase motivation andcolearning, and ultimately the success andmaintenance of the projects. Also, active par-ticipation by the community allows local ex-pertise and priorities to drive the research anddemonstrates that the community has the ca-pacity to solve its own problems.1-2,14 There-fore, utilizing the CPPE process within anongoing CBPR partnership has the potentialto transition a community into the action-oriented phases of research, while remain-ing true to CBPR principles. Once in theaction phases of research, integrating CBPRand CPPE promotes the sustainability of re-search efforts through the continued utiliza-tion of a community participatory structurethat promotes resource sharing and employslocal knowledge and expertise to drive thetranslation and dissemination of study find-ings. Despite the projected appeal and ap-propriateness of the CPPE process withinCBPR, only 1 known published study has ex-plored its utility and effectiveness.15 Further
exploration and utilization of CPPE withinother health-disparate communities providesvaluable information needed to more fullyunderstand how to appropriately engageat-risk communities to transition from theneeds-assessment phase to the intervention-planning and implementation phases.
Formation of the CBPR partnership andcommunity-needs assessment
The Dan River Region, located in south-central Virginia and north-central NorthCarolina, is a medically underserved region,suffering from health and economicdisparities.16,17 During the last 3 years, 3 com-prehensive needs assessments have beencompleted in this region.18-20 These needs ass-essments identified obesity as a priority healthissue for the region. In addition, concernsrelated to the capacity of community orga-nizations to design and implement effectiveand sustainable solutions were detailed.
On the basis of these assessments, inNovember 2009, the Danville Regional Foun-dation, the largest philanthropic foundationin the region, hosted the first roundtable “Re-gional Conversation on Obesity” to discussthe development of a unified community ef-fort. The Danville Regional Foundation in-vited representatives from key sectors, includ-ing civic, faith-based, public/private healthcare, local government, and education whohad previously demonstrated long-term com-mitment to addressing regional health issues.Research faculty from Virginia Tech, includ-ing a native of the Dan River Region, par-ticipated in the round table discussion. In-cluding Virginia Tech staff and faculty, 22of 24 (92%) invited regional stakeholders at-tended the roundtable. As a result, opportu-nities to develop a community-academic part-nership to reduce obesity were realized. Insubsequent follow-up meetings, 2 local orga-nizations, the Danville Regional Foundationand the Martinsville Henry County Coalitionfor Health and Wellness, pooled resourceswith Virginia Tech researchers to cooperateas the organizing steering committee for thepartnership.
Copyright © 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

46 FAMILY & COMMUNITY HEALTH/JANUARY–MARCH 2012
The steering committee organized a follow-up roundtable for previous invitees inFebruary 2010, and expanded the invitationlist to gain a wider representation of re-gional community members. Additional sec-tors invited included small business owners,county public health care providers, countyschools representatives, and grassroots so-cial justice organizations. Seventy percentof invited regional stakeholders attended.Meeting agenda items focused on exploringinterest in formally organizing a collaborativeobesity task force. The researchers formally in-troduced the principles of CBPR and the CPPEprocess as a possible approach to initi-ate obesity-related interventions. There wasan overwhelmingly positive response fromthe stakeholders to support a community-academic partnership. Because of the com-plex nature of the health disparities influ-encing obesity, the stakeholders confirmedthat a collaborative regional obesity task forcewas the most effective mechanism to assessand execute strategies beyond individual-levelinterventions to include various social andcommunity-level influences. Researchers andcommunity stakeholders agreed that a CBPRpartnership based on mutual trust, commit-ment to the process, shared learning, andshared power would be appropriate. Of theattendees responding to a brief survey, 93%expressed an interest in participating in a fu-ture CPPE workshop.
This article describes how the community-academic partnership executed each stepof the CPPE process to move from theneeds-assessment phase to the action-orientedphases. The ways in which the CPPE processhas empowered the partnership to launch re-search efforts prioritized by the CBPR partner-ship, hereafter referred to as the Dan RiverRegion Obesity Task Force, is also discussed.
METHODS
Study area and participants
The Dan River Region includes the cityof Danville, Pittsylvania county, and Henry
county in Virginia, as well as Caswell county,North Carolina. This predominately rural re-gion is suffering in the current economic re-cession with unemployment rates almost dou-ble those of the state and national averages.21
Furthermore, each of these counties havebeen designated by the US Department ofHealth and Human Services as a medicallyunderserved area.16 In the region, 50% arewomen, 27% black, 16.5% live below the Fed-eral Poverty Level, and only 9% have obtaineda bachelor’s degree.22 High indices of poverty,low educational attainment, and health dis-parities persist in each of these areas mak-ing this region 1 of the most health disparateregions in the Commonwealth.17,23 Despitethese challenges, a tremendous asset to theregion is the motivated stakeholders from avariety of public, private, and government sec-tors within each county willing to collaboratein addressing these concerns.
CPPE process steps 1 and 2: problemassessments and identification ofpotential interventions
An overview of the CPPE steps and associ-ated approaches executed by the Dan RiverRegion Obesity Task Force are illustrated inTable 1. The primary purpose of the problem-assessment phase of the CPPE process isto gain insight into the root causes of theidentified problem.14 This phase consists ofpreliminary problem assessment, the CPPEcausal analysis workshop, supplemental datacollection and model validation, and causalmodel data analysis.14 As mentioned, the re-gional roundtables and comprehensive needsassessments were previously executed andobesity was identified as the priority problem.Therefore, initiation from the “preliminaryproblem assessment phase” was not neces-sary. The causal analysis workshop providesa stepwise approach that allows interventionideas to emerge by working backwardfrom the identified priority problem toexplore the potential mechanisms and rootcauses of the problem.14 Unlike traditionalsocial science whereby causal models are
Copyright © 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

Engaging the Dan River Region to Reduce Obesity 47
Table 1. Summary of the CPPE Process and Results
CPPE Step Approach and Goal Participants Results
Step 1:problemassessment(April 2010)
*Obesity waspreviouslyidentified bythe communityas the priorityproblem
Causal modelworkshop
Goal(s):to identify rootcauses of obesity;create visual modelsfor these causes
Total attendance(n = 28 of 38 invited;74% participationrate)
Community members(n = 25);
Academic members(n = 3)
6 causal models:EducationNutritionSocial normsPhysical activityGeographic planningEnvironment
Step 2:identificationand priorityranking ofpotentialinterventions(April 2010)
Causal modelworkshop (day 2)
Goal(s):prioritize causal
models;develop potential
intervention ideasfor prioritizedmodels
Total attendance(n = 27 of 38 invited;71% participationrate)
Community members(n = 24);
Academic members(n = 3)
3 prioritizedinterventions:Social support to
promote physicalactivity
Social marketing toshift health-relatedcultural and socialnorms
Using communitygardens toincreaseaccessibility tofresh/local foods
*representing theprioritized causalmodels: physicalactivity, social norms,and nutrition
Steps 3 & 4:planning anddevelopment ofinterventionproposals(April2010–ongoing)
Monthlysubcommitteemeetings
Goal(s):HIPPOPOC tables to
further developinterventionideas14
develop, write, andsubmit fundingproposals toconductproposedinterventions
Total attendance(n = ∼ 25)
Community members(n = ∼18);
Academic members(n = ∼7)
Obesity Task Forcesubcommittees:
Nutrition (n = ∼9)Physical (n = ∼6)Education (n = ∼5)Social marketing(n = ∼5)
Interventiondevelopment:Subcommittees
utilize HIPPOPOCtemplates tofurther developintervention ideas14
Grant proposalssubmitted (n = 6)
Funded (n = 4)2; Virginia Foundationfor Healthy Youth2; Danville RegionalFoundation "Make itHappen!" Grants
(continues)
Copyright © 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
48 FAMILY & COMMUNITY HEALTH/JANUARY–MARCH 2012
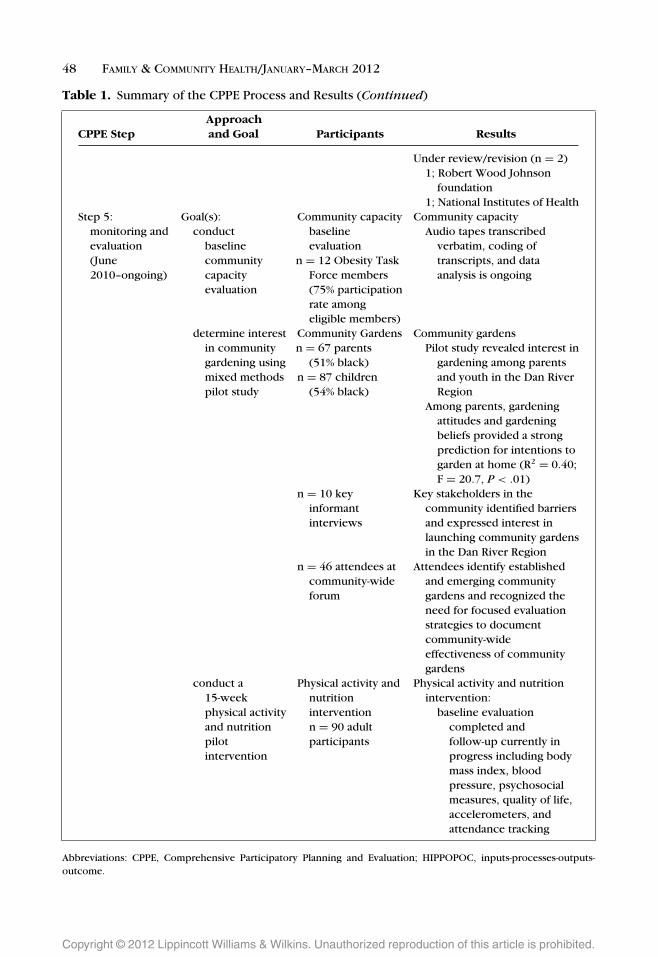
Table 1. Summary of the CPPE Process and Results (Continued)
CPPE StepApproachand Goal Participants Results
Under review/revision (n = 2)1; Robert Wood Johnson
foundation1; National Institutes of Health
Step 5:monitoring andevaluation(June2010–ongoing)
Goal(s):conduct
baselinecommunitycapacityevaluation
Community capacitybaselineevaluation
n = 12 Obesity TaskForce members(75% participationrate amongeligible members)
Community capacityAudio tapes transcribed
verbatim, coding oftranscripts, and dataanalysis is ongoing
determine interestin communitygardening usingmixed methodspilot study
Community Gardensn = 67 parents
(51% black)n = 87 children
(54% black)
Community gardensPilot study revealed interest in
gardening among parentsand youth in the Dan RiverRegion
Among parents, gardeningattitudes and gardeningbeliefs provided a strongprediction for intentions togarden at home (R2 = 0.40;F = 20.7, P < .01)
n = 10 keyinformantinterviews
Key stakeholders in thecommunity identified barriersand expressed interest inlaunching community gardensin the Dan River Region
n = 46 attendees atcommunity-wideforum
Attendees identify establishedand emerging communitygardens and recognized theneed for focused evaluationstrategies to documentcommunity-wideeffectiveness of communitygardens
conduct a15-weekphysical activityand nutritionpilotintervention
Physical activity andnutritioninterventionn = 90 adultparticipants
Physical activity and nutritionintervention:
baseline evaluationcompleted andfollow-up currently inprogress including bodymass index, bloodpressure, psychosocialmeasures, quality of life,accelerometers, andattendance tracking
Abbreviations: CPPE, Comprehensive Participatory Planning and Evaluation; HIPPOPOC, inputs-processes-outputs-outcome.
Copyright © 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

Engaging the Dan River Region to Reduce Obesity 49
developed on the basis of underlying theoriesand directional hypotheses as well as testedthrough empirical analytical techniques, thecommunity-engaged developmental step ofthe CPPE causal models are different. For ex-ample, CPPE causal models do not necessarilyhave to portray a hierarchal structure or infercausation, rather they are meant to uncoverthe complexity of problems and encourageparticipants to discuss potential solutions.Furthermore, while generating a testablehypothesis is certainly an intermediate goalof the CPPE process, it is not the central goalthat drives the initial steps in the buildingof causal models. Doing such could stiflethe communication and acceptance of theCPPE process when trying to engage diversecommunity stakeholders.
Remaining true to CBPR principles, thesteering committee structured the workshopto encourage equitable participation, and uti-lized a skilled facilitator who was independentof the community-academic team to lead theCPPE workshops. During day 1 of the work-shop, in a large group discussion, participantswere asked to “broadly describe their visionfor a healthy Dan River Region.” The facili-tator listed all responses on large easel pads.These responses reflected numerous aspects,which were all broadly related to health andhealthy living. The group then began to re-duce this list to those items specifically re-lated to obesity, and then sorted those itemsinto major themes, with care given to provideample discussion around potential gaps andoverlap of ideas. Six major themes emerged,and the facilitator randomly divided the par-ticipants into 6 small working groups withan average of 5 people per group. Before thestart of the meeting, colored sticky notes wereplaced underneath the unassigned chairs, andcolor matching was used for random assign-ment to groups. Members of the researchteam and steering committee participated ineach group. The role of research staff was tofacilitate all voices being heard in the smallgroups, and to document the process, butnot to actively direct the discussion. Eachgroup drafted creative visual representations
that linked the root causes, influential factors,and determinants back to their obesity-relatedtheme. A spokesperson from each grouppresented the information back to the largergroup.
During day 2 of the workshop, while in thelarge group, participants began to review thecausal models developed the previous day.To prioritize intervention efforts, participantsranked models that the newly developed Obe-sity Task Force and community were bestpositioned to address. Participants chose tofurther develop the top 4 models and thefacilitator randomly divided the group into4 small working groups with an average of6 people per group. To ensure consistency inthe continuous development of the models,the designated spokesperson from the previ-ous day remained with the same model; how-ever, the facilitator randomly reassigned theother community members to alternate causalmodel groups to offer fresh insights, alterna-tive ideas, and to encourage communicationamong the participants. One to 2 members ofthe research team and/or steering committeeassisted in each of the small group facilitationsbut did not direct the process. Participantsconcluded the workshop with a review andvalidation of the causal models and interven-tion priorities. Participants provided oral feed-back about the logistics of the workshops, aswell as steps to organize the next task forcemeeting to maintain planning and implemen-tation momentum.
At the end of each day, members of thesteering committee debriefed with the facil-itator. To honor and utilize the richness ofinformation provided by the participants, thecausal models were coded for componentstied to a social ecological framework.24 Socialecological frameworks attend to the personal,interpersonal, organizational, societal, and po-litical contexts in which behavior occurs, andhow these contexts influence individual be-havior. Two researchers independently codedthe root causes within the causal models into4 primary levels: individual, peer/family, localcommunity, and the larger society (Figures 1–4).24 These researchers then met to synthesize
Copyright © 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

50 FAMILY & COMMUNITY HEALTH/JANUARY–MARCH 2012
Figure 1. Education causal model.
findings, resolve uncertainty, and to gain con-sensus in socioecological coding.
CPPE steps 3 and 4: planning andintervention proposal development
In June 2010, the Dan River Region Obe-sity Task Force formalized its partnership andhosted its first meeting. A schedule for meet-ing frequency and structure were established.Quarterly meetings were organized as a largegroup meeting to promote development andprogression of the partnership. Monthly sub-committee meetings were organized aroundkey themes from the causal models and theprioritized intervention areas, and task forcemembers began to further develop interven-tion strategies. To aid intervention develop-ment, and as proposed in the CPPE pro-cess, subcommittees completed a HIPPOPOC
(Inputs, Processes, Outputs, Outcomes) tem-plate for each intervention.14 Key steps of theHIPPOPOC process include formulating andprioritizing broad objectives and design of in-terventions, as well as identifying inputs, pro-cesses, outputs, and outcomes.
CPPE steps 5: monitoring and evaluation
A variety of process and outcome evalu-ation methods have been initiated to pro-mote task force development and advance theprioritized interventions; however, monitor-ing and evaluation remain in the very earlystages. As described in Table 1, evaluation ap-proaches that have been launched include keyinformant surveys, cross-sectional surveys, arandomized-controlled trial, and environmen-tal mapping of physical activity and nutritionoutlets.
Copyright © 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

Engaging the Dan River Region to Reduce Obesity 51
Figure 2. Nutrition causal model.
RESULTS
Table 1 further summarizes participants in-volved in each of the CPPE steps and resultsto provide supporting evidence of successfulexecution of each CPPE step.
CPPE process steps 1 and 2: problemassessment and identification ofpotential interventions
Thirty-eight community members and 4members of the Virginia Tech research teamwere invited by e-mail and word of mouthto participate in the 2-part CPPE workshop.Snowball sampling, beginning with the atten-dees of both obesity roundtables, was usedto assist in identifying community membersto participate. Aligned with CBPR principlesand CPPE process objectives, targeted partic-
ipants represented or worked closely withthe communities most affected by obesity,agreed to collaboratively develop and imple-ment community-driven interventions, andwere dedicated to the immediate and long-term process to achieve the projected goalsof the Obesity Task Force. Stakeholders rep-resented the following sectors: health care,education, local government, civic organiza-tions, faith-based institutions, public schools,higher-education institutions, local businessowners, public housing, and community ac-tivism. On the basis of an average attendancerate for both days, 41% (n = 11) of the commu-nity participants were African American, 59%(n = 16) were white, and 85% were female.
As detailed in Table 1, 6 causal models weredeveloped. As a result of the causal modelworkshop, day 2 was used to further develop4 of the 6 models, as illustrated in Figures
Copyright © 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

52 FAMILY & COMMUNITY HEALTH/JANUARY–MARCH 2012
Figure 3. Social norms causal model.
1–4, into potential intervention ideas. Usingselection criteria set by the participants thatincluded areas of overlap, potential partner-ship opportunities, resource availability, andgeneral enthusiasm for an idea, 3 prioritizedintervention ideas materialized (Table 1).
CPPE steps 3 and 4: planning andintervention proposal development
Since the CPPE workshops, the ObesityTask Force has continued to meet monthlyto advance intervention development and im-plementation. Convening over a 90-minutelunch, attendees typically meet as a largegroup for 30 minutes, then divide into smallerworking subcommittees for the remainingtime. Subcommittees completed the HIP-POPOC intervention templates for a socialsupport physical activity intervention, a so-
cial marketing campaign, community gardenprogramming, and youth and school based ed-ucation wellness programming. As a result ofthis planning phase, the Obesity Task Forceprioritized and reorganized their subcommit-tees to focus on 2 interventions that gainedthe most momentum during development andwere best positioned to receive funding. Thenutrition subcommittee focused on develop-ing a community garden/education programlocated in the city of Danville, whereas thephysical-activity subcommittee focused on de-veloping and implementing a social supportphysical activity program in Caswell county.
The successful series of subcommitteemeetings and collaborative engagement ofcommunity and academic members has leadto successful grant proposals by membersof the Obesity Task Force. In September2010, grant funding was secured from the
Copyright © 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

Engaging the Dan River Region to Reduce Obesity 53
Figure 4. Physical activity causal model.
Virginia Foundation for Healthy Youth to fur-ther progress and evaluate the Obesity TaskForce, to plan and promote the developmentof community gardens, and to assess the nu-trition and built environment as it related toobesity. Two community members also suc-cessfully applied for and received the DanvilleRegional Foundation “Make it Happen” grantto launch their community garden projects.In addition, a Robert Wood Johnson Grant iscurrently under review to focus on the pub-lic health impact of community gardens andthe effectiveness of community gardening ef-forts to impact the “in home” accessibility offruits and vegetables among public housingresidents in the Dan River Region. Finally, anR21 National Institutes of Health grant pro-posal is under revision to advance the region’scapacity to provide social support program-ming to promote physical activity.
CPPE phase 5: monitoring andevaluation
The ongoing community capacity evalua-tion framework has included key informantinterviews of Obesity Task Force membersto establish the extent to which the partner-ship is collaborative, participatory, and pro-ductive. Development and execution of thistheory-based evaluation was guided by com-munity input and focused on community ca-pacity dimensions perceived as most relevantand appropriate to the progress of the ObesityTask Force.8,25
To advance the prioritized interventions,numerous other evaluations have beenlaunched. As a result of the nutrition sub-committee progress, a mixed methods studywas executed to inform development ofa community garden program in the DanRiver Region.26 The qualitative phase, which
Copyright © 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

54 FAMILY & COMMUNITY HEALTH/JANUARY–MARCH 2012
included 10 regional key informants, wasdesigned to elicit perceived benefits andchallenges of community gardens at theenvironmental, community, and individuallevels. The quantitative phase targeted low-resourced youth (n = 87) and their parents(n = 67), and included a variety of validatedtheory-based questionnaires to understandfactors impacting fruit, vegetable, and garden-ing behaviors. This research has provided thepartnership with a clearer lens to concep-tualize and launch future regional commu-nity garden efforts (unpublished manuscriptin review). In addition, the physical-activitysubcommittee pooled resources and acquiredadditional partners to launch a 2-group ran-domized 15-week nutrition and physical activ-ity pilot study called “Better Together: HealthyCaswell County.” The study aims to deter-mine the effectiveness of increasing accessto physical activity, with and without weeklynutrition and physical activity education ses-sions. Ninety participants were enrolled andsome of the outcomes being assessed in-clude body mass index, blood pressure, self-reported physical activity levels, self-reporteddietary intake, psychosocial measures, andquality of life. While the study is ongoing, pre-liminary analysis indicates a significant timeeffect and group by time effect for body massindex (unpublished data).
Finally, although not associated with aparticular subcommittee, global informationsystem (GIS) mapping and audit efforts areunderway to attend to the geographic andenvironmental causal models, and to betterunderstand the contextual factors related toobesity in the Dan River region. For exam-ple, block-level GIS maps are being developedto provide spatial data including walkability,physical activity resources, and food outlets inall 3 counties. Data collection and analysis arestill underway for each of these environmen-tal indices. In brief, a walkability index wascalculated from intersection density, residen-tial density, and land use mix for each blockgroup. Block groups were subsequently cate-gorized as high, medium, or low walkabilityon the basis of the calculated index.27 The
availability, type, and quality of physical ac-tivity resources are being assessed with thePhysical Activity Resource Assessment.28 Fur-thermore, baseline data on food quality,price, and availability is currently being col-lected and analyzed in accordance with theNutrition Environment Measurement Surveyprocedures.29 Once this data is collected, an-alyzed, and summarized, the information willbe shared with the Obesity Task Force, andwill be used to inform policy efforts and fu-ture intervention projects.
DISCUSSION
This article documents the process used tofoster a cohesive community-academic part-nership and discusses the interventions andevaluation data that reflect a successful part-nership. The CPPE workshop helped to ad-vance the capacity-building process and tran-sitioning the community into action-orientedplanning. Engagement of local expertise todrive the research and intervention prioritieswas a key aspect in launching this partnership.
Similar to Ndirangu and colleagues,15 wefound the CPPE process aligns with andfosters many of the fundamental principlesin CBPR, making it particularly useful insuch community-academic partnerships. Bydesign, the CPPE process is adaptive, pro-viding flexibility for those who are beyondthe needs assessment or problem identifica-tion stages.14,15 During the CPPE process pre-sented here, community members acted asthe experts for conceptualizing the obesity-related causal models, developing locally rel-evant interventions, and prioritizing thoseinterventions for collective success, honor-ing the overall CBPR mission of the partner-ship. Community and academic team mem-bers emerged as equitable owners for exe-cuting and evaluating interventions for thisregion.1,2 For this newly formed Obesity TaskForce, the interactive nature of the causalanalysis workshop initiated trusting relation-ships, which is noted as being a criticalcomponent to promote long-term successof partnerships.1-3 Promotion of partnership
Copyright © 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

Engaging the Dan River Region to Reduce Obesity 55
equity has transcended the ongoing monthlytask force and subcommittee meetings, as at-tendance and participation remains high, andtalented community members have assumedkey roles in leading agenda items.
In addition to supporting the evolution ofthis partnership, the results of the causal anal-ysis workshop positioned the Obesity TaskForce to readily develop ideas into pilotprojects and funding proposals. Early tangi-ble success is reflected in the causal mod-els, dynamic HIPPOPOC working documents,and submitted and funded grant proposals.Furthermore, the socioecological frameworkgrounding the casual models provides a theo-retical foundation to guide effective interven-tion development. Utilizing the causal modelsto encourage Obesity Task Force members tobe mindful of personal, interpersonal, organi-zational, societal, and political contexts influ-encing obesity will aid in the development ofcomprehensive programs. Importantly, otherCBPR initiatives have realized success throughapplication of the socioecological model toaddress health disparities.30 In addition, aneighboring rural community facing similareconomic and health challenges has demon-strated the importance of linking individualhealth behavior strategies to broader servicesand policies to improve regional health.31
Although there has been little applicationof the CPPE process to other CBPR coali-tions, our findings support the utility of theCPPE process to transition into an action-
oriented research agenda.15 For communitiesthat are further accomplished in identifyinghealth needs and building CBPR coalitions,the CPPE process offers a unique and action-oriented alternative approach to other tradi-tional comprehensive planning models.32-35
Given the dearth of published research re-lated to application of CPPE, future researchis needed to evaluate the utility of the CPPEprocess in other health-disparate communi-ties and across other health contexts. Thecontinued utilization of the CPPE process inthis community as well as in subsequent stud-ies can help to create a path by which theapplication and effectiveness of participatorymethods are looked at not only for communi-ties initiating progress, but also for those whohave achieved greater progress.
In conclusion, as a result of the CPPE pro-cess, a collaborative community coalition isuniquely positioned in the Dan River Re-gion to make collective steps toward obesityreduction and improved community health.Creating a sense of community power andpromoting community ownership of the in-dividual, social, and environmental healthproblems and solutions will be imperativeto improving the obesity risk factors andthe long-term health of residents in this re-gion. Continued monitoring and evaluationof these efforts are critical to understand-ing the long-term effects related to obe-sity, as well as partnership productivity andsustainability.
REFERENCES
1. Israel BA, Eng E, Schultz AJ, Parker EA. Methodsin Community-Based Participatory Research forHealth. San Francisco, CA: Jossey-Bass; 2005.
2. Minkler M. Community-Based Participatory Re-search for Health. San Francisco, CA: Jossey-Bass;2008.
3. Greenwood DJ, Levin M. Introduction to Action Re-search: Social Research for Change. Thousand Oaks,CA: Sage Publications; 2007.
4. Israel BA, Schultz A, Parker EA, Becker AB. Review ofcommunity based research: assessing partnership ap-proaches to improve public health. Annu Rev PublicHealth. 1998;19:173-202.
5. Wallerstein N, Duran B. Community-based participa-tory research contributions to intervention research:the intersection of science and practice to improvehealth equity. Am J Public Health. 2010;100(suppl1):S40-S46.
6. Viswanathan M, Ammerman A, Eng E, et al.Community-Based Research: Assessing the Evi-dence. Evidence Report/Technology Assessment No.99. Pub. No. 04-E022-2. Rockville, MD: Agency forHealthcare Research and Quality; 2004.
7. Berkowitz B. Studying the outcomes of community-based coalitions. Am J Community Psychol. 2001;29(2):213-227.
Copyright © 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

56 FAMILY & COMMUNITY HEALTH/JANUARY–MARCH 2012
8. Butterfoss FD, Francisco VT. Evaluating communitypartnerships and coalitions with practitioners inmind. Health Promot Pract. 2004;5(2):108-114.
9. Zakocs RC, Edwards EM. What explains communitycoalition effectiveness? A review of the literature. AmJ Prev Med. 2006;30(4):351-361.
10. Stith S, Pruitt I, Dees JE, et al. Implementing comm-unity-based prevention programming: a review of theliterature. J Prim Prev. 2006;27(6):599-617.
11. Cargo M, Mercer S. The value and challenges of par-ticipatory research: strengthening its practice. AnnuRev Public Health. 2008;29:325-350.
12. Westfall JM, VanVorst RF, Main DS, HerbertC. Community-based participatory research inpractice-based research networks. Ann Fam Med.2006;4(1):8-14.
13. David J, Zackus L, Lysack C. Revisiting communityparticipation. Health Policy Planning. 1998;13(1):1-12.
14. Lefevre P, Kolsteren P, De Wael M, ByekwasoF, Beghin I. Comprehensive Participatory Plan-ning and Evaluation. Antwerp, Belgium: TropicalMedicine; 2000. http://www.ifad.org/pub/bsf/cppe/cppe.pdf. Accessed February 10, 2010.
15. Ndirangu M, Perkins H, Yadrick K, et al. Conductingneeds assessment using the comprehensive partici-patory planning and evaluation model to develop nu-trition and physical activity interventions in a ruralcommunity in the Mississippi Delta. Prog Commu-nity Health Partnersh. 2007;1(1):41-48.
16. US Department of Health and Human Services.Medically underserved areas/populations. http://muafind.hrsa.gov/. Published December 4, 1997. Ac-cessed April 16, 2010.
17. Virginia Department of Health. Virginia health equityreport: unequal health across the Commonwealth: asnapshot. http://www.vdh.state.va.us/healthpolicy/documents/health-equity-report-summary.pdf. Pub-lished November 2008. Accessed July 16, 2010.
18. Beachler M; MPB Consulting. Obesity preventionand reduction program development report forthe Danville Regional Foundation, MPB Consulting,Chapel Hill, NC. 2009.
19. Byington R, Naney C, Hamilton R, Behringer B; MDC,Inc. Dan River Region health assessment. http://www.danvilleregionalfoundation.org/region/documents/2008-CommunityandEconomicDevelopment.pdf. Published October 2007. Accessed June 16,2010.
20. Virginia Department of Health. Commonwealth’shealth approach and mobilization plan for inactivity,obesity, and nutrition (CHAMPION). Richmond,VA: Virginia Department of Health; 2006. http://www.vahealth.org/NuPAFP/Champion/Files/PDFs/CHAMPION%20Obesity%20Prevention%20Plan.pdf.Accessed June 16, 2010.
21. US Department of Labor. Regional and stateunemployment. http://www.bls.gov/news.release/
pdf/laus.pdf. Published February 2011. AccessedMarch 16, 2011.
22. US Census Bureau. State and county quickfacts.http://quickfacts.census.gov/qfd/states/51/51143.html. Published July 2009. Accessed January 9, 2011.
23. Woolf SH, Jones RM, Johnson RE, et al. Avertabledeaths associated with household income in Virginia.Am J Public Health. 2010;100(4):750-755.
24. Stokols D. Translating social ecological theory intoguidelines for community health promotion. Am JHealth Promot. 1996;10(4):282-298.
25. Granner ML, Sharpe PA. Evaluating community coali-tion characteristics and functioning: a summary ofmeasurement tools. Health Educ Res. 2004;19(5):514-532.
26. Zanko A, Bonner J, Motley M, Chau C, Zoellner JM,Hill JL. Exploring community gardens in a health dis-parate population: findings from a mixed methodspilot study. Ann Behav Med. 2011;41(S1):B-081.
27. Chau CN, Luebbering CR, Kolivras KN, Zoellner JM,Hill JL. Using GIS to Determine EnvironmentalFactors Related to Obesity in a Health DisparateRegion. Presented at: International Society for Be-havioral Nutrition and Physical Activity; Melbourne,Australia; 2011.
28. Lee R, Booth K, Reese-Smith Y, Regan G, Howard H.The Physical Activity Resource Assessment (PARA)instrument: evaluating features, amenities, andincivilities of physical activity resources in urbanneighborhoods [published online September 14,2005]. Int J Behav Nutr Phys Act. 2005;2:13.
29. Glanz K, Sallis JF, Saelens BE, Frank LD. Nu-trition environment measures survey in stores(NEMS-S)—development and evaluation. Am J PrevMed. 2007;32(4):282-289.
30. Wynn TA, Taylor-Jones MM, Johnson RE, BostickPB, Fouad M. Using community-based participa-tory approaches to mobilize communities for pol-icy change. Fam Community Health. 2011;34(1S):S102-S114.
31. Buckner-Brown J, Tucker P, Rivera M, et al. Racialand ethnic approaches to community health: re-ducing disparities by addressing social determinantsof health. Fam Community Health. 2011;34(S1):S12-S22.
32. Eng E, Blanchard L. Action-oriented community di-agnosis: a health education tool. Int Q CommunityHealth Educ. 2006;26(2):141-158.
33. Green L, Kreuter M. Health Promotion Planning.Mountain View, CA: Mayfield Publishers; 1999.
34. Hennessey SL, Smith ML, Esparza AA, Hrushow A,Moore M, Reed DF. The community action model:a community-driven model designed to address dis-parities in health. Am J Public Health. 2005;95(4):611-616.
35. Green LW, Kreuter MW. Health Program Planning:An Educational and Ecological Approach. NewYork, NY: McGraw-Hill; 2005.
Copyright © 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.