C. difficile and ASP Guidelines and Best Practices · Montefiore to take a position as a CDC, ......
39
C. difficile and ASP Guidelines and Best Practices Belinda Ostrowsky, MD, MPH, FSHEA, FIDSA February 27 and 28, 2018
Transcript of C. difficile and ASP Guidelines and Best Practices · Montefiore to take a position as a CDC, ......

C. difficile and ASP
Guidelines and Best Practices
Belinda Ostrowsky, MD, MPH, FSHEA, FIDSA
February 27 and 28, 2018

Disclosure
• I have no financial disclosures
• I have made a recent transition from
Montefiore to take a position as a CDC,
Medical Field Officer in NY (I will share our
Montefiore ASP experience)

C. difficile Issues as Targets for ASP
1. Testing
2. Formulary issues
3. Treatment of C. difficile (new agents/guidelines)
4. Review of antibiotic/medication use (before &
after C. difficile diagnosis)
5. ASP as part of the solution
6. Mention-- C. auris

CDC Antibiotic Threats Pathogen Est. Annual
Cases Est. Annual Deaths
Summary MDRO 2 million 23,000 Urgent (3) CRE 9,000 600 C. difficile 250,000 14,000 Severe (13) MDRO: Pseudomonas Acinetobacter
6,700 7,300
400 500
MRSA 80,000 11,000 VRE 20,000 1,300 Concerning (3) VRSA <5 <5
•CDC. Antibiotic resistance threat in the US. 2013. Available at http://www.cdc.gov/drugresistance/threat-report-2013/
•MDRO= multi-drug resistant organisms, CRE= Carbapenem Resistant Enterobacteriaceae, CDI= C. difficile, MRSA= methicillin resistant S. aureus, VRE= vancomycin resistant enterococcus, VRSA= vancomycin resistant S. aureus
•http://www.cdc.gov/drugresistance/biggest_threats.html

Faces of Resistance (C. difficile)
IDSA. Faces of Resistance. 2017
http://www.idsociety.org/Templates/threeColumn.aspx?pageid=32212254747
•My mom

Why ASP for C. difficile (CDI)?
• Rates of CDI remain high
• CDI is publically reported
• CDI transmission is likely multifactorial:
– Infection control, environment, inter-facility transfer
– Association with common antimicrobial use
• ASP offers strategies to prevention & control CDI:
– At several points in prescribing
– Complementary to other interventions
Lessa et. Al. N Engl J Med 2015; 372:825-834
Elixauser et al, AHRQ at:http://www.hcup-us.ahrq.gov/reports/statbriefs/sb50.jsp
Lesser et al. CID. 2012;55(S2):S65-70.

UK Experience CDI
•CDI Annual Lab Testing
•Nu
mb
er o
f R
epo
rts
•Interventions: Infection control
•+ ASP
•Public Health England. Health Protection Report- Infection Report. 2015. 9 (21).

ASP for CDI Patient Status
Normal flora
Disruption of flora
C. difficile colonization
C. difficile colitis
Fulminant colitis
Death from C. difficile
Steps
1. Antibiotic damage
2. CDI healthcare exposure
3. CDI toxin production
4. Toxin hyperproduction
5. Severe sepsis/shock
ASP Activities
Adapted from:APIC Guide to Prevention of C. difficile Infection. 2013,
• Formulary
• Abx before
• Appropriate testing
• CDI treatment
• Abx/Meds after

Stewardship of CDI Testing • Know what type of testing at your lab (don’t use toxin alone)
• Colonization varies (can be high 16-50%+)
• Who you test:
– Don’t test your patient for CDI if they had < 3 unformed stools in
the past day.
– Don’t test patients who received laxatives within the past 48
hours.
– Don’t retest (especially multiple on same day).
– Don’t test for cure.
• Timely Testing: delays affect the patient, surrounding patients and
reporting.
.ASM A Practical Guidance Document for the Laboratory Detection of Toxigenic Clostridium difficile 2010. http://www.asm.org/images/pdf/Clinical/clostridiumdifficile9-21.pdf
Hopkins One Minute Guide on C. difficile testing https://medicine-matters.blogs.hopkinsmedicine.org/2016/03/one-minute-guide-to-clostridium-difficile-testing/
2017 IDSA/ SHEA CDI in adults & Children. CID. 2018; 1-48- online IDSA site.

Formulary Issues and CDI:
• The Case for a new drug--Fidaxomicin:
– Enthusiasm over 1st new CDI therapy in 25 years
– Questions: efficacy, incremental benefits, appropriate
patients, costs
– ASP gathered stakeholders to review data and
discuss place in therapy
– Formulated institutional CDI treatment algorithm
– Presented findings/algorithm to P & T for approval
– New guidelines- time to reassess
• Other Formulary discussions: Preferential drugs on
formulary, restrictions (e.g. quinolones).

CDI Clinical Case You are treating a 50 y/o female with 4 episodes of watery
diarrhea per day. She was recently admitted 3 months ago with
C.difficile associated diarrhea, treated with oral metronidazole
500mg every 8h for 10 days with complete resolution. Now she
has a BP of 120/70, P 75, R 16, O2 100%, Tmax 99F. She has
no abdominal tenderness, normal bowel sounds and no
distention. WBC count is 13 with 80% neutrophils. Cr is 0.7,
Albumin is 4. Stool CDI test is positive.
What is the best regimen for this patient?
How do you guide your providers to the best
management of this patient?

A. Place on contact isolation, treat this episode
the same as her first episode of CDI
(metronidazole)
B. Place on contact isolation, start po
vancomycin 125mg every 6 hours for first
recurrence of CDI
C. Start oral vancomycin 250mg every 6 hours
D. Start oral vancomycin 125mg every 6 hours
with oral metronidazole 500mg every 8
hours
Answer: past would have been A, now
guidelines say B (with some caveats)

Written C. difficile Policy • For facilities with no current policy:
– Content areas to address • CDI Treatment
• Formulary/Criteria for novel drugs
• Review of antibiotics/ meds before and after
– Stakeholders to develop and review
– Dissemination and implementation plan
– Measure of uptake/ compliance
• For facilities with current policy:
– Extending/consolidation policies (testing, isolation, environmental cleaning)

Let’s step back and look at:
– Professional guidelines
– Literature
– Practical issues
to help us formulate our CDI policy…

Severe C. difficile Infection • Increased odds ratio for morbidity/mortality:
– age >70 years
– leukocyte count >20,000 cells/mL
– albumin level <2.5 g/dL
– creatinine level >2 mg/dL
– small bowel obstruction or ileus
– CT showing colorectal inflammation
• IDSA/SHEA simplifies:
– WBC > 15, 000 cell/ ml
– Creatinine level > 1.5 mg/ dl
Henrich. Emerg Infect Dis. 2009 March; 15(3): 415–422
2017 IDSA/ SHEA CDI in adults & Children. CID. 2018; 1-48- online IDSA site.

SHEA/ IDSA Guidelines
Topics 2010 SHEA/ IDSA CDI Guidelines
2017 SHEA/ IDSA CDI Updated Guidelines
General: Assessment Strength rec Quality of evidence
Adapted Canadian Task force: A-C I-III
GRADE System: Strong- Weak (S-W) High- Very low (HG-VL)
Additions N/A Pediatrics ASP 2 recs (A-II) 3 recs (S/M, best
practice)
2010 SHEA/ IDSA CDI in adults. ICHE 2010. 31 (5): 431-455.
2017 IDSA/ SHEA CDI in adults & Children. CID. 2018; 1-48- online IDSA site.

Treatment (adult)
2010 SHEA/ IDSA CDI Guidelines
2017 SHEA/ IDSA CDI Updated Guidelines
Initial, non- severe
Metronidazole 500mg oral (A-I)
Vancomycin 125 oral (S/HG) Fidaxomicin 200mg oral (S/HG) Metronidazole 500mg oral (W/HG)- if unavailable
Initial, severe
Vancomycin 125mg oral (B-I)
Vancomycin 125 oral (S/HG) Fidaxomicin 200mg oral (S/HG)
Initial, fulminant
Vancomycin 500 mg oral & PR (CIII)
Vancomycin 500 mg oral (S/M) & metronidazole (S/M) & PR (W/L)
1st recurrence
Same, based on severity (A-II)
Vancomycin (W/L), vancomycin taper (W/L) OR Fidaxomicin (W/M)
2nd + recurrence
Vancomycin taper (B-III) No metronidazole (neurotoxicity) (B-II)
Vancomycin taper or pulsed (W/L) Vancomycin then rifaxamin (W/L) Fidaxomicin (W/L) Fecal transplant (S/M)
2010 SHEA/ IDSA CDI in adults. ICHE 2010. 31 (5): 431-455.
2017 IDSA/ SHEA CDI in adults & Children. CID. 2018; 1-48- online IDSA site.

v Additional Treatment Issues
2010 SHEA/ IDSA CDI Guidelines
2017 SHEA/ IDSA CDI Updated Guidelines
Fidaxomicin Predates In many regimens IVIG Not addressed No rec Probiotics Not recommended (C-
III) “Insufficient Evidence”/No rec
PPI Not addressed “Insufficient Evidence”/No rec
Prolonged prophylaxis
No rec (C-III) “Insufficient Evidence”/No rec
2010 SHEA/ IDSA CDI in adults. ICHE 2010. 31 (5): 431-455.
2017 IDSA/ SHEA CDI in adults & Children. CID. 2018; 1-48- online IDSA site.

Vancomycin Oral for CDI
AHRQ. Early Diagnosis, Prevention, and Treatment of Clostridium difficile: Update. 2016. /http://www.effectivehealthcare.ahrq.gov/search-for-guides-reviews-and-reports/?pageaction=displayproduct&productID=2208

Vancomycin ASP Considerations
• Making oral Vancomycin solution from IV solution
– Pharmacy to compound
– Stability/ storage
• Optimizing dosing:
• Encouraging 125 mg for most cases (except fulminant)

Fidaxomicin RCT FIDAXOMICIN
Recurrence/Initial Cure
VANCOMYCIN Recurrence/Initial Cure
RR (CI)
Louie (2011)
39/253 (15%) 67/265 (25%)
0.61 (0.43, 0.87)
Corneley (2012)
28/221 (13%) 60/223 (27%) 0.47 (0.31,0 .71)
Total 67/474 (14%) 127/488 (265) 0.55 (0.42, 0.71)
•FDA approved based on 2 RCTs
•Excluded: life threatening CDI , > 1 CDI in 3 month, IBD
•Similar efficacy in hyperendemic strains
Implications: Who would benefit most with relative high cost? Candidate for ASP
Corneley, et al. Lancet Infect Dis 2012;12:281-9.
Louie, et al. N Engl J Med 2011;364:422-31.

Probiotics Probiotic Type Studies Outcome
lactobacillus
vs. placebo 6 RCTs
N=1251 Prevent CDI: favors lactobacillus
RR 0.27, 95% CI 0.15-0.49
S. boulardii
vs. placebo 6 RCTs
N=1244 Prevent CDI: not significant RR 0.77,
95% CI 0.38-1.54
Multiorganism
probiotics vs.
placebo
5 RCT
N=3960 Prevent CDI: favors multi-organism
RR 0.50, 95%, CI 0.28-0.88
•Preparations vary (pathogen, single vs. multiple)
•Data is mixed (series meta analysis)
•Implications: True effectiveness remains unclear
Candidate for ASP Hempel, et al. JAMA 2012;307:1959-69. Johnston, et al. Ann Intern Med 2012;157:878-88.
Allen, et al. Lancet 2013;382:1249-57. Pozzoni, et al. Am J Gastroenterol 2012;107:922-31.

Intravenous Immunoglobulins (IVIG) • Use 1st described in children with multiple CDI episodes
• Most small case series (1-20 patients)
• Varying:
– Ages (2-81 y/o)
– Dosing (150-400mg/kg, standard 30gm dose)
– Frequency (once- over weeks) and timing
– Outcomes:
• Cure rate 50-100%
• Recurrence 0-100%
• Implications: optimal regimen and when to give in
disease course is not well established Candidate for ASP
Leung, et al. J Pediatr 1991;118:633-7.
Abougergi and Kwon. Dig Dis Sci 2011;56:19-26.
AHRQ. Early Diagnosis, Prevention, and Treatment of Clostridium difficile: Update. 2016

Fecal Microbial Transplant (FMT)
– First reported in 1958 with pseudomembranous colitis
– Mainly case reports (recurrences)
– Meta-analysis 2013- 300 patients- cure rates 85-90%
– RCT Netherlands: Outcome
• Vancomycin regimen, bowel lavage
& donor feces via nasoduodenal tube 13/16 (2/3)
• A standard vancomycin regimen 4/13
• A standard vancomycin regimen &
bowel lavage 3/13
• Implication: Likely effective- importance of microbiome “yuck factor” •Kassam. Fecal microbiota transplantation… Am J. gastro. 2013. 108;500-508.
•vanNood. Duodenal infusion of donor.. NEJM. 2013; 368: 407-415.
•FDA backs down on fecal transplant rule- http://www.medpagetoday.com/Gastroenterology/GeneralGastroenterology/40628

“rePOOPulating”- The “poop pill”
• A variation on stool transplant--processed feces until only
bacteria- encapsulated in 3 layer gelatin capsule
• Initial were smaller case series
– None had recurrences
– Advantages: covers more of GI tract, no invasive
procedure, more comfortable / acceptable (9.6/10)
• Letter Editor- non responders- some standardized regimens
• Recent—Non-inferiority, unblinded, randomized trial
conducted in 3 academic centers, 116 patients- FMT vs.
pills
– Non inferior to prevent CDI recurrence at 12 weeks
–
•Louie, ID Week abstract 89, Oct 3, 2013 and petrof Stool substitute… “repoopulating” the gut. Microbiome. 2013;1:3-9.
•Stollman at al. Am J. gastroenterology. 2015; 110:600-601.
• Kao. JAMA. 2017;318(20):1985-1993. doi:10.1001/jama.2017.17077

Monoclonal Antibodies • Two human monoclonal Ab bind & neutralize C.
difficile toxins: • Actoxumab Toxin A
• Bezlotoxumab Toxin B
• Recent NEJM:
• Randomized control trial, very complex methods
• Lower rates of recurrence among those receiving
Bezlotoxumab w/ standard of care for 1 OR recurrent CDI
– NNT to prevent 1 episode of recurrence= 10
• Actoxumab was not efficacious when given alone & provided
no benefit when given concurrently with Bezlotoxumab
• Implications: Preliminary, more study needed; Candidate
for ASP
•Wilcox MH et al. N Engl J Med 2017;376:305-317

Proton Pump Inhibitors (PPI) and CDI
• Data mixed
• 2 studies & editorial in May 2010: “Less is more”
– Respective cohort: 5 years, 1166 patients
• Recurrent CDI higher PPI (25.2 vs 18.5%)
• Many PPI no indications
– Pharmcoepidemiologic cohort: >100,000 discharges/5 yrs
• Dose relationship
• FDA warning- PPI & CDI
• Implications: Many no indication, associated with VAP, expense, after CDI Dx- stronger case
Linsky, Arch Int Med 2010, Howell, Arch Int Med 2010; Katz, Arch Int Med 2010
FDA Drug Safety Communication. Available at: http://www.fda.gov/Drugs/DrugSafety/ucm290510.htm

Prophylaxis for CDI when on
Systemic Antibiotics? Retrospective Study 203 patient w/ prior CDI & on
antibiotics.
Recurrence:
Oral vancomycin No vancomycin
(125 OR 250 mg po BID)
4.2 % 26.2%
OR 0.12, CI (.04-.4), p < 0.001
Issues: small number & retrospective
Considerations: Promotion of VRE, costs/ cost
effectiveness (practical– target patients/ populations)
•Pallin. CID. 2016: 63 (5): 651-653.

•Combine Best Practices:
• Reassess based on new guidelines
Examples of CDI Policies
•CDI ASP & Treatment Policies

What Impact Could Reduced
Antibiotic Use have on CDI?
• CDC Study:
• Mixed methods, data sources
• In 323 hospitals, >55% patients received
antibiotic
• 37% prescribing could be improved
• Wide variety in prescribing
• Estimated 30% reduction in antibiotic use, could
decease CDI by 26%
CDC. MMWR. Mar 7, 14. 63(09);194-200.

Strategies to Review
Antibiotic Prescribing Before CDI1
• Review common and
high volume antibiotics
• Review antibiotics in
CDI cases
• Systemic approach
• Identify antibiotic prescribing
most associated with CDI
• Tailored ASP interventions
1 ERASE Cdiff Toolkit. AHRQ. 2013. Available at: http://www.ahrq.gov/professionals/quality-patient-safety/patient-safety-resources/resources/cdifftoolkit/index.html#

Review Medications After CDI Diagnosis
• Antibiotics (short/ long term):
– Are they still needed (appropriate)?
– Can they be narrowed or the course shortened?
• Other Drugs:
– Anti-motility agents
– Narcotic
– Laxatives
– Immunosuppression

Layering of ASP Activities Over Time 2008-2018
• Improved CDI testing
• MALDI-TOF + Stewardship intervention for positive blood cultures
• SENTRI-7/Antibiotic surveillance report
• Enhanced auditing
• Extended ID consultation
• Stepwise changes to restrictions
• Default duration of 7 days (approved by P&T)
• Antibiotic prescribing screens
• Antibiotic empiric regimen card
• Sepsis protocol
• Noon conferences & other education
Education Antibiotic Directed
Laboratory
Technology Decision &
Other Support
•35

ASP as Part of the Solution
Patient Status
Normal flora
Disruption of flora
C. difficile colonization
C. difficile colitis
Fulminant colitis
Death from C. difficile
Steps
1. Antibiotic damage
2. CDI healthcare exposure
3. CDI toxin production
4. Toxin hyperproduction
5. Severe sepsis/shock
Adapted from:APIC Guide to Prevention of C. difficile Infection. 2013,
Interventions
ASP
Inf. Control & Cleaning
Clinical
ASP & Lab
Critical care, GI, ID & Surgery

Collaboration—
Working Together in NYS on CDI*
Dates Facilities Collaborators Interventions Outcomes
2008- 20091
35 NYS DOH +GNYHA/ UHF
-IPC & Cleaning Bundles -Education
Mean HO- CDI
2010- 2012,2,3
10 GNYHA/ UHF + AHRQ/ CDC + Montefiore
-CDI directed ASP -Education
CDI Targeted
antibiotics AHRQ CDI
Toolkit 2015- on 80 GNYHA/ UHF
+ NYSCHSP + Montefiore
-ASP Course -ASP survey -CDI Point Prevalence -CDI ASP Posters
Facilities (n) 80 61 53
16
•GYNHA/ UHF=Greater NY Hospital Association/ United Hospital Fund, NYSCHSP= NYS Council Health Systems Pharmacists, HO-CDI= Hospital onset CDI
1) Koll. J. Healthcare Quality. 2013: 36 (3): 35-45.
2) Ostrowsky. ICHE. 2014: suppl 3:S86-95.
3) AHRQ Toolkit Available at: http://www.ahrq.gov/professionals/quality-patient-safety/patient-safety-resources/resources/cdifftoolkit/index.html#
•* Addition NYSDOH collaborative LTCF and CDI
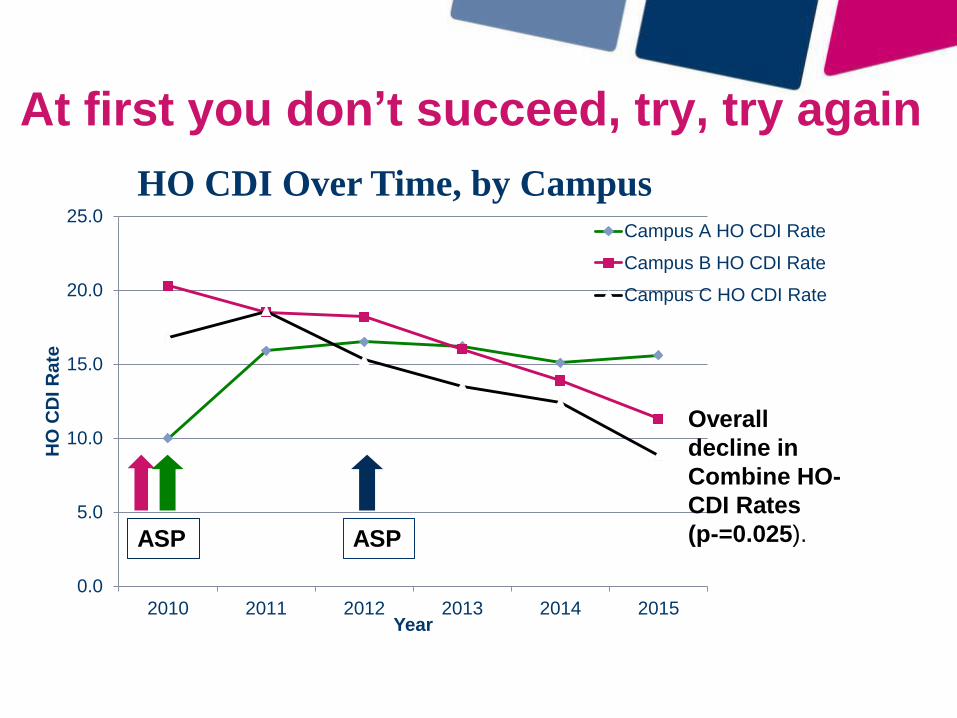
At first you don’t succeed, try, try again
0.0
5.0
10.0
15.0
20.0
25.0
2010 2011 2012 2013 2014 2015
HO
CD
I R
ate
Year
Campus A HO CDI Rate
Campus B HO CDI Rate
Campus C HO CDI Rate
Overall
decline in
Combine HO-
CDI Rates
(p-=0.025). ASP ASP
HO CDI Over Time, by Campus

Conclusions • CDI rates remain high
• New CMS regulatory requirements
• ASP can help:
– Testing
– Formulary
– Treatment for CDI (role for novel agents)
– Antibiotic/medication exposures before & after CDI
• Simple tools can help direct ASP to CDI (show in
workshop)
• It may take time to see results
• ASP interventions complement to other strategies

C. auris (“The other C. diff”)
• Why is this concerning?
– Resistant fungi
– Difficulty in laboratory diagnosis
– Outbreaks in healthcare facilities
• especially relating to environmental contamination
& Infection prevention breaches
– Epi center if NY/ NJ
https://www.cdc.gov/fungal/diseases/candidiasis/candida-auris-qanda.html

What are the C. auris ASP Issues?
• Antifungal review
• Transitions of care- sharing of information:
– Review of antimicrobial regimen
• Intended durations (not restarted on
transfer)
– Status for isolation (related issues)