Bypassing the Blues APSR.pdf · Bypassing the Blues: A Study to Improve the Quality of Life...
43
Bypassing the Blues: A Study to Improve the Quality of Life Following Cardiac Bypass Surgery Bruce L. Rollman, M.D., M.P.H. Associate Professor of Medicine and Psychiatry Charles F. Reynolds, M.D. Professor of Geriatric Psychiatry and Neuroscience Bea Herbeck Belnap, Dr. Biol. Hum. Senior Research Associate University of Pittsburgh School of Medicine All work supported by R01 HL70000
Transcript of Bypassing the Blues APSR.pdf · Bypassing the Blues: A Study to Improve the Quality of Life...

Bypassing the Blues:A Study to Improve the Quality of Life
Following Cardiac Bypass Surgery
Bruce L. Rollman, M.D., M.P.H.Associate Professor of Medicine and Psychiatry
Charles F. Reynolds, M.D.Professor of Geriatric Psychiatry and Neuroscience
Bea Herbeck Belnap, Dr. Biol. Hum.Senior Research Associate
University of Pittsburgh School of Medicine
All work supported by R01 HL70000

Depression
• Affects 16-35% of patients with CVD
• Mortality associated with post-MI depression
greater than any medical predictor of risk
• Seldom diagnosed and treated in cardiac patients
• Failure to recognize is a failure to provide the best
care for our patients
Rumsfeld JS. Circulation 2005; 111:250-253
Will Treatment for Depression Improve
CAD Outcomes?

Montreal Heart Attack Readjustment Trial (M-HART)Frasure-Smith N. Lancet 1997; 350:473
ENRICHDJAMA 2003; 289:3106-16
SADHARTGlassman AH, et al. JAMA 2002; 288:701-709
CREATELesperance F, et al. JAMA 2008; 297:367-379
Prior Treatment Trials

Issues with Prior Trials• Single antidepressant agent
• Inadequate treatment adherence
• Treatment preference(s) not accounted for
• PCP not included as a partner
• Generalizability of screening
• Short follow-up
• Impact of depression treatment on HRQoL,
health services utilization, employment, and
economic outcomes not assessed
• Study power

Wagner Chronic Care Model
www.improvingchroniccare.org

Meta-Analysis of Collaborative Care on 6-Month
Depression Outcomes by Source
Gilbody S. Arch Intern Med 2006;166:2314-2321

To examine if treating post-CABG depression will
improve HRQoL and functional status, decrease
cardiovascular morbidity and health care costs
To study the effect of depression and our
intervention on subgroups defined by age, gender,
race, and co-morbid illness
To identify predictors for post-CABG depression
Bypassing the BluesObjectives

Bypassing the BluesStudy Design

Blinded Assessments
Assessment Instruments:
Month:
0
inpatient
0.5 2 4 8 12 Every 6
Months
Sociodemographic Characteristics
Health-Related Quality of Life
1) MOS SF-36 (MCS/PCS)
2) Duke Activity Status Index (DASI)
Psychiatric Symptoms
1) Patient Health Questionnaire (PHQ)
2) Depression Interview and Structured Hamilton (DISH)
3) PRIME-MD PQ-Anxiety Module/HRS-A
Medical Co-Morbidity/Biologic/Physiologic Variables
1) Medical/Surgical History
2) Biologic/Physiologic measures
3) Cardiovascular morbidity
Recovery Modifiers
1) Perceived Social Support Scale (PSSS)
2) MOS Specific Adherence Scale for Cardiac Patients
3) LOT Optimism
4) WHO Work Survey
5) Insurance status
Health Care Costs
1) Health Care Utilization

8 Pittsburgh-Area
Study Hospitals
Jefferson Regional
Mercy Hospital
UPMC-Passavant
UPMC-Presbyterian
UPMC-Shadyside
VA Medical Center
Westmoreland Regional
West Penn Hospital

Tablet PC


Patient Health Questionnaire
(PHQ-2)
In the past two weeks, have you had:
• Little interest or pleasure doing things?
• Feeling down, depressed, or hopeless?

PHQ-2Major Depression
Sensitivity Specificity
Primary care patientsPast 2 weeks,
≥1 vs. 0
Kroenke K. Med Care 2003; 41:1284
98% 59%
Cardiac patientsPast month,
≥1 vs. 0
McManus D. Am J Cardiol 2005; 9:1076
90% 69%

PHQ-9
Kroenke K. J Gen Intern Med 2001; 16:606-13

PHQ-9Major Depression
Sensitivity Specificity
Primary care patients
Past 2 weeks, ≥10 vs. <10
Kroenke K. J Gen Intern Med 2001;16:606
88% 88%
Cardiac patients
Past 2 weeks, ≥10 vs. <10
McManus D. Am J Cardiol 2005; 9:1076
54% 90%

Screening Summary
Approached Post-CABG 3,058
PHQ-2 Completed 2,486 (81%)
PHQ-2 (+) Screen 1,387 (56%)
Protocol-Elig./Consented 1,268 (91%)
PHQ-9 Completed (2-wk f/u) 1,100 (87%)
PHQ-9≥10 337 (31%)
Randomized 302 (90%)

Screening by Gender
Overall Male Female
PHQ-2 (+) 56% 53% 62%
PHQ-9 ≥10 31% 27% 38%

Baseline SociodemographicsDepressed
N=302Non-DepN=151
P
Age, mean 64 66 .04
Male 59% 63% .38
Caucasian 90% 80% .002
Marital statusSingleMarriedSep/Div/Widowed
7%
68%
25%
7%
69%
24%
.97
Working 38% 42% .45

Clinical Characteristics
DepressedN=302
Non-DepN=151
P
Hypertension 81% 78% .41
Diabetes 42% 38% .38
Smoked, past year 28% 14% .002
Hyperlipidemia 78% 71% .09
MI, prior 43% 42% .84
CHF 19% 18% .73
COPD 20% 9% .003
EF, mean 51% 50% .84

Baseline Mental Health
DepressedN=302
Non-DepN=151
P
PHQ-9 (SD) 13.5 (3.4) 1.9 (1.4) <.001
DISH (SD) 16.2 (7.0) 3.5 (2.8) <.001
SF-36 MCS (SD) 43.1 (11.4) 61.6 (6.1) <.001
SF-36 PCS (SD) 30.3 (6.8) 37.2 (7.5) <.001
Hx of Depression 40% 5% <.001
On SSRI/SNRI 22% 0% <.001

Bypassing the Blues
Implementing the
Chronic Care Model

Wagner Chronic Care Model
www.improvingchroniccare.org

Bypassing the BluesPatient Intervention
• Informed of randomization/control status
• Given brochure on depression and heart disease
• Care manager phones at regular intervals X 8 mo. to:
– Provide basic psychoeducation
– Assess treatment preferences • Coach with self-management workbook
• Promote adherence/adjust pharmacotherapy
• Facilitate MHS referral when appropriate
– Monitor treatment response

Bypassing the BluesPCP Intervention
• Informed of patient’s randomization status
• Provided guidance re: pharmacotherapy
• Can initiate, adjust, or discontinue meds as
indicated
• Provided feedback re: pt.’s symptoms and progress
• Offered assistance referring patient to a MHS
• Informed of patient’s status at end of intervention








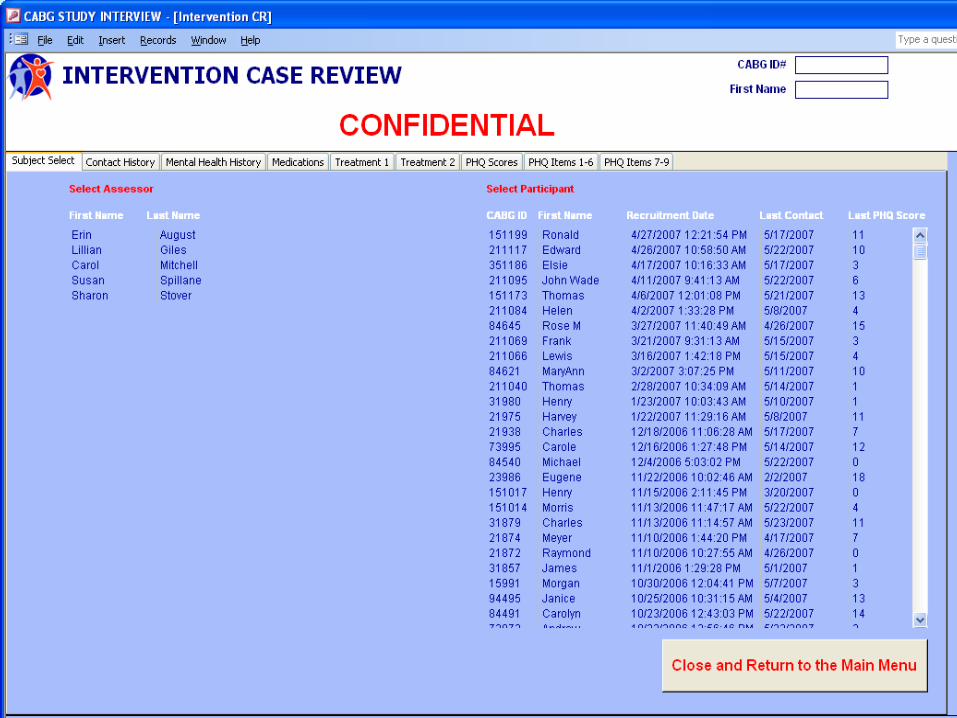
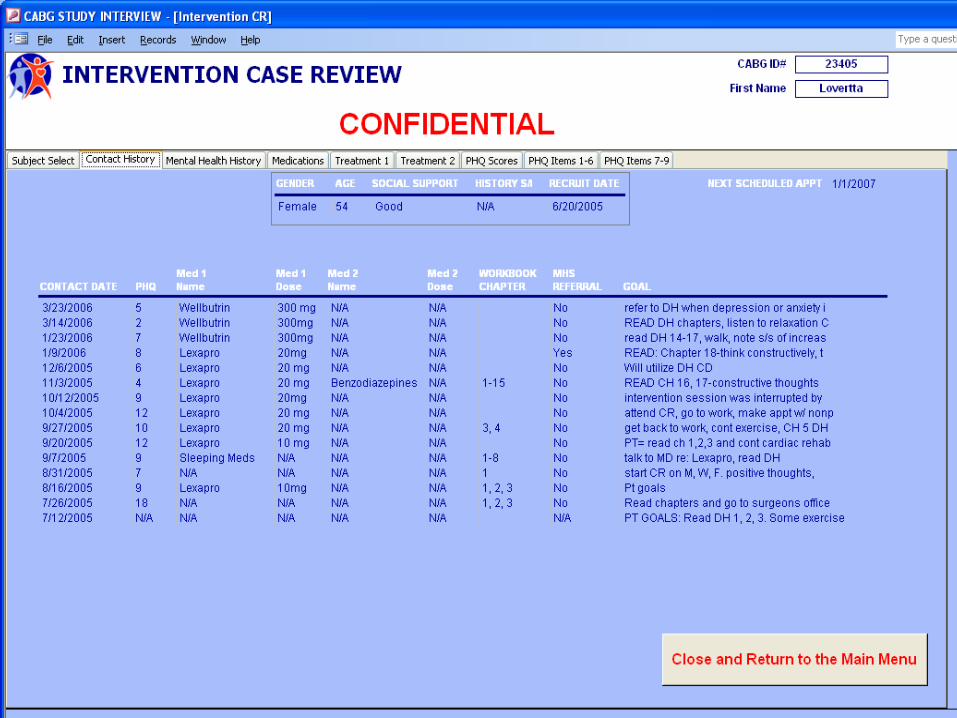
Quality ControlDigital Audiotape Monitoring

Bypassing the Blues
Case Review Registry