BUSINESS PLAN 2014 2017 - hospiceintheweald.org.uk · HOSPICE IN THE BUSINESS PLAN 2014 – 2017...
80
HOSPICE IN THE BUSINESS PLAN 2014 – 2017 Mission: Compassionate, Individualised, Holistic and Supportive care for all patients with a terminal illness, their families and carers.
Transcript of BUSINESS PLAN 2014 2017 - hospiceintheweald.org.uk · HOSPICE IN THE BUSINESS PLAN 2014 – 2017...

HOSPICE IN THE
BUSINESS PLAN
2014 – 2017
Mission: Compassionate, Individualised, Holistic and
Supportive care for all patients with a terminal illness,
their families and carers.

Page | 1
THEME
The theme which describes our approach over the next three years is: Forward Thinking, Focused and Strategic. Forward thinking in making sure we keep doing what we are excellent at - providing compassionate Hospice Palliative Care - but also being more commercial and business-like. Making clear the two things can and do go together. We will also be ambitious and visionary.
Focused on numbers: caring for more and more patients, families and carers and being able to meet more and more unmet need. Focused on numbers of supporters and the funds coming in – sustainability of our community fundraising. Making the case to the NHS in the respect of the money we save them, so they fund us more than in the past.
Strategic in our approach - doing things differently if we need to and in working with partners, known and unknown. Getting closer to real and genuine 24/7 delivery across all our services and joining up palliative care regardless of who delivers it. Having research and evidence-based practice affect our everyday work.

Page | 2
FOREWORD Hospice in the Weald is a local charity firmly rooted in the communities of West Kent and northern East Sussex serving the needs of people with a terminal illness. Irrespective of recent changes in the structures of the NHS and social services, we know there is still a significant gap in care being offered to such people at their time of greatest need.
You will see in this Business Plan our intention to fill this gap. Our Hospice sees about 1100 new referrals each year (2013/14 figures) which is the envy of most hospices. However, we are confident that before the end of 2017, we can be looking after some 1600 referrals annually and be delivering our outstanding Hospice Palliative Care (HPC) to those patients, their families and carers. Obviously we cannot do this alone and need both the partnership of many health and social care professionals and, of course, the continuing fundraising support of the community we serve.
This Business Plan sets out our strategic direction for the next three years and beyond. You will see that we began its formulation in the summer of 2013, six months before the end of our first Business Plan. We published the ‘thrust’ we proposed to take in a ten point plan and sought views from a wide range of stakeholders. After a long consultation process we feel that we have a Business Plan which is ambitious and visionary. It is focused on numbers, seeing more and more patients, families and carers and on raising funds to enable us to expand our services.
We will not compromise on quality. We will maintain our record of spending 90p in every £1 raised on patient care. Hospice in the Weald’s annual running costs are over £6 million and only 16% of that comes from government/NHS. We will continue to make the case for more funding from the NHS but will not let its absence limit us.
The Board of Trustees meet regularly with the CEO and all of the Directors who together make up the Hospice Leadership Team (HLT). We know it is the Hospice workforce, our staff and volunteers, who make our Hospice Palliative Care the world class service it is and that compassionate care can fit harmoniously with a necessary commercial emphasis in these challenging times. The theme that describes our approach is on the previous page and we are confident that, as in the past, we will deliver on the promises in the Business Plan. Hospice in the Weald is doing everything it can to make sure the local community we serve has the Hospice Palliative Care it deserves.
Peter Lewis Rob Woolley Chairman CEO

Page | 3
CONTENTS FOREWORD……………………………………………………………………………………………………………… 2
1. INTRODUCTION & CORE VALUES…………………………………………………………………………….. 5
2. MISSION & STRATEGY……………………………………………………………………………………………… 9
2.1 Mission……………………………………………………………………………………………………………… 9
2.2 Strategy Generally……………………………………………………………………………………………… 10
2.3 Strategic Aims……………………………………………………………………………………………………. 12
3. CONTEXT………………………………………………………………………………………………………………….. 13
4. OVERVIEW OF HOSPICE IN THE WEALD STRUCTURE………………………………………………… 15
5. CLINICAL LEADERSHIP – SHARED MEDICAL AND NURSING DIRECTORATE
OBJECTIVES………………………………………………………………………………………………………………
17
5.1 Increasing Referrals to All Clinical Services…………………………………………………………. 18
5.2 24/7 Working……………………………………………………………………………………………………… 19
5.3 Closer Working with other Partners (Known and Unknown)………………………………. 19
5.4 Maintaining and Improving the Quality of Care Across All Services……………………. 20
6. MEDICAL DIRECTORATE…………………………………………………………………………………………… 21
6.1 Counselling Support Service (CSS) Objectives.……………………………………………………. 23
7. NURSING DIRECTORATE…………………………………………………………………………………………… 25
7.1 Hospice in the Home Objectives.……………………………………………………………………….. 27
7.2 In-Patient Unit (IPU) Objectives.………….……………………………………………………………… 28
7.3 Hospice Day Service (HDS) Objectives..………………………………………………………………. 29
7.4 Lymphoedema Objectives..………………………………………………………………………………… 30
8. COMMERCIAL DIRECTORATE……………………………………………………………………………………. 32
8.1 Retail Objectives………………………………………………………………………………………………… 8.2 we:train Objectives…………………………………………………………………………………………….
33
34
Page | 4
9. FINANCE DIRECTORATE……………………………………………………………………………………………. 36
9.1 Accounts Objectives…………………………………………………………………………………………… 36
9.2 Information & Communication Technology (ICT) Objectives……..…………………….. 38
9.3 Maintenance Department Objectives…………………………………………………………….. 39
10. FUNDRAISING DIRECTORATE…………………………………………………………………………………….
10.1 Fundraising Objectives……………………………………………………………………………………..
42
43
11. PERSONNEL DIRECTORATE………………………………………………………………………………………. 47
11.1 Personnel Objectives…………………………………………………………………………………………
11.2 Support Services – Catering and Housekeeping Objectives……………………………….
49
50
12. BUDGET & FINANCIAL IMPLICATIONS………………………………………………………………………. 52
13. MONITORING & EVALUATION OF THE BUSINESS PLAN……………………………………………. 60
INDEX………………………………………………………………………………………………………………………. 61
APPENDIX A - MANAGEMENT & GOVERNANCE CONTACTS……………………………………… 62
APPENDIX B - GLOSSARY OF TERMS USED………………………………………………………………… 65
APPENDIX C – BIBLIOGRAPHY………………………………………………………………………………….. 68
APPENDIX D – MAPS………………………………………………………………………………………………… 70
APPENDIX E - COMMON MISCONCEPTIONS…………………………………………………………….. 72
APPENDIX F - SWOT & PEST ANALYSES………………………………………………………………………………. 73
APPENDIX G – MAP OF SHOPS…………………………………………………………………………………. 77
APPENDIX H – SYNOPSIS………………………………………………………………………………………….. 78
Page | 5
1. INTRODUCTION & CORE VALUES
This Business Plan is for anyone and everyone that is interested in our work and the community that we serve. Hospice in the Weald is a local charity rooted in the community and is not part of any large national charity or the NHS. As well as being a local charity, we are a complex organisation and in many respects like a business. We will need to become even more business-like in the future. As the external environment and changes within NHS and social care become more commercial, we will need to become more business-like. Our first ever Business Plan (2011-2014)1 set out to tell everyone what we do, how we do it and how we aimed to meet our Strategic Aims. That Business Plan is still available on our website and we have, generally, kept the same format and structure to enable people to follow the journey of our development. As always we use the term ‘Hospice’ to describe and mean the organisation – Hospice in the Weald. People very often misunderstand what ‘Hospice’ means until they are in need of our multifaceted and integrated services. We will continue to inform the community we serve what Hospice in the Weald does. In this Business Plan we have moved our six Core Values to the front of the document. We have set them out on pages 7 and 8 with the definitions of what they mean to us. We defined them over three years ago and have refined the definitions over this period. They are what drive us and the operating principles for our internal conduct and relationship with the external world. As you will see we view them as inextricably linked to each other, like a jigsaw.
Changes in society are going to have a major impact on hospices, our services and our fundraising. The modern hospice movement will need to respond to changes so that we are able to ensure we can still meet the needs of the people in our community diagnosed with a terminal illness. We hope that you see in this Business Plan that at Hospice in the Weald we intend to make changes where they are required. We will measure our progress and seek ways to make that measurement a focus of our work. However, we will not become focused on targets and will ensure that there are no unintended outcomes from a focus on measurement. We have again tried hard to share various drafts of this Business Plan as it has emerged. We tried various ways to gather comments and thoughts from stakeholders. The process of Business Planning does not end so if you are reading this and have something you want to say about it, please don’t hesitate to contact the member of staff you think is most relevant in Appendix B.

Page | 6
Hospice Palliative Care Our definition: Hospice in the Weald defines “Hospice Palliative Care” as: Compassionate, Individualised, Holistic and Supportive care for the whole person which aims to relieve suffering and improve the quality of living and dying. The purpose of Hospice Palliative Care (HPC) is to help patients, families and carers address: physical, psychological, social, spiritual and practical issues, and their associated expectations, needs, hopes and fears. Prepare for and manage the dying process and cope with loss and grief during the illness and bereavement. Our Hospice palliative care is appropriate for any adult patient living with a terminal (progressive life-limiting) illness due to any diagnosis. It may be appropriate at any time from diagnosis and at any time they may have unmet needs and are willing to accept our care. We do not feel that labels and definitions such as specialist or generic palliative care are helpful for patients, families or carers and so the term Hospice Palliative Care is used to encompass the type of care we deliver based on an individual’s needs and wishes.
One major thing we learned from the delivery of our previous Business Plan and when consulting on this one, was that people don’t really understand the nuances and subtlety that exists around the terminology for palliative and/or end of life care. Hospice in the Weald is about the quality of life for terminally ill patients, families and carers as much as it is about the quality of death. We want to reach people earlier than we have in the past so we can avoid the misery of a late referral and that is part of what Hospice Palliative Care (HPC) is about.
You will see throughout this Business Plan small versions of our 2014/17 Business Plan
symbol:
These Business Plan Symbols have been inserted to show a SMARTa objective for a Directorate, Service or Department. The vast majority of Hospice in the Weald’s objectives cross more than one of the Directorates, Services and/or Departments but the 2014/17 Business Plan Symbol is helpful as it shows who is leading on any stated objective.
a The meaning of many acronyms found in this Business Plan (e.g. SMART) can be found in the Glossary of
Terms (Appendix C). There is also a Bibliography pointing to useful external websites (Appendix D).

Page | 7
CORE VALUES

Page | 8

Page | 9
2. MISSION & STRATEGY
2.1 Mission
We set out our Mission in our previous Business Plan, setting it down in words for the first
time. It has not really changed and we don’t think it will significantly change in the near
future but we have replaced “life-limiting illness” with “terminal illness”. We recognise that
most people in the community we serve have an understanding of “terminal illness” but
often, “life-limiting” and “progressive life-limiting” needs explaining. The change does not
alter what we do or how we do it. The Mission in full is:
We sometimes use it in a shortened version but it can be seen in three parts:
i. Hospice in the Weald strives to ensure that the community we serve has access to:
We are about serving which is why we refer to our services: Counselling Support Service,
Hospice Day Service, Hospice in the Home, Lymphoedema and In-Patient Unit.
We are also about community and the community we serve; the people of West Kent and
northern East Sussex are at our core. They give the funds for excellent hospice care to be
provided and in doing so have enabled our growth and development over many years.
When we say we “strive to ensure”, this reflects the reality that we cannot directly provide
Hospice Palliative Care to all the patients in our area we would like to reach. (Please refer to
Appendix E (i) for a map of our catchment area). In any GP practice (see Appendix E (ii)), 1%
of the patient population is in the last year of life2 & b. Within the population of 350,000
which we serve, close to 3,200 could potentially benefit from our services each year. A
major theme of this Business Plan is to see more and more patients in order to meet more
and more unmet need. However, even if a person with a terminal illness is not referred to
Hospice in the Weald we still want them to have access to:
b The NCPC website can provide useful information at http://www.ncpc.org.uk/
Hospice in the Weald strives to ensure that the
community we serve has access to:
Compassionate, Individualised, Holistic and
Supportive Care for all Patients with Terminal
Illness, their Families and Carers.

Page | 10
ii. Compassionate, Individualised, Holistic and Supportive Care
Indeed we think access to this kind of palliative care should be a human right. It is why our
Medical and Nursing Directorates are always determined to be a provider of excellent
palliative care education. We have created a Commercial Directorate to help drive this
forward, sharing our in-house expertise with known and new partners in a cost effective and
sustainable way.
iii. Families and Carers
As set out in our core values supporting patients, families and carers is central to what we
do. Hospice in the Weald will always take a holistic approach and see the whole person and
their circumstances with a special emphasis on families and carers (anyone significant to the
patient as decided by the patient). We also recognise that there are times when differences
of opinion exist between patients, their families and carers and we will explore with them
ways in which to work with discordance.
The table on the following page may aid understanding of our mission and philosophy of
care. Any staff member can also assist in explaining it further. In addition, a list of common
misconceptions about the Hospice can be found in Appendix F.
2.2 Strategy Generally
We set out in our previous Business Plan what we think strategy and strategic thinking is about. Our opinion has not changed and we try very hard to shape the future for people with a terminal illness in our community.
Strategy and strategic thinking is often misunderstood by both those who make strategy
and those that deliver services and/or commission the delivery of services. Often, strategy,
policy and delivery are used interchangeably. We think that strategic thinking is useful in
building a better understanding of plausible futures and, as a result, an organisation should
be in a better position to shape the future as well as react to it. (Please refer to Appendix G
for details of how SWOT & PEST analysis assisted in the formation of our strategic aims).
We have struggled over the last three years to measure the contribution that our many
(over 200) objectives have made to moving forward on our Strategic Aims. We have decided
to reduce the number of Strategic Aims to six (from eight). We are confident these six
Strategic Aims are still valid and we will work harder to measure our success in moving them
forward.

Page | 11
Compassionate, individualised,
holistic & supportive care for
all patients with terminal illness,
their families and carers.
Compassionate
Compassionate care is part of our culture at the Hospice. It includes empathy, active listening and sensitivity and is about valuing patients, their families and carers at a potentially difficult time. It embraces human kindness, dignity
and respect.
Striving to care for patients in the environment they would choose and actively encouraging patient, family and carer involvement in care decisions because social and personal factors can be as important as medical ones for
patients at the end of life.
Talking to people about how they want to live while they are dying.
Holistic
Delivering excellent specialist palliative care.
Our Hospice care is provided in a way that ensures the whole
person and their cirumstances are addressed - their physical, emotional, social and spritiual
needs considered.
Open and honest conversations when required together with pre and post bereavement support
as well as co-ordination of practical help.
Acting in a timely way can help get things right - being proactive
rather than reactive.
Trying to help people live as they would choose until they die. Thinking about how and
where to die.
Supportive
Supportive care can help the patient, their family and carers to cope with a terminal illness from diagnosis, through treatment and continuing illness or death, and into bereavement.
It can help the patient to maximise the benefits of treatment and to live as well as possible with the effects of the
disease.
Availability of support can be a critical part of having as good a death as possible - ensuring the burdens of patients, carers and families are shared.
Going the extra mile.
Designated palliative care at its best.
Individualised
This is about treating everyone as an individual; an
extension of being person-centred. It includes everyone
with different needs and wants.
Accepting and recognising the unique circumstances of each
patient, carer and family - beliefs, community, home, support, relationships and
age.
Assessing and managing pain and other symptoms in a way
that is appropriate to each patient, their family and
carers.
Giving information at the patient's own pace and in a
way that they can easily understand.

Page | 12
2.3 Strategic Aims
Our six Strategic Aims for the period this Business Plan covers are:
One of the key reasons for our change to six Strategic Aims (from eight) is our success in
achieving on our many objectives from the previous Business Plan. A second reason is the
uncertain status of the National End of Life Care Strategy (NEoLC)3. In common with other
hospices we do not know what weight or currency this document has with the NHS,
nationally or locally and we feel there is no choice but to lose our past focus on this.
However, we now have a Clinical Commissioning Group (CCG)4 that has published its own
‘local’ End of Life Care Strategy5 in partnership with Kent County Council (KCC). We will work
hard, as a strategic partner, to make the ambitions in this strategy a reality. We will also
measure how our objectives impact on our six Strategic Aims.
1. To build and nurture our culture of improvement. To use creativity and
innovation continually to improve all aspects of our work and develop
ways to measure and evaluate that improvement.
2. To develop, in partnership with statutory organisations locally, a fully
integrated palliative care service available 24 hours a day and seven days a
week (24/7), to meet more and more unmet need.
3. To work in partnership with others to help influence the community’s attitudes to death and dying to one where conversations are open, honest and perceived in a more positive light.
4. To strive to make the best use of all ICT systems to maximise the benefits
to patients, families and their carers. To explore how we utilise Information and Communication Technology in all we do.
5. To build on our reputation for high quality Training, Education, Learning
and Development in palliative care by delivering this to more and more health and social care staff and partners in a cost-effective and sustainable way.
6. To raise funds to permit the high quality of service and further
development without the risk of interruption due to funding shortfalls from one year to the next. To make best use of all assets.

Page | 13
3. CONTEXT
As we finalise this Business Plan the external environment in which the Hospice operates feels just as uncertain as it did three years ago – but very different. We said in our previous Business Plan it was being developed at “a very uncertain time in respect to the NHS and how it deals with commissioning and delivery of medical care.” This combined with the most uncertain time in respect of the economy and the “age of austerity” meant we worried a great deal about how Hospice in the Weald would continue with its vital work. It feels different because despite still being uncertain, most of what we were worried about did not have a significant impact upon us. The NHS does have a new local shape with the local Clinical Commissioning groups (CCG’s) but the various white papers and restructures have had little effect on patients, families and carers in need of palliative care. We did our best to help implement the national End of Life Care Strategy but the reality is that no government organisation or agency seems to be responsible for taking it forward so we feel that it’s time to end our best endeavours to see it as a reality. The last three years have been successful for Hospice in the Weald. Despite having too many SMART objectives we did deliver the vast majority of them. Perhaps the thing we are not good at is celebrating the many and on-going successes that the Hospice workforce (staff and volunteers) have achieved. We had to work harder than ever before to raise the £6 million it now takes to run Hospice in the Weald each and every year. We saw more patients, families and carers over the last three years than in any period in our 33 year history. However, we are not satisfied or complacent. We will continue to grow, evolve and develop to see more and more people and to meet more and more unmet need. It is clear that Hospice Palliative Care is what patients with a terminal illness need and their families and carers need; and they deserve the care we offer. With Governments having to have a commitment to reducing the UK budget deficit we recognise that public funding will become ever scarcer. We will still make the case for the Hospice getting its fair share - we save the NHS and Social Services a substantial amount of money. However, we see that we must increasingly rely on our own efforts to fund the running costs of all that we do to raise the £6 million a year. We know the community wants our services and as long as they keep giving and we run a cost effective organisation, then we will continue to deliver the Hospice Palliative Care we are renowned for. As we produced the 2011 – 2014 Business Plan, a research report had been produced by DEMOS: Dying for Change6 and we mentioned it in that plan and tried to move forward ideas from it. It suggested “to allow people the deaths they want, end of life care must be radically transformed… “. Change is difficult and transformation ever more so, but Hospice in the Weald has embraced the findings in the research and will continue to do so.

Page | 14
Over the last few years there has been much work by The Commission into the Future of Hospice care7. This commission was established in response to the DEMOS Report and has subsequently captured, published and stored some seventeen reports and working papers.8 The hospice movement understands what the challenges are and in this Business Plan we have anticipated our community’s needs at Hospice in the Weald. The Board of Trustees, Hospice Leadership Team, Managers, Staff and Volunteers are determined to meet the changing and growing needs of the community we serve. We currently, in February 2014, have circa 1100 new palliative care referrals a year. This rate is already seen as excellent by everyone that understands palliative care and has been grown carefully and safely over the last five years or so. However, we are confident that we can make a ‘step change’ and by the end of 2017 we aim to be having circa 1600 new Hospice Palliative Care Referrals. We will do this whilst staying true to our Mission, Core Values and Philosophy of Care. We will not compromise on our high standards or quality. In addition to more partnership working, we will explore mergers with other relevant and appropriate local charities if it helps patients, families and carers and does not compromise who we are and what we do. The West Kent Clinical Commissioning Group (CCG) appears to spend about £2 million a year on palliative care patients9 across their whole geographical area and we spend over £6 million in the 60% of their area we cover. We will work with them as partners to improve access to Hospice Palliative Care and will lead on many aspects of palliative care in our locality. We will strive to ensure other health and social care agencies and organisations see us as a leading provider of palliative care and a driving force for development of local palliative care services. You will gather from this Business Plan that we have a vision where everyone with a terminal illness has access to the care they want and need. You will also see that our ambition is to meet our assessment of that need and raise the funds to provide the resources to do so. We have considered the ‘do nothing option’ and the consequence of this is that significant unmet need would remain; people with a terminal illness in need of compassionate care that would not receive it. We are convinced that we absolutely have to grow the number of people we see and ‘scale up’ our Hospice in the Home Service.

Page | 15
4. OVERVIEW OF HOSPICE IN THE WEALD STRUCTURE
Hospice in the Weald is a local charity which is governed by a Board of Trustees. We currently have 15 Trustees, the majority of whom took up their Trusteeship during the last three years. Our Trustees normally serve one or two terms of three years but we do keep our governance arrangements under constant review. The Board is the body legally responsible for making sure the charity is doing what it was set up to do. They carry out their roles for free and must act responsibly and only in the interests of the charity, use reasonable care and skill and make well-informed decisions. The Trustees delegate the day-to-day management of the organisation to the CEO and Directors. The management structure has changed many times over the Hospice’s 33 year history. In 2010 the Trustees and CEO set out a structure with four Directorates. During 2013 a review of the management structure saw a change to six Directorates: Medical, Nursing, (who share Clinical Leadership), Commercial, Finance, Fundraising and Personnel. Each Directorate is led by a Director and with the CEO they form the Hospice Leadership Team (HLT). The creation of the six Directorate structure has come about from the review but also with a view to ensuring this Business Plan and our ambitious aims and objectives can be delivered as effectively as possible. The total salary cost for the six Directors is less than the total costs of the pre 2010 leadership structure. The Senior Management Team (SMT) that developed and delivered the previous Business Plan have had management time freed up to concentrate on driving change at Service and Departmental level. The SMT did an excellent job in delivering the past objectives and all the managers, staff and volunteers remain the most important asset that the Hospice has. We made clear in our previous Business Plan that no one Directorate is more important than another. Without the Medical and Nursing Directorate there is no Hospice care but we need the Fundraising Directorate to gather in funds to pay doctors and nurses. We will increasingly need to be more commercial and need the Commercial Directorate to support clinical bids made in response to tendering opportunities from Health & Social care commissioners, allowing us to ensure the best value for money.
What we mean by being more commercial and more business-like is making profits from selling goods and services in the open market from the skills, knowledge and abilities we have. We will reinvest any and all profits back into Hospice Palliative Care at Hospice in the Weald, so that when Weald Enterprise (see page 32) profits, the community we serve also profits. We are not intending to be like some commercial businesses aiming to get greater market share or widen the market and we will always ensure all of our Hospice Palliative Care is given completely free of charge and stay true to our core values (see pages 8 and 9). Hospice in the Weald has always been a social enterprise. We realise that the external environment is changing and the NHS and Government at all levels are moving to tenders and bids. We will make bids when we think it can benefit the community we serve. Bids will be made by Hospice in the Weald directly or by our Commercial Directorate under Weald Enterprise Group.

Page | 16
v

Page | 17
5. CLINICAL LEADERSHIP – SHARED MEDICAL AND NURSING DIRECTORATE OBJECTIVES
Traditionally, like other hospices, Hospice in the Weald provides Specialist Palliative Care. By Specialist Palliative Care we mean care provided by multidisciplinary teams who have undergone specific training and/or accreditation in palliative care and work as part of an expert team assessing and advising on symptom control and pain relief. Although these patients have a terminal illness they may not always be in the last year of their life. Specialist Palliative Care practice builds on the care provided by generalist palliative care providers and reflects a higher level of expertise in complex symptom management, spiritual support, psychosocial support, cultural support and bereavement support. Over the past three years we at Hospice in the Weald, whilst wishing to remain true to our Specialist Palliative Care roots, have expanded our services to offer care to patients with generalist palliative care needs. This is often referred to as End of Life Care (EoLC), generic, or designated palliative care and includes the care of those affected by life-limiting or terminal illness who are thought to be in their last year of life. The development of the Hospice in the Home Service delivering Hospice Palliative Care (see definition on page 7) offers an equity of service to all patients with a progressive life limiting illness including enhanced care in their last few weeks or month of life. Since the previous Business Plan was written in 2011, we have achieved the vast majority of the Clinical Leadership objectives set out in that plan. We have adapted to the changing NHS with the establishment of Clinical Commissioning Groups (CCG) as commissioners and have supported West Kent CCG4 in the development of their EoLC strategy3 with both the Medical and the Nursing Directors sitting on the recently formed multi-agency End of Life Care Strategy Implementation Group. The Hospice in the Home (HitH) service has been successfully launched and is now fully embedded as a primary service within the organisation. This Business Plan will focus on reaching a wider patient population at the end of their lives with increased emphasis on patients with non-malignant conditions and the frail elderly population in need of End of Life Care including those with dementia. We recognise that in order to be the leading provider of specialist and generic palliative care for the future, our services need to be available and accessible to patients, families and carers whenever needed. This is driving one of our objectives – to ensure appropriate services are available 24/7 - to be a realistic alternative to acute hospital care for our patient population. One of our major successes over the past three years has been the external training delivered to organisations delivering end of life care across the CCG including the use of end of life care tools such as Advance Care Planning (ACP), Do Not Attempt Cardio-Pulmonary Resuscitation (DNACPR) and Preferred Priorities of Care (PPC). We successfully tendered for the contracts to deliver the ‘Six Steps to Success’ programme10 to care homes and community hospitals as well as delivering our on-going training commitments.

Page | 18
Summer 2012 saw further development of our Electronic Healthcare Record system - Infoflex. This major project took six months and re-designed the structure of the database in order to allow easier identification of key patient information and to provide clinically relevant and accurate statistics. During the course of this Business Plan we hope to see the introduction of an Electronic Palliative Care Co-ordination System (EPaCCS) across the CCG to allow sharing of key patient information between healthcare professionals. Our system will need to be able to interface with this to allow seamless provision of care regardless of setting or time of day for patients at the end of their life. Evidence-based practice has always been at the centre of our clinical care and is embedded in practice via our clinical guidelines and clinical audit programme. We strive to deliver high quality care and now routinely measure ourselves using the National Institute for Heath and Care Excellence (NICE) quality markers for palliative care11. To enhance our evidence-based practice we have increased our activity in research projects locally, nationally and internationally. Over the coming years, we want to build on this and in collaboration with other palliative care providers in Kent and Medway, contribute to the evidence base for palliative care. 5.1 Increasing Referrals to All Clinical Services
Over the next three years we want to expand our existing services to reach more patients in the last year of their life. This will include patients who previously have not been considered to be hospice or specialist palliative care patients. We wish to extend our expertise to help health and social care professionals and hospitals to improve end of life care for all adults in our catchment area.
Over the next three years we will look at ways to increase referrals to all clinical services to ensure we continue to meet the needs of the community we serve and to build on referral numbers so that by end 2017 we have increased referrals to 1600 a year.
Year 1: To review the way in which Hospice in the Weald receives and processes external referrals identifying barriers and bottlenecks.
Year 1: To have in place a way of taking telephone referrals from clinicians.
Years 1 and 2: Market our services to known and unknown referrers emphasising the role Hospice in the Weald plays in supporting patients in the last few weeks of life and those with generic palliative care needs.
Year 1: Increase referrals to 1265 a year (a 15% increase on 2013/14 figures).
Year 2: To explore the feasibility of receiving self-referrals and increase referrals to 1430 a year (a 30% increase on 2013/14 figures).
Year 3: Increase referrals to 1600 a year (a 45% increase on 2013/14 figures).

Page | 19
5.2 24/7 Working
To ensure Hospice in the Weald is available and accessible for patients at all times of day and night offering the correct level of assessment, advice, practical support and services that the patients, family and carers need at that time. By 2016 to be able to offer a genuinely 24/7 service with emergency visits at home and overnight admissions to the In-Patient Unit where needed.
Year 1: To look across the whole Hospice at current working patterns and out-of-hours arrangements, looking at gaps in service provision.
Year 1: To look at examples of working patterns in other hospices and to utilise their experience to develop our own provision.
Year 2: To look into the need for this provision, discussing new ways of working with Out of Hours (OOH) GPs and Accident and Emergency (A&E) to establish the feasibility of changing our practice.
Year 2: To accurately cost out any major changes to rotas to provide full medical and nursing cover 24/7.
Years 2 and 3: To implement any changes towards the end of 2015 to allow for this new way of working to be fully implemented in 2016/17.
5.3 Closer Working with other Partners (Known and Unknown)
As part of increasing our profile in the wider health economy and marketing our services, we need to be more visible and involved in areas where we could actively make a difference to the lives of palliative care patients.
We will identify key individuals within other organisations and look at ways which we can work more closely together to increase referrals.
Maidstone & Tunbridge Wells NHS Trust To look into the possibility of having a more pivotal role in the palliative care service across
the hospital:
Year 1: Have preliminary discussions with the hospital management teams, the clinical staff and the Clinical Commissioning Group (CCG) with regard to how better to integrate palliative care locally across all settings.
Year 1: To write a paper by the end of 2014 exploring the options of closer working with the hospital in order to provide them with robust 24/7 cover and more joined-up care for patients, families and carers.
Years 2 and 3: Depending on the outcome of these discussions and proposals, to move this forward during 2015 and 2016.
Other Partners
Year 1: Identify partners through current contacts that we have not traditionally worked in partnership with.
Years 1 and 2: Identify development opportunities to implement new ways of working with the newly identified partners.

Page | 20
5.4 Maintaining and Improving the Quality of Care Across All Services
To continually evaluate our services and to keep quality and compassionate care at the heart of all that we do. To build on the work already undertaken to measure ourselves against the NICE quality markers for palliative care, ensuring we have an easily accessible, clear and accurate account of the quality as well as the quantity of clinical work that we do in all settings. We will review and improve, through measuring patient outcomes, the effectiveness of our care.
Year 1: Work on outcome measures to produce a ‘dashboard-like’ picture showing quantity and quality of service provision. Have this readily available to staff, volunteers and Trustees by the middle of 2014 with an aim to make it public via the website by end 2014.
Year 1: As well as evaluations of service currently undertaken, take part in the National Bereavement Survey (VOICES)12 audit within 2014 and continue to look for other evidence-based methods of patient, family and carer feedback that we may wish to use.
Year 1: We will actively review the results of current research into patient-reported outcome measuring tools as they emerge and evaluate the benefits of each tool for Hospice in the Weald use.
Year 2: Ensure our electronic health record, Infoflex, is capturing the correct data to measure quality as well as quantity in order to improve our ability to prove the benefits of hospice care.
Year 2: Build on the current audit programme to ensure good quality, robust auditing of clinical practices and guidelines. Aim to have two audits published in poster format at suitable conferences
Year 2: Following the review of measuring tools, we will introduce the most appropriate one and use this throughout our Hospice Palliative Care and link the findings from this into our current Quality Markers.
Year 3: We will utilise the results from the use of this tool to influence further service developments.
Year 3: Aim to have a further three audits published in poster format at suitable conferences.
We will explore the outcomes from the Palliative Care Funding Review (PCFR)13
categorisation of patients to ensure that the definitions are translated and understood by Hospice in the Weald staff. We will embed these categories into our Electronic Health record, Infoflex to ensure we are concentrating our services on the patients with the greatest need of our expertise.
Years 2 and 3: To tie in with the review of Infoflex, we will concentrate on clearly defining the categories emerging from the PCFR and embed this recording into the Infoflex system to help ensure appropriate resources are targeted to the patients with most need.

Page | 21
6. MEDICAL DIRECTORATE The past three years have seen real growth for Hospice in the Weald on the In-Patient Unit, within Hospice in the Home and Hospice Day Service. The medical workforce has needed to expand in order to accommodate this growth and with the addition of a full-time Specialty Doctor to our team we are now able to review patients in all of our services whenever a medical review may be needed. In February 2014 a third consultant was appointed, giving us the ability to offer a truly pro-active and consultant-led service, increasing consultant home visits, out-patient visits and ultrasound provision. This additional resource will also allow us to build on our Evidence Based Practice culture, improving the quantity and quality of our clinical audits and guidelines and allowing us to become more involved in research projects and to really become a research-active Hospice. During the period this Business Plan covers we want to reach more patients in the last year of their lives and the objectives for the Medical Directorate reflect that ambition. We want to be involved earlier in patients’ illnesses especially for those patients with non-malignant disease where palliative care might not have been routinely considered by their healthcare professionals. We want to increase availability to those professionals of advice and support but also to meet these patients and introduce them to our Hospice services and make improvements to their symptom control. The Counselling Support Service intends to expand. In the latter half of 2013 the team underwent a restructure, with the addition of two senior counsellor roles and introducing interns into the team. This improved structure will allow the service to offer support to people who have not traditionally been our clients. This will include bereavement support for relatives of people who have died not under the care of Hospice in the Weald and professional support and supervision for professional carers working in other organisations (such as care homes). With the establishment of the Commercial Directorate, we will have the facility to offer these services for a fee and will be looking into contracts with the CCG and private care facilities in order to offer this as equitably as possible. We will not let this impact on the service we provide, free of charge, to our patients and their families and carers. Chaplaincy forms part of the Medical Directorate and plays a vital role across all services, offering spiritual support to all patients regardless of religious beliefs or affiliations. Over the past few years, our full time chaplain has made huge in-roads into highlighting spiritual care for all patients, families, carers, staff and volunteers, making this a fundamental part of the holistic supportive care we deliver. We have strengthened links with local clergy and are building up a team of pastoral volunteers to help ensure we have 24/7 chaplaincy support for the In-Patient Unit. Over the course of this Business Plan, a labyrinth will be installed in the grounds as an additional resource for spiritual care and our Chaplain will help ensure this is used to its maximum potential by the Hospice and the community.

Page | 22
Medical
Evidence-Based Practice
To embed evidence-based practice in all clinical areas through the increased and improved use of audit projects, clinical guidelines and research participation. Clinical audit To routinely measure and evaluate our practice against established national and local guidance and to find new and innovative ways of disseminating results to staff and other stakeholders.
Year 1: Complete three audits into our clinical practice against established guidelines and agree the number of audits to be carried out in years 2 and 3.
Year 2: Publish the results from two audits at national meetings/conferences.
Year 2: Look at ways of disseminating audit results including use of Intranet and in-house posters.
Clinical Guidelines To ensure our clinical guidelines are up to date with current practice and research. To ensure our guidelines are thoroughly reviewed regularly and incorporate all the relevant evidence. To embed the use of these guidelines in all clinical practice.
Year 1: Carry out a review of all clinical guidelines to prioritise those with less up-to-date references.
Year 2: Look at ways to disseminate clinical guidelines including using the Intranet to ensure all clinical staff are able to find and use them quickly.
Year 1 onwards: Use our audit results to modify and review our guidelines, ensuring their content is relevant and appropriate for Hospice in the Weald.
To increase research participation at Hospice in the Weald To be recognised as a palliative care centre for research purposes and to be actively recruiting patients into portfolio studies by end 2014.
Year 1: Establish relationship with Maidstone and Tunbridge Wells Research and Development department14 so that research studies being undertaken by the Hospice can be supported by the acute trust for research governance purposes.
Year 1: Identify the process that other hospices in the Kent Surrey & Sussex (KSS) region have followed to increase their research activity and write a proposal about resources that would be needed at Hospice in the Weald to facilitate those processes locally.
Year 2: Stimulate research interest across the whole of Hospice in the Weald and identify areas of special interest for staff. Start to collect potential research questions that could later be developed into full proposals.

Page | 23
Years 2 and 3: Work with other palliative care researchers in the KSS region, university colleagues including the Centre for Health Service Studies (CHSS)15 and the Research Design Service to develop a research proposal that would be appropriate to submit when funding sources become available.
Improved access to palliative care for patients with non-malignant diseases
To improve links with the hospital medical teams in order to improve access to palliative care for patients who don’t traditionally receive hospice care such as patients with heart failure or frail, elderly patients with end of life care needs. We aim for our referrals to better reflect the causes of death as indicated by the GP’s GSF register (ie those patients the GP would not be surprised about dying in the next year). In order to achieve this we will encourage more referrals for patients with a non-malignant diagnosis and expect to see an increase of 30% from the 2013/14 figures.
Year 1: Establish closer working practices with the hospital Macmillan team and ensure no duplication of effort.
Year 1: Hospice in the Weald consultants to meet with hospital consultants to look at the feasibility of setting up palliative care clinics within hospitals or joint clinics with different specialists (e.g. respiratory or cardiology).
Year 2: To prioritise those areas with the most perceived need and clinician co-operation and to drive these forward.
Year 3: To look to expand this provision, taking on board previous issues to ensure a 30% increase in referrals.
To establish outreach palliative care clinics in GP surgeries in order to ensure openness to less traditional referrals and hands-on practical support for complicated patients.
Year 1: Improve visibility of consultants within Hospice in the Home for GPs. Increase consultant visits to GP surgeries both ad-hoc and at Gold Standards Framework (GSF) meetings, initially focusing on any surgeries with low or late referral patterns looking to have attended 80% practices by end of the year.
Year 2: Discuss with larger practices the possibility and need for e.g. monthly outreach clinics, focusing especially on surgeries furthest from the Hospice. Look to pilot one or two outreach clinics by the end of the year.
6.1 Counselling Support Service (CSS) Objectives
Bereavement Counselling for more and more people in West Kent
CSS will develop commercial strategies to expand its current service provision to those ineligible for counselling support under the charitable remit:
Year 1: Review the literature and ensure that our offer of intervention is evidence-based in keeping with current research and guidance.

Page | 24
Year 1: Analyse the external environment for market opportunities to innovate and expand current services and evaluate new business options in order to produce a CSS Business Development Strategy in conjunction with the Commercial Director.
Year 1: Source funding to support this expansion, either from statutory sources or individual, private payments.
Year 2: Aim to increase the number of bereavement sessions by 15% from 2013/14 figures.
Year 3: Aim to increase the number of bereavement sessions by 20% from 2013/14 figures. Provide professional carers with psychological support/supervision
The Counselling Support Service (CSS) aims to be the leading provider of professional psychological support (counselling, supervision and debriefing) to staff working in EoLC within our catchment area and will:
Year 1: Identify professional environments that are likely to be interested in the psychological wellbeing of their staff.
Year 1: Design and create promotional literature to advertise and explain the level of service on offer.
Year 1: Aim to have seen 20 professionals under this arrangement.
Year 2: Ensure CSS has appropriate and relevant resources in the form of Counsellors, Rooms, and Clinical Supervisors to accommodate up to 40 professionals in this year.
Year 3: Aim to expand this provision to 60 professionals during this year. Psychological Assessment Skills (PAS) Training (Level 2)
The Counselling Support Service (CSS) will deliver PAS training both internally and externally for practitioners providing Level 2 support (as detailed in the NICE guidance Improving Supportive and Palliative Care for Adults with Cancer).16
Year 1: In conjunction with our Training Centre and the Clinical Management Team (CMT), identify which staff may benefit from PAS training by the end of May 2014, and then at six monthly intervals.
Year 2: Identify external demand for such training, approaching nursing homes, hospitals and other relevant care providers.
Year 3: Aim to provide at least four courses per year, where demand exists. Aim to deliver at a ratio of 60% external: 40% internal delegates, with external delegates being charged a fee (to be agreed with the Commercial Director).

Page | 25
7. NURSING DIRECTORATE As predicted in the last Business Plan, the past three years have seen real growth for Hospice in the Weald, with the increased need to work differently to meet these changes. The Nursing Directorate has been at the centre of these changes in relation to the services it provides. The largest change has been within the Hospice in the Home service where the service has grown from a small pilot to one that covers the entire catchment area. The next three years will see this service further develop to care for patients, their families and carers with palliative care needs. Fully integrating the nurses within this service and the development of the role of Carer Support Co-ordinator will be crucial to building on the success of the previous three years, ensuring that patients, families and carers wishes are at the centre of the high quality service provided. The In-Patient Unit has cared for more people and has begun to adapt and respond to the increasing need for what has traditionally been termed ‘out of hours’ admissions. Some of the rooms are being adapted to enable the Hospice to care for patients with a non-malignant condition and especially those with neurological conditions. Although formal rotational posts for staff working within the Nursing Directorate have not been established, many staff have experienced working within other Hospice services and have incorporated their learning from these areas into their practice. The success of increasing referrals to the Hospice Day Service (formerly the Day Therapy Centre) has led to a total transformation of what is now offered. The service changed its name in 2013 to better reflect what it now offers. The evaluation of the former model provided the opportunity to rethink how this service was offered and to redefine the aim. As a result a more enabling model has emerged led by an Advanced Nurse Practitioner and supported by a multi-professional team including volunteers. The service is now more flexible and individualised with plans and ambitions to take these changes into the community we serve to reach and support more people. The Lymphoedema Service remains the leading provider of Lymphoedema care in this area. The service has been commissioned for some time to provide Lymphoedema care to patients across the West Kent Clinical Commissioning Group (CCG) catchment area and has now been commissioned to take on the responsibility of providing care to parts of the High Weald, Lewes and Havens CCG and Hastings and Rother CCG which are outside of our traditional Hospice area. The creation of a Commercial Directorate late in 2013 will incorporate much of the external work previously delivered by the Education Learning & Development Service. The education and development of our staff remains a high priority as excellent clinical education is core to all we do and without this the provision of high quality services could be hindered. The Nursing Directorate will play its part to ensure the high standards of care that the Hospice is accustomed to delivering are maintained. We will build on the success of the external clinical education learning and development programmes commissioned and delivered over the last three years to ensure that all health and social care staff caring for patients at the end of their lives have access to high quality, appropriate and where required, tailor-made training opportunities.

Page | 26
Following the review of the physical therapies provided at Hospice in the Weald, the role of Lead Therapist was established. This role is currently looking at the therapies provided (Physiotherapy and Occupational Therapy) to ensure that the required level of support is available to care for patients in their preferred place of choice, which is predominantly their Usual Place of Residence (UPR). This includes the creation and development of Therapy Assistant positions and Therapy volunteer roles. We recognised in the previous Business Plan that we would need to adapt to a different model of care and explored as one of these ways the creation of a Federation Model as described in the DEMOS report. Although there was initial interest in the theory behind the model, the creation of the CCGs and the Palliative Care Funding review13 meant that the focus moved elsewhere. The focus from the CCG has now changed and we believe it is appropriate and timely to revisit the model. The next three years will prove challenging and exciting as we take the need for growth and development to the next level, reaching and supporting more people than ever with a terminal diagnosis. The Nursing Directorate will be evaluating progress and responding to the need to ensure that all identified barriers will be removed or minimised. We will be working closely with existing and new partners to ensure the maximum number of people benefit from our hospice philosophy of care. It is recognised that the areas that will experience the largest growth are caring for frail and elderly patients at the end of their lives and those with a dementia diagnosis and we are developing our service to be able to respond to these areas of growth. We will therefore:
Introduce a Clinical Nurse Specialist role with the responsibility of taking the lead for the development of Dementia care offered by the Hospice
We will continue to strive to be a provider of excellent palliative care education, utilising the in-house expertise we already have and complementing this with external experts where appropriate. As this cuts across all Clinical Directorates, but predominantly nursing, the objectives for the next three years will be “owned” by the Nursing Directorate in close working with the Commercial Directorate.
To make Hospice in the Weald Education & Development and we:train (see page 33 for information about we:train) the provider of choice in the local area for specialist training
Year 1: We will identify on-going funding opportunities from commissioners of EoLC training through existing and new contacts also increasing by 10% the amount of bespoke packages delivered externally to care homes, nursing homes and social care agencies by the start of year 2.

Page | 27
Develop EoLC master classes with external partners, for example Alzheimer’s Society, universities and colleges.
We will have identified funding opportunities to deliver a minimum of two masterclasses in Palliative Care in year 1, three in year 2 and four in year 3 with the aim of having a minimum of 35 participants at each event. The masterclasses will be run in conjunction/partnership with external partners, for example specialist charities, universities and national charities. Over the next three years, the Nursing Directorate will continue to strive to deliver high-quality, compassionate, individualised, holistic and supportive care. Each Service has operational objectives that they wish to achieve to support this and are listed below in their individual sections. As a whole we will be working across the Services to achieve the following more strategic objectives:
We will work to ensure that we fully understand the users of our services (patients, families and carers), their needs and wishes and will ensure they are engaged in service development.
Year 1: We will redefine what HitW understands by the terms “service user” and “user involvement” and set out a plan of our approach for working in partnership with them.
Year 2: We will establish a robust system to ensure we fully capture their views and embed these in service design proposals.
Year 3: We will ensure that service users are embedded as co-designers of our service developments and that systems and structures exist to perpetuate this co-design approach.
We will review how patients who are no longer or not in need of continued In-
Patient Hospice Palliative Care are cared for through Continuing Health Care17 funding and who are currently being admitted/transferred to nursing homes.
Years 2 and 3: We will undertake a full and detailed exploration of options available to patients in this group. This will include a feasibility study, including costings, of the options for Hospice in the Weald and we will then progress the approved option. 7.1 Hospice in the Home Objectives
To offer care to more and more patients in our catchment area with Hospice Palliative Care needs
Year 1: We will have reviewed the referral pathway with the aim of minimising barriers to referrals. These options will also include direct referrals from patients and healthcare professionals and will build on the success of the step change programme implemented in 2013/14. We will aim to increase the number of referrals to the service, including patients for End of Life Care by 15% to 1265 referrals a year.
We will introduce a new role at Associate Clinical Nurse Specialist level to work in partnership with the Care Homes (Nursing and Residential) to ensure all of their End of Life Care patients have access to Hospice Palliative Care.
Page | 28
We will revisit, in conjunction with the Commercial Directorate, the concept of creating a Federated Model of Care.
Year 2: We will have increased the number of referrals to the service by 30% to 1430 a year.
Year 3: We will have increased the referrals by 45% to 1600 a year. To deliver care that is responsive to and meets the patient’s needs regardless of
location and time of day
Year 1: We will fundamentally review the way the service is delivered with an emphasis on matching patient’s needs to staff and volunteer skill. We will work closely with the Enhanced Rapid Response Service18 pilot study commissioned by the CCG and Kent Community Healthcare Trust and voluntary agencies to reduce any overlaps in service provision and to ensure gaps in service do not exist.
Year 2: We will build on success and plan how Hospice in the Home can achieve the delivery of 24/7 assessments and delivery of care. We will present an option appraisal for consideration to the Board of Trustees and plan the implementation of the agreed option.
Year 3: We will continue to implement the decisions from the option appraisal and evaluate its effectiveness. To enable those caring for patients with a terminal illness under our care to continue
with their normal role while caring for their relative or friend
Year 1: To undertake a review of the support provided for carers at Hospice in the Weald and to identify three areas in which to establish and pilot satellite support clinics. To utilise this information and feed into the review of respite services which will include a review in relation to the ways in which volunteers are utilised to provide respite in patients’ homes.
Year 2: Following a review of the pilot, work with other partners, including the Commercial Directorate, to establish three further satellite support clinics. To work with partner organisations to pilot carer information and education sessions for all carers.
Year 3: Following this, roll-out these sessions across the catchment area and work with the Commercial Directorate to open them to all carers (not just carers of Hospice in the Weald patients) and to increase the satellite support clinics across the catchment area.
7.2 In-Patient Unit (IPU) Objectives
To make better use of the beds on the In-Patient Unit and ensure the facilities are fit for the future needs of our population
Year 1: From April 2014, change the use of the Ashdown Room (currently used as a three- bed day procedure area) to provide a room that can accommodate more comfortably the needs of patients requiring a larger space due to either physical needs (e.g. large electric wheelchairs) or for spiritual needs (e.g. patients wishing to have their families around them). We will monitor the use of this room during the first six months, gaining feedback
Page | 29
from patients and their carers to ensure the correct multifunctional equipment is purchased and used.
Year 1: To relocate the clinical procedures area to a smaller space with two beds in response to the change in the delivery of certain day procedure treatments.
Year 1: We will review all patient rooms ensuring they are all equipped with up to date and appropriate pressure relieving mattresses and seating making them suitable for both patients’ complex needs and relatives staying with patients.
Year 1: We will appropriately equip and change the use of the Tonbridge Room (currently used as a meeting room) to allow an appropriate space for the exercise and rehabilitative needs of Hospice in the Weald patients; preparing patients for home and offering sessions for all hospice patients to assist with improving their quality of life.
Year 1: We will fundamentally review the need and use of the bookable respite bed. We will consult with referrers and patients to evaluate the need and availability of the bed and present the results to the Hospice Leadership Team and Clinical Governance Committee for agreement.
Year 2: We will undertake a review of the current ceiling hoist system with a view to replacing them with more up to date and comfortable/flexible systems.
Closer working with other agencies to ensure we meet the needs of the changing
patient population.
Year 1: To look at examples of working patterns in other Hospices and to utilise their experience to develop our own provision where appropriate.
Years 2 and 3: To implement any changes including job shadowing with other organisations, statutory and voluntary, to enhance the care we offer. This new way of working to be fully implemented in 2016/17.
7.3 Hospice Day Service (HDS) Objectives Increase the attendance from the current 20 patients a day to 30 patients a day
Promote the new model of care both externally and within the Hospice Day Service, increasing the number of patients attending on a weekly and sessional basis. More focus on patient goals and increase carer support and flexibility in the service.
Year 1: Helping patients live well. All HDS patients should have agreed goals to achieve during their attendance.
Year 2: Have structured group programmes developed and running which patients can attend either as part of the Hospice Day Service day or on a bookable basis. These programmes will include Condition Management Techniques, Health Education/ Community Based Resources, Mobility and Activities of Daily Living.
Year 1: Have carried out a marketing campaign to encourage an increase of direct referrals to HDS by 10%.
Year 1: Have two “drop in sessions” per week running for patients and carers to attend on an ad-hoc basis.

Page | 30
To help facilitate the increase in HDS attendances, during the first half of Year 1, carry out a comprehensive review of transport options for patients attending for the traditional day and also those attending for short sessions or the drop-in service.
Year 1: carry out a review of Complementary Therapies provided by Hospice in the Weald including the structure and management of Therapy Volunteers. Depending upon the review outcome, in Year 2, facilitate changes required to provide as full as possible a service to potentially include therapy volunteers working at our outreach sessions and in collaboration with Hospice in the Home for End of Life Care patients at home.
Look at how the Hospice Day Service (HDS) can feed into the review of respite across the hospice
Look at the feasibility of using HDS as emergency/crisis daily respite for patients until a more suitable permanent solution can be found.
During the first six months of Year 1: work with other Hospice in the Weald clinical services to review and evaluate respite/crisis care with a view to HDS becoming a flexible service to offer daily attendance over a short period to support carer/patient needs.
Year 1: offer a flexible daily attendance for patients who need emergency support (this may be as a result of carer breakdown, social or psychological distress, or symptom control). Develop working relationships with external providers to meet the longer term care needs of these patients.
Outreach Hospice Day Service (HDS)
Explore the feasibility of working with new partners to hold HDS outside of the hospice building. If this looks successful then set up a pilot and review before considering rolling-out across catchment area.
Year 2: Work with the HitH pilot supporting carers; conduct and complete a feasibility study on patient/carer need and the logistics of developing and running an additional HDS as a satellite service in a rural setting.
Year 2: Depending on the results of the feasibility study set up a six month pilot satellite HDS for one day a week.
Year 3: Evaluate the HDS satellite pilot and if successful roll out across catchment area. 7.4 Lymphoedema Objectives
To review the payments received for patients with lymphoedema without specialist palliative care needs.
Year 1: Renew and renegotiate existing contracts in 2014/15 for High Weald, Lewes and Havens CCG, Hastings and Rother CCG and Dartford, Gravesham and Swanley CCG to include the additional administration time these contracts take to fulfil.
Year 2: Negotiate contracts for (non-specialist palliative care) Sussex patients in Hospice catchment areas.

Page | 31
Year 3: Explore the use of an option appraisal for patients to access the service through self-funding or private health insurance funding. This paper will be presented initially to the Clinical Management Team for discussion and then the Hospice Leadership Team and the Board.
To reduce expenditure on lymphoedema consumables
Aim to reduce spending on garments and bandages by 30% per patient (average) by 2017 from a baseline taken from the average monthly spend in 2013 by ensuring the selection of best value for money items and increasing the amount of garments prescribed by the GP using the FP10 system.
Year 1: Reduce hosiery budget by 10% per patient based on 2013 expenditure.
Year 2: Reduce hosiery budget by a further 10% per patient based on 2013 expenditure.
Year 3: Reduce hosiery budget by a further 10% per patient based on 2013 expenditure.
To ensure we continue to offer high quality care
Years 1 and 2: Develop a patient satisfaction survey in Year 1 and administer the same in year 1 and 2.
Year 3: Publish the results and any planned improvements on the website. Identify standards in areas which indicate high quality care and produce tools to measure these on a regular basis; for example audits to look at communication to GP following appointments, the use of intensive treatments, appointment choice offered to patients and the reduction of acute admissions due to cellulitis. Discuss these audits with the Hospice Audit and Research Group and Clinical Governance Committee.

Page | 32
8. COMMERCIAL DIRECTORATE
In 2013 as part of an on-going review of the Hospice’s organisational structure the Commercial Directorate was created. The Commercial Directorate incorporates all trading activities, including Retail, as well as the Training Centre and the co-ordination of bids to the public sector. Our previous business plan talked about “great opportunity” within our charity shops and we are confident that after three years of focus and direction our retail operations are on track to be a consistent source of income that can be relied upon to deliver £1 million towards the Hospice in the Weald running costs each year - the systems and processes are in place, embedded and robust. After a strong year of 21% growth in financial year 2011-12 and facing inclement market conditions in 2012-13, a management decision was made to invest resources in market development, encouraging existing customers to spend more and targeting new customers. The Retail department was brought out of the Fundraising directorate, with the Head of Retail reporting directly to the CEO in developing a comprehensive programme for growth and development. As a result of that programme we have rebranded over 75% of our shops to better reflect our organisational aims, opened five new shops (see Appendix H), and developed an online sales programme. Implementation of the Smart Till system (an electronic point of sale (EPoS) system developed specifically for the charity retail market), has led to a greater than 200% increase in the value of retail Gift Aid. Additionally, a warehouse-based system of working enabled our shops to respond in the best possible way to customer demand. A separate three year ‘Retail Business Plan’19 is available to view and download via our website and contains further information regarding the proposed plans and development of retail operations. Over the course of the 2014 – 2017 Business Plan the Commercial Director will work in a coaching capacity with managers who are dealing with ‘commercial issues’, finding a balance to minimise management time wasted and maximise income, as well as developing strategies to ‘see and take’ commercial opportunities in all guises as they arise. To involve all staff and volunteers across the whole organisation in seeking, recognising and taking such commercial opportunities. Commercial opportunities will be taken through the Hospice in the Weald Trading Company trading as Weald Enterprise Group, from this the abbreviated acronym ‘we’ will be used as a prefix to create a brand for each opportunity. During the financial year 2014-15 Weald Enterprise will operate under a one year operational plan, developed by March 2014. When the current Retail Business Plan ends in 2015 it will be superseded by a three-year Commercial Business Plan written and signed off by March 2015. Under we:train, we will refocus the previous Education, Learning & Development service to become, among other things, a training enterprise with a structure and culture that is outward-looking and commercial in focus. We will develop high quality training packages

Page | 33
which meet the needs of the local market. Working closely alongside colleagues in both the Nursing and Medical Directorates we will contribute to making Hospice in the Weald Education & Development and we:train the provider of choice in the local area for specialist training. The Commercial Directorate will also work closely on business development within the Counselling Support Service to explore commercial opportunities. Our shops will continue to operate under the Hospice in the Weald brand and focus on realising the maximum potential from each donation. Sustainable physical expansion alongside cultivation of new business in existing shops will form the backbone of a strategy for market development. 8.1 Retail Objectives
Busy and exciting shops full of bargains & treasures
We will sell more to more people; consistently reviewing and evaluating how we advertise and promote our shops to target new customers. We will cultivate repeat spend and donation and ensure both customers and donators in Hospice in the Weald shops are aware of their contribution to the charity. The shop Loyalty Card scheme will be a priority with a target of 10,000 new members per year and an annually set income budget.
Engage customers through e-newsletter.
Formalise house styles for shop literature.
Develop a plan to advertise and promote our shops to target new customers.
Redesign the loyalty card and develop a plan for securing 10,000 unique sign-ups a year.
Develop ways of using Loyalty card data to cultivate repeat spend and donation with an annually set income.
Have a system for integrating our shops’ customer database with Donorflex by August 2014, with a subsequent weekly/monthly transfer.
Provide data to facilitate partnership marketing through colleagues in Corporate Fundraising.
Explore messaging mediums that increase the awareness of the value to the charity of shopping and donating to Hospice in the Weald shops.
Report regularly on measurable data (for example average basket values, units per transaction, event attendance).
Making the most of every donation
Commitment to ensuring we make the most of each donation will see development of online and multi-channel sales. We will sell through a greater number of online ‘marketplaces’ as well as further developing our own website. Greater, and more varied items will be sold online with costs kept to no greater than 35% of sales.
Set and agree measures to ensure consistent newness on the shop floor. Monitor monthly.
Carry out a root and branch operations and logistics review.

Page | 34
Identify 3 (1 a year) additional online marketplaces to expand current multichannel sales progress.
Develop channels for sale of unsalable items to reduce reliance on current methods. Achieve 100K income from this by year 3.
Preparing for the future
Physical expansion will continue, in a way that is appropriate to the external Political, Economic, Social and Technological (P.E.S.T.) environment. We will research and develop a plan to develop a ‘multi-function’ site which will integrate our shops with Hospice services. A plan will be produced by the end of the first year.
Produce a PEST analysis focussed on potential physical expansion.
Based on the findings of the PEST analysis develop a 3 year business plan for physical expansion including a minimum of 2 sites in year 1.
Research and develop a plan for a “multi-function” site.
Consider areas outside of our fundraising area. 8.2 we:train Objectives
Readers of this Business Plan need to understand that we:train is our new approach to deliver training to Health and Social care workers and others. Hospice in the Weald has always delivered some training to people from other organisations but has done this without charging those attending and so has borne the costs itself. Our new commercial approach will seek to cover costs and if possible make a small profit to support the Hospice in the delivery of its core purpose. Any and all profits will go to the Hospice. Successful business ventures require a well-defined market and a robust understanding of customer needs and wants. We will use established business analysis tools PEST and SWOT (Strengths, Weaknesses, Opportunities, Threats) to identify opportunities within the market and take a 4Cs approach to developing our business.
Understand our market and its potential
Undertake PEST, SWOT and stakeholder analyses for we:train opportunities.
Identify potential customers by building a market map.
Use a stakeholder analysis to identify customer needs and wants.
Use 4Cs model to develop a marketing mix which meets needs and wants identified above.
Explore formal training provider accreditation status which has currency with identified customers and have this in place by March 2015.
Carry out a competitor analysis on the basis of identified market and accreditation status. The 4Cs (Customer value, Cost, Communication, Convenience) updates the traditional 4Ps (Price, Product, Place, Promotion) analysis of the marketing mix, placing focus firmly on the customers perspective.

Page | 35
To make Hospice in the Weald Education & Development and we:train the provider of choice in the local area for specialist and other training.
Identify on-going funding opportunities from commissioners of training and strive to ensure that we make bids for all West Kent and East Sussex tenders/specifications that relate directly to End of Life Care and our services. We will also identify and make bids for relevant tenders/specifications which fall outside what traditionally have been considered our services and operations. As part of seeking to be the provider of choice we will work closely with external organisations, helping to build their capacity where it is appropriate. We will ensure that our bids offer commissioners comprehensive value for money while remaining evidence-based and delivering maximum impact.
Deliver relevant and contemporary training that inspires the modern professional.
To maintain and build upon our reputation as a leading healthcare training provider by expanding our portfolio of training interventions to cover a broader spectrum of subjects across a much wider external audience with the aim of increasing our audience reach by 50%. We will utilise internal skills and services to design, pilot; market and deliver subjects that are uniquely situated in the market place and have been assessed as having a real training need within our customer reach. Where appropriate, we will work in partnership with other healthcare/training providers to ensure needs are identified and addressed within the appropriate time frame to best meet the needs of the subject.
To create a suite of 5 distinctive and dynamic management training courses by Jan 2015 that interlink with each other to improve management skills to any organisation and to support continued professional development, across any sector.
To be creating training packages collaboratively with at least 5 new partners by April 2016.
Run regular continuing professional development sessions to keep up-to-date with contemporary practices and theory.
Deliver relevant, modern training interventions that inspire the modern professional.
Plan for and receive formal training provider accreditation status by March 2015.
Page | 36
9. FINANCE DIRECTORATE In January 2013, as part of an on-going review of the Hospice’s organisational structure, the Finance Directorate was created. The new Directorate manages the Information Communication Technology (ICT), Accounts and Maintenance functions. The Personnel Directorate also came into being to manage the Personnel, Catering and Housekeeping functions rendering the old Operations Directorate redundant. The new structure has enabled the Finance Directorate to concentrate on supporting services and departments in accomplishing their own objectives along with fulfilling the day to day functions of their own departments, with the aim of facilitating the efficient and effective running of the Hospice. During the period covered by this Business Plan this will be further embedded and core areas of work driven forward. The core areas covered in regard to the Business Plan are:
Technical advances in ICT.
Ensuring the reliability of all ICT systems.
Making the best use of Hospice buildings including Retail outlets.
Providing efficient and effective reactive helpdesks for both ICT & Maintenance.
Making value for money decisions regarding asset replacement / refurbishment.
Using budgets wisely and taking ownership of this with managers at all levels.
Providing up to date management information on a timely basis.
Providing support for grant and bid applications.
Making the Hospice environmentally friendly and as ‘green’ as possible.
Developing and implementing procurement controls and authorisation levels. The following objectives have been developed to enhance the support given by the Finance Directorate together with improving the day to day processing systems in each department.
9.1 Accounts Objectives
Procurement System
Tabs Facilities Management (Tabs FM) software currently provides a Hospice room booking system and ICT & Maintenance helpdesks. The software also contains a procurement/ordering module which will be developed to provide an effective and efficient procurement system providing appropriate controls and authorisation levels to meet the Hospice procurement policy requirements. It will include the following features:
Quick editing and authorisation of orders.
Detailed search functions for orders and invoices.
Easy checking and authorisation of invoices.
Analysis of spend against budget per cost code.

Page | 37
Feedback on ease of use and information available. Year 1:
We will prepare electronic training sheets and work flow charts for use with Tabs FM in regard to monitoring actual spend against budgets by cost code, obtain feedback from order authorisers on these work flows, analyse feedback and adjust work flows taking into consideration all feedback obtained and develop a paperless electronic invoice authorisation system to be trialled across both the Charity and Retail companies.
Year 2:
Using the above, develop a paperless electronic payment system using Tabs FM and Lloydslink BACS payment systems.
Review of Banking Needs
We currently have three banking suppliers, Lloyds, Barclays and Santander. A review of our banking needs is overdue and will take place during the lifespan of this Business Plan.
Due to the expansion in Retail outlets, there has been a large increase in the number of banking transactions through Barclays and Santander and an electronic paperless system has been developed to process these. To be able to streamline bank transaction processing further, a plan is to be developed to explore our current banking needs for both Hospice in the Weald and Hospice in the Weald (Trading) Ltd (the new Commercial Directorate in the organisation structure). A decision will be made as to whether changing our banking suppliers will be beneficial, and if the findings are positive a review of the market will be undertaken.
Year 2:
We will review both Hospice and Retail banking needs and prepare a detailed requirements list to take to the ‘market’ and identify the most suitable bank based on the banking facilities provided and the Value for Money (VFM) ethos.
Year 3:
We will source one bank to fulfil all our banking needs, obtain feedback from a current customer and analyse findings. We will prepare a detailed implementation plan and move all eight bank accounts to the new provider.
Provide support to all Hospice Services in regards to making bids to endeavour to increase our current Government funding of £1m to £2m. The NHS Primary Care Trusts (PCT’s) were disbanded in 2012 and Clinical Commissioning Groups (CCG’s) created in their place. Our traditional method of Government core funding via Grants in Aid20 is now under threat as CCG’s move to commissioning the services they provide from external suppliers at an agreed sum. To mitigate the risk of losing this £1m all the Hospice Services will need to become proactive in identifying and bidding for all the relevant contracts that become available.

Page | 38
The Accounts department is to act as the support for bid makers and ‘contract managers’, providing and checking figures for consistency and accuracy, to ensure that opportunities for funding are made in a timely and appropriate manner.
Year 1:
We will be the central point for ensuring consistency across all bids, checking all figures and calculations within bids. Prepare a detailed list of staff costs per hour for delivering training and be available to answer any and all questions regarding commissioning and making bids and managing contracts. We will provide training on the preparation of bids.
9.2 Information & Communication Technology (ICT) Department Objectives The Business Plan objectives for ICT supplement those in the three-year ICT Strategy published in the last quarter of 2012. Many have been implemented in the last 15 months. The remaining ones include the virtualisation of the servers (partitioning a physical server into smaller virtual servers to help maximise resources), which is being delivered as part of a new contract with KMHIS (Kent and Medway Health Informatics Services) to manage the Hospice servers off-site. This contract necessitates an upgrade of the link to the internet to optical fibre and supports the needs for mobile working as described below.
Mobile Working.
The plan is to enable staff and volunteers to work flexibly, both within the Hospice building and externally. This will allow staff to be more efficient in the use of salaried time, by reducing time spent travelling to and from the Hospice. It will enable doctors and other clinicians to update records whilst with patients instead of having to enter data back in the office, and for patients to be included in describing their view of symptoms. It will also allow staff and volunteers to work flexibly both off-site and on-site e.g. by hot-desking, enabling them to take their bespoke desktops to wherever they need to work and making the best use of office space within Hospice premises. This will be achieved by equipping staff and volunteers with mobile devices (laptops, tablets, notepads etc.), augmented by workstations within each Service/Department with monitors, telephones and access to the network. Implementation will take place as follows: Year 1:
We will conduct a trial in Hospice in the Home to ensure access to the required applications, prove security, identify the correct type of mobile devices, and confirm the speed of access to the core systems from local and remote sites via Wi-Fi and 3G. Costs for rolling out to all departments and services will be estimated for the 2014/15 budget. This paper will be presented to HLT outlining the plan to implement mobile working across the Hospice.
Integrated Hospice Databases
The current ICT strategy includes the plan to re-assess the patient database (Infoflex) to see if it is the right long term solution. This will be reviewed in the light of the changing organisation of the NHS. There are also a number of areas where the existing databases and

Page | 39
application systems used in the Hospice need to be reviewed and future requirements assessed, for example:
The direction of CCG systems.
Improved systems integration.
Removing duplicate data. Developments in technology and the needs of the Hospice will be brought together to look at what is available in the market and what is being developed for the near future. Year 2:
We will review Donorflex to include Corporate Relationship Management (CRM) requirements and ability to link to other Hospice systems. Electronic mailshots and lottery modules will be included in the review.
Year 3:
We will review Infoflex to include the potential decision of the CCG on the system to be used in this area. Patient Direct
The intention is to look at technologies and methods for communicating with patients directly, rather than using telephone and face-to-face meetings only. This approach will build on the technologies used to support mobile working as mentioned in the section above, and potentially could save money and improve patient access. Year 1:
We will assess the market in terms of mobile devices and software, and look at patient acceptance of/ability to use tablet devices for instance, to communicate directly with carers and support staff at the Hospice.
Year 2:
We will roll out technologies to provide a ‘Patient Direct’ service where appropriate if the review of year 1 is feasible and acceptable.
9.3 Maintenance Department Objectives
As a co-location and best use of space project (COLBUS) was completed in 2013 and the labyrinth construction and car park refurbishments will be completed early in 2014, the shift for maintenance is to provide both reactive and proactive support to all services and departments in an efficient and effective manner. Tabs FM software, currently being used for the reactive maintenance is to be developed to be an asset register, covering the Hospice building and all Retail shops. All areas of ‘Going Green’ (see 9.3 – 3) are to be assessed and where feasible implemented to make the Hospice as environmentally friendly as possible.

Page | 40
Enabling proactivity
To enable proactivity, the asset register will be created using Tabs FM. The need for long term budgeting has also been identified for large scale equipment replacement and refurbishment using VFM. Tabs FM is to be developed to provide effective monitoring of repairs and maintenance throughout all the Hospice premises to enable as accurate budgeting as possible.
Year 1:
We will identify all material maintenance assets and asset tag (barcode) them for input onto Tabs FM.
Year 2:
We will develop and implement a schedule for Planned Preventative Maintenance (PPM) using Personal Digital Assistants (PDA) to allocate tasks efficiently and effectively and create a reporting system using Tabs FM to produce costings for the repairs and maintenance of those assets held on the register. We will prepare an analysis of costs using the Tabs FM reporting system to produce accurate long term budgets for equipment replacement / refurbishment. Effective and efficient support for Services and Departments
A review of the working practices of the Maintenance Team is to be undertaken to enhance the support given to all Services and Departments, including support to fulfil their own objectives in the Business Plan. Tabs FM to be developed to provide the monitoring and feedback tool to enable maintenance to review and improve the support provided.
Year 1:
We will source PDA’s for each team member and develop a training plan on the use of PDA’s, develop working practices and identify key performance indicators (KPI’s) and set up a monitoring system of the KPI’s identified using Tabs FM.
Year 2 onwards:
We will analyse the data provided on an annual basis to embed a culture of continuous improvement within the maintenance function. Go Green
An analysis of our carbon footprint in regard to all aspects of energy efficiency will be undertaken with a resulting reduction in our energy consumption of 20% over 3 years. To enable this all available alternative sources of energy will be reviewed. Statistics will be produced in April of 2014, 2015 and 2016 to monitor the energy efficiency savings. Years 1, 2 & 3 - Area’s to be explored:
Solar energy panels.
Wind turbine.
Heat recovery systems.
Page | 41
Electric vehicles – hybrid vehicles.
Rain water harvesting.
Recycling & paper light.
Energy efficient lighting.
Energy efficient boilers.
Timer control systems on ventilation equipment.
Energy Saving Trust.21
Each area will be subjected to various criteria including the following:
Initial outlay
Actual savings over a predetermined interval.
Comparison with other initiatives to establish cost effectiveness.
Availability of external funding, subsidies or sponsorship.
Impact on the local community.
Professional guidance.

Page | 42
10. FUNDRAISING DIRECTORATE Hospice in the Weald is well known and respected across our catchment area of West Kent and East Sussex and we are dependent on our reputation throughout the community we serve in order to raise the funds we need. It is these funds that ensure we can continue to provide our services and enable our philosophy of care to reach local patients, families and carers at home or at the Hospice. As the Hospice plans to see more patients and meet more and more unmet need, we need to raise more funds to ensure that everyone who needs our services has access to them. The Hospice has successfully fundraised from the local community for over 30 years and we must continue to evolve our fundraising effort to be able to react to both the changing external environment and the changing needs of the organisation. At the forefront of all activity undertaken by the Fundraising Directorate is the responsibility to the organisation to inspire and motivate others to give to Hospice in the Weald – whether that is through fundraised income, volunteering time or acting as an advocate for the Hospice. To effectively inspire and motivate, we must continually meet the challenge of keeping both existing and potential supporters informed and knowledgeable about the vital difference our services make to patients, families and carers in the community we serve. Following the successful delivery of the Fundraising objectives from our first Business Plan including an amended Fundraising Directorate structure, the establishment of income streams through Major Investors and Lottery giving, an ambitious Events programme and an increased profile in the local area through strong media links and relationships, these next three years will take on a different focus for the Fundraising Directorate. As part of ensuring sustainability for the Hospice we will extend our supporter base more widely in the local community by testing areas with Direct Mailings and using our shops more strategically to promote Events and campaigns. While we know our patients are based in the West Kent and East Sussex area, increasingly those who have been affected by our services, including family, carers, friends, and colleagues of patients, are from further afield and we want to engage with everyone who has been directly affected by the high level of care provided by our Services and Departments in order to maximise the fundraising potential from these supporters. The Hospice has historically seen about 20% of our income come through Gifts in a Will22 left to us. In effect people who leave us a Gift in their Will fund the care for one in five of our patients. The trend over the past few years is that this figure is increasing slightly, and is likely to continue to do so over the next five to ten years. Our priority is to enable people in the local community to choose to support us in this way by providing them with the information and support they need in order to do this.

Page | 43
10.1 Fundraising Objectives The focus of the Fundraising Directorate over the duration of this Business Plan is to ensure that our fundraising activities are ambitious, innovative, and that we continue to capitalise on opportunities by working effectively together as a team. Whilst we need to grow income, we will do so efficiently and effectively and continue to deliver value for money. By focusing on developing a wider supporter base, we are confident that we will be providing the Hospice with long term sustainable income. As the economic climate remains somewhat unsettled as well as the external environment with changes to the NHS and CCG commissioning bodies, the priority for the Fundraising Directorate will be ensuring there is a minimal risk to the income from the community on which we depend and on which we may become increasingly reliant in the future. Though much of our work remains focused on our engagement across the wider local community, we also recognise the need to work closely with our colleagues within the organisation. Our fundraising ambitions will only be effective if they match the expanding needs of our clinical services and if we work closely with our colleagues in our extensive Commercial Directorate. We will use our communications channels, including social media and other technology, to share stories of our patients, their families and carers to engage new supporters and maintain the reputation of Hospice in the Weald in the local community. We will also make best use of technology within the organisation to ensure that those who come into contact with the Hospice, whether as a patient, family member, carer or supporter receive a consistent first class experience from an organisation that prides itself on individualised Hospice care. We will proactively seek long term partnerships with businesses in the community we serve not only to maximise our fundraising potential, but also to ensure that we continue to deliver value for money and are able to demonstrate to all of our supporters that the money given to the Hospice stays locally with 90p of every £1 funding patient care in the local community. Supporter Acquisition
We will double the number of records on our supporter database to which we proactively mail newsletters and direct mail from 40,000 at the start of 2014 to 80,000 by the start of 2017. We will value and cherish our supporters with a relationship fundraising approach.
By making better use of data imports from our shops’ Loyalty Cards, capturing details from visitors to the Hospice, through better use of our own Hospice communication channels, and through greater segmentation of our database for mailing activity, we will acquire new supporters and re-engage with past supporters.

Page | 44
New supporters will be placed on a clearly defined supporter journey based on how they have come into contact with the Hospice. For example, if they have shared their details with us because they have visited someone in the Hospice, work for a local business, or have registered for one of our Hospice events. This will enable us to better plan our communications with individual supporters so they receive information that is not only relevant to them specifically, but helps keep our costs down and will ensure we do not inundate any one supporter with too much information. We will work hard to continue our approach of Relationship Fundraising so that all supporters have a tailored, individual communications plan from us with at least one request to give within 12 months of being added to our Supporter database with the aim of becoming active supporters who give regularly to the Hospice.
Year 1: We will have extended our supporter database to 50,000.
Year 2: We will have extended our supporter database to 65,000.
Year 3: We will have extended our supporter database to 80,000. From those to whom we send regular communications (newsletters, direct mail) we will increase our active supporters – those who have given to us in the past 12 months – from 12.5% of our database in 2014 to 22.5% of our database by 2017. Supporter Database The most important tool we have in the Fundraising Directorate is our database. Supporter communications are recorded in the database and it drives our ability to inform, educate and ask existing and potential supporters of Hospice in the Weald.
Following on from the previous Business Plan and to enable our primary objective of increasing the overall supporters of the Hospice, we will make Donorflex the main, non-clinical, database across the organisation and ensure it is the only database being used for external non-clinical mailings by working closely with the ICT and other Departments and Services.
In Year 1, to ensure regular imports continue from both the Lottery and Commercial Directorate databases into Donorflex so all supporter information is held centrally in Donorflex and to carry out a data cleanse to remove incorrect, incomplete or duplicated data. By the end of Year 1 ensure that any supporter data held by the Finance and Personnel Departments is being imported into Donorflex and any relevant mailings from the Personnel Department are generated from Donorflex mailing data.
By end 2015 work alongside the ICT Department to review Donorflex and its capabilities/limitations, explore competitors in the database marketplace and investigate an alternative Customer Relationship Management (CRM) solution which meets database integration plans with Hospice-wide Enterprise Resource Planning.

Page | 45
Website The Hospice in the Weald website is, and will remain, one of the most important communication tools for the organisation not only for the Fundraising Directorate, but as the main source of information about our Services for the community. The responsibility of the website falls under the remit of the Fundraising Director with the support of the cross-departmental Website Content Group.
We will look to redevelop the Hospice in the Weald website to ensure it can reflect developments at the Hospice, that content is kept up to date, and that it has the ability to adapt easily to meet the needs of the organisation through the growth period over the next three years. The website must also reflect developments in technology to meet the needs and expectations of our supporters and those that we help through our services.
Development of the website will look to include (but not be limited to): mobile optimisation, e-newsletter signup, community chat rooms, online help/resource for patients, families & carers, service signposting & FAQs, social media integration, improved online donation pathways and e-commerce systems.
Year 1: Devise a plan for complete website redevelopment including external tender process and briefing document to be approved by the Hospice Leadership Team by June 2014. Tender contract to be agreed by August 2014 for design and implementation by January 2015. Establish agreed measures for traffic and conversion rates for fundraising tools (online donations, e-commerce, communications sign ups) with similar measures of success agreed by the Website Content Group for other Services and Departments.
Year 2: Continue to evaluate website against agreed measures. Aim to see an increase in online donation activity, using online donations received in the financial year 2013-14 as a base point and agreed year on year % improvement as target.
Lottery The Hospice in the Weald lottery is a crucial form of sustainable, regular income for the Hospice. We currently have 7,200 weekly players and aim to grow this income stream significantly over the next three years so that by March 2017 the lottery is generating £1,000,000 a year for Hospice in the Weald.
We will recruit a team of lottery salespeople to secure new weekly players through door to door sales, telesales and static sites. We will continue to use our Hospice communication channels to promote the lottery to our supporters. We will develop a lottery product for our corporate partners, so that their employees can establish lottery syndicates. We will establish a meaningful way to monitor and measure drop off rates and develop a retention plan by the end of year one, establish a benchmark and then achieve an increase in year two and year three.

Page | 46
Year 1: Recruit a new team of lottery salespeople and increase weekly players to 12,500 a week by the end of year one, generating £550,000 in year one. Introduce a second raffle, increasing raffle income to £90,000 a year.
Year 2: Increase lottery and raffle income by 20% to £780,000.
Year 3: Increase lottery and raffle income by 15% to £1,000,000.
Corporate Fundraising – working with businesses in our community Having had a more informal and reactive approach to Corporate Fundraising since the 2008 recession, we now want to pursue a more targeted and proactive approach to this growing income stream. Even through the difficult period following the 2008 recession, local businesses have continued to be generous to Hospice in the Weald through event sponsorship and regular fundraising. We want to further engage these businesses as they recognise the value and benefits of having a mutually beneficial partnership with the Hospice. Having recruited a Corporate Fundraising Manager and with a Corporate Fundraising Plan in place, we have ambitious growth targets for the duration of the Business Plan.
We will not only maximise income which can be raised through businesses, but also to help our chosen partners to maximise their reciprocal benefit from supporting us, whether this be through employee volunteering, team building activities, or just the feel good factor from making a significant contribution towards patient care.
Year 1: Recruit 30 companies to participate in the Hospice fundraising week. Secure £40,000 from new corporate partners by end of year one. Secure minimum of one charity of the year partnership worth over £5,000.
Year 2: Retain 70% of partnerships from year one, establish seven new partnerships worth over £5,000. Secure £60,000 from new corporate partners by end of year two. Secure minimum of one charity of the year partnership worth over £5,000.
Year 3: Retain 70% of partnerships from year two and establish ten new partnerships worth over £5,000. Secure £80,000 from new corporate partners by end of year three. Secure minimum of one charity of the year partnership worth over £5,000.
Hospice Events – new flagship event; the next big thing
To research, identify and implement a new mass participation fundraising event with over 1,000 participants by 2017 with improved year on year performance by the end of the Business Plan period.
Year 2: Research and plan new large scale fundraising event which will show a profit of at least £50,000 with the event scheduled to take place in Year 2 and in each subsequent year.
Year 3: Deliver marketing & event plans with agreed fundraising target and event objectives including measurable data (average donation, non-donation rate, entry conversation, event sponsors etc.) as applicable.

Page | 47
11. PERSONNEL DIRECTORATE In 2013 as part of an on-going review of the Hospice’s organisational structure the Finance Directorate was created. The new Directorate manages the ICT, Accounts and Maintenance functions. The Personnel Directorate also came into being to manage the Personnel, Catering and Housekeeping functions rendering the old Operations Directorate redundant. The appointment of a Personnel Director reflects the importance the organisation places on providing appropriate support and expertise in the management of its key resource – staff and volunteers. Historically the Hospice in the Weald Personnel Department has focused on the development and administration of personnel policy and procedure. As a consequence the Hospice enjoys a framework of well-structured and robust policies to support managers in the daily management of their staff. Work will continue to review and regularly update those policies and frameworks to ensure that they meet current need and comply with legislation. We will also work to ensure that administration procedures, including payroll are as efficient as we can reasonably make them. The major challenge going forward is to develop expertise within the Personnel Department so that personnel staff can act as ‘internal consultants’ to managers. That is, providing them with advice and guidance on people related matters (staff and volunteers) as they develop plans to improve the operation of their departments and services. In this way the Personnel function can provide a more proactive service and be of greater help to management and the organisation rather than just dealing with administration or reacting to events that have already occurred. In the following section the terms ‘personnel’ and ‘workforce’ are used interchangeably. As part of recognising that Hospice Palliative Care is a British social movement that has much to share with the world we will, between 2014 and 2017, explore a ‘Twinning Partnership’ arrangement with a hospice from a developing country. We think there are benefits for both a partner hospice and for Hospice in the Weald. Mainly the benefits are for the hospices’ workforce but also for the communities we serve. We won’t ever fundraise for them and will be careful it does not have a negative impact on our clinician’s time. We don’t know where the long process of exploring this will lead and cannot answer many questions at this point – the start of the process. The CEO and Personnel Director will take forward this ‘Twinning Partnership’. The objectives for the Personnel Department are part of three interlinked themes:
Maintaining staff turnover at an appropriate level.
Developing a management culture that is supportive to the employee and which encourages the employee to achieve higher levels of performance.
Recruiting and training the volunteers that will allow us to develop and support Hospice in the Weald services.
Staff Turnover Staff turnover is a measure of the rate at which staff leave an organisation. For the Hospice in the Weald, staff turnover is measured by the total number of staff leaving in a defined
Page | 48
period divided by the average number of staff employed in the same period. Staff turnover can be good for an organisation. New staff bring enthusiasm and can contribute new ideas and fresh approaches. However, excessive turnover creates difficulties. It drives up recruitment and training costs; it absorbs management time, dilutes organisational expertise and makes the provision of a consistently high standard of service problematic. Hospice in the Weald has experienced a period of reorganisation and change and unfortunately staff turnover has risen during this period. We wish to see staff turnover at a healthy, modest and stable level. Clearly a Personnel Department cannot influence the wide range of personal factors that can motivate an individual to change jobs but it can facilitate a review a number of factors known to be associated with staff turnover e.g. recruitment of the right staff, providing appropriate remuneration, ensuring a motivational and supportive management culture. Management Culture The length of time an employee or volunteer stays in post is often governed by the nature of the relationship the person has with his or her manager. We wish to encourage a coaching management culture that strives for an environment of high standards but with high support for staff and volunteers. “Coaching is a particularly powerful tool in the modern workplace – one that has proven to be a highly effective way of developing individual and organisational performance by unlocking capability. At its best, this key management tool can deliver considerable benefits, helping managers get the most from their teams, boosting employee engagement and developing high performance workplaces.” (Institute of Learning and Development 2011 Report ‘Creating a Coaching Culture’).23 It is our intention to develop a coaching culture within Hospice in the Weald whereby every manager sees it as a natural part of their role to coach their staff for improved performance and feels comfortable in doing so. Coaching has the potential to be a low cost method of developing expertise in the workforce and improving the retention of both staff and volunteers. Whilst coaching clearly takes place already within the organisation we wish to see it extended so that it becomes a core management practice throughout the organisation. Volunteer Recruitment The Hospice is very fortunate that it is already very well supported by approximately 900 volunteers in a wide variety of roles. The volunteers provide help and expertise which we simply could not afford to buy and the delivery of many Hospice in the Weald services depends on their dedication. To continue the expansion of services we must attract even more volunteers to complement those already helping us. The objective is to attract and induct an additional 200 volunteers with the skills required by our services and departments. It is of course, also necessary to retain or replace as necessary the volunteers which we already have. The expansion of volunteers will not be matched by an increase in paid staff and so it is implicit in this objective that we must expand the use of Co-ordinating

Page | 49
Volunteers whose role it will be to co-ordinate and monitor the work of their fellow volunteers. 11.1 Personnel Objectives
To ensure staff turnover is between 15% and 20% measured over the three year
period of this Business Plan. This target is in line with the range of staff turnover figures typically reported by other hospices.
To produce a report on the competitiveness of Hospice in the Weald employee
reward for Trustee consideration. - Deadline 31st October 2014. Any approved changes to be implemented by April 2015 at latest.
Recruitment – Attracting and Selecting the Right Candidates. To develop and
implement a recruitment and selection training programme and to have 80% of managers responsible for recruitment to attend training. Deadline 31st December 2014.
Education and Development. To develop a budgeted workforce (staff & volunteers)
development plan for CEO approval. Deadline 30th June 2014. Coaching Culture
Year 1:
85% staff with a direct responsibility for managing the work of others will have received formal training on the principles and practice of coaching. Deadline June 2015.
Competencies related to effective coaching will be defined and incorporated into all management Person Specifications and will be incorporated into the recruitment process for these roles. Deadline August 2014.
Responsibility for coaching and developing staff and volunteers will be incorporated in the general responsibilities of all management role descriptions. Deadline June 2014.
Staff Appraisal Policy & Procedure to be revised to incorporate reference to the purpose and value of coaching.
Year 2:
Not less than 20% of the above population will have undergone some further development to enhance their effectiveness as a coach. Deadline December 2015.
Staff opinion, when surveyed, will show that in excess of 50% of respondents agree that Hospice in the Weald has a ‘coaching culture’ that supports the development of staff knowledge and skills. Deadline December 2015. Target to be 55% by December 2016.
Volunteer Recruitment Cumulative Addition to Volunteers Numbers
Year 1: Grow the number of volunteers by 50 by 31st December 2014.
Year 2: Grow the number of volunteers by a further 75 by 31st December 2015 (125 cumulatively).
Page | 50
Year 3: Grow the number of volunteers by a further 75 by 31st December 2016 (200 cumulatively).
11.2 Support Services – Catering and Housekeeping Objectives
The Hospice benefits from a high standard of catering and housekeeping and staff cope with a high level of activity. For example, Catering prepare and cook approximately 24,000 fresh meals a year and our laundry washes c120,000 items a year taking up c6570 hours of washing machine time. The focus for these teams during the duration of the Business Plan will be on maintaining standards whilst adapting to the changing requirements of the patient services. Catering Food Hygiene
To retain the confidence and support of the Tunbridge Wells Borough Council in
respect of food hygiene in order to retain the highest rating (5) under The National Food Hygiene Rating Scheme24 by:
Compliance with food hygiene and safety procedures (including food handling practices and procedures, and temperature control.
Compliance with structural requirements (including cleanliness, layout, condition of structure, lighting, ventilation, facilities etc).
Confidence in management/control procedures. To ensure that all points in our operation which are critical to food safety are clearly identified.
Patient Food Service
Actively promote and pursue a flexible and explorative approach to the service of food and refreshments by:
Publishing a questionnaire and feedback form for patients, visitors and staff.
Recruiting additional volunteer In-Patient Unit Hosts.
Revenue
Carry out a feasibility study (during 2014) into increasing catering income (Business Plan 2015) by:
Extended use and availability (longer opening times) for the staff dining room.
Dual tariffs for staff and visitors.
Wider range of refreshment options for the Coffee Shop; extended opening times and increased seating to accommodate (and educate) our local community and ‘passing trade’.
More refreshment choices for In-Patient Unit visitors out of normal service hours.
Page | 51
Housekeeping
Cleaning
Maintenance of in-house cleaning and laundry services and infection control measures in accordance with Hospice in the Weald policies and procedures:
Policies & procedures to be updated to the laid down schedule to ensure on-going relevance and work standards and systems adhere to the principles of The British Institute of Cleaning Services25 and the National Health Service Training Manual26 for domestic students.
Establish the principles and culture of quality control within the cleaning function:
Frequency of cleaning.
Formalised fault reporting & monitoring via Tabs FM.
Accountability by signing off cleans by room and area. Health
Introduce the basic principles of Body Mechanics to Support Services staff with awareness that motion should be productive and movement economic to help make physical work easier and prevent personal injury by:
Establishing and delivering a course of training and certification in collaboration with the Training Centre
Exploring with we:train the opportunities for marketing the course externally to Hospice in the Weald.
Revenue
Carry out a feasibility study (2014/15) into marketing housekeeping services (cleaning) to the local community. The customer base within our shops may provide the springboard for a viable Business Plan to be constructed during 2015/16. We believe the initiative has the potential to:
Extend our services and raise our profile in the community and gain goodwill and open a possible revenue stream.

Page | 52
12. BUDGET & FINANCIAL IMPLICATIONS
We mentioned in our last Business Plan that often charities judge their success by a focus on fundraising and the funds coming in. We try to see the funds coming in as inputs and whilst they are vital for us to continue our much needed work and fund our intentions to meet more unmet need, we want to be judged and judge ourselves on outcomes. The quality of our Services and the outcomes we strive to deliver for patients, families and carers. You will see in the budget that we have set in this Business Plan that we plan to take over £500,000 from our financial reserves in 2014/15. We are confident that we can grow our fundraising efforts to move back to a balanced budget before the end of the period this Business Plan covers. A few years ago the Charity Commission guidance to local charities like Hospice in the Weald was to keep 2 years running costs as financial reserves. However, their guidance in recent years leaves the level to Trustees to decide upon. The Trustees are aware that the community we serve gives so generously with the expectation funds are spent on the services we provide. They are also aware of the current unmet need. Trustees and the Hospice Leadership Team are acting in a prudent way in setting this budget and aims in the Business Plan. We are confident we have found the right balance and are committed to deliver on all we say.

Page | 53
12.1 Contribution Summary 2014/15
Hospice in The Weald Budget to
31st March 2015
Contribution Summary
£
Central
971,126
Commercial Directorate
828,456
Finance Directorate
-721,303
Fundraising Directorate
3,585,125
Medical Directorate
-796,576
Nursing Directorate
-3,765,571
Personnel Directorate
-755,977
Investments realised gains
150,000
Funded from reserves
HitH Step Change
410,000
IPU move to 15 Hospice beds
97,837
Totals 3,117
Investment unrealised gains
0
Total for the year 3,117
12.2 Income from Statutory Sources 2014/15
CENTRAL
Budget to 31st March
2015
Income from Statutory Sources
£
Drug Funding
54,000
Hospice Day Services
27,000
Hospice in the Home
356,000
In Patient Unit
306,000
Lymphoedema
85,844
Medical
95,000
Pension Funding
47,282
Contribution 971,126

Page | 54
12.3 Commercial Directorate Budget 2014/15
COMMERCIAL DIRECTORATE
Budget to 31st March
2015
Income
£
Weald Enterprise - WE:Train
45,000
Retail
2,435,242
Total Income 2,480,242
Expenditure
Weald Enterprise - WE:Train
99,751
Retail
1,552,035
Total Expenditure 1,651,786
Contribution 828,456
12.4 Medical Directorate Budget 2014/15
MEDICAL DIRECTORATE
Budget to 31st March
2015
Income
£
Chaplaincy
3,600
Consultants Fees
2,000
Counselling Support Services
7,800
Medical DWP & Cremation Fees
12,000
Total Income 25,400
Expenditure
Chaplaincy
57,307
Counselling Support Services
267,482
Medical
497,187
Total Expenditure 821,976
Contribution -796,576

Page | 55
12.5 Finance Directorate Budget 2014/15
FINANCE DIRECTORATE
Budget to 31st March
2015
Income
£
Accomodation Charge
6,000
ICT
500
Finance
87,100
Maintenance
60
Shop rentals
45,000
Total Income 138,660
Expenditure
Building, Extention & COLBUS Depn
211,898
Depn Equipment
27,940
Finance
132,407
Freehold Shops Repairs & Renovations
0
Heat & Light
72,000
ICT
159,393
Insurance
22,420
Maintenance
233,905
Total Expenditure 859,963
Contribution -721,303

Page | 56
12.6 Fundraising Directorate Budget 2014/15
FUNDRAISING DIRECTORATE
Budget to 31st March
2015
Income
£
Collections - Stores & Street
5,460
Community Events
458,600
Corporate
138,000
Donations - General
190,000
Direct Marketing
114,000
Donations - Lottery & Raffle
12,500
Friends Groups
50,000
Gift Aid
250,000
Gifts in Wills
1,210,000
Hospice Events
317,009
In Memory
550,000
Lottery
640,000
Major Investors
350,000
Travel Club
28,200
Trusts
125,250
Total Income 4,439,019
Expenditure
Community Events Costs
15,000
Direct Mailing Costs
20,000
Donorflex
5,000
Friends Group Costs
5,000
Hospice Event Costs
61,592
In Memory Costs
5,000
Lottery
264,695
Major Investors
4,500
Publicity & Marketing
144,115
Staff Costs
313,592
Travel Club
15,400
Total Expenditure 853,894
Contribution 3,585,125

Page | 57
12.7 Nursing Directorate Budget 2014/15
NURSING DIRECTORATE
Budget to 31st March
2015
Income
£
Hospice Day Services
2,400
Education Learning and Development
0
Hospice in the Home
800
In Patient Unit
20,200
Therapies
0
Lymphoedema
5,000
Total Income 28,400
Expenditure
Drugs
54,000
Education Learning and Development
57,524
Hospice Day Services
375,642
Hospice in the Home
1,690,864
In Patient Unit
1,212,278
Lymphoedema
219,366
Therapies
184,297
Total Expenditure 3,793,971
Contribution -3,765,571
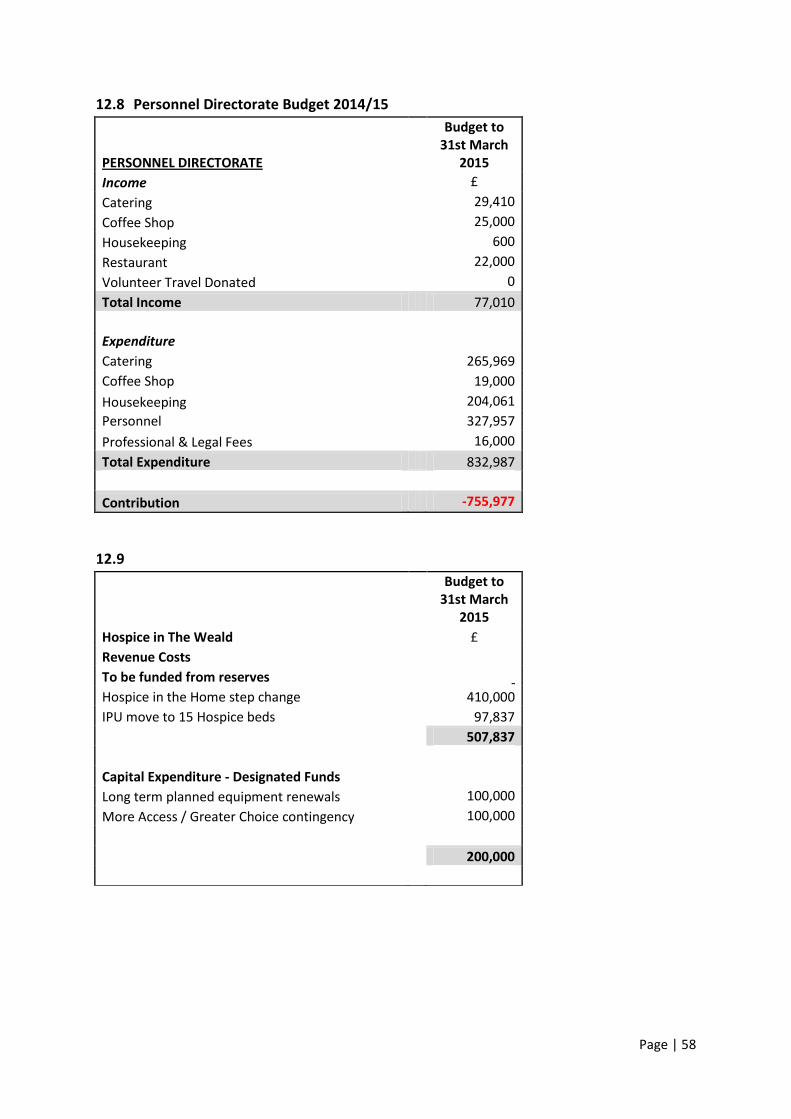
Page | 58
12.8 Personnel Directorate Budget 2014/15
PERSONNEL DIRECTORATE
Budget to 31st March
2015
Income
£
Catering
29,410
Coffee Shop
25,000
Housekeeping
600
Restaurant
22,000
Volunteer Travel Donated
0
Total Income 77,010
Expenditure
Catering
265,969
Coffee Shop
19,000
Housekeeping
204,061
Personnel
327,957
Professional & Legal Fees
16,000
Total Expenditure 832,987
Contribution -755,977
12.9
Budget to 31st March
2015
Hospice in The Weald
£
Revenue Costs
To be funded from reserves
Hospice in the Home step change
410,000
IPU move to 15 Hospice beds
97,837
507,837
Capital Expenditure - Designated Funds
Long term planned equipment renewals
100,000
More Access / Greater Choice contingency
100,000
200,000

Page | 59
12.10 Summary of 2015/16
Hospice in The Weald Budget to
31st March 2016
Contribution Summary
£
Central
1,000,000
Commercial Directorate
1,200,000
Finance Directorate
-742,942
Fundraising Directorate
4,064,000
Medical Directorate
-820,473
Nursing Directorate
-4,401,610
Personnel Directorate
-778,656
Investments realised gains
180,000
Totals -299,682
Funded from reserves
300,000
Total for the year 318
12.11 Summary of 2016/17
Hospice in The Weald Budget to 31st
March 2017
Contribution Summary
£
Central
1,000,000
Commercial Directorate
1,400,000
Finance Directorate
-765,230
Fundraising Directorate
4,270,000
Medical Directorate
-845,087
Nursing Directorate
-4,533,659
Personnel Directorate
-802,016
Investments realised gains
220,000
Totals -55,992
Funded from reserves
56,000
Total for the year 8

Page | 60
13. MONITORING & EVALUATION OF THE BUSINESS PLAN Hospice in the Weald has been transformed over the period of the previous Business Plan (2011 – 2014) in respect of how we monitor and evaluate our work. The Medical and Nursing Director, along with our Clinical Governance Committee (made up of Trustees and external advisors) have done a plethora of things which have led that transformation. Among them some ground-breaking work on the NICE Palliative Care Quality Markers. The Hospice now has some excellent ways to measure quality developed from nationally recognised bespoke quality markers. We are also in a very different position than previously to be able to monitor progress against our aims and objectives in this Business Plan. We will again produce a summary of this Business Plan in a small compact format and produce an update on progress in each year in our Annual Review. In addition we will also, within six months, produce a ‘Balanced Scorecard’27 approach to our work and produce a ‘Social Value Statement’.28 We will ensure wide distribution of all of these documents alongside an easy to read document containing our key messages. Please refer to the Synopsis (Appendix I) for an overview of this Business Plan. A large part of the monitoring and evaluation of the Business Plan is actions that take place internally. We now have a well-used and clearly defined ‘traffic light’ system and exception reporting. We also ensure that each objective in the Business Plan is clearly set to have an effect on at least one strategic aim and we will monitor its progress. The Hospice Leadership Team and Board of Trustees keep a close watch on how we are doing in respect of delivering the aims and objectives set out in the plan. We have not in this Business Plan, addressed the issues related to ‘risk’. However, Hospice in the Weald has a very robust and comprehensive risk management strategy which when adopted in 2012 built upon a risk management policy. It provided a practical way forward to ensure that the key risks are identified and then controlled via meaningful control actions. Any and all risks associated with this Business Plan will be dealt with under our risk strategy and we will undertake a review of that strategy within the first three months to ensure it remains ‘fit for purpose’. We will not record the risks in this Business Plan as risk management is a dynamic and ever-changing process with risks being identified and being kept under constant review. A Business Plan is, in many respects, just one snapshot in time.
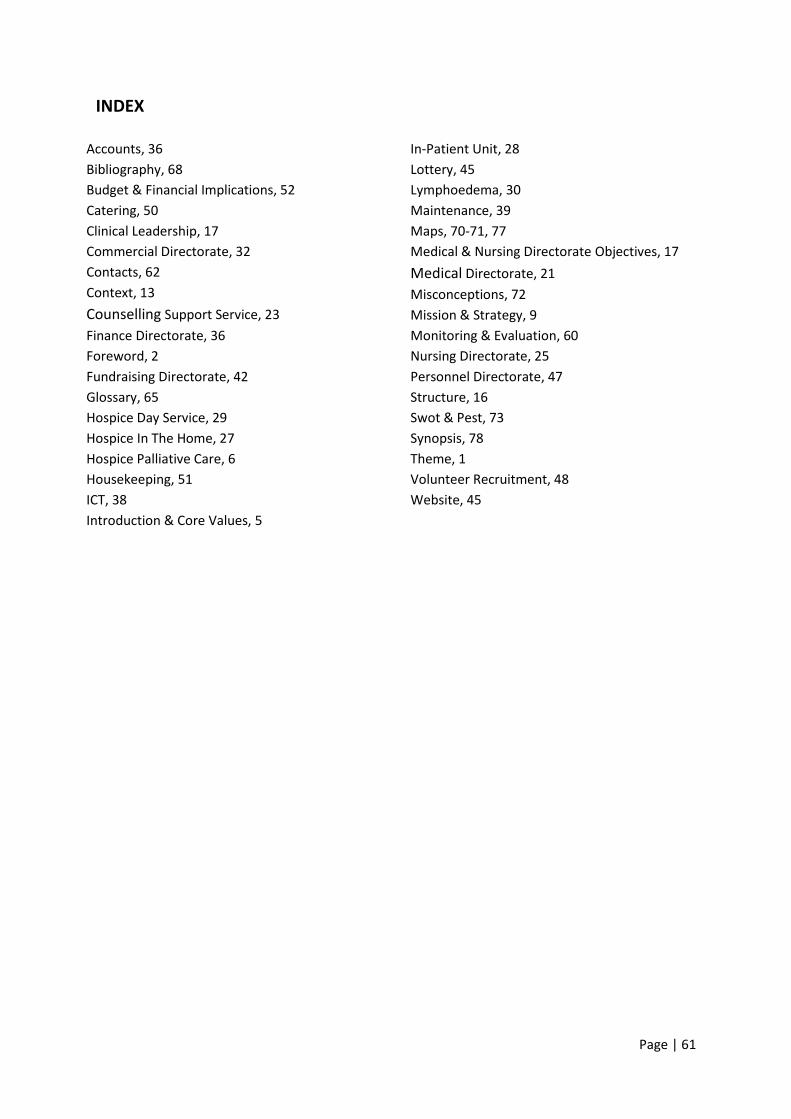
Page | 61
INDEX
Accounts, 36
Bibliography, 68
Budget & Financial Implications, 52
Catering, 50
Clinical Leadership, 17
Commercial Directorate, 32
Contacts, 62
Context, 13
Counselling Support Service, 23
Finance Directorate, 36
Foreword, 2
Fundraising Directorate, 42
Glossary, 65
Hospice Day Service, 29
Hospice In The Home, 27
Hospice Palliative Care, 6
Housekeeping, 51
ICT, 38
Introduction & Core Values, 5
In-Patient Unit, 28
Lottery, 45
Lymphoedema, 30
Maintenance, 39
Maps, 70-71, 77
Medical & Nursing Directorate Objectives, 17
Medical Directorate, 21
Misconceptions, 72
Mission & Strategy, 9
Monitoring & Evaluation, 60
Nursing Directorate, 25
Personnel Directorate, 47
Structure, 16
Swot & Pest, 73
Synopsis, 78
Theme, 1
Volunteer Recruitment, 48
Website, 45

Page | 62
APPENDIX A - MANAGEMENT & GOVERNANCE CONTACTS Rob Woolley Chief Executive Officer 01892 820518 [email protected] Rob became CEO Hospice in the Weald in 2010 after being in charge of another adult Hospice, Trinity and a Children’s Hospice, Brian House. He enjoyed a long career in the RAF medical services in various management roles and, since leaving in 1996, has been the CEO of a number of Charities. Rob’s interest in the not for profit sector in general, and specialist palliative care in particular, is longstanding. He has a Social Science degree, a Masters in Business Administration (MBA) and a Post Graduate qualification in Voluntary Sector Studies. Prior to his arrival he was in his second year of a PhD with the International Observatory in End of Life Care but has put those studies on hold – however, he definitely aims to return to them one day! Helen McGee Medical Director 01892 820503 [email protected] Dr Helen McGee is a Consultant in Palliative Medicine. She trained at Edinburgh University and then moved to London where she completed her specialist training working in several hospices, acute hospitals and the community setting. She is an active Fellow of the Royal College of Physicians and has been based in Kent since 2006. She has a Postgraduate Certificate in Medical Education and her specialist interests include teaching and advance care planning. Helen is Honorary Lecturer at the University of Kent. Paula Wilkins Nursing Director 01892 820515 [email protected] Paula completed her nurse training at St Bartholomew’s Hospital, London where she worked as a Staff Nurse, Senior Staff Nurse and then Sister in Oncology/Haematology. After this Paula moved to St Thomas’ Hospital (Later becoming Guy’s and St Thomas’ NHS Foundation Trust) where she furthered her career in both haematology and Nurse Leadership obtaining her Masters degree in 2003. She is passionate about ensuring that patients receive an excellent standard of care and that the care delivered is individualised to the patient, carer and family’s needs. Karen Harper PA to the Medical Team 01892 820534 [email protected]
Page | 63
Karen joined us in 2009 as Medical Team PA and looks after our Medical Director, Consultants and Doctors. She also administrates our Clinical Management Team and Clinical Governance meetings. Karen previously worked for BUPA at their Wellness Centres in Canary Wharf as Client Services Team Leader, overseeing the GP Practice, Musculoskeletal Clinic & Dental Surgery. Nick Farthing Commercial Director 01892 820535 [email protected]
Nick joined Hospice in the Weald in 2011 as Head of Retail following a career in corporate retail. Appointed as Commercial Director in 2013 he is passionate about combining the strengths of charity retail, High Street best practice, and fundraising innovations to achieve a truly integrated approach to donor development. Nick graduated from the University of Central Lancashire in 2008 and has always had a passion for education, training and development. He is responsible for the Hospice in the Weald Training Centre and leads on taking commercial opportunities that add to the funding of Hospice in the Weald.
Jo Lavender Finance Director 01892 820523 [email protected] Jo joined the Hospice in November 2002 as Accounts Office Manager after running her own accountancy business and gaining a BA (Hons) in Finance and Accounts whilst bringing up two children. Jo progressed through the Finance office to Finance Manager and then Head of Finance. In 2010 Jo was successful in becoming the Operations Director widening the scope of her job to take in not just Finance but Personnel, ICT, Facilities, Catering and Housekeeping. In 2012 the Finance Directorate was formed and Jo was successful in becoming the Finance Director managing Accounts, ICT and Maintenance. Jo is currently completing exams to become a qualified accountant through ACCA. Sarah Pugh Interim Fundraising Director (until Summer2014) 01892 820536 [email protected] Sarah joined Hospice in the Weald as Interim Fundraising Director in November 2013. Sarah has over 12 years’ experience leading fundraising teams. Before joining Hospice in the Weald, Sarah was head of Corporate Fundraising at Breast Cancer Care for six years, where her team raised over £4 million annually through partnerships with companies including Asda, Boots and Dorothy Perkins. Prior to this, Sarah was Head of Corporate and Events Fundraising at The National Autistic Society and Senior Corporate Partnerships Manager at RNID (now Action on Hearing Loss). Sarah started her career in the corporate sector in account management and new business development roles at an advertising agency and law firm.

Page | 64
Beth Swarbrigg Fundraising Director (on maternity leave until Summer 2014) 01892 820536 [email protected]
Beth joined Hospice in the Weald as Fundraising Director in April 2012. Born and educated in Canada, Beth graduated from Mount Allison University in 2001 before moving to Japan to teach English in Japanese primary and middle schools. A professional fundraiser for over 10 years, Beth has held positions at Trinity Hospice (London), the British Red Cross, and Macmillan Cancer Support and has worked on several high profile fundraising campaigns. Prior to entering into the charity sector, Beth worked for the Ottawa Citizen in Canada on the general news desk and working with the Editorial Department. Mike Todd Personnel Director 01892 820510 [email protected]
Mike was appointed Personnel Director in May 2013. Prior to this he had held senior human resources management roles in the financial services sector and the oil industry. Mike has a business degree and is a Fellow of the Chartered Institute of Personnel and Development. Peter Lewis Chairman Via 01892 820552 [email protected]
Peter was founding and Executive Chairman of the Ashtead Group plc from 1984 – 2001. He was non-executive Chairman of the Game group from June 1998 – June 2011 and brings a wealth of experience in marketing as well as general and strategic management. Clare Lisney Executive Assistant 01892 820552 [email protected]
Clare was appointed Executive Assistant in February 2014. She started working at the Hospice in June 2011 where she worked as the Lottery and Fundraising Administrator before being promoted to the Lottery Co-ordinator position in January 2012.

Page | 65
APPENDIX B - GLOSSARY OF TERMS USED
ABV Average Basket Value
ACP Advance Care Plan/Planning is a process of discussion between an individual and their care providers irrespective of discipline. The difference between ACP and planning more generally is that the process of ACP is to make clear a person’s wishes and will usually take place in the context of an anticipated deterioration in the individual’s condition in the future, with attendant loss of capacity to make decisions and/or ability to communicate wishes to others.
A&E Accident and Emergency
Balanced Scorecard A management system used to help align business activities to strategy
CCG Clinical Commissioning Group
CEO Chief Executive Officer
CHSS Centre for Health Service Studies
CMT Clinical Management Team
COLBUS Co-location and Best Use of Space
Continuing Care The term NHS continuing care means fully funded care for people who do not require care in an NHS acute hospital, but who nevertheless require a high degree of on-going health care. Anybody can qualify for NHS continuing care funding if their needs satisfy eligibility criteria, although the largest group of people who receive continuing care funding are elderly people. Continuing care funding is intended to cover the entire cost of care, including all medical care, nursing care, personal care, living costs and accommodation costs, the same as if their care was being provided in an NHS hospital.
CRM Customer Relationship Management
CSS Counselling Support Service
DEMOS A think-tank focused on power and politics. Demos has established itself as the leading independent think-tank in British politics, driven by the goal of a society populated by free, capable, secure and powerful citizens.
DNACPR Do Not Attempt Cardio Pulmonary Resuscitation. This refers to a form which is a means of communicating the decision that has been made by the patient to those who may encounter the patient in the event of a cardiopulmonary arrest.
Donorflex Fundraising and Customer Relation Management Software
ELD Education Learning and Development
Enterprise Resource Planning
A suite of integrated applications that can be used to store and manage data.
EoLC End of Life Care (generally refers to the last year of life) and is the services that are used to support those with advanced, progressive, incurable illness to live as well as possible until they die. These are services that enable the supportive and end of life care needs of

Page | 66
both patient and family to be identified and met through the last phase of life and into bereavement. It includes management of pain and other symptoms, and provision of psychological, social, spiritual and practical support. This support is not confined to discrete special services but includes those services provided as an integral part of the practice of any health or social care professional in any setting.
EPaCCS Electronic Palliative Care Co-ordination System
Evidence Based Practice
An approach where practical decisions should be based on research studies.
FP10 A prescription written by Trust Doctor and is taken to any community pharmacy for dispensing.
Governance A framework through which work organisations are accountable for continuously improving the quality of their services.
GSF Gold Standards Framework is a framework to enable a gold standard of care for all people nearing the end of their lives. GSF is a systematic evidence based approach to optimising the care for patients nearing the end of life in the community and helping them live as well as possible.
HDS Hospice Day Service
HLT Hospice Leadership Team
HitH Hospice in the Home
HitW Hospice in the Weald
Holistic See our Mission on page 10 for definition
HPC Hospice Palliative Care (See definition on page 7)
ICT Information Communication Technology
Infoflex A database containing information regarding patients, carers and families.
KMHIS Kent & Medway Health Information Services
KPI Key Performance Indicator
KSS Kent, Surrey and Sussex
Labyrinth A walking meditation designed to help the discovery of inspiration or spiritual meaning.
Lymphoedema Localised fluid retention and tissue swelling
MTW Maidstone and Tunbridge Wells
NHS National Health Service
NICE National Institute for Health and Care Excellence
OOH Out of Hours
Option Appraisal Process involving assessing options to identify projects which may be undertaken.
Palliative Active Holistic Care to those with Advanced Progressive Illness
PAS Psychological Assessment Skills
PDA Personal Digital Assistant
Person Specification Describes the attributes, knowledge, experience and skill required to do a job.
PEST Political, Environmental, Social, Technological

Page | 67
PPC Preferred Priorities of Care/Preferred Place of Care. This is a document that individuals hold themselves and take with them if they receive care in different places. It has space for the individual’s thoughts about their care and the choices they would like to make, including saying where, if possible, they would want to be when they die. Information about choices and who might be involved in their care can also be recorded so any care staff can read about what matters to the individual, thereby ensuring continuity of care. If anything changes, this can be written in the plan so it stays up-to-date.
PPM Planned Preventative Maintenance
Quality Markers Statistical measures defining priority areas for quality improvement.
R&D Research and Development
Relationship Fundraising
A donor based approach to fundraising (See Relationship Fundraising by Ken Burnett).
SMART Specific, Measurable, Achievable, Realistic, Timely
SMT Senior Management Team
SMT Exec Senior Management Team Executive
Specialist Palliative Care
Palliative care provided by multidisciplinary teams who have undergone specific training.
SWOT Strengths, Weaknesses, Opportunities, Threats
TABS FM Our electronic reporting system for ICT, Maintenance, room bookings.
UPR Usual Place of Residence
VFM Value for Money
VOICES Views of Informal Carers for the Evaluation of Services

Page | 68
APPENDIX C – BIBLIOGRAPHY 1. Hospice in the Weald Business Plan (2011-2014):
http://www.hospiceintheweald.org.uk/docs/BusinessPlan/BUSINESS-PLAN-2011.pdf 2. Find Your 1%
http://dyingmatters.org/gp_page/about-campaign
3. National End of Life Care Strategy:
https://www.gov.uk/government/publications/end-of-life-care-strategy-fourth-annual-report
4. West Kent Clinical Commissioning Group (CCG):
http://www.westkentccg.nhs.uk/homepage/#
5. West Kent End of Life Care Strategy: http://www.westkentccg.nhs.uk/about-us/publications/
6. DEMOS Report: Dying for Change
www.demos.co.uk/files/Dying_for_change_-_web_-_final_1_.pdf
7. Help the Hospices Commission into the Future of Hospice Care:
http://www.helpthehospices.org.uk/our-services/commission/
8. Future ambitions for hospice care: our mission and our opportunity: http://www.helpthehospices.org.uk/our-services/commission/resources/
9. CCG spending: http://www.england.nhs.uk/ourwork/commissioning/
10. National End of Life Care Programme Six Steps to Success “The Route to success in end
of life care – achieving quality in care homes”: www.nhsiq.nhs.uk/download.ashx?mid=8208&nid=8207
11. NICE Quality Markers for Palliative Care: http://guidance.nice.org.uk/QS13
12. National Bereavement Survey (VOICES):
http://www.ons.gov.uk/ons/rel/subnational-health1/national-bereavement-survey--voices-/2011/national-bereavement-survey--voices---2011.html?format=print
13. Palliative Care Funding Review (PCFR):
https://www.gov.uk/government/publications/independent-palliative-care-funding-review 14. Maidstone and Tunbridge Wells Research and Development Department:
http://www.mtw.nhs.uk/a-z-of-services/research-development.asp
15. Centre for Health Service Studies (CHSS) and the Research Design Service: http://www.kent.ac.uk/chss/

Page | 69
16. NICE guidance “Improving Supportive and Palliative Care for Adults with Cancer”: http://www.nice.org.uk/nicemedia/pdf/csgspmanual.pdf
17. NHS Continuing Healthcare: http://www.nhs.uk/chq/Pages/2392.aspx?CategoryID=68
18. Enhanced Rapid Response Service pilot study: http://www.kentcht.nhs.uk/home/our-services/intermediate-care-east-kent/rapid-response-west-kent/?entryid109=237054
19. Retail Business Plan:
http://www.hospiceintheweald.org.uk/docs/shops/Business-Plan-Final.pdf
20. Grant in Aid:
http://www.hmrc.gov.uk/vcs/guidance0809.htm
21. Energy Saving Trust:
http://www.energysavingtrust.org.uk/ 22. Gifts in a Will:
http://www.hmrc.gov.uk/individuals/giving/will.htm
23. Institute of Learning and Development 2011 Report “Creating a Coaching Culture
https://www.i-l-m.com/Why-ILM/Research-reports/Coaching-culture
24. The National Food Hygiene Rating Scheme:
http://www.food.gov.uk/policy-advice/hygieneratings/
25. The British Institute of Cleaning Services:
http://www.bics.org.uk/
26. The NHS Healthcare Cleaning Manual:
http://www.dhsspsni.gov.uk/cleaning_manual_section_1_contents_and_introduction.pdf
27. Balanced Scorecard: http://www.hbs.edu/faculty/Publication%20Files/10-074.pdf
28. Social Value Statement:
https://www.gov.uk/government/publications/public-services-social-value-act-2012-1-year-on

Page | 70
APPENDIX D - MAPS Our Hospice serves a community of approximately 350,000 over an area of 400 square miles of West Kent and northern East Sussex. Please see below for full details of towns and post code areas - our catchment area is based on the location of GP surgeries rather than the individual addresses of patients. (i) Hospice in the Weald Area

Page | 71
(ii) Clinical Commissioning Groups

Page | 72
APPENDIX E - SOME COMMON MISCONCEPTIONS Some myth busting facts about Hospice in the Weald: Myth: “There are never any beds at the Hospice” Only 2.4% of patients presented for admission waited 4 days or more for a bed to become available. (2013 admission audit) Myth: “It takes ages for patients to be admitted” 85% of patients presented for admission are admitted that day or the next day. (2013 admission audit) Myth: Nobody leaves the Hospice alive 50% of all admissions to the In-Patient Unit are discharged. (2013 monthly figures) Myth: “The Hospice doesn’t deal with emergencies” The In-Patient Unit has on average 5 emergency admissions per month of which 1 admission per month is out of normal office hours. The Hospice in the Home team make more than 60 urgent visits a month and over 200 urgent phone calls (2013 monthly figures). All urgent referrals are contacted by a Clinical Nurse Specialist within 24hrs of our receiving the referral. (2013 response time audit) Myth: “The Hospice only works office hours” The In-Patient Unit and Hospice in the Home are staffed to provide 24/7 care to our patients. We provide on average 64 visits / month to patients at weekends or bank holidays and an additional 33 overnight visits / month. (2013 monthly figures) Myth: “The Hospice is only for cancer patients” The majority of our patients do have a cancer diagnosis but current figures show 33% of the patients we look after have a non-malignant condition. (2013 monthly figures) Myth: “The Hospice makes no difference” 73% patients known to the Hospice who express a preference about where they would like to die, are enabled to achieve this choice. Overall only 14% of patients known to the Hospice die in hospital compared to 40% of the local general population. (2013 Quality markers and CCG figures) Myth: “The Hospice only looks after old patients” On average we have 3 referrals per month (about 3% of all our referrals) for patients under the age of 45. (2013 monthly figures) Myth: “Counselling is only available for bereaved people” 47% of our counselling sessions are for patients or family members before the patient dies with this support continuing for the family into bereavement if wanted. We contact all relatives a few weeks after death to offer bereavement support even if they haven’t had contact with us beforehand. (2013 monthly figures)

Page | 73
APPENDIX F - SWOT & PEST ANALYSES In the creation of this Business Plan we have looked at both the Internal and External Environments. The internal factors are shown as SWOT (strengths, weaknesses, opportunities, threats) and the external as PEST (political, economic, sociological and technological). We have tried to make sure our Strategic Aims and Objectives address the findings of our SWOT and PEST analysis. (NB – the numbering in brackets after some entries are part of a prioritisation process with the highest being the most important.) SWOT
Strengths
Reputation/well defined charity (9)
Quality of Service/ Standard of care (9)
Cash raised + reserves (3)
Respected clinical environment/ high qualified clinical staff (3)
Skills/knowledge/professionalism (2)
Structure- Organisational (2)
Staff (2)
Staff are willing to go the extra mile (1)
Not NHS/Independent (1)
Volunteers (1)
Relationships with other providers (1)
Effective & dynamic Fundraising department
Developing leadership
ICT
Catchment Area
Confidence in brands/goodwill
Policies/procedures/philosophy and values
A focus on EoLC/ specialist in our field
Demand expectations – are ahead of our time?
Finance
Departments not meeting needs of other departments/services
Confidence in reputation over capability to deliver
Fundraising - Static income - Dependency on gifts in wills
Weaknesses
Technology/IT development/lack of remote IT access (4)
Staff turnovers- cost/consistency/size-critical mass (4)
Not always proactive (4)
Limited salary/establishment (4)
Recruiting/attracting right skills (staff & volunteers) (3)
Lack of commerciality (2)
Beginning of “silo” working (2)
Location re. public transport (2)
Space (1)
Not true “24/7” working (1)
Existing ways of working/change culture (1)
Not linked to “right” NHS structures (1)
Morale/commitment (1)
Lack of management skills
Communication within workforce difficult
Marketing
Need to see more patients
Not NHS
ICT skills
ELD space for variety of use
Going paper-light
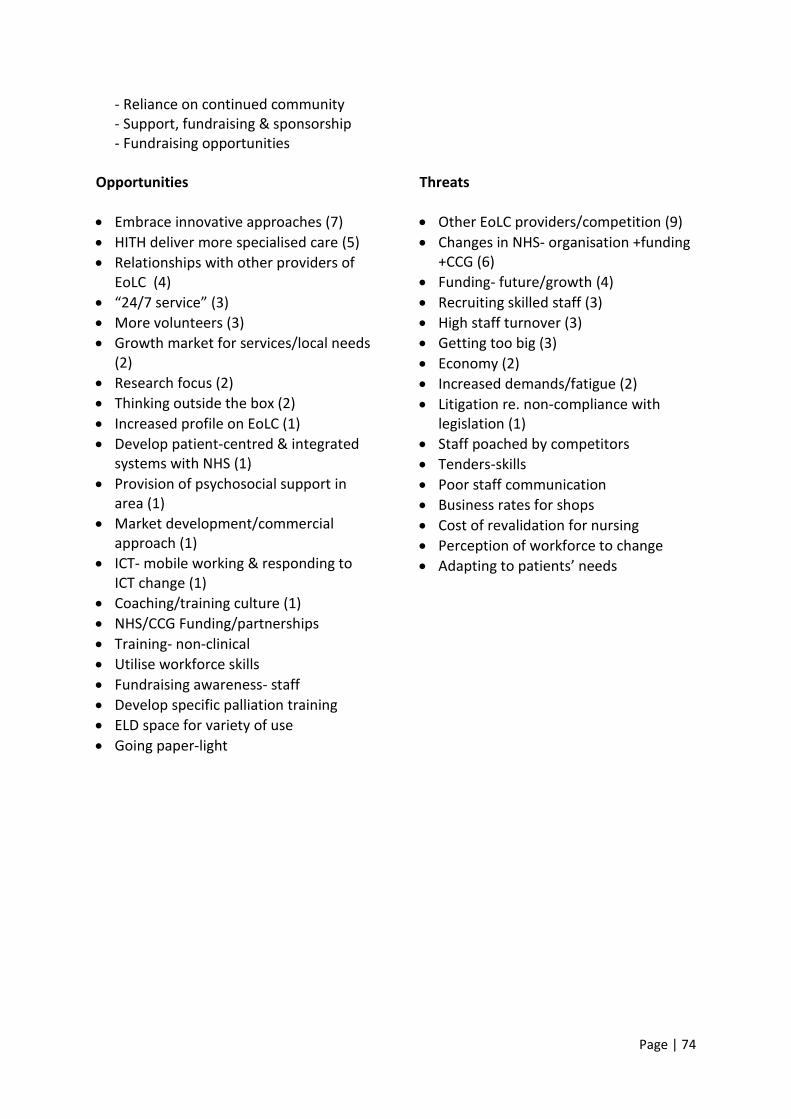
Page | 74
- Reliance on continued community - Support, fundraising & sponsorship - Fundraising opportunities
Opportunities
Embrace innovative approaches (7)
HITH deliver more specialised care (5)
Relationships with other providers of EoLC (4)
“24/7 service” (3)
More volunteers (3)
Growth market for services/local needs (2)
Research focus (2)
Thinking outside the box (2)
Increased profile on EoLC (1)
Develop patient-centred & integrated systems with NHS (1)
Provision of psychosocial support in area (1)
Market development/commercial approach (1)
ICT- mobile working & responding to ICT change (1)
Coaching/training culture (1)
NHS/CCG Funding/partnerships
Training- non-clinical
Utilise workforce skills
Fundraising awareness- staff
Develop specific palliation training
ELD space for variety of use
Going paper-light
Threats
Other EoLC providers/competition (9)
Changes in NHS- organisation +funding +CCG (6)
Funding- future/growth (4)
Recruiting skilled staff (3)
High staff turnover (3)
Getting too big (3)
Economy (2)
Increased demands/fatigue (2)
Litigation re. non-compliance with legislation (1)
Staff poached by competitors
Tenders-skills
Poor staff communication
Business rates for shops
Cost of revalidation for nursing
Perception of workforce to change
Adapting to patients’ needs

Page | 75
PEST - Political
CCG-understanding of EoLC/developments (9)
Foundation Trusts (6)
Health and Social Care Agenda (5)
Palliative Care funding review/EoLC strategy (4)
Competitive nature of new NHS (3)
Government changes (2)
Existence of NHS? (1)
Public Health Finance (1)
WKEoLC Strategy (1)
Changes in legislation
Patients’ universal benefits
Impact from National Reports
Change to Euthanasia law
Increased role of the charitable sector
Economical
CCG/NHS Funding- reduced (9)
Pay structure- compete with private sectors (6)
Competition for funds e.g. other charities (4)
Contracts/bids/tenders (4)
Drop in donors (3)
Palliative Care funding Review (2)
Funds from trusts (1)
NHS Finance (1)
Coming out of recession/continued austerity (1)
Less disposable income (1)
End users older- less care from relatives (1)
Growth at low/no cost? (1)
Limited local community- fundraising (1)
Focus on charitable sector
Patient held budgets/patient tariff
Charity fatigue
Mergers/groupings
National budgets e.g. VAT changes
Cost improvement review
Care funding changes e.g. Scotland
Foundation status of NHS trust
Distribution - “centric service”

Page | 76
Social
Aging population/changing demographic (9)
Maintain balance of ‘charity’ with ‘professional’ and ‘commercial’ (9)
Role for a hospice? – Care at home /other providers (9)
Expectations of patients & community (4)
Lifestyle trends-less altruistic? (3)
Affluent catchment area (1)
Improving economy-staffing pressure on costs (1)
Change ways of giving
Lots of charities
Communication channels
Volunteers- more/less?
Increased use of community resources
Brand
Increased demand for services=less satisfaction/damaged reputation
Social media
Reduction in social care
Lack of funding for aging population
Growing profile of EoLC- Dignity in Dying
Technological
Reaction time to communication changes in the marketplace (7)
Cross database integration (6)
Remote working (6)
Develop online interaction with hospice (3)
New equipment=maintenance costs/expense (3)
Security implications (2)
Hospice in the Weald behind other organisations with ICT (2)
Mobile technology-keep up to date/speed of change (1)
Sharing information with other organisations (1)
Research- funding/organisation/governance (1)
Social media/networking- Next big thing? (1)
Keep website up to date (1)
Quality of public IT access
Use technology to increase fundraising
4G
Expectations of patients for access to records
New developments- staying with the ‘flow’ standard
Opportunities for improved communications technology
ICT use higher rate than we can cope with
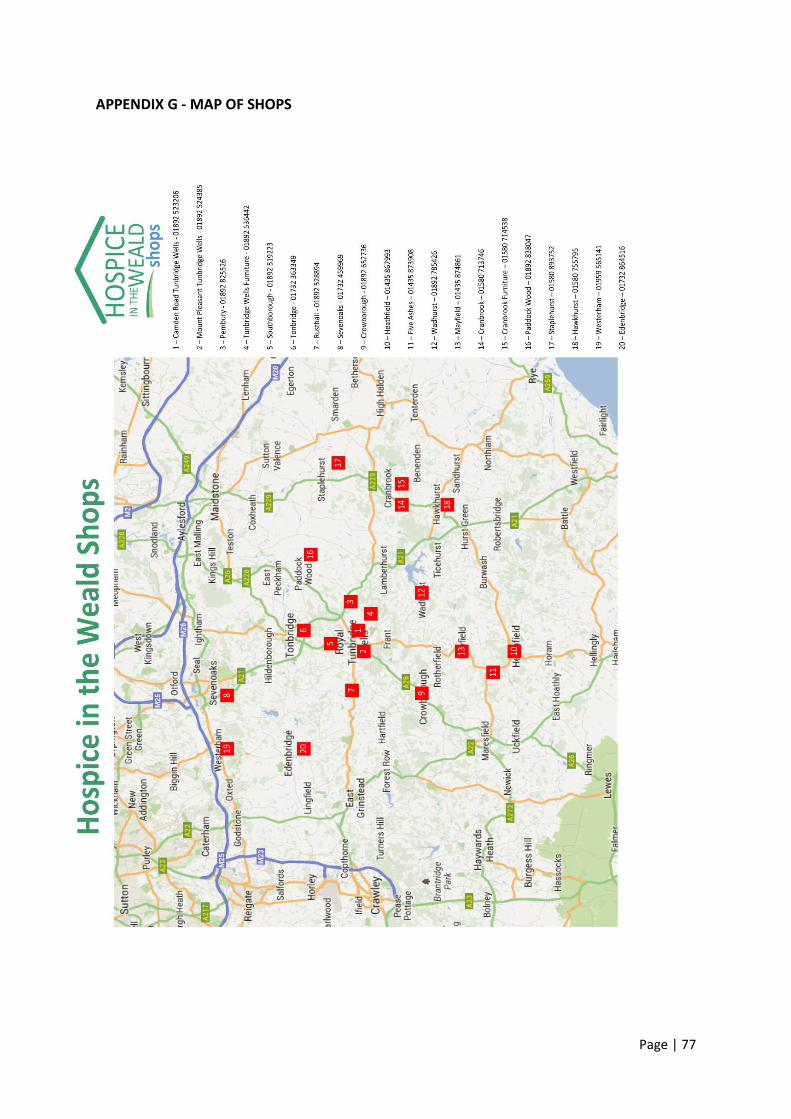
Page | 77
APPENDIX G - MAP OF SHOPS

Page | 78
APPENDIX H - SYNOPSIS
The Business Plan is to deliver: 1. Increase Hospice Palliative Care referrals from circa 1100 a year (2013/14 figures) to
1600 by 2017 (p19). 2. An easily accessible, clear and accurate account of the quality as well as the quantity, of
clinical work that we do in all settings (p20). 3. Improved access to Hospice Palliative Care for patients with non-malignant diseases
(p24). 4. Bereavement counselling for more people in West Kent (p23). 5. Increased income from our fundraising efforts to ensure sustainability (p46).
Enabled by: 6. Improved monitoring of quality of care (p20). 7. Embedding evidence-based practices in all clinical areas (p23). 8. Increasing the attendance numbers of Hospice Day Service patients from 20 to 30 a day
(p29). 9. Making Hospice in the Weald the provider of choice in the local area for palliative care
training, and other training under we:train (p34). 10. Implementing ICT systems which support mobile working (p38). 11. Doubling the number of Hospice supporters and funders to 80,000 (p43). 12. A ‘coaching’ culture amongst the Hospice workforce (staff and volunteers) (p49).
Supported by: 13. Concentrating our services on the patients with the greatest need of our expertise (p20). 14. Closer Partnership working with other agencies/organisations (p23 & p29). 15. Increasing Loyalty Card holders to 10,000 (p33). 16. A new purchase ordering system (p36). 17. Integrated Hospice databases (p38). 18. A redeveloped website (p45). 19. Increased volunteer recruitment (p49).
While reviewing: 20. 24/7 working across all Hospice Palliative Care services (p19). 21. Methods of closer working with local hospital and care homes (p19). 22. How patients who are not in need of continued In-Patient Hospice Palliative Care are
cared for through Continuing Health Care funding (p27). 23. The payments received for patients with Lymphoedema but without specialist palliative
care needs (p30). 24. Use of multi-function shops (p34). 25. Banking facilities (p37). 26. Systems to provide direct access by patients (p39). 27. The high rate of staff turnover (p49). 28. The income levels from the supply of catering (p50).

CONTACTS Page 79
Hospice in the Weald Maidstone Road
Pembury Tunbridge Wells
Kent TN2 4TA
Switchboard: 01892 820500
www.hospiceintheweald.org.uk
Registered Charity No. 280276 Registered in England No. 1499846