Burns & Poisoning
20
Burns Definition A burn is a type of injury to the skin caused by heat, electricity, chemicals, light, radiation or friction. Most burns only affect the skin ( epidermal tissue and dermis). Rarely deeper tissues, such as muscle, bone, and blood vessels can also be injured. Managing burns is important because they are common, painful and can result in disfiguring and disabling scarring. Burns can be complicated by shock, infection, multip le organ dysf unc ti on syndrome, elec troly te imba lance and respiratory distress. Large burns can be fatal, but modern treatments, developed in the last 60 years, have si gnif icantl y improved the prognosi s of such burns, especially in children and young adults. Causes 1. Dry hea t o This is the most common type of burn and includes burns cause by hot objects such as exhaust or cigarettes or lighters. Wet heat/ Scalding Scalding is caused by hot liquids (water or oil) or gases (steam), most commonly occurring from exposure to high temperature tap water in baths or showers or spill ed hot drinks. A so called immersion burn is created when an extremity is held under the surface of hot water, and is a common form of burn seen in child abuse. A blister is a "bubble" in the skin filled with serous fluid as part of the body's reaction to the heat and nerve damage. The blister "roof" is dead. Steam is a common gas that causes scalds. The injury is usually regional and usually does not cause death. More damage can be caused if hot liquids enter an orifice. However, deaths have occurred in more unusual circumstances, such as when people have accidentally broken a steam pipe. The demographics that are of the highest risk to suffering from scalding are young children, with their delicate skin, and the elderly over 65 years of age. 2. Fri cti on o When two objects rub together very quickly friction generates heat, causing another kind of dry burn. 3. Chemical burns o Most chemicals that cause severe chemical burns are strong acids or bases. ] Chemical burns can be caused by caustic chemical compounds such as sodium hydroxide or silver nitrate, and acids such as sulfuric acid. Hydrofluoric acid can cause damage down to the bone and its burns are sometimes not immediately evident. 1
-
Upload
francis-caster-matutes -
Category
Documents
-
view
219 -
download
0
Transcript of Burns & Poisoning

8/3/2019 Burns & Poisoning
http://slidepdf.com/reader/full/burns-poisoning 1/19
Burns
Definition
A burn is a type of injury to the skin caused by heat, electricity, chemicals,
light, radiation or friction. Most burns only affect the skin (epidermal tissue and
dermis). Rarely deeper tissues, such as muscle, bone, and blood vessels can also be
injured. Managing burns is important because they are common, painful and can
result in disfiguring and disabling scarring. Burns can be complicated by shock,
infection, multiple organ dysfunction syndrome, electrolyte imbalance and
respiratory distress. Large burns can be fatal, but modern treatments, developed in
the last 60 years, have significantly improved the prognosis of such burns,
especially in children and young adults.
Causes
1. Dry heat
o This is the most common type of burn and includes burns cause by hot
objects such as exhaust or cigarettes or lighters.
Wet heat/ Scalding
Scalding is caused by hot liquids (water or oil) or gases (steam), most
commonly occurring from exposure to high temperature tap water in baths
or showers or spilled hot drinks. A so called immersion burn is created when
an extremity is held under the surface of hot water, and is a common form of
burn seen in child abuse. A blister is a "bubble" in the skin filled with
serous fluid as part of the body's reaction to the heat and nerve damage.
The blister "roof" is dead. Steam is a common gas that causes scalds. The
injury is usually regional and usually does not cause death. More damage can
be caused if hot liquids enter an orifice. However, deaths have occurred in
more unusual circumstances, such as when people have accidentally broken
a steam pipe. The demographics that are of the highest risk to suffering from
scalding are young children, with their delicate skin, and the elderly over 65years of age.
2. Friction
o When two objects rub together very quickly friction generates heat,
causing another kind of dry burn.
3. Chemical burns
o Most chemicals that cause severe chemical burns are strong acids or
bases.]Chemical burns can be caused by caustic chemical compounds
such as sodium hydroxide or silver nitrate, and acids such as sulfuric
acid. Hydrofluoric acid can cause damage down to the bone and its
burns are sometimes not immediately evident.
1

8/3/2019 Burns & Poisoning
http://slidepdf.com/reader/full/burns-poisoning 2/19
4. Electrical burns
o Electrical burns are caused by either an exogenous electric shock
or an uncontrolled short circuit . (A burn from a hot, electrified
heating element is not considered an electrical burn.) Common
occurrences of electrical burns include workplace injuries, or being
defibrillated or cardioverted without a conductive gel. Lightning is also
a rare cause of electrical burns. Since normal physiology involves avast number of applications of electrical forces, ranging from
neuromuscular signaling to coordination of wound healing, biological
systems are very vulnerable to application of supraphysiologic electric
fields. Some electrocutions produce no external burns at all, as very
little current is required to cause fibrillation of the heart muscle.
Therefore, even when the injury does not involve any visible tissue
damage, electrical shock survivors may experience significant internal
injury. The internal injuries sustained may be disproportionate to the
size of the burns seen (if any), and the extent of the damage is not
always obvious. Such injuries may lead to cardiac arrhythmias, cardiac
arrest, and unexpected falls with resultant fractures.
5. Radiation burns
o Radiation burns are caused by protracted exposure to UV light (as
from the sun), tanning booths , radiation therapy (as patients
who are undergoing cancer therapy), sunlamps, radioactive
fallout , and X-rays. By far the most common burn associated with
radiation is sun exposure, specifically two wavelengths of light UVA,
and UVB, the latter being more dangerous. Tanning booths also emit
these wavelengths and may cause similar damage to the skin such as
irritation, redness, swelling, and inflammation. More severe cases of
sun burn result in what is known as sun poisoning. Microwave burns
are caused by the thermal effects of microwave radiation.
Effects/ Local or Systemic Responses to burn
I. Cardiovascular Response
Hypovolemia is the immediate consequence of fluid loss resulting in
decreased perfusion and oxygen delivery.
2
8/3/2019 Burns & Poisoning
http://slidepdf.com/reader/full/burns-poisoning 3/19
Cardiac output decreases before any significant change in blood volume is
evident.
As fluid loss continues and vascular volume decreases, cardiac output
continues to fall and blood pressure drops. This is the onset of burn shock.
In response, the sympathetic nervous system releases catecholamines,resulting in an increase in peripheral resistance (vasoconstriction) and an
increase in pulse rate. Peripheral vasoconstriction further decreases
cardiac output.
Myocardial contractility may be suppressed by the release of
inflammatory cytokine necrosis factor.
II. Burn Edema
o Edema is defined as the presence of excessive fluid in the tissuespaces.
Patients with more severe burns develop massive systemic edema. Edema is
usually maximal after 24 hours. It begins to resolve 1 to 2 days post-burn and
usually is completely resolved in 7 to 10 days post-injury.
Edema in burn wounds can be reduced by avoiding excessive fluid during
the early post-burn period. Unnecessary over-resuscitation will increase
edema formation in both burn tissue and non-burn tissue.
As edema increases in circumferential burns, pressure on small blood vesselsand nerves in the distal extremities causes an obstruction of blood flow and
consequent ischemia. This complication is known as compartment syndrome.
The physician may need to perform an escharotomy, a surgical incision into
the eschar (devitalized tissue resulting from a burn), to relieve the
constricting effect of the burned tissue
III. Effects on Fluids, Electrolytes, and Blood Volume
Circulating blood volume decreases dramatically during burn shock.
In addition, evaporative fluid loss through the burn wound may reach 3 to 5 L
or more over a 24-hour period until the burn surfaces are covered.
Usually hyponatremia (sodium depletion) is present. Immediately after burn
injury, hyperkalemia (excessive potassium) results from massive cell
destruction. Hypokalemia (potassium depletion) may occur later with fluid
shifts and inadequate potassium replacement.
At the time of burn injury, some red blood cells may be destroyed and others
damaged, resulting in anemia.
The hematocrit may be elevated due to plasma loss.
Abnormalities in coagulation, including a decrease in platelets
(thrombocytopenia) and prolonged clotting and prothrombin times, also occur
with burn injury.
3

8/3/2019 Burns & Poisoning
http://slidepdf.com/reader/full/burns-poisoning 4/19
IV. Pulmonary Response
Inhalation injury is the leading cause of death in fire victims. Inhalation injury
has a significant impact on survivability of a burn patient. Deterioration in
severely burned patients can occur without evidence of a smoke inhalation
injury.
Bronchoconstriction caused by release of histamine, serotonin, and
thromboxane, a powerful vasoconstrictor, as well as chest constriction
secondary to circumferential full-thickness chest burns causes deterioration.
Even without pulmonary injury, hypoxia (oxygen starvation) may be present.
More than half of all burn victims with pulmonary involvement do not initially
demonstrate pulmonary signs and symptoms. Any patient with possible
inhalation injury must be observed for at least 24 hours for respiratory
complications. Airway obstruction may occur very rapidly or develop in hours.
Decreased lung compliance, decreased arterial oxygen levels, and
respiratory acidosis may occur gradually over the first 5 days after a burn.
Indicators of possible pulmonary damage include the following:
o History indicating that the burn occurred in an enclosed area
o Burns of the face or neck
o Singed nasal hair
o Hoarseness, voice change, dry cough, stridor, sooty sputum
o Bloody sputum
o Labored breathing or tachypnea (rapid breathing) and other signs of
reduced oxygen levels (hypoxemia)
o Erythema and blistering of the oral or pharyngeal mucosa
V. Other Systemic Responses
Destruction of red blood cells at the injury site results in free hemoglobin in
the urine.
The immunologic defenses of the body are greatly altered by burn injury.
Serious burn injury diminishes resistance to infection. As a result, sepsis
remains the leading cause of death in thermally injured patients.
Loss of skin also results in an inability to regulate body temperature. Burn
patients may therefore exhibit low body temperatures in the early hours after
injury.
Two potential gastrointestinal complications may occur: paralytic ileus
(absence of intestinal peristalsis) and Curling’s ulcer.
Classifications
4
8/3/2019 Burns & Poisoning
http://slidepdf.com/reader/full/burns-poisoning 5/19
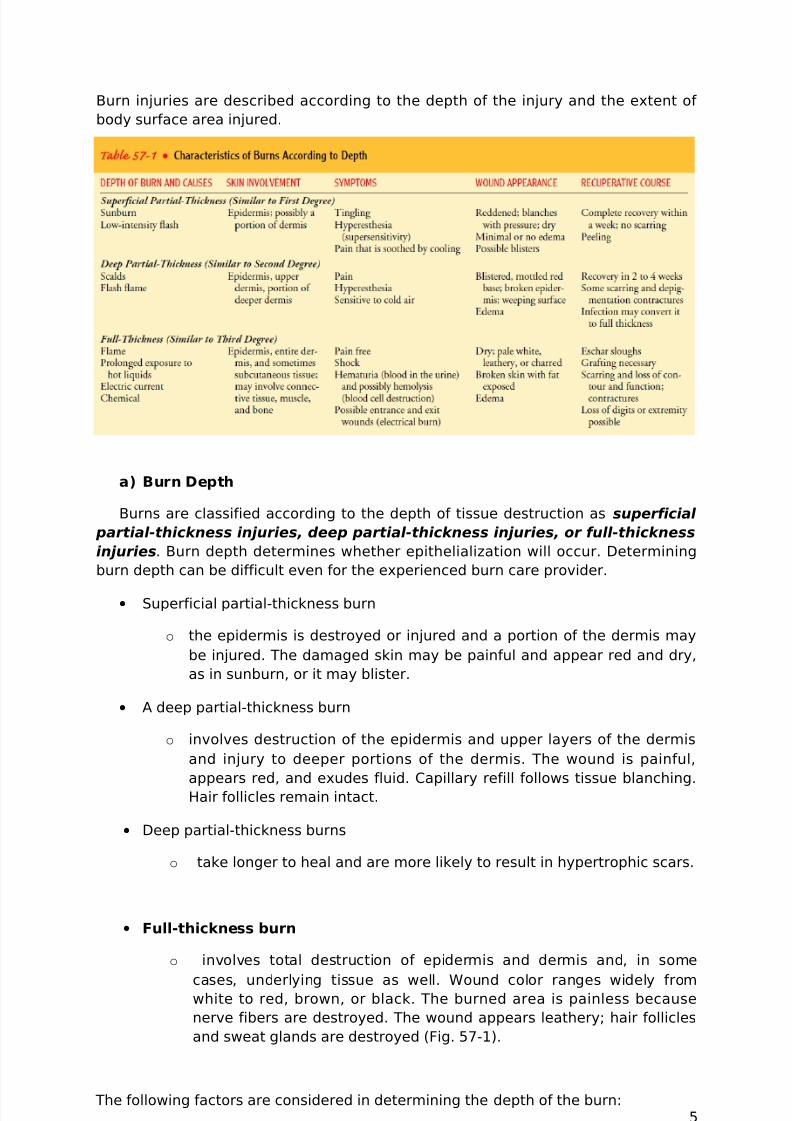
Burn injuries are described according to the depth of the injury and the extent of
body surface area injured.
a) Burn Depth
Burns are classified according to the depth of tissue destruction as superficial
partial-thickness injuries, deep partial-thickness injuries, or full-thickness
injuries. Burn depth determines whether epithelialization will occur. Determining
burn depth can be difficult even for the experienced burn care provider.
• Superficial partial-thickness burn
o the epidermis is destroyed or injured and a portion of the dermis may
be injured. The damaged skin may be painful and appear red and dry,
as in sunburn, or it may blister.
• A deep partial-thickness burn
o involves destruction of the epidermis and upper layers of the dermis
and injury to deeper portions of the dermis. The wound is painful,
appears red, and exudes fluid. Capillary refill follows tissue blanching.Hair follicles remain intact.
• Deep partial-thickness burns
o take longer to heal and are more likely to result in hypertrophic scars.
• Full-thickness burn
o involves total destruction of epidermis and dermis and, in some
cases, underlying tissue as well. Wound color ranges widely fromwhite to red, brown, or black. The burned area is painless because
nerve fibers are destroyed. The wound appears leathery; hair follicles
and sweat glands are destroyed (Fig. 57-1).
The following factors are considered in determining the depth of the burn:5

8/3/2019 Burns & Poisoning
http://slidepdf.com/reader/full/burns-poisoning 6/19
• How the injury occurred
• Causative agent, such as flame or scalding liquid
• Temperature of the burning agent
• Duration of contact with the agent
• Thickness of the skin
A number of different classification systems exist. The traditional system divided
burns in first-, second-, or third-degree.
By degree
Three degrees of burns
First-degree burns are usually limited to redness (erythema), a white plaque
and minor pain at the site of injury. These burns involve only the epidermis. Most
sunburns can be included as first-degree burns.
Second-degree burns manifest as erythema with superficial blistering of the
skin, and can involve more or less pain depending on the level of nerve
involvement. Second-degree burns involve the superficial (papillary) dermis and
may also involve the deep (reticular) dermis layer. Deep dermal burns usually take
more than three weeks to heal and should be seen by a surgeon familiar with burn
care, as in some cases severe hypertrophic scarring can result. Burns that require
more than three weeks to heal are often excised and skin grafted for best result.
Third-degree burns occur when the epidermis is lost with damage to the
subcutaneous tissue. Burn victims will exhibit charring and extreme damage of the
epidermis, and sometimes hard eschar will be present. Third-degree burns result in
scarring and victims will also exhibit the loss of hair shafts and keratin. These burns
may require grafting. These burns are not painful, as all the nerves have been
damaged by the burn and are not sending pain signals; however, all third-degree
burns are surrounded by first and second-degree burns.
b) Extent of Body Surface Area Injured
Various methods are used to estimate the TBSA affected by burns among them are
the rule of nines, the Lund and Browder method, and the palm method.
RULE OF NINES
The rule of nines is a quick way to calculate the extent of
burns. The system assigns percentages
in multiples of nine to major body surfaces.
FIGURE 57-2 The rule of nines: Estimated percentage of
total body surface area (TBSA) in the adult is arrived at by
sectioning the body surface into areas with a numerical value
6

8/3/2019 Burns & Poisoning
http://slidepdf.com/reader/full/burns-poisoning 7/19
related to nine. (Note: The anterior and posterior head total 9% of TBSA.) In burn
victims, the total estimated percentage of TBSA injured is used to calculate the
patient’s fluid replacement needs.
LUND AND BROWDER METHOD
A more precise method of estimating the extent of a burn which recognizes that the
percentage of TBSA of various anatomic parts, especially the head and legs, and
changes with growth is by dividing the body into very small areas and providing an
estimate of the proportion of TBSA accounted for by such body parts, one can
obtain a reliable estimate of the TBSA burned. The initial evaluation is made on the
patient’s arrival at the hospital and is revised on the second and third post-burn
days because the demarcation usually is not clear until then.
PALM METHOD
In patients with scattered burns, a method to estimate the percentage of burn is the
palm method. The size of the patient’s palm is approximately 1% of TBSA.
Prevention
Don’t play with fire.
Avoid octopus connection.
Be cautious in handling hot objects and chemicals.
Use appropriate protective devices when handling hot objects.
Keep flammable objects from children’s reach.
Hold the rubber part of the wire in plugging or unplugging the socket.
Avoid prolonged exposure to sunlight and UV rays.
Use sunblocks and SPF creams and powders to protect your skin.
Store chemicals in appropriate containers.
Escape and rescue (On-the-Scene Care)
The first priority of on-the-scene care for a burn victim is to prevent injury to
the rescuer. If needed, fire and emergency medical services should be
requested at the first opportunity.
AIRWAY, BREATHING, CIRCULATION
o Although the local effects of a burn are the most evident, the systemic
effects pose a greater threat to life. Therefore, it is important toremember the ABCs of all trauma care during the early postburn
period:
Airway
Breathing
7
8/3/2019 Burns & Poisoning
http://slidepdf.com/reader/full/burns-poisoning 8/19
Circulation; cervical spine immobilization for patients with high-
voltage electrical injuries and if indicated for other injuries;
cardiac monitoring for patients with all electrical injuries for at
least 24 hours after cessation of dysrhythmia
Some practitioners include “DEF” in the trauma assessment:disability, exposure, and fluid resuscitation.
The circulatory system must also be assessed quickly.
o Apical pulse and blood pressure are monitored frequently. Tachycardia
(abnormally rapid heart rate) and slight hypotension are expected
soon after the burn.
The neurologic status is assessed quickly in the patient with extensive burns.
Often the burn patient is awake and alert initially, and vital information can
be obtained at that time.
A secondary head-to-toe survey of the patient is carried out to identify other
potentially life-threatening injuries.
Preventing shock in a burn patient is imperative.
NURSING ALERT No food or fluid is given by mouth and the patient is placed in a
position that will prevent aspiration of vomitus because nausea and vomiting
typically occur due to paralytic
ileus resulting from the stress of injury. Usually, rescue workers will cool the wound,
establish an airway, supply oxygen, and insert at least one large-bore intravenous
line.
Emergency Procedures at the Burn Scene
• Extinguish the flames. When clothes catch fire, the flames can be extinguished
if the victim falls to the floor or ground and rolls (“drop and roll”); anything available
to smother the flames, such as a blanket, rug, or coat, may be used. Standing still
forces the victim to breathe flames and smoke, and running fans the flames. If the
burn source is electrical, the electrical source must be disconnected.
• Cool the burn. After the flames are extinguished, the burned area and adherent
clothing are soaked with cool water, briefly, to cool the wound and halt the burning
process. Once a burn has been sustained, the application of cool water is the best
first-aid measure. Soaking the burn area intermittently in cool water or applying
cool towels gives immediate and striking relief from pain and limits local tissue
edema and damage. However, never apply ice directly to the burn, never wrap burn
victims in ice, and never use cold soaks or dressings for longer than several
minutes; such procedures may worsen the tissue damage and lead to hypothermiain patients with large burns.
• Remove restrictive objects. If possible, remove clothing immediately. Adherent
clothing may be left in place once cooled. Other clothing and all jewelry should be
removed to allow for assessment and to prevent constriction secondary to rapidly
developing edema.
8
8/3/2019 Burns & Poisoning
http://slidepdf.com/reader/full/burns-poisoning 9/19
• Cover the wound. The burn should be covered as quickly as possible to
minimize bacterial contamination and decrease pain by preventing air from coming
into contact with the injured surface. Sterile dressings are best, but any clean, dry
cloth can be used as an emergency dressing. Ointments and salves should not be
used. Other than the dressing, no medication or material should be applied to the
burn wound.
• Irrigate chemical burns. Chemical burns resulting from contact with a corrosive
material are irrigated immediately. Most chemical laboratories have a high-pressure
shower for such emergencies. If such an injury occurs at home, brush off the
chemical agent, remove clothes immediately, and rinse all areas of the body that
have come in contact with the chemical. Rinsing can occur in the shower or any
other source of continuous running water. If a chemical gets in or near the eyes, the
eyes should be flushed with cool, clean water immediately. Outcomes for the
patient with chemical burns are significantly improved by rapid, sustained flushing
of the injury at the scene.
Emergency Medical Management
The patient is transported to the nearest emergency department.
The hospital and physician are alerted that the patientis en route to the
emergency department so that life-saving measures can be initiated
immediately by a trained team.
Initial priorities in the emergency department remain airway, breathing, and
circulation.
For mild pulmonary injury, inspired air is humidified and the patient is
encouraged to cough so that secretions can be removed by suctioning. For
more severe situations, it is necessary to remove secretions by bronchial
suctioning and to administer bronchodilators and mucolytic agents. If edema
of the airway develops, endotracheal intubation may be necessary.
Continuous positive airway pressure and mechanical ventilation may also be
required to achieve adequate oxygenation.
After adequate respiratory status and circulatory status have beenestablished, the patient is assessed for cervical spinal injuries or head injury
if the patient was involved in an explosion, a fall, a jump, or an electrical
injury.
Once the patient’s condition is stable, attention is directed to the burn wound
itself. All clothing and jewelry are removed. For chemical burns, flushing of
the exposed areas is continued. The patient is checked for contact lenses.
These are removed immediately if chemicals have contacted the eyes or if
facial burns have occurred.
It is important to validate an account of the burn scenario provided by thepatient, witnesses at the scene, and paramedics. Information needs to
include time of the burn injury, source of the burn, place where the burn
occurred, how the burn was treated at the scene, and any history of falling
with the injury.
9
8/3/2019 Burns & Poisoning
http://slidepdf.com/reader/full/burns-poisoning 10/19
A history of preexisting diseases, allergies, and medications and the use of
drugs, alcohol, and tobacco is obtained at this point to plan care.
The physician evaluates the patient’s general condition, assesses the burn,
determines the priorities of care, and directs the individualized plan of
treatment, which is divided into systemic management and local care of theburned area. Nonsterile gloves, caps, and gowns are worn by personnel while
assessing the exposed burned areas. Clean technique is maintained while
assessing burn wounds.
Assessment of both the TBSA burned and the depth of the burn is completed
after soot and debris have been gently cleansed from the burn wound.
Careful attention is paid to keeping the burn patient warm during wound
assessment and cleansing. Assessment is repeated frequently throughout
burn wound care.
Photographs may be taken of the burn areas initially and periodicallythroughout treatment; in this way, the initial injury and burn wound can be
documented. Such documentation is invaluable for insurance and legal
claims.
Clean sheets are placed under and over the patient to protect the area from
contamination, maintain body temperature, and reduce pain caused by air
currents passing over exposed nerve endings.
An indwelling urinary catheter is inserted to permit more accurate monitoring
of urine output and renal function for patients with moderate to severe burns.
Baseline height, weight, arterial blood gases, hematocrit, electrolyte values,
blood alcohol level, drug panel, urinalysis, and chest x-rays are obtained.
If the patient is elderly or has an electrical burn, a baseline electrocardiogram
is obtained. Because burns are contaminated wounds, tetanus prophylaxis is
administered if the patient’s immunization status is not current or is
unknown.
Although the major focus of care during the emergent phase is physical
stabilization, the nurse must also attend to the patient’s and family’s
psychological needs. Burn injury is a crisis, causing variable emotionalresponses.
The patient’s and family’s coping abilities and available supports are
assessed. Circumstances surrounding the burn injury should be considered
when providing care. Individualized psychosocial support must be given to
the patient and family. Because the emergent burn patient is usually anxious
and in pain, those in attendance should provide reassurance and support,
explanations of procedures, and adequate pain relief.
Because poor tissue perfusion accompanies burn injuries only intravenous
pain medication (usually morphine) is given, titrated for the patient.
If the patient wishes to see a spiritual advisor, one is notified.
10

8/3/2019 Burns & Poisoning
http://slidepdf.com/reader/full/burns-poisoning 11/19
MANAGEMENT OF FLUID LOSS AND SHOCK
Next to handling respiratory difficulties, the most urgent need is preventing
irreversible shock by replacing lost fluids and electrolytes.
Intravenous lines and an indwelling catheter must be in place before
implementing fluid resuscitation.
Baseline weight and laboratory test results are obtained as well. These
parameters must be monitored closely in the immediate post-burn
(resuscitation) period.
Controversy continues regarding the definition of adequate resuscitation and
the optimal fluid type for resuscitation. Refinement of resuscitation
techniques remains an active area of burn research.
Fluid Replacement Therapy.
The total volume and rate of intravenous fluid replacement are gauged by the
patient’s response.
The adequacy of fluid resuscitation is determined by following urine outputtotals, an index of renal perfusion. Output totals of 30 to 50 mL/hour have
been used as goals. Other indicators of adequate fluid replacement are a
systolic blood pressure exceeding 100 mm Hg and/or a pulse rate less than
110/minute.
NURSING ALERT Clinical parameters are far more important in resuscitation than
any formula. Indeed, the patient’s individual response is the key to assessing the
adequacy of fluid resuscitation.
Additional gauges of fluid requirements and response to fluid resuscitation
include hematocrit and hemoglobin and serum sodium levels. If the
hematocrit and the hemoglobin levels decrease or if the urinary output
exceeds 50 mL/hour, the rate of intravenous fluid administration may be
decreased. The goal is to maintain serum sodium levels in the normal range
during fluid replacement.
Appropriate resuscitation endpoints for burn patients remain controversial.
Fluid Requirements.
11

8/3/2019 Burns & Poisoning
http://slidepdf.com/reader/full/burns-poisoning 12/19
The projected fluid requirements for the first 24 hours are calculated by the
clinician based on the extent of the burn injury. Some combination of fluid
categories may be used: colloids (whole blood, plasma, and plasma
expanders) and crystalloids/electrolytes (physiologic sodium chloride or
lactated Ringer’s solution).
Adequate fluid resuscitation results in slightly decreased blood volume levels
during the first 24 post-burn hours and restores plasma levels to normal by
the end of 48 hours.
Chemical burns of the eye
Treatment in chemical burns:
1. If you feel that you can safely approach the victim then do so carefully.
2. If necessary, wear protective clothing to protect yourself from contamination.
3. Ventilate the room if possible because many chemicals affect breathing.
4. When cooling the burn with water, ensure that the contaminated water drains
away from both the victim and yourself. It may be necessary to flood the
injured part for longer to ensure that the chemical is totally washed away.
This may take more than 20 minutes.
5. Call emergency hotline. Make sure you have mentioned that it is a chemical
burn so that additional help can be sent for if necessary and so that any
antidotes can be sent with the ambulance.
6. If possible, remove contaminated clothes from the victim because these may
keep burning, but only do this if you can do it without contaminating yourself
or causing the victim more harm.
7. Cover the burn with a clean, non-fluffy material as appropriate and tie loosely
in place if necessary.
8. Treat the shock and reassure the victim until emergency help arrives on the
scene.
Treatment in chemical burns in the eye:
1. Protect yourself, the victim, and bystanders from further contamination.
2. Hold the affected eye under cold running water for at least 10 minutes to
flush out the chemical, allowing the injured person to blink periodically. You
may need to hold the eyelid open. Make sure that the water flow is gentle. Do
not allow contaminated water to fall across the good eye and so contaminate
that eye also.
3. Ask the injured person to hold a non-fluffy sterile or clean pad across the eye,
ting it in place if hospital treatment may be delayed.
4. Take or send the person to hospital with details of the chemical if possible.
12
8/3/2019 Burns & Poisoning
http://slidepdf.com/reader/full/burns-poisoning 13/19
Poisoning
• Toxicology - study of the harmful effect of various substances on the body.
• Poison - comes from the Latin word - potare - meaning to drink.
- A poison is any substance that, when ingested, inhaled, absorbed,
applied to the skin, or produced within the body in relatively small
amounts, injures the body by its chemical action. Emergency
treatment is initiated with the following goals:
• To remove or inactivate the poison before it is absorbed
• To provide supportive care in maintaining vital organ systems
• To administer a specific antidote to neutralize a specific poison
• To implement treatment that hastens the elimination of the
absorbed poison
I. TYPES OF POISON:
1. Ingested Poisons
– are poisons that are swallowed. They may be accidental or
intentional.
They can produce:
Immediate effects – poison is caustic to the body tissues (i.e.,strong acid/alkali).
e.g. Alkaline products - toilet bowl cleaners, bleach,
nonphosphate detergents, and button batteries (batteries used to
power watches, calculators, or cameras).
Acid products – toilet bowl cleaners, pool cleaners, metal
cleaners, rust removers, battery acid.
Delayed effects – poison must be absorbed into the
bloodstream before they become harmful.
e.g.
a. Foods carrying bacteria that cause food
poisoning.
Suspect food poisoning if:
1. The victim ate food that "didn't taste right" or that
may have been old, improperly prepared,
contaminated, left at room temperature for a long
time, or processed with an excessive amount of
chemicals.
2. Several people who ate together become ill.
b. Prescription drugs taken as deliberate or
accidental overdose.
c. Alcohol in excess
13

8/3/2019 Burns & Poisoning
http://slidepdf.com/reader/full/burns-poisoning 14/19
d. Plants eaten deliberately when seeking an
effect, or by accident
2. Inhaled Poisons: Carbon Monoxide Poisoning
– carbon monoxide poisoning may occur as a result of industrial
or household incidents or attempted suicide.
- It is implicated in more deaths than any other toxin except alcohol.
- CO exerts its toxic effect by binding to circulating hemoglobin and
thereby reducing the oxygen-carrying capacity of the blood.
Hemoglobin absorbs carbon monoxide 200 times more readily than
it absorbs oxygen. Carbon monoxide–bound hemoglobin, calledcarboxyhemoglobin, does not transport oxygen.
3. Contact Poisons
– skin contamination poisoning/chemical burns are challenging
because of the large number of offending agents with diverse actions
and metabolic effects. The severity of a chemical burn is determined
by:
the mechanism of action,
penetrating strength and concentration, and the amount and duration of exposure of the skin to
the chemical.
4. Injected Poisons
– poisons that enters the body through a bite, sting, or syringe.
e.g.
a. Prescription drugs taken as a deliberate or
accidental overdose
b. Illegal drugs
c. Insect bite or stings
II. SIGNS AND SYMPTOMS:
1. Ingested Poison
Alteredmental status
History of ingestingpoisons
Burnsaround themouth
Odd breathodors
Nausea &vomiting
Abdominalpain
Diarrhea
14
8/3/2019 Burns & Poisoning
http://slidepdf.com/reader/full/burns-poisoning 15/19
2. Inhaled Poison
History of
inhaling poisons
Breathing
difficulty
Chest pain
Cough,hoarseness,burningsensation in thethroat
Cyanosis (bluishdiscoloration of skin andmucousmembranes)
Dizziness,headache
Seizures,
unresponsivene
ss (advanced
stages)
3. Contact Poison
History of exposures
Liquid orpowder on theskin
Burns
Itching,irritation
Redness,
rashes, blisters
4. Injected Poison
i. Bee sting
Signs and Symptoms
• Stingers may
be present.
• Pain
• Swelling
• Possible
allergicreaction
ii. Spider bite
Signs and Symptoms
•
Nite mark• Swelling
• Pain
• Nausea and
vomiting
• Difficulty
breathing or
swallowing.
iii. Marine Organisms
Signs and Symptoms
• Possible
marks.
• Pain
• Swelling
• Possible
allergic
reaction.
iv. Snake bite
Signs and Symptoms
• Bite mark
• Pain
Comparative Characteristics of Snake
CHARACTERISTIC VENOMOUS NON-VENOMOUS
Movement Cortina, side locomotion winding Semicortina curvature
Head Semi-angular Oblongated
Body Rectangular Circular
Skin Rough Smooth
Pupil Vertical Round
15
8/3/2019 Burns & Poisoning
http://slidepdf.com/reader/full/burns-poisoning 16/19
Ways/ manner of attack Nonconstrictor Constrictor
Bite marks With fang marks Horeshoe shape
v. Dog bite
Signs and Symptoms
• Bite mark
• Bleeding
III. ANTIDOTE
Antidotes prevent the poison from working or reverse the effects of the poison.
The antidotes for some particular toxins are manufactured by injecting thetoxin into an animal in small doses and extracting the resulting antibodies fromthe host animals' blood. This results in an antivenom that can be used tocounteract poison produced by certain species of snakes, spiders, and othervenomous animals. A number of venoms lack a viable antivenom, and a bite orsting from an animal producing such a toxin often results in death. Some animalvenoms, especially those produced by arthropods (e.g. certain spiders,scorpions, bees, etc.) are only potentially lethal when they provoke allergicreactions and induce anaphylactic shock; as such, there is no "antidote" forthese venoms because it is not a form of poisoning and anaphylactic shock canbe treated (e.g., by the use of epinephrine).
• Atropine is an antidote for certain nerve gases and insecticides.
• N-acetylcysteine (Mucomyst) is used to neutralize acetaminophen (Tylenol) overdoses. Acetaminophen, in normal doses, is one of the safestmedications known, but after a massive overdose, the liver is damaged, andhepatitis and liver failure develop. Mucomyst works as an antidote bybolstering the body's natural detoxification abilities when they areoverwhelmed.
• It may also be possible to reverse the harmful effect of a drug even if noantidote exists.
o If a person with diabetes takes too much insulin, a dangerously low blood sugar (hypoglycemia) will cause weakness, unconsciousness,
and eventually death. Sugar given by mouth or IV is an effectivetreatment until the insulin wears off.
o When the poison is a heavy metal, such as lead, special medicines(chelators) bind the poison in the bloodstream and cause it to beeliminated in the urine.
o Another "binder" is sodium polystyrene sulfonate (Kayexalate), whichcan absorb potassium and other electrolytes from the bloodstream.
• Once the poison has moved past the stomach, other methods are needed.
1. Activated charcoal acts as a "super" absorber of many poisons. Oncethe poison is stuck to the charcoal in the intestine, the poison cannotget absorbed into the bloodstream. Activated charcoal has no taste,but the gritty texture sometimes causes the person to vomit. To beeffective, activated charcoal needs to be given as soon as possibleafter the poisoning. It does not work with alcohol, caustics, lithium (Lithobid), or petroleum products.
16

8/3/2019 Burns & Poisoning
http://slidepdf.com/reader/full/burns-poisoning 17/19
2. Whole bowel irrigation requires drinking a large quantity of a fluidcalled Golytely. This flushes the entire gastrointestinal tract beforethe poison gets absorbed.
• Some other toxins have no known antidote. For example, the poisonaconitine, a highly poisonous alkaloid derived from various aconite specieshas no antidote, and as a result is often fatal if it enters the human body insufficient quantities.
IV. FIRST AID CARE/EMERGENCY
KEY FIRST AID PRINCIPLES FOR DEALING WITH POISONS
1. Protect yourself and bystanders from the source of the poison by making thescene safe and wearing protective clothing if necessary.
2. Monitor and maintain the victim’s airway and breathing and be prepared toresuscitate if necessary.
3. Seek appropriate medical help or call the Poison Control Hotline to deal withdangerous substances.
4. Monitor the victim’s level of consciousness and be prepared to turn intorecovery position if necessary.
5. Support the victim if he vomits and place in the recovery position untilmedical help arrives.
6. Treat any burns caused by corrosive poisons by flooding the affected areawith running water.
7. Try to identify the source of the poison because this will help determineappropriate medical treatment.
FIRST AID CARE
1. Ingested poisoning
Chemicals
a. Monitor and maintain the airway and breathing. Be prepared toresuscitate if necessary.
b. Monitor consciousness. If the person becomes unconscious, put into
the recovery position.
c. Call 911 or the Poison control Hotline for advice on how to proceed.
d. Treat any burns, wearing protective clothing if necessary.
e. Support the person if he vomits and place in the recovery position if necessary.
f. Reassure the person while you are waiting for emergency assistanceto arrive.
g. Identify the poison if possible because this will help medical staff determine what treatment is appropriate.
Food
a. Monitor and maintain the airway and breathing. If there arebreathing difficulties call 911.
17
8/3/2019 Burns & Poisoning
http://slidepdf.com/reader/full/burns-poisoning 18/19
b. Help the person into a comfortable position.
c. Call for medical advice on treatment and care.
d. Give plenty of fluids to drink, particularly if the person has vomitingand diarrhea.
e. Support the person if he/she vomits, providing a bowl and towel asnecessary.
Remember: Do not underestimate food poisoning, particularlyin the very young or in the elderly.
2. Inhaled poison
Where possible, remove the victim from the chemical. If this is notpossible, ensure that the area is well-ventilated (open doors and
windows). If in doubt, do not stay in the room yourself. Many chemicalshave no odor or obvious effect and you may not be aware that you arebeing poisoned.
a. Monitor and maintain the victim’s airway and breathingand be prepared to resuscitate if necessary.
b. If the victim becomes unconscious, place in recoveryposition.
c. If the victim is conscious help into the most comfortableposition. If there are breathing problems, this position ismost likely to be sitting up.
d. Call 911 and provide as much information as you can.
2. Injected poison
Bee Sting
1. Remove stinger.
2. Wash wound.
3. Cover the wound.
4. Apply a cold pack.
5. Watch for signals of allergicreaction
Spider Bite
1. Wash wound.
2. Apply a cold pack.
3. Get medical care to receive
antivenin.
4. Get local emergency number, if
necessary.
Marine Organisms
1. If jellyfish- soak area in vinegar
2. If sting ray- soak in nonscalding
hot water until pain goes away.
3. Clean and bandage the wound.
4. Call emergency number, if necessary.
Snake bite
1. Wash wound.
2. Keep bitten part still, and lower
than the heart.
3. Call local emergency number.
Dog bite
1. If bleeding is minor- wash wound.
2. Control bleeding.
3. Apply antibiotic ointment.
18
8/3/2019 Burns & Poisoning
http://slidepdf.com/reader/full/burns-poisoning 19/19
4. Cover the wound.
5. Get medical attention if wound bleeds severely or if you suspect animal has
rabies.
6. Call local emergency number or contact animal control personnel.
4. Contact poison1. Do not contaminate yourself. Wear protective clothingif available.
2. Wash away the chemical with water, taking care toflush the contaminated water away from both yourself and the victim.
3. Monitor and maintain the victim’s airway and breathing and be preparedto resuscitate if necessary.
4. Call 911 and reassure the victim until help arrives.
REFERENCES:
Books
Smeltzer, S.C & Bare (2008). Brunner & Suddarth’s Textbook of Medical Surgical Nursing11th Edition, Vol. 2, Philadelphia: Lippincott Williams & Wilkins.
Nettina, S (2001). The Lippincott Manual of Nursing Practice 7th Edition, Vol. 2, Philadelphia:Lippincott Williams & Wilkins.
Websites
http://www.emedicinehealth.com/poisoning/page9_em.htm
http://en.wikipedia.org/wiki/Burn
http://www.medicinenet.com/burns/article.htm
http://www.rcyofuplb.org/index.php/Basic-First-Aid/First-Aid-for-Poisoning.html
19








![Detecting Carbon Monoxide Poisoning Detecting Carbon ...2].pdf · Detecting Carbon Monoxide Poisoning Detecting Carbon Monoxide Poisoning. Detecting Carbon Monoxide Poisoning C arbon](https://static.fdocuments.in/doc/165x107/5f551747b859172cd56bb119/detecting-carbon-monoxide-poisoning-detecting-carbon-2pdf-detecting-carbon.jpg)