Burden of illness, metabolic control, and complications in relation to depressive symptoms in IDDM...
7
ORIGINAL ARTICLES Burden of Illness, Metabolic Control, and Complications in Relation to Depressive Symptoms in IDDM Patients B. Karlson* 1 , C.-D. Agardh 2 1 Department of Applied Psychology, Lund University, Lund, Sweden 2 Department of Internal Medicine, University Hospital, Lund, Sweden Relationships between demographic-, treatment-, and sickness-related factors, metabolic control (HbA 1c ), perceived burden of illness, and degree of depressive symptoms were examined in a group of 155 insulin-dependent diabetic patients, aged 35.3 ± 8.9 years. The patients completed a questionnaire measuring depressive symptoms and three aspects of perceived burden of illness. No gender differences in HbA 1c level or occurrence of late diabetic complications were found. Both men and women showed a modestly elevated degree of depression compared with norm groups. Self-reported burden of illness was strongly related to depression but was largely unrelated to objective disease-related measures. Level of depression was correlated neither with degree of metabolic control nor with the presence of such late diabetic complications as retinopathy and nephropathy. Some 44 % of the variance in depression could be explained by worries about complications in those patients with the lowest HbA 1c levels, by perceived restrictions in everyday life in patients with intermediate metabolic control, and by problems of glycaemic regulation in patients with poor metabolic control. Degree of depression was largely unrelated to disease severity, but was found to be related to the perceived daily burden of living with the disease, the specific worries and concerns associated with a depressed mood varying with degree of metabolic control. 1997 by John Wiley & Sons, Ltd. Diabet. Med. 14: 1066–1072 (1997) No of Figures: 1. No of Tables: 3. No of Refs: 20 KEY WORDS psychosocial adaptation; depression; disease perception; type 1 diabetes mellitus Received 29 July 1996; revised 9 April 1997; accepted 28 April 1997 since depression may be primary and be associated with Introduction decreased adherence to therapy, just as poor glycaemic Whereas patients with chronic disease have been found control and its associated malaise may render the generally to have an increased frequency of anxiety, individual more susceptible to psychiatric illness. 2,8 affective and other psychiatric disorders, 1,2 in patients Worries about glycaemic control and diabetic compli- with diabetes mellitus a depressed affect is more common. cations may be causally linked to a depressive state. 4 This may range from a depressed mood, 3 through a sub- Sanders et al. 11 found that fear for the future and fear of clinical depressive state, to a genuine clinical depression, severe hypoglycaemia were common sources of anxiety the latter having been reported to be more common and depression in diabetic patients. Connell et al. 12 also than in the general population. 2 The aetiology of found the perceived threat of diabetes to be related to depression in diabetes is not fully understood and depression. Although in the non-diabetic population is probably multifactorial. 4 The presence of chronic depression is reported to be more common in women, 13 complications in diabetes has been found to be associated this relationship has not always been found in patients with depression in some 5 but not all studies, 6–9 whereas with diabetes. 9 diabetes duration does not appear to be related. 4 In The aim of the present study was to examine relation- some studies, an association between poor metabolic ships between self-reported measures of the perceived control and depression has been obtained 8,10 but very burden of illness and the level of depressive symptoms, strict glycaemic control can also contribute to as well as relationships of both of these measures to depression. 4 A causal relationship between diabetes objective demographic-, treatment-, and sickness-related control and depression is difficult to establish, particularly factors, in patients with insulin-dependent (Type 1) diabetes mellitus (IDDM). We also set out to determine *Correspondence to: Bjo ¨ rn Karlson, Lund University, Department of the contribution of these various factors to depressive Applied Psychology, Paradisgatan 5, S-223 50 Lund, Sweden. symptoms in the patients studied. Sponsors: Malmo ¨ hus la ¨ns landstings utvecklingsfond 1066 CCC 0742–3071/97/141066–07$17.50 1997 by John Wiley & Sons, Ltd. DIABETIC MEDICINE, 1997; 14: 1066–1072
Transcript of Burden of illness, metabolic control, and complications in relation to depressive symptoms in IDDM...

ORIGINAL ARTICLES
Burden of Illness, Metabolic Control,and Complications in Relation toDepressive Symptoms in IDDM PatientsB. Karlson*1, C.-D. Agardh2
1Department of Applied Psychology, Lund University, Lund, Sweden2Department of Internal Medicine, University Hospital, Lund,Sweden
Relationships between demographic-, treatment-, and sickness-related factors, metaboliccontrol (HbA1c), perceived burden of illness, and degree of depressive symptoms wereexamined in a group of 155 insulin-dependent diabetic patients, aged 35.3 ± 8.9 years.The patients completed a questionnaire measuring depressive symptoms and three aspectsof perceived burden of illness. No gender differences in HbA1c level or occurrence of latediabetic complications were found. Both men and women showed a modestly elevateddegree of depression compared with norm groups. Self-reported burden of illness wasstrongly related to depression but was largely unrelated to objective disease-relatedmeasures. Level of depression was correlated neither with degree of metabolic controlnor with the presence of such late diabetic complications as retinopathy and nephropathy.Some 44 % of the variance in depression could be explained by worries about complicationsin those patients with the lowest HbA1c levels, by perceived restrictions in everyday lifein patients with intermediate metabolic control, and by problems of glycaemic regulationin patients with poor metabolic control. Degree of depression was largely unrelated todisease severity, but was found to be related to the perceived daily burden of living withthe disease, the specific worries and concerns associated with a depressed mood varyingwith degree of metabolic control. 1997 by John Wiley & Sons, Ltd.
Diabet. Med. 14: 1066–1072 (1997)
No of Figures: 1. No of Tables: 3. No of Refs: 20
KEY WORDS psychosocial adaptation; depression; disease perception; type 1 diabetesmellitus
Received 29 July 1996; revised 9 April 1997; accepted 28 April 1997
since depression may be primary and be associated withIntroductiondecreased adherence to therapy, just as poor glycaemic
Whereas patients with chronic disease have been found control and its associated malaise may render thegenerally to have an increased frequency of anxiety, individual more susceptible to psychiatric illness.2,8
affective and other psychiatric disorders,1,2 in patients Worries about glycaemic control and diabetic compli-with diabetes mellitus a depressed affect is more common. cations may be causally linked to a depressive state.4This may range from a depressed mood,3 through a sub- Sanders et al.11 found that fear for the future and fear ofclinical depressive state, to a genuine clinical depression, severe hypoglycaemia were common sources of anxietythe latter having been reported to be more common and depression in diabetic patients. Connell et al.12 alsothan in the general population.2 The aetiology of found the perceived threat of diabetes to be related todepression in diabetes is not fully understood and depression. Although in the non-diabetic populationis probably multifactorial.4 The presence of chronic depression is reported to be more common in women,13
complications in diabetes has been found to be associated this relationship has not always been found in patientswith depression in some5 but not all studies,6–9 whereas with diabetes.9diabetes duration does not appear to be related.4 In The aim of the present study was to examine relation-some studies, an association between poor metabolic ships between self-reported measures of the perceivedcontrol and depression has been obtained8,10 but very burden of illness and the level of depressive symptoms,strict glycaemic control can also contribute to as well as relationships of both of these measures todepression.4 A causal relationship between diabetes objective demographic-, treatment-, and sickness-relatedcontrol and depression is difficult to establish, particularly
factors, in patients with insulin-dependent (Type 1)diabetes mellitus (IDDM). We also set out to determine
*Correspondence to: Bjorn Karlson, Lund University, Department of the contribution of these various factors to depressiveApplied Psychology, Paradisgatan 5, S-223 50 Lund, Sweden. symptoms in the patients studied.Sponsors: Malmohus lans landstings utvecklingsfond
1066 CCC 0742–3071/97/141066–07$17.50 1997 by John Wiley & Sons, Ltd. DIABETIC MEDICINE, 1997; 14: 1066–1072

ORIGINAL ARTICLESmanual,15 one a group of non-diabetic healthy subjectsPatients and Methodsand the other a group of psychiatric outpatients, themean scores for each gender being transformed separatelyPatientsinto T-scores on the basis of the scores of the two
A sample of 200 patients aged 35.3 ± 8.9 years control groups.(mean ± SD) was selected by drawing every secondpatient from a list of patients, sorted by date of birth, Medical Measurescomprising all patients who visited the outpatient diabetesclinic of the Department of Internal Medicine at the The patients’ degree of metabolic control was assessedUniversity Hospital in Lund, Sweden during a 5-month by measuring glycosylated haemoglobin (HbA1c) levelsperiod. Of the 200 questionnaires, 155 (77.5 %) were within 6 weeks before or after they answered theanalysable when returned, 43.6 % of the patients in this questionnaire. The following diabetic complications werefinal group being women (aged 35.1 ± 8.3 years, with a classified on the basis of the patients’ medical records:diabetes onset at the age of 16.5 ± 9.7 years and a retinopathy (background or proliferative), nephropathydiabetes duration of 18.9 ± 9.9 years) and 56.4 % being (incipient nephropathy, i.e. urinary albumin 30–men (aged 35.6 ± 9.3 years, with a diabetes onset at the 300 mg l−1; or clinical, i.e. urinary albumin .300 mg l−1
age of 17.6 ± 10.6 years and a diabetes duration of and/or serum creatinine .116 mmol l−1 for men and17.2 ± 11.3 years). HbA1c measures were available for .100 mmol l−1 for women). Hypertension was defined152 subjects and documentation of late diabetic compli- as a diastolic blood pressure of $90 mmHg beingcations was available from the medical records for 129. obtained and/or a systolic blood pressure $160 mmHgAll the patients were insulin-dependent, 87.6 % showing and/or antihypertensive treatment being prescribed.a diabetes onset prior to age 30 and 12.4 % an onsetbeween the ages of 30 and 41. The insulin dosage was Analytical Techniques44.3 ± 20.1 IU day−1 and injection regimens varied: oneinjection (5.5 %), two injections (28.3 %), three (25.2 %), Glycosylated haemoglobin (HbA1c) levels were analysedfour or more (39.4 %), and insulin pump (CSII: 1.6 %). by fast liquid chromatography (normal value , 5.3 %).The study was approved by the ethics committee of Urinary albumin concentration was measured by tur-Lund University, subjects giving their informed consent bidimetry using an automated analyser (Cobras Mira,to participate. Roche), antibodies (rabbit anti-human albumin), and
a technique described by Dakopatts in Copenhagen;detection limit 5 mg l−1. Serum creatinine concentrationTesting Procedures and Self-reportedwas measured by the kinetic Jaffe technique.Measures
A questionnaire consisting of two parts was mailed to Statisticsthe patients. The time frame for assessment was thepreceding 2 weeks. The first part was the depression Since subjects with different levels of HbA1c may differ
in their perception of and adaptation to their disease,scale from the Symptom Check List SCL-90,14 for whicha standardized sum score (range 0–4) was computed. they were divided in terms of their HbA1c level into
three groups (HbA1c ,6.9 %, 6.9–8.6 %, and .8.6 %,The other part, referred to as the ‘Burden of Illness’ (BI)questionnaire, consisted of seven questions concerning the first and last of these comprising the lowest and
highest quartiles, respectively).three different aspects of BI. Two of these aspects, eachassessed by a separate question, concerned the degree For analysing differences between these groups and
between insulin regimens, the chi-square test for trendto which the subject had been distressed by worriesconcerning late diabetic complications and by perceived was employed for the categorical variables, and the
ANOVA test for trend, using linear contrast, for thedifficulties in maintaining blood glucose control duringthe preceding two weeks. The third aspect was assessed continuous data. An ordinary chi-square test was used
for examining gender differences in the case of categoricalby five questions that comprised a ‘Restrictions’ scale,concerning the extent to which the presence of diabetes variables. Correlations of variables were computed as
Eta coefficients for gender, as Spearman’s correlationswas found to be disturbing by the need to be tied tofixed hours; the need for careful everyday planning; by for ordinal data and dummy variables, and otherwise as
Pearson’s product–moment correlations. In order torestrictions of eating and drinking and on doing thingsthey wanted to do, and by their daily living being reduce the risk for type 1 errors, for the data presented
in Table 1 only group differences with p-values ,0.01restricted by hypoglycaemia or the fear of it. The fiveitems on the scale employed the same type of Likert were considered as significant, and for the data presented
in Table 2 only correlations for which p , 0.001, althoughscale as the SCL-90 and a standardized sum score similarto that for the SCL-90 was computed. p-values ,0.01 are also indicated. A hierarchical multiple
regression analysis was employed for predicting the levelThe level of depression in the group was comparedwith that of two control groups described in the SCL-90 of depression on the basis of certain of the variables. In
1067DEPRESSIVE SYMPTOMS IN DIABETES MELLITUS
1997 by John Wiley & Sons, Ltd. Diabet. Med. 14: 1066–1072 (1997)

ORIGINAL ARTICLESTable 1. Characteristics of the HbA1c subgroups
Total group ,6.9 6.9 – 8.8 .8.8 P-value(n = 155) (n = 38) (n = 75) (n = 39)
M SD M SD M SD M SD
Age (years) 35.3 8.9 34.2 8.6 36.8 9.3 33.8 8.2 0.78Age at diabetes onset (years) 16.9 10.1 17.8 10.2 16.2 10.2 17.7 10.3 0.64Diabetes duration (years) 17.8 10.6 15.2 10.7 19.6 11.0 17.0 9.2 0.50Insulin dosage (IU day−1) 44.6 19.8 38.5 15.3 45.3 14.3 47.6 29.9 0.03HbA1c (%) 7.8 1.4 6.0 0.7 7.7 0.5 9.6 0.7
n % n % n % n %
Gender (men/women) 88/68 56.4/43.6 20/18 52.6/47.4 44/31 58.7/41.3 20/18 56.4/43.6 1.0Number of injections day−1 0.24
1–2 43 34.4 9 29.0 19 30.6 15 46.93 30 24.0 8 25.8 17 27.4 5 15.6.3 or CSII 52 41.6 14 45.2 26 41.9 12 37.5
Retinopathy 0.17no signs 48 38.1 14 45.2 21 34.4 11 34.4background 52 41.3 14 45.2 25 41.0 13 40.6proliferative 26 20.6 3 9.6 15 24.6 8 25.0
Nephropathy 0.45no signs 93 73.2 26 83.9 42 67.7 23 71.9incipient 25 19.7 3 9.7 15 24.2 7 21.9clinical signs 9 7.1 2 6.5 5 8.1 2 6.3
Hypertension 0.003yes 21 16.4 1 3.2 10 15.9 10 31.3no 107 83.6 30 96.8 53 84.1 22 68.8
Antihypertensive treatment 0.02yes 19 14.8 1 3.2 10 15.9 8 25.0no 109 85.2 30 96.8 53 84.1 24 75.0
In the lower part of the table, column percentages are givenp-values refer to comparisons of the subgroups. Continuous data were analysed by a one-way ANOVA test for trend using linear contrast. Forcategorical data the chi-square test for trend was employed.
the correlation and regression analyses, retinopathy and supports the reliability of the scale. Since it could beargued that the Restrictions scale simply measures aspectsnephropathy were recorded into two dichotomized (0, 1)
dummy variables. For the first of these dummy variables, of depression, a factor analysis including the SCL-90items and the seven BI items was conducted, using a1 indicates the lack of retinopathy or of nephropathy,
respectively, in contrast to its presence. For the second varimax rotation. Three factors with Eigenvalues greaterthan 1.0 and explaining 63 % of the total variance weredummy variable, 1 indicates the presence of the most
severe complications (proliferative retinopathy and clini- extracted. The first factor comprised all but one of thedepression items, the second factor comprised the fivecal signs of nephtopathy, respectively), in contrast to
having no complications or less severe ones. The number Restrictions scale items, and the third factor comprisedthe two questions concerning glucose regulation andof insulin doses was dummy coded in a similar way.
For the first dummy variable, 1 indicates having less worries concerning complications, as well as thedepression scale item of ‘crying easily’ (the Eigenvaluesthan three injections per day. For the other dummy
variable, 1 indicates either having more than three of the three factors were 9.5, 2.0, and 1.0, respectively).The factor solution thus supports the cohesiveness andinjections per day or receiving CSII treatment. The
reliability of the Restrictions scale was computed as face validity of the Restrictions scale and its measuringsomething different from depressive symptoms. The thirdCronbach’s alpha, based on internal consistency. When
used to test another group of Type 1 diabetic patients factor included the two BI questions associated with themedical outcome of the disease and one of the depression(n = 82), the Restrictions scale had been found to
have satisfactory reliability (Cronbach’s alpha = 0.86, items, its thus not appearing to primarily indicatedepression. The two BI questions belonging to the thirdunpublished data), as was the case in this study as well
(Cronbach’s alpha = 0.85). The demonstration of such factor were treated as individual variables in order totake account of the uniqueness of their respectivehigh and quite similar alpha coefficients in two separate
samples of insulin-dependent diabetic patients further contents. Calculations were carried out using SPSSfor Windows.
1068 B. KARLSON, C.-D. AGARDH
Diabet. Med. 14: 1066–1072 (1997) 1997 by John Wiley & Sons, Ltd.

ORIGINAL ARTICLESTable 2. Correlations between self-reported and objective data
Depressive Restrictions r Complication Glycaemicsymptoms r worries regulation
problems r
Demographic dataGender −0.24a −0.12 −0.18 −0.23a
Age 0.07 0.10 0.04 0.00Diabetes duration 0.00 −0.11 0.00 −0.07Age at onset 0.14 0.18 0.06 0.11
Medical statusHbA1c 0.15 0.14 0.20a 0.40c
Retinopathyno signs −0.10 0.04 −0.19 −0.09proliferative −0.03 −0.12 0.06 0.03
Nephropathyno signs −0.04 0.03 0.00 0.04clinical signs −0.07 −0.18 −0.12 −0.02
Hypertension −0.03 0.01 0.23a 0.09Antihypertensive treatment −0.02 −0.06 0.20 0.06
Insulin regimenInsulin dosage (IU day−1) 0.13 0.04 0.08 0.10Number of injections day−1
,3 0.10 0.08 0.19 0.03.3 or CSII −0.07 −0.17 −0.14 −0.04
Depressive symptoms 0.56b 0.52b 0.56b
Significance testing of Eta coefficient for gender, of Spearman rank correlations for independent variables ofordinal data level and of Pearson’s product–moment correlation for interval data variables, are two-tailed.Male = 1; female = 0. a = p , 0.01, b = p , 0.0001.
Results
Group Characteristics
The HbA1c level was 7.8 % ± 1.4 (mean ± SD) for theentire group, no significant differences being found eitherbetween the insulin regimens or for gender. Backgroundretinopathy was present in 41.7 %, proliferative retino-pathy in 20.5 %, incipient nephropathy in 19.5 %,and clinical nephropathy in 7.0 % of the patients.Hypertension was present in 17.3 % of the patients, mostof whom (91 %) were on antihypertensive treatment. Nodifferences in the occurrence of any of the complicationswere found between genders or between the insulin regi-mens.
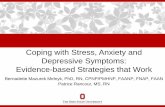
The mean scores on the depression scale were1.1. ± 0.9 for the women and 0.7 ± 0.7 for the men. The
Figure 1. Burden of Illness and depressive symptoms in theT-score for the entire group was 63 on the basis of theHbA1c subgroupsscores for the non-diabetic healthy control group and
42 on the basis of those for the psychiatric outpatientthe total group and the HbA1c levels for the subgroups
group. The mean scores for each of the three HbA1c are shown in Table 1.subgroups on the depression scale and the Burden ofIllness scales are shown in Figure 1. The groups differed Correlations Between Psychologicalin worries about complications (p = 0.02) and perceived Variables and Demographic and Medicalglycaemic regulation problems (p , 0.0001). For the Variableslatter, pairwise comparisons showed the low and inter-mediate HbA1c level subgroups to differ from the high Correlations between all the independent variables and
the three BI subscales (restrictions, complication worries,subgroup. Demographic and medical characteristics of
1069DEPRESSIVE SYMPTOMS IN DIABETES MELLITUS
1997 by John Wiley & Sons, Ltd. Diabet. Med. 14: 1066–1072 (1997)

ORIGINAL ARTICLESand glycaemic regulation problems) as well as depressive shown to contribute significantly in each block were
included, again entered hierarchically in blocks. Assymptom scores are shown in Table 2.Depressive symptom scores were found to be signifi- shown in Table 3, the initial contribution of female
gender disappeared when the interaction variables werecantly correlated with all three BI subscales (p , 0.001)and showed a weak positive correlation with female entered. Interactions which contributed to the degree of
depression were found between good metabolic controlgender (p , 0.01) whereas no correlation was foundwith HbA1c, age, age at onset, diabetes duration or the and ‘complication worries’ (p , 0.0001), between inter-
mediate metabolic control and ‘perceived restrictions’occurrence of any particular type of diabetic compli-cations. (p = 0.001), and between poor metabolic control and
‘perceived glycaemic regulation problems’ (p , 0.002).The three BI subscales correlated positively with eachother (p , 0.0001). The degree of restrictions reported Altogether, 44.0 % of the variance in depression could
be explained. Thus, the BI variables differed in the levelswas not correlated with any of the other variables, andworries about complication showed only weak positive of glycaemic regulation at which they contributed most
to the variance in depression.correlations with HbA1c level and with hypertension(p , 0.01 for both). Perceived problems of glycaemicregulation, however, were positively correlated with DiscussionHbA1c level (r = 0.40, p , 0.0001). Thus, there werealmost no zero-order correlations between the objective The relative contributions of demographic-, treatment-
and sickness-related variables and Burden of Illness todata and the self-reported measures, although the latterwere correlated with each other. level of depression in insulin-dependent diabetic patients
was examined by use of multivariate analysis afterThe report of perceiving oneself to have problems inglycaemic regulation was thus related both to depression certain relationships between the variables assessed had
been explored.(Table 1) and to HbA1c, although depression and HbA1c
were not significantly correlated with each other (r = 0.15, Although the term depression is sometimes used inthis study, this does not refer to clinically diagnosedp = 0.06). When ‘perceived glycaemic regulation prob-
lems’ was controlled for, the correlation between HbA1c depression, but rather to a broad range of depressivesymptoms, measured dimensionally by use of the SCL-and depression was reduced (r = −0.10, p = 0.23), indicat-
ing most of the overlap between HbA1c and depression 90. In our study women displayed higher depressionscores than men, in accordance with previous epidemiol-to be accounted for by these self-reported problems
in regulation. ogical studies in the general population.5 The differencewas of the same magnitude as that obtained in the controlgroups included in the SCL-90 manual.15 Reference toInteractionsthe control groups indicated the depression level in thepresent group to be above the mean for a group of non-To analyse whether relations between the three aspects
of perceived burden of illness and depression differed diabetic healthy subjects and below that for a psychiatricoutpatient group, for both the men and the women.with respect to level of metabolic control, interaction
effects between the BI variables and HbA1c subgroups Thus, the elevation in the level of depressive symptomswas about the same for both genders.in accounting for the degree of depression were tested
by analysis of variance. Interaction effects were found Each of the three separate aspects of BI was shown tobe a dimension which differed from depression but wasbetween HbA1c subgroup membership and the ‘compli-
cation worries’ (p , 0.0001) and ‘restrictions’ (p = 0.005) related to the level of depressive symptoms. This is inline with other findings, showing a strong relationshipvariables, but not ‘perceived glycaemic regulation prob-
lems’ (p = 0.07). This indicates the level of depression between threat of illness and depression.12
‘Perceived glycaemic regulation problems’ was alsoassociated with different worries or concerns to differbetween various levels of glycaemic regulation. found to be related to HbA1c and accounted for the
overlap between HbA1c and depression. It can beconceived as a link between the latter two variables,Regression Analysisalthough the mechanisms of such an indirect relationshipmay be of various kinds. Patients with poor metabolicA multiple regression analysis was conducted to deter-
mine the relative contribution to the depressive symptom control may worry about not being able to regulate theirglycaemia, worries which may result in depression.scores of variables being entered hierarchically in blocks,
first the demographic variables (gender, age, age at Conversely, patients who for any reason are depressed,and perceive themselves as having problems in regulatingdiabetes onset, and diabetes duration), then those of
treatment regimen (insulin dosage and number of injec- their glucose levels, may be more likely to have poormetabolic control, due either to ineffectiveness in copingtions or CSII), then the objective disease-related measures
(the complications), and finally the variables of interaction emotionally with stress16 or to difficulties in adherenceto a regimen. However, the weak correlation betweenbetween the HbA1c subgroups and the three BI aspects.
In a second regression analysis, only those variables HbA1c and depression, and the complex causal relation-
1070 B. KARLSON, C.-D. AGARDH
Diabet. Med. 14: 1066–1072 (1997) 1997 by John Wiley & Sons, Ltd.

ORIGINAL ARTICLESTable 3. Relations of depressive symptom scores in the patients as a whole to demographic, medical, and attitude variables.Regression analysis was performed hierarchically in blocks
Variables Values at the end of each block
Slope SE of slope Stand. regr. 95 % CI p-value Overall R2
coeff. (%)
Block 1Gender −0.39 0.13 −0.24 −0.64–−0.14 0.003 5.8
Block 2Gender −0.10 0.11 −0.06 −0.31–0.11 0.36HbA1c low group × complication worry 0.45 0.10 0.53 0.26–0.64 ,0.0001HbA1c mid group × restrictions 0.37 0.11 0.40 0.15–0.58 0.001HbA1c high group × glycaemia 0.40 0.13 0.55 0.15–0.65 0.002 44.0regulation problem
Male = 1; female = 0. The last three variables of block 2 are interaction terms between the BI variables and the low, mid and high subgroupsof HbA1c, defined as HbA1c ,6.9, 6.9–8.8, and .8.8 %, respectively.
ship between the two,8 call for caution in interpreting such somatic changes, this being part of a transient crisisreaction. It should be noted, however, that data werethe results.
Complication worries and perceived glycaemic regu- not available regarding all the complications, for examplemacrovascular disease and neuropathy, both of whichlation problems, but not perceived lifestyle restrictions
and depression, increased from the lowest to the highest have been reported to be associated with a decreasedquality of life.18HbA1c level subgroup. People in different levels of
metabolic control differed in the major worries and Depression was found to be related more to dailyconcerns or worries regarding glycaemic regulation,concerns connected with their depression. Although
those with good metabolic control were characterized restrictions in activities, and anticipated complications,the impact of these different worries on mood varyingby the lowest degree of worry of the three groups
regarding complications, a high degree of depression with glycaemic control level. The relations found betweendepression and burden of illness are open to variouswas found to be associated with that worry rather than
with the other aspects of burden of illness. One can interpretations. The increase in the prevalence ofdepression that has been reported in diabetes2 may resultspeculate that their good metabolic control may have
been the result of their aims of preventing complications, from perceived burden of illness, in line with previousfindings showing threat of illness to be strongly relatedworry about this making them feel depressed, whereas
perceived restrictions did not have this effect, these to depression.12 Another interpretation is that depressionin diabetic patients, whatever its basis may be, negativelypatients possibly finding them to be worthwhile. Low
emotional well-being in metabolically well-regulated affects the experiencing of the disease. Such reportedperceptions and depressive symptoms may be a function,patients has been suggested previously to be due to
over-ambitious aims and to feelings of failure.17 In in turn, of dimensions not measured in the present study,such as personality traits, adaptive strategies, or the statecontrast, for those with an intermediate level of metabolic
control a depressed mood was mainly associated with or trait of negative affectivity that has been describedas a general tendency toward distress and negativeperceived restrictions. Such patients may be thought to
have adopted a less tight metabolic control in order to reporting.19–20 Clinically, one should be sensitive to thefact that diabetic patients’ depressive feelings may becope with their major concerns. The depressed mood in
the most poorly regulated patients was associated, in largely unrelated to the severity of the disease per se,being related instead to their perceptions of the dailyparticular, with their experiencing problems of glycaemic
regulation, which may indicate feelings of failure to cope burdens of living with their condition. The specificworries and concerns of patients with depressed moodwere dominating.
Degree of depression was not found to be related to varies with degree of metabolic control.any of the chronic complications. This failed to lendsupport to the assumption that depression is directly Acknowledgementsrelated to the severity of the disease. The Burden ofIllness variables were likewise not related to the presence We thank A. Sternerup-Hansson, Lund University Com-
puting Centre, and M. Hagnell and P.-E. Isberg, Depart-of these chronic complications. The absence of suchdirect relationships may be due to most patients adapting ment of Statistics, Lund University, for statistical advice.
The study was supported by grants from Malmohus lansto the development or worsening of late diabeticcomplications, and to the depressed mood elicited by lanstings utvecklingsfond.
1071DEPRESSIVE SYMPTOMS IN DIABETES MELLITUS
1997 by John Wiley & Sons, Ltd. Diabet. Med. 14: 1066–1072 (1997)

ORIGINAL ARTICLES11. Sanders K, Mills J, Martin FIR, Horne DJDeL. EmotionalReferences
attitudes in adult insulin-dependent diabetics. J PsychosomRes 1975; 19: 241–246.1. Klerman GL. Depression in the medically ill. Psychiatr
12. Connell CM, Wayne KD, Gallant MP, Sharpe PA. ImpactClin North Amer 1981; 4: 301–317.of social support, social cognitive variables, and perceived2. Gavard JA, Lustman PJ, Clouse RE. Prevalence ofthreat on depression among adults with Diabetes. Healthdepression in adults with diabetes. An epidemiologicalPsychol 1994; 13: 263–273.evaluation. Diabetes Care 1993; 16: 1167–1178.
13. Hagnell O, Essen-Moller E, Lanke J, Ojesjo L, Rorsman3. Surridge DHC, Williams Erdahl DL, Lawson JS, DonaldB. The Incidence of Metal Illness over a Quarter of aMW, Monga TN, Bird CE, Letemendia FJJ. PsychiatricCentury. Stockholm: Almqvist & Wiksell International,aspects of diabetes mellitus. Br J Psychiatry 1984; 145:1990.269–276.
14. Derogatis LR, Lipman RS, Covi L. SCL-90: An outpatient4. Lustman PJ, Griffith LS, Gavard JA, Clouse RE. Depressionpsychiatric rating scale-preliminary report. Psychopharma-in adults with diabetes. Diabetes Care 1992; 15: 1631–col Bull 1973; 9: 13–28.1639.
15. Derogatis LR. SCL-90-R. Administration, Scoring and5. Haire-Joshu D, Heady S, Thomas L, Schechtman K, FisherProcedures. Manual II. Towson: Clinical PsychometricEB Jr. Depressive symptomatology and smoking amongResearch Inc., 1992.persons with diabetes. Res Nurs Health 1994; 17: 273–282.
16. Peyrot MF, McMurray JF Jr. Stress buffering and glycaemic6. Robinson N, Fuller JH, Elmeades SP. Depression andcontrol. The role of coping styles. Diabetes Care 1992;diabetes. Diabetic Med 1988; 5: 268–274.15: 842–846.7. Leedom L, Meehan WP, Procci W, Zeidler A. Symptoms
17. Lundman B, Asplund K, Norberg A. Tedium amongof depression in patients with type II diabetes mellitus.patients with insulin-dependent diabetes mellitus. J AdvPsychosomatics 1991; 32: 280–286.Nurs 1988; 13: 23–31.8. Lustman PJ, Griffith LS, Clouse RE, Cryer PE. Psychiatric
18. Lloyd CE, Matthews KA, Wing RR, Orchard TJ. Psychoso-illness in diabetes mellitus. J Nerv Ment Dis 1986; 174:cial factors and complications of IDDM. The Pittsburgh736–742.Epidemiology of Diabetes Complications Study. VIII.9. Popkin MK, Callies AL, Lentz RD, Colon EA, SutherlandDiabetes Care 1992; 15: 166–172.DE. Prevalence of major depression, simple phobia and
19. Costa PT, McCrae RM. Neuroticism, somatic complaints,other psychiatric disorders in patients with long-standingand disease: Is the bark worse than the bite? J Pers 1987;type I diabetes mellitus. Arch Gen Psychiatry 1988; 45:55: 299–316.64–68.
20. Watson D, Pennebaker JW. Health complaints, stress,10. Mazze RS, Lucido D, Shamoon H. Psychological andand distress: exploring the central role of negativesocial correlates of glycemic control. Diabetes Care 1984;
7: 360–366. affectivity. Psychol Rev 1989; 96: 234–254.
1072 B. KARLSON, C.-D. AGARDH
Diabet. Med. 14: 1066–1072 (1997) 1997 by John Wiley & Sons, Ltd.