Building Stronger Communities for Better Health - JCPES PL USA - 2004

of 18
-
Upload
publichealthbydesign -
Category
Documents
-
view
217 -
download
0
Transcript of Building Stronger Communities for Better Health - JCPES PL USA - 2004
-
8/14/2019 Building Stronger Communities for Better Health - JCPES PL USA - 2004
1/18
-
8/14/2019 Building Stronger Communities for Better Health - JCPES PL USA - 2004
2/18
Building Stronger Communities for Better Health
-
8/14/2019 Building Stronger Communities for Better Health - JCPES PL USA - 2004
3/18
Founded in 1970, the Joint Center for Political and Economic Studies informs and illuminates the nations major publicpolicy debates through research, analysis, and information dissemination in order to: improve the socioeconomic statusof black Americans, expand their effective participation in the political and public policy arenas, and promote communi-cations and relationships across racial and ethnic lines to strengthen the nations pluralistic society.The Joint Centers new Health Policy Institute works to improve the health status of black Americans and other ethni-cally diverse groups by expanding their participation in relevant political, economic, and health policy arenas. It providesa national platform for minority health issues and gives voice to groups that would otherwise be excluded from theseimportant debates through its ongoing analysis of health and related policy issues and through timely distribution of vital
information.PolicyLink is a national nonprofit research, communications, capacity building, and advocacy organization based inOakland, California. Since 1999 PolicyLink has worked to advance a new generation of policies to achieve economicand social equity from the wisdom, voice, and experience of local constituencies. Its research and analysis in the field ofhealth explores how the social, economic, and physical environments of local communities affect health and contributeto health disparities.Opinions expressed in this publication are those of the author(s) and do not necessarily reflect the views of the staff orgoverning board of the Joint Center or PolicyLink.This is a project of the Joint Centers Health Policy Institute, which is supported by a grant from the W.K. Kellogg Foun-dation.
Copyright 2004 by theJoint Center for Political and Economic StudiesandPolicyLinkPrinted in the United States.All rights reserved.
-
8/14/2019 Building Stronger Communities for Better Health - JCPES PL USA - 2004
4/18
FOREWORD
Over the past five years, racial and ethnic disparities in health care and health status have been highlighted in a series ofgovernmental and non-governmental reports. The nature and extent of the problem should be obvious to all who arepaying attention. However, less is known or shared about solutions that can be adopted in local communities, especiallywhere the problems are most severe.
The importance of community cannot be overstated. It is the community environment that determines the toxins peopleare exposed to, their opportunities for exercise, healthy eating and living, and the health care services they can access.Moreover, people of color are exposed to an additional stress in the form of racism, which can have a harmful long-termimpact on their health. In short, the overall vitality of a community the economic opportunities available, the socialsupport networks, and the public infrastructure plays a major role in families ability to improve their health and well-being. This brief offers a framework for strengthening communities to improve the health and well-being of residents. Itnotes that communities can have positive or negative effects on health. Our policy goal should be to increase the positivesand reduce the negatives.
A collaboration between the Joint Center for Political and Economic Studies and PolicyLink, this brief is one of fourthat outline strategies for achieving better health through community-focused solutions. The other three focus on dietand fitness; asthma; and special issues for Latino immigrants. The briefs, written by PolicyLink staff and consultants, arebased on a review of the literature as well as on interviews with African American and Latino community health leaders(or those serving African American and Latino populations) and elected officials from across the country.
The Joint Center and PolicyLink are grateful to the W. K. Kellogg Foundation for their support of the Joint CentersHealth Policy Institute, which made these publications possible. This document could not have been accomplishedwithout the hard work and dedication of our staff and consultants, who are listed on the acknowledgements page. Wealso appreciate the participation by elected officials, community leaders, and health practitioners in interviews and aforum where they shared with us their experiences and strategic thinking and provided helpful feedback on proposedsolutions. We hope this document will be useful in your work to ensure that everyone can live in a healthy community.
Eddie N. Williams Angela Glover BlackwellPresident President Joint Center for PolicyLinkPolitical and Economic Studies
-
8/14/2019 Building Stronger Communities for Better Health - JCPES PL USA - 2004
5/18
AcknowledgementsThe Joint Center and PolicyLink would like to express sincere gratitude to the staff and consultants who assisted in thecompletion of our joint project, including the final publication of these four issue briefs. Their valuable input and hardwork contributed greatly to the quality of the final products.Special thanks go to Regina Aragon, who was a part of the PolicyLink health team from start to finish and was particu-larly involved in the briefs on broad community factors and on Latino health. She added important insights, excellentwriting skills, and a deep level of research. Samuels and Associates assisted in the research, drafting, and editing of thebrief on physical activity and healthy eating, adding their extensive knowledge and experience from the field.
Joint Center Team
Program StaffDr. Margaret C. Simms, Senior Vice President for ProgramsDr. Gail Christopher, Director of the Health Policy InstituteEdit and Design StaffDenise L. Dugas, Vice President for Communications and MarketingMarc DeFrancis, Senior EditorDavid Farquharson, Creative Director
PolicyLink Team
Angela Glover Blackwell, PresidentMildred ThompsonJudith BellRebecca FlournoyVictor RubinRay ColmenarRosia Blackwell-Lawrence
-
8/14/2019 Building Stronger Communities for Better Health - JCPES PL USA - 2004
6/18
Building Stronger Communities for Better Health
1Joint Center for Political and Economic Studies / PolicyLink
RECENT POLICY ATTENTION TORACIAL AND ETHNIC HEALTH
DISPARITIESThe 1998 launch of the Department of Health and Hu-man Services (DHHS) Initiative to Eliminate Racial andEthnic Disparities in Health put the issue on the nationalpolicy agenda. Healthy People 2010a DHHS-led effortto establish a set of key health indicators for the nationand measure health improvement over timesubsequent-ly emphasized the importance of measuring differences inhealth outcomes by race and ethnicity as a first step towardeliminating disparities.1
In a 2003 report, Unequal Treatment: Confronting Racial
and Ethnic Disparities in Health Care,2 the Institute ofMedicine documented major differences in the way peopleof color and whites are treated within the health care sys-tem. In February 2004, the DHHS Agency for HealthcareResearch and Quality issued the National Health CareDisparities Report, the first federal effort to measure differ-ences among various populations in their access to and useof health care services.3 Together with the ongoing workof state and national governmental and private organiza-tions and the work of advocates and community leadersacross the country, these efforts have heightened awarenessof health disparities and helped to mobilize practitioners,policymakers, and public health officials at the local, state,
and national levels.
In most cases, policy efforts to reduce disparities haveattempted to expand access to health care and improveindividuals experiences within the health care system.However, as important as access is, researchers at theCenters for Disease Control and Prevention (CDC) haveestimated that lack of access to care accounts for only afraction of total mortality (death) in the United States.Most mortality is instead the result of environmental con-ditions, social and economic factors, behavior, and geneticpredisposition.4 As the following summary indicates, there
INTRODUCTION
The problem of health disparitiesspecifically, the higher
incidence of certain diseases and health conditions amongcommunities of colorfirst emerged on the nationalpolicy agenda in 1998. Community leaders, public healthofficials, and an array of state and national organizationsseized on the issue, seeking to educate policymakers andthe public and advocating for an expansion of policy ini-tiatives across the country. Such efforts have focused mostoften on expanding access to health care and improvingindividuals experiences within the health care system.
Improving access to health care and the quality of that careremain critically important and challenging goals. But re-search on the causes of illness and mortality in the United
States suggests that improving health care and health out-comes in communities of color would be most successfulwith a simultaneous focus on those communities social,economic, and physical environments. Far from being amere backdrop for interventions designed to change in-dividual health and health behavior, community environ-ments must be understood to have equal importance.
This issue brief presents a framework for understandinghow community conditions affect individuals health bothdirectly and indirectly. It discusses how attention to thesedeterminants of health requires a shift from a narrow focuson treatment to a broader approach that includes preven-tion and health promotion. The overarching roles thatrace, ethnicity, and socioeconomic status play in healthstatus are explored within this context, and the case ismade that the legacy of racism must be addressed if thecontinuing health disparities between white Americansand Latino and African Americans are to be eliminated.
Included are key findings from our interviews with AfricanAmerican and Latino elected officials and communityhealth leaders. Their discussions also suggest that resolvinghealth disparities will require making changes in commu-nity environments. The final sections of this brief discuss
the implications of this community-effects concept fordesigning new policy and program strategies. Accordingto the interviews, such changes will require approachesranging from local neighborhood action to securing publicfunding and effecting policy changesthat will not beeasy given current fiscal and political constraints. None-theless, the interviews, current research, and the experi-ences of African Americans and Latinos all underscore theneed for continued leadership and action in the effort toimprove the health status of these populations.
Community organizing iskey; when you empowerpeople in one area, it hasresidual effects.Councilman Tom Perez, Montgomery County,Maryland
-
8/14/2019 Building Stronger Communities for Better Health - JCPES PL USA - 2004
7/18
2 Joint Center for Political and Economic Studies / PolicyLink
is a growing body of research identifying how communityconditions of all kinds affect a host of chronic diseasesand other health conditions. Thus, the social, economic,
and physical environments of communities, including theeffects these environments have on individual behavior,are an important focus for new policy approaches aimed atimproving health among black and Latino populations.
A CONCEPTUAL FRAMEWORK OFCOMMUNITY EFFECTS ON HEALTH
In its 2002 report Reducing Health Disparities Througha Focus on Communities, PolicyLink proposed a frame-work, based on emerging research, to describe how social,economic, and physical environments in neighborhoodsaffect health.5 This framework, updated for this publica-tion, is based on various conceptual models found in thepublic health literature and on the theory and practice ofcommunity building (that is, community driven effortsto improve neighborhood and family conditions).6 It alsoreflects many public health practitioners increasing focuson neighborhoods, as well as a parallel increase in concernabout health among urban planners, community leaders,and municipal administrators.
Neighborhood factors influence health at least four ways:(1) direct effects on both physical and mental health,
(2) indirect influences on behaviors that have health conse-quences, (3) health impacts resulting from the quality andavailability of health care, and (4) health impacts associ-ated with the availability of opportunity structures.7,8Opportunity structures include such things as access tohealthy and affordable food, safe and enjoyable spaces forexercise and recreation, capital for business or home-basedassets, and transportation resources that facilitate employ-ment and education.
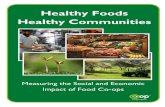
Depending on circumstances in a given community orneighborhood, the factors listed in the accompanyingtable Conceptual Framework of Community Effects
on Health can have protective or negative effects onhealth. For example, the amount of social capital,9 or closeconnections to others Conceptual Framework of Commu-nity Effects on Health within and beyond the community,has been shown to correlate with better mentaland insome cases physicalhealth, as community residents sharea sense of collective resiliency and are supportive of oneanother. Conversely, the lack of social capital has beenshown to contribute to poorer health status. For example,
a lack of trust or connection to neighbors could lead to areluctance or inability to help one another in the event ofa health or economic crisis.
A given community factor also may have multiple effects.For example, the prevalence of crime in a neighborhoodcan have a direct health effect by increasing injuries due toviolence, and can also discourage commercial developmentin an area and restrict residents willingness and ability toexercise outdoors. While these interactions can make itdifficult to isolate and measure the impact of any singlefactor, they also suggest that multi-pronged strategies forimproving neighborhoods can positively improve healthoutcomes and reduce health disparities.
Exploring how community factors can affect health also
requires applying a life course approach, which recogniz-es that a given factor will have different effects on commu-nity residents as they age. A lack of public transportation,for example, is likely to affect youths more than adult resi-dents, who are more likely to have access to cars. Likewise,the quality and availability of preschools will affect youngchildren and their parents. The elderly, on the other hand,who are more susceptible to social isolation, may find itdifficult to drive, thus have more need for public transit orother transportation means to get to friends, family, andneighborhood centers. In addition to taking into accountresidents age and the duration of their exposure to a par-ticular community environmental factor (which may vary
depending on residential mobility), in the application ofthis framework one must also consider that the effects willvary according to a communitys economic, political, andsocial characteristics at a given time.
THE OVERARCHING EFFECTS OF RACE,ETHNICITY, AND SOCIOECONOMICSTATUS
The effects of community environment on health statusapply to all population groups and regions of the coun-try. However, because a community is shaped by therace, ethnicity, and socioeconomic status of its residents,these effects become public policy issues when racial andeconomic disparities result in health disparities among dif-ferent communities. In short, racial and economic dispari-ties between neighborhoods help to create and maintainhealth disparities, and must therefore be the focal point forunderstanding and addressing health status.
-
8/14/2019 Building Stronger Communities for Better Health - JCPES PL USA - 2004
8/18
Building Stronger Communities for Better Health
3Joint Center for Political and Economic Studies / PolicyLink
Many researchers have documented the relationshipbetween socioeconomic status, or social class, and health,10with findings that education and income levels are among
the strongest predictors of health status.11
Likewise, thereis evidence that the widening gap between the rich and thepoor is contributing to health disparities.12
Income, education, and type of employment influencean individuals exposure to a wide range of risk factorssuch that rates of mortality and morbidity (poor health)increase as socioeconomic status decreases. This gradienteffect wherein each socioeconomic group has betterhealth than the group just below it is especially signifi-cant at the lower range of the socioeconomic ladder.13
In a long-term study (known as the Alameda Study) of
the predominantly African American residents in WestOakland, California, a federally defined poverty area,researchers found that living in a poor neighborhood isitself a health risk. The additional risk to health associatedwith living in the neighborhood could not be explainedby individual residents ages, incomes, gender, or educa-tion, nor by race or baseline health status, all of which theresearchers adjusted the data to control for.14
The interplay between social class and race or ethnicityis important. Research has shown that race and ethnicityoften determine a persons socioeconomic status to a majordegree.15 Further, research has shown that both race and
ethnicity have effects on health independent of socioeco-nomic status. Even after the data are adjusted to removethe effects of socioeconomic status, racial differences per-sist in the quality of education, the family wealth associ-ated with a given level of income, the purchasing power ofincome, the stability of employment, and the health risksassociated with occupational status.16
The Role of Residential Segregation
Class, race, and ethnicity also influence where individuals
live, primarily through patterns of residential segregation.Racism is also a factor even though the degree of segrega-tion between black and white appears to have decreasedin recent yearsas measured by the dissimilarity index,which identifies the extent to which neighborhood resi-dents would need to move to be evenly distributed by raceor ethnicity.17 However, low-income African Americansare still far more likely than people of other races to live inhigh-poverty, racially segregated neighborhoods18 and areless likely than Latinos, for example, to enter less segre-gated neighborhoods as their income rises.19
As whites and higher income people of color leave inner
cities for the suburbs, they are increasingly likely to leavebehind economically depressed communities with limitedjob opportunities, poorly performing public schools,and old, substandard housing stock. At the same time,in many metropolitan areas, first-ring suburbs, home tonewly arrived African American and Latino families, areexperiencing new concentrations of poverty and seriouschallenges of disinvestment.20 The proportion of the poorwho live in neighborhoods of highly concentrated povertydeclined from 1990 to 2000, particularly in the East andMidwest. Nevertheless, the overall poverty rate for the na-tion remained nearly constant through the decade, and thepoor population was predominantly comprised of African
Americans and Latinos.21
Racial segregation has ramifications in the economic,physical, and political environments. Low-income com-munities of color routinely receive fewer tax dollars forvital infrastructure services, from education to sanitation,yet have larger numbers of polluting industries in their
Everyone is focused on health behaviors these days, but theenvironment people are constrained within far exceeds the
effect of any individual change. Our program can link kids toasthma specialists and ensure they have the right medicines andresources like bed covers, but at the end of the day, if they gohome to neglected buildings that are roach infested, and moldyhousing, we will not be able to stabilize their asthma. Jacqueline Martinez, Northern Manhattan Community Voices
-
8/14/2019 Building Stronger Communities for Better Health - JCPES PL USA - 2004
9/18
4 Joint Center for Political and Economic Studies / PolicyLink
midst.22 These conditions make it even more challengingto build the necessary additional protective responses.
STRATEGIES FOR REDUCING HEALTHDISPARITIES: IMPLICATIONS OFTHE FRAMEWORK AND INTERVIEWFINDINGS
Acknowledgment of Political Obstacles
The need for new and expanded strategies to eliminatehealth disparities in the United States is clear, althoughgiven the current economic environment of growing state
and federal budget deficits, pursuing such a policy agendawill not be easy. In interviews conducted for this study,African American and Latino elected officials said theyfind it difficult to promote expanded investment in minor-ity communities in the midst of what several described asan ideological battle over the appropriate role of govern-ment. As one state official said quite succinctly, We arecurrently fighting just to hold on to what we have!
In light of this political environment, a number of electedofficials and community health leaders emphasized theimportance of local leadership in furthering a communitydriven approach to racial and ethnic health disparities.
Rather than waiting for federal or state officials to adoptpolicies toward this end, interviewees stressed the need forlocal initiative and action.
Refocusing on Prevention
Fundamentally, addressing the community determinantsof health requires a shift from efforts focused on treat-ment to those focused on prevention or health promotion.This shift need not result in a deemphasis of advocacy toimprove access and quality within the health care system.
Such work will remain important to the overall goal ofeliminating health disparities. But a simultaneous focus onprevention is needed.
The Need for Multiple Strategies AcrossSectors
The community-effects framework and our interviewfindings suggest the need for strategies and policies to be
multi-pronged and function across sectors. Thus, preven-tion strategies in the health field need to be connectedwith strategies in sectors such as education, housing, pub-
lic safety, economic development, and community plan-ning. Some health care organizations have succeeded instretching the traditional boundaries of health care by co-locating, within one institution, the activities of schools,programs to promote home ownership, intergenerationalsocial services, business development opportunities, andrecreational services. However, as several intervieweesnoted, building alliances across sectors is a major challengebecause local service providers and leaders are often morefocused on their own issues or programs. One intervieweenoted that overcoming the perceived competition forfundinga dynamic sometimes exacerbated by fundersthemselvesis an important first step to creating effective
coalitions with shared community goals.
Efforts to improve the health of Latino immigrantsprovide another example of how strategies to reducedisparities must consider community factors beyondpublic healths traditional scope. Latinos access to andwillingness to use medical services can be influenced byimmigration laws and program eligibility rules that havefar-reaching impacts on their lives. Their access to care isalso constrained by substandard and overcrowded housing,marginal employment, limited public transportation, andlanguage barriers.
Notwithstanding these risk factors, what is referred to asthe Hispanic health paradox has been well documented:
When it comes to diet andnutrition, it isnt any singleinfluence. The absence of safeand affordable exercise venuesin inner-city neighborhoodsand the lack of promotion of
exercise in schools, togetherwith targeted advertising forunhealthy foods, affect youngpeoples ability to choosehealthier lifestyles. Ohio State Representative Tyron Yates
-
8/14/2019 Building Stronger Communities for Better Health - JCPES PL USA - 2004
10/18
Building Stronger Communities for Better Health
5Joint Center for Political and Economic Studies / PolicyLink
Latino immigrant health status actuallydeclinesas thelength of residency in the United State increases.23 Someresearchers have linked this trend to the economic and so-
cial stress of living as an immigrant, including a weakeningof community and social networks for second- and third-generation Latinos as they become more acculturated.Changing diet and exercise patterns may also be factors,as immigrants over time adopt less healthy American dietsand more sedentary lifestyles.24
The Need for a Sustained Investment and aLong-Term Policy Agenda
A focus on community factors will require a long-terminvestment of both public- and private-sector resources
as well as a long-term commitment to policy change andadvocacy. Expanding employment opportunities andimproving the quality of public schools can take years toaccomplish. However, as a number of community healthleaders and elected officials noted, organizing communityresidents to identify and respond to local problems bringsbenefits to the communityin particular a feeling of self-determination and collective efficacythat extend beyondthe specific goal into other areas of residents lives.
PROMISING POLICY APPROACHES TOREDUCING HEALTH DISPARITIES
Beyond the continued importance of the issues of access,affordability, and quality of health care services,25 the com-munity-effects framework proposed in this brief suggeststhat local, state, and federal policymakers already haveavailable a number of policy options for reducing healthdisparities by improving the social, economic, and physical
environments of local communities. This brief illustratesthe critical intersection between health and the communi-ty environment, including the presence of environmental
toxins, housing conditions, access to jobs and transporta-tion, the quality of education, and health promotingactivities. African Americans and Latinos are especiallyaffected by disparities in these life-quality factors, so sig-nificant health improvements can occur only when thesefactors receive serious attention and show improvement aswell.
Long- and short-term policy approaches with the goal ofreducing the social, economic, and physical isolation ofpoor communities through revitalization efforts and op-portunities for wider resident participation are outlinedbelow.
Expand Economic Opportunities
Promote job training and economic develop-ment. Programs that reach a diverse range of clientswith both job-specific and academic training arenecessary. The models exist but the resources forputting the programs into effect widely have notbeen secured. New innovations with communitybenefit agreements suggest how economic develop-ment can ensure benefits to long-time low-incomeresidents.26 For example, some communities weresuccessful in obtaining living wage requirementsfor residents employed in development projects.
Facilitate access from isolated neighborhoods tonew job centers. As suburban areas continue to grow,inner-city residents are increasingly isolated fromjobs and other economic opportunities. Suburbanlow-income residents similarly find themselves
Can Schools Help Bridge Divergent Community-Driven Efforts?
As community-based institutions, schools may be in a position to help bridge divides that interfere with coalitionbuilding across sectors. The quality of schools themselves, particularly public, inner-city schools, establishes a trajec-tory for socioeconomic status, which in turn affects health. In addition, with many schools already serving a conven-ing role for children, the expanded after-hour use of school buildings for other community meetings and events is alogical next step. And, as one interviewee asked, with 25 percent of the kids in Harlem suffering from asthma, whywouldnt she target interventions towards schools? Through the schools, she can make contact with children at highrisk for asthma, as opposed to hoping that their parents will seek medical care, something which, lacking healthinsurance or other financial means, they might not do.
-
8/14/2019 Building Stronger Communities for Better Health - JCPES PL USA - 2004
11/18
6 Joint Center for Political and Economic Studies / PolicyLink
Cultural CharacteristicsValues, attitudes, and norms(related to a range of behaviors,including diet) deriving fromrace/ethnicity, gender, religion,and nationality, as well as fromother types of social and culturalgroupings.
Common value systemsprovide cohesion, a sense ofcommunity, and access tokey cultural institutions withhealthy cultural norms/attributes.
Racism, language barriers, andacceptance of unhealthy behav-iors are difficult to counteract ifcommunity norms and expec-tations that promote healthybehavior and community safetyare absent.
Social Support and NetworksNetworksof friends, family,
colleagues, and neighborhoodacquaintances within the com-munity and beyond it, such asthrough churches and clubs.
Social capital can provideaccess to social supports and
economic opportunities,as well as to certain healthservices and resources. Adultrole models and peer networksare influential among youngpeople.
Residents lack social supportsand role models, particularly
access to networks outside theneighborhood that could linkthem to employment and otherkey opportunities (sometimesreferred to as absence of bridg-ing social capital).
Community Leadership andOrganizationLevel of capacity for mobiliza-tion, civic engagement, andpolitical power.
Community leaders andorganizations provide neededsupport and services. Politicalpower allows needed resourcesto be leveraged into the neigh-borhood.
Lack of leadership, organiza-tion, and political powerimpedes the flow of resourcesneeded for neighborhoodproblem-solving and hampersdevelopment of communityleadership.
Reputation of theNeighborhoodResidents and outsiders percep-tions of the neighborhood mayaffect behavior connected with it.
Neighborhoods perceived asgood or improving, withimportant social and economicattributes, are conducive tonew investment.
Poor and bad neighbor-hoods are subject to negativestereotypes and discriminatedagainst, limiting success ofisolated improvement efforts.
COMMUNITY
CHARACTERISTICS
PROTECTIVE
FACTORS
RISK
FACTORS
ECONOMIC
ENVIRONMENT
SOCIALENVIRONM
ENT
RACIALETHNICANDECONOMICINFLU
ENCE
Employment, Income, Wealthand AssetsQuality and quantity of employ-ment opportunities available toresidents; the amount of col-lective wealth and assets in thecommunity.
Living-wage jobs with healthbenefits, safe workplaces, sav-ings, retirement, and home-eownership provide economicstability.
Low-wage jobs with unsafeworking conditions and nobenefits result in racial andeconomic segregation andconcentrated poverty, whichlead to higher stress levels andpremature mortality.
Neighborhood EconomicConditionsPresence of commercial services,including grocery stores, banks,
and restaurants.
Commercial presence attractspublic and private investmentin services and infrastructure.
Disinvestment leads to lossof jobs and businesses and todeclines in property values.
-
8/14/2019 Building Stronger Communities for Better Health - JCPES PL USA - 2004
12/18
Building Stronger Communities for Better Health
7Joint Center for Political and Economic Studies / PolicyLink
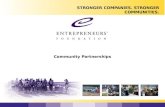
Environmental QualityAir, water, land shared across aregion.
Policies and practices thatmaintain a clean, healthyenvironment.
Presence of and exposure totoxics and pollution.
Built Environment andInfrastructureHousing, parks and recreationalsites, and workplaces.
Urban design supports accessto affordable, high-qualityhousing, recreation, and safeworkplaces, thus supportingphysical activity and promot-ing health.
The environment may containexposure to lead paint, inad-equate sanitation, and pestinfestation and may includemore dangerous types of workand unsafe work environments.In addition, urban design may
inhibit physical activity.
Public SafetyThe ways in which the designand social climate of communi-ties influence safety, including theprevalence of crime, violence, andtraffic/pedestrian accidents.
Getting the desired and neces-sary amount of police and fireprotection results in reducedcrime and increases in street/sidewalk activity and inter-action.
Prevalence of violence breedsfear, isolation, and a reluctanceto seek even needed services,as residents avoid leaving theirhomes and spending timeoutside.
Geographic Access to Oppor-tunities Throughout the Region
Mobility and the ability to con-nect to resources within andbeyond the neighborhood.
Convenient location and mo-bility allow access to services,
employment, and cultural andrecreational resources.
Homes are isolated from jobcenters, particularly areas
without public transit access,and are at a distance from rec-reational facilities or safe parksfor exercise and other health-promoting activities.
Health ServicesAccessibility, affordability, andquality of care for individuals andfamilies.
Necessary, accessible care is de-livered in a culturally sensitivemanner in satisfactory healthfacilities with well-trained andculturally appropriate practi-tioners.
There may be a lack of ac-cess to necessary health careservices, while what is availablemay be of poor quality andculturally inappropriate.
Community and PublicSupport ServicesNeighborhood-level publicservices, including schools, parks,transit, sanitation, police andfire protection, and child-carecenters. Community institutionsinclude churches, social clubs,and block groups.
Quality support services actas important neighborhoodinstitutions, providing servicesas well as venues for neighbor-hood meetings and leadershipdevelopment.
Needed services are notavailable, while those in theneighborhood may be of poorquality and undependable.
COMMUNITY
CHARACTERISTICS
PROTECTIVE
FACTORS
RISK
FACTORS
PHYSICALENVIRONM
ENT
SERVICES
RACIALETHNICAND
ECONOMICINFLUENCE
-
8/14/2019 Building Stronger Communities for Better Health - JCPES PL USA - 2004
13/18
8 Joint Center for Political and Economic Studies / PolicyLink
isolated without adequate public transportation.Policies that provide workers with transportationto new job centers could significantly improve
the economic standards of poor communities.Strong transportation systems also facilitate accessto health care for many low-income residents.
Support inclusive housing policies. Regulatoryand financing strategies that require a set-aside ofnew housing units for low- and moderate-incomehouseholds foster mixed-income communitiesand reduce concentrated poverty. In addition toproviding decent housing, such programs trans-late into access to jobs, schools, retail businesses,and the social connections that can enhance
quality of life and access to opportunities.
Encourage public and private reinvestment in low-income communities. Direct subsidies, tax credits,loan guarantees, and other incentives that subsidizeprivate investment in low-wealth communities cancreate double bottom line outcomes, benefitingboth investors and communities when they are tiedto concrete community benefits. Such benefits shouldinclude local employment opportunities, businessesthat serve the community, and living-wage jobs.In economically strong urban centers, these effortsmust be implemented hand in hand with afford-able housing to avoid residential displacement.
Expand Health-Care Access and Quality
Expand access to affordable, quality health care.African Americans and, to an even greater extent,Latinos are disproportionately represented amongthe nations 43 million non-elderly uninsured.27 Inaddition to preserving existing health care programs
such as Medicare, Medicaid, and the ChildrensHealth Insurance Program (CHIP), the long-termgoal should be universal access to health care. For
African Americans and Latinos in rural areas, thescarcity and inadequacy of health care service isfurther exacerbated by the lack of public transporta-tion to access those services. Cultural and languagecompetency standards for health-care providers andthe recruitment and training of minority healthprofessionals should also be part of the solution.
Revise eligibility rules that restrict access tocare. Eligibility rules that restrict access to healthcare based on immigration status pose additionalobstacles for Latinos and other immigrants. Key
steps are expanding access and ensuring enroll-ment upon eligibility. In some areas, commu-nity health outreach workers play an importantrole in efforts to link immigrants with avail-able services. These types of programs shouldbe expanded and targeted, as appropriate.
Improve the Physical Environment ofCommunities
Improve air quality. Low-income communi-ties are far more likely to be located near freeways,
industrial sites, and high levels of diesel traffic andtrucking facilities, which contribute to poor airquality and a higher incidence of asthma. In someareas, environmental justice advocates are usinglitigation to seek enforcement of current Clean AirAct standards. Other efforts involve changing busand truck idling rules, relocating bus depots fur-ther from homes and schools, and ensuring thatnew schools are not sited next to freeways. (SeeBreathing Easier, the second issue brief in this
A Note About Racism
The legacy of racism in the United States, and the many ways it continues to impact the lives and health of peopleof color, was a frequent and powerful theme that emerged in PolicyLink conversations with African American andLatino elected officials and community health leaders.
The interviews make it clear that, until the nation comes to grips with racism and the various ways it continues toaffect healthwhether through limited educational and economic opportunities, residential segregation, or the cu-mulative mental and physical effects of stressthe ultimate goal of eliminating health disparities will remain elusive.
-
8/14/2019 Building Stronger Communities for Better Health - JCPES PL USA - 2004
14/18
Building Stronger Communities for Better Health
9Joint Center for Political and Economic Studies / PolicyLink
series, for additional information and policy ap-proaches to reduce the incidence of asthma.)
Expand the availability of open space. Increasingthe number, safety, and affordability of exercise ven-
ues, such as parks and walking paths, is an importantprerequisite for increased physical activity. Policiesand practices to encourage more pedestrian- andexercise-friendly communities must be as relevant forlow-income neighborhoods as for new subdivisions.
Expand affordable housing. Decent affordable hous-ing is critical for families economic stability as wellas for their health, given the prevalence of asthma,lead poisoning, and other problems associatedwith dilapidated units. Enforcement of habitabilitystandards, increased focus on lead abatement efforts,
and additional funds for affordable housing construc-tion could be secured through further low-incomehousing tax credits, a national housing trust fund,or increased enforcement of Community Reinvest-ment Act requirements for financial institutions.
Encourage brownfields redevelopment. Brown-fields, defined as abandoned, idle, or under-usedindustrial or commercial facilities where expan-sion or redevelopment is complicated by a realor perceived environmental contamination, aredisproportionately found in low-income, urban
communities of color. Their commercial redevelop-ment is an untapped opportunity that will requirenew approaches to environmental remediation.
Expand Opportunities for Quality Educationand for Social and Civic Engagement
Improve the quality of public education. Educationremains a key determinant of health. Middle-class
flight to the suburbs and suburban sprawl have inten-sified the racial and economic segregation of schools,and continuing inequities in education funding
have perpetuated significant disparities in per-pupilfunding levels. Poorly funded school systems aremore likely to lack strong physical education classesand facilities, contributing to growing disparities infitness. In addition, school systems without adequatefunding for new school construction or moderniza-tion are more likely to have air quality problems with-in school buildings, which can trigger asthma attacks.
Expand support for non-governmental socialinstitutions serving as community anchors. Acrossthe country, community health centers, educationalinstitutions, and neighborhood-based commu-nity development organizations are uniting diverseinterests within the community in pursuit of thecommon goal of better health. They are putting intopractice the concepts in this framework, and shouldbe better supported and replicated through appro-priate governmental and philanthropic initiatives.
Support community organizing strategies and localleadership development. Expansion of leadershipdevelopment opportunities, particularly amongpeople of color, and support for local organizingefforts often bear residual benefits for communi-ties above and beyond a given issue or campaign.This is a relatively low-cost option that can bringcommunities substantial long-term rewards.
CONCLUSION
The community effects framework illustrated mostconcisely in the Conceptual Framework table em-phasizes that the determinants of health, and thereforeeffective strategies to eliminate racial and ethnic healthdisparities, cannot be viewed solely within the scope of
traditional health policy. Instead, policymakers and localhealth leaders will need to look to other sectors, includingeconomic development, transportation, housing, employ-ment development, and education, for policy solutions thataddress more environmental and community conditions.
While this proposed shift in focus toward prevention andcommunity environments is not entirely new, neither willit be easy. However, a range of policy options and strate-
Community members senseof ownership is key. You must
create an expectation forparticipation in order to fostera pattern of participation. Sylvia Drew Ivie, T.H.E. Clinic for Women
-
8/14/2019 Building Stronger Communities for Better Health - JCPES PL USA - 2004
15/18
10 Joint Center for Political and Economic Studies / PolicyLink
gies exist, some with shorter time horizons than others.Some of these options will require new resources, butothers can be achieved by redirecting current resources or
by changing existing regulations.
Meeting the challenge posed by todays health disparitieswill require the full participation of the public, private,and philanthropic sectors. Local initiatives supported byboth the public and private sectors can serve as the basisfor further targeted investments. Private foundations havealready aimed grant-making at comprehensive initiativesrooted in local communities. Finally, all strategies thatstrengthen communities of color will benefit from localleadership and initiative.
As policymakers, advocates, and community leaders, now
is the time to work together to move this important agendaforward. The health of our communities demands it.
-
8/14/2019 Building Stronger Communities for Better Health - JCPES PL USA - 2004
16/18
Building Stronger Communities for Better Health
11Joint Center for Political and Economic Studies / PolicyLink
Notes
1. For more information, see the Healthy People website:
http://www.healthypeople.gov.
2. B. Smedley, A. Stith, and A. Nelson, eds., UnequalTreatment: Confronting Racial and Ethnic Disparities inHealth Care(Washington, DC: National Academy Press,2003): 1-28.
3. This report is available online: http://qualitytools.ahrq.gov/disparitiesReport/download_report.aspx.
4. J. M. McGinnis and W. Foege, Actual Causes of Deathin the United States,Journal of the American Medical Asso-ciation270 (1993): 22072212.
5. PolicyLink, Reducing Health Disparities Through a Focuson Communities (PolicyLink Report, November 2002),12-21. This report was prepared through a grant from TheCalifornia Endowment (TCE).
6. Ibid.
7. I. G. Ellen, K. Dillman, and T. Mijanovich, Neighbor-hood Effects on Health: Exploring the Links and Assessingthe Evidence,Journal of Urban Affairs, Vol. 23 (2001).
8. S. MacIntyre and A. Ellaway, Ecological Approaches:Rediscovering the Role of the Physical and Social Envi-ronment, in Social Epidemiology, edited by L. Berkmanand I. Kawachi (London: Oxford University Press, 2000):332-348.
9. Social capital is defined as Those features of socialorganization such as the extent of interpersonal trustamong citizens, norms of reciprocity, and density of civicorganizations that facilitate cooperation for mutualbenefit. I. Kawachi, B. Kennedy, V. Gupta, and D.Prothrow-Stith, Social Capital, Income Inequality, andMortality,American Journal of Public Health87 (1997):
149198.
10. Reports of research relating health to socioeconomicstatus includes the following: N. E. Adler et al., Socio-economic Status and Health: The Challenge of the Gradi-ent,American Psychologist49 (1994): 1524; E. Backlundet al., A Comparison of the Relationships of Educationand Income with Mortality: The National LongitudinalMortality Study, Social Science & Medicine49 (1999):137384; M. Haan, G. A. Kaplan, and T. Camacho,
Poverty and Health: Prospective Evidence from theAlameda County Study,American Journal of Epidemiology125(1987)(6): 989998; J. S. House and D. R. Wil-
liams, Understanding and Reducing Socioeconomic andRacial/Ethnic Disparities in Health, in Promoting Health:Intervention Strategies from Social and Behavioral Research,edited by B. D. Smedley and S. L. Syme (Washington,DC: Institute of Medicine/National Academy Press,2000): 81-124. N. Krieger and E. Fee, Social Class: TheMissing Link in U.S. Health Data,Journal of HealthServices24 (1994): 2544.
11. Blau and Duncan were among the first sociologists toemploy a causal framework this way. See P. Blau and O.D.Duncan, The American Occupational Structure(New York:Wiley, 1967).
12. See R. G. Wilkinson, Unhealthy Societies: The Afflic-tions of Inequality(London: Routledge, 1996).
13. N. E. Adler et al., Socioeconomic Status and Health:The Challenge of the Gradient,American Psychologist, 49(1994): 15-24; M. G. Marmot et al., Health Inequali-ties Among British Civil Servants: The Whitehall HealthStudy, Lancet337 (1991).
14. Ibid.; Haan, Kaplan, and Camacho, Poverty andHealth: Prospective Evidence from the Alameda CountyStudy.
15. J. S. House and D.R. Williams, Understanding andReducing Socioeconomic and Racial/Ethnic Disparities inHealth, in Promoting Health: Intervention Strategies fromSocial and Behavioral Research, edited by B.D. Smedleyand S.L. Syme (Washington, D.C.: Institute of Medicine/National Academy Press, 2000): 81-124.
16. D. Williams, Race and Health: Basic Questions,Emerging Directions, Annals of Epidemiology 7 (1997):322333.
17. Racial Integrations Shifting Patterns: Enclaves Per-sist, BlackWhite Divide Shrinks, The Washington Post,April 1, 2001, p. A-1.
18. D. S. Massey, Residential Segregation and Neighbor-hood Conditions in U. S. Metropolitan Areas, in N. J.Smelser, W. J. Wilson and F. Mitchel, eds.,America Be-coming: Racial Trends and Their Consequences(Washington,DC: National Academy Press, 2001): 391-434.
-
8/14/2019 Building Stronger Communities for Better Health - JCPES PL USA - 2004
17/18
12 Joint Center for Political and Economic Studies / PolicyLink
19. Ibid., p. 411.
20. M. Orfield,American Metropolitics: The New Suburban
Reality (Washington: The Brookings Institution Press,2002): 162-167.
21. G. T. Kingsley and K. Pettit, Concentrated Poverty:A Change in Course(Washington, D.C.: Urban InstitutePolicy Brief, 2003); P. A. Jargowsky, Stunning Progress,Hidden Problems: The Dramatic Decline of ConcentratedPoverty in the 1990s(Brookings Institution Center on Ur-ban and Metropolitan Policy, Living Cities Census Series,2003).
22. A. Blackwell and H. McCulloch, Opportunities forSmart Growth (PolicyLink and Funders Network for
Smart Growth Translation Paper, December 1999).
23. R. E. Zambrana and O. CarterPokras, HealthData Issues for Hispanics: Implications for Public HealthResearch,Journal of Health Care for the Poor and Under-served, 12(1)(February 2001): 2034.
24. P. Gordon-Larsen et al., Acculturation and Over-weight-Related Behaviors Among Hispanic Immigrants tothe U.S.: The National Longitudinal Study of AdolescentHealth, Social Science & Medicine57 (2003): 202334;S. Guendelman and B. Abrams, Dietary Intake AmongMexican American Women: Generational Differences
and a Comparison With White Non-Hispanic Women,American Journal of Public Health85 (1995): 2025; J. N.Variyam, J. R. Blaylock, and D. M. Smallwood, Diet-Health Knowledge and Nutrition: The Intake of Dietary Fatsand Cholesterol(Economic Research Service, U.S. Depart-ment of Agriculture, Technical Bulletin No. 1855, 1997).
25. In the interviews with African American and Latinoelected officials and health leaders, universal access to careemerged as a continuing priority.
26. A Community Benefits Agreement is a legally enforce-able contract, signed by community groups and develop-ers, setting forth a range of community benefits that devel-oper agrees to provide as part of a development contract.
27. C. Hoffman, and M. Wang, Health Insurance Coveragein America, 2002 Data Update(The Kaiser Commissionon Medicaid and the Uninsured, Kaiser Family Founda-tion, December 2003): 12. To access this report online seethe foundations website at www.kff.org.
-
8/14/2019 Building Stronger Communities for Better Health - JCPES PL USA - 2004
18/18
Joint Center for Political and Economic Studies1090 Vermont Avenue, Suite 1100
Washington, DC 20005www.jointcenter.org