Brugada Syndrome - JACC: Case Reports · 2019-06-07 · Brugada Syndrome Death Reveals its...
2
IMAGING VIGNETTE ECG CHALLENGE Brugada Syndrome Death Reveals its Perpetrator Kiersten Frenchu, MD, Shane Flood, MD, Lauren Rousseau, MPAS, PA-C, CCDS, Athena Poppas, MD, Antony Chu, MD ABSTRACT Rapid diagnosis of Brugada syndrome is critical to therapy, which is aimed at reversing provoking factors to suppress/terminate malignant arrhythmias. This case highlights the diagnosis and peri-operative management of patients with Brugada syndrome at high risk for sudden cardiac death. (Level of Difficulty: Beginner.) (J Am Coll Cardiol Case Rep 2019;1:55–6) © 2019 The Authors. Published by Elsevier on behalf of the American College of Cardiology Foundation. This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/). B rugada syndrome is an inherited channelopathy that confers an increased risk of sudden cardiac death (SCD). Approximately 25% of individuals affected with Brugada syndrome demonstrate a mutation in the SCN5a sodium channel (1). Baseline electrocardiography (ECG) results may be electrophysiologi- cally normal and therefore confound the diagnosis. Provoking factors may be required to unmask the Brugada ECG pattern (2). This case highlights the discovery and management of a patient with heretofore undiagnosed Brugada syndrome. CASE REPORT A 50-year-old female with a history of essential hypertension and hyperlipidemia presented with fever and abdominal pain. She denied any chest pain, palpitations, or syncope prior to admission, and acute appendicitis was diagnosed. Her baseline ECG was unremarkable. Pre-operatively, she developed spontaneous ventricular fibrillation (VF) and was found unresponsive and required a 200-J biphasic shock for termination. After defibrillation, her ECG revealed new ST-segment elevations, right bundle branch pattern, and coved, persis- tently elevated ST-segments in V 1 and V 2 , consistent with type 1 Brugada syndrome (Figure 1). DISCUSSION Treatment of this patient required rapid diagnosis of Brugada syndrome by ECG findings and clinical history. This patient’s post-arrest ECG is demonstrative for type 1 Brugada, with coved ST-segment elevations of >2 mm in V 1 to V 2 and a negative T-wave in the setting of right bundle branch block (1,2). Importantly, the QTc complex is normal in patients with Brugada syndrome as the most common mutations involve sodium channel defects (as opposed to potassium channel defects that lead to QTc abnormalities). Treatment of Brugada syndrome is aimed at prevention of SCD with an automatic implantable cardioverter- defibrillator (AICD); however, that was contraindicated in this patient due to her active infection (2). She was managed acutely with quinidine, the most effective general therapy, with a plan to administer isoproterenol to prevent further episodes of arrhythmia if needed for electrical storm (2). Therapy consisting of hydration, SEE PAGE 57 ISSN 2666-0849 https://doi.org/10.1016/j.jaccas.2019.05.016 From the Department of Internal Medicine, Brown University Rhode Island Hospital, Providence, Rhode Island. The authors have reported that they have no relationships relevant to the contents of this paper to disclose. Manuscript received April 1, 2019; revised manuscript received April 29, 2019, accepted May 2, 2019. JACC: CASE REPORTS VOL. 1, NO. 1, 2019 ª 2019 THE AUTHORS. PUBLISHED BY ELSEVIER ON BEHALF OF THE AMERICAN COLLEGE OF CARDIOLOGY FOUNDATION. THIS IS AN OPEN ACCESS ARTICLE UNDER THE CC BY-NC-ND LICENSE ( http://creativecommons.org/licenses/by-nc-nd/4.0/ ).
Transcript of Brugada Syndrome - JACC: Case Reports · 2019-06-07 · Brugada Syndrome Death Reveals its...

J A C C : C A S E R E P O R T S V O L . 1 , N O . 1 , 2 0 1 9
ª 2 0 1 9 T H E A U T H O R S . P U B L I S H E D B Y E L S E V I E R O N B E H A L F O F T H E A M E R I C A N
C O L L E G E O F C A R D I O L O G Y F OU N D A T I O N . T H I S I S A N O P E N A C C E S S A R T I C L E U N D E R
T H E C C B Y - N C - N D L I C E N S E ( h t t p : / / c r e a t i v e c o mm o n s . o r g / l i c e n s e s / b y - n c - n d / 4 . 0 / ) .
IMAGING VIGNETTE
ECG CHALLENGE
Brugada Syndrome
Death Reveals its PerpetratorKiersten Frenchu, MD, Shane Flood, MD, Lauren Rousseau, MPAS, PA-C, CCDS, Athena Poppas, MD, Antony Chu, MD
ABSTRACT
ISS
Fro
rep
Ma
Rapid diagnosis of Brugada syndrome is critical to therapy, which is aimed at reversing provoking factors to
suppress/terminate malignant arrhythmias. This case highlights the diagnosis and peri-operative management of
patients with Brugada syndrome at high risk for sudden cardiac death. (Level of Difficulty: Beginner.)
(J Am Coll Cardiol Case Rep 2019;1:55–6) © 2019 The Authors. Published by Elsevier on behalf of the
American College of Cardiology Foundation. This is an open access article under the CC BY-NC-ND license
(http://creativecommons.org/licenses/by-nc-nd/4.0/).
B rugada syndrome is an inherited channelopathy that confers an increased risk of sudden cardiac death(SCD). Approximately 25% of individuals affected with Brugada syndrome demonstrate a mutation inthe SCN5a sodium channel (1). Baseline electrocardiography (ECG) results may be electrophysiologi-
cally normal and therefore confound the diagnosis. Provoking factors may be required to unmask the BrugadaECG pattern (2). This case highlights the discovery and management of a patient with heretofore undiagnosedBrugada syndrome.
SEE PAGE 57
CASE REPORT
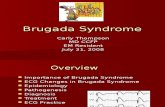
A 50-year-old female with a history of essential hypertension and hyperlipidemia presented with fever andabdominal pain. She denied any chest pain, palpitations, or syncope prior to admission, and acute appendicitiswas diagnosed. Her baseline ECG was unremarkable. Pre-operatively, she developed spontaneous ventricularfibrillation (VF) and was found unresponsive and required a 200-J biphasic shock for termination. Afterdefibrillation, her ECG revealed new ST-segment elevations, right bundle branch pattern, and coved, persis-tently elevated ST-segments in V1 and V2, consistent with type 1 Brugada syndrome (Figure 1).
DISCUSSION
Treatment of this patient required rapid diagnosis of Brugada syndrome by ECG findings and clinical history.This patient’s post-arrest ECG is demonstrative for type 1 Brugada, with coved ST-segment elevations of>2 mm in V1 to V2 and a negative T-wave in the setting of right bundle branch block (1,2). Importantly, the QTccomplex is normal in patients with Brugada syndrome as the most common mutations involve sodium channeldefects (as opposed to potassium channel defects that lead to QTc abnormalities).
Treatment of Brugada syndrome is aimed at prevention of SCD with an automatic implantable cardioverter-defibrillator (AICD); however, that was contraindicated in this patient due to her active infection (2). She wasmanaged acutely with quinidine, the most effective general therapy, with a plan to administer isoproterenol toprevent further episodes of arrhythmia if needed for electrical storm (2). Therapy consisting of hydration,
N 2666-0849 https://doi.org/10.1016/j.jaccas.2019.05.016
m the Department of Internal Medicine, Brown University Rhode Island Hospital, Providence, Rhode Island. The authors have
orted that they have no relationships relevant to the contents of this paper to disclose.
nuscript received April 1, 2019; revised manuscript received April 29, 2019, accepted May 2, 2019.

FIGURE 1 Type 1 Brugada Syndrome
Frenchu et al. J A C C : C A S E R E P O R T S , V O L . 1 , N O . 1 , 2 0 1 9
Brugada Syndrome: Death Reveals its Perpetrator J U N E 2 0 1 9 : 5 5 – 6
56
electrolyte replenishment, and antipyretic administration was optimized. In regard to management, there arecurrently conflicting views of the use of amiodarone and lidocaine in Brugada syndrome and evidence thatprocainamide should be avoided (2).
Perioperatively, the patient received an infusion of isoproterenol. She underwent an uncomplicated lapa-roscopic appendectomy, with slow peritoneal insufflation and deflation to avoid increased vagal tone, anothertrigger for ventricular arrhythmias in the setting of Brugada syndrome.
The patient had no further arrhythmia episodes. Her echocardiogram result was normal. Prior to discharge,an AICD was placed after her infection resolved. Later, she reported that her father had died suddenly at age 45years. Genetic testing was recommended for her and her first-degree family members.
CONCLUSIONS
Rapid diagnosis of Brugada syndrome unmasked by triggers is critical to therapy designed to reverse provokingfactors and suppress or terminate lethal episodes of ventricular arrhythmia. This case outlines perioperativemanagement of patients with Brugada syndrome at high risk for SCD, particularly those with an index pre-sentation secondary to acute illness. Following is an overview of Brugada management:
� Acute management of Brugada syndrome includes optimizing hydration, correcting electrolyte abnormal-ities, and using antipyretics and quinidine.
� A secondary preventative of SCD from type 1 Brugada syndrome following VF arrest involves placement ofan AICD.
� For patients undergoing surgery, vigilant planning is required.� Genetic testing should be recommended to the patient and the patient’s first-degree family members.
ADDRESS FOR CORRESPONDENCE: Dr. Kiersten Frenchu, Brown Medicine, 245 Chapman Street, ProvidenceRhode Island 02905. E-mail: [email protected].
RE F E RENCE S
1. Juang JJ, Horie M. Genetics of Brugada syn-drome. J Arrhythm 2016;32:418–25.
2. Antzelevitch C, Fish JM. Therapy for the Bru-gada syndrome. Handb Exp Pharmacol 2006:305–30.
KEY WORDS electrocardiography, suddencardiac death