Bronchiectasis and autoimmune disease
19
Chapter 13 Bronchiectasis and autoimmune disease D.J. Dhasmana and R. Wilson Summary The association between bronchiectasis and autoimmune disease is well recognised, and best described with rheumatoid arthritis. The prevalence of bronchiectasis in rheumatoid arthritis varies considerably in studies, with obliterative bronchiolitis a common feature. The prognosis of rheumatoid arthritis with bronchiectasis seems to be worse than either condition alone. The advent of high-resolution computed tomography has increased the sensitivity of detecting bronch- iectasis, but this should be assessed for clinical significance. Traction bronchiectasis results from interstitial fibrosis pulling the airway wider, rather than damage weakening the bronchial wall, and is less likely to lead to bronchial suppuration. Bronchial wall damage in bronchiectasis is caused by inflam- mation, but it is difficult to differentiate damage caused by severe or recurrent infections, predisposed to by immunosup- pression related to the autoimmune disease itself or its treatment, from damage caused by the autoimmune process. Increased use of new immunomodulatory or immunosuppres- sive agents has proved successful in modifying autoimmune disease processes, but has also led to emergence of infective complications that can cause bronchiectasis or exacerbate pre- existing disease. Keywords: Autoimmune, bronchiectasis, immunosuppression, rheumatoid arthritis, Sjo ¨gren’s syndrome, vasculitis Host Defence Unit, Royal Brompton Hospital, London, UK. Correspondence: R. Wilson, Royal Brompton Hospital, Fulham Road, London, SW3 6NP, UK, Email [email protected] Eur Respir Mon 2011. 52, 192–210. Printed in UK – all rights reserved. Copyright ERS 2011. European Respiratory Monograph; ISSN: 1025-448x. DOI: 10.1183/1025448x.10004310 A n association between bronchiectasis and autoimmune disease has long been recognised. The main autoimmune diseases in which bronchiectasis has been described are discussed in this chapter with emphasis on rheumatoid arthritis, for which there is best evidence of a true association. When information is available we discuss estimated prevalence, pathogenesis, clinical features and management where this differs from that in usual bronchiectasis and prognosis. In addition, we have discussed screening and risk stratification in the context of immunosuppression following the use of biological agents such as anti-tumour necrosis factor (TNF) in autoimmune disease. 192 BRONCHIECTASIS AUTOIMMUNITY
Transcript of Bronchiectasis and autoimmune disease

Chapter 13
Bronchiectasis andautoimmune diseaseD.J. Dhasmana and R. Wilson
Summary
The association between bronchiectasis and autoimmunedisease is well recognised, and best described with rheumatoidarthritis. The prevalence of bronchiectasis in rheumatoidarthritis varies considerably in studies, with obliterativebronchiolitis a common feature. The prognosis of rheumatoidarthritis with bronchiectasis seems to be worse than eithercondition alone. The advent of high-resolution computedtomography has increased the sensitivity of detecting bronch-iectasis, but this should be assessed for clinical significance.Traction bronchiectasis results from interstitial fibrosis pullingthe airway wider, rather than damage weakening the bronchialwall, and is less likely to lead to bronchial suppuration.Bronchial wall damage in bronchiectasis is caused by inflam-mation, but it is difficult to differentiate damage caused bysevere or recurrent infections, predisposed to by immunosup-pression related to the autoimmune disease itself or itstreatment, from damage caused by the autoimmune process.Increased use of new immunomodulatory or immunosuppres-sive agents has proved successful in modifying autoimmunedisease processes, but has also led to emergence of infectivecomplications that can cause bronchiectasis or exacerbate pre-existing disease.
Keywords: Autoimmune, bronchiectasis, immunosuppression,rheumatoid arthritis, Sjogren’s syndrome, vasculitis
Host Defence Unit, Royal BromptonHospital, London, UK.
Correspondence: R. Wilson, RoyalBrompton Hospital, Fulham Road,London, SW3 6NP, UK, [email protected]
Eur Respir Mon 2011. 52, 192–210.Printed in UK – all rights reserved.Copyright ERS 2011.European Respiratory Monograph;ISSN: 1025-448x.DOI: 10.1183/1025448x.10004310
An association between bronchiectasis and autoimmune disease has long been recognised. Themain autoimmune diseases in which bronchiectasis has been described are discussed in this
chapter with emphasis on rheumatoid arthritis, for which there is best evidence of a trueassociation. When information is available we discuss estimated prevalence, pathogenesis, clinicalfeatures and management where this differs from that in usual bronchiectasis and prognosis. Inaddition, we have discussed screening and risk stratification in the context of immunosuppressionfollowing the use of biological agents such as anti-tumour necrosis factor (TNF) in autoimmunedisease.
19
2B
RO
NC
HIE
CT
AS
ISA
UT
OIM
MU
NIT
Y

There are several recurringthemes that are worth noting:1) high-resolution computedtomography (HRCT) scan-ning, which has significant-ly increased the sensitivity ofimaging of bronchiectasis, wasnot available when older stu-dies were performed and sothe diagnosis of bronchiecta-sis may be less certain; 2)presence of radiological bron-chiectasis versus symptomaticdisease; and 3) the use ofretrospective data in analysesof complex often heteroge-neous populations. Anothertheme is traction bronchiec-tasis that may be present inpatients with lung fibrosis dueto involvement of the lungparenchyma by autoimmunedisease-causing fibrosis. Thescarring pulls the airwaysapart as it contracts. The air-way mucosa is normal withintact mucociliary clearanceand possibly for this reasonpatients are not usually proneto bacterial infections. How-ever, in some cases with trac-tion bronchiectasis there willalso be bronchiectasis in partsof the lung without fibrosis,suggesting that an inflam-matory process has involvedthe airways and damaged thestructure of the bronchial wall.These patients may be moreprone to the clinical syndromeof bronchiectasis. A summaryof the features of the mainstudies carried out are shownin table 1.
Autoantibodies should not beroutinely tested for during theinvestigation of a patient withbronchiectasis; they shouldonly be tested for if thereare particular clinical featuresraising autoimmunity as apossible association [50]. Inaddition, rheumatoid factor is
Ta
ble
1.
Sum
mary
of
the
featu
res
of
bro
nchie
cta
sis
ind
iffere
nt
auto
imm
une
dis
ease
s
Dis
ea
se
Ap
pro
xim
ate
pre
va
len
ce
inm
ain
stu
die
sP
ati
en
tse
lec
tio
na
nd
stu
dy
typ
eC
om
me
nts
[Re
f.]
RA
2–5
0%
Mix
ed
sele
cte
dand
unse
lecte
dLarg
est
bod
yof
data
,va
riab
leconclu
sions
but
larg
est
evi
dence
base
of
auto
imm
une
dis
ease
s[1
–12]
Sjo
rge
n’s
,10–4
6%
Mix
ed
sele
cte
dand
unse
lecte
dM
ost
data
base
don
incid
enta
lfin
din
gs
on
HR
CT,
patie
nts
often
asy
mp
tom
atic
[13–1
6]
SL
E,
2–2
1%
Vario
us,
inclu
din
gla
rge
pro
spectiv
eand
cro
ss-s
ectio
nal
Fre
quent
find
ing
of
bro
nchie
cta
sis
on
HR
CT
but
poor
corr
ela
tion
with
sym
pto
ms;
com
plic
atio
ns
of
infe
ctio
nand
thro
mb
osi
sare
signfic
ant
and
may
dom
inate
ove
rclin
ically
meanin
gfu
lb
ronchie
cta
sis
[17–1
9]
AS
7–2
3%
Mix
ed
sele
cte
dand
unse
lecte
dTra
ctio
nb
ronchie
cta
sis
com
mon,
but
usu
ally
asy
mp
tom
atic
;m
orb
idity
usu
ally
thro
ugh
non-r
esp
irato
rycom
plic
atio
ns
[17,
20–2
4]
Sc
lero
de
rma
f59%
Mix
ed
sele
cte
dand
unse
lecte
dN
SIP
,p
ulm
onary
hyp
ert
ensi
on
and
tractio
nb
ronchie
cta
sis
com
mon;
prim
ary
bro
nchie
cta
sis
less
soand
perh
ap
sm
ore
in’d
iffuse
’d
isease
[25–2
9]
RP
f50%
Mix
ed
sele
cte
dand
unse
lecte
dS
eve
ralold
stud
ies
pre
-1986
and
pre
-HR
CT
solik
ely
gro
ssove
rest
imate
[30–3
4]
MC
TD
12%
Vario
us
sele
cte
dW
here
pre
sent,
tractio
nb
ronchie
cta
sis
more
likely
than
prim
ary
bro
nchie
cta
sis,
again
usu
ally
asy
mp
tom
atic
[35–3
7]
PM
/DM
Rare
Prim
ary
bro
nchie
cta
sis
not
desc
ribed
NS
IPand
org
anis
ing
pneum
onia
com
mon,
tractio
nb
ronchie
cta
sis
rare
lyre
port
ed
and
prim
ary
bro
nchie
cta
sis
rare
[38–4
0]
Va
sc
uliti
sV
ario
us
accord
ing
toty
pe
Mix
ed
sele
cte
dand
unse
lecte
dG
ranulo
mato
sis
with
poly
angiit
is(W
egener’
s)and
MP
Am
ost
com
mon
of
prim
ary
vasc
ulit
ides;
BP
I-A
NC
Alin
ked
toP
seud
om
onas
[41–4
9]
RA
:rh
eum
ato
idart
hrit
is;
SLE
:sy
stem
iclu
pus
ery
them
ato
sus;
AS
:anky
losi
ng
spond
yliti
s;R
P:
rela
psi
ng
poly
chond
ritis
;M
CTD
:m
ixed
connectiv
etis
sue
dis
ease
;P
M/D
M:
poly
moyo
sitis
/derm
ato
myo
sitis
;H
RC
T:hig
h-r
eso
lutio
ncom
pute
dto
mogra
phy;
NS
IP:nonsp
ecifi
cin
ters
titia
lpneum
onia
;M
PA
:m
icro
scop
icp
oly
angiit
is;B
PI-
AN
CA
:b
acte
ricid
al/
perm
eab
ility
-incre
asi
ng
pro
tein
-antin
eutr
op
hil
cyt
op
lasm
icantib
od
ies.
19
3D
.J.
DH
AS
MA
NA
AN
DR
.W
ILS
ON

nonspecific but high levels do characterise a group of patients with prominent small airwaysdisease in whom immunosuppression should be considered. Anti-cyclic citrullinated peptidewhich is more specific for rheumatoid arthritis has not as yet been investigated in relation tobronchiectasis.
Rheumatoid arthritis
The association of rheumatoid arthritis and bronchiectasis is well described [1, 51] and it is themajor autoimmune condition associated with bronchiectasis. One important question whichremains unanswered is how the two conditions are related and how one develops in the context ofthe other. One hypothesis is that the initial event is recurrent antigen stimulation from recurrentlower respiratory tract infections, and the immunopathological sequence of events that followsleads to the development of a multi-system inflammatory disorder with a predilection forarthropathy. An alternative hypothesis is that bronchiectasis arises from the immunosuppressionassociated with rheumatoid arthritis itself and/or its treatments.
Prevalence
The reported prevalence of rheumatoid arthritis with bronchiectasis varies considerably largelydue to patient selection and study type. Reports describe between approximately 2% and 50%prevalence of bronchiectasis in the largest studies of rheumatoid arthritis published between 1967and 2006 [1–12]. A major issue is whether radiological evidence of bronchiectasis, either by chestradiography or by HRCT scanning, represents disease that is clinically significant. Studies thathave tried to explore this demonstrate poor correlation with radiology [3, 8, 9, 52]. In moststudies, the prevalence is calculated on the HRCT findings rather than on clinical evidence ofbronchiectasis and patients may be entirely asymptomatic with incidental HRCT findings.
Most reports of prevalence have used heterogeneous populations and so carry several potentialconfounding characteristics including duration of illness, age (mean age of 45–64 yrs acrossstudies), cigarette smoking history and drug-treatment schedules, which might include cor-ticosteroids and immunosuppressants, such as methotrexate, which could influence susceptibilityto infection. Moreover, the data is typically retrospective bringing with it recall and reporter bias.DESPAUX et al. [8] report prospective data on 46 unselected patients with rheumatoid arthritis(34 females, 12 males; mean age 60.1 yrs) collected over an 18-month period. In this study inwhich all patients had a HRCT, they found 23 (50%) patients with radiological evidence ofbronchiectasis, 18 of whom were previously undiagnosed. 13 (57%) of these 18 patients wereasymptomatic, thus giving a total of 22% (10 out of 46 patients) with clinically significantbronchiectasis. In two other prospective studies of 75 consecutive patients [10] and 63consecutive patients [12] with rheumatoid arthritis, 19% and 29% of patients, respectively, werefound to have bronchiectasis on HRCT, although it is not clear what proportion of these weresymptomatic. A retrospective uncontrolled study of 20 life-long nonsmokers showed a highproportion of bronchiectasis with five (25%) out of 20 demonstrating basal bronchiectaticchanges, but whilst three of these five gave a past history of pleurisy or pneumonia none hadongoing symptoms [3]. In other more heterogeneous studies, sub-group analysis has not beenable to demonstrate a relationship between smoking and bronchiectasis in rheumatoid arthritis[8, 9, 52]. We are not aware of any study that has attempted to correlate the severity ofbronchiectasis using one of the accepted scoring systems with severity of arthritis, either in termsof joint damage or immunological measures.
The immunological diagnosis of rheumatoid arthritis may also complicate prevalence data. Inparticular, there may be other autoimmune diseases present within the population studied, such asSjogren’s syndrome [53, 54]. With modern day biochemical and immunological markers, there isa more robust system to better differentiate autoimmune diseases from one another, which willallow better definition of disease in the future.
19
4B
RO
NC
HIE
CT
AS
ISA
UT
OIM
MU
NIT
Y

Finally, the patient’s ethnic status may have an additional impact on the development ofbronchiectasis with rheumatoid arthritis. This is rarely mentioned within studies. The largestcohorts are described in France close to the Alps [8] and close to the North Atlantic [4], NorthAfrica [9], New England in the USA [2] and in central and northern England, UK [3]. Theantigenic stimulation by community pathogens is likely to vary markedly in these differentsettings.
Pathogenesis
Whilst the association of bronchiectasis and rheumatoid arthritis has long been recognised[1, 8, 51], the mechanisms of how one condition develops in the context of the other remainsunclear. While the co-existence of the two separate conditions is possible, the frequency ofbronchiectasis in rheumatoid arthritis is well above that found in the non-rheumatoid arthritispopulation and suggests that these are not chance findings [4, 7, 8]. Three mechanisms have beenconsidered: 1) bronchiectasis gives rise to the development of rheumatoid arthritis; 2) bron-chiectasis and rheumatoid arthritis are caused by similar immunological processes, or because ofimmunosuppression due to rheumatoid arthritis or its treatments; and 3) other diagnoses and/orcomorbid conditions drive the development of rheumatoid arthritis or bronchiectasis. These willbe discussed in turn, although in reality there may well be several mechanisms interacting in aparticular case.
Bronchiectasis gives rise to the development of rheumatoid arthritis
The nature of the complex immunological mechanisms present in the bronchiectatic airways hasbeen studied. The neutrophil plays a central role in what has been called ‘‘the vicious circlehypothesis’’, but in addition abnormal mucus clearance and cellular immune responses areimportant [55–58]. In this context, one proposed mechanism is that persistent immunologicalpressure stimulated by chronic bacterial infection drives a sequence of events that leads to theformation of autoantibodies to ‘‘self’’ components and ultimately the development of a systemicinflammatory disorder. For this mechanism to operate lung disease would need to precederheumatoid arthritis. Most reports suggest that this is the case. DESPAUX et al. [7] described froman extensive literature review that 90% of 289 reports published since 1928 document respiratorysymptoms prior to articular symptoms. While this study combines old reports with variablediagnostic criteria for both rheumatoid arthritis as well as bronchiectasis, in an era beforecomputed tomography (CT) imaging, the temporal sequence is in fact corroborated in severalindividual and more recent studies [4, 5, 54]. Even in newly diagnosed rheumatoid arthritispresent for ,1 year, with normal chest radiographs and normal respiratory function tests, 58% ofpatients were found to have HRCT evidence of bronchiectasis. This study demonstratesestablished bronchiectasis, albeit subclinical, by the time of a formal diagnosis of rheumatoidarthritis [59]. However, since the bronchiectasis was subclinical, sufficient antigenic stimulation bybacterial infection seems unlikely.
Bronchiectasis is caused by similar immunological processes or byimmunosuppression due to rheumatoid arthritis or its treatments
HRCT has made it clear that airway disease is common in rheumatoid arthritis (fig. 1). Follicularbronchiolitis is due to lymphoid aggregates, with or without germinal centres, which lie in the wallof bronchioles and sometimes compress their lumens. This appears as centrilolobular nodules,peribronchial nodules and patches of ground-glass shadowing [60]. Airway wall thickening(indicating bronchitis without dilatation) and bronchiectasis (fig. 1a and b) are both morecommon in patients than matched controls [61].
There is a recognised association of rheumatoid arthritis and obliterative bronchiolitis, also known as‘‘constrictive bronchiolitis’’, in which bronchioles are destroyed and replaced by scar tissue (fig. 1c).
19
5D
.J.
DH
AS
MA
NA
AN
DR
.W
ILS
ON
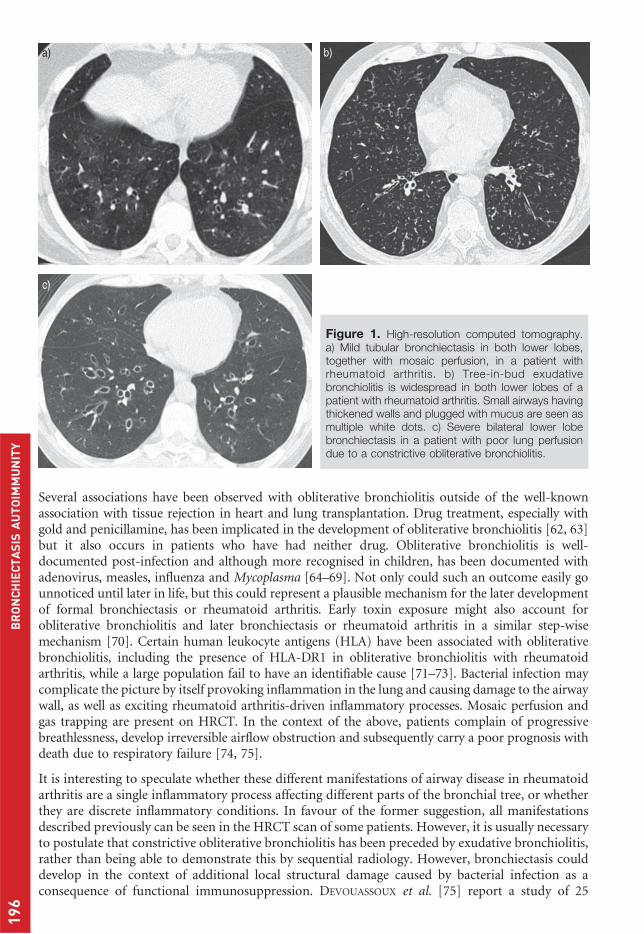
Several associations have been observed with obliterative bronchiolitis outside of the well-knownassociation with tissue rejection in heart and lung transplantation. Drug treatment, especially withgold and penicillamine, has been implicated in the development of obliterative bronchiolitis [62, 63]but it also occurs in patients who have had neither drug. Obliterative bronchiolitis is well-documented post-infection and although more recognised in children, has been documented withadenovirus, measles, influenza and Mycoplasma [64–69]. Not only could such an outcome easily gounnoticed until later in life, but this could represent a plausible mechanism for the later developmentof formal bronchiectasis or rheumatoid arthritis. Early toxin exposure might also account forobliterative bronchiolitis and later bronchiectasis or rheumatoid arthritis in a similar step-wisemechanism [70]. Certain human leukocyte antigens (HLA) have been associated with obliterativebronchiolitis, including the presence of HLA-DR1 in obliterative bronchiolitis with rheumatoidarthritis, while a large population fail to have an identifiable cause [71–73]. Bacterial infection maycomplicate the picture by itself provoking inflammation in the lung and causing damage to the airwaywall, as well as exciting rheumatoid arthritis-driven inflammatory processes. Mosaic perfusion andgas trapping are present on HRCT. In the context of the above, patients complain of progressivebreathlessness, develop irreversible airflow obstruction and subsequently carry a poor prognosis withdeath due to respiratory failure [74, 75].
It is interesting to speculate whether these different manifestations of airway disease in rheumatoidarthritis are a single inflammatory process affecting different parts of the bronchial tree, or whetherthey are discrete inflammatory conditions. In favour of the former suggestion, all manifestationsdescribed previously can be seen in the HRCT scan of some patients. However, it is usually necessaryto postulate that constrictive obliterative bronchiolitis has been preceded by exudative bronchiolitis,rather than being able to demonstrate this by sequential radiology. However, bronchiectasis coulddevelop in the context of additional local structural damage caused by bacterial infection as aconsequence of functional immunosuppression. DEVOUASSOUX et al. [75] report a study of 25
a) b)
c)
Figure 1. High-resolution computed tomography.a) Mild tubular bronchiectasis in both lower lobes,together with mosaic perfusion, in a patient withrheumatoid arthritis. b) Tree-in-bud exudativebronchiolitis is widespread in both lower lobes of apatient with rheumatoid arthritis. Small airways havingthickened walls and plugged with mucus are seen asmultiple white dots. c) Severe bilateral lower lobebronchiectasis in a patient with poor lung perfusiondue to a constrictive obliterative bronchiolitis.
19
6B
RO
NC
HIE
CT
AS
ISA
UT
OIM
MU
NIT
Y

patients with rheumatoid arthritis and obliterative bronchiolitis and demonstrate HRCT evidence ofbronchiectasis in 44% of the cohort. All patients were breathless and bronchorrhoea was present in44%. They go on to report that in a follow-up of approximately 4 years, treatment was poorlyeffective, chronic respiratory failure occurred in 40% and death in four patients.
Rheumatoid arthritis itself is associated with increased morbidity and specifically an increased riskof infection when compared with the general population [76–78]. In a predisposed individual,regular infection with poor immunological clearance of microbes could subsequently lead toformation of bronchiectasis. In contrast to the reports described previously, SHADICK et al. [2]describes 23 patients with rheumatoid arthritis and bronchiectasis, in whom 18 (78%) patientshad rheumatoid arthritis symptoms prior to the diagnosis of bronchiectasis. These patients had amean duration of arthritic symptoms of 25 years prior to bronchiectasis, 17 out of 18 patients hadused corticosteroids and respiratory symptoms were present for an average of 4.3 years prior tothe formal diagnosis of bronchiectasis. When compared with the five patients who describedbronchiectasis before rheumatoid arthritis, those with late bronchiectasis used more disease-modifying agents, had more severe joint disease, were more likely to have rheumatoid nodules andcarried a greater morbidity. This would support the idea that advanced rheumatoid arthritisdisease and increasingly immunosuppressive medications might contribute to the development of‘‘secondary’’ bronchiectasis as a late complication of rheumatoid arthritis.
Methotrexate forms part of many rheumatoid arthritis treatment regimens and despite earlyclinical impressions, probably does not significantly increase the infection risk in patients withpoorly controlled rheumatoid arthritis [79–81]. This may be because the immunosuppressivenature of unchecked inflammation in rheumatoid arthritis in the absence of methotrexateis greater than that conferred by methotrexate itself. However, long-term corticosteroids,cyclophosphamide and azathioprine certainly do lower the threshold for opportunistic infectionand with the emergence of biological agents such as anti-TNF, the complication of seriousinfection and ensuing bronchiectasis becomes more likely [82]. In patients with recurrentinfections on rheumatoid arthritis-treatments it is difficult to define the nature of any immuneparesis, and where specific functional defects are demonstrated it is difficult to ascribe them to thedisease or the therapy that has been prescribed. Gold has been associated with functional antibodydefects, but in a study of rheumatoid arthritis patients with and without bronchiectasis, evidenceof antibody deficiency was apparent in those with bronchiectasis as well as those without, andindependent of any co-incident gold therapy [83]. Other reports of late bronchiectasis may havecase-specific explanations, where resistant pathogens, abnormal airways and/or impaired clearancelead to unchecked infection and inflammation and usually localised bronchiectasis [84].
Other diagnoses or comorbid conditions that drive the development ofrheumatoid arthritis and bronchiectasis
In most cases today, a clear diagnosis of rheumatoid arthritis and bronchiectasis can be made thatis based upon the history, clinical features and immunology profile. However, in older studies it isworth noting that either the diagnosis of rheumatoid arthritis may be incorrect, or there may besignificant comorbid conditions that drive the disease phenotype. For example, the finding ofgreater numbers of abnormal Schirmer’s tests (test of tear production) by MCMAHON et al. [54] ina case-controlled study of 32 patients with rheumatoid arthritis and bronchiectasis whencompared with rheumatoid arthritis without bronchiectasis did increase the possibility thatSjogren’s syndrome was involved in the pathogenesis of one or both conditions, possibly byaffecting mucociliary clearance in the lung. However, this finding was not reproduced byMCDONAGH et al. [52], and KELLY and GARDINER et al. [53] who found no significant difference inabnormal tear production in their rheumatoid arthritis patients with bronchiectasis (six out of 10patients) compared with those without bronchiectasis (18 out of 30 patients).
The cystic fibrosis transmembrane conducatance regulator (CFTR) mutation DF508 present incystic fibrosis (CF) has been implicated through a study of a French cohort that has demonstrated
19
7D
.J.
DH
AS
MA
NA
AN
DR
.W
ILS
ON
its increased presence in rheumatoid arthritis with bronchiectasis [85]. In this study, four (15.4%)out of 26 Caucasians with a median age of 59 years with rheumatoid arthritis and bronchiectasiscarried the heterozygote genotype compared with none from 29 consecutive rheumatoid arthritispatients without bronchiectasis, and none from 29 patients with diffuse bronchiectasis. This is astriking difference when noted in the context of a 2.8% allelic frequency in the general CaucasianEuropean population. In addition, those with the mutation demonstrated more frequent sinusitis,lower nasal potential differences and a trend towards more severe lower respiratory tract disease,while there was no relationship to the severity of articular features.
HLA associations are well characterised for rheumatoid arthritis and the HLA-DRB1 gene locusfrom the DR4 ‘‘family’’ is perhaps the most closely associated susceptibility locus implicated inrheumatoid arthritis [86]. In a large case-controlled study of patients’ HLA associations in a UKcohort, HILLARBY et al. [87] demonstrated the predicted DR4 association in 79% of rheumatoidarthritis alone patients but no pattern of DR4 subtypes in those with rheumatoid arthritis andadditional respiratory features, including pulmonary fibrosis and bronchiectasis. However, therewas a significant association of rheumatoid arthritis and bronchiectasis with DQB1*0601,DQB1*0301, DQB1*0201 and DQA1*0501 when compared with rheumatoid arthritis alone. Thegroup of patients with bronchiectasis in a separate prospective HRCT study of 68 consecutiverheumatoid arthritis patients showed a low prevalence of DQA1*0501 when compared with therheumatoid arthritis group without bronchiectasis [6].
Immune dysregulation is seen in both bronchiectasis and rheumatoid arthritis, and a shared defectin both rheumatoid arthritis and bronchiectasis may impact upon the shape of the final diseasephenotype. Common variable immunodeficiency (CVID) is the most common primaryimmunodeficiency and is frequently associated with both respiratory tract infections andautoimmune conditions including rheumatoid arthritis [88]. Defective antibody production hasbeen recognised in rheumatoid arthritis and with rheumatoid arthritis treatments. A UK study of80 patients was carried out and comprised of 20 patients with rheumatoid arthritis andbronchiectasis, 20 patients with each disease separately and 20 healthy matched controls. Threeout of 20 from the rheumatoid arthritis-bronchiectasis group demonstrated an impaired antibodyresponse post-immunisation, two out of 20 rheumatoid arthritis alone patients showed a poorresponse (both groups of patients contained individuals on gold therapy) and the control groupdemonstrated neither. Immunological defects, when investigated, are likely to be more commonthan is currently believed and may play important roles as co-factors in the developingbronchiectasis [89].
Yellow nail syndrome (YNS) is a heterogeneous disorder that includes bronchiectasis and has beenassociated with rheumatoid arthritis-drug therapy, particularly penicillamine. YNS does occur inrheumatoid arthritis and other autoimmune diseases independent of drug therapy and itsaetiology remains unclear [90, 91]. Abnormal T-cell responses that are thought to drive disease inYNS may similarly drive a specific phenotype in the presence of rheumatoid arthritis and act as aco-factor in development of bronchiectasis.
Management of bronchiectasis in the presence of rheumatoid arthritis
There are no specific features in the management of bronchiectasis associated with rheumatoidarthritis. We have not identified any patients requiring antibody replacement in our own group ofrheumatoid arthritis-bronchiectasis patients, but it would be reasonable to measure total antibodylevels and specific antibody responses to polysaccharide (pneumococcal and Haemophilusinfluenzae type b and protein (tetanus)). Some patients have progressive obliterative small airwaysdisease. Our own experience is that there is a poor response in these patients to increasingimmunosuppression, and this approach to treatment creates more problems by making infectionsworse. Once the patient is established by the rheumatologist on a regimen that may includemethotrexate, we have adopted the strategy of trying to reduce the level of bronchial infection byusing antibiotic prophylaxis, including the ketolide antibiotic azithromycin as a putative
19
8B
RO
NC
HIE
CT
AS
ISA
UT
OIM
MU
NIT
Y

immunomodulator [92], and treating exacerbations aggressively. We hypothesise that avoiding theantigenic stimulation of bacterial infections may reduce the inflammatory processes causingobliterative bronchiolitis.
Prognosis
The presence of bronchiectasis with rheumatoid arthritis appears to carry a significantly worseprognosis, although only one report examines mortality and morbidity in this specific context.SWINSON et al. [93] studied a UK cohort of 32 rheumatoid arthritis patients with bronchiectasisalongside matched controls with either rheumatoid arthritis alone or bronchiectasis alone. Theyfound the mortality in the group with both diseases to be considerably higher, with a standardisedmortality ratio five times and 2.4 times greater than that of the rheumatoid arthritis alone andbronchiectasis alone groups, respectively. The groups shared similar scores of physical activity andof radiological destruction (Larsen score). While several parameters carried high relative risks ofmortality including grip strength and presence of rheumatoid nodules, the finding of a raisedwhite cell count and the presence of circulating immune complexes carried the highest relativerisks, the latter being the only one which demonstrated confidence intervals outside parity (relativerisk 4.5, 95% CI 1.4–13.9). The 5-year survival rate in the combined rheumatoid arthritis-bronchiectasis group can be calculated at 69%. Finally, it is interesting to note that those in thecombined disease group did have a lower baseline forced expiratory volume in 1 s (FEV1), as wellas lower forced vital capacity (FVC) and fewer patients with signs of reversibility. Airflowobstruction in the presence of lung restriction has been identified in one large bronchiectasis studyas a risk factor for mortality. In this study, carried out over 13 years, 29.7% of patients withbronchiectasis of many different aetiologies died [94]. In contrast, MCMAHON et al. [54] reportedno significant effect of bronchiectasis on the activity and outcome measures of arthritis whencompared with those with rheumatoid arthritis alone.
Sjogren’s syndrome
The study of the association of Sjogren’s syndrome and bronchiectasis has been made moredifficult by: the presence of primary, secondary and mixed syndromes; serological overlap withsystemic lupus erythematosus (SLE; in particular, Sjogren syndrome-related antigen A) and alsosystemic sclerosis; and the inconsistencies in the literature about how the diagnosis ofbronchiectasis was made. The diagnosis of Sjogren’s syndrome includes the presence of dry eyesand dry mouth for 3 months, a positive Schirmer’s test, anti-Ro and anti-La autoantibodies and aminor salivary gland biopsy demonstrating a focus score .1. While the use of this definition wasnot clear across all studies, an international consensus was obtained to rectify the differences [95].Clinically significant bronchiectasis is uncommon and so most information on the prevalence ofbronchiectasis in Sjogren’s syndrome necessarily comes from imaging studies of patients withrespiratory symptoms or from studies in those who are asymptomatic. Bronchiectasis is variablyreported in such studies ranging from ,10% to 46% [13–16]. In a study of 24 German patientswith primary Sjogren’s syndrome (excluding smokers and those with other autoimmune disease orother unrelated bronchopulmonary disorders), 19 were found to have HRCT abnormalities and 11of these bronchiectatic changes (46% of all patients) [14]. These changes were more central,predominantly lower lobe, bilateral in eight cases and unilateral in three cases. The precisesymptoms of these patients are not given but the cohort comprised of patients referred forinvestigation over a 10-year period to a tertiary referral centre.
The aetiology of Sjogren’s syndrome is unknown but viral infection is implicated, includ-ing Epstein–Barr virus (EBV), cytomegalovirus and retroviruses such as HIV and humanT-lymphocyte virus, with good evidence from animal studies [96]. Both B- and T-cells arerecognised to infiltrate exocrine glands but the pathogenesis is likely to involve a complex interplayof glandular epithelial and endothelial cells, dendritic cells and B- and T-cells in the context of anenvironmental insult in a predisposed individual [97]. Hydration of the airways may be impaired
19
9D
.J.
DH
AS
MA
NA
AN
DR
.W
ILS
ON
together with inspissations of secretions as a result of atrophied respiratory tract mucus glands.Bronchiectasis is proposed to develop subsequently due to recurrent bacterial infections which arepredisposed to by impaired mucociliary clearance. Neutrophilic inflammation provoked byinfection leads to thickened dilated lower airways and eventually bronchial wall destruction.Amyloid has been recognised in Sjogren’s syndrome and may be implicated in the development ofbronchiectasis with its presence confirmed in peribronchial walls, as well as the interstitium [98].
Management of bronchiectasis associated with Sjogren’s syndrome
There are no clinical studies reported in the literature. In our own practice we have attempted toimprove mucus clearance by nebulising normal saline regularly several times per day andemphasising to patients the importance of physiotherapy. Recently we have begun to nebulise 7%hypertonic saline which has an osmotic effect, with success in individual cases. Optimal antibioticmanagement of lower respiratory tract infections may shorten the length of infective exacerbationsand so reduce airway wall damage.
Systemic lupus erythematosus
The first reports of bronchiectasis in SLE emerged in the early 1960s with the use of bronchogramsand pulmonary function tests [99–101]. With the advent of CT imaging, there has been a greaterunderstanding of the radiological abnormalities in SLE. However, there remains some uncertaintyabout the significance of the reported abnormalities and the prevalence of clinically significantbronchiectasis. FENLON et al. [17] prospectively studied 34 patients with SLE with HRCT dataalongside various clinical and lung function data. Of note, they found seven (21%) patients withbronchiectasis on HRCT, second only to interstitial lung disease (ILD) (11 patients), mediastinalor axillary lymphadenopathy (six patients) and pleuropericardial abnormalities (five patients).However, while the presence of HRCT abnormalities was high they found no correlation withsymptoms or disease activity, and none of the patients had recurrent respiratory infections. In aseparate cross-sectional study of 60 Norwegian adults of childhood-onset SLE, any HRCTabnormality was found in only five patients and in just one (,2%) was there radiological evidenceof bronchiectasis; none had clinical evidence of bronchiectasis [18]. These patients had a medianduration of 11 years of disease by the time of cross-sectional imaging. In contrast, BANKIER et al.[19] reported a much higher frequency of CT abnormalities with 17 out of 48 patients with SLEshowing abnormalities (45 of whom had normal chest radiographs). They went on to showcorrelation of extent of disease radiologically with duration of clinical history (r50.93), gastransfer (r50.8) and ratio of FEV1/FVC (r50.77). However, once again there was poor correlationof bronchiectasis on CT scans and clinical symptoms of the disease. Lung fibrosis may causetraction bronchiectasis and it is not clear in reports whether bronchiectasis is present in parts ofthe lung not affected by fibrosis.
As with other systemic diseases, it has been suggested that confounding factors might explain theassociation of bronchiectasis with SLE, including the increased risk of infection associated with amulti-system disease and use of immunosuppressive treatments to control the disease. Mannose-binding lectins (MBL) have been suggested to play a role in SLE in a report of two patients withSLE who went on to develop CVID [102]. The infrequent MBL haplotype 4Q-57Glu was presentin both, while the haplotype 4P-57Glu in the second case was associated with recurrent respiratoryinfections, bronchiectasis and low circulating levels of MBL. This report raises the possibility ofMBL polymorphisms in the development of autoimmune disease and significant infections whichcause bronchiectasis.
The clinical features of bronchiectasis in SLE are not described in the literature. However, it isapparent that the most common pulmonary complications are infection and vascular events [103].While the reported frequency of clinical bronchiectasis is low, as described previously, there maybe under-diagnosis of post-infective bronchiectasis in patients who have not had HRCT examination.
20
0B
RO
NC
HIE
CT
AS
ISA
UT
OIM
MU
NIT
Y

Respiratory function tests frequently demonstrate reduced spirometry (typically subclinical), reducedgas diffusion and, depending on severity of disease, decreased lung capacity. These changes appear tobe independent of cigarette smoking [103–105].
HRCT features reported in SLE include pleuritis with or without pleural effusion, acute interstitialpneumonia and acute pulmonary haemorrhage and thrombosis [17, 106]. Morbidity andmortality in SLE are associated with infection and vascular complications [107, 108]. There isgreater mortality in the first 5 years, partly linked to the use of immunosuppressive therapy inaggressive SLE disease and the subsequent complications of infection surrounding this.
Ankylosing spondylitis
There are several pulmonary manifestations of ankylosing spondylitis which include apicalfibrobullous disease, secondary infection, chest wall restriction, obstructive sleep apnoea,spontaneous pneumothorax and bronchiectasis [109]. A typical course is the development ofchronic bi-apical fibrobullous areas with nodules that eventually coalesce to form cysts, cavitiesand bronchiectasis, and later superadded infection with Aspergillus and environmental Myco-bacteria species may occur. Abnormalities evident on HRCT in those either asymptomatic or withearly disease are well documented with frequencies of all abnormalities in the region of 40% to80% [20–22, 110]. However, little is published regarding bronchiectasis specifically. HRCTevidence of bronchiectasis has been found in 7–23% of ankylosing spondylitis patients in thelargest cohort studies performed to date [17, 20, 21–24]; in most studies, patients do not reportsymptoms of bronchiectasis. Traction bronchiectasis is the most likely explanation in this contextcaused by pleuropulmonary fibrosis. FENLON et al. [111] reported a total of six (23%) cases ofbronchiectasis from their prospective cohort study of 26 patients with ankylosing spondylitis froman out-patient setting in Ireland, of which four were primary bronchiectasis and two had tractionbronchiectasis. The four with primary bronchiectasis consisted of three patients with significantsmoking histories, two each with disease in the upper and lower lobes and only one withsymptoms of cough and breathlessness. The latter patient with bronchiectasis had ankylosingspondylitis for significantly longer duration of 28 years, and had an abnormal plain chestradiograph (demonstrating upper lobe bronchiectasis) with restrictive respiratory function tests.Three out of four patients with bronchiectasis in a separate study from Brazil were also currentsmokers, although this population with several radiological abnormalities may have had otherinfective causes [23].
Tracheobronchomegaly or Mounier–Kuhn syndrome, which is due to a congenital cartilageabnormality, has also been reported with ankylosing spondylitis and this mechanism mayinfluence the development of bronchiectasis in some cases [112]. HLA-B27 does not appear tocorrelate with general HRCT abnormalities where this has been assessed, and while it is possiblethat ankylosing spondylitis disease severity correlates indirectly with respiratory abnormalities ingeneral, there are too few cases with bronchiectasis to assess any relationship with this specifically[23, 113, 114]. There is insufficient data to comment on the timing of bronchiectasis comparedwith the development of ankylosing spondylitis, although it appears that the majority of thosefound to have bronchiectasis are asymptomatic with incidental findings on imaging only [20–24,110, 115]. Ankylosing spondylitis mortality is usually caused by non-respiratory illnesses such ascardiovascular disease, renal failure and amyloid and through complications of treatment, andonly occasionally through respiratory disease [116–118].
Scleroderma/systemic sclerosis
Lung involvement in scleroderma or systemic sclerosis is very common. HRCT has played animportant role in better characterising and following up abnormalities, and disease has also beenwell documented by post mortem examination with the identification of pulmonary disease insystemic sclerosis in 80% of one cohort [25–27]. The findings of an ILD, typically a nonspecific
20
1D
.J.
DH
AS
MA
NA
AN
DR
.W
ILS
ON
interstitial pneumonia (NSIP) pattern and pulmonary hypertension, are quite common on HRCT.Any honeycombing is usually mild and localised and the more typical pattern is the near-confluentground-glass opacification, fine reticular markings and associated traction bronchiectasis. Primarybronchiectasis is uncommon [28, 29], as are reports of clinically significant disease.
In one of the larger studies of systemic sclerosis patients alone, ANDONOPOULOS et al. [29]investigated 22 patients with a full history, respiratory function tests, blood tests and HRCTimaging. Cylindrical bronchiectasis was evident in 13 (59%) out of 22 patients and was morecommon in diffuse rather than limited systemic sclerosis disease, although this finding fell shortof statistical significance and did not correlate with gas transfer, ground-glass opacification orwith the patient’s duration of illness. In another single case report of clinically significantbronchiectasis, there were other potential causes including Sicca syndrome and immunosup-pressant treatment [119].
Relapsing polychondritis
The tracheobronchial tree is affected and typically leads to thickened and sometimes narrowedairways, impaired clearance and the development of airway infection and inflammation. Lowerrespiratory tract symptoms and significant disease developed after the initial diagnosis of relapsingpolychondritis in an early and one of the largest prospective studies of 23 patients with relapsingpolychondritis [30]. However, this was not the case in the only other smaller prospective series20 years later where in six out of nine patients the respiratory symptoms were the presentingsymptoms of relapsing polychondritis [31]. Cohort studies since 1966 report a prevalence ofrespiratory symptoms in up to 50% of those with relapsing polychondritis, although given thenature and time of these studies, accurate prevalence of bronchiectasis is not possible to estimate.A small number of cohort studies have analysed the natural history, morbidity and mortality ofpatients with relapsing polychondritis. Respiratory infection appears to play a significant part.Bronchiectasis is not defined by today’s standards of HRCT imaging given that these studies werecarried out between 1966 and 1986. However, it can be implied that together with vasculitis andvalvular heart disease, respiratory infection carries a worse prognosis [30, 32, 33]. MICHET et al.[32] describe their single-centre experience of 112 patients in the US in which they identifiedrespiratory infection as one of the leading causes of death alongside vasculitis and cancer. Offurther interest is that only 10% of deaths were directly attributed to airway involvement of thedisease, that anaemia was a significant poor prognostic marker and that the use of corticosteroidsdid not impact on survival.
BEHAR et al. [34] analysed past records of a cohort of 160 patients collected over 10 years from tworeferral centres and scrutinised records from 15 patients who had undergone any thoracic CTimaging. They identified increased attenuation in the tracheal walls of all 15 patients (withnarrowing in one third of these patients), and also in the bronchial walls of 11 patients (73% ofthose scanned). Of the 11 patients who had complete lung view imaging, three were found to havebronchiectasis (two upper lobe, one diffuse), two demonstrated no significant airway stenoses andone showed widespread tracheal and bronchial stenoses. 12 (83%) out of 15 patients demonstratedthickened airway walls.
Mixed connective tissue disease
Mixed connective tissue disease (MCTD) is a distinct clinicopathological entity with uniquepositive antibodies against ribonucleoprotein that shares several clinical and radiological featureswith SLE, systemic sclerosis and polymyositis/dermatomyositis (PM/DM). The frequency ofrespiratory manifestations in MCTD is reported to be between 20% and 80%, more commonly thehigher end of this range, although the reports are typically based upon radiological findings ratherthan clinical significance [35, 120, 121]. The prevalence of bronchiectasis is not available in theseolder studies, once again because of the absence of HRCT. MCTD is not usually associated with
20
2B
RO
NC
HIE
CT
AS
ISA
UT
OIM
MU
NIT
Y
primary bronchiectasis, rather with traction bronchiectasis associated with architectural distor-tions and the interstitial pneumonia patterns more commonly seen in this disorder [36, 37].KOZUKA et al. [37] analysed the abnormal HRCT imaging of 41 patients with confirmed MCTDand characterised the radiological abnormalities that were observed. They identified 18 patientswith traction bronchiectasis. Primary bronchiectasis was observed in five (12%) out of 41 patients,although no clinical features were reported in this study to assess the significance of this.
Polymyositis/dermatomyositis
PM/DM is typically associated with ILD with a strong correlation with anti-Jo1 antibodies, mostcommonly an NSIP pattern and also an organising pneumonia [38, 39]. Primary bronchiectasis isnot reported and traction bronchiectasis is rarely reported, especially given that honeycombing isan infrequent finding in contrast to ground-glass opacification and patchy consolidation [38–40].
Bronchiectasis and vasculitis
It has long been recognised that immune complexes and autoantibodies can accompany bronchialinfection [41, 122–125]. ABRAMOWSKY and SWINEHART [123] demonstrated renal failure associatedwith immune complexes in patients with CF and immune complex-mediated injury was proposedin CF patients who presented with purpuric lesions late in their disease course [124]. Immunecomplexes adhere to the endothelium through binding with the C1q component of complementcausing vasculitis and/or the complexes interfere with the intended complement-mediatedclearance of pathogens.
The vasculitic process may be localised or involve many systems with increasing severity. Theextent of disease may be such as to require aggressive immunosuppressive therapy withcorticosteroids and cyclophosphamide to control the vasculitis, alongside continued antimicrobialtreatment for concomitant bacterial infection [126]. Evidence of immune-mediated injury andvasculitis has been demonstrated in the context of H. influenzae and Staphylococcus aureus, as wellas Pseudomonas aeruginosa [2, 42, 125].
Antineutrophil cytoplasmic antibodies (ANCA) form an important component of vasculitides ofwhich classical ANCA (c-ANCA) against the antigen proteinase-3 and perinuclear ANCA(p-ANCA) against myeloperoxidase make up the major pathogenic types [43]. Of the primaryvaculitides, granulomatosis with polyangiitis (Wegener’s) with associated c-ANCA antibodies andmicroscopic polyangiitis (MPA) with myeloperoxidase antibodies have been most linked withbronchiectasis. A chronic pulmonary illness typically predates the development of ANCA-associated disease in various reports and although other ANCA may exist their roles may be morespecific [41, 44–46]. In a retrospective cohort study of 26 patients with MPA in Japan, nine (35%)were diagnosed with bronchiectasis, four of whom had bronchiectatic symptoms prior to thediagnosis of MPA [45]. The precise role and timing of the development of autoantibodies to self-components remains unclear. FORDE et al. [47] analysed sera from a large number of patients witha wide variety of inflammatory and infective disorders in order to investigate any association ofautoantibodies with acute and chronic infection. They concluded that antibodies to neutrophiliccytoplasmic components were predominantly associated with chronic bacterial infection, whileantibodies to monocyte cytoplasmic components were predominantly associated with chronicgranulomatous disorders such as sarcoidosis. The implication was that persistent stimulation ofphagocytic cell components by bacterial infection drives the formation of autoantibodies to thosecomponents and a pathological humoral response.
More recently, studies have begun to confirm the temporal relationship of immune-complexactivity with infection. MAHADEVA et al. [48] identified and characterised a new antigenbactericidal/permeability-increasing protein (BPI)-ANCA in the context of Pseudomonas infection.They went on to identify this in several patient groups including those with CF and non-CF
20
3D
.J.
DH
AS
MA
NA
AN
DR
.W
ILS
ON
bronchiectasis, inflammatory bowel disease and renal failure [49]. Other groups explored itsbehaviour in the context of Pseudomonas and proposed that high levels of BPI-ANCA correlatedwith chronic Pseudomonas infection and poorer prognosis [46, 127, 128]. Of note, BPI binds withhigh affinity to lipopolysaccharide (LPS) on Gram-negative bacteria, and the presence of highlevels of circulating antibodies to BPI may interfere with clearance of LPS bacteria giving rise toconcomitant severe infection.
There are several other rare primary immunodeficiencies that are associated with bronchiectasisand vasculitis about which little is known. For example, an X-linked lymphoproliferative disorderlinked to a specific T-cell defect in EBV immunity that is associated with multi-system vasculitis,bronchiectasis, respiratory failure and death [129] and an, as yet, poorly defined syndromeconsisting of childhood dermatitis, profoundly elevated immunoglobulin E, severe pneumonia(and subsequent bronchiectasis) and multiple central neurological abnormalities [130].
The use of immunosuppressive agents and bronchiectasis
There is an increasing use of immunomodulatory or immunosuppressive therapy that is provingsuccessful in modifying autoimmune disease processes [82]. However, their availability has raisedfresh concerns, mainly surrounding opportunistic infection and cancer [131–135]. In theautoimmune diseases discussed herein, those drugs used frequently include steroid-sparing agentssuch as azathioprine and methotrexate, alternative potent immunosuppressive drugs such asleflunomide and cyclophosphamide, biological agents that include anti-TNF agents (etanercept,infliximab and adalimumab), anti-CD20 molecules (rituximab), interleukin (IL)-6 receptorantagonists (tocizilimab) and co-stimulatory inhibitor molecule (abatacept).
Reactivation of tuberculosis (TB) is a recognised risk of the use of anti-TNF therapy and theBritish Thoracic Society and others have issued guidelines for their use in those at risk of TBreactivation [136, 137]. TB and nontuberculous Mycobacteria [138] are pathogens that can bothcause bronchiectasis and infect patients with existing bronchiectasis. Care must be taken to stratifythe risk of reactivation following immunosuppressive therapies, and one should be aware thattraditionally non-pathogenic strains can emerge as fatal infections [139]. Evidence for latent TBinfection should be sought with the use of a detailed history, chest radiograph or CT, tuberculinskin testing and interferon-c release assays (IGRA). IGRAs are now well established and should beused to ‘‘risk-stratify’’ in the context of anti-TNF therapy. While in theory latent viruses includingherpes zoster and EBV, fungus, opportunistic bacteria and parasites are all more likely to re-emerge with immunosuppressive therapy, this has not been a consistent finding [140–145].
There may be a gradation of risks within this group of agents. Anti-CD20 therapy in the form ofrituximab may generally be considered less aggressive. CD20 is expressed by haematopoieticprogenitor cells and newly differentiated plasma cells, and while reactivation of latent virus is welldocumented, infection with other bacteria or parasites or TB is infrequently reported [146, 147].Safety and long-term data are still emerging with tocilizumab, an IL-6 receptor antagonist foundto be effective in rheumatoid arthritis and still being investigated for SLE [147–150]. To date, nosurprising opportunistic infection data has emerged and meta-analyses have placed a figure ofapproximately six additional infections per 100 patient-years; those infections are mostly termed‘‘pneumonia’’ [149, 151]. Abatacept, a newer co-stimulatory modulator that interferes with T-cellactivation may not share the same documented risks of TB reactivation and may prove to be bettertolerated than anti-TNF therapies, although longer term safety data on this drug is still emerging[152–155].
In general, physicians using these agents must be diligent and counsel patients about the risks ofinfections, particularly if patients already have susceptibility to infection due to concomitantbronchiectasis. In this case the patient should be co-managed with a respiratory physician, sputumshould be screened for Mycobacteria sp. and other opportunistic pathogens, the patient shouldhave an antibiotic management plan if infective exacerbations develop, and antibiotic prophylaxis
20
4B
RO
NC
HIE
CT
AS
ISA
UT
OIM
MU
NIT
Y
should be considered if infective exacerbations become frequent. These agents often providemarked improvement in the patient’s control of their autoimmune disease, which means thatwhen the agents are used in bronchiectasis patients with associated autoimmune disease, treatmentof chronic bronchial infection and infective exacerbations of bronchiectasis should be intensifiedto allow the agent to be continued when this is deemed to be safe. Good communication betweenthe rheumatologist and pulmonologist is essential.
Statement of interest
None declared.
References1. Walker WC. Pulmonary infections and rheumatoid arthritis. Q J Med 1967; 36: 239–251.
2. Shadick NA, Fanta CH, Weinblatt ME, et al. Bronchiectasis. A late feature of severe rheumatoid arthritis.
Medicine (Baltimore) 1994; 73: 161–170.
3. Hassan WU, Keaney NP, Holland CD, et al. High resolution computed tomography of the lung in lifelong non-
smoking patients with rheumatoid arthritis. Ann Rheum Dis 1995; 54: 308–310.
4. Allain J, Saraux A, Guedes C, et al. Prevalence of symptomatic bronchiectasis in patients with rheumatoid
arthritis. Rev Rhum Engl Ed 1997; 64: 531–537.
5. Despaux J, Polio JC, Toussirot E, et al. Rheumatoid arthritis and bronchiectasis. A retrospective study of fourteen
cases. Rev Rhum Engl Ed 1996; 63: 801–808.
6. Cortet B, Perez T, Roux N, et al. Pulmonary function tests and high resolution computed tomography of the
lungs in patients with rheumatoid arthritis. Ann Rheum Dis 1997; 56: 596–600.
7. Despaux J, Toussirot E, Wendling D. Bronchectasies et polyarthrite rhumatoide. Frequence et aspects
etiopathogeniques. Revue de la litterature. [Bronchiectasis and rheumatoid arthritis. Incidence and
etiopathogenic aspects. Review of the literature]. Rev Med Interne 1997; 18: 144–152.
8. Despaux J, Manzoni P, Toussirot E, et al. Prospective study of the prevalence of bronchiectasis in rheumatoid
arthritis using high-resolution computed tomography. Rev Rhum Engl Ed 1998; 65: 453–461.
9. Kochbati S, Boussema F, Ben Miled M, et al. Bronchiectasis in rheumatoid arthritis. High resolution computed
pulmonary tomography. Tunis Med 2003; 81: 768–773.
10. Zrour SH, Touzi M, Bejia I, et al. Correlations between high-resolution computed tomography of the chest and
clinical function in patients with rheumatoid arthritis. Prospective study in 75 patients. Joint Bone Spine 2005; 72:
41–47.
11. Lieberman-Maran L, Orzano IM, Passero MA, et al. Bronchiectasis in rheumatoid arthritis: report of four cases
and a review of the literature - implications for management with biologic response modifiers. Semin Arthritis
Rheum 2006; 35: 379–387.
12. Mohd Noor N, Mohd Shahrir MS, Shahid MS, et al. Clinical and high resolution computed tomography
characteristics of patients with rheumatoid arthritis lung disease. Int J Rheum Dis 2009; 12: 136–144.
13. Koyama M, Johkoh T, Honda O, et al. Pulmonary involvement in primary Sjogren’s syndrome: spectrum of
pulmonary abnormalities and computed tomography findings in 60 patients. J Thorac Imaging 2001; 16: 290–296.
14. Lohrmann C, Uhl M, Warnatz K, et al. High-resolution CT imaging of the lung for patients with primary
Sjogren’s syndrome. Eur J Radiol 2004; 52: 137–143.
15. Uffmann M, Kiener HP, Bankier AA, et al. Lung manifestation in asymptomatic patients with primary Sjogren
syndrome: assessment with high resolution CT and pulmonary function tests. J Thorac Imaging 2001; 16:
282–289.
16. Yazisiz V, Arslan G, Ozbudak IH, et al. Lung involvement in patients with primary Sjogren’s syndrome: what are
the predictors? Rheumatol Int 2010; 30: 1317–1324.
17. Fenlon HM, Doran M, Sant SM, et al. High-resolution chest CT in systemic lupus erythematosus. AJR Am J
Roentgenol 1996; 166: 301–307.
18. Lilleby V, Aaløkken TM, Johansen B, et al. Pulmonary involvement in patients with childhood-onset systemic
lupus erythematosus. Clin Exp Rheumatol 2006; 24: 203–208.
19. Bankier AA, Kiener HP, Wiesmayr MN, et al. Discrete lung involvement in systemic lupus erythematosus:
CT assessment. Radiology 1995; 196: 835–840.
20. El Maghraoui A, Chaouir S, Abid A, et al. Lung findings on thoracic high-resolution computed tomography in
patients with ankylosing spondylitis. Correlations with disease duration, clinical findings and pulmonary
function testing. Clin Rheumatol 2004; 23: 123–128.
21. Senocak O, Manisali M, Ozaksoy D, et al. Lung parenchyma changes in ankylosing spondylitis: demonstration
with high resolution CT and correlation with disease duration. Eur J Radiol 2003; 45: 117–122.
22. Souza AS, Muller NL, Marchiori E, et al. Pulmonary abnormalities in ankylosing spondylitis: inspiratory and
expiratory high-resolution CT findings in 17 patients. J Thorac Imaging 2004; 19: 259–263.
20
5D
.J.
DH
AS
MA
NA
AN
DR
.W
ILS
ON

23. Sampaio-Barros PD, Cerqueira EM, Rezende SM, et al. Pulmonary involvement in ankylosing spondylitis. Clin
Rheumatol 2007; 26: 225–230.
24. Turetschek K, Ebner W, Fleischmann D, et al. Early pulmonary involvement in ankylosing spondylitis:
assessment with thin-section CT. Clin Radiol 2000; 55: 632–636.
25. D’Angelo WA, Fries JF, Masi AT, et al. Pathologic observations in systemic sclerosis (scleroderma). A study of
fifty-eight autopsy cases and fifty-eight matched controls. Am J Med 1969; 46: 428–440.
26. Schurawitzki H, Stiglbauer R, Graninger W, et al. Interstitial lung disease in progressive systemic sclerosis:
high-resolution CT versus radiography. Radiology 1990; 176: 755–759.
27. Remy-Jardin M, Remy J, Wallaert B, et al. Pulmonary involvement in progressive systemic sclerosis: sequential
evaluation with CT, pulmonary function tests, and bronchoalveolar lavage. Radiology 1993; 188: 499–506.
28. Wells AU. High-resolution computed tomography and scleroderma lung disease. Rheumatology (Oxford) 2008;
47: Suppl. 5, v59–v61.
29. Andonopoulos AP, Yarmenitis S, Georgiou P, et al. Bronchiectasis in systemic sclerosis. A study using high
resolution computed tomography. Clin Exp Rheumatol 2001; 19: 187–190.
30. McAdam LP, O’Hanlan MA, Bluestone R, et al. Relapsing polychondritis: prospective study of 23 patients and a
review of the literature. Medicine (Baltimore) 1976; 55: 193–215.
31. Tillie-Leblond I, Wallaert B, Leblond D, et al. Respiratory involvement in relapsing polychondritis. Clinical,
functional, endoscopic, and radiographic evaluations. Medicine (Baltimore) 1998; 77: 168–176.
32. Michet CJ, McKenna CH, Luthra HS, et al. Relapsing polychondritis. Survival and predictive role of early disease
manifestations. Ann Intern Med 1986; 104: 74–78.
33. Dolan DL, Lemmon GB, Teitelbaum SL. Relapsing polychondritis. Analytical literature review and studies on
pathogenesis. Am J Med 1966; 41: 285–299.
34. Behar JV, Choi YW, Hartman TA, et al. Relapsing polychondritis affecting the lower respiratory tract. AJR Am J
Roentgenol 2002; 178: 173–177.
35. Bodolay E, Szekanecz Z, Devenyi K, et al. Evaluation of interstitial lung disease in mixed connective tissue disease
(MCTD). Rheumatology (Oxford) 2005; 44: 656–661.
36. Daimon T, Johkoh T, Honda O, et al. Nonspecific interstitial pneumonia associated with collagen vascular
disease: analysis of CT features to distinguish the various types. Intern Med 2009; 48: 753–761.
37. Kozuka T, Johkoh T, Honda O, et al. Pulmonary involvement in mixed connective tissue disease: high-resolution
CT findings in 41 patients. J Thorac Imaging 2001; 16: 94–98.
38. Mino M, Noma S, Taguchi Y, et al. Pulmonary involvement in polymyositis and dermatomyositis: sequential
evaluation with CT. AJR Am J Roentgenol 1997; 169: 83–87.
39. Ikezoe J, Johkoh T, Kohno N, et al. High-resolution CT findings of lung disease in patients with polymyositis and
dermatomyositis. J Thorac Imaging 1996; 11: 250–259.
40. Arakawa H, Yamada H, Kurihara Y, et al. Nonspecific interstitial pneumonia associated with polymyositis and
dermatomyositis: serial high-resolution CT findings and functional correlation. Chest 2003; 123: 1096–1103.
41. Sitara D, Hoffbrand BI. Chronic bronchial suppuration and antineutrophil cytoplasmic antibody (ANCA)
positive systemic vasculitis. Postgrad Med J 1990; 66: 669–671.
42. Hilton AM, Hasleton PS, Bradlow A, et al. Cutaneous vasculitis and immune complexes in severe bronchiectasis.
Thorax 1984; 39: 185–191.
43. Falk RJ, Jennette JC. Anti-neutrophil cytoplasmic autoantibodies with specificity for myeloperoxidase in patients
with systemic vasculitis and idiopathic necrotizing and crescentic glomerulonephritis. N Engl J Med 1988; 318:
1651–1657.
44. Benucci M, Nenci G, Taccetti G, et al. Bronchiectasis worsening by p-ANCA (bactericidal/permeability-
increasing protein) positive vasculitis. A case report and review of the literature. Ann Ital Med Int 2005; 20:
258–261.
45. Takahashi K, Hayashi S, Ushiyama O, et al. Development of microscopic polyangiitis in patients with chronic
airway disease. Lung 2005; 183: 273–281.
46. Matsuyama W, Wakimoto J, Watanabe A, et al. Bronchiectasis with myeloperoxidase antineutrophil cytoplasmic
antibody and bactericidal/permeability-increasing protein antineutrophil cytoplasmic antibody. Intern Med 1999;
38: 813–816.
47. Forde AM, Feighery C, Jackson J. Anti-phagocyte antibodies and infection. Autoimmunity 1998; 28: 5–14.
48. Mahadeva R, Zhao MH, Stewart S, et al. Vasculitis and bronchiectasis in a patient with antibodies to bactericidal/
permeability-increasing protein and a1-antitrypsin deficiency. Chest 1997; 112: 1699–1701.
49. Dunn AC, Walmsley RS, Dedrick RL, et al. Anti-neutrophil cytoplasmic autoantibodies (ANCA) to bactericidal/
permeability-increasing (BPI) protein recognize the carboxyl terminal domain. J Infect 1999; 39: 81–87.
50. Pasteur MC, Bilton D, Hill AT, et al. British Thoracic Society guideline for non-CF bronchiectasis. Thorax 2010;
65: Suppl. 1, i1–i58.
51. Aronoff A, Bywaters EG, Fearnley GR. Lung lesions in rheumatoid arthritis. Br Med J 1955; 2: 228–232.
52. McDonagh J, Greaves M, Wright AR, et al. High resolution computed tomography of the lungs in patients with
rheumatoid arthritis and interstitial lung disease. Br J Rheumatol 1994; 33: 118–122.
53. Kelly C, Gardiner P. The relationship between rheumatoid arthritis and bronchiectasis. Ann Rheum Dis 1994; 53:
482–483.
20
6B
RO
NC
HIE
CT
AS
ISA
UT
OIM
MU
NIT
Y
54. McMahon MJ, Swinson DR, Shettar S, et al. Bronchiectasis and rheumatoid arthritis: a clinical study. Ann Rheum
Dis 1993; 52: 776–779.
55. Gaga M, Bentley AM, Humbert M, et al. Increases in CD4+ T lymphocytes, macrophages, neutrophils and
interleukin 8 positive cells in the airways of patients with bronchiectasis. Thorax 1998; 53: 685–691.
56. Lapa e Silva JR, Guerreiro D, Noble B, et al. Immunopathology of experimental bronchiectasis. Am J Respir Cell
Mol Biol 1989; 1: 297–304.
57. Silva JR, Jones JA, Cole PJ, et al. The immunological component of the cellular inflammatory infiltrate in
bronchiectasis. Thorax 1989; 44: 668–673.
58. Tsang KW, Chan K, Ho P, et al. Sputum elastase in steady-state bronchiectasis. Chest 2000; 117: 420–426.
59. Metafratzi ZM, Georgiadis AN, Ioannidou CV, et al. Pulmonary involvement in patients with early rheumatoid
arthritis. Scand J Rheumatol 2007; 36: 338–344.
60. Howling SJ, Hansell DM, Wells AU, et al. Follicular bronchiolitis: thin-section CT and histologic findings.
Radiology 1999; 212: 637–642.
61. Shannon TM, Gale ME. Noncardiac manifestations of rheumatoid arthritis in the thorax. J Thorac Imaging 1992;
7: 19–29.
62. Penny WJ, Knight RK, Rees AM, et al. Obliterative bronchiolitis in rheumatoid arthritis. Ann Rheum Dis 1982;
41: 469–472.
63. Murphy KC, Atkins CJ, Offer RC, et al. Obliterative bronchiolitis in two rheumatoid arthritis patients treated
with penicillamine. Arthritis Rheum 1981; 24: 557–560.
64. Isles AF, Masel J, O’Duffy J. Obliterative bronchiolitis due to Mycoplasma pneumoniae infection in a child. Pediatr
Radiol 1987; 17: 109–111.
65. Laraya-Cuasay LR, DeForest A, Huff D, et al. Chronic pulmonary complications of early influenza virus infection
in children. Am Rev Respir Dis 1977; 116: 617–625.
66. Wiebicke W, Seidenberg J. [Obliterating bronchiolitis following measles]. Pneumologie 1990; 44: 1220–1222.
67. Marinopoulos GC, Huddle KR, Wainwright H. Obliterative bronchiolitis: virus induced?Chest 1991; 99: 243–245.
68. Becroft DM. Bronchiolitis obliterans, bronchiectasis, and other sequelae of adenovirus type 21 infection in young
children. J Clin Pathol 1971; 24: 72–82.
69. Milner AD, Murray M. Acute bronchiolitis in infancy: treatment and prognosis. Thorax 1989; 44: 1–5.
70. Wright JL. Inhalational lung injury causing bronchiolitis. Clin Chest Med 1993; 14: 635–644.
71. Schlesinger C, Meyer CA, Veeraraghavan S, et al. Constrictive (obliterative) bronchiolitis: diagnosis, etiology, and
a critical review of the literature. Ann Diagn Pathol 1998; 2: 321–334.
72. Sweatman MC, Markwick JR, Charles PJ, et al. Histocompatibility antigens in adult obliterative bronchiolitis
with or without rheumatoid arthritis. Dis Markers 1986; 4: 19–26.
73. Markopoulo KD, Cool CD, Elliot TL, et al. Obliterative bronchiolitis: varying presentations and
clinicopathological correlation. Eur Respir J 2002; 19: 20–30.
74. Worthy SA, Muller NL. Small airway diseases. Radiol Clin North Am 1998; 36: 163–173.
75. Devouassoux G, Cottin V, Liote H, et al. Characterisation of severe obliterative bronchiolitis in rheumatoid
arthritis. Eur Respir J 2009; 33: 1053–1061.
76. Doran MF, Crowson CS, Pond GR, et al. Frequency of infection in patients with rheumatoid arthritis compared
with controls: a population-based study. Arthritis Rheum 2002; 46: 2287–2293.
77. Doran MF, Crowson CS, Pond GR, et al. Predictors of infection in rheumatoid arthritis. Arthritis Rheum 2002;
46: 2294–2300.
78. Gabriel SE, Crowson CS, Kremers HM, et al. Survival in rheumatoid arthritis: a population-based analysis of
trends over 40 years. Arthritis Rheum 2003; 48: 54–58.
79. McLean-Tooke A, Aldridge C, Waugh S, et al. Methotrexate, rheumatoid arthritis and infection risk: what is the
evidence? Rheumatology (Oxford) 2009; 48: 867–871.
80. Takayanagi N, Tsuchiya Y, Tokunaga D, et al. Pulmonary infections in patients with rheumatoid arthritis. Nihon
Kokyuki Gakkai Zasshi 2007; 45: 465–473.
81. Grennan DM, Gray J, Loudon J, et al. Methotrexate and early postoperative complications in patients with
rheumatoid arthritis undergoing elective orthopaedic surgery. Ann Rheum Dis 2001; 60: 214–217.
82. Strand V, Singh JA. Newer biological agents in rheumatoid arthritis: impact on health-related quality of life and
productivity. Drugs 2010; 70: 121–145.
83. Snowden N, Moran A, Booth J, et al. Defective antibody production in patients with rheumatoid arthritis and
bronchiectasis. Clin Rheumatol 1999; 18: 132–135.
84. Takanami I, Imamuma T, Yamamoto Y, et al. Bronchiectasis complicating rheumatoid arthritis. Respir Med 1995;
89: 453–454.
85. Puechal X, Fajac I, Bienvenu T, et al. Increased frequency of cystic fibrosis DF508 mutation in bronchiectasis
associated with rheumatoid arthritis. Eur Respir J 1999; 13: 1281–1287.
86. Holoshitz J. The rheumatoid arthritis HLA-DRB1 shared epitope. Curr Opin Rheumatol 2010; 22: 293–298.
87. Hillarby MC, McMahon MJ, Grennan DM, et al. HLA associations in subjects with rheumatoid arthritis and
bronchiectasis but not with other pulmonary complications of rheumatoid disease. Br J Rheumatol 1993; 32: 794–797.
88. Agarwal S, Cunningham-Rundles C. Autoimmunity in common variable immunodeficiency. Curr Allergy Asthma
Rep 2009; 9: 347–352.
20
7D
.J.
DH
AS
MA
NA
AN
DR
.W
ILS
ON

89. Beutler A, Mackiewicz SH. Association of rheumatoid arthritis with Kartagener’s syndrome in a patient with
HLA-DR1-DR4-B27 haplotype. Z Rheumatol 1992; 51: 253–255.
90. Bokszczanin A, Levinson AI. Coexistent yellow nail syndrome and selective antibody deficiency. Ann Allergy
Asthma Immunol 2003; 91: 496–500.
91. Maldonado F, Tazelaar HD, Wang CW, et al. Yellow nail syndrome: analysis of 41 consecutive patients. Chest
2008; 134: 375–381.
92. Davies G, Wilson R. Prophylactic antibiotic treatment of bronchiectasis with azithromycin. Thorax 2004; 59:
540–541.
93. Swinson DR, Symmons D, Suresh U, et al. Decreased survival in patients with co-existent rheumatoid arthritis
and bronchiectasis. Br J Rheumatol 1997; 36: 689–691.
94. Loebinger MR, Wells AU, Hansell DM, et al. Mortality in bronchiectasis: a long-term study assessing the factors
influencing survival. Eur Respir J 2009; 34: 843–849.
95. Vitali C, Bombardieri S, Jonsson R, et al. Classification criteria for Sjogren’s syndrome: a revised version of the
European criteria proposed by the American-European consensus group. Ann Rheum Dis 2002; 61: 554–558.
96. James JA, Harley JB, Scofield RH. Role of viruses in systemic lupus erythematosus and Sjogren syndrome. Curr
Opin Rheumatol 2001; 13: 370–376.
97. Fox RI. Sjogren’s syndrome. Lancet 2005; 366: 321–331.
98. Jeong YJ, Lee KS, Chung MP, et al. Amyloidosis and lymphoproliferative disease in Sjogren syndrome: thin-
section computed tomography findings and histopathologic comparisons. J Comput Assist Tomogr 2004; 28:
776–781.
99. Cassidy JT, Kennedy JD. Systemic lupus erythematosus presenting as bronchiectasis. Ir J Med Sci 1961; 422:
65–69.
100. Chisholm JC. Bronchiectasis and systemic lupus erythematosus. J Natl Med Assoc 1967; 59: 269–272.
101. Clause HP, Sanger PW, Taylor FH, et al. Systemic lupus erythematosus and bronchiectasis. Coll Works
Cardiopulm Dis 1963; 66: 544–550.
102. Torres-Salido M, Cortes-Hernandez J, Balada E, et al. Systemic lupus erythematosus as a first presentation of
common variable immunodeficiency associated with infrequent mannose-binding lectin gene polymorphisms.
Rheumatol Int 2011; 31: 537–541.
103. Swigris JJ, Fischer A, Gillis J, et al. Pulmonary and thrombotic manifestations of systemic lupus erythematosus.
Chest 2008; 133: 271–280.
104. Eichacker PQ, Pinsker K, Epstein A, et al. Serial pulmonary function testing in patients with systemic lupus
erythematosus. Chest 1988; 94: 129–132.
105. Gold WM, Jennings DB. Pulmonary function in patients with systemic lupus erythematosus. Am Rev Respir Dis
1966; 93: 556–567.
106. Wiedemann HP, Matthay RA. Pulmonary manifestations of systemic lupus erythematosus. J Thorac Imaging
1992; 7: 1–18.
107. Ippolito A, Petri M. An update on mortality in systemic lupus erythematosus. Clin Exp Rheumatol 2008; 26:
Suppl. 51, S72–S79.
108. Borchers AT, Keen CL, Shoenfeld Y, et al. Surviving the butterfly and the wolf: mortality trends in systemic lupus
erythematosus. Autoimmun Rev 2004; 3: 423–453.
109. Kanathur N, Lee-Chiong T. Pulmonary manifestations of ankylosing spondylitis. Clin Chest Med 2010; 31:
547–554.
110. Kiris A, Ozgocmen S, Kocakoc E, et al. Lung findings on high resolution CT in early ankylosing spondylitis. Eur J
Radiol 2003; 47: 71–76.
111. Fenlon HM, Casserly I, Sant SM, et al. Plain radiographs and thoracic high-resolution CT in patients with
ankylosing spondylitis. AJR Am J Roentgenol 1997; 168: 1067–1072.
112. Padley S, Varma N, Flower CD. Tracheobronchomegaly in association with ankylosing spondylitis. Clin Radiol
1991; 43: 139–141.
113. Eulry F, Mayaudon H, Sirvin-Bordier L, et al. HLA B27 and respiratory involvement in axial
spondylarthropathies. A retrospective study in 107 male patients. Rev Rhum Engl Ed 1998; 65: 560–566.
114. Hillerdal G. Ankylosing spondylitis lung disease – an underdiagnosed entity? Eur J Respir Dis 1983; 64: 437–441.
115. Casserly IP, Fenlon HM, Breatnach E, et al. Lung findings on high-resolution computed tomography in
idiopathic ankylosing spondylitis – correlation with clinical findings, pulmonary function testing and plain
radiography. Br J Rheumatol 1997; 36: 677–682.
116. Zochling J, Braun J. Mortality in ankylosing spondylitis. Clin Exp Rheumatol 2008; 26: Suppl. 51, S80–S84.
117. Braun J, Pincus T. Mortality, course of disease and prognosis of patients with ankylosing spondylitis. Clin Exp
Rheumatol 2002; 20: Suppl. 28, S16–S22.
118. Lehtinen K. Mortality and causes of death in 398 patients admitted to hospital with ankylosing spondylitis. Ann
Rheum Dis 1993; 52: 174–176.
119. Lavie F, Rozenberg S, Coutaux A, et al. Bronchiectasis in a patient with CREST syndrome. Joint Bone Spine 2002;
69: 515–518.
120. Prakash UB, Luthra HS, Divertie MB. Intrathoracic manifestations in mixed connective tissue disease. Mayo Clin
Proc 1985; 60: 813–821.
20
8B
RO
NC
HIE
CT
AS
ISA
UT
OIM
MU
NIT
Y
121. Prakash UB. Lungs in mixed connective tissue disease. J Thorac Imaging 1992; 7: 55–61.
122. Davis CA, Abramowsky CR, Swinehart G. Circulating immune complexes and the nephropathy of cystic fibrosis.
Hum Pathol 1984; 15: 244–247.
123. Abramowsky CR, Swinehart GL. The nephropathy of cystic fibrosis: a human model of chronic nephrotoxicity.
Hum Pathol 1982; 13: 934–939.
124. Soter NA, Mihm MC, Colten HR. Cutaneous necrotizing venulitis in patients with cystic fibrosis. J Pediatr 1979;
95: 197–201.
125. Finnegan MJ, Hinchcliffe J, Russell-Jones D, et al. Vasculitis complicating cystic fibrosis. Q J Med 1989; 72:
609–621.
126. Tanaka E, Tada K, Amitani R, et al. Systemic hypersensitivity vasculitis associated with bronchiectasis. Chest
1992; 102: 647–649.
127. Moss RB, Lewiston NJ. Immune complexes and humoral response to pseudomonas aeruginosa in cystic fibrosis.
Am Rev Respir Dis 1980; 121: 23–29.
128. Dorlochter L, Carlsson M, Olafsdottir EJ, et al. Anti-neutrophil cytoplasmatic antibodies and lung disease in
cystic fibrosis. J Cyst Fibros 2004; 3: 179–183.
129. Dutz JP, Benoit L, Wang X, et al. Lymphocytic vasculitis in X-linked lymphoproliferative disease. Blood 2001; 97:
95–100.
130. Hay BN, Martin JE, Karp B, et al. Familial immunodeficiency with cutaneous vasculitis, myoclonus, and
cognitive impairment. Am J Med Genet A 2004; 125A: 145–151.
131. Bongartz T, Sutton AJ, Sweeting MJ, et al. Anti-TNF antibody therapy in rheumatoid arthritis and the risk of
serious infections and malignancies: systematic review and meta-analysis of rare harmful effects in randomized
controlled trials. JAMA 2006; 295: 2275–2285.
132. Galloway JB, Hyrich KL, Mercer LK, et al. Anti-TNF therapy is associated with an increased risk of serious
infections in patients with rheumatoid arthritis especially in the first 6 months of treatment: Updated results
from the British Society for Rheumatology Biologics Register with special emphasis on risks in the elderly.
Rheumatology (Oxford) 2011; 50: 124–131.
133. Culver EL, Travis SP. How to manage the infectious risk under anti-TNF in inflammatory bowel disease. Curr
Drug Targets 2010; 11: 198–218.
134. Lakatos PL, Miheller P. Is there an increased risk of lymphoma and malignancies under anti-TNF therapy in IBD?
Curr Drug Targets 2010; 11: 179–186.
135. Mariette X, Tubach F, Bagheri H, et al. Lymphoma in patients treated with anti-TNF: results of the 3-year
prospective French RATIO registry. Ann Rheum Dis 2010; 69: 400–408.
136. British Thoracic Society Standards of Care Committee. BTS recommendations for assessing risk and for
managing mycobacterium tuberculosis infection and disease in patients due to start anti-TNF-a treatment.
Thorax 2005; 60: 800–805.
137. Dixon WG, Hyrich KL, Watson KD, et al. Drug-specific risk of tuberculosis in patients with rheumatoid arthritis
treated with anti-TNF therapy: results from the British Society for Rheumatology Biologics Register (BSRBR).
Ann Rheum Dis 2010; 69: 522–528.
138. Salvana EM, Cooper GS, Salata RA. Mycobacterium other than tuberculosis (MOTT) infection: an emerging
disease in infliximab-treated patients. J Infect 2007; 55: 484–487.
139. Maimon N, Brunton J, Chan AK, et al. Fatal pulmonary mycobacterium xenopi in a patient with rheumatoid
arthritis receiving etanercept. Thorax 2007; 62: 739–740.
140. Strangfeld A, Listing J, Herzer P, et al. Risk of herpes zoster in patients with rheumatoid arthritis treated with
anti-TNF-a agents. JAMA 2009; 301: 737–744.
141. Calabrese LH, Zein N, Vassilopoulos D. Safety of antitumour necrosis factor (anti-TNF) therapy in patients with
chronic viral infections: hepatitis C, hepatitis B, and HIV infection. Ann Rheum Dis 2004; 63: Suppl. 2,
ii18–ii24.
142. Fabre S, Gibert C, Lechiche C, et al. Primary cutaneous nocardia otitidiscaviarum infection in a patient with
rheumatoid arthritis treated with infliximab. J Rheumatol 2005; 32: 2432–2433.
143. Slusher JR, Maldonado ME, Mousavi F, et al. Central nervous system Aspergillus fumigatus presenting as cranial
nerve palsy in a patient with ankylosing spondylitis on anti-TNF therapy. Rheumatology (Oxford) 2008; 47:
739–740.
144. Miceli-Richard C, Gestermann N, Amiel C, et al. Effect of methotrexate and anti-TNF on Epstein–Barr virus
T-cell response and viral load in patients with rheumatoid arthritis or spondylarthropathies. Arthritis Res Ther
2009; 11: R77.
145. McKeown E, Pope JE, Leaf S. Epstein–Barr virus (EBV) prevalence and the risk of reactivation in patients with
inflammatory arthritis using anti-TNF agents and in those who are biologic naive. Open Rheumatol J 2009; 3:
30–34.
146. Cooper N, Arnold DM. The effect of rituximab on humoral and cell mediated immunity and infection in the
treatment of autoimmune diseases. Br J Haematol 2010; 149: 3–13.
147. Toussirot E, Pertuiset E, Sordet C, et al. Safety of rituximab in rheumatoid arthritis patients with a history of
severe or recurrent bacterial infection: observational study of 30 cases in everyday practice. Joint Bone Spine 2010;
77: 142–145.
20
9D
.J.
DH
AS
MA
NA
AN
DR
.W
ILS
ON

148. Pham T, Claudepierre P, Constantin A, et al. Tocilizumab: therapy and safety management. Joint Bone Spine
2010; 77: Suppl. 1, S3–S100.
149. Nishimoto N, Ito K, Takagi N. Safety and efficacy profiles of tocilizumab monotherapy in Japanese patients with
rheumatoid arthritis: meta-analysis of six initial trials and five long-term extensions. Mod Rheumatol 2010; 20:
222–232.
150. Yokota S, Imagawa T, Mori M, et al. Efficacy and safety of tocilizumab in patients with systemic-onset juvenile
idiopathic arthritis: a randomised, double-blind, placebo-controlled, withdrawal phase III trial. Lancet 2008; 371:
998–1006.
151. Nishimoto N, Miyasaka N, Yamamoto K, et al. Long-term safety and efficacy of tocilizumab, an anti-IL-6
receptor monoclonal antibody, in monotherapy, in patients with rheumatoid arthritis (the STREAM study):
evidence of safety and efficacy in a 5-year extension study. Ann Rheum Dis 2009; 68: 1580–1584.
152. Bigbee CL, Gonchoroff DG, Vratsanos G, et al. Abatacept treatment does not exacerbate chronic Mycobacterium
tuberculosis infection in mice. Arthritis Rheum 2007; 56: 2557–2565.
153. Taylor PC. How do the efficacy and safety of abatacept and infliximab compare in the treatment of active RA?Nat
Clin Pract Rheumatol 2009; 5: 126–127.
154. Merrill JT, Burgos-Vargas R, Westhovens R, et al. The efficacy and safety of abatacept in patients with non-life-
threatening manifestations of SLE: results of a 12-month exploratory study. Arthritis Rheum 2010; 62: 3077–3087.
155. Ruperto N, Lovell DJ, Quartier P, et al. Long-term safety and efficacy of abatacept in children with juvenile
idiopathic arthritis. Arthritis Rheum 2010; 62: 1792–1802.
21
0B
RO
NC
HIE
CT
AS
ISA
UT
OIM
MU
NIT
Y