
Grad Pore č AD d.o.o. Pula - Naslovna - parentium.com · Grad Pore č AD d.o.o. Pula
Upload
willa-watkinsCategory
view
227download
2
BRONCHIBRONCHIAAL ASTL ASTHHMA MA PhPharmaarmaccololooggyy a andnd
CCliniclinicalal AAspespeccttss
Cvičenie č. 7Cvičenie č. 7
MUDr. M. LaššánováMUDr. M. Laššánová
DEFINDEFINITION ABITION AB
Asthma bronchiale is chronic inflammatory disease of airways connected with bronchial hyperreactivity and totally or partially reversible obstruction of airways, which in the most cases dissapears spontaneously or with treatment.

ASTHMA BRONCHIALEASTHMA BRONCHIALE
reversible obstruction daily symptom variability family history beginning at any age, most often
10-15% children 5-10% adults
no smoking allergy, rinitis, eczema - may / may not
GINAGINA1995, 2002, 20061995, 2002, 2006
Celosvetová iniciatíva pre astmu

ETIOPATOGENESISETIOPATOGENESIS INFLAMMATIONINFLAMMATION activation of mastocytes,
macrophages, eosinophils, helper Th-lymfocytes => formed and released inflammatory mediators: histamine, leucotriens, prostaglandins, bradykinin
bronchoconstriction, mucus secretion, plasma exudation and bronchial hyperreactivity, airway remodelation
insufficient anti-inflammatory therapy => progressive destructive changes fixing of airway obstruction to emphysematous changes

Triggers of Symptoms and Triggers of Symptoms and Exacerbations Exacerbations
allergens factors of air pollution (including cigarette smoke) respiratory infections, particularly viral (RSV,
rhinoviruses, influenza viruses, chlamydia) physical activity and hyperventilation (by osmotic
processes) wheather changes food and drugs (ASA, NSAID, -blockers) emotional stress gastroesophageal reflux
KLINICAL SYMPTOMS OF ABKLINICAL SYMPTOMS OF AB
Emphasis on early diagnosis Emphasis on early diagnosis management begins with right analysis of
symptoms
- to them belong: dyspnoe cough chest distress wheezing

CClasification of Asthma according to clinical symptoms and lung lasification of Asthma according to clinical symptoms and lung function:function:
DEGREE OF SERIOUSNESS
SYMPTOMS DURING DAY SYMPTOMS DURING NIGHT
LUNG FUNCTION
IV. severe persistent A
sy. continuously, attacks often, physical activity limited Often
PEF 60%Nvariability of PEF 30%
III. moderate persistent
sy. daily, attacks 2/week, influencing activity 1/week
PEF = 60-80%Nvariability of PEF 30%
II. mild persistent A
sy. 2/week daily, attacks 2/week, changing activity
2/month
PEF 80%Nvariability of PEF =20-30%
I. mild intermittent A
sy. 2/week, only mild or no attacks, aktivity unchanged
2/monthPEF 80%Nvariability of PEF 30%
GINA
2002

GINA
2006

KLINICAL SIGNS OF ABKLINICAL SIGNS OF AB depends on the stage of asthma intermittent attacks of expiration type dyspnoe, ich
worsening at night and at dawn wheezing: intermittent, more significant at expiration cough: usually not productive, can be basic sign anxiety, pressure, chest tightness, dyspnoe sputum production usually little, if than väzký
mucus prodromal signs prior attack: itching under the chin,
discomfort between shoulder blades, fear, anxiety typical is vanishing of signs after b-dilatances or
antiinflammatory therapy, unsuccessful ATB th.
DIAGNOSTICDIAGNOSTIC PRINCIPLE: simple examinations made
repeatedly are more usefull than complete examinations made at one time or during long intervals limitation of expiratory flow at asthma has variable character findings may vary from completely normal to absolutely pathological
Functional diagnostics Allergologic diagnostics Specifying of inflammation markers

SPIROMETRIA BRONCHODILATION TESTS (BDT)
it verifies the degree of obstruction reversibility BRONCHOPROVOKING TEST (BKT)
BKT with histamine, ACh, adenosine, excercise, cold... negativenegative BKT excludes dg. of ABexcludes dg. of AB (absence of
bronchial hyperreactivity...) PEF variability by výdychomerom (self monitoring)
ARTERIAL BLOOD GASES (at exacerbation)
Determination of NO in exhaled air (early marker of asthmatic inflammation)
SPUTUM EXAMINATION eosinophils and their effective products, Curshmann´s
spirals, Charcot-Leyden´s crystalls
EXAMINATIONS AT ABEXAMINATIONS AT AB

SPIROMETRIASPIROMETRIA• simple, reproductible• gives informations about
restriction of air flow• – FVC (forced vital
capacity) – FEV1 (sec. vital cap.) – FEV3 (forced expiratory
flow at 50% expiration) – FEV1/VC – Tiffaneau´s
index (FEV3/VC)– PEF (peak expiratory
flow in l/min)
DIFERENTIAL DIAGNOSISDIFERENTIAL DIAGNOSIS
chronic obstructive pulmonary disease asthma cardiale at older adults viral bronchiolitis at children hyperventilatory syndrom fixed obstacles in the airways (tumors,
extramural compression, foreign particles) diffuse interstitial lung processes pneumothorax chest wall diseases (kyphoscoliosis,
neuromuscular diseases)

Beginning in middle age Beginning in younger age
Symptoms progress slowlyprogress slowly Symptoms from day to day changing
Long anamnesis of smoking Symptoms in the afternoon or early morning
Dyspnoe at excercise Also allergy, rhinitis, eczema
Larger irreversible restriction of air flow
Usually reversible restriction of air flow bmedzenie
Family history of asthma
CHOPDCHOPDCHOPDCHOPD Asthma BronchialeAsthma BronchialeAsthma BronchialeAsthma Bronchiale
PulmonaryPulmonaryfunctionsfunctions
SymptomsSymptoms
CH O P DCH O P DCH O P DCH O P D

SymptomsSymptoms PulmonaryPulmonaryfunctionsfunctions
A S T H M AA S T H M AA S T H M AA S T H M A
GOALS of Optimal AB ControlGOALS of Optimal AB Control
- elimination or significant reduction of reduction of symptomssymptoms
- prevention of exacerbationsprevention of exacerbations- maintaining lung functionslung functions closest to
physiological values - maintaining normal physical and living
activity - absence of treatment adverse effects - prevention of irreversibleirreversible bronchial
obstruction (remodelation of lower airways)- preventing asthma mortalitypreventing asthma mortality

THERAPY OF ABTHERAPY OF AB
NonpharmacologicalNonpharmacological Patients´ education avoiding risk factors and triggers-
PharmacologicalPharmacological A N T I I N F L A M M A T O R Y
relieves inflammation and bronchial hyperreactivity regular, long-term use
B R O N CH O D I L A T O R Y eliminates the symptoms of expiratory flow limitation rescue therapy in exacerbation

Administration of Drugs at AB
peroral parenteralby inhalation directly to the site of action fast beginning of actionmaximum efficacy lower therapeutic doses = minimalise risk of AE limitationslimitations from the site of patient from the site of patient (technique of
inhalation, cooperation...) inspiratory resistanceinspiratory resistance, needs to be overcomed
Administration of Drugs at AB
peroral parenteralby inhalation directly to the site of action fast beginning of actionmaximum efficacy lower therapeutic doses = minimalise risk of AE limitationslimitations from the site of patient from the site of patient (technique of
inhalation, cooperation...) inspiratory resistanceinspiratory resistance, needs to be overcomed

Inhalatory Systems
Nowadays


THERAPY OF ABTHERAPY OF ABA: A: CONTROLLERSCONTROLLERS
preventive drugs, controlling inflammationcontrolling inflammation are taken regularly,long timeregularly,long time to maintain control
antiinflammatory drugsantiinflammatory drugs
long acting inhalatory bronchodilatorslong acting inhalatory bronchodilators
B: B: RELIEVERSRELIEVERS
substances releasing bronchospasm
relieving = fast acting bronchodilators
C: OTHER ANTIASTHMATIC DRUGSC: OTHER ANTIASTHMATIC DRUGS Monoclonal Ab against IgE = omalizumab (50 pat. in SR) ketotifen Imunosupressives (MTX, CysA...)
inhalatory corticoids ICS
long-acting 2-sympathomimetics
(long-acting betaagonists ) LABA, (8-15h.) antileukotriens LTRAs
leukotriene receptor antagonists inhibitors of 5-lipooxygenase (zileuton)
retard methylxanthines cromones
A: A: CONTROLLERSCONTROLLERS

B: RELIEVERS
inhalatory short-acting 2-
sympathomimetics (short-acting
betaagonists ) SABA (do 4-6 h.)
inhalatory anticholinergics short-acting
systemic corticoids p.o./i.v. („rescue“
treatment)

INHALATORY CORTICOIDS INHALATORY CORTICOIDS ICSICSthe most effective antiinflammatory antiasthmatics to long-term use at all forms of AB
Mechanism of action:1. inhibition of cytokine transcription antiinflam. ef. 2. inhibition of mediators of inflam. release3. decrease of airways reactivity 4. restriction of vasodilation antioedematic ef.5. affect synthesis of eikosanoids 6. control activation of adhesive molecules
7. increase of susceptibilityincrease of susceptibility resp. protection of 2 receptors against down-regulation at long-term treatment with 2 mimetics
ICSICS AE locally can reduce with the use of attachments
and rinsing the mouth with NaHCO3
oropharyngeal candidosis dysphonia seldomly irritation to cough
risk of systemicsystemic AE is , depends on dose ,efficacy and pharmacokinetic of steroid
inflammationinflammation in airways, bronchibronchialal hyperreahyperreacctivittivityy and obobsstrutruction ction of airways
risk of AEAE (acute exacerbations) and control symptsymptoommss of disease
ICSICS beclomethasone budesonide fluticasone ciclesonide – 1 times per day, minimal syst.
AE, prodrugprodrug-activation dirrectly in lungs, the part resorbed is inactive => systemic ef. !!!!!!
mometasone flunisolide dexamethasone triamcinolone
Principles of Treatment with Principles of Treatment with ICSICS
1. ICS need to be administered at each new dg. AB
2. Treatment is essential to start early
3. We administer attack doses of ICS
4. Reduction of dose only after longer stabilisation (6 months) – than minimal effective dose
5. If not sufficient low doses of ICS, we don´t increase them, but add LABA, possibly with methylxanthines, antileucotriens
6. High doses of ICS we try to avoid
relativelly small therapeutic benefit compared to higher incidence of AE

ICS ICS in the Treatment ofin the Treatment of ABAB – – „stable disease“„stable disease“
mildmild per perssististentent ast asthhmama monotmonothheraperapy y with small doses ofwith small doses of ICS ICS
( 500µg BDP/d)addition of LABALABA will not reduce the
symptoms unless they are deteriorated pulmonary functions decrease
moderatemoderate per perssististentent ast asthhmama if insufficient control addadd LABA LABA at failure in the next step d doseose ICS ICS (cca. 800µg BDP/d)

ICS ICS in the Treatment ofin the Treatment of AB AB – – „exacerbations“„exacerbations“
ddoubleouble dose of ICSICS at treatment of AE iisnsn
´t´t ef efffeectivective
veveryry highhigh d dosesoses ICS ICS (2000-4000µg BDP)
to 1-2 W mmay be effectiveay be effective
the bestthe best to addadd high dose ofhigh dose of ICS ICS
toto regular maintenance therapy
ICS+LABAICS+LABA
at severesevere AE AE systsystemicemic CCSS

ßß22- SYMPAT- SYMPATHHOMIMETIOMIMETICSCS
Mechanism of action = agonistic, activating influence on ß2 receptors of sympathic NS
1. 1. Long-actingLong-acting ßß22SMSM (long-acting betaagonists ) = LABA
Controllers – to long-term,regular bronchodilation
2. 2. Short-actingShort-acting ßß22SMSM (short-acting betaagonists ) = SABA
Relievers – to short-term, acute management of exacerbation
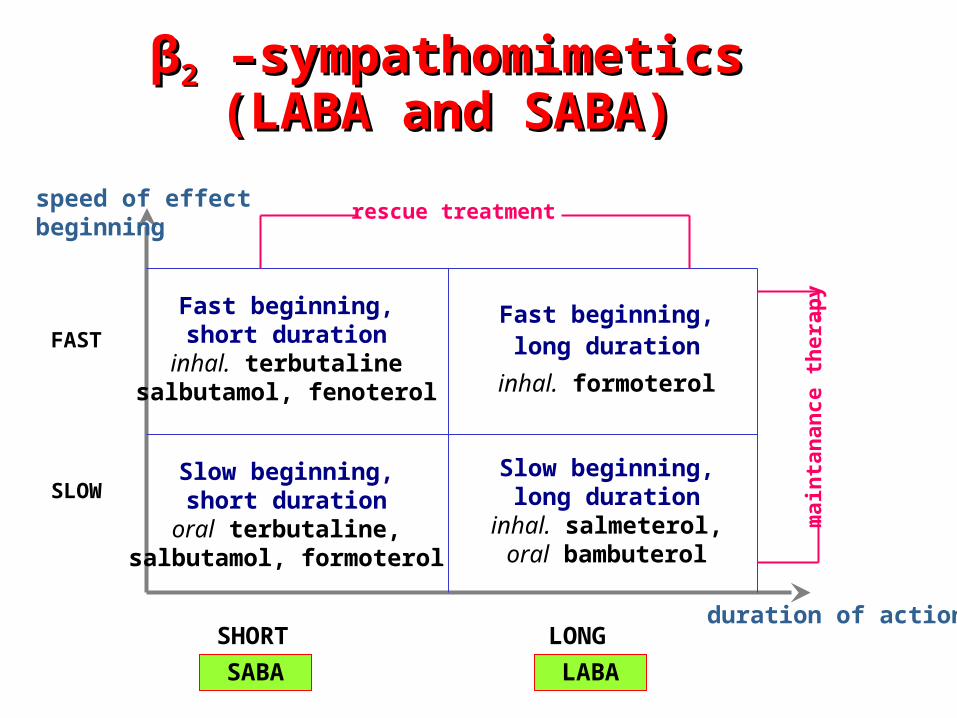
ββ22 –sympathomimetics –sympathomimetics(LABA and SABA)(LABA and SABA)
Fast beginning,short duration
inhal. terbutalinesalbutamol, fenoterol
Fast beginning, long duration
inhal. formoterol
Slow beginning,short durationoral terbutaline,
salbutamol, formoterol
Slow beginning,long duration
inhal. salmeterol,oral bambuterol
speed of effect beginning
FAST
SLOW
SHORT LONGduration of action
rescue treatment
mai
nta
nan
ce t
her
apy
LABASABA

ß2- sympatho MIMETICS = SM
Anti M -cholinergic = PsL
activate sympathic NS
dilate bronchi
block parasympathic NS
dilate bronchi

LoLoccalialisation ofsation of RReceptoreceptorss
cholinergcholinergicic (parasympat(parasympathhic)ic)
aadrenergdrenergicic
(sympat(sympathhic)ic)

LABALABA the best, fast and intense acting b-dilatans
duration ofduration of action action >>12 hours12 hours
MMAA:: Bronchodilation through β2 => relaxation of smooth
muscle
Improve mucociliar clearens
Lower vascular permeability
Modulate release of mediators from mastocytes a bazophils
Provide long-term safety against bronchoconstriction
Length of this bronchodilation effect at long-term regular administration decreases sign of tollerance for down regulation of β2 receptors => inhibition =
concomitant administration of ICS
LABA in long-term therapy of asthma never can administer lonely, without ICS!

MoleMoleccululaar mechanir mechanissmm of of positive positive interainteractionction ICS a ICS andnd LABA LABA
Glucocorticoid receptor
ß2-Adrenoceptor
Corticosteroid
Anti-inflammatory effect
• Effect of corticosteroids on ßEffect of corticosteroids on ß22-adrenoceptors -adrenoceptors • Effect of ßEffect of ß22-agonists on glucocorticoid receptors-agonists on glucocorticoid receptors
ß2-Agonist
Bronchodilatation
LABA: zlepšenie utilizácie KS a internalizácie GR do jadra (translokácia GR)ICS: prevencia desenzitizácie a znižovania expresie β2 receptora
LABA formoterol salmeterol
MonotMonothheraperapyy LABA: LABA: effectivity of LABA vs. ICS improving sleeping, but withoutwithout ef efffeect toct to
ppulmonaryulmonary fun functionsctions discontinuationdiscontinuation ICS ICS and addingadding LABA LABA at
persistent asthma loosingloosing ccontrolontrol good controlled patient with asthma with persistent
asthma at low dose ICS replacement byreplacement by LABA LABA loosingloosing ccontrolontrol ( eNo and Eo in sputum)
withoutwithout e efffefect on inflam.ct on inflam. in airways (biopsia)

LABA LABA in the Treatment ofin the Treatment of ABAB - - ConclusionConclusion the most effectivethe most effective bronchodilat bronchodilatorsors at AB effective at children and also adults formoterolformoterol suitable also for AEAE (since fast
beginnig + long duration of action) clinically withoutwithout antiinflam.antiinflam. effect most effectivelly inin ccombinombination withation with ICS ICS formoterol can be as rescue
bronchodilator more effective than SABA at pat. not responding to SABA !!!
atat AB AB alwaysalways pre prescribe together with scribe together with ICS !!!ICS !!!
CCONTROLONTROL of of ABAB 1.1. llooww dose ICS ICS
2. if nno controlo control reached: highhigh dose ICSICS costsadd LABALABA most effectivemost effectiveadd low-dose low-dose methylxanthinesmethylxanthines cheapestadd LTRAs LTRAs little effective, expensive
3. ICS+LABAICS+LABA = the best strategy of AB treatment
4. 15 studies: addingadding LABA LABA to ICS is more more eeffffeectivective than ddoubling of oubling of ICSICS dose dose !

FixFixeded ccombinombinationation ICS+LABA ICS+LABA – – ADVANTAGESADVANTAGES
compliance costs control of asthma faster control of asthma dose ICS to reach control in 1 inhalation divice deposition of ICS and LABA at the at the
same placesame place can occur molecular interaction ICS+LABAICS+LABA frequency of AEAE more than d dose ofose of ICS ICS
formoterol + budesonide salmeterol + fluticasone

Specific Label Changes for Long-Acting Beta-Agonists (LABAs).
1. Contraindicate the use of LABAs for asthma in patients of all ages without concomitant use of an asthma-controller medication such as an inhaled corticosteroid.
2. Stop use of the LABA, if possible, once asthma control is achieved and maintain the use of an asthma-controller medication, such as an inhaled corticosteroid.
3. Recommend against LABA use in patients whose asthma is adequately
controlled with a low- or medium-dose inhaled corticosteroid.
4. Recommend that a fixed-dose combination product containing a LABA and an inhaled corticosteroid be used to ensure compliance with concomitant therapy in pediatric and adolescent patients who require the addition of a LABA to an inhaled corticosteroid.
Chowdhury BA, Dal Pan G. The FDA and Safe Use of Long-Acting Beta-Agonists in the Treatment of Asthma. N Engl J Med. 2010 Feb 24.

ANTILEUKOTRIENE DRUGSANTILEUKOTRIENE DRUGS
controllers,controllers, for long-term control of symptoms antagonists of leukotriene 1 (CysLT1) receptors
montelukast, zafirlukast, pranlukast inhibitors of 5-lipooxygenase
zileuton taken perorally MA: - additive antiinflam. effect to ICS
- reduce tissue eosinophilia - mild bronchodilation ef. - bronchoprotective ef.

ANTILEUKOTRIENE DRUGSANTILEUKOTRIENE DRUGS role in therapy of AB - still unclear are less effective than low doses of ICS as additive drugs (in combination with ICS)
reduce the need of steroid dose at severe asthma
again less effective than standard ICS+LABA
advantageous – aspirin asthma, by excercise induced asthma, „preschool wheezing“
compliance at taking tablet form
METHYLXANTHINESMETHYLXANTHINES controllers, to long-lasting control of symptoms Improvement of clinical symptomatology
bronchodilation - without signif. increase of FEV1/ improvement of lung function parameters through inhibition of fosfodiesterase I. to IV. => cAMP
antiinflam., immunomodulatory effects positive effect on phenomenon of „corticoid resist.“
AE: cephalea, nausea, vomiting, tachycardia, palpitations, plasm. conc. (TDM) arrhytmias, epileptic spasms even death
potential toxicity, profile of AE bronchodilators of the third choice

METHYLXANTHINESMETHYLXANTHINES
Proven benefit bring only drug formsdrug forms providing long-lasting action with controlled releasewith controlled release
with controlled release - p.o. aminophylline, theophylline for
using during day time always + ICS – less effective than ICS+LABA
with short-lasting ef. - p.o., i.v.with short-lasting ef. - p.o., i.v. aminophylline, teophylline
others:others: doxophylline, cilomilast (select. inhibitor of PDE4)

SABASABA
basic relieversbasic relievers used ad hoc to relieve or to remove symptoms no reason for regular administration
salbutamol (Ventolin) fenoterol /Australia – deregistered for AE KVS/
terbutaline
INHALATORY ANTICHOLINERGIC INHALATORY ANTICHOLINERGIC DRUGSDRUGS
Relievers of the second choice, at AERelievers of the second choice, at AE
competitivecompetitive antagonists antagonists on M1, M2 and M3 on M1, M2 and M3
receptors of parasympathicus
cholinergic tonuscholinergic tonus
Division:Division:
with short-lastingshort-lasting effect: ipratropium bromideipratropium bromide with prolongedprolonged effect: oxitropium bromideoxitropium bromide
with long-lastinglong-lasting effect: tiotropium bromidetiotropium bromide CHOCHP

Pre-gangliovýnerv
Parasympatickéganglion
Post-gangliovýnerv
ACh
Hladký sval
Nicotinový receptor (+)
M1 receptor (+)
M2 receptor (–)
M3 receptor (+)
MusMusccarariinnicic receptory receptorys in s in airwaysairways
Barnes PJ. Eur Respir Rev 1996

INHALATORY ANTICHOLINERGIC INHALATORY ANTICHOLINERGIC DRUGSDRUGS
decrease n. vagus tonus cause relaxation but no bronchoprotective action are in general less effective than β–
mimethics and have a little slower beginning of action
advantageous combinations v 1 inhalation system:
ipratropium ipratropium+salbutamol
ipratropium+fenoterol
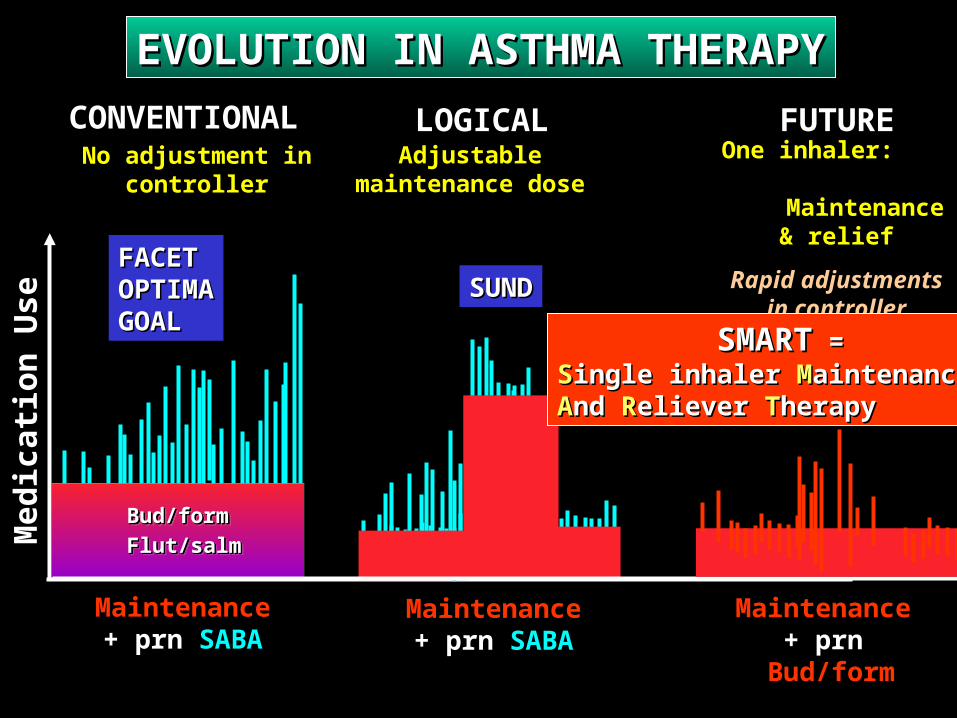
EVOLUTION IN ASTHMA THERAPYEVOLUTION IN ASTHMA THERAPY
No adjustment in No adjustment in controllercontroller
CONVENTIONALCONVENTIONAL
Med
icat
ion
Use
Med
icat
ion
Use
MaintenanceMaintenance+ prn+ prn SABA SABA
FACETFACETOPTIMAOPTIMAGOALGOAL
Adjustable Adjustable maintenance dosemaintenance dose
LOGICALLOGICAL
MaintenanceMaintenance+ prn+ prn SABA SABA
SUNDSUND
One inhaler: One inhaler: Maintenance Maintenance
& relief& relief
Rapid adjustments Rapid adjustments in controller in controller
replacing SABAreplacing SABA
FUTUREFUTURE
Maintenance Maintenance + prn+ prn Bud/form Bud/form
Bud/formBud/form
Flut/salmFlut/salm
Bud/formBud/form
Flut/salmFlut/salm
SMARTSMART = = SSingle inhaler ingle inhaler MMaintenance aintenance AAnd nd RReliever eliever TTherapyherapy
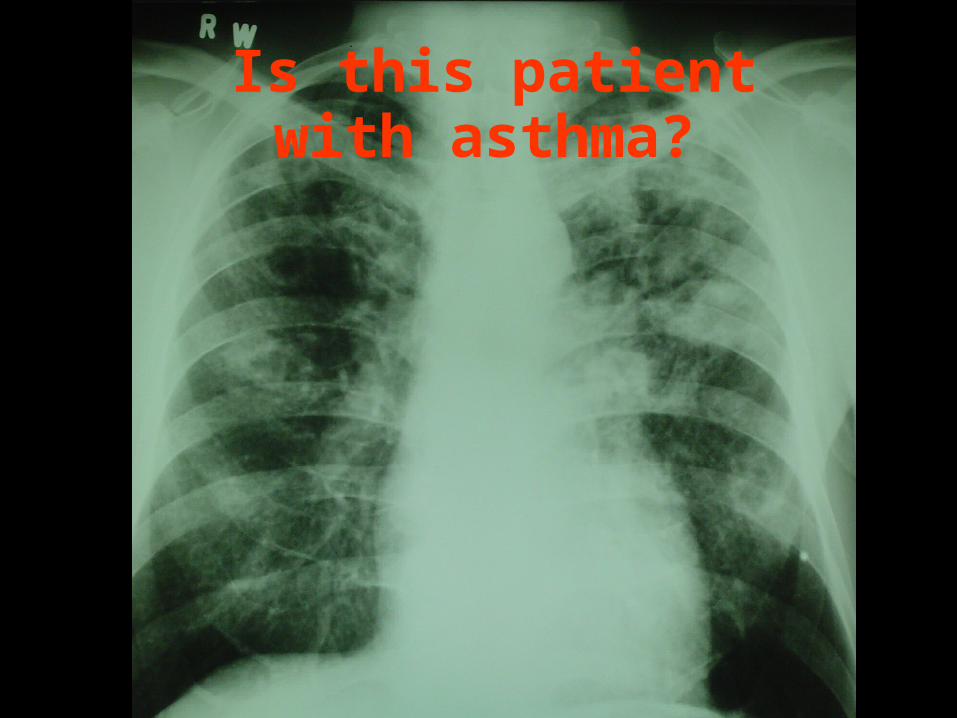
Is this patient with asthma?


















