
"Innovation and Wealth Creation: the British Library Perspective”
Upload
geoffrey-roseCategory
view
215download
3
FUTURE OF DISEASE PREVENTION British Perspective on the U.S. Preventive Services Task Force Guidelines
GEOFFREY ROSE, DM, DSc
The cl inical approach to prevent ion , cogently documented in the Tusk Force guidelines, implies the medical i za t lon o f prevenHon. The concen t ra t ion o f resources on those m o s t in need is efficien~ the w iden ing o f phys i c ians ' responsi- bility is welcome, a n d the inf luence o n the recipients dif-
f u s e s into the community . The Tusk Force repor~ however , f a i l s to s t ress the prob lems a n d the l imi ta t ions o f this ap- proach . The adverse effects o f "ffabeling'" can be serious. They need to be measured a n d taken in to accoun~ a n d there should be no screening wi thout counsel ing a n d long- term care; the lat ter c a n n o t be guaran teed unless there is a c o m p r e h e n s i v e genera l p r ac t i t i oner sys~ent Screening readi ly generates overmedicat ion, par t i cu lar ly s ince m a n y phys i c ians lack the skills, the incl ination, o r the s ta f f to p r o v i d e exper t a n d con t inu ing health advice. C o n c e r n
f o r high-risk indiv iduals shou ld be on ly o n e p a r t o f a much wider preven t ive strategy. This is i l lustrated by the close corre la t ions be tween the preva lence o f high-risk s tatus a n d the p o p u l a t i o n mean value (0 .85 fo r hyper tens ion vs. mean blood pressure, 0.97 f o r excess use o f a l coho l vs. p o p u l a t i o n mean intake). The medical approach, impor- tan t though i t is, mus t n o t d i s t rac t a t tent ion f r o m the m o r e
f u n d a m e n t a l p o p u l a t i o n strategy o f p reven t iom Key words: prevent ion; high-rislg populat ion; labe l in~ coun- sel ing, s c r e e n i n ~ overntedication. J GEN INTratN MED 1990;5(suppl) :S128- 8132.
BRITAIN p ioneered the great publ ic health m ovemen t of the 19th century, leading to bet ter publ ic services and a bet ter environment ; but, like the rest of Europe, we have lagged behind the United States in the new style of prevent ive medicine, in wh ich peop l e are encouraged to do things for themselves. I f there is a broad contrast be tween our two approaches to prevent ive medic ine , it is in this emphasis: to the east of the Atlantic, the em- phasis is more on societal action; to the west, on indi- vidual and medical responsibili t ies. Both, of course, are necessary; but to neglect the societal approach wou ld be dangerous, since in every count ry it seems that life expec tancy and the incidences of major diseases are de te rmined more by social and economic factors than by expendi tu re on health services or by the efforts and skills of physicians.
Received from the Department of Epidemiology and Popula- tion Sciences, London School of Hygiene and Tropical Medicine, and St Mary's Hospital, London, England.
Presented at the conference, Frontiers in Disease Prevention, The Johns Hopkins University, June 5 - 6 , 1989.
Address correspondence and reprint requests to Dr. Rose: Lon- don School of Hygiene and Tropical Medicine, University of London, Keppel Street, London, WC1E 7Ht, England.
$128
THE "HIGH-RISK APPROACH"
The recent repor t of the U.S. Preventive Services Task Force I concerns itself whol ly wi th the prevent ive potent ia l of action by physicians, guided by screening examinations. It seems to make sense, thus, to focus our main prevent ive efforts on suscept ible or high-risk indi- viduals and sectors of the popula t ion . They need spe- cial help, hence they and their medical advisers are l ikely to be bet ter motivated; and, for a given input, the benefit is l ikely to be larger. Other advantages are indi- rect, but perhaps in the long run are even more impor- tant. Physicians and their staff see high-risk individuals as "a lmos t pat ients ." By accept ing responsibi l i ty for them and by incorporat ing them as patients wi th in the medical care system, physicians b e c o m e drawn into prevent ion. Correspondingly, screening is a power fu l s t imulus to publ ic interest in health; at the same time, patients who are identified as having posi t ive test re- suits then serve to diffuse interest and information among their contacts.
An obvious pr ice that has to be paid for this high- risk strategy is the medical izat ion of prevent ion. Well peop l e are t reated as though they were patients. Those who thought that they were wel l have a fr ightening label at tached to them; though the consequences of that labeling could be t raumatic and long-lasting, they may yet be undetectable . It subt ly alters individuals ' self-confidence and their pe rcep t ions of themselves. This seems to cause more concern in Europe than in the United States. For example , the "Gu ide to Clinical Pre- vent ive Services ''1 r e commends b lood pressure mea- surements every two years for everyone aged 3 years or more. The yield of treatable hyper tension in chi ldren is tiny; but, even leaving cos t -e f fec t iveness aside, the repor t does not discuss whe the r this might be out- weighed by the psychological harm of label ing o ther chi ldren whose b lood pressures are above the average. Indeed, the impor tance of such effects is unknown.
The harm from labeling can be mit igated by wise counsel ing and by cont inuing support . 2 The wor ry is that these will not always be provided, especia l ly if screening becomes divorced f rom responsibi l i ty for long-term care. "No screening wi thout long-term after- ca re" should be our rule, and this impl ies that the screeners ought also to be the long-term carers.
In Britain we are fortunate in our p r imary health care system. Everyone has a general pract i t ioner, and
JOURNAL OF GENERAL INTERNAL MEDICINE, Volume S (September/October Supplement), 1990 $129
those pract i t ioners have lists of all the peop l e for whose health they are responsible. In a single year, 75% of the popula t ion will consult their general practi t ioner, or 90% within a per iod of three years. "Oppor tun i s t i c screening," taking advantage of these contacts, can thus achieve almost comple t e coverage of the popula- tion. More importantly, the system provides cont inui ty of care; and this at least gives the oppor tun i ty to link risk detect ion with long-term prevent ive care. This sys- tem is seen as the foundat ion for our personal preven- tive services.
The Task Force repor t also envisages a prevent ive service founded on pr imary health care; but in the ab- sence of a comprehens ive general pract i t ioner system, its implementa t ion will be difficult.
Coping with Health Information: Problems of "Labeling"
The United States seems to be moving rapidly towards a situation where peop le will be as familiar wi th their b lood pressure and cholesterol as they have been, for many years, wi th their weight. (Possibly Eu- rope will fo l low suit, but some years behind.) At first the novelty of such information creates both interest and fear, and this in turn motivates peop l e to seek a remedy. This capaci ty to arouse will p robab ly be short- lived. Most overweight people , having grown up wi th the knowledge of their weight, usually seem ready to accept i t - - e s p e c i a l l y when they know that many around them have the same problem. Hence we see that despite adequate knowledge, the prevalence of over- weight in Western countr ies continues to rise. So long as the underlying causes of unheal thy behavior persist, it is naive to bel ieve that heal th educat ion and the ef- forts of physicians can overcome social forces.
The same may wel l occur wi th cholesterol screen- ing. Just n o w this has novel ty and impact , but these may soon wear off. Those who are found to have familial hypercholes te ro lemia will p robab ly cont inue to accept the need for treatment, because they are conspicuous ly different f rom those around them. This is good for the individuals concerned; but it is of small re levance to the publ ic health, since this whole group contr ibutes less than 1% of total coronary deaths. The main argu- ment for the cholesterol screening program is the need to detect those wi th only modera te hypercholes terole- mia, and it is here that we should be cautious about the long-term impact. Current interest will not be sustained.
Behind the high-risk approach to resolving our p rob lems lies the bel ief that they are due to a trouble- some or unfor tunate minor i ty that needs to be identi- fied, segregated, and given special t reatment. The as- sumpt ion here is that most of us are all right and do not need to change our ways. This reassuring v iew explains this strategy's popular i ty . However , to the extent that
most of us are not in fact all right, focusing attention on the deviant minor i ty may be missing the major prob- lems. 3 Indeed, by giving false reassurance to the major- ity, it could be posi t ively harmful. In the case of the main cardiovascular risk factors, we know that the major publ ic health p rob lem arises f rom excess risk among the masses of peop l e wi th values at or a little above the mean, not among the deviant minority. In this respect screening is at best irrelevant: the main part of our p rob lem can be touched only by changes in the populat ion. The same may prove to be true of other mass health and behavioral concerns, including over- weight, alcoholism, depression, violence, and sexual promiscui ty.
This does not mean that the high-risk approach is not important , only that it is certainly insufficient and possibly, on its own, mere ly marginal. It is analogous to emergency famine rel ief in the Third World: it saves many lives, bu t it leaves the under lying causes un- touched. The danger is that we may be misled into bel ieving that we have done all that is needed.
The Danger of Overuse of Medications
When a screening examinat ion finds evidence of special risk or of early disease, then physician and pa- t ient alike expec t some action. Indeed, it would be wrong to reveal a previously hidden threat wi thout at the same t ime indicating a route of escape. The Task Force repor t r ightly emphasizes behavioral counseling; but to the physician this may appear t ime-consuming, beyond his or her skills, or unl ikely to be effective, and to the patient, too, it may appear unimpress ive or trou- blesome. To both parties, therefore, the prescr ip t ion of a drug may offer a more attractive alternative, and this is why screening inevitably st imulates the overuse of medicat ions.
We all tend to be more influenced by our own exper ience than by the exper ience of others. In several areas American trials have repor ted more encouraging results than European, and the European att i tude to consequent action has been correspondingly cautious. The Hyper tension Detect ion and Follow-up Program trial 4 repor ted that t rea tment of mild hyper tension im- pressively reduced mortal i ty whi le the British Medical Research Counci l (MRC) tr iaP (which inc luded a pla- cebo-treated control group) did not. The British trial est imated that overall, among persons aged 3 5 - 6 4 years wi th diastolic pressures of 9 0 - 109 m m Hg, the prevent ion of one stroke required 850 patient-years of treatment. This depressing statistic has considerably dampened European enthusiasm for t reatment, at least unless diastolic pressure is sustained at 1 O0 m m Hg or more. Physicians are being encouraged to take m u c h longer than before to establish a firm baseline and to pos tpone decisions on medicat ion.
The MRC trial also showed that benefit, measured
$130 Rose, BRITISH PERSPECTIVE
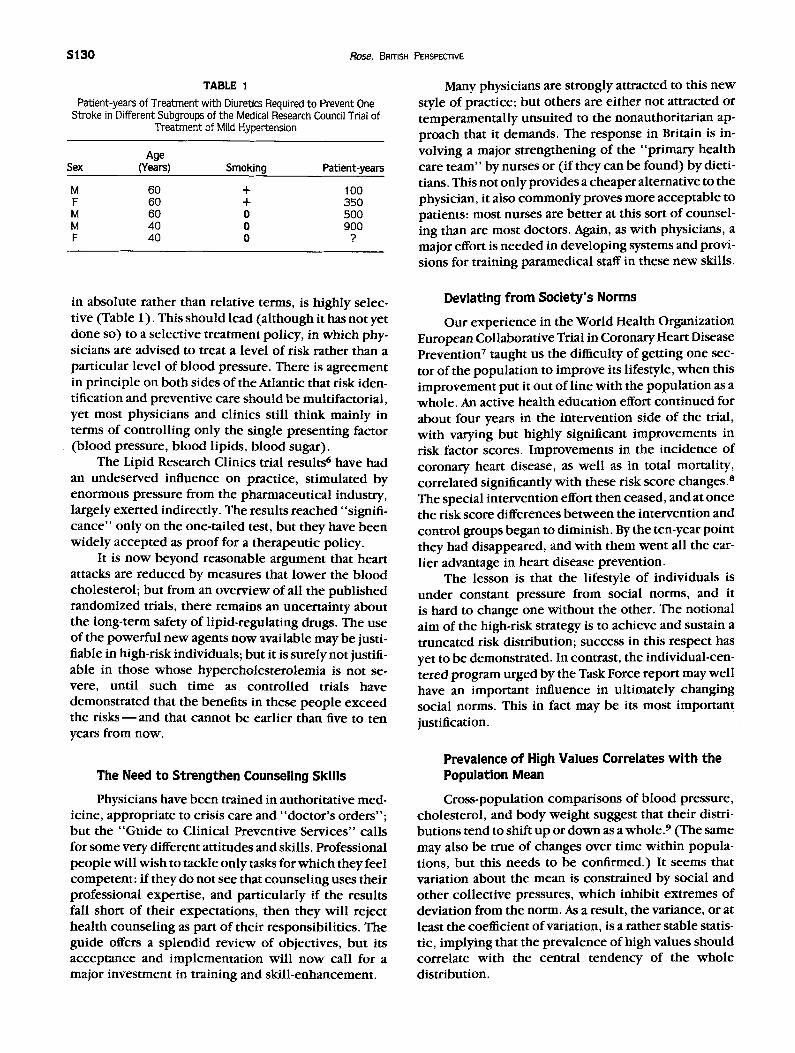
TABLE 1 Patient-years of Treatment with Diuretics Required to Prevent One
Stroke in Different Subgroups of the Medical Research Council Trial of Treatment of Mild Hypertension
Age Sex (Years) Smoking Patient-years
M 60 + 100 F 60 + 350 M 60 0 500 M 40 0 900 F 40 0 ?
Many physicians are strongly at tracted to this n e w style of practice; but others are ei ther not at tracted or t emperamenta l ly unsui ted to the nonauthori tar ian ap- proach that it demands. The response in Britain is in- volving a major s t rengthening of the "p r ima ry health care t e am" by nurses or (if they can be found) by dieti- tians. This not only provides a cheaper alternative to the physician, it also c o m m o n l y proves more acceptab le to patients: most nurses are be t te r at this sort of counsel- ing than are most doctors. Again, as wi th physicians, a major effort is needed in deve lop ing systems and provi- sions for training paramedical staff in these new skills.
in absolute rather than relative terms, is highly selec- tive (Table 1). This should lead (a l though it has not yet done so) to a select ive t rea tment policy, in which phy- sicians are advised to treat a level of risk rather than a part icular level of b lood pressure. There is agreement in pr inc ip le on bo th sides of the Atlantic that risk iden- tification and prevent ive care should be multifactorial , yet most physicians and clinics still think mainly in terms of control l ing only the single present ing factor (b lood pressure, b lood lipids, b lood sugar).
The Lipid Research Clinics trial results 6 have had an undeserved influence on pract ice, s t imulated by enormous pressure f rom the pharmaceut ica l industry, largely exer ted indirectly. The results reached "signifi- cance" only on the one-tai led test, bu t they have been wide ly accep ted as p roof for a therapeut ic policy.
It is n o w beyond reasonable argument that heart attacks are reduced by measures that lower the b lood cholesterol; bu t f rom an overv iew of all the publ i shed randomized trials, there remains an uncer ta inty about the long-term safety of l ipid-regulating drugs. The use of the power fu l new agents n o w available may be justi- fiable in high-risk individuals; but it is surely not justifi- able in those whose hyperchoIes te ro lemia is not se- vere, until such t ime as control led trials have demonst ra ted that the benefits in these p e o p l e exceed the r i s k s - - a n d that cannot be earlier than five to ten years f rom now.
The Need to Strengthen Counseling Skills
Physicians have been trained in authori tat ive med- icine, appropr ia te to crisis care and "doc to r ' s orders" ; but the "Gu ide to Clinical Preventive Services" calls for some very different att i tudes and skills. Professional p e o p l e will wish to tackle only tasks for wh ich they feel competen t : if they do not see that counsel ing uses their professional expert ise, and part icular ly if the results fall short of their expectat ions, then they will reject heal th counsel ing as part of their responsibili t ies. The guide offers a splendid rev iew of objectives, bu t its accep tance and implementa t ion will n o w call for a major investment in training and ski l l -enhancement .
Deviating from Society's Norms
Our exper ience in the World Health Organizat ion European Collaborative Trial in Coronary Heart Disease Prevent ion 7 taught us the difficulty of gett ing one sec- tor of the popula t ion to improve its lifestyle, w h e n this improvemen t put it out of l ine wi th the popula t ion as a whole . An active health educat ion effort con t inued for about four years in the intervent ion side of the trial, wi th varying but highly significant improvement s in risk factor scores. Improvemen t s in the incidence of coronary heart disease, as wel l as in total mortality, corre la ted significantly wi th these risk score changes. 8 The special intervent ion effort then ceased, and at once the risk score differences be tween the intervent ion and control groups began to diminish. By the ten-year point they had disappeared, and wi th them wen t all the ear- l ier advantage in heart disease prevent ion.
The lesson is that the lifestyle of individuals is under constant pressure f rom social norms, and it is hard to change one wi thout the other. The notional aim of the high-risk strategy is to achieve and sustain a t runcated risk distribution; success in this respect has yet to be demonstrated. In contrast, the individual-cen- tered program urged by the Task Force repor t may wel l have an important influence in ul t imately changing social norms. This in fact may be its most impor tant justification.
Prevalence of High Values Correlates with the Population Mean
Cross-populat ion compar isons of b lood pressure, cholesterol , and body weight suggest that their distri- but ions tend to shift up or down as a whole.9 (The same may also be true of changes over t ime wi th in popula- tions, but this needs to be confirmed.) It seems that variation about the mean is constrained by social and o ther col lect ive pressures, wh ich inhibit ex t remes of deviation f rom the norm. As a result, the variance, or at least the coefficient of variation, is a rather stable statis- tic, implying that the prevalence of high values should correlate wi th the central t endency of the who le distribution.
JOURNAL OF GENERAL INTERNAL MEDICINE, Volume S (September/October Supplement), 1990 $131
This predic t ion has been hard to test, because of a lack of standardized measurements carried out in a wide range of populat ions. The Intersalt s tudy 1° pro- vided just such a data set. Standardized quest ionnaires and examinat ions were adminis tered to 52 popula t ion samples in 35 countries, involving 10,079 individuals in all. This has provided an oppor tun i ty to examine, for a number of variables, the relat ion be tween the preva- lence of high values and the average for the whole pop- ulat ion sample. The results are clear and remarkably consistent. The correlat ion coefficients be tween preva- lence and mean are 0.85 for systolic and 0.86 for dia- stolic hypertension, 0.94 for overweight , 0 .78 for so- d ium intake, and 0 .97 for alcohol intake (in each case, p < 0 . 0 0 1 ) . The correlat ions are similar for men and women , and (within the age range of 2 0 - 64 years) for younger and older people . Because of measurement errors, the values of these coefficients will tend towards underest imation, perhaps impor tant ly so. Prevalence and mean are thus seen to be strongly corre- lated. Which determines which? Who leads, the popu- lation or the deviants? Presumably there is an interac- tion at all levels of the distribution, in bo th directions, be tween the more normal and the more deviant. The heavy drinkers discourage their more sober friends to drink more, whi le society 's disapproval of deviance works in turn to restrain the heavy drinkers. Surely, however , the chief pr imary force must come from the behavioral norms of the majority. Usually, the dog wags the tail, and the risk distr ibution p robab ly does like- wise. To he lp the minority, the majori ty must change.
THE POPULATION APPROACH TO PREVENTION
The pr inciple underlying the popula t ion approach to prevent ion is that the incidence rate of major dis- eases reflects the envi ronment and lifestyle of the pop- ulation. The high-risk strategy seeks to he lp suscept ible or heavily exposed individuals; the popula t ion strategy seeks to reduce overall exposure to the causes of ill health. Small shifts in the risk distribution of the popu- lation as a who le can offer unexpec ted ly large benefits. For example , a reduct ion of 10% in the mean serum cholesterol level of the popula t ion wou ld reduce by two-thirds the n u m b e r of peop l e wi th values current ly in the top d e c i l e - - a m u c h greater effect than could be expec ted f rom a p rogram of screening and treating indi- viduals. A reduct ion of as little as 3 m m Hg in the mean diastolic pressure of the popula t ion might wel l save as many lives as wou ld all exist ing ant ihypertensive medi- cation. 9 A reduct ion of 30% in mean alcohol intake might benefit health as m u c h as would the total eradica- t ion of heavy drinking. 11
The high-risk strategy offers a relatively large ben- efit to a minor i ty of individuals; the l imit to its pub l ic health effect is set by the fact that the group it identifies as at conspicuous risk general ly contr ibutes only a mi-
nori ty of the total burden of disease. It cannot cope with the p rob lem of our unheal thy populat ions, in which most peop le have unacceptab le levels of such risk fac- tors as b lood pressure, cholesterol , overweight , inade- quate exercise, aggression, and so on. Some broader and more fundamental response is required.
The Physician and Society: the Frontiers of Medicine
Society's expecta t ions of the physician are contin- uously being renegotiated. The 19th-century publ ic health reformers were as m u c h concerned wi th the en- v i ronment as wi th treating the sick. Then the scientific revolut ion in medic ine gave us enormous ly enhanced powers , but only wi th in a d iminished territory: we sim- ply t reated the sick, but m u c h bet ter than before. Now we are seeking once again to move out, this t ime into the new area of individuals ' choices of personal life- styles. The physician 's frontiers are cultural ly depen- dent and negotiable, and American physicians o ccu p y an evidently more expanded terr i tory than their Euro- pean counterparts . Nevertheless, we are all c learly moving in the direct ion of a greater concern wi th h o w peop l e conduc t their lives.
This necessary deve lopmen t has its dangers. To say " w e know that smoking is bad for your hea l th" is a p rope r message f rom medical scientists to the public; but to say "so it is wrong for you to smoke" is a judg- ment that belongs to the smoker, not to the physician. Lifestyle choices involve a balancing of health against many other social and personal considerations, and the decision depends on the part icular weights assigned to each i tem in the balance sheet. Those weights are for the individual to choose; and health is c o m m o n l y as- signed a lesser weight by the publ ic than by physicians (especial ly by those member s of the publ ic w h o are not current ly ill). The role of the physician in prevent ion is to inform, to challenge, and to assist, not to take com- mand. This is c lear ly and wisely set out in the Task Force repor t ' s introduct ion, but one fears that it wil l
often be overlooked.
CONCLUSION
The Task Force repor t provides an excel len t route map in this newly deve loped and exci t ing area of coop- eration be tween physicians and the publ ic . It is to be c o m m e n d e d as m u c h for the roads that it marks " c lo sed" as for the ones that it commends . Those w h o consul t a map before setting out on a journey are less l ikely to get lost, and that will surely be true here; but the map by itself does not ensure arrival. What is needed now is the organization of health care and its system of financing, the suppor t ing staff, and the train- ing f rom which to deve lop an efficient and effective prevent ive medic ine service, buil t around and inte- grated with the existing therapeut ic service.
$13~, Black, PREVENTION IN DEVELOPING COUNTRIES
Finally, and needing an even higher priority, there must be a parallel effort to remedy the underlying causes of ill health in the environment and in socioeco- nomic structures. Together, the populat ion and the clinical approaches will achieve greater success than either by itself could hope for.
REFERENCES 1. U.S. Preventive Services Task Force. Guide to clinical preventive
services: an assessment of the effectiveness of 169 interventions. Baltimore: Williams and Wilkins, 1989.
2. Mann AH. The psychological effect of a screening programme and clinical trial for hypertension upon the participants. Psychol Med. 1977;7:431-8.
3. Rose G. The strategy of prevention: lessons from cardiovascular disease. Br MedJ. 1981;282:1847-51.
4. Hypertension Detection and Follow-up Program Cooperative Group. Five-year findings of the Hypertension Detection and
Follow-up Program. 1. Reduction in mortality of persons with high blood pressure, including mild hypertension. JAMA. 1979;242:2562-71.
5. Medical Research Council Working Party on Mild to Moderate Hypertension. MRC trial of treatment of mild hypertension: prin- cipal results. Br MedJ. 1985;291:97-104.
6. Lipid Research Clinics Program. The Lipid Research Clinics cor- onary primary prevention trial results. JAMA. 1984 ;251:351-74.
7. Kornitzer M, Rose G. WHO European collaborative trial of multi- factorial prevention of coronary heart disease. Prev Med. 1985;14:272-8.
8. Rose G. European collaborative trial of multifactorial prevention of coronary heart disease. Lancet. 1987;i:685.
9. Rose G. Sick individuals and sick populations. Int J Epidemiol. 1985;14:32-8.
I0. Intersalt Cooperative Research Group. Intersalt: an international study of electrolyte excretion and blood pressure. Results for 24-hour urinary sodium and potassium excretion. Br Med J. 1988;297:319-28.
l l . Kreitman N. Alcohol consumption and the preventive paradox. Br J Addict. 1986;81:353-63.
Prevention in Developing Countries
ROBERT E. BLACK, MD, MPH
Developing countr ies have implemented p r i m a r y health care p r o g r a m s directed p r i m a r i l y a t p r e v e n t i o n a n d man- agement o f impor tan t in fect ious a n d nu t r i t iona l p rob lems o f children. Successful p r o g r a m s have emphas i zed the need f o r ind iv idual a n d communi t y involvement a n d have been charac ter i zed by responsible g o v e r n m e n t po l ic ies f o r equitable implementa t ion o f ef f icacious a n d cost-effective health interventions. Unfortunately, detmloping countr ies mus t also f a c e increases in the chron ic disease a n d social prob lems commonly associated with indus tr ia l i zed coun- tries. Prevent ion efforts, f o r example, to reduce tobacco s m o k i n ~ to modi fy the dieg to reduce injuries, o r to aver t env i ronmen ta l contaminat ion , are needed to con ta in f u - ture morbid i ty a n d rapidly increas ing medical care costs. Developing countr ies can build o n the ir successful ap- p roaches to p r o g r a m implementat ion a n d add o ther mea- sures directed a t p re se rva t ion o f health a n d p r e v e n t i o n o f disease in adul t as well as chi ld popula t ions . Key words: injuries; developing countries; mortality; lOex, tmn t io~ smoking. J GEN IN't'vatN MED 1990;5(suppl ) :S132-8135 .
PREVENTION IN DEVELOPING COUNTRIES is a broad, a n d
s o m e w h a t d a u n t i n g , t o p i c . O n e m a y a p p r o a c h i t b y
c o n s i d e r i n g t w o q u e s t i o n s : " C a n w e i n t h e U n i t e d
S ta t e s l e a r n f r o m d e v e l o p i n g - c o u n t r y e x p e r i e n c e s ,
b o t h s u c c e s s e s a n d f a i l u r e s , i n h e a l t h c a r e ? " a n d " C a n
d e v e l o p i n g c o u n t r i e s l e a r n f r o m o u r s u c c e s s e s a n d fa i l -
u r e s i n h e a l t h c a r e ? "
Received from the Department of International Health, The Johns Hopkins University School of Hygiene and Public Health, 615 North Wolfe Street, Baltimore, Maryland 21205.
Presented at the conference, Frontiers in Disease Prevention, The Johns Hopkins University, June 5 - 6, 1989.
Address correspondence and reprint requests to Dr. Black.
LESSONS FROM DEVELOPING COUNTRIES
To begin with developing-country lessons, it is necessary to trace some trends internationally. Health sector efforts have evolved substantially in the last 40 years. Until the 1940s, the emphasis was on curative or palliative care delivered at hospitals or health centers by doctors. Nurses and auxiliaries were aides to the doctor, rather than providers of care. Beginning in the 1940s, there was some shift from the attention to indi- viduals to the focus on communities. This included an emphasis on preventive programs, such as environmen- tal sanitation or health education. These efforts were (and are, since this is still a common health sector ori- entation in some developing countries) often delivered from health facilities or by selective outreach activities. The services were delivered at one level by doctors and nurses and at a second level by auxiliaries who staffed small dispensaries or mobile teams. This approach im- proved availability of services, but access was uneven, utilization was low, and the impact on health was modest.
An important reorientation in health sector strat- egy was that toward a concern for the entire population, i.e., the goal of "heal th for all." This objective was included in the constitution of the World Health Orga- nization in 1948, but it took several decades to begin to see real action. The international meeting in Alma-Ata in 1978 declared the goal of "Health for All by the Year 2000 ." This goal of universal coverage required greater stress on equity in health care and health out- comes. There was recognit ion that services were not


















