
British Orthopaedic Association and British Association of Plastic ...
45
British Orthopaedic Association and British Association of Plastic Surgeons The Management of Open Tibial Fractures September 1997
Transcript of British Orthopaedic Association and British Association of Plastic ...

Printed in England by Chandlers Printers Ltd., Saxon Mews, Reginald Road, Bexhill-on-Sea, East Sussex.
British Orthopaedic Association35-43 Lincoln’s Inn Fields
London WC2A 3PNTel: 0171-405 6507Fax: 0171-831 2676
British Orthopaedic Associationand
British Association of Plastic Surgeons
The Management of Open Tibial Fractures
September 1997

A Report by the BOA/BAPS Working Partyon
The Management of Open Tibial Fractures
Membership of the BOA/BAPS Working Party
Orthopaedic Members:
Mr C M Court-Brown (Chairman)Mr A T CrossMr D M Hahn
Prof. D R MarshMr K Willett
Plastic Surgery Members:
Mr A A W F QuabaMr J Small
Mr J S Watson
Acknowledgements: R Keith Harrison, MMAA, AIMI, LSIAD, RMIP
Chief Medical Artist, Withington HospitalChairman, Medical Artists Association of Great Britain
September 1997
i

CONTENTS
PageForeword 1
Introduction 2
1. Epidemiology of Open Fractures 3— Table 1 6— Table 2 7— Table 3 8
2. Injury Recognition 9— History— Examination
— Skin— Signs of Compartment Syndrome— Signs of Vascular Injury— Signs of Nerve Injury
— X-ray
3. Communication 12Figure 1 13
4. Timing 15
5. Pre-Operative Management 15— Compartment Syndrome in Open Fractures— Multiple Injuries— The Decision to Amputate— Prevention of Wound Infection
6. The First Orthopaedic Procedure 19— Wound Extension— Wound Excision— Treatment of Skin and Subcutaneous Tissues— Treatment of Muscle
ii
— Treatment of Bone— Lavage— Fracture Stabilisation— Wound Closure— Summary
Figure 2 23
7. Safe Incisions and Fasciotomy 24— Incisions
— Medial Incision— Antero-Lateral IncisionFigure 3 25Figure 4 26
— FasciotomyFigure 5 28
8. Commonly Used Methods of Soft Tissue Reconstruction 29— Introduction— Advantages and Disadvantages of Split Skin Grafts,— Local Flaps and Free Flaps
— Skin Grafts— Local Flaps— Free Flaps— Which Method of Skin Closure?
— Types of Available Flap— Local Flaps
— Fasciocutaneous Flaps— Muscle Flaps
— Microvascular Free FlapsFigures 6-9 33-36Table 4 37Table 5 38
References39-40
iii

FOREWORD
We congratulate the authors of this excellent combined report. What a pleasure it isto find two surgical specialties cooperating in this way. The working party has care-fully analysed the available data, considered the various options for management andproffered clear advice which we hope will be useful for all surgeons managing thesedifficult injuries.
The message of collaboration was conveyed in the first edition of the report pub-lished in 1993. This stressed that, in order to avoid repeated surgery and long termdisability, it is necessary to evaluate each injury and to establish communicationbetween the two disciplines as soon as possible, with the aim of providing optimalconditions for wound and fracture healing. The working party feels that this messagenow needs re-emphasising and it is our hope that this latest report, by up-dating andrepeating the principles of management, will lead to a further improvement inoutcomes.
Professor T Duckworth Mr B P MorganPresident PresidentBritish Orthopaedic Association British Association of Plastic Surgeons
1

INTRODUCTION
The first edition of this booklet was issued following a combined meeting of theBritish Orthopaedic Association and the British Association of Plastic Surgeons inCambridge in September 19911. This meeting highlighted the importance of co-oper-ation between Orthopaedic Surgeons and Plastic Surgeons in the management ofopen fractures and also drew attention to the fact that surgical practice frequently fellshort of acceptable standards. The principal aim of the first booklet was to encourageearly co-operation between Orthopaedic and Plastic Surgeons. This goal was par-tially achieved and the interest stimulated by the publication of the booklet for a timesubstantially improved the awareness and management of the problems associatedwith these fractures. Unfortunately, however, optimal management is still not uni-formly practised throughout the United Kingdom.
A number of significant problems remain. All too often, out of hours trauma contin-ues to be undertaken by junior surgeons who are often unsupervised. ManyConsultants profess little interest in Trauma Surgery, and thus inappropriate proce-dures may be performed. The recent BOA census2 suggested that few OrthopaedicSurgeons had a primary interest in Trauma, and that less than 3% of surgeons over 55years of age have an interest in trauma. A survey by Court-Brown and McQueen3
(1997) confirmed these findings and showed that only about 8% of OrthopaedicSurgeons profess to have a primary interest in trauma, whereas about 80% taketrauma call. It is probable that a similar situation exists in Plastic Surgery. Thisexplains why the results of open fractures fall short of those obtained by mostEuropean Centres.
This booklet seeks to emphasise the importance of early co-operation and manage-ment of open fractures. It documents their epidemiology and, using the open tibialdiaphysis as an example, it describes the primary management of a lower limbwound and methods of soft tissue reconstruction. We believe that the management ofopen fractures must be improved. Inadequate or inappropriate primary managementleads to complications which are not only potentially devastating for the patient butare very expensive. If local facilities are inadequate for prompt treatment of openfractures then these hospitals should not accept these patients and should makearrangements for immediate transfer to a larger unit where they can receive optimaltreatment.
2

Objectives
To improve the understanding of the often complex diagnostic and managementproblems associated with complex tibial fractures.
To increase awareness of the importance of a multidisciplinary approach to manage-ment.
To encourage early transfer to a specialist centre if local facilities are not optimal.
3
1. EPIDEMIOLOGY OF OPEN FRACTURES
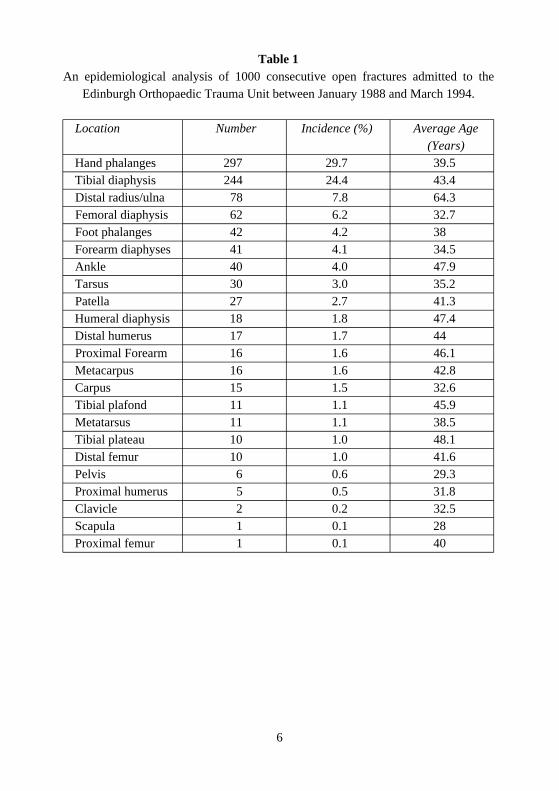
A review of 1,000 consecutive open fractures occurring between January 1988 andMarch 1994 in Edinburgh4 suggests that open fractures occur with a frequency ofabout 23 per 100,000 patients per year. However the frequency of different openfractures varies considerably. This is demonstrated in Table 1 (p.6). It is obvious thatopen phalangeal fractures and open fractures of the tibial diaphysis are very muchmore common than all other open fractures. Together they comprise about 54% of allopen fractures presenting to the average hospital. Some open finger injuries willrequire plastic surgery but Table 2 (p. 7) indicates that it is mainly fractures of thetibial diaphysis, tibial plafond and ankle that require combined treatment byOrthopaedic Trauma Surgeons and Plastic Surgeons. Open carpal fractures fre-quently require plastic surgery but these are rare injuries. The relative frequency ofopen tibial diaphyseal fractures and their requirement for plastic surgery means thatopen tibial diaphyseal fractures are the most appropriate fracture to illustrate theimportance of co-operation between Plastic Surgeons and Orthopaedic TraumaSurgeons.
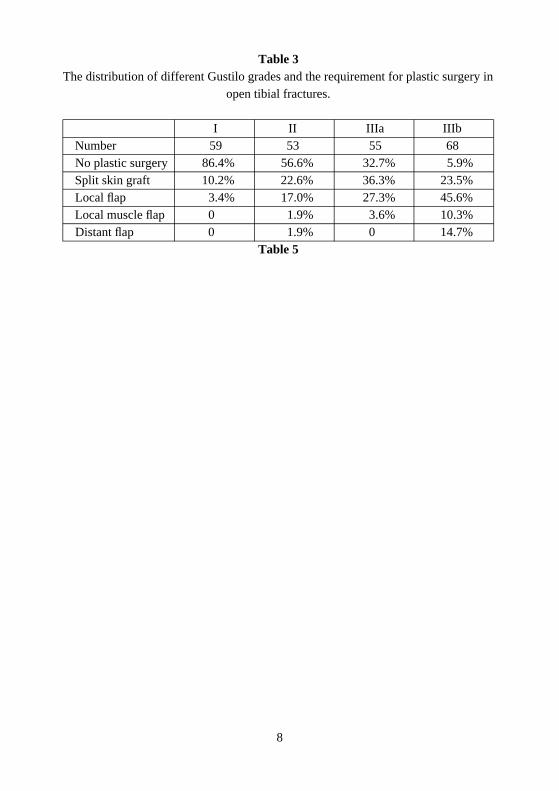
Of the 244 open tibial diaphyseal fractures detailed in Tables 1 and 2, 59 (24.1%)were Gustilo type I5 in severity, 53 (21.7%) were type II, 55 (22.5%) were typeIIIAand 68 (27.9%) were type IIIB. The remaining 9 (3.7%) were type IIIC6 fractures.Table 3 (p. 8) details the requirement for plastic surgery in all open tibial diaphysealfractures up to Gustilo type IIIB in severity. Analysis of the IIIC fractures shows thatplastic surgery was only performed in two patients with one receiving a split skingraft and the other a local flap. The remaining seven patients had amputations beforedefinitive plastic surgery would have been required. Table 3 not only indicates theincreasing requirement for plastic surgery in more severe open tibial diaphyseal frac-tures but it also shows there is a greater requirement for flap cover in the more severefracture types. Different Plastic Surgeons disagree about the relative requirements oflocal and free flaps but it is likely that Table 3 does provide an indication of therequirement for both split skin grafting and flap cover in the different grades of opentibial fracture. It is of particular interest that about 70% of all Gustilo type IIIB opentibial diaphyseal fractures require flap cover.
Extrapolation of the data given in Tables 1–3 permits the frequency of open tibialdiaphyseal fractures to be assessed. There are probably about 3,250 open tibial frac-tures per year in the United Kingdom. Assuming that about 80% of OrthopaedicSurgeons take trauma call, it seems likely that each surgeon will see three or fouropen tibial diaphyseal fractures per year and that only one of these will be Gustilo
4

IIIB in severity, these being the most difficult open fractures to treat. PlasticSurgeons will undertake flap cover for a number of conditions other than trauma but,as with all complex surgical procedures, post-traumatic flap cover does require spe-cialist expertise and we suggest that one or two surgeons in each Plastic Unit spe-cialise in this discipline. It is evident that few Orthopaedic and Plastic Surgeons willgain sufficient experience to adequately treat open tibial fractures and it is obviousthat if patients are to receive optimal treatment open tibial fractures should be man-aged in centres where both Orthopaedic Trauma Surgeons and Plastic Surgeons cangain experience in their management. There is no doubt that better handling of thesedifficult fractures would not only help the patient but lead to less secondary surgeryand therefore less expense.
5
6
Table 1An epidemiological analysis of 1000 consecutive open fractures admitted to the
Edinburgh Orthopaedic Trauma Unit between January 1988 and March 1994.
Location Number Incidence (%) Average Age(Years)
Hand phalanges 297 29.7 39.5Tibial diaphysis 244 24.4 43.4Distal radius/ulna 78 7.8 64.3Femoral diaphysis 62 6.2 32.7Foot phalanges 42 4.2 38Forearm diaphyses 41 4.1 34.5Ankle 40 4.0 47.9Tarsus 30 3.0 35.2Patella 27 2.7 41.3Humeral diaphysis 18 1.8 47.4Distal humerus 17 1.7 44Proximal Forearm 16 1.6 46.1Metacarpus 16 1.6 42.8Carpus 15 1.5 32.6Tibial plafond 11 1.1 45.9Metatarsus 11 1.1 38.5Tibial plateau 10 1.0 48.1Distal femur 10 1.0 41.6Pelvis 6 0.6 29.3Proximal humerus 5 0.5 31.8Clavicle 2 0.2 32.5Scapula 1 0.1 28Proximal femur 1 0.1 40

7
Table 2The requirement for plastic surgery in the 1000 open fractures detailed in Table 1.
Location Number Incidence (%) Plastic Surgery (%)Ankle 40 4.0 55Tibial diaphysis 244 24.4 54.9Tibial plafond 11 1.1 54.5Carpus 15 1.5 46.6Tarsus 30 3.0 40Tibial plateau 10 1.0 30Distal femur 10 1.0 30Femoral diaphysis 62 6.2 29Forearm diaphyses 41 4.1 19.5Patella 27 2.7 18.5Metacarpus 16 1.6 12.5Distal radius/ulna 78 7.8 10.3Proximal forearm 16 1.6 6.2Humeral diaphysis 18 1.8 5.5Hand phalanges 297 29.7 2.6Foot phalanges 42 4.2 2.4Distal humerus 17 1.7 0Metatarsus 11 1.1 0Proximal femur 1 0.1 100Clavicle 2 0.2 50Proximal humerus 5 0.5 20Pelvis 6 0.6 0Scapula 1 0.1 0
8
Table 3The distribution of different Gustilo grades and the requirement for plastic surgery in
open tibial fractures.
I II IIIa IIIbNumber 59 53 55 68No plastic surgery 86.4% 56.6% 32.7% 5.9%Split skin graft 10.2% 22.6% 36.3% 23.5%Local flap 3.4% 17.0% 27.3% 45.6%Local muscle flap 0 1.9% 3.6% 10.3%Distant flap 0 1.9% 0 14.7%
Table 5

2. INJURY RECOGNITION
One of the most significant factors in the outcome of any limb injury is the amount ofenergy absorbed by the tissues at the time of the injury. High energy tibial fractures,whether open or closed, may be associated with a poor prognosis and they thereforeconstitute the group of fractures that are most likely to benefit from early seniororthopaedic input and a combined Orthopaedic Surgery and Plastic Surgeryapproach. It is essential that the examining doctor recognises all high energy andopen tibial fractures and they are subsequently assessed on an emergency basis by anexperienced Orthopaedic Consultant.
The clues to the energy of the injury lie in the history, clinical examination and theradiological appearances. All findings should be clearly documented to facilitateearly decision making.
History
Knowledge of the mechanism of injury is essential. It will often give the only indica-tion of the level of energy transfer to the tissues. The patient will sometimes be ableto give a good history but often it will be obtained from the paramedics who bringthe patient to the hospital. The features that should alert the admitting doctors to thepossibility of a high energy injury include:
Any road traffic accident. Drivers, passengers or pedestrian.
Falls from a significant height.
Any injury mechanism involving extensive or localised crushing.
Missile wounds.
Contamination from the scene of the accident.
A history of entrapment or lying immobile on the injured limb for a prolongedperiod.
Any suggestion of possible limb ischaemia.
Examination
Systematic examination of the affected limb will reveal the following features ofhigh energy injury:
9

Skin
Large or multiple wounds.
Imprints or tattooing from dirt or tyres.
Crush or burst wounds.
Closed degloving. Skin is intact but with no blood supply due to shearingbetween the deep fascia and subcutaneous tissues. It can be difficult to diag-nose but may be suspected from the boggy feel of the skin or the abnormallooseness of the skin when it is pinched.
Signs of Compartment Syndrome
More pain than expected, even when the fractured leg is immobilised. Neverassume that severe pain is from the bone. Relentless pain unrelieved by opiatesis more likely to be produced by ischaemic muscle.
Pain on passive stretching of the muscles in the affected compartment.
A tense, swollen limb.
Sensory disturbance of the foot.
Tender or indurated muscle compartment (Late sign).
Signs of Vascular Injury
Absence of peripheral pulses or reduced capillary return after correction ofhypovolaemia and reduction of limb deformity.
Signs of Nerve Injury
Abnormal sensation is more important than loss of motor power as it occursearlier.
Never merely ask “Can you feel this?”. Compare the two sides.
Check all peripheral nerve territories, particularly that of the posterior tibialnerve, the plantar surface of the foot. Always examine several zones of eachnerve territory in case of a partial nerve lesion.
10

X-ray
The fracture pattern can often give clues to the degree of energy transferthrough the bone. Important features include:
Multiple bone fragments.
Wide displacement of fracture fragments.
Any segmental injury.
Air in the tissues.
More than one fracture in the same limb.
High energy injuries are never simple problems and the degree of tissue damage caneasily be underestimated. Poor outcomes often result if experienced senior staff arenot involved at an early stage and the presence of any of the above features meansthat the responsible Orthopaedic Consultant must be alerted.
11

3. COMMUNICATION
Communication between Consultant Orthopaedic and Consultant Plastic Surgeons isessential if combined care is to be delivered promptly and satisfactorily. Once theadmitting Orthopaedic Consultant has recognised that a patient has sustained a highenergy tibial injury he or she should initially decide whether it is best for the patientto remain under his or her care. If the Consultant does not have the facilities or expe-rience to manage such complex tibial injuries the case should be transferred to thecare of an appropriate colleague just as might occur if the patient had a spinal orpelvic injury. This should be done on the day of injury, after resuscitation.
The next step is for initial contact between Orthopaedic and Plastic teams to bemade, almost certainly at Consultant level, before the patient goes to theatre. Themechanism of initiating a combined approach will vary between districts.
Ideally the Plastic Surgery Service and the Orthopaedic Trauma Service, staffed by aConsultant with an interest in orthopaedic trauma, should be on one site to which allsevere injuries are channelled. If the Plastic Surgery Team is not on site it is essentialthat the Consultant Orthopaedic Surgeon communicates with his or her localConsultant Plastic Surgeon by telephone before embarking on the first operativeprocedure.
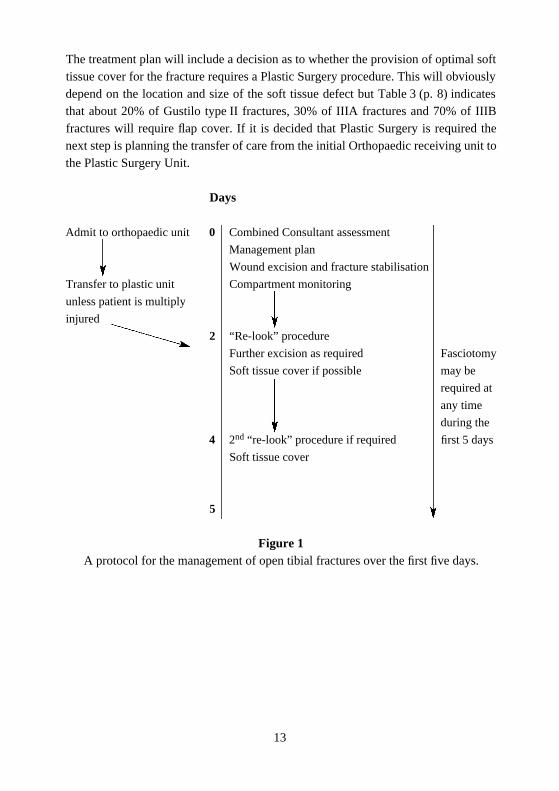
The purpose of communication is to establish a joint treatment plan for the first fivedays. Such a treatment plan is illustrated in Figure 1 (opposite). The minimalresponse from the Plastic Surgery Service is advice. Ideally the Consultant PlasticSurgeon, like the Orthopaedic Consultant, should have an interest in severe limbinjuries. Where the two specialties are on the same site it should be possible for themto examine the patient together shortly after admission. It is more difficult when thespecialties are on split sites. This however is no reason for there not to be a jointapproach to the management of the patient.
A telephone discussion may be all that is necessary to formulate a joint plan. If thesurgeons involved are used to managing trauma cases together a telephone discussionwill establish the location and size of the tissue defect, the method of bone fixationand the type of plastic reconstruction that will be required. Where there is any doubtabout the requirement for Plastic Surgery there is no alternative but for theConsultant Plastic Surgeon to see the patient before or in the early stages of the firstoperation. This may present the Consultant Plastic Surgeon with a number of prob-lems because of the travelling and the interruption of other work but the benefits ofembarking on a properly constructed treatment plan greatly outweigh these.
12
13
The treatment plan will include a decision as to whether the provision of optimal softtissue cover for the fracture requires a Plastic Surgery procedure. This will obviouslydepend on the location and size of the soft tissue defect but Table 3 (p. 8) indicatesthat about 20% of Gustilo type II fractures, 30% of IIIA fractures and 70% of IIIBfractures will require flap cover. If it is decided that Plastic Surgery is required thenext step is planning the transfer of care from the initial Orthopaedic receiving unit tothe Plastic Surgery Unit.
Days
Admit to orthopaedic unit 0 Combined Consultant assessment
Management plan
Wound excision and fracture stabilisation
Transfer to plastic unit Compartment monitoring
unless patient is multiply
injured
2 “Re-look” procedure
Further excision as required Fasciotomy
Soft tissue cover if possible may be
required at
any time
during the
4 2nd “re-look” procedure if required first 5 days
Soft tissue cover
5
Figure 1A protocol for the management of open tibial fractures over the first five days.

4. TIMING
The timing of Plastic Surgery is extremely important. Definitive soft tissue covermust be achieved within five days of the injury and, ideally, much sooner. Providingthere has been a thorough excision of all devitalised tissue, and this may well requiremore than one operation, it is accepted that the wound does not have to be covered bya flap or skin graft immediately. Indeed there are advantages in waiting until woundexcision is certain, swelling is decreasing, the threat of compartment syndrome isless and the method of bone fixation is finalised. However, the wound should be cov-ered within a maximum of five days7. With complex micro-vascular flaps it has beenshown that the success rate of the flap transfer is diminished if performed after thefifth day8, 9.
Following the initial orthopaedic operation in which wound excision and skeletal sta-bilisation is performed the Orthopaedic and Plastic Surgeons must decide whether a“relook” procedure 48 hours later is required and if so where it should be done. Ifsoft tissue injury is severe enough to warrant Plastic Surgical intervention the secondoperation should ideally take place within the Plastic Surgery Unit. This allows theConsultant Plastic Surgeon to assess the soft tissues, perform any further woundexcision that is required and close the wound using either split skin grafting or flapcover. If there is residual contamination or devitalised tissue there is still time to per-form a third wound excision procedure and provide soft tissue cover on or before thefifth day.
If the planned soft tissue reconstruction is a micro-vascular free flap it needs to bescheduled in the Plastic Surgery operating theatre. This is another important reasonfor early communication. Microvascular cases require relatively long operatingtimes, expert anaesthetic support and careful post-operative management. Theyshould always be performed by surgeons with microvascular experience.
If this protocol is followed, unnecessary anaesthetics can be avoided and treatmentcan proceed quickly, minimising the incidence of chest infection, deep venousthrombosis, anaemia and other problems.
14

5. PRE-OPERATIVE MANAGEMENT
The immediate management tasks are:
Assessment of the injury, as described in the recognition section, with particular ref-erence to compartment syndrome.
Formulation of the provisional treatment plan as described in the sections dealingwith communication and timing. The provisional treatment plan should consider:
Integration with care of other injuries.Consideration of early amputation in severe cases.Prevention of contamination by hospital organisms.
These tasks have to proceed in parallel with any resuscitation or other therapeuticmeasures that are required.
Compartment Syndrome in Open Fractures
There is a widespread belief that open tibial diaphyseal fractures do not present withcompartment syndrome because of the misconception that the soft tissue damageassociated with the fracture automatically decompresses the compartment. This is notthe case and there is now ample evidence that even Gustilo type III open tibial dia-physeal fractures can be complicated by compartment syndrome, with Keating et al10
reporting an incidence of 6%. In fact, the incidence of compartment syndrome inopen fractures is similar to that encountered in closed fractures. There are two rea-sons why compartment syndromes may occur in open fractures. Firstly some of thecompartments may remain closed despite the severity of the injury and secondly it isnow recognised that compartment syndromes can be localised. This means that whilesome of the musculature in a compartment may have been decompressed as a resultof overlying fascial damage adjacent parts of the muscle may still be enclosed inintact fascia and consequently develop a high compartment pressure.
The clinical symptoms and signs are identical to those seen in closed fractures. Theseare pain out of proportion to the injury, pain on stretching the muscle group,swelling, and sensory and motor dysfunction. Surgeons should abandon palpation ofthe peripheral pulses as a diagnostic test for compartment syndrome as by the timethe pulses have disappeared the muscles have undergone irreversible necrosis andamputation is inevitable. A number of patients with open tibial fractures will beunconscious on admission or will be placed on ventilators early in their management.Obviously the surgeon cannot rely on clinical symptoms and signs in these patients
15

and it is suggested that compartment monitoring be utilised.
There is no doubt that compartment monitoring is useful in diagnosing compartmentsyndrome. McQueen et al11 indicated that compartment pressure monitoring signifi-cantly reduces the delay to fasciotomy in acute compartment syndrome.Compartment pressure can either be measured using a “stick” method which can bepainful and labour intensive or by continuous monitoring. The technique of continu-ous monitoring is described by McQueen12. Isolated pressure measurement using a“stick” method provides a reliable assessment of tissue pressure at a given time.However compartment pressures are not static and to establish the diagnosis multiplereadings may be required. The continuous method requiring the insertion of one needle has the advantage of demonstrating pressure trends. The pressure thresholdfasciotomy has now been established13. The differential pressure between the dias-tolic blood pressure and the total tissue pressure should always be more than 30 mmof mercury. When it is less than 30 mm of mercury fasciotomy should be performedunless there is clear evidence that the total tissue pressure is rapidly dropping and thedifferential pressure is increasing.
Where surgeons do not have access to compartment monitoring or are dealing withunconscious or ventilated patients they should always consider the possibility ofcompartment syndrome. The incidence of this complication is much higher thanmany surgeons realise and the basic message is that if there is any doubt at all aboutthe presence of a compartment syndrome immediate fasciotomy must be performed.
Multiple Injuries
A further analysis of the 244 open tibial diaphyseal fractures presented in Tables 1and 2 (p. 6, 7) has shown that 19% of open tibial diaphyseal fractures in the UnitedKingdom occur in the multiply injured patient. The patient’s other injuries should notalter the approach to the tibial fracture and the necessity for combined plastic andorthopaedic planning remains. Whatever the other injuries wound excision must beperformed and the muscle compartments released if necessary. It is now acceptedthat the multiply injured patient must have skeletal stabilisation and that the overallsurvival is improved if the patient undergoes adequate stabilisation in the early stagesdespite the presence of other injuries14.
The Decision to Amputate
Some limbs, particularly those subjected to prolonged ischaemia, crushing or nervedamage, although theoretically salvageable may function very poorly. The patient
16

may well have multiple operations carried out over a prolonged period of time andend up with a leg which is painful and functions poorly. This is often to the detrimentof the patient’s morale, employment and social status. Furthermore it is a commonexperience that function and morale are very poor following a late amputation afterfailure of reconstruction15,16. An early correct decision regarding amputation istherefore very important and if a leg is so badly damaged that amputation is consid-ered to be an option there should be an early joint assessment by an OrthopaedicSurgeon and a Consultant Plastic Surgeon both of whom should be experienced inthe management of severe leg injury.
Although a late decision to amputate is inadvisable it can also be unkind to make toohasty a decision. The patient and their relatives often need time for the severity of theinjury to sink in and to allow them to participate in the decision and feel it is the cor-rect one. Unless the soft tissues of the leg have been so extensively damaged by theinjury that it is clear that retaining the limb could be life threatening, it is usually bet-ter to perform initial salvage surgery, and amputate if necessary at the time of thesecond look procedure. This will normally be within 48 hours.
Various extremity scores have been devised17,18 to assist in predicting the outcomeof reconstructive attempts. These scores may be useful but it is unwise to dependexclusively on them and it is important that an experienced surgeon should be giventhe opportunity to assess doubtful cases at the earliest opportunity.
Prevention of Wound Infection
The first orthopaedic procedure has as one of its objectives the removal of micro-organisms contaminating the fracture from the scene of the injury. However by farthe greatest micro-biological threat comes from organisms in the hospital environ-ment many of which will have developed antibiotic resistance. Contamination canoccur very quickly and must be prevented. To minimise contamination a number ofprocedures are suggested:
The surgeon should assess the microscopic contamination of the wound andsend a swab for bacteriological analysis.
The wound should be immediately covered with a Betadine swab or cling film,preferably after taking a polaroid photograph. The wound should not be uncov-ered again until the patient is in theatre.
The patient should be given ATT and antibiotics.
17

It is recommended that a broad spectrum antibiotic be used in every patient with anopen tibial injury regardless of the severity. There is considerable debate about whichantibiotics or combination of antibiotics should be used but it is essential that sur-geons and microbiologists in any unit have a consistent protocol. It is now acceptedthat it is unnecessary to give patients with an isolated open fracture long courses ofantibiotics and a three dose regime of an appropriate antibiotic should be satisfactoryfor all Gustilo type I, II and IIIA fractures. Gustilo type IIIB fractures with associatedmuscle damage should be covered by Penicillin in addition to the broad spectrumantibiotic. The surgeon may choose to increase the course of antibiotics for thesefractures19,20.
18

6. THE FIRST ORTHOPAEDIC PROCEDURE
All open high energy tibial fractures should be classified as a surgical emergency andthe first orthopaedic procedure should be undertaken within six hours of injury. Allopen fractures require surgical exploration irrespective of the size of the skin wound.This vital procedure must be performed by a senior Orthopaedic Surgeon and, if atall possible, a senior member of the Plastic Team should also attend the first surgicalexploration. If this is not possible communication should already have been estab-lished with a detailed description of the injury passed onto the Plastic Surgeon.
The most important aspects of the first orthopaedic operation are:
Wound extension.
Wound excision.
Fracture stabilisation.
Wound Extension
The size of the traumatic skin wound does not always reflect the degree ofdamage to the soft tissues of the leg. Therefore the skin wounds in all openfractures, including Gustilo type I fractures, must be extended to allow ade-quate inspection of both the soft tissues and bone ends. The arbitrary distinc-tion between fractures that are open from within and open from without shouldbe abandoned as both require wound excision. Wound extensions should belongitudinal and transverse incisions should be avoided. The exact directionand length of the wound extension will depend on the extent and location ofthe subcutaneous damage. However the surgeon should open up all areas ofsubcutaneous soft tissue damage. When undertaking wound extension it isvital that the surgeons be aware of the position of the medial and lateral perfo-rators so that these are not damaged during the procedure. These can bemapped using a hand-held doppler. The surgeon should also avoid cuttingundamaged skin overlying the subcutaneous border of the tibia.
Wound Excision
The objective of wound excision is to remove all devitalised or contaminatedtissue so that at the end of the procedure the remaining tissue looks clean andhealthy and has an adequate blood supply. The courage to excise tissue onlycomes with experience; hence the need for the primary procedures to be per-
19

20
formed by senior surgeons. In cases where assessment of tissue viability is dif-ficult, particularly in multiply injured or hypovolaemic patients where tissueperfusion is poor, it is often difficult to decide on the extent of wound excision.The leg should be re-explored under general anaesthetic within 48 hours toensure that the wound excision has been thorough. The principal tissues to beconsidered in wound excision are skin and the subcutaneous tissues, muscleand bone.
Treatment of Skin and Subcutaneous Tissues
The wound edges must be excised until good dermal bleeding is encounteredhowever large a skin defect this creates. The surgeon may well find that thereare further areas of skin degloving which will become devitalised by the timeof the second relook procedure. These may eventually have to be excised inorder to provide the optimal environment for fracture healing but they may beleft initially provided they have a good dermal blood supply.
On the day of injury it may be possible to salvage degloved skin for use as askin graft. If it is in good condition it can be defatted and applied straight awayas a full thickness skin graft. If it is damaged as well as degloved, a split thick-ness skin graft can be taken from it. This can either be stored or applied imme-diately. These procedures can only be done on the day of injury as after thistime the skin is not salvageable.
Skin is remarkably resistant to direct trauma and the extent of the skin excisionaround the wound may be very limited to removing only the contused edges ofthe wound. Subcutaneous fat however is susceptible to direct trauma and thearea of subcutanteous necrosis can often be larger than the area of dead skin.The difficult decision, whether to excise viable skin to get rid of all subcuta-neous necrosis to permit better subsequent reconstruction, is one of the mainreasons why the early involvement of Plastic Surgeons is so important.
Treatment of Muscle
Unlike skin, muscle is very sensitive to direct trauma and it is often difficult todelineate the extent of muscle damage at the time of primary wound excision.The usual methods of assessing the vitality of muscle, namely colour and con-tractility can be notoriously unreliable. All obviously devitalised or contami-nated muscle must be removed. The fascia must be released longitudinallyover the muscle compartments. As muscle is particularly susceptible to crush-

ing injury there must be a low threshold for re-inspection at a second relookoperation within 48 hours and again at further operations if necessary until it iscertain that all devitalised muscle has been removed.
Treatment of Bone
The basic philosophy regarding excision of bone is the same as for the soft tis-sues. All devitalised separate bone fragments should be removed as should allbone fragments that are only attached by devitalised soft tissues. Separate frag-ments that have retained their blood supply can be left. In tibial diaphysealfractures it is not uncommon to have to remove all separate bone fragmentsalthough in femoral diaphyseal fractures the bone fragments attached to thelinea aspera are usually vital and can be retained. In the femur there is alsooccasionally periosteal and soft tissue stripping from a considerable length ofbone which remains attached proximally. There may well be viableintramedullary and intra-cortical circulation present and the periosteallydepleted bone should not be removed.
The excision of bone often causes anxiety to junior surgeons. However a num-ber of techniques are available to reconstruct large bony defects and there is noneed to worry about later problems of restoring bone integrity when carryingout a bone excision. An inadequate excision is far more likely to give problemsof non-union or infection.
Lavage
After all contaminated and devitalised tissue has been excised the woundshould be thoroughly irrigated. It is suggested that the surgeon use at least sixlitres of normal saline or Hartmann’s solution either by free flow from the giv-ing set or a pulsed lavage system. At the moment there is little evidence thatthe use of antiseptic or antibiotic solutions is preferable.
Fracture Stabilisation
Following wound excision the Orthopaedic Surgeon must select a method ofbone stabilisation. The choice may be determined by such factors as the posi-tion of the fracture and the extent of the soft tissue damage or contamination. Itis likely however that external skeletal fixation or interlocking intramedullarynailing will be used for diaphyseal fractures and either plating or externalskeletal fixation for proximal or distal metaphyseal fractures. The surgeon
21

should select a technique with which he or she is familiar. It is not the remit ofthis document to recommend any particular method but there are a number ofpotential problems that the surgeon must be aware of with each stabilisationtechnique.
If plating is employed care must be taken not to strip soft tissues from the boneunnecessarily and thereby reduce its vascularity. The plate must be coveredwith soft tissues at the end of treatment and this may necessitate the use oflocal or free flaps.
Intramedullary nailing of open diaphyseal fractures has become an acceptedtechnique. Both reamed and unreamed nails have been used with success. Thetheoretical advantages of unreamed nails with respect of endosteal blood sup-ply and spread of infection appear to be balanced in clinical practice by thebenefits of reaming in inducing bone healing and the greater strength of thelarger implants. Surgeons should proceed with caution in nailing tibial frac-tures where there is evidence of significant intramedullary contamination.Great care must be taken not to spin a short isolated tibial fragment whenreaming segmental fractures.
If external skeletal fixation is used care must be taken to place the pins so asnot to compromise either the potential skin flaps or access to the vessels formicrovascular anastomoses. Figure 2 shows the safe arc for placement ofexternal fixator pins.
Wound Closure
The excised primary wound should never be closed. It is impossible to closean excised wound in an oedematous area without tension. There is debate as towhether skin extensions should be closed primarily but if there is any sugges-tion of excessive skin tension it is always safer to achieve skin cover as a secondary procedure.
Summary
At the end of the first orthopaedic procedure the following goals should havebeen met:
All devitalised tissues should have been excised with the wound beingextended as far as is required to achieve this.
The fracture should have been stabilised to permit subsequent plasticsurgery preferably using a method which is definitive and does notrequire to be changed at a later date.
22


7. SAFE INCISIONS AND FASCIOTOMY
It is important that surgeons understand where they can incise safely to avoid damag-ing perforating vessels. These incisions are important in extending the open woundsand for fasciotomies. There are two safe incisions:
Medial Incision
A longitudinal incision 1–2 cms posterior to the medial border of the tibia(Figure 3, opposite). The surgeon should cut straight down through fasciawithout undermining the tissues superficial to the deep fascia. This incision isanterior to the line of the posterior tibial neurovascular bundle and is thereforeanterior to the perforators that arise from the posterior tibial artery and passthrough the fascia to the skin. This relationship with the perforating arteries iscrucial. By placing the longitudinal incision anterior to these perforators theyare preserved and hence the medial fasciocutaneous flap, either proximally ordistally based, is preserved. This medial longitudinal incision lies posterior toany external fixator pins that may be used.
Antero-Lateral Incision
A longitudinal incision is made between the anterior border of the tibia and themid-lateral line about 2 cms lateral to the anterior border of the tibia (Figure 4,p. 26). Again the surgeon incises straight down to fascia. This longitudinalincision is anterior to the line of the perforating arteries that come from theperoneal artery and run through the deep fascia between the peroneal andsuperficial calf muscle groups. By placing this incision antero-laterally it pre-serves both the proximally and distally based lateral fasciocutaneous flaps.
A longitudinal incision over the distal fibula is likely to cut these perforatorsand hence sacrifice the lateral fasciocutaneous flap. This lateral fasciocuta-neous flap may be an important simple reconstructive flap needed in thepatient. If it is necessary to make a longitudinal exposure of the fibula in anopen leg injury it is worth discussing this with the Plastic Surgeon involved inthe reconstruction.
24



Fasciotomy
If compartment syndrome is diagnosed fasciotomies are required. All fourcompartments can be exposed through one incision but the dissection is diffi-cult and it is often difficult to visualise all four compartments. It is recom-mended that two longitudinal incisions using the safe incisions alreadydescribed be employed. The anterior and lateral compartments can be decom-pressed through an antero-lateral incision and the superficial and deep poste-rior compartments are decompressed through the medial incision. Figures 3, 4and 5 indicate where the deep fascia can be incised without compromising sub-sequent Plastic Surgery procedures. The antero-lateral incision (Figures 4 and5) goes through the deep fascia to decompress the anterior compartment.Subsequent lateral dissection under the deep fascia will release the lateral com-partment. The medial longitudinal incision (Figures 3 and 5) passes downthrough the deep fascia to decompress the superficial posterior muscle com-partment which comprises the gastrocnemius and soleus muscles. Releasingthe deep posterior musculature is a somewhat more difficult dissection. Thedeep posterior muscle compartment can be seen distally posterior to the tibiacovered by its fascia and anterior to the posterior tibial neurovascular bundle.This is divided using a longitudinal incision but to gain proximal access thesuperficial muscle group has to be elevated from the posterior border of thetibia. There are segmental arteries that pass from the posterior tibial artery tothe tibia and these should be preserved. The individual muscles in the deepcompartment are not separately exposed.
Fasciotomy wound closure can be achieved by a number of techniques. It isoften possible to close one of the fasciotomy wounds directly and close thesecond wound by either controlled tension techniques or with split skin graft-ing. Occasionally it may be necessary to split skin graft both wounds and veryoccasionally flap cover may be required.
27


8. COMMONLY USED METHODS OF SOFT TISSUERECONSTRUCTION
Introduction
Cooperation between the Consultant Orthopaedic Surgeon and Consultant PlasticSurgeon has been emphasised. The following methods of soft tissue reconstructionare those commonly used by Plastic Surgeons specialising in lower limb trauma andare described here for guidance if wound excision has to be carried out without thepresence of a Consultant Plastic Surgeon. These techniques are complex and timeconsuming and should only be carried out by Plastic Surgeons specifically trained inlower limb reconstruction.
There are three ways to close wounds; in order of increasing surgical complexity:
Skin grafting.
Local flaps.
Microvascular free flaps.
Depending on case mix and individual surgeon preference there is a wide variationbetween units in the balance of the use of these methods. Each method has its advan-tages and disadvantages. Even the local flaps, although simple in concept, have manypitfalls and subtleties in their design and in the process of raising them. The outlinedrawings to follow give an indication of the position of these flaps and are designedto help the surgeon to preserve all the reconstructive options. They are not a guide toperforming the procedures which should be carried out by experienced PlasticSurgeons. Microvascular flaps are even more technically and anaestheticallydemanding and should only be done in those Plastic Units where they are regularlyundertaken.
29

Advantages and Disadvantages of Split Skin Grafts,Local Flaps and Free Flaps
Skin Grafts
Skin grafts are technically simple to perform. When put on as mesh skin grafts theycan cover large soft tissue defects. They require a vascularised bed for survival sothey cannot be used on bare cortical bone without overlying periosteum, on openjoints or tendons without their paratenon. Heavily infected wounds are a relative con-tra-indication for grafting but not an absolute contra-indication. Split skin grafts pro-vide a wound with very thin skin cover which is not durable. If it overlies muscle itwill probably be satisfactory but if it overlies tendon or bone it is vulnerable andoften provides poor quality skin cover. Split skin grafting also has the disadvantagesof not bringing in a new blood supply and providing skin cover which is difficult tore-operate through. It should therefore not be used to close a wound that requires tobe re-opened for further surgery.
Local Flaps
Local flaps can be used to provide closure for many, but not all, leg defects (Table 3,p. 8). They require considerable planning. When successful they provide flap coverthat is fixed, durable, provides its own blood supply and is suitable as a cover forareas in which there may be further surgery. Local flaps however can be cosmeticallyunattractive and can produce extra scarring on the leg with some of the fasciocuta-neous flaps producing “dog ears” which are very noticeable. It may be possible toreduce the “dog ears” by islanding the flaps, but this requires considerable expertise.The flap donor site has to be resurfaced with a split skin graft. This is rarely a func-tional problem but does provide a noticeable cosmetic problem.
Free Flaps
These flaps have the ability to cover both small and large defects. They require theflap to be taken from another part of the body so the flap donor site defect, called asecondary defect, is distant. The cosmetic aspect of this will need to be discussedwith the patient. These free flaps provide powerful ways of closing wounds. Theybring in a new blood supply and provide very suitable cover through which to under-take further surgery. They are however technically difficult to do and require both agreat deal of operating time and considerable anaesthetic expertise.
30

Which Method of Skin Closure?
When deciding on the method of closure of a soft tissue defect the Orthopaedic andPlastic Surgeon should consider not just the initial healing of the wound but therequirement for secondary surgery at a later date. Not infrequently Plastic Surgeonsconsider soft tissue closure to be an end in itself. However both the Plastic andOrthopaedic Surgeons should realise that in a difficult open tibial fracture multipleoperations may be required and the soft tissue cover that is chosen, whether it be skingraft, local flap or free flap should allow for further orthopaedic procedures to be per-formed. If there is a likelihood of bone grafting being required then a flap should beused rather than split skin graft. A wound that is covered with a split skin graft can-not be re-opened. If such a wound needs to be re-opened it will have to be initiallyresurfaced by a flap before any orthopaedic procedure is undertaken.
Types of Available Flap
Local Flaps
The development of local flaps has greatly simplified the closure of many woundsthat cannot be closed by split skin graft. Local flaps are classified into two anatomicalgroups:
Fasciocutaneous flaps.
These can be designed on the medial or lateral aspects of the leg. Theycan be proximally based or, in some circumstances, distally based.Proximally based flaps (Figures 6, p. 33 and 7, p. 34), though generallyreliable may prove troublesome following trauma in the elderly or inpatients with diabetes. Distally based fasciocutaneous flaps (Figures 8,p. 35 and 9, p. 36) are relatively new flaps and their place in the recon-struction of the leg is still being evaluated. However they are gaining inimportance and most of the local flaps detailed in Table 3 (p. 8) were infact distally based fasciocutaneous flaps.
Muscle flaps.
These are generally reliable and are thought to be particularly useful incovering bare bone and preventing deep infection. They are of relatively
31

small size and may involve some functional loss in the leg. In practicethey are rarely used to reconstruct defects after leg trauma because localfasciocutaneous flaps are now preferable. Fasciocutaneous flaps are big-ger, more versatile and give better quality cover than muscle flaps. Thecommonest muscle flap used by surgeons is the gastrocnemius flap. Thisis used to resurface the knee and proximal third of the tibia. Previouslythis has been used successfully as a myocutaneous flap, but the use of alocal fasciocutaneous flap in this situation reduces potential functionaldeficit. The pure gastrocnemius muscle flap is useful and can be coveredby split skin; however, surgeons should be aware of the fact that themuscle adheres closely to the bone and may be difficult to elevate againshould further surgery be required.
Microvascular Free Flaps
Although technically demanding and time-consuming the technique of microvascularflap cover is so powerful and flexible that many units will use free flaps in almost anysituation where flap cover is required. They are particularly indicated in large or dis-tal defects. Free flaps are regarded as being virtually 100% successful in units whichundertake them regularly, particularly if the Godina approach for proximal or middlethird defects is used. The latissimus dorsi flap is the most commonly used free flapfor resurfacing large tibial defects8. It is popular because of its large size, its long andreliable vascular pedicle and its relatively good donor site defect. Other free flapsmay be considered in any given tibial defect but they are beyond the scope of thisbooklet.
The vascular access for anastomising free flaps is most important and requires care-ful consideration. Broadly speaking it is performed at one of two sites:
In proximal and middle third free flaps anastomosis is to the popliteal vesselsor their continuation in the mid calf. Exposure is by a midline posteriorincision21.
In the distal half anastomosis is to the posterior tibial vessels and vena comi-tans; occasionally to the long saphenous vein medially.
The various flap options for covering tibial defects at all levels are summarised inTable 4 (p. 37) and the advantages and disadvantages of the various methods ofcovering soft tissue defects in Table 5 (p. 38).
32
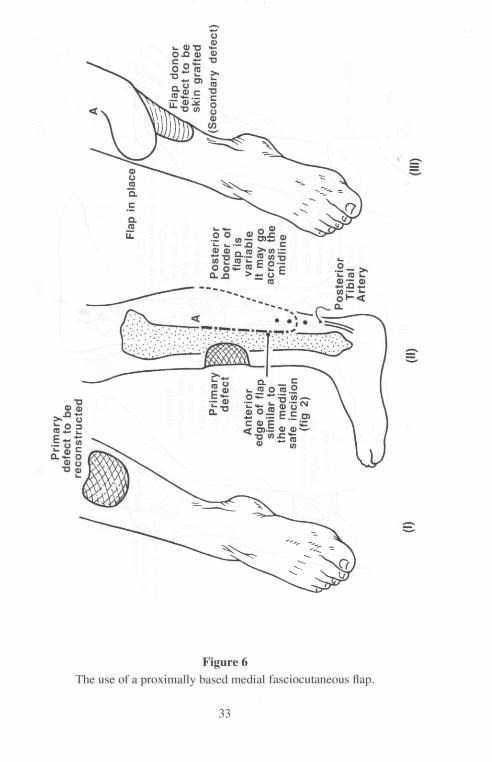
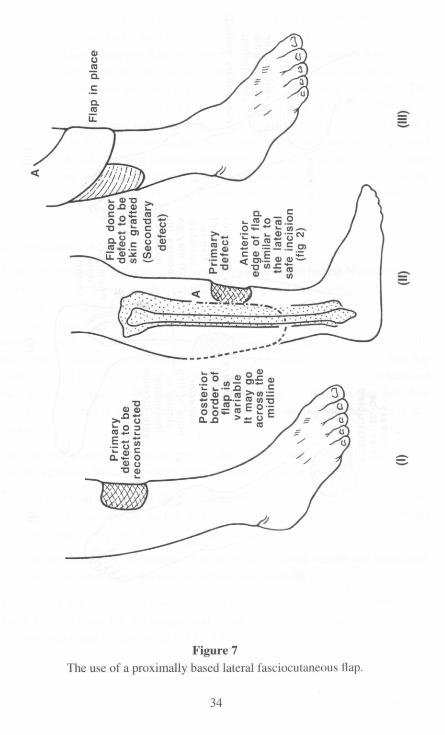

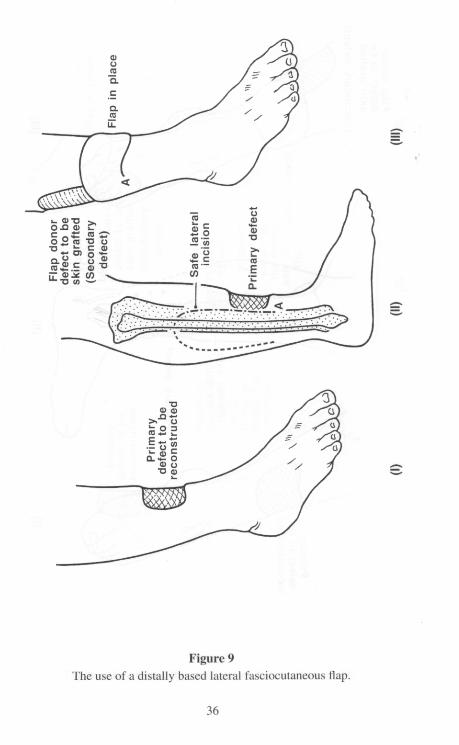
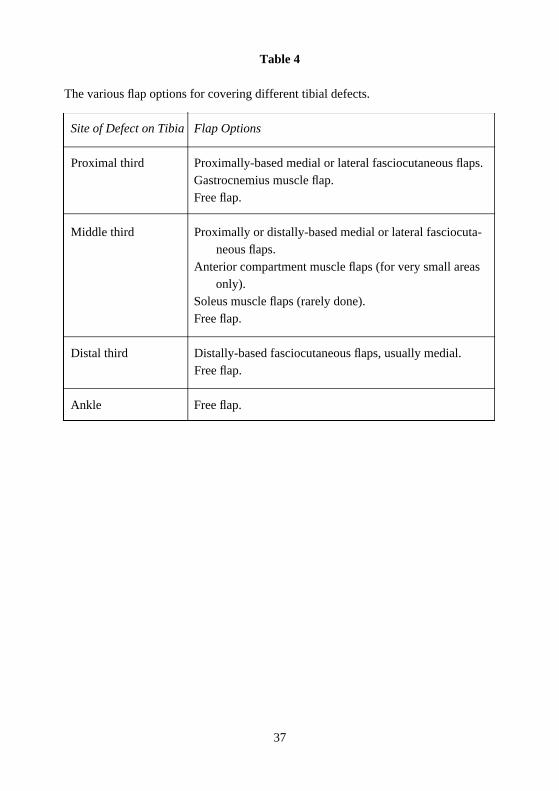
Table 4
The various flap options for covering different tibial defects.
Site of Defect on Tibia Flap Options
Proximal third Proximally-based medial or lateral fasciocutaneous flaps.Gastrocnemius muscle flap.Free flap.
Middle third Proximally or distally-based medial or lateral fasciocuta-neous flaps.
Anterior compartment muscle flaps (for very small areasonly).
Soleus muscle flaps (rarely done).Free flap.
Distal third Distally-based fasciocutaneous flaps, usually medial.Free flap.
Ankle Free flap.
37

The advantages and disadvantages of the various methods of soft tissue closure.
A d v a n t a g e s D i s a d v a n t a g e s
Skin grafts S t r a i g h t f o r w a r d . Do not take on bare corticalCan be put on any bed with a b o n e .blood supply particularly Do not allow re-operation atp e r i o s t e u m . that site.Mesh grafts expand the area Cosmetically poor.of skin used. Not a durable cover.
Local fla p s
Muscle fla p s Gastrocnemius flaps are very Can produce functional loss.useful around the knee and For the middle third of the tibiaproximal third of the leg they are only suitable for very
small defects.In the distal third of the tibiathey have virtually no place inmodern reconstruction.Re-opening of the site of amuscle free flap requirescareful planning.
F a s c i o c u t a n e o u s Simple in concept although not Produces quite a noticeablefla p s always technically simple. cosmetic defect.
Produce good, durable cover. Cannot be used if theCan be re-opened for bony perforators have been lost.s u r g e r y .Bring in their own blood supply.
Free fla p s Bring in their own blood supply. Technically demanding.Suitable for small to extremelylarge defects.Need careful planning of thesecondary defect on anotherpart of the body.
38

References
1. The Early Management of Severe Tibial Fractures: The Need for Combined Plastic and
Orthopaedic Management. BOA/BAPS, London, January 1993.
2. Phillips H. The SAC and Training in Trauma, in British Orthopaedic News, Edition 14,
Summer 1996.
3. Court-Brown CM & McQueen MM. Trauma Management in the United Kingdom, J
Bone Joint Surg (Br) 1997; 79B: 1–3.
4. Court-Brown CM & Brewster N. Epidemiology of open fractures. In Court-Brown MM,
McQueen MM, Quaba AA (Eds). Management of open fractures. Martin Dunitz, London,
1996.
5. Gustilo RB, Anderson JT. Prevention of infection in the treatment of one thousand and
twenty-five open fractures of long bones: retrospective and prospective analysis. J Bone
Joint Surg (Am) 1976; 58–A: 453–8.
6. Gustilo RB, Mendoza RM, Williams DN. Problems in the management of type III
(severe) open fractures: a new classification of type III open fractures. J Trauma 1984;
24: 742–6.
7. Caudle RJ & Stern PJ. Severe open fractures of the tibia. J Bone Joint Surg 1987; 69A:
801–7.
8. Godina M. The tailored latissimus dorsi flap. Plast Reconstr Surg 1987; 80: 304.
9. Fischer MD, Gustilo RB & Varecka TF. The timing of flap coverage, bone grafting and
intramedullary nailing in patients who have a fracture of the tibial shaft with extensive
soft tissue injury. J Bone Joint Surg (Am) 1991; 73A: 1316–22.
10. Keating JF, O’Brien PJ, Blachut PA, Meek RN & Broekhuyse HM. Intramedullary nail -
ing of open fractures of the tibia. Clin. Orthop 1997, in press.
11. McQueen MM, Christie J & Court-Brown CM. Acute compartment syndrome in tibial
diaphyseal fractures. J Bone Joint Surg 1996; 78B: 95–98.
12. McQueen MM. How to monitor compartment pressures. Techniques in Orthopaedics
1996; 11(1): 99–101.
13. McQueen MM & Court-Brown CM. Compartment monitoring in tibial fractures: the
pressure threshold for decompression. J Bone Joint Surg 1996; 78B: 99–104.
14. Johnson KD, Cadambi J & Seubert GB. Incidence of adult respiratory distress syndrome
in patients with multiple musculoskeletal injuries: effect of early operative stabilisation of
fractures. J Trauma 1985; 25: 375–84.
15. Bondurant FJ, Cotler HB, Buckle R, Miller-Crotchett P & Browner BD. The medical and
economic impact of severely injured lower extremities. J Trauma 1988; 28: 1270–3.
16. Pozo JL, Powell B, Andrews BG, Hutton PA & Clarke J. The timing of amputation for
lower limb trauma. J Bone Joint Surg 1990; 72B: 288–92.
17. Johansen K, Daines M, Howey T, Helfet D & Hansen ST. Objective criteria accurately
predict amputation following lower extremity trauma. J Trauma 1990; 30: 568–73.
39

18. Robertson PA. Prediction of amputation after severe lower limb trauma. J Bone Joint
Surg 1991; 73B: 816–8.
19. Wilkins J & Patzakis M. Choice and duration of antibiotics in open fractures. Orthop
Clin North Am 1991; 22: 433–7.
20. Robinson, D, On E, Hadas N, Halperin N, Hofman S & Boldur I. Microbiologic flora con -
taminating open fractures: its significance in the choice of primary antibiotic agents and
the likelihood of deep wound infection. J Orthop Trauma 1989; 3: 283–6.
21. Godina MD, Zoran MA, Lister GD. Preferential use of the posterior approach to blood
vessels of the lower leg in microvascular surgery. Plast Reconstr Surg 1991 Aug; 88(2):
387–91.
40

Printed in England by Chandlers Printers Ltd., Saxon Mews, Reginald Road, Bexhill-on-Sea, East Sussex.
British Orthopaedic Association35-43 Lincoln’s Inn Fields
London WC2A 3PNTel: 0171-405 6507Fax: 0171-831 2676
British Orthopaedic Associationand
British Association of Plastic Surgeons
The Management of Open Tibial Fractures
September 1997


















