Brief Intervention for Problem Substance Use in Persons With Moderate to Severe TBI Angelle M....
29
Brief Intervention for Problem Substance Use in Persons With Moderate to Severe TBI Angelle M. Sander, Ph.D. Assistant Professor Department of Physical Medicine & Rehabilitation Baylor College of Medicine/ Harris County Hospital District Project Co-Director Rehabilitation Research and Training Center on Community Integration in Persons With Traumatic Brain Injury The Institute for Rehabilitation and Research
-
Upload
hubert-lawson -
Category
Documents
-
view
214 -
download
0
Transcript of Brief Intervention for Problem Substance Use in Persons With Moderate to Severe TBI Angelle M....
Brief Intervention for Problem Substance Use in Persons With
Moderate to Severe TBI Angelle M. Sander, Ph.D.
Assistant Professor
Department of Physical Medicine & Rehabilitation
Baylor College of Medicine/
Harris County Hospital District
Project Co-Director
Rehabilitation Research and Training Center
on Community Integration in
Persons With Traumatic Brain Injury
The Institute for Rehabilitation and Research

Grant Support
• Rehabilitation Research and Training Center on Community Integration in Persons With Traumatic Brain Injury – Co-Project Directors: Angelle M. Sander, Ph.D.
& Margaret A. Struchen, Ph.D.– Director of Training: Karen Hart, Ph.D.– Co-Investigator: Sunil Kothari, M.D.

Brief Intervention for Problem Substance Use
• Joint project between The Institute for Rehabilitation and Research (Texas) and Ohio State University
• Principal Investigators– Angelle Sander, Ph.D. (Texas)– John Corrigan, Ph.D. & Jenny Bogner, Ph.D. (Ohio)
• Level I trauma centers– Ben Taub General Hospital (Houston)– Grant Hospital (Columbus)
Pre-Injury Substance Abuse
• Blood alcohol levels at time of injury- 36 to 51% positive
• Structured interviews or questionnaires- 37 to 66% positive for alcohol abuse
• Other drug use- 36 to 37%
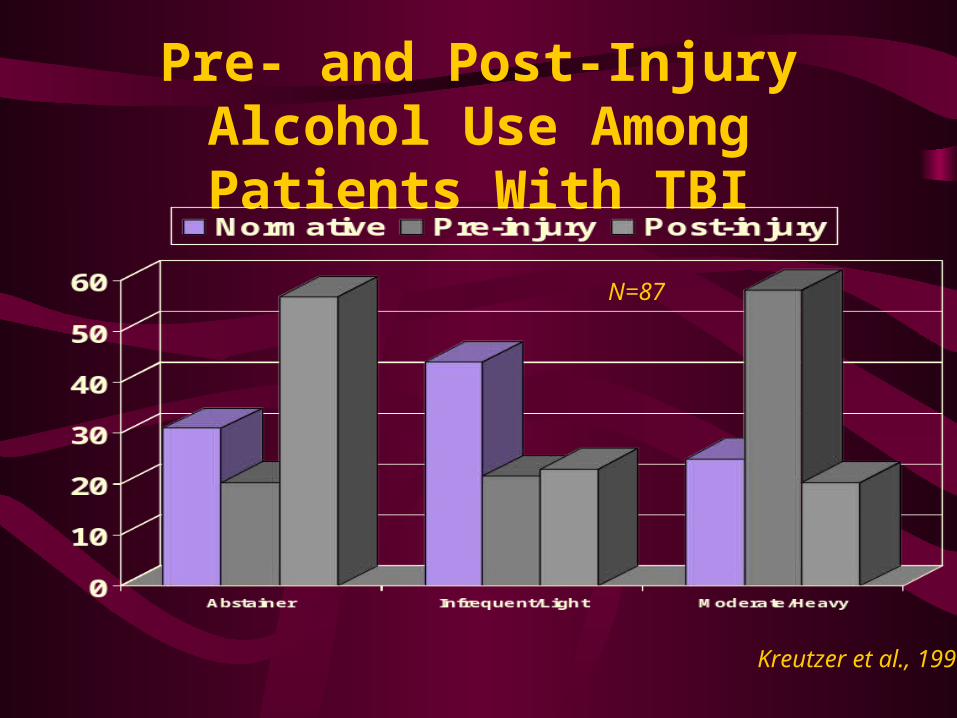
Pre- and Post-Injury Alcohol Use Among Patients With TBI
Kreutzer et al., 1990
N=87

Impact of Alcohol Abuse History on Outcome After TBI
• Associated with a reduced rate of good outcome on the Glasgow Outcome Scale (Ruff et al., 1990)
• Associated with emotional and behavioral deterioration at 6 months post-injury (Dunlop et al., 1991)
• Associated with re-injury/subsequent TBI (Kaplan & Corrigan, 1992)

Impact of Alcohol Abuse History on Outcome After TBI
• Associated with impaired event-related potentials indicating cognitive slowing in response to stimulation (Baguley et al., 1997)
• Associated with poor neuropsychological test performance (Brooks et al., 1989; Dikmen et al., 1993)

Impact of Alcohol Abuse History on Outcome After TBI
• Predictive of employment (Sherer et al., 1999; MaMillan et al., 2002)
• Predictive of independent living status (MacMillan et al., 2002)
• Predictive of life satisfaction (Corrigan et al., 2001)

Barriers to Substance Abuse Treatment After TBI
• Cognitive deficits, including impaired memory, judgment, and awareness
• Social environment
• Boredom, inactivity
• Lack of experienced referral sources
• Not ready to change
Transtheoretical Stages of Change Model
(Prochaska et al., 1992)
• Persons with problem behaviors operate at different stages of readiness for change.
• Intervention works best if it is matched with the person’s readiness for change.
Stages of Readiness for Change
• Precontemplation: problems not acknowledged and no change considered
• Contemplation: acknowledges problem, but no commitment to change
• Preparation: sets goals for change; may begin preliminary attempts to change

Stages of Readiness for Change
• Action: makes changes in behavior and in the environment to support changes
• Maintenance: changes established and goal is to prevent relapse
Readiness to Change Alcohol Use After TBI
• Occurrence of trauma may result in a “teachable moment” (general trauma and spinal cord injury)
• The majority of persons with TBI in an inpatient rehab program were in contemplation or action stage (Bombardier et al., 1997).
• Those with higher BALS or higher preinjury alcohol consumption showed greater readiness to change.
Randomized Trial of a Brief Substance Abuse Intervention
• Persons with complicated mild, moderate, and severe TBI admitted to trauma services at one of the 2 participating Level I trauma centers
• Persons who screen positive for history of alcohol and/or drug abuse are randomly assigned to receive brief intervention or hospital standard of care.
Exclusion Criteria • Age <18• Glasgow Coma Scale score >12 upon ER
admission AND no positive CT/MRI findings
• If no GCS available, then loss of consciousness < 20 minutes
• Discharged to an inpatient rehab facility other than those associated with the 2 Level I trauma centers
• Discharged to a nursing home or long-term care facility or to a prison
Screening Criteria for Randomization to Treatment
• Admit blood alcohol level > or = .08• Laboratory tests positive for cannabis,
cocaine, or any other illicit substance• Positive response to at least 2 CAGE
questions• Score of >5 on the Drug Abuse Screening
Test• Alcohol Use Questionnaire: >14 drinks per
week for men; >7 for women; one day per week of 5 or more drinks; any illicit drug use

Brief Intervention • Videotape created by Ohio Valley Center for
Brain Injury Prevention and Rehabilitation (Ohio State University): education regarding the impact of alcohol on functioning after TBI (10 minutes)
• Brief (10-15 minute) motivational interview: encourage discussion of recovery goals and how substance use will help or hinder goals; non-directive
• Delivered when fully oriented, up to one month post-discharge
Follow-Up Measures (3-4 months)
• Alcohol Expectancy Questionnaire-III– 40 Likert items– 8 factors
• Positive expectancies: Global Positive, Social and Physical Pleasure, Social Expressiveness, Sexual Enhancement, Power and Aggression, Tension Reduction
• Negative Expectancies: Cognitive and Physical Impairment, Careless Unconcern
– Global Positive and Cognitive and Physical Impairment used for current study
Follow-Up Measures • Readiness to Change Questionnaire
– 12 Likert items assessing a person’s belief about drinking or drug use and the perceived importance of change
– “Sometimes I think I should cut down on my drinking.”
– Precontemplation, Contemplation, and Action scales
– Currently using 10 items based on Bombardier & Heinemann’s validation study for TBI
Follow-Up Measures
• Alcohol and drug use questions from the TBI Model Systems national dataset– Adapted from questions used in the CDC’s
National Household Survey on Drug Abuse – “During the past month, how many days per
week or month did you drink any alcoholic beverages on the average?”
– “On the days when you drank, about how many drinks did you drink on the average?”

Follow-Up Measures
• Alcohol and drug use questions from the TBI Model Systems national dataset– “…how many times during the past month did
you have five or more drinks on one occasion?”
– “During the past month, have you used illicit or non-prescription drugs?”
Status of Study
• Data collection began August 2004
• 106 persons enrolled and screened for problem history– 73 Texas– 33 Ohio
• 70 met criteria for problem substance use history and randomized to treatment or standard of care– 48 Texas– 22 Ohio

Demographics By Center
Texas Ohio
Gender
Male 72% 76%
Race
White 19% 79%
Black 32% 12%
Hispanic 43% 3%
Education
<12 years 47% 12%
Unemployed 28% 45%

Injury Severity by Center
Texas Ohio
ER admit GCS score
11.55 (SD=3.81)
11.15 (SD=4.91)
Length of Stay 16.88 (SD=25.19)
9.33 (SD=8.72)

Proportion of Persons Meeting Problem Substance Use Criteria
0
10
20
30
40
50
60
70
80
90
BAL TOXLAB
CAGE DAST AlcoholUse
IllicitDrug Use
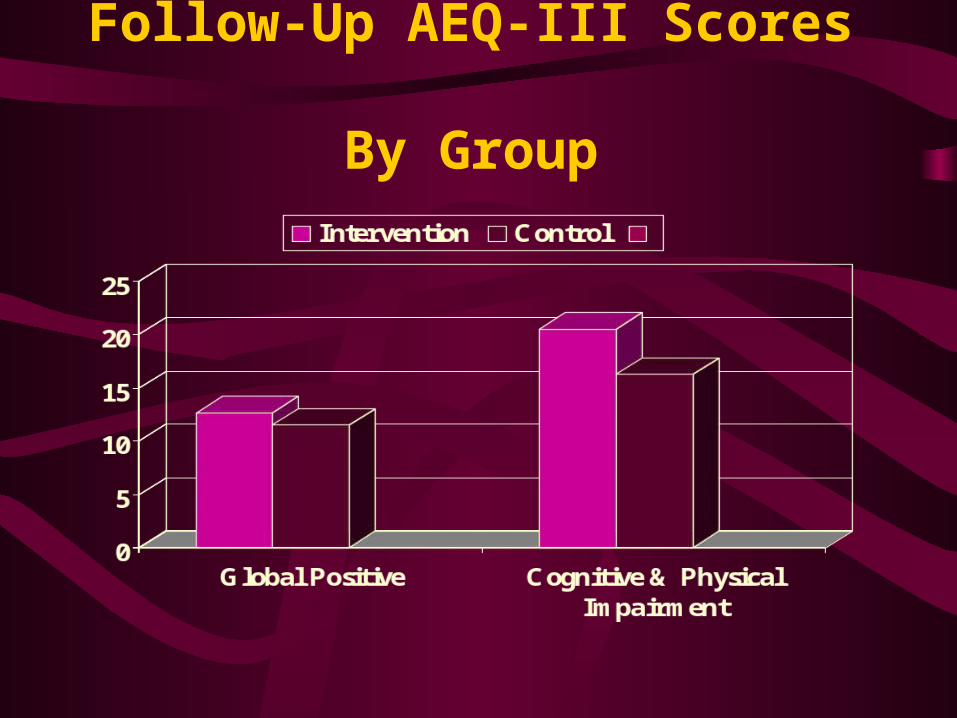
Follow-Up AEQ-III Scores By Group
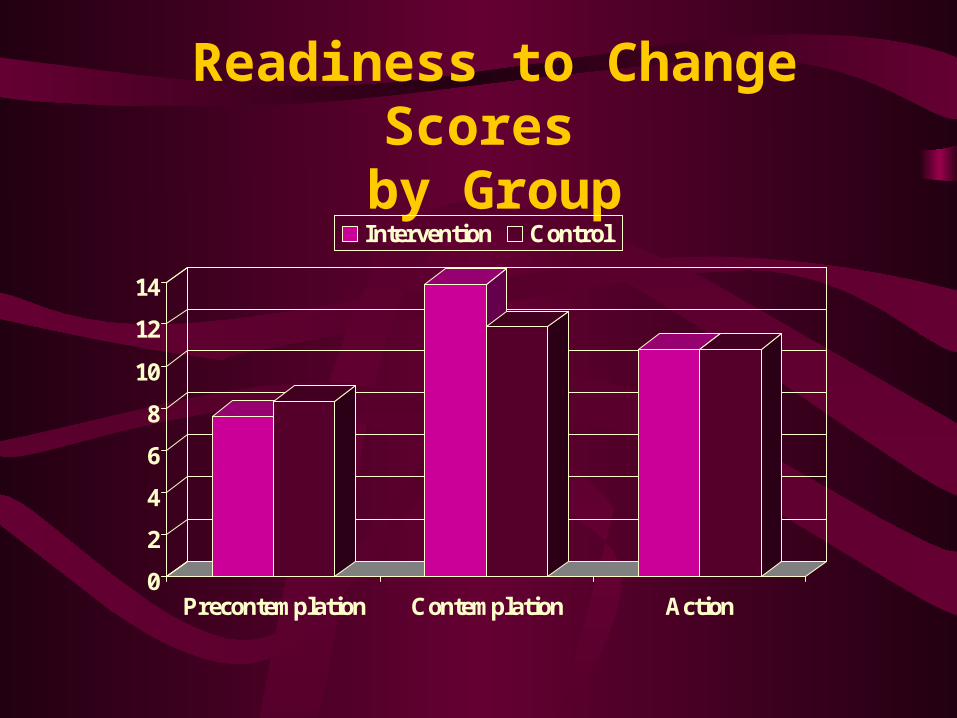
Readiness to Change Scores by Group
0
2
4
6
8
10
12
14
Precontemplation Contemplation Action
Intervention Control

Follow-Up Alcohol Use By Group
Acknowledgements
• Allison Clark, M.A. and Dan Graves, Ph.D. for data analyses
• Allison Clark, M.A., Marie Silva, M.S.W. for project coordination
• Jason Ferguson- consumer advisor