Bridging Public Health and Clinical Practice: A Pilot of ...
54
University of Kentucky University of Kentucky UKnowledge UKnowledge Theses and Dissertations--Public Health (M.P.H. & Dr.P.H.) College of Public Health 2017 Bridging Public Health and Clinical Practice: A Pilot of the CDC’s Bridging Public Health and Clinical Practice: A Pilot of the CDC’s Stopping Elderly Accidents, Deaths, and Injuries (STEADI) Fall Risk Stopping Elderly Accidents, Deaths, and Injuries (STEADI) Fall Risk Screening and Prevention Program in an Academic Medical Screening and Prevention Program in an Academic Medical Center Family and Community Medicine Clinic Center Family and Community Medicine Clinic Carolyn C. Shammas University of Kentucky, [email protected] Follow this and additional works at: https://uknowledge.uky.edu/cph_etds Part of the Public Health Commons Right click to open a feedback form in a new tab to let us know how this document benefits you. Right click to open a feedback form in a new tab to let us know how this document benefits you. Recommended Citation Recommended Citation Shammas, Carolyn C., "Bridging Public Health and Clinical Practice: A Pilot of the CDC’s Stopping Elderly Accidents, Deaths, and Injuries (STEADI) Fall Risk Screening and Prevention Program in an Academic Medical Center Family and Community Medicine Clinic" (2017). Theses and Dissertations--Public Health (M.P.H. & Dr.P.H.). 162. https://uknowledge.uky.edu/cph_etds/162 This Graduate Capstone Project is brought to you for free and open access by the College of Public Health at UKnowledge. It has been accepted for inclusion in Theses and Dissertations--Public Health (M.P.H. & Dr.P.H.) by an authorized administrator of UKnowledge. For more information, please contact [email protected].
Transcript of Bridging Public Health and Clinical Practice: A Pilot of ...

University of Kentucky University of Kentucky
UKnowledge UKnowledge
Theses and Dissertations--Public Health (M.P.H. & Dr.P.H.) College of Public Health
2017
Bridging Public Health and Clinical Practice: A Pilot of the CDC’s Bridging Public Health and Clinical Practice: A Pilot of the CDC’s
Stopping Elderly Accidents, Deaths, and Injuries (STEADI) Fall Risk Stopping Elderly Accidents, Deaths, and Injuries (STEADI) Fall Risk
Screening and Prevention Program in an Academic Medical Screening and Prevention Program in an Academic Medical
Center Family and Community Medicine Clinic Center Family and Community Medicine Clinic
Carolyn C. Shammas University of Kentucky, [email protected]
Follow this and additional works at: https://uknowledge.uky.edu/cph_etds
Part of the Public Health Commons
Right click to open a feedback form in a new tab to let us know how this document benefits you. Right click to open a feedback form in a new tab to let us know how this document benefits you.
Recommended Citation Recommended Citation Shammas, Carolyn C., "Bridging Public Health and Clinical Practice: A Pilot of the CDC’s Stopping Elderly Accidents, Deaths, and Injuries (STEADI) Fall Risk Screening and Prevention Program in an Academic Medical Center Family and Community Medicine Clinic" (2017). Theses and Dissertations--Public Health (M.P.H. & Dr.P.H.). 162. https://uknowledge.uky.edu/cph_etds/162
This Graduate Capstone Project is brought to you for free and open access by the College of Public Health at UKnowledge. It has been accepted for inclusion in Theses and Dissertations--Public Health (M.P.H. & Dr.P.H.) by an authorized administrator of UKnowledge. For more information, please contact [email protected].

STUDENT AGREEMENT: STUDENT AGREEMENT:
I represent that my capstone and abstract are my original work. Proper attribution has been
given to all outside sources. I understand that I am solely responsible for obtaining any needed
copyright permissions. I have obtained needed written permission statement(s) from the
owner(s) of each third-party copyrighted matter to be included in my work, allowing electronic
distribution (if such use is not permitted by the fair use doctrine) which will be submitted to
UKnowledge as Additional File.
I hereby grant to The University of Kentucky and its agents the irrevocable, non-exclusive, and
royalty-free license to archive and make accessible my work in whole or in part in all forms of
media, now or hereafter known. I agree that the document mentioned above may be made
available immediately for worldwide access unless an embargo applies.
I retain all other ownership rights to the copyright of my work. I also retain the right to use in
future works (such as articles or books) all or part of my work. I understand that I am free to
register the copyright to my work.
REVIEW, APPROVAL AND ACCEPTANCE REVIEW, APPROVAL AND ACCEPTANCE
The document mentioned above has been reviewed and accepted by the student’s advisor, on
behalf of the advisory committee, and by the Director of Graduate Studies (DGS), on behalf of
the program; we verify that this is the final, approved version of the student’s capstone including
all changes required by the advisory committee. The undersigned agree to abide by the
statements above.
Carolyn C. Shammas, Student
Sarah B. Wackerbarth, PhD, Committee Chair
Corrine Williams, ScD, MS, Director of Graduate Studies

BridgingPublicHealthandClinicalPractice:APilotoftheCDC’sStopping
ElderlyAccidents,Deaths,andInjuries(STEADI)FallRiskScreeningand
PreventionPrograminanAcademicMedicalCenterFamilyand
CommunityMedicineClinic
CAPSTONEPROJECTPAPER
Apapersubmittedinpartialfulfillmentofthe
Requirementsforthedegreeof
MasterofPublicHealthinthe
UniversityofKentuckyCollegeofPublicHealth
By
CarolynC.Shammas,M.D.,J.D.
Lexington,KentuckyApril19,2017
CapstoneCommittee:
SarahB.Wackerbarth,Ph.D.(Chair)
JonathanR.Ballard,M.D.,M.P.H.,M.Phil.(CommitteeMember)
RichardC.Ingram,Ph.D.(CommitteeMember)

2
Acknowledgments
IwouldliketothankthemembersoftheCapstoneCommittee,Dr.Wackerbarth,Dr.
BallardandDr.Ingram,fortheirinvaluableguidanceandencouragementthroughout
thisprocess.Theyhavecontributedtremendouslytomyeducationalandprofessional
growth.IamalsoindebtedtoDr.Ballardforhisinvaluablementorshipandwithout
whomthefallpreventionqualityimprovementprojectwhichformedthebasisforthe
capstonewouldnothavebeenpossible.Mythanksalsotothemembersofthefall
preventionworkgroupandtothestaffoftheUniversityofKentuckyFamilyand
CommunityMedicineClinicwhowerekeytothedevelopmentandrolloutofthepilot.I
wouldalsoliketoexpressmysincereappreciationtotheUniversityofKentucky
PreventiveMedicineProgramDirector,Dr.TishaJohnson,whosesupportandleadership
havecontributedsomuchtomyoutstandingresidencyexperience.
IamalsogratefultoallofthehighlysupportiveandknowledgeablestaffoftheKentucky
DepartmentforPublicHealth,particularlyDr.ConnieWhite,Mr.DustinFalls,Ms.Rebel
Baker-Chreste,Mr.GaryKupchinskyandMs.JoyMills;andtheKentuckyInjury
PreventionandResearchCenter,particularlyMr.CharlesSparrowandMs.Jeanne
Harris,forinspiringandfacilitatingmypassionforfallprevention.
Finally,mydeepestgratitudetoS.Ramanath;mysonanddaughter;andparticularlymy
parents,whohaveneverwaiveredintheirsupportandwithoutwhomthisjourney
couldnothavebeenundertakenorcompleted.

3
Abstract
Background:Fall-relatedmorbidityandmortalityintheolderadultpopulationis
apressingpublichealthproblembothnationallyandinKentucky,whichhasafallrate
abovethenationalaverage.ImplementationoftheCDC’sStoppingElderlyAccidents,
Deaths,andInjuries(STEADI)fallpreventionprogram,offersanopportunityto
effectivelyreducefalls,fall-relatedinjuriesandassociatedcosts.Theimplementation
processalsoservestofostercooperativeinterdisciplinaryandinterdepartmental
relationshipswithinhealthcaresystems,andbridgepublichealthandclinicalpractice.
Purpose:ThecapstonedescribesandevaluatesapilotofSTEADIatthe
UniversityofKentucky’sFamilyandCommunityMedicine(UKFCM)Clinic.Itfocuseson
pilotdevelopmentbyaninterdisciplinary/interdepartmentalworkgroupandpartnership
withotherkeystakeholders,suchastheKentuckyDepartmentforPublicHealth(KDPH).
Itpresentslessonslearned,recommendationsforimprovementandnextstepsin
STEADIimplementation.ItalsoreviewstheliteratureonSTEADIpilotprogramsand
facilitatorsandbarrierstoimplementation.
Methods:Thefive-daypilotwasconductedattheUKFamilyandCommunity
MedicineClinic.Patientsage65yearsandolderwerescreenedandevaluatedforfall
riskusingapaperformbasedontheSTEADIalgorithm.Thepilotwasevaluatedusing
theeight-stepKottermodelfororganizationalchange.
Results:Sixty-fourpatients(fiftypercent)ofpatientsage65andolderwere
screened,ofwhomforty-fourpercentscreenedpositiveforincreasedfallrisk.
MeaningfulstatisticsregardingothercomponentsofSTEADIweregenerallynot

4
obtainableduetoambiguitiesinthedesignoftheform.Thepilotevaluation
demonstratedseveralstepsintheKotterframeworkthatwereparticularlysuccessful:
creatingasenseofurgency;buildingaguidingcoalition;andgeneratingshort-term
gains.Lessonslearnedandrecommendationsincludedclarificationoftheassessment
andinterventionsectionsofthetemplatebeforeincorporationintotheambulatory
electronichealthrecord(AEHR);additionaltrainingofprovidersandstaff;andgreater
attentiontoworkflow.
Implications:STEADIpresentsanopportunitytobridgepublichealthandclinical
practiceandifbroadlyimplemented,promisestoreducetheCommonwealth’shighrate
ofolderadultfall-relatedmorbidityandmortality,aswellasassociatedcosts.

5
TableofContents
ListofAbbreviations
I. Introduction.…………………………………………………………………………………………………….…7
EpidemiologyandImpactofFalls.………………………………………………………………….....7
StoppingElderlyAccidents,Deaths,andInjuries(STEADI)………………………………11
ReimbursementandOtherIncentives……………………………………………………………..14
II. LiteratureReview.…………………………………………………………………………………………….17
NewYork……………………………………………………………………………………………….………..18
Oregon……………………………………………………………………………………………………………..20
Ohio………………………………………………………………………………………………………………….21
ImplementationfromaDepartmentofPublicHealthPerspective………………….22
OtherPilots………………………………………………………………………………………………………23
Conclusion………………………………………………………………………………………………………24
III. CapstoneProject…………………………………………………………………………………………….25
Methods…………………………………………………………………………………………………………..25
Background………………………………………………………………………………………………………26
PilotDevelopmentandRollout………………………………………………………………………..27
Results………………………………………………………………………………………………….............32
Evaluation………………………………………………………………………………………………………..33
LessonsLearned……………………………………………………………………………………………….40
Recommendations/NextSteps………………………………………………………………………..43
IV. Conclusion………………………………………………………………………………………………………45
References……………………………………………………………………………………………………….48
Appendix………………………………………………………………………………………………………….52

6
ListofAbbreviations
ACA AffordableCareActAEHR AmbulatoryElectronicHealthRecordAWV AnnualWellnessVisitCDC CentersforDiseaseControlandPreventionCEE ClinicalEngagementandTrainingCMS CentersforMedicare&MedicaidServicesCPT CurrentProceduralTerminologyCST ClinicalServiceTechnicianEHR ElectronicHealthRecordKDPH KentuckyDepartmentforPublicHealthKIPRC KentuckyInjuryandPreventionResearchCenterKSAC KentuckySafeAgingCoalitionKSPAN KentuckySafetyandPreventionAlignmentNetworkKVIPP KentuckyViolenceandInjuryPreventionProgramLPN LicensedPracticalNurseMACRA MedicareAccessandCHIPReauthorizationActMIPS Merit-basedIncentivePaymentSystemMOC MaintenanceofCertificationODH OhioDepartmentofHealthOHSU OregonHealth&ScienceUniversityPACT PatientAlignedCareTeamSFPP StateFallsPreventionProjectSTEADI StoppingElderlyAccidents,Death,andInjuriesTJC TheJointCommissionTUG TimedUpandGoUHS UnitedHealthServicesUKFCM UniversityofKentuckyFamilyandCommunityMedicineUKHC UniversityofKentuckyHealthCareUSPSTF UnitedStatesPreventiveServicesTaskForceVA VeteransAdministrationVIPP ViolenceInjuryandPreventionCenter(VIPP)

7
Introduction:
EpidemiologyandImpactofFalls
Fallsaretheleadingcauseofunintentionalinjuryandinjury-relateddeathin
adultsage65andolder(Bergen,Stevens,&Burns,2016).TheCDCestimatesthatin
2014,28.7percentofolderadultslivinginthecommunityreportedfallingwithinthe
pastyear,resultingin7millioninjuriesand27,000deaths(Bergenetal.,2016).In
Kentucky,thestatisticsareevenmorecompelling,with32.1percentofolderadults
havingreportedafallwithinthepastyear(Bergenetal.,2016).Thereareanumberof
riskfactorsforfalls,includingage;historyoffalls;lowerbodyweakness;gaitorbalance
impairment;psychoactiveandothermedications;chronicdiseasessuchasdiabetesand
arthritis;andhomehazards(Stevens,2005).Fearoffalling,resultingindecreased
physicalactivity,isalsoariskfactor(Phelan,Mahoney,Voit&Stevens,2015).According
toonestudy,theriskoffallingwas19percentwithoneriskfactor,butalmost
quadrupledwhenfourormoreriskfactorswerepresent(Tinetti,Speechley,&Ginter,
1988).Womenaremorelikelytofallandtosufferafall-relatedinjury,butmenare
morelikelytodieasaresultofafall(Peel,20).AccordingtotheWorldHealth
Organization,socioeconomicriskfactorsforfallsincludelowincomeandeducational
levels,inadequatehousing,lackofsocialinteractions,limitedaccesstohealthandsocial
servicesandlackofcommunityresources(WHO,2007).
ItisunclearwhyKentucky’sfallrateexceedsthatofotherstates,socioeconomic
factorsandhighratesofchronicdiseasessuchasarthritisanddiabetes,mayplayarole.
Asisthecasenationwide(Baldwin,Breiding,&Sleet,2016),fallsrepresenttheleading

8
causeoftraumaticbraininjuryintheolderadultpopulationinKentucky(KSPAN,2009-
2014).Thestate’s11.9percentfall-relatedinjuryrateexceedsthe10.7percentnational
average(Bergenetal.,2016).Ithasthedubiousdistinctionofbeingoneofthetopten
statesforbothpercentageofolderadultsreportingfallsandfall-relatedinjurieswithin
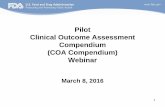
thepastyear(Bergenetal.,2016)asshowninFigure1below.
Figure1:Percentagesoffallsandfallinjuriesinthepreceding12monthsreportedbyadultsaged³65years(N=147,319)–BehavioralRiskFactorSurveillanceSystem,UnitedStates,2014
Therateofemergencydepartmentvisitsandinpatientdischargesforfall-related
injuriesvariesbycounty(Figure2andFigure3).TheUniversityofKentuckyHealthCare
(UKHC)system,locatedinFayetteCounty,servesanumberofcountiesthathavehigh
ratesofemergencydepartmentvisitsandinpatientdischargesforinjuresduetofalls.
UKFMCsees50,000patientsperyear,primarilyfromFayetteandsurroundingcounties;
Source: Bergen et al, 2016

9
approximately8percentofpatientsarecoveredbyMedicare(J.Ballard,personal
communication,April12,2017andApril18,2017).AccordingtoU.S.CensusBureau
estimates(2015),12.0percentofFayetteCounty’sand15.2percentofKentucky’s
populationareage65orolder,comparedtotheU.S.averageof14.9percent.
Figure2:EDVisitstoKentuckyhospitalsforunintentionalfalls(2008-2012)
Retrieved April 19, 207from Kentucky Injury Prevention and Research Center (a bona fide agent of the KY Department for Public Health), KY-IBIS site: https://kyibis.mc.uky.edu/kiprc; http://www.safekentucky.org/images/Data/falls-by-county-maps/ED_falls.jpg

10
Figure3:Inpatienthospitaldischargerateforunintentionalfalls(2010-2014)
Fallsnotonlytakeatollintermsofhumansuffering,butareassociatedwith
staggeringdirectandindirectmedicalcosts.Fall-relatedMedicareexpendituresare
estimatedatmorethan$31billion,andareexpectedtogrowto$100billionby2030
(Burnsetal.,2016).InKentucky,totalhospitalchargesamountedtocloseto$366.5
millionin2014(KentuckyInjuryandPreventionandResearchCenter,2017).Total
inpatienthospitalchargesmorethantripledfrom2005to2014(KentuckyInjuryand
PreventionResearchCenter,2017).Althoughnotallrelatedtofalls,thefinancialburden
ofhospitalizationinKentuckyislargeandgrowing.
Retrieved April 19, 2017 from Kentucky Injury Prevention and Research Center (a bona fide agent of the KY Department for Public Health), KY-IBIS site: https://kyibis.mc.uky.edu/kiprc; http://www.safekentucky.org/images/Data/falls-by-county-maps/ED_falls.jpg

11
Fallsalsoresultinincreasednursinghomeplacement,lossofindependenceand
decreasedqualityoflife(Stevens&Burns,2015).Thereisagrowingimperativeto
addresstheproblemoffall-relatedinjury,deathandcostnationallyandinKentucky,
particularlygivenaprojectedincreaseof55percentintheU.S.populationage65and
olderby2030,accompaniedbyariseinthenumberoffallstoalmost49million,with12
millioninjuries(Bergenetal.,2016).
StoppingElderlyAccidents,Deaths,andInjuries(STEADI)
TheCentersforDiseaseControlandPrevention(CDC)hassoughttoreducefalls
throughtheevidence-basedStoppingElderlyAccidents,Deaths,andInjuries(STEADI)
initiative.TheSTEADItoolkitwasdesignedtoimprovefallsriskscreeningandprevention
ratesinprimarycaresettings(Caseyetal.,2016).TheSTEADIalgorithmandeducational
materialsincludedinthetoolkit,facilitatefallpreventionawarenessandcommunication
betweenprovidersandpatients.
Surprisingly,lessthanhalfofolderadultswilldisclosehavinghadafalltoa
healthcareprovider(CDC,2015).Reluctancetotalktoaprovideraboutfallsisduetoa
numberoffactors,includingembarrassment,fearoflossofautonomy,beingoverly
optimisticaboutcapabilities,andthemistakenassumptionthatfallsareanormalpart
ofaging(Childetal.2012;Moylan&Binder,2007;Stevens&Burns,2015;Yardley,
Donovan-Hall,Francis,&Todd,2006).Moreover,physiciansoftenfailtoinquireabout
fallsforanumberofreasons,includingunclearrolesamongmembersoftheprimary
careteam;unclearorchangingclinicalrecommendations;andlackoffamiliaritywithfall

12
interventionsandresources(Caseyetal.,2016;Jones,Ghosh,Horn,Smith,&Vogt,
2011;Landis&Galvin,2014;Stevens&Phelan,2013).
Whilethereissubstantialevidencetosupporttheeffectivenessoffallsscreening
andmultidimensionalinterventionstoreducerisk(Gillespieetal.,2012),itisestimated
thatphysiciansonlyaskwhetherapatienthasfallenaboutone-thirdofthetime(Jones
etal.,2011).Anumberofbarrierstoproviderscreeninghavebeencited:lackofrole
clarityamongprimarycareteammembers;unclearorchangingfallsriskreduction
recommendations;complicatedandfragmentedfinancialandqualityincentives;lackof
awarenessandknowledgeaboutfallpreventioninterventionsandresources(Caseyet
al.,2016;Childetal.,2012;Chouetal.,2006;Jonesetal.,2011;Landis&Galvin,2014;
Stevens&Phelan,2013).
STEADIwasdevelopedtoaddresstheseissuesandassistprimarycareproviders
inscreeningolderadultpatientsforfallriskandlinkingthemtoappropriate
interventions.TheSTEADIalgorithm(Figure4)isbasedonthe2010AmericanGeriatric
SocietyandBritishGeriatricSocietyClinicalPracticeGuidelines,aswellinputfrom
providers(Stevens&Phelan,2013).Itincludesscreening(askingthreekeyquestions
relatedtofallrisk,suchasnumberoffallsinthepastyear);evaluationofgait/balance;
assessmentofriskfactors(e.g.medicationsandcognitiveimpairment);and
interventions(e.g.acommunity-basedexerciseorfallpreventionprogram)(CDC,2016).
Theeffectivenessoffallinterventions,includingseveralcommunity-basedgroup
exerciseprograms,wasdemonstratedina2012CochraneReviewofalmost160
randomizedcontrolledtrials,withatotalofmorethan179,000participants(Gillespieet

13
al.,2012;Kaniewski,2015).Evaluationbyaclinician,andtreatmentofriskfactorsresult
ina24reductioninfallrate(Gillespieetal.,2012).Community-basedprogramsmay
alsoachievesubstantialcostsavings;theSteppingOnprogram,forinstance,hasbeen
showntohaveareturnoninvestmentof64percent(Houryetal.,2016).
Optimally,thealgorithminitsentiretywouldbeimplementedinallprimarycare
practices,asmultidimensionalinterventions,particularlythosethatincludegait,balance
andstrengthtraining,havethegreatestimpactonreducingfalls(Stevens&Burns,
2015).Recognizingthatthealgorithmmaynotbeperformedinitsentiretyduetotime
andotherconstraints(seebarrierstoimplementationbelow),providersareaskedto
Figure4:AlgorithmforFallRiskAssessment&Interventions
CDC, 2016

14
focusonthreekeyactions:1)screening;2)reviewingmedicationstoreduce/eliminate
thosethatincreasefallrisk;and3)prescribingVitaminDtoimprovemusculoskeletal
health(Bergenetal.,2016).Inadditiontotheclinicaldecisionsupportalgorithm,the
CDChasdevelopedaSTEADItoolkitwithresourcesforproviders,suchastrainingvideos
andpatienteducationalmaterials(CDC,2016).
TheCDC(2015)projectsthatforevery5,000providerswhoimplementSTEADI
overa5-yearperiod,morethan6millionolderadultscouldbescreened;1millionfalls
prevented;and$3.5billionindirectmedicalcostssaved.
ReimbursementandOtherIncentives
FallriskscreeningandevaluationispartoftheWelcometoMedicareVisitand
AnnualMedicareVisit,andthereforeareanavenueofreimbursementforfall-related
providerservices.Fallriskscreening,however,isonlyoneofanumberofevaluationsto
beperformedduringthevisit,anddoesnotincluderobustassessmentorintervention.
Inaddition,itshouldbenotedthatMedicareWellnessAnnualvisitsareunderutilized,
withautilizationrateof12.8percentinKentucky,andonly17.7percentnationally
(CMS,2015).
HealthcareprovidersandsystemsaregivenincentivestoimplementSTEADIfall
preventionthroughtheMedicareAccessandCHIPReauthorizationAct(MACRA’s)
Merit-basedIncentivePaymentSystem(MIPS).LandisandGalvin(2015),studiedfall-
relatedmeasuresinCMS’PhysicianQualityReportingSystem(PQRS),thepredecessor
toMIPS,withagoalofreducingfall-relatedinjuriesandcostsby10percent.Four

15
primarycarepractices,locatedinwesternNorthCarolina(aregionofthestatewitha
highfallrate),withovertwothousandolderadultpatients,participatedinthequality
improvementproject.Almost70percentofeligiblepatientswerescreened.Ofthose
withreportedfalls,closeto90percentwereassessed.Alittleunderaquarterofthose
patientshadadocumentedplanofcare.Disappointingly,thestudyfailedto
demonstrateasignificantreductioninfall-relatedhospitalizationsorcosts,whichthe
authorssuggestmayhavebeendueto“inadequateimplementationofthe
managementcomponentoftheprogram.”(LandisandGalvin,2015,p.2413)
AninitiativebytheCDC,throughacooperativeagreementwiththeAmerican
CollegeofPreventiveMedicine(ACPM),isaimedatgainingCMSapproval,alengthyand
arduousprocess,fornewfall-relatedCPTcodeswhichareneededinordertobillfor
theseservices(ACPM,n.d.).Professionalmaintenanceofcertification(MOC)credits,as
wellasqualityimprovementrecognitionofferedbyhealthcaresystemsandinsurers
havealsobeenusedtoincentivizeSTEADIimplementation(Caseyetal.,2016;Gearon,
2015).
AchangeinUnitedStatesPreventiveServicesTaskForce(USPSTF)
recommendations,whichguideprimaryphysicianpractice,wouldlikelypromotefall
screeningandpreventionuptake(Tinetti&Brach,2012).Multidimensionalfallrisk
assessmentisnotcurrentlyrecommendedforallcommunity-dwellingolderadults,but
onlyforselectedindividualsbasedontheircircumstances(USPSTFCrecommendation)
(Moyer,2012).ThisUSPSTFrecommendationis,however,underreview(USPSTF,2017),
andifchangedfromaGradeCtoaGradeAorBrecommendation,wouldinfluence

16
reimbursement,particularlygiventhattheAffordableCareAct(ACA)mandates
Medicarecoverageforpreventiveservices(Tinetti&Brach,2012).

17
LiteratureReview:
AliteraturereviewofSTEADIimplementationwasconductedinPubMed,Webof
ScienceandAgeLineusingthefollowingterms:PubMed:”STEADI”AND"Accidental
Falls/preventionandcontrol"[majr]AND"Aged"[mesh]Filters:Review,5years,English;
WebofScienceusingonlykeywords;AgeLineusingthefollowingsearchterms:(DE
"Falls")OR(DE"AccidentPrevention").Theliteraturewassupplementedbyonline
resourcesandinformationprovidedbytheOhioDepartmentofHealth.
ShortlyfollowingthedevelopmentoftheSTEADIdecisionsupporttoolin2011,
theCDC’sStateFallsPreventionProject(SFPP)providedfundingtohealthdepartments
inColorado,NewYorkandOregon,todevelopfallpreventionstrategiesinclinical
practices,healthcaresystemsandcommunityorganizations(Casey,Parker,Winkler,
Liu,Lambert,&Eckstrom,2016;Shubert,Smith,Schneider,Wilson&Ory,2016;Stevens
&Phelan,2013).Thesethreestateshavejustrecentlycompletedthefive-year
implementationperiod(Shubertetal.,2016).Todate,neitherColoradonorNewYork
havepublishedadescriptionorevaluationofSTEADIimplementationintheirrespective
states.ResultsoftheNewYorkprogramhavebeenreportedinthepopularpressand
variouswebsites.Additionally,asmallstudyoffallprevention-relatedproviderattitudes
andpracticeswaspublishedin2015(Smith,Stevens,EhrenreichWilson,Schuster,
Cherry&Ory,2015).
TheOhioDepartmentofHealth,withtheassistanceofaconsultingfirm,hasalso
recentlycompleteda6-monthevaluationofapilotprojectinoneoftheirlargehealth
caresystems(RAMA,2015;RAMA,2016).Allofthesestate-initiatedprogramsidentify

18
importantcomponentsofsuccessfulimplementationandidentifybarriers.The
foundationfortheUKFCMpilotanalysis,however,istheKotter-basedevaluationofthe
STEADIinitiativeinOregon.Importantly,thereisapaucityofpublicationsdescribing
STEADIqualityimprovementprojects,initiatedbyprimarycarepracticesoutsideofthe
CDC-fundedpilots.TheUKFMCpilotmayrepresentoneofthefirstclinicalpracticesto
collaboratewithpublichealthentitiestoimplementSTEADIintheabsenceofa
categoricalCDCgrant.Additionally,theincorporationofafallpreventiontoolintothe
AllscriptsEHR,thesystemusedinthispilot,hasnotheretoforebeendescribed.
NewYork
NewYork’sSTEADIprogramwasapartnershipbetweenaregionalhealth
system,UnitedHealthServices(UHS),BroomeCountyHealthDepartment,Broome
CountyOfficeforAgingandtheNewYorkStateDepartmentofHealth(Smith,2015;
UHS,2013;Gearon,2015).BroomeCountywasselectedfortheprogrambecause
approximately17percentofitsresidentsare65yearsorolder(UHS,2013),andfall
preventionwasatoppriorityinthecounty(Gearon,2015).Theinitialpilot,championed
byaninternalmedicinephysicianandanursemanager(UHS,2013),wasconducted
usingapaperform,followedbythedevelopmentofanEHRtemplate.Aswasthecase
inOregon,thealgorithmandworkflowweresimplifiedandadaptedtomeettheneeds
ofthepractice.
Thesuccessoftheinitialpilotledtoexpansiontomorethanfifteenclinicsites,
whichreportedascreeningrateofover85percent(“Dr.Floyd;”2014).Accordingtoa

19
2015U.S.News&WorldReport(2015)article,thehealthsystemreportedhaving
screened17,500patientsandthecounty’sfallratehasdeclinedby25percentbetween
2010and2013.Importantly,inthe18monthsafterimplementation,therewasa12
percentreductionincountyhospitalizationsandemergencydepartmentforfractures
relatedtofalls(Gearon,2015).
AstudybySmithetal.(2015),conductedaspartoftheCDCgrant,examined
primarycareproviderbeliefs,knowledgeandfall-relatedactivitiespriortoreceivinga
one-hour,physicianchampion-led,ClinicalEngagementandEducation(CEE)training
session.TheCEE’saimwastoassistcliniciansinidentifyingwaystointegrateSTEADI
intopractice.Thesessionbroughttogetherthirty-eightprovidersandstaff,representing
elevenpractices,todiscusstheproblemoffallsandtocollectivelydevelopwaysto
incorporatefallpreventionintoclinicalpractice(Smithetal.,2015).Resultsindicated
thatfallswererankedasalowerprioritythandiabetesandseveralotherchronic
diseases;andwerenotroutinelyscreenedfororintervenedupon(Smithetal.,2015).
Unfortunately,thisstudywasunable,duetoinadequatepost-trainingdata,toassess
theimpactofSTEADItrainingonproviderattitudes(Smithetal.,2015).Itdid,however,
givemeaningfulfeedbacktotheCDCregardingphysiciantimeconstraints,andledto
theCDC’sfocusonthreekeyscreeningquestions(hasthepatientfalleninthepastyear,
dotheyhaveafearoffalling,and/orunsteadinessinstandingorwalking)andtwokey
interventions(vitaminDsupplementationandmedicationreview)(Gearon,2015).

20
Oregon
STEADIwasimplementedinOregonthroughapartnershipbetweentheOregon
HealthAuthority(OHA)andtheOregonHealth&ScienceUniversity(OHSU)(Caseyet
al.,2016).Thefirststepinsystem-wideimplementation,wasthedevelopmentofapilot
involvinggeriatrics-trainedprovidersintheInternalMedicine&GeriatricsClinic.These
clinicchampionsrefinedclinicworkflowandtheelectronichealthrecordtool.Thepilot,
conductedoverseveralmonths,screenedfifty-sixpatientsage75patientsorolder.Fall
riskwasdeterminedusingthequestionscontainedintheSTEADItoolkit’sStay
Independentbrochure(AppendixA)whichincludethethreekeyquestionsinthe
algorithmaswellasquestionstargetedtoadditionalriskfactors.Ofthe80percentof
patientswhohadrecordedriskscores,56percentweredeterminedtobeathighrisk.
Ofthoseathighrisk,92percentwerefullyevaluatedattheinitialvisit.Impressively,
over90percenthadadocumentedvisionassessment,vitaminDlevelandfall-related
careplan.TheSTEADIworkflowandEHRwererevisedanumberoftimesbeforebeing
fullyimplementation.Duringthefirst18monthsofimplementation,45percentof
eligiblepatientswerescreened,35percentofwhomwereidentifiedasbeinghighrisk
(Caseyetal.,2016).
TheOHSUteamsurveyedhealthcareteammemberstoidentifyfacilitatorsand
barriersandusedsurveyresultstochangehowtheprogramwasimplemented.
Facilitatorsincluded:aclinicculturethatwassupportiveofnewprotocolssuchas
STEADI;theopportunityforproviderstoreceiveMaintenanceofCertification(MOC)
credits;theavailabilityofclinicchampionstoassistinimplementation;well-prepared

21
clinicstaff;anEHRSTEADItoolthatwaseasytouse;patientreceptivitytoscreening;
strongevidencetosupportfallsscreening;anduseofSTEADItostreamlinethe
screeningprocessandpreventfalls.Timeconstraints,competingmedicalinterestsand
thecomplexityofscreeningwereidentifiedasbarriers(Caseyetal.,2016).Notably,
poorreimbursementwasnotidentifiedasabarriertoimplementation(Caseyetal.,
2016).
InanalyzingthesuccessoftheOHSUprogram,theauthorsidentifiedfour
importantprocesses:developmentofworkflowthatdidnotdisturbthedailypractice
routine;incorporationofSTEADIintotheEHR;pilotingofworkflowandtheEHR
templatebyclinicchampionspriortoimplementation;andtrainingofpersonnelonuse
oftheEHRtool,workflowandfallprevention.Theyalsonotedtheimportanceofearly
buy-infromalllevelsoftheorganization,partnershipwiththestatehealthdepartment
andlinkagetocommunityinterventions(Caseyetal.,2016).
Ohio
TheOhioDepartmentofHealth(ODH)ViolenceInjuryandPreventionCenter(VIPP),
whilenotoneoftheoriginalCDCgrantrecipients,beganencouragingproviderstouse
STEADIin2013(RAMA,2015).Inordertofacilitateuptakeoftheprogram,ithas
recentlyembarkedonaninitiativetoimplementSTEADI.Thestate,withtheassistance
ofRAMAConsulting,embarkedonacollaborativeprojectwiththeOhioHealthsystem,
toamongotherthings,developastatewideworkgroup;pilotSTEADIinfiveOhioHealth
settings;identifybestpractices;assessbarrierstoimplementation;developpromotional

22
materials;andevaluatethepilot.Thefivepilotsiteswerechosenbasedonhavingan
olderadultpatientbase,adequatestaffandfacilitiesandtheuseoftheEpicEHR.
ConsistentwithOregon’sfindings,theextensivereportnotedtheimportanceof
aphysicianchampion,organizationalbuy-in,integrationofSTEADIintotheEHR,
incremental,tailoredanditerativeimplementation,trainingandtechnicalsupport,
attentiontoworkflowandlinkagetocommunityinterventions.Moreover,anadequate
reimbursementmechanismandotherincentiveshelpedtoensuresustainability(RAMA,
2015;RAMA,2016).
The6-monthquantitativeandqualitativeevaluation,basedondatacollected
fromavarietyofsources,includingtheEHRandfocusgroups,showedthatalmost450
patientshadbeenscreened,althoughduetodatacollectiondifficultiestheinitialreport
wasnotabletodeterminethepercentageofeligiblepatientsscreened(RAMA,2016).
Notsurprisingly,themostfrequentlyreportedbarrierwaslackofstafftimeor
availability(RAMA,2016).
ImplementationfromaDepartmentofPublicHealthPerspective
Anumberoflessonshavebeenlearnedbystatehealthdepartmentgrantees
chargedwithimplementingSTEADI.AnarticlebyThoreson,Shields,Dowler&Baer
(2015),eachofwhomisfromoneofthegranteestates,summarizedthekeyelements
insuccessfulfallpreventionprogramimplementation,suchasbuildinganinfrastructure
andensuringsustainability.Shubertetal.(2016)identifiednineimportantchallenges
departmentsofpublichealthfaceinimplementingSTEADI:1)changingphysician

23
practice,whichnecessitatesfinding“meaningfulvaluepropositions”forpracticingand
buildingrelationships;2)limitedknowledgeonthepartofprovidersandsystems
regardingthevalueandavailabilityofcommunity-basedinterventions;3)alarge
numberofcompetingeffortstoimproveefficiency;4)lackofuniformityofmotivators
amonghealthcaresystems;5)lackofacomprehensiveandcentralizedsystemfor
community-basedinterventionsandresources;6)lackofbidirectionalreferralsystems;
7)theneedtocreatedemandforcommunityservicesthroughproviderreferralwhile
havinganadequatesupplyofcommunityprograms;8)findingappropriatepartners;and
9)sustainability.Whilemanyoftheseissuesmustbesolvedbyhealthcaresystems,
cliniciansandcommunityorganizationspublichealthentitiescanbringstakeholders
together,provideeducationandfacilitateproblem-solving.
OtherPilots
ApilotstudyattheTampaJamesA.HaleyVA,testedwhetherSTEADIcouldbe
adaptedforusebythePatientAlignedCareTeam(PACT)(Ferguson,Friedman&Bulat,
2016).ThePACTwascomprisedofaphysician,nurseandclerk(Ferguson,2016).Lack
ofrobustleadershipsupport,difficultyinintegrationintotheworkflowandduplication
ofaspectsoftheexistingVAfallpreventionprogram,wereamongthebarriers
identified.Morepositively,pilotparticipantsreportedincreasedfallprevention
awarenessanduseoftoolkiteducationalmaterials.

24
Conclusion
TheliteratureonSTEADIpilotstudiesidentifiesanumberofelementsneeded
forsuccessfulimplementation.Aphysicianchampion,buy-infromhealthsystem
leadership,incorporationofthedecisionsupporttoolintotheEHR,andcollaboration
withhealthdepartmentandcommunityorganizations,facilitateasuccessfulprogram.
Timeconstraints,competingclinicaldemandsandintegrationintotheclinicworkflow
continuetorepresentsignificantchallengesandnecessitateaniterativeprocess.The
UKFMCpilot,discussedbelow,wascharacterizedbyanumberofthefactorsneededfor
successfulimplementation,butwillrequirefurtherrevisionsinordertobefully
integratedintotheclinicandthroughoutUKHC.

25
CapstoneProject:Thepurposeofthisprojectwastodescribeandevaluate,usingtheKottermodel,apilot
oftheSTEADIpreventionprogram.Thepilotwasdevelopedbyan
interdisciplinary/interdepartmentalworkgroupandfacilitatedthroughpartnershipwith
otherkeystakeholders.
Methods
ThecapstoneprojectwasbasedonaUKFamilyandCommunityMedicinefall
preventionqualityimprovementprojectusingtheCDC’sSTEADItoolkit.Itwas
developedbyaninterdisciplinaryandinterdepartmentalworkgroup,incooperation
withtheKentuckyDepartmentforPublicHealth.Thepilotdevelopmentprocessand
pilotdesignaredescribedmorefullyinthebackgroundsection.Descriptivestatistics
wereusedintheanalysisofpilotresults.ThepilotwasevaluatedusingtheKotter
LeadingChangemodel(Kotter,1995)whichiscomprisedofeightsteps:1)creatinga
senseofurgency;2)buildingaguidingcoalition;3)formingastrategicvisionand
initiatives;4)enlistingavolunteerarmy;5)enablingactionbyremovingbarriers;6)
generatingshort-termwins;7)sustainingacceleration;and8)institutingchange.
ThisprojectwasreviewedbytheUniversityofKentuckyInstitutionalReview
Boardandaswasdeterminedtomeetfederalcriteriatoqualifyasanexemptstudy.

26
Background
UniversityofKentuckyHealthCare(UKHC),anacademicmedicalcenteranda
leaderinhealthcareinthestate,seeksto“offercarethatispatient-centered,multi-
disciplinaryandcollaborative”(StrategicPlan,2016,p.4)andiscommittedtoevidence-
basedcareandcontinuousqualityimprovement(StrategicPlan,2016,p.40).Atthe
timethattheUniversityofKentuckyFamilyandCommunityMedicine(UKFCM)quality
improvementprojectcommenced,UKHCalreadyhadaninpatientfallscreening,
assessmentandpreventionprograminplace.Ithadalsoimplementedascreening
programtoidentifypatientsatriskoffallingwhileattendingmedicalappointmentsin
UKHCclinics.UKFCMrecognizedtheopportunitytoexpandtheorganization’sexisting
fallpreventioneffortsthroughpilotingSTEADI,andlaterincorporatingthealgorithm
intoitsenterprise-wideambulatoryelectronicrecord.
Thefallpreventionqualityimprovementprojectpresentedauniqueopportunity
topartnerwiththeKentuckyDepartmentforPublicHealth(KDPH).KDPH,
understandingthesignificantpublichealthproblemthatfallsandfall-relateddeathsand
injuriespresent,hasbeeninvolvedinavarietyofeffortstoreducefallsinthestate,and
hassoughttocollaboratewithhealthcareprovidersandothercommunitystakeholders
toimplementSTEADI.Thehealthdepartment,aswellastheKentuckyInjuryPrevention
andResearchCenter(KIPRC),apartnershipbetweenKDPHandtheUniversityof
KentuckyCollegeofPublicHealth,haveengagedinanumberofactivitiesthatsupport
fallsprevention.KIPRC’sKentuckyViolenceandInjuryPreventionProgram(KVIPP),
tracksandreportsstateandcountyfall-relatedinjurydata(C.S.Sparrow,personal

27
communication,April4,2017).Foroverfiveyears,theKentuckySafeAgingCoalition
(KSAC),asubcommitteeoftheKentuckySafetyandPreventionAlignmentNetwork
(KSPAN),hashostedanannualFallsSummit(D.Falls,personalcommunication,April4,
2017).TheSummit,attendedbymembersofthehealthcareandpublichealth
community,hasincludedinformationonSTEADI(KSPAN,2009-2014).Datacollectionis
fundedthroughtheCDCCoreStateViolenceandInjuryPreventionProgramGrant.
SupportfortheSummithasbeenprovidedbytheosteoporosisprogram,aspartofthe
CDCPreventiveHealthandHealthServicesBlockGrant,andKentuckyViolenceand
InjuryPreventionProgram(KVIPP)(D.Falls,personalcommunication,April5,2017;C.S.
Sparrow,personalcommunication,April4,2017).Giventhedemonstratedcommitment
ofUKHC,UKFCMandthestatehealthdepartmenttofallprevention,thequality
improvementpilotpresentedaclearopportunitytointroduceSTEADIintoclinical
practice.
PilotDevelopmentandRollout
Thefallpreventionpilotworkgroupwasledbytwophysicianchampions–the
UKFCMclinicdirector,Dr.JonathanBallard,andthisauthor,aresidentphysician.The
clinicdirectorhadextensiveexperienceinqualityimprovementandhadstrongworking
relationshipswithprojectpartnerswithintheUKHCorganization.Thisauthorhadbeen
involvedinfallpreventionprojectsatKIPRCandKDPH.Itwasrecognizedthatinorderto
besuccessful,theprojectworkgroupshouldbeinterdisciplinaryandinterdepartmental.
Aworkgroupwasestablishedandincludedaninformaticist;practicemanager;assistant

28
chiefnurseexecutive;familypracticepatientservicescoordinator(senior);physical
therapistfromUKHC’sKentuckyClinicOutpatientTherapy;andanurseclinicalmanager
fromthetheKentuckyNeuroscienceInstitute.Valuableinputwasalsoprovidedbythe
UKHCTraumaInjuryandPreventionOutreachCoordinator,whowasinvolvedinleading
anenterprise-wideefforttoprovidefallpreventioneducationandlinkstocommunity
resources,suchastheCountyExtensionService’sevidence-basedAMatterofBalance
program,toallolderadultsadmittedtoUKHealthCare.Laterworkgroupmeetingswere
alsoattendedbyrepresentativesfromKIPRCandKDPH.
Workgroupmeetingswereheldovera3-monthperiodpriortothepilotrollout
andmetaftertheconclusionofthepilottodiscussresults.Onedaypriortotherollout,
thepilotwaspresentedatthemonthlyUKFCMpractice-widemeeting,whichwas
attendedbyhealthcareproviders,clinicalservicetechnicians(CSTs),LicensedPractical
Nurses(LPNs)andotheradministrativestaff.KDPHrepresentativeswerealsopresent,
asobservers,duringtheFamily&CommunityMedicinepractice-widemeeting
introducingthepilot,andbroughtwiththemSTEADIeducationalmaterials.
The5-daypilotwasoriginallydesignedtoincludeonlytwoclinicteams,soasnot
tooverburdenandpossiblydisruptclinicworkflow,butwaslaterextendedtoincludeall
fiveteams.Residentphysicianswerepresentatthemonthlypracticemeetingandthey
alsoparticipatedintherollout.Aspartoftheinitialqualityimprovementpilot,apaper
versionoftheSTEADIambulatoryscreeningandassessmenttool(Figure5),ratherthan
anelectronicversion,wasused.TheCDC’sSTEADIalgorithmwasprintedonthebackof
theformforprovidersforreference.Theinformaticistlaterdevelopedmock-upsof

29
proposedchangestotheexistingAmbulatoryElectronicHealthRecord(AEHR)(Figure6)
includingmodificationofthefallriskscreeningquestions(Figure7).Itwasalso
proposedthattheassessmentandinterventionssectionsbeaddedtotheAEHR,
followingfurtherrevisionstoresolveambiguities.ThepresentationtotheAEHRUser
Group,whichmustapproveallchangestotheAEHR,wasmadethreemonthsfollowing
pilotcompletion.

30
Figure5:AmbulatoryFallRiskScreeningToolforPatientsAge65andOlder

31
Figure6:FallRiskScreeninginAEHRatTimeofPilot
Figure7:ProposedAEHRFallRiskScreeningChanges

32
Results
Therewere129patientsage65orolderseenintheUKFCMclinicduringthefive-
daypilot.Ofthose,64,or49.61percent,werescreenedforfallrisk.Ofthosescreened,
28answeredyestooneorbothofthefirsttwoscreeningquestions.Basedonapositive
responsetoatleastoneofthesequestions,44percentweredeterminedtohave
screenedpositive.Thirteenofthe64screened(20.31percent)hadfalleninthepast
year,and21ofthe64(32.81percent)wereworriedaboutfallingorfeltunsteadywhile
walkingorstanding.Thequestion“wasprotocolimplemented”referredtothepre-
existingfallsprotocolinplacetopreventapatientfromfallingwhileintheclinic.While
thiswasexplainedbrieflyintheclinicpracticemeeting,itmayhaveneededfurther
clarification,asitwasoftenleftblank.
Completionoftheproviderriskassessmentwasrelativelylow,with25percent
ofprovidersnotrespondingeitheryesornotomedicationreview,and32percentwith
noresponseregardingvitaminDsupplementation.Thequestionregardingmedication
review(psychoactive/anticholinergic/sedating,includingOTCmedications)appearsto
havebeensubjecttodifferentinterpretations.A“Yes”responsemayhavemeant
medicationswerereviewedorthattheywerereviewedandcontainedoneofthehigh-
riskmedications.Anegativeresponsemayhaveindicatedthatmedicationreviewwas
notconductedorthatmedicationswerereviewedandthepatientwasnottakinghigh
riskmedications.TherewasasimilarlackofclarityregardingtheVitaminD
supplementationquestion.Possibleinterpretationsincluded:VitaminDwasprescribed

33
atthisvisit;thepatientwasalreadytakingVitaminD;thepatientdidnotneeda
supplementbasedontestresultsorotherfactors;ortheproviderhadnotaddressed
theissue.
Someoftheformshadthescreeningquestionscompleted,butlackedanyother
responses,makingitunclearwhethertheCST/LPNdidnotgivetheformtotheprovider,
ortheproviderfailedtocompletetheassessment.Duetotheaforementioned
ambiguitiesintheform,reliablestatisticscannotbereportedregardingprovider
assessmentsandinterventions.
Evaluation
TheKotter8-stepprocessfororganizationalchange(Kotter,1995)providesthe
frameworkforevaluationoftheUKFCMpilot.TheKottermodelwasselectedfollowing
completionoftheUKFCMpilot.While,inretrospect,itwouldhavebeenvaluablehadit
beenusedprospectivelytoguidethedevelopmentandexecutionofthepilot,itis
nonethelessusefulforevaluativepurposesandcanhelptoguidefurther
implementation.
Step1:Createasenseofurgency
Thefirststepintheprocessofeffectivechangeisto“createasenseofurgency
amongrelevantpeople”(Kotter,1995;Kotter&Cohen,2002,p.3).Asenseofurgency
forthepilotwaseffectivelyconveyedthroughconnectingwithaudiencesinavisually
andemotionallycompellingmanner(KotterandCohen,2002p.22)andwasconsistent

34
withKotter’sobservationthat:“Peoplechangewhattheydolessbecausetheyaregiven
analysisthatshiftstheirthinkingthanbecausetheyareshownatruththatinfluences
theirfeelings.”(Kotter&Cohen,2002p.1).
Emotionhelpedtocreateasenseofurgencyatseveralpointsinthe
developmentoftheUKFCMproject.Workgroupmembers,aswellasclinicproviders
andstaff,couldrelatepersonallyaswellasprofessionallytotheproblemoffallsinolder
adults.Manyhadfamilymemberswhohadfallenand/orhadtreatedpatientswhohad
sufferedfall-relatedinjuries.Thepractice-widemeetingduringwhichthepilotwas
introduced,openedwiththepresenter,aphysicianchampion,askingattendeestoraise
theirhandiftheyhadaparent,grandparent,otherfamilymemberorneighborwhohad
beenimpactedbyafall.Theproblemoffallswasdemonstratedvisuallywithpicturesof
anolderadultinahospitalbedandanx-rayofahipfracture,whilethepresenter
relatedapersonalstoryofherolderadultparentswhohadfallen.
Asenseofurgencywasenhancedbythetimelinessofthequalityimprovement
project.ACDCarticleonfallsprevention,publishedseveralweekspriortothe
presentation,includedamapwithKentuckyhighlightedasoneofthestateswiththe
highestratesofreportedfalls(Bergenetal.,2016).Mapsoffall-relatedhospitaland
emergencyroomadmissionsbycounty,createdbyKIPRC,werealsoincludedinthe
presentation.Enthusiasmtoplayaroleinchangingthosemapswaspotentiatedby
presentingCDCestimatesofhowmanyfallscouldbepreventedbyimplementing
STEADI.Thepresentation,modifiedtoincludepilotresults,wasalsomadetotheAEHR

35
UserGroupwhenrequestingthattheSTEADItoolbeincorporatedintotheelectronic
healthrecord.
Asenseofurgencywasalsocontributedtobytheinvolvementofseveral
workgroupmembersinotherprojectsthatdove-tailedwiththepilot.UKHChadrecently
achievedprestigiousMagnetStatus,thehighestawardforinstitutionalnursing
excellence.Qualityimprovementandinterdisciplinaryrelationshipsareimportantin
beinggrantedthisrecognition(ANCC,2011);thepilotrepresentedanopportunityto
supportthisrequirement.Othermembersoftheworkgrouphadparticipatedinafall
preventioninitiativeundertakeninanotherdepartmentwhichhadnotbeenfully
implementedduetobarrierssuchastimeconstraints.Workgroupmembersfromthis
departmentwishedtolearnwhethertheUKFCMclinicencounteredthesame
difficultiesand,ifso,howtheycouldbeovercome.Anadditionalincentivewastheuse
oftheprogramtomeetMIPSandTheJointCommission(TJC)reportingrequirements.
Publichealthpractitionersinvolvedintheproject,inadditiontofurtheringthe
implementationofSTEADIinthestate,werealsointerestedingaininginsightsinto
clinicalpracticeandqualityimprovementprocesses.
Step2:Buildaguidingcoalition
Organizationalchangeisledbyaguidingteamorcoalition,“withthecredibility,
skills,connections,reputationandformalauthorityrequiredtoprovidechange
leadership”(Kotter&Cohen,2002,p.4).Theworkgroupteampossessedthe“titles,
informationandexpertise,reputationsandrelationships”(Kotter,1995)neededto

36
movetheprojectforward.Thepilotproject,guidedbyphysicianchampions,brought
togetherkeystakeholders,fromvariousdepartmentsanddisciplineswithinUKHC,and
formedvaluablerelationshipsbetweentheUKhealthcaresystemandrepresentatives
fromKIPRCandKDPH,allofwhombroughttheiruniqueperspectivetoandroleinfall
prevention.
Step3:Formastrategicvisionandinitiatives
Theguidingteamorcoalitionischargedwithdeveloping“sensible,clear,simple,
upliftingvisionsandsetsofstrategies”(Kotter&Cohen,2002,p.4).Thefallprevention
workgroupwasguidedbyandbuiltuponthevisionoftheCDC’sandstatepublichealth
entitiestoreducefall-relatedratedmorbidity,mortalityandassociatedcosts.Thegroup
wasalsodrivenbytheorganizationalvisionofcontinuousqualityimprovementand
patient-centeredcare.Thisorganizationalvisionwascarriedoutthroughongoing
qualityimprovementprojectswithintheUKFCMpracticeandtheclinicdirectorhad
substantialexperienceleadingoroverseeingqualityimprovementteams.TheNursing
DepartmentexecutiveintheworkgrouphadbeeninvolvedinachievingMagnetStatus
andcontinuousqualityimprovementintheambulatoryspace.Theinitiativeto
incorporatethetemplateintotheAEHR,andthepotentialtogatherdataon
performancemeasuresandoutcomeswasavisionsharedbytheworkgroup,andwould
nothavebeenpossiblewithouttheearly,activeinvolvementandexpertiseofthe
informaticist.

37
Step4:Enlistavolunteerarmy
Thepilotwasdevelopedprimarilybyvolunteers.Thepilotrolloutinvolvedallclinic
providersandstaff,ratherthanonlyvolunteerswhoofferedtoparticipate.Nextstepsin
enterprise-wideSTEADIimplementationmayincludeenlistingvolunteerstopilotthe
programintheirrespectiveclinics,participateinothereffortstoimplementthe
programandincorporatereferralloopsforcommunity-basedfallprevention
interventions.
Step5:Enableactionbyremovingbarriers
Anassessmentoffacilitatorsandbarrierswasnotpartoftheinitialpilot,butis
animportantnextphaseinSTEADIimplementation.TheliteratureonSTEADI,aswellas
fallsscreeningpre-datingSTEADI,hasidentifiedanumberofbarriers,suchastimeand
competingclinicaldemands,whichlikelyimpactedthepilot.Whileanswerstothe
STEADIscreeningquestionsregardingfallhistoryandfearoffallingorunsteadiness,
completedbyaCSTorLPN,hadaresponserecordedonallofthe64forms,the
responseratewasnotasrobustfortheotherquestionswhichwereassessedby
providers.MedicationreviewandvitaminDquestionshavingresponseratesof25
percentand32percent,respectively.Asdiscussedintheresultssection,TUGtestand
otherriskfactorassessmentshadlowresponserates,asdidinterventions.Designflaws
inthetoolresultedinambiguousresponsesandsuboptimaldataanalysis.
Improvements,reflectingfeedbackfromprovidersandstaff,willneedtobe
madepriortoincorporationintotheAEHR,andmayrequireseveraliterationsbecoming

38
anoptimallyeffectivetemplateanddatasource.Likewise,barriersrelatedtoworkflow,
whichreceivedlittleattentionduringthepilotrollout,will,aswasdescribedinthe
Oregonreport,requirefurtherstudyandrefinement.
Gapsincommunicationrepresentedabarrierinpilotimplementation.The
overallgoalofreducingfallsthroughSTEADIwascommunicatedduringthemonthly
practice-widemeetingwhichtookplaceonedaypriortothestartofthepilot.While
informationregardingthepilotstartdateandtheroleofclinicteammembersin
completingtheforms,wasprovidedduringthemeeting,thiswasinadequatetoensure
thatthepilotransmoothly.Thepilotwasinitiallyintendedtoincludeonlythreeofthe
fivepracticeteams,butaftertwodays,onlyfourformshadbeencompleted,prompting
theexpansionofthepilottoincludeallfiveteams.Whensomestaffwereaskedifthey
hadbeenscreeningpatients,itwaslearnedthatthesestaffmemberswerenotawareof
thepilot,asthepractice-widemeetinghadbeenheldontheirdayoff.Therewasalso
lackofcommunicationwhenoneofthestaffwasabsentandanotheremployee,who
hadnotattendedthemeeting,wascalledintoassumethatemployee’sduties.Anemail
withdetailedpilotinformationcouldhavebeensenttophysiciansandotherproviders,
however,CSTsandnursingstaffdidnotroutinelyutilizeemailforcliniccommunication.
Conveningabriefdailyteamhuddlewouldhavehelpedtoensureallmembersofeach
teamwereawareofthepilotandtheirrespectiveroles.

39
Step6:Generateshort-termwins
Theoverallsuccessofthepilotwasusedtomovetheprojectforwardtowards
enterprise-wideimplementation.Resultsofthepilot,particularlythepercentageof
patientsscreenedandthepercentageofpositivescreens,wascommunicatedtothe
teamandtheAEHRUserGroup.PresentationtotheAEHRUserGroupresultedin
modificationstotheAEHRfallsscreeningtemplatetoincludetheSTEADIscreening
questions(Figure6andFigure7).Theassessmentandinterventionsportionofthetool
werereferredtotheAEHRUserGroupteaminchargeofscreeningtemplates,for
furtherrevisiontoeliminateambiguities,priortoinclusionintheAEHR.
Step7:Sustainacceleration
Short-termwinsarebuiltuponinordertogainmomentumand“createwaveafterwave
ofchangeuntilthevisionisareality.”(Kotter&Cohen,2002,p.5).Therewas
substantialmomentumfromthepointofinceptionthroughpilotrolloutand
presentationtotheAEHRUserGroup.Thechallengewillbetosustainaccelerationand
takethestepsneededtosuccessfullyimplementSTEADI,includingtrainingstaff;
identifyingbarriers;improvingworkflow;optimizingtheAEHRtemplate;facilitatingand
monitoringuptakeinotherprimarycareclinics;andgatheringdataforquality
performancereporting.Continuedcooperationwithpublichealthentitieswillfacilitate
themonitoringoffallratereductionandothermetrics.Coordinationwithuniversity
andcommunityresources,suchastheExtensionService,willbeneededtoensurethat

40
momentumisnotlostinlinkingpatientstocommunityresources,andclosingtheloop
throughAEHRinterventionandoutcomedocumentation.
Step8:Institutechange
Thefinalstepintheprocessoforganizationalchangeis“tomakechangestickby
nurturinganewculture”(Kotter&Cohen,2002,p.5).Therecurrentlyexistsastrong
cultureofqualityimprovementwithinUKHC.TheSTEADIinitiativeappearedtobewell-
receivedbybothclinicstaff,providersandtheAEHRUserGroup,butitistooearlyto
knowwhethertheSTEADIpilotwillresultinfullimplementationintheUKFCMclinicand
inotherprimarycarethroughouttheUKhealthcaresystem.
Basedonthepilotplanningprocess,rolloutandevaluation,anumberoflessonslearned
wereidentified.
LessonsLearned
LessonslearnedduringthedevelopmentandrolloutoftheUKFCMpilotincluded:
• Communication--Themonthlypractice-widemeetingwasaneffective
foruminwhichtopresentthepilot;nonethelesssomeprovidersandstaff
wereabsentduetotheirindividualschedules.Emailswithkeypointsofthe
pilot,sentpriortoandafterthemeeting,wouldatleastinpartaddressed
thisproblem.Thesekeypointscouldalsohavebeenreviewedandreinforced
attheweeklyteammeetingandteamhuddlesheldimmediatelypriortothe
startofclinic.

41
• STEADIformdesign–Afterthepilotwasconducteditbecameclearthat
therewereanumberofambiguitiesintheassessmentandintervention
portionsofthepaperform,whichwouldhavebeenapparenthaditbeen
testedpriortouse.Theassessmentandinterventionsectionsoftheformwill
needtoberevisedbytheAEHRUserGroupcommitteeoverseeingscreening
templates,priortoincorporationintotheAEHR.
• Divisionoftasks–Duringthedevelopmentprocessitwasdecidedthatthe
TUGtest,whichincludesanassessmentofpatientgaitandbalance,was
outsideoftheCST’sscopeofpractice.Hadthetestbeenlimitedtorecording
thetimeittookforthepatienttocompletetheTUG,itcouldhavebeen
performedbytheCST,therebyreducingtheburdenontheproviderand
likelyincreasingthenumberoftestsdoneduringthepilot.
• Training–TherewerenoformalSTEADItrainingsessionsconductedaspart
ofthepilot.ATUGtestvideowasnotshownduringthepracticemeetingdue
totechnicaldifficulties.Alinktothevideowasemailedtoproviders,but
giventhatthepracticemeetingandemailoccurredthedaybeforethepilot
commenced,providersmayhavenothadenoughtimetoviewthevideo.
• Referralstofallpreventionprograms–Therewerenoreferralsmadeto
communityoruniversity-affiliatedfallpreventionorexerciseprograms,
whichmayhavebeenattributabletolackofproviderfamiliaritywiththese
programs.AshasbeennotedintheSTEADIliterature,processesthat
seamlesslylinkpatientstofallpreventionprogramsareneededinorderto

42
ensurethatpatientsreceiveevidence-basedinterventionsandthat
participationandcompletionoftheinterventionisdocumentedinthe
patient’selectronichealthrecord.
• Interdisciplinary,interdepartmentalcooperation–Collaborationamong
differentdisciplinesanddepartmentswaskeytothepilot’ssuccess.The
experiencesofworkgroupmemberswhohadparticipatedinfall-related
projectsinotherdepartments,theinpatientsettingandinitialambulatory
screeningprojecthelpedguidepilotdevelopment.Interdepartmental
collaborationwas,andwillcontinuetobeinstrumentalintheintegrationof
theSTEADItoolintotheenterprise-wideAEHRpreventivehealthnoteform.
• Theroleofpublichealth–BothUKFCMandpublichealthentitiesbenefited
bytheSTEADIpilotpartnership.UKFCMwasabletoimprovethequalityof
careitprovidestoolderadultpatientsthroughtheuseofaclinicaldecision
supporttooldevelopedbytheCDCandpromotedthroughthestatehealth
department.ItwasabletoprovidepatientswithCDCeducationalmaterials
suppliedbyKDPH.KDPHgainedinsightsintothechallengesfacedby
cliniciansandhealthcaresystemsinSTEADIimplementation,whichwill
informitsstatewideimplementationefforts.

43
Recommendations/NextSteps
• Asurveyand/ormeetingsshouldbeconductedinordertosolicitfeedbackfrom
providersandstaffwhoparticipatedinthepilot.Facilitatorsandbarriers,aswell
aspotentialsolutionstochallengesshouldbeidentifiedandincorporatedinto
theAEHRtoolandenterprise-wideSTEADIimplementation.
• TheAEHRtemplateshouldberevisedtoeliminate/reduceambiguitiesthatwere
presentinthepaperform.Providersshouldtestthetoolpriortointegrationinto
theAEHR.Thescreeningquestions,medicationreviewandvitaminD
supplementation(ifappropriate)shouldbefeaturedprominently.
• TheAEHRtoolshouldbelinkedtoreimbursementforMedicareannualwellness
visits,whichincludefallriskscreening.Thismayalsoservetoincreaseutilization
ratesforthesevisits,whichareonly12.8%inKentucky,and17.7%nationally
(CMS,2015).
• STEADItoolkittrainingsessionsshouldbeconducted,preferablyinsmallgroup
sessions,aswasdoneintheOregonpilot(Caseyetal.,2016).KDPHcould
participateinthetrainingofcliniciansandstaff,asthismodelhasbeenused
successfullyinotherSTEADIimplementationprojects.OnlineCDCSTEADI
training,forwhichcontinuingeducationcreditsaregranted,shouldalsobe
encouraged.
• Workflowandtaskallocationamongteammembersshouldbeformallyassessed
andrefinedbasedonproviderandstafffeedback.Inaddition,engagingother
UKHCprofessionals,suchasPharmacists,whocouldcontributeexpertisein

44
medicationmanagementandreducetheburdenonproviders.TheCDChas
recentlylaunchedonlineSTEADItrainingandcontinuingeducationcreditsfor
pharmacists(CDC,2017).ThePhysicalTherapydepartmentshouldcontinueto
beinvolved,andcouldassistinperforminggaitandbalanceassessments.
• Providersandstaffshouldreceiveadditionalinformationandeducationon
evidence-baseduniversityandcommunityfallpreventioninterventions,suchas
Stepping-OnandTaiChi:MovingforBetterBalance.
• Referralstocommunity-basedprogramsshouldbedocumented,withfollowup
regardingwhetherthepatientparticipatedinandcompletedtheprogram.The
referralprocesswouldideallybeincorporatedintotheAEHR.
• Relationshipswithcommunityorganizationsandpublichealthentitiesshouldbe
continuedandstrengthened.KDPH’scontinuedinvolvement,particularlyinthe
areaoftraining,willbeimportantinsuccessfulimplementationbothwithinthe
UKHCsystemandstatewide.Asastatehealthdepartment,KDPHcanactasa
“connector”byprovidingforumsinwhichUKHCcanshareitsmodelwithother
stakeholders(Shubertetal.,2016).

45
Conclusion:
TheSTEADIalgorithmandtoolkitpromisetoreducefallsinolderadults
nationallyandinKentucky.UKFMCembarkedonthefirststepinimplementingSTEADI
inamajorhealthcaresystemintheCommonwealth.Thefive-daypilotresultedin
screeningalmost50percentofeligiblepatients.Thepilotdevelopmentandrollout
containedmanyofKotter’selementsforsuccessfulorganizationalchange.Thethreekey
strengthswhichhelpedtoensurethepilot’ssuccesswere:1)creatingasenseof
urgencythroughcouplingcompellingepidemiologicaldataregardingthehighrateof
fallsinKentucky,totheemotionalandpersonalimpactoffallsonindividualsandtheir
families;2)buildingaguidingcoalitionofstakeholders,includingthe
interdisciplinary/interdepartmentalworkgroupandKDPH;and3)generatingshortterm
winsbycompletingapilotthatachievedascreeningrateofclosetohalfofallalleligible
patientsandadvocatingforintegrationofSTEADIintotheAEHR.Challengesincluded
effectivecommunicationwithclinicstaffandambiguitiesinthepaperSTEADIform
whichhinderedpilotdataanalysis.Nextstepsintheimplementationprocessinclude
formalassessmentofworkflowandbarriers,suchascost,time,staffingandresources.
FurtherrevisionoftheAEHRtemplatewillbeneededinordertooptimizeuptakeand
enablethecollectionandanalysisofdataforreimbursementandreportingofquality
measures.Reimbursementandotherincentiveswillalsoberequiredtobuildabusiness
caseandachievebuy-infromhealthcaresystemleadership.

46
ImplementationofSTEADIthroughoutUKHC,aswellasstatewidecommunity-
basedprimarycarepracticeswhopartnerwithUKHC,willbeincrementalandtailored
totheuniqueneedsandenvironmentofeachclinicalsite.Optimally,thealgorithminits
entiretywouldbeimplemented,asmultidimensionalinterventions,particularlythose
thatincludegait,balanceandstrengthtraining,havethegreatestimpactonreducing
falls(Stevens&Burns,2015).Amorelimitedapproach,focusingonthreekeyactions:
screening,reviewingmedicationstoreduce/eliminatethosethatincreasefallriskand
prescribingVitaminD,toimprovemusculoskeletalhealth(Bergenetal.,2016)mayalso
beconsideredinordertopromotebetteruptake.
Finally,continuedpartnershipwithkeystakeholders,oneofthestrengthsofthe
UKFCMpilot,willbeneededtoassurethatSTEADI’saimofreducingfallratesinolder
adultisachieved.Publichealthentitiesandothercommunitypartnerswillbecriticalin
providingtraining,evidence-basedinterventionsandoutreachtovulnerableand
underservedolderadults.Strongcollaborativerelationshipswillneedtobeforged
betweenhealthcareprovidersandcommunityorganizationstocreateaseamless
referralprocess.
Injuryanddeathresultingfromfallsisasignificantpublichealthproblemin
Kentucky,whichhasreportedratesabovethenationalaverage.Furtherresearch
regardingtheetiologyofthestate’shighratesoffallsandfall-relatedinjuriesisneeded
inordertodeveloptargetedsolutions.Fallsandfall-relatedinjurieswillhaveagrowing
impactasthepopulationages.TheUKFCMSTEADIpilotrepresentsanimportantfirst

47
stepinreducingtherateofinjuries,deaths,aswellasthecosts,attributabletofallsin
theolderpopulationinKentucky.

48
References
AmericanCollegeofPreventiveMedicine(ACPM),ACPM-CDCCooperativeAgreement. Retrievedathttp://www.acpm.org/general/custom.asp?page=cdcprojects. AccessedApril26,2017.AmericanNursesCredentialingCenter(ANCC)(2011).MagnetRecognitionProgram
AProgramOverview.Retrievedathttp://nursecredentialing.org/Documents/Magnet/MagOverview-92011.pdf.AccessedApril1,2017.
Baldwin,G.,Breiding,M.,&Sleet,D.(2016).UsingthepublichealthmodeltoaddressunintentionalinjuriesandTBI:aperspectivefromtheCentersforDiseaseControlandPrevention(CDC).NeuroRehabilitation,39(3),345-349.
BergenG.,StevensM.R.,BurnsE.R.(2016).FallsandFallInjuriesAmongAdultAged≥65Years–UnitedStates,2014.MMWRMorbMortalWklyRep,65:993-998.DOI:http://dx.doi.org/10.15585/mmwr.mm6537a2.
BurnsE.R.,StevensJ.A.,Lee,R.(2016).Thedirectcostsoffatalandnon-fatalfallsamongolderadults—UnitedStates.JSafetyRes,58:99–103.doi:10.1016/j.jsr.2016.05.001.Epub2016May28.
CaseyC.M.,ParkerE.M.,WinklerG.,LiuX.,LambertG.H.,EckstromE.(2016). LessonsLearnedfromImplementingCDC’sSTEADIFallsPrevention
AlgorithminPrimaryCare.Gerontologist.00(00):1-10.Epub2016Apr29.CentersforDiseaseControlandPrevention(CDC)(2015).TakeaStandonFalls.
Retrievedfromhttp://www.cdc.gov/features/older-adult-falls/index.html.AccessedApril26,2017.
CentersforDiseaseControlandPrevention(CDC)(2016).STEADIMaterialsforHealthCareProviders.Retrievedfromhttps://www.cdc.gov/steadi/materials.html.AccessedApril1,2017.
CentersforDiseaseControlandPrevention(CDC)(2017).STEADI–OlderAdultFall Prevention.Retrievedfromhttps://www.cdc.gov/steadi/.AccessedApril11, 2017.CentersforMedicare&MedicaidServices(CMS)(2015).BeneficiariesUtilizingFree PreventiveServicesbyState,2015.Retrievedfrom
https://downloads.cms.gov/files/Beneficiaries%20Utilizing%20Free%20Preventive%20Services%20by%20State%20YTD%202015.pdf.AccessedApril1,2017.
Child,S.,Goodwin,V.,Garside,R.,Jones-Hughes,T.,Boddy,K.,&Stein,K.(2012).Factorsinfluencingtheimplementationoffall-preventionprogrammes:asystematicreviewandsynthesisofqualitativestudies.Implementationscience,7(1),91.
Chou,W.C.,Tinetti,M.E.,King,M.B.,Irwin,K.,&Fortinsky,R.H.(2006).Perceptionsofphysiciansonthebarriersandfacilitatorstointegratingfallriskevaluationandmanagementintopractice.JournalofGeneralInternalMedicine,21(2),117-122.
Dr.FloyduseshealthITtoimprovefallriskscreeningforelderlypatients(2014).

49
Retrievedfromhttps://www.healthit.gov/providers-professionals/dr-floyd-uses- health-it-improve-fall-risk-screening-elderly-patients.AccessedApril1,2017.FergusonN.,FriedmanY.&BulatT.(2016)ImplementingCDCSTEADI(Stopping
ElderlyAccidents,Deaths,andInjuries)ToolkitintoVAPACT(PatientAlignedCareTeam).JournaloftheAmericanGeriatricsSociety.May1;64:S50.A95.
Fortinsky,R.H.,Iannuzzi-Sucich,M.,Baker,D.I.,Gottschalk,M.,King,M.B.,Brown,C.J.,&Tinetti,M.E.(2004).Fall-RiskAssessmentandManagementinClinicalPractice:ViewsfromHealthcareProviders.JournaloftheAmericanGeriatricsSociety,52(9),1522-1526.
Gearon,C.J.AFocusonFalls:HospitalsPushtoImprovePopulationHealth.U.S.News&WorldReport.October8,2015.Retrievedfromhttp://health.usnews.com/health-news/hospital-of-tomorrow/articles/2015/10/08/a-focus-on-falls-anatomy-of-a-hospital-push-to-improve-population-health.AccessedFebruary6,2017.
Gillespie,L.D.,Robertson,M.C.,Gillespie,W.J.,Sherrington,C.,Gates,S.,Clemson,L.M.,&Lamb,S.E.(2012).Interventionsforpreventingfallsinolderpeoplelivinginthecommunity.CochraneDatabaseSystRev,9(11).
Houry,D.,Florence,C.,Baldwin,G.,Stevens,J.,&McClure,R.(2016).TheCDCinjurycenter’sresponsetothegrowingpublichealthproblemoffallsamongolderadults.Americanjournaloflifestylemedicine,10(1),74-77.
Jones,T.S.,Ghosh,T.S.,Horn,K.,Smith,J.,&Vogt,R.L.(2011).Primarycarephysiciansperceptionsandpracticesregardingfallpreventioninadult's65yearsandover.AccidentAnalysis&Prevention,43(5),1605-1609.
Kaniewski,M.,Stevens,J.A.,Parker,E.M.,&Lee,R.(2015).AnintroductiontotheCentersforDiseaseControlandPrevention’seffortstopreventolderadultfalls.Evidence-BasedProgrammingforOlderAdults,23.
KentuckyInjuryandPreventionResearchCenter,abonafideagentfortheKentucky DepartmentforPublicHealth.April12,2017.DataSource:KentuckyInpatient
HospitalizationandOutpatientServicesDatabase,KentuckyOfficeofHealthPolicy.Datafor2010–2014areprovisionalandsubjecttochange.Retrievedfromhttps://kyibis.mc.uky.edu/kiprc;http://www.safekentucky.org/images/Data/falls-by-county/senior-falls-KY.htmlhttp://www.safekentucky.org/images/Data/falls-by-county/senior-falls-KY.html.
KentuckySafeAgingCoalition(KSPAN)(2009-2014)KentuckySafeAgingCoalition(KSAC).Retrievedfrom
http://www.safekentucky.org/index.php/top-menu-older-adults-safety.AccessedApril1,2017.
KentuckySafeAgingCoalition(KSPAN).RetrievedApril12,2017fromKentuckyInjuryPreventionandResearchCenter(abonafideagentoftheKYDepartmentforPublicHealth),KY-IBISsite:https://kyibis.mc.uky.edu/kiprc;http://www.safekentucky.org/images/Data/falls-by-county/senior-falls-KY.html.
KentuckySafetyandPreventionAlignmentNetwork(KSPAN)(2014).KentuckySafe

50
AgingCoalition(KSAC).Retrievedfromhttp://www.safekentucky.org/images/Data/falls-by-county/senior-falls-KY.html.
Kotter,J.R.(1995).Leadingchange–whytransformationeffortsfail.Harvardbusinessreview,85(1),96-+.
Kotter,J.P&Cohen,D.S(2002).TheHeartofChange.HarvardBusinessSchoolPress.Boston,Massachusetts.
Landis,S.E.,&Galvin,S.L.(2014).Implementationandassessmentofafallscreeningprograminprimarycarepractices.JournaloftheAmericanGeriatricsSociety,62(12),2408-2414.
Moyer,V.A.(2012).Preventionoffallsincommunity-dwellingolderadults:US PreventiveServicesTaskForcerecommendationstatement.Annalsof
internalmedicine,157(3),197-204.Moylan,K.C.,&Binder,E.F.(2007).Fallsinolderadults:riskassessment,
managementandprevention.TheAmericanjournalofmedicine,120(6),493-e1.
Phelan,E.A.,Mahoney,J.E.,Voit,J.C.,&Stevens,J.A.(2015).Assessmentandmanagement offallriskinprimarycaresettings.MedicalClinicsofNorthAmerica,99(2),281-293.
RAMA(2015),ImplementationofSTEADI(StoppingElderlyAccidents,Deaths,andInjuriesinOhioHealthCareProviders,FinalReport.ProvidedbytheOhio
DepartmentofHealth.RAMA(2016)ImplementationofSTEADI(StoppingElderlyAccidents,Deaths,andInjuriesinOhioHealthCareProviders,6-MonthEvaluationReport.Providedby
theOhioDepartmentofHealth.Shubert,T.E.,Smith,M.L.,Prizer,L.P.,&Ory,M.G.(2013).Complexitiesoffall
preventioninclinicalsettings:Acommentary.TheGerontologist,gnt079.Smith,M.L.,Stevens,J.A.,Ehrenreich,H.,Wilson,A.D.,Schuster,R.J.,Cherry,C.O.B.,
&Ory,M.G.(2015).Healthcareproviders’perceptionsandself-reportedfallpreventionpractices:findingsfromalargeNewYorkhealthsystem.Frontiersinpublichealth,3.
Stevens,J.A.(2005).Fallsamongolderadults—riskfactorsandpreventionstrategies.Journalofsafetyresearch,36(4),409-411.
Stevens,J.,Phelan,E.(2013).DevelopmentofSTEADI:AFallPreventionResourceforHealthCareProviders.HealthPromotionPractice.14(5):706-714.
Stevens,J.A.,Burns,E.(2015).ACDCCompendiumofEffectiveFallInterventions:What WorksforCommunity-DwellingOlderAdults.In:DivisionofUnintentionalInjuryPreventionNationalCenterforInjuryandPreventionControl.2015.Retrievedfrom
http://www.cdc.gov/homeandrecreationalsafety/falls/compendium.html.AccessedMarch13,2017.
Thoreson,S.R.,Shields,L.M.,Dowler,D.W.,&Bauer,M.J.(2015).Publichealthsystemperspectiveonimplementationofevidence-basedfallpreventionstrategiesforolderadults.Evidence-BasedProgrammingforOlderAdults,70.
Tinetti,M.E.,Speechley,M.,&Ginter,S.F.(1988).Riskfactorsforfallsamongelderly

51
personslivinginthecommunity.NewEnglandjournalofmedicine,319(26),1701-1707.
Tinetti,M.E.,&Brach,J.S.(2012).Translatingthefallpreventionrecommendationsintoacoveredservice:canitbedone,andwhoshoulddoit?.Annalsof
internalmedicine,157(3),213-214.UHS(2013).UHSandBroomeCountypilotnationwidefall-preventionprogram.
Retrievedfromhttp://www.uhs.net/about-us/media-lounge/2013/UHS-and-Broome-County-pilot-nationwide-fall-prevention-program/.AccessedFebruary6,2017.
UnitedStatesCensusBureau.QuickFactsKentucky.Retrievedfromhttps://www.census.gov/quickfacts/table/AGE775215/21,21067,00.AccessedApril11,2017.
UnitedStatesPreventiveServicesTaskForce(USPSTF)(2017).Retrievedfromhttps://www.uspreventiveservicestaskforce.org/Page/Document/UpdateSummaryFinal/falls-prevention-in-older-adults-counseling-and-preventive-medication?ds=1&s=fall.AccessedMarch4,2017.
UKHealthCare.RationalizingHealthCareinKentucky2015-2020StrategicPlan.Retrievedfromhttps://ukhealthcare.uky.edu/uploadedFiles/about/leadership/strategic-plan(1)/home/2015-2020-strategic-plan.pdf.AccessedFebruary21,2017.
WorldHealthOrganization.(2015).WHOglobalreportonfallspreventioninolderage.2007.Geneva:WorldHealthOrganization(WHO).Retrievedfromhttp://www.who.int/ageing/publications/Falls_prevention7March.pdf.AccessedApril26,2017.
Yardley,L.,Donovan-Hall,M.,Francis,K.,&Todd,C.(2006).Olderpeople'sviewsofadviceaboutfallsprevention:aqualitativestudy.HealthEducationResearch,21(4),508-517.

52
AppendixA:StayIndependentBrochure
CDC,2016