
Brian R. Odum, DO Resident Physician University of ... · Brian R. Odum, DO Resident Physician...
32
Brian R. Odum, DO Resident Physician University of Missouri-Columbia Department of Pathology and Anatomical Sciences
Transcript of Brian R. Odum, DO Resident Physician University of ... · Brian R. Odum, DO Resident Physician...
Brian R. Odum, DO
Resident Physician
University of Missouri-Columbia
Department of Pathology and Anatomical Sciences
Patient Presentation
A 13 year old male without significant
past medical history was transferred to
the pediatric intensive care unit at our
institution from an outside hospital for
further management of new onset
intraparenchymal brain hemorrhage.
History of Present Illness
He had been in his usual state of health until five weeks prior to admission when he began experiencing intermittent epistaxis and noted an associated petechial rash and several ecchymoses
Approximately three weeks after the onset of these symptoms, the patient fell while skate boarding, striking the back of his head against concrete At the time of the injury he denied loss of consciousness,
nausea, vomiting, or significant headache
In the days following the fall, he reported persistent intermittent frontal headaches unresponsive to acetaminophen and non-steroidal anti-inflammatory medications.
Outside Hospital
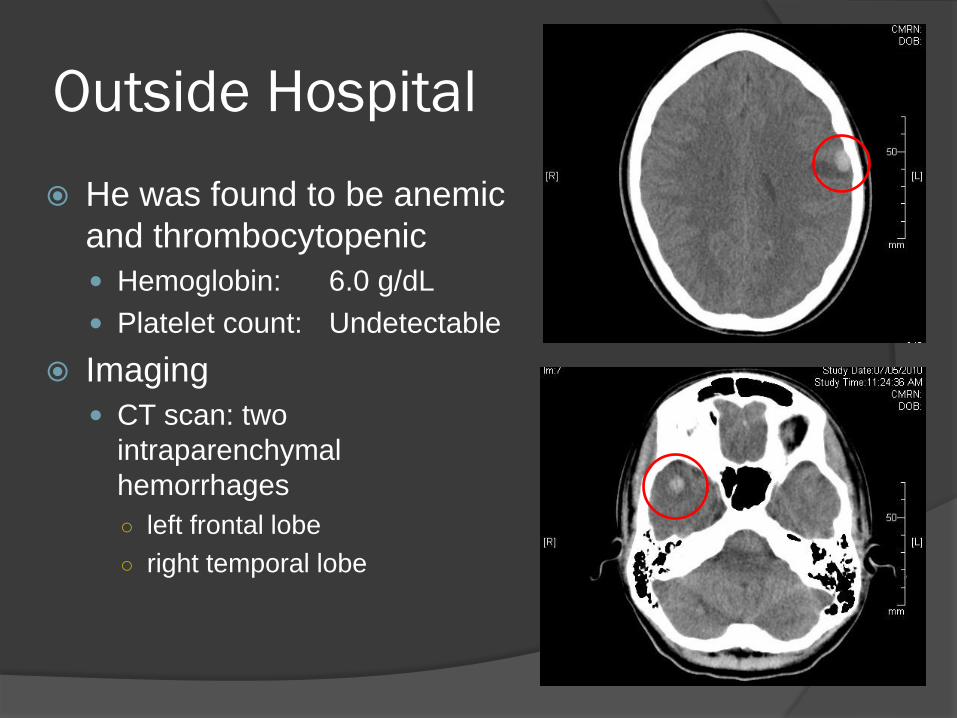
He was found to be anemic
and thrombocytopenic
Hemoglobin: 6.0 g/dL
Platelet count: Undetectable
Imaging
CT scan: two
intraparenchymal
hemorrhages
○ left frontal lobe
○ right temporal lobe
On Admission
Complete blood count revealed a Hgb: 5.6 g/dL,
WBC: 10.3x103/µL ○ normal differential
Plt: 5x103/ µL.
Peripheral smear revealed Severe normochromic normocytic anemia
Mild reticulocytosis without schistocytosis
Severe thrombocytopenia
Bone marrow biopsy Mildly hypercellular, normoblastic bone marrow
Increased megakaryocytes
No evidence of hematologic malignancy
Bacterial blood cultures negative
Serology for ehrlichia negative
Diagnosis
Immune Thrombocytopenia (ITP)
Having excluded hypoplastic, infectious, and
neoplastic etiologies for thrombocytopenia
Initial Treatment
IVIg
○ 1 gm/kg
Initiated almost immediately
Bolus platelet transfusion
○ 2 apheresis units
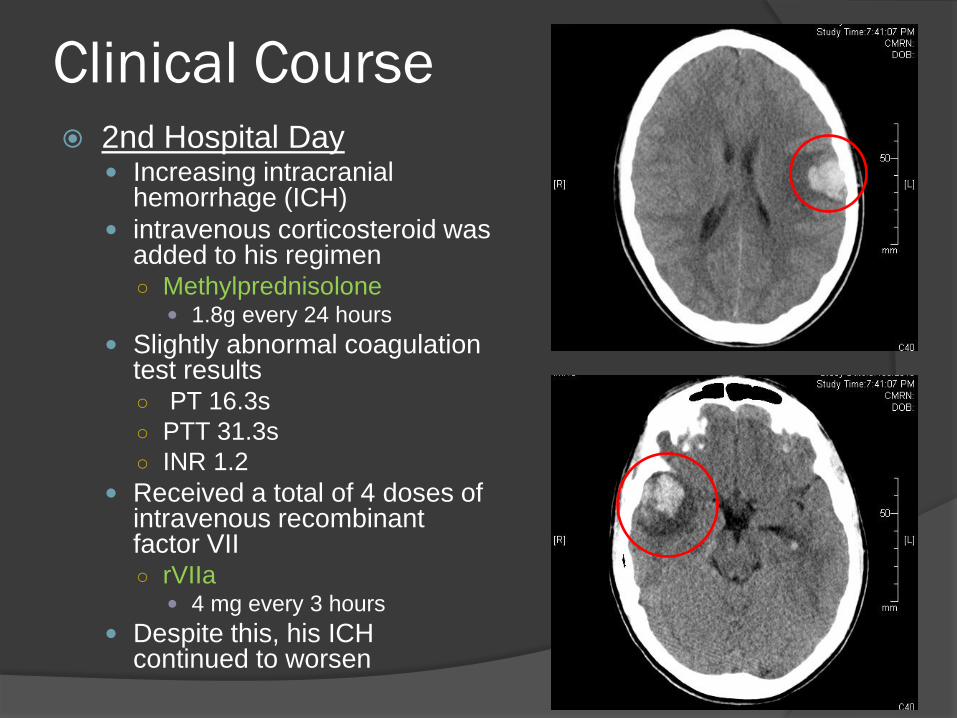
Clinical Course 2nd Hospital Day
Increasing intracranial hemorrhage (ICH)
intravenous corticosteroid was added to his regimen ○ Methylprednisolone
1.8g every 24 hours
Slightly abnormal coagulation test results ○ PT 16.3s
○ PTT 31.3s
○ INR 1.2
Received a total of 4 doses of intravenous recombinant factor VII ○ rVIIa
4 mg every 3 hours
Despite this, his ICH continued to worsen
Clinical Course
3rd Hospital Day IVIG discontinued in favor of
corticosteroids
Received a third unit of apheresis platelets via bolus infusion.
These measures continued to fail to produce significant rise in platelet count ○ Maximum uncorrected increment
2x103/µL
○ Maximum corrected count increment 1104 m2/µL
Low-dose continuous platelet infusion (platelet drip) initiated ○ Transfusion rate: ½ apheresis unit
every 3 hrs
4th Hospital Day He began showing some
evidence (albeit intermittent) of rising platelet counts ○ Maximum platelet count
25x103/µL
Hemorrhage stabilized
Infusion of intravenous rVIIa discontinued
Methylpredinsolone taper begun
5th and 6th Hospital Days Ongoing platelet drip
Platelet count continued to fluctuate ○ Range of 4x103/µL to 21x103/µL
ICH remained stable
Clinical Course
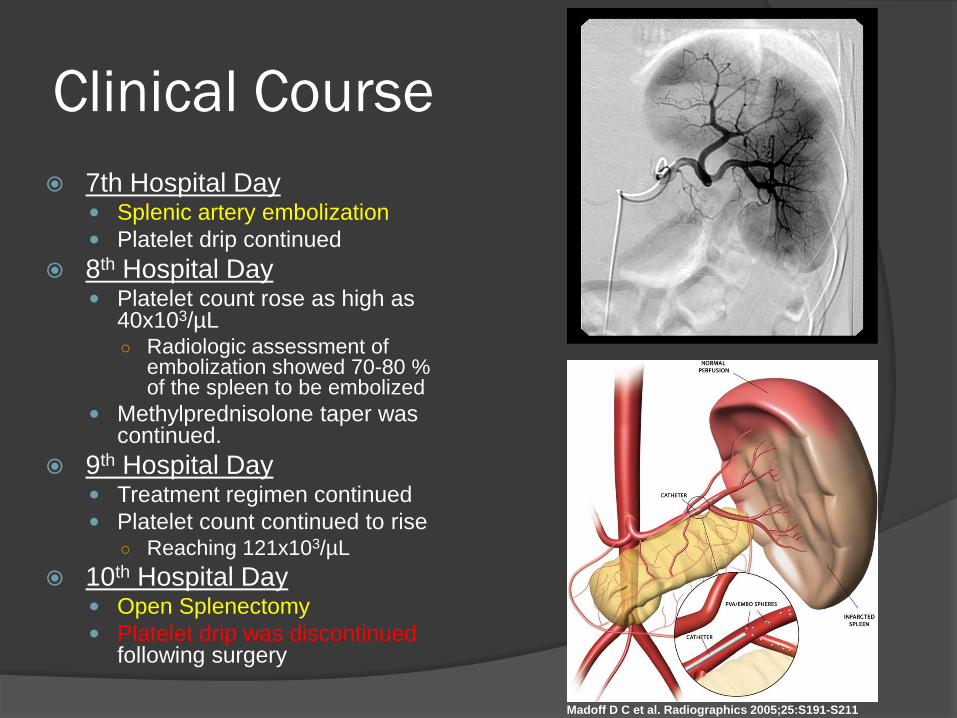
7th Hospital Day Splenic artery embolization
Platelet drip continued
8th Hospital Day Platelet count rose as high as
40x103/µL ○ Radiologic assessment of
embolization showed 70-80 % of the spleen to be embolized
Methylprednisolone taper was continued.
9th Hospital Day Treatment regimen continued
Platelet count continued to rise ○ Reaching 121x103/µL
10th Hospital Day Open Splenectomy
Platelet drip was discontinued following surgery
Madoff D C et al. Radiographics 2005;25:S191-S211
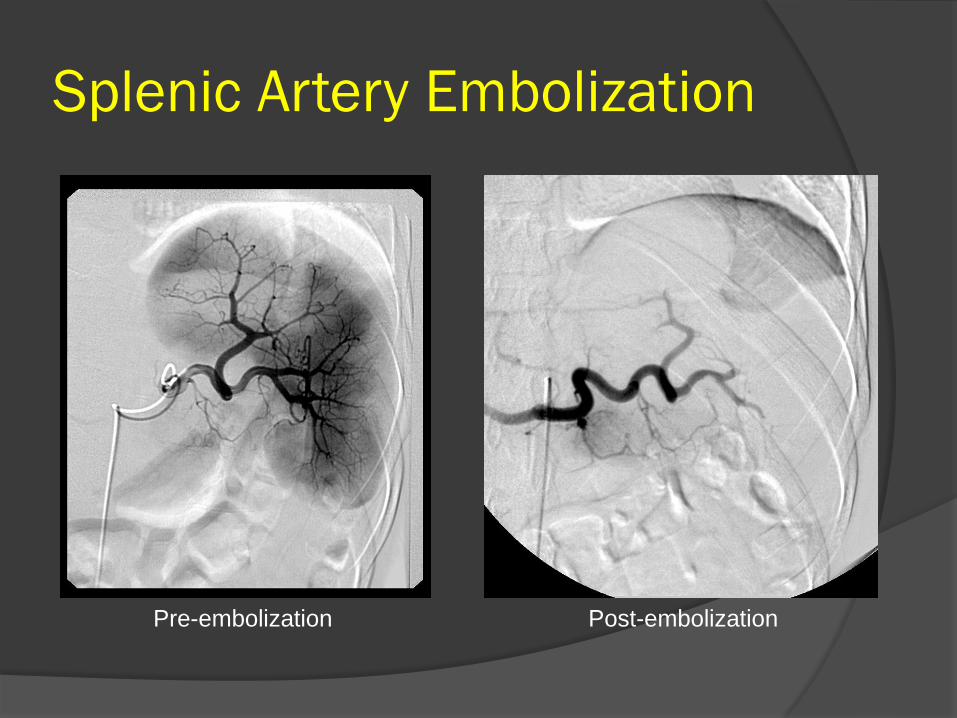
Splenic Artery Embolization
Pre-embolization Post-embolization

Splenectomy O = megakaryocyte
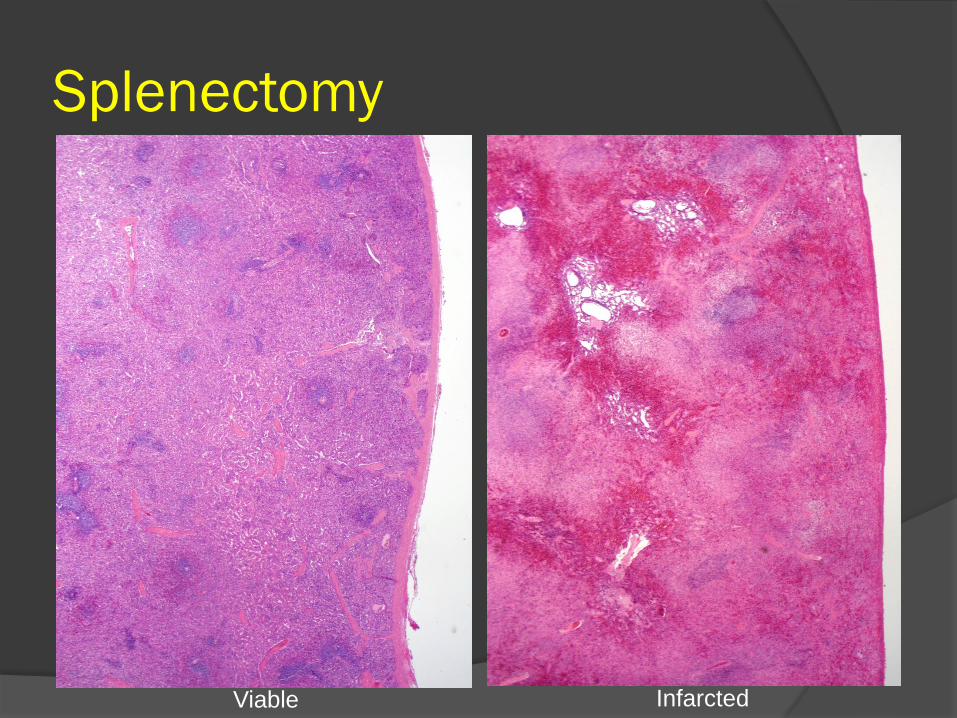
Splenectomy
Viable Infarcted

Clinical Course
14th Hospital Day Platelet count rose to a high of 141x103/µL
15th Hospital Day Platelet count rose to 172x103/µL
Platelet drip discontinued ○ decline in platelet count to 41x103/µL
16th Hospital Day Platelet count gradually decreases
○ Low of 14x103/µL
17th Hospital Day Platelet drip re-initiated
○ Platelet count gradually increases to 32x103/µL
11th Hospital Day Platelet count dropped to
41x103/µL in the morning
Continued to decline throughout the day ○ Low of 11x103/µL
Platelet drip re-initiated ○ Platelet count rose to 29x103/µL.
12th Hospital Day Platelet count remained stable
○ mid to high 20x103/µL range
13th Hospital Day Platelet counts again fell
○ possibly in response to continued methylprednisolone taper
No increase in ICH and no overt bleeding
Platelet drip was increased ○ one full unit every four hours
Corticosteroid dose was increased
Clinical Course
Days 18-24 Platelet drip continued
Platelet count fluctuates ○ Peaks at 104x103/µL
○ Danazol (started day 23) 300 mg bid
25th Hospital Day Platelet drip discontinued
○ decline in platelet count to 14x103/µL
26th Hospital Day Platelet count drops
continuously to 3x103/µL ○ Epistaxis
○ Bleeding from incisions
Aminocaproic acid started ○ 3,000 mg q6h
Platelet drip re-initiated
27th and 28th Hospital Days Platelet count rose
incrementally ○ 15x103/µL to 20 x103/µL
range
29th Hospital Day Platelet drip continued
Azothioprine added ○ 50 mg daily
30th Hospital Day No changes
Platelet count increased to 104 x103/µL
31st Hospital Day Platelet drip discontinued
Platelet count decreased to 13x103/µL
Clinical Course
32nd Hospital Day Platelet drip re-initiated
33rd and 34th Hospital Days Platelet count increased to
63x103/µL
35th Hospital Day Platelet drip discontinued
Platelet count decreased to 9x103/µL
Days 36-40 Condition remained stable
Platelet count remained stable
○ 10x103/µL-13x103/µL
41st Day
Discharged!!!! Platelet count 13x103/µL
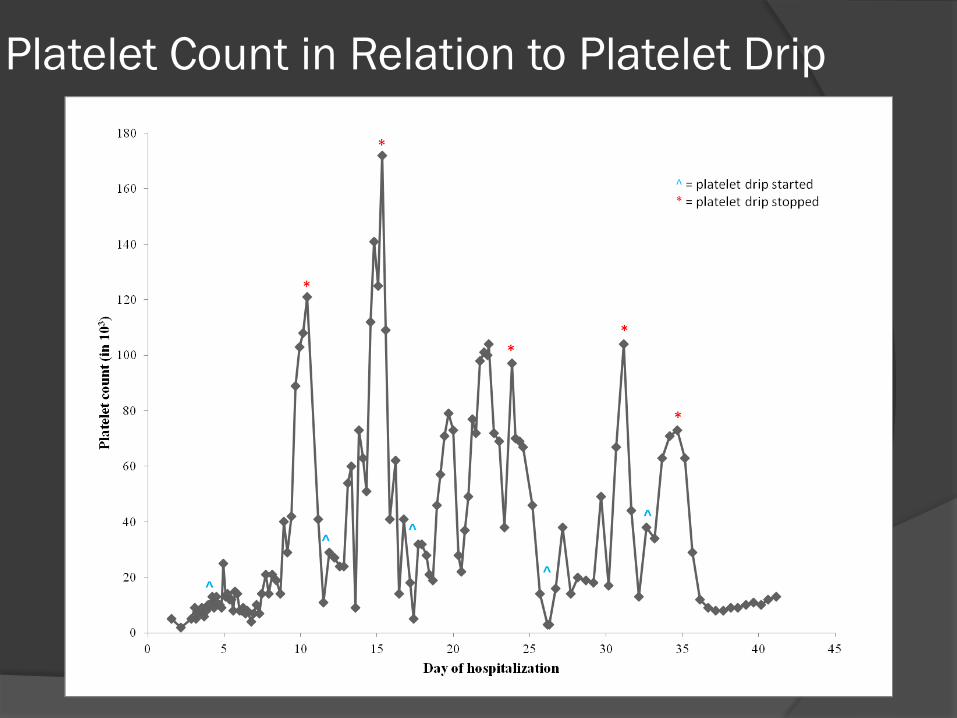
Platelet Count in Relation to Platelet Drip

Total Platelet Use
Apheresis Platelets
12 units over the course of his
hospitalization
Platelet Drip
193 platelet aliquots over the course of his
hospitalization

Immune Thrombocytopenia (ITP)
acquired autoimmune disease characterized by isolated thrombocytopenia (<100x103/µL) in the absence of a known underlying etiology
Previously known as Idiopathic Thrombocytopenic Purpura Nomenclature changed in light of consensus
opinion of an International Working Group on ITP(1)
○ Patients rarely show signs of bleeding (purpura)
○ Research points toward an autoimmune pathogenesis

Immune Thrombocytopenia (ITP)
Pathogenesis
Conventional theories of pathogenesis have
centered on increased autoantibody-mediated
destruction of platelets via the mononuclear
phagocyte (reticuloendothelial) system
Evolving theories of pathogenesis are more
complex
○ inhibition of platelet production(2,3)
○ T-cell mediated platelet destruction(4)
Additional research into potential genetic
mechanisms is underway(5)

Immune Thrombocytopenia (ITP)
Diagnosis(6)
ITP is a diagnosis of exclusion
Other etiologies of thrombocytopenia must be ruled out
Work-up(6)
History
Physical exam
Complete blood count
Peripheral blood smear
Bone marrow biopsy

Immune Thrombocytopenia (ITP)
Clinical Features Onset
○ Adults Insidious onset
Chronic course
○ Children Acute onset
- Often following a viral illness
Generally short-lived
Symptoms ○ Variable
Absent to minimal bleeding/bruising versus widespread hemorrhage from the GI tract, skin, and/or mucosal surfaces
Intracranial hemorrhage (ICH) is a rare, potentially life-threatening, complication(7)
Immune Thrombocytopenia (ITP)
Treatment(8) Medical
○ First line Corticosteroids
Intravenous immunoglobulin (IVIg)
Rh immunoglobulin (Rhogam, Winro)
- Only effective in Rh+ patients
○ Second line Additional immunotherapy
- azathioprine, cyclosporine A, cyclophosphamide, rituximab, danazol, dapsone, mycophenolate mofetil, thrombopoeitin receptor agonists, or vinca alkaloids
Interventional ○ Splenic artery embolization
Surgical ○ Splenectomy
Platelet Transfusion in ITP
Controversial topic
No absolute contraindication
Generally ineffective(9,10)
Transfused platelets are vulnerable to the same destructive mechanisms as native platelets
Rarely results in significant post-transfusion increments
Potentially useful in the setting of life-threatening hemorrhage
Platelet Transfusion in ITP
Conventional wisdom regarding platelet
transfusion in ITP has recently been
challenged
Some studies have shown significant post-
transfusion increments in ITP patients(11)
Platelet transfusion, when given
concurrently with immunosupression, may
effectively control bleeding(12)

Our Patient
Platelet transfusion was initiated in an attempt to stabilize the ICH, while hopefully increasing platelet count to a level where splenectomy would be a safe option Plt goal = 50x103/µL
○ *per surgeon request
Initial bolus platelet infusions were ineffective ○ Maximum uncorrected increment 2x103/µL
○ Maximum corrected count increment 1104 m2/µL
Platelet drip started with three initial goals 1. Provide a steady stream of platelets in the hopes that some
would reach the bleeding sites and stabilize the ICH
2. Minimize donor exposure in a patient requiring serial transfusions
3. Manage platelet supply in the blood bank of a hospital that is a level 1 trauma center and has an active cardiothoracic/vascular surgery service
Our Patient
Platelet drip in combination with immunosuppression worked! ICH stabilized
Platelet count increased, allowing for a safe surgery
Platelet count rose in excess of the stated goal (50x103/µL) Peaks ranged from 73x103/µL to 172x103/µL
○ Remained elevated as long as the platelet drip continued
Platelet count plummeted when the drip was stopped Bottomed out at 3x103/µL to 9x103/µL
Significant recovery occurred only when the drip was re-initiated

Our Patient: Response to Platelet Drip

Our Patient
Why did the platelet drip work? Perhaps duration of platelet transfusion is more
important than volume of platelets transfused ○ PLADO study(13)
In the setting of prophylactic platelet transfusion for patients with hypo-proliferative thrombocytopenia, there was no significant difference in bleeding risk, regardless of the dose of platelets transfused.
- Low
- Intermediate
- High
○ Platelet drip use has been proposed for prophylactic and therapeutic use in thrombocytopenic patients with non-immunologic platelet refractoriness(14,15)
Efficacy confined to isolated case reports
Conclusions
In ITP patients with severe persistent thrombocytopenia despite aggressive medical therapy, alternative treatments should be considered Especially in the presence of clinically significant or
potentially life-threatening bleeding
Conventional wisdom regarding platelet transfusion in ITP should be reconsidered
The use of platelet drip in patients with ITP resistant to conventional therapy needs further investigation
○ Randomized, controlled, prospective trials are needed to validate platelet drip as a potential treatment modality
Long Term Follow-Up
@ 1 week Platelet count 15-16x103/µL
Epistaxis
@ 2 months Platelet count 185x103/µL
@ 2.5 months MRSA abscess at site of
surgical excision
@ 5 months Platelet count 635x103/µL
@ 8 months Platelet count 100x103/µL
○ Likely chronic ITP
○ Interval development of psychiatric symptoms Self-mutilation and
insomnia
@ 11 months Platelet count 123x103/µL
@ 13 months Platelet count 105x103/µL
Began danazol wean
@15.5 months Danazol stopped
@16 months Platelet count 67x103/µL
Continued azothiaprine

References 1. Rodeghiero FR, Gernsheimer ST, Michel M, Provan D, Arnold DM, Bussel
JB, Cines DB, Chong BH, Cooper N, Godeau B, Lechner K, Mazzucconi MG, McMillan R, Sanz MA, Imbach P, Blanchette V, Kuhne T, Ruggeri M, George JN. Standardization of Terminology, Definitions and Outcome Criteria in Immune Thrombocytopenic Purpura of Adults and Children: Report from an International Working Group. Blood 2009; 113.11: 2386-93.
2. Chang, M. Immune Thrombocytopenic Purpura (ITP) Plasma and Purified ITP Monoclonal Autoantibodies Inhibit Megakaryocytopoiesis in Vitro. Blood 2003; 102.3: 887-95.
3. McMillan, R. Suppression of in Vitro Megakaryocyte Production by Antiplatelet Autoantibodies from Adult Patients with Chronic ITP. Blood 2003; 103.4: 1364-9.
4. Olsson B, Andersson PO, Jernås M, Jacobsson S, Carlsson B, Carlsson LMS, Wadenvik H. T-cell-mediated Cytotoxicity toward Platelets in Chronic Idiopathic Thrombocytopenic Purpura. Nat Med 2003; 9.9: 1123-4.
5. Bergmann AK, Grace RF, Neufeld EJ. Genetic Studies in Pediatric ITP: Outlook, Feasibility, and Requirements. Ann Hem 2010; 89.S1: 95-103.
6. Neylon AJ, Saunders PWG, Howard MR, Proctor SJ, Taylor PRA. Clinically Significant Newly Presenting Autoimmune Thrombocytopenic Purpura in Adults: A Prospective Study of a Population-based Cohort of 245 Patients. Br J Haem 2003; 122.6: 966-74.
7. Roganovic J, Kalinyak K. Intracranial Hemorrhage in Children with Idiopathic Thrombocytopenic Purpura. Pediatr Int 2006; 48.5: 517.

References 8. Provan D, Stasi R, Newland AC, Blanchette VS, Bolton-Maggs P, Bussel JB, Chong
BH, Cines DB, Gernsheimer TB, Godeau B, Grainger J, Greer I, Hunt BJ, Imbach PA, Lyons G, McMillan R, Rodeghiero F, Sanz MA, Tarantino M, Watson S, Young J, Kuter DJ. International consensus report on the investigation and management of primary immune thrombocytopenia. Blood 2010;115:168-86.
9. Roback JD, Grossman BJ, Harris T, Hillyer CD. Hemotherapy Decisions and Their Outcomes. Technical Manual. 17th ed. Bethesda, MD: AABB, 2011. 588.
10. AABB, American Red Cross, and America’s Blood Centers. Circular of information for the use of human blood and blood components. Bethesda, MD: AABB, 2009.
11. Carr JM, Kruskall MS, Kaye JA, and Robinson SH. Efficacy of Platelet Transfusions in Immune Thrombocytopenia. Am J Med 1986; 80.6: 1051-4.
12. Bussel JB, Kunicki, TJ, Michelson, AD. Platelets: New understanding of platelet glycoproteins and their role in disease. Am Soc Hem 2000; 2000: 222-40.
13. Slichter SJ, Kaufman RM, Assmann SF, McCullough J, Triulzi DJ, Strauss RG, Gernsheimer TB, Ness PM, Brecher ME, Josephson CD, Konkle BA, Woodson RD, Ortel TL, Hillyer CD, Skerrett DL, McCrae KR, Sloan SR, Uhl L, George JN, Aquino VM, Manno CS, McFarland JG, Hess JR, Leissinger C, Granger S. Dose of Prophylactic Platelet Transfusions and Prevention of Hemorrhage. N Eng J Med 2010; 362.7: 600-13.
14. Tormey CA, Champion M, Ross R, Neal Z, Wu Y, Snyder EL. Outcome in thrombocytopenic patients with non-immunologic platelet refractoriness managed with continuous platelet infusion (platelet drip). Transfusion 2005; 45 Supplement 140A-141A.
15. Slichter, SJ. Platelet transfusion therapy. Hematol Oncol Clin N Am 2007; 21: 697-729.


















