Bree Collaborative Meeting · Bree collaborative to support collaborative learning and ... Removed...
79
Bree Collaborative Meeting November 20 th , 2019 | Puget Sound Regional Council
Transcript of Bree Collaborative Meeting · Bree collaborative to support collaborative learning and ... Removed...

Bree Collaborative Meeting
November 20th, 2019 | Puget Sound Regional Council

Agenda
Welcome and IntroductionsChair Report and Meeting Minutes
Action Item: Approve minutes
Implementation: 2020 and 2021Final Adoption: Shared Decision Making
Action Item: Adopt
Final Adoption: Palliative Care Action Item: Adopt
BREAKPresentation for Public Comment: Risk of Violence to Others
Action Item: Disseminate for Public Comment
Presentation for Public Comment: Maternity Bundle Action Item: Disseminate for Public Comment
Workgroup Update: Opioid Prescribing Next Steps and Close Slide 2

September 18th Meeting Minutes
Slide 3

Implementation: 2020 and 2021
Ginny Weir, MPHDirector, Bree Collaborative
November 20th, 2019 | Bree Collaborative Meeting
Implementation Funding ESHB 1109
(31) $300,000 of the general fund—state appropriation for fiscal year 2020 and $300,000 of the general fund—state appropriation for fiscal year 2021 are provided solely for the Bree collaborative to support collaborative learning and targeted technical assistance for quality improvement initiatives. The collaborative must use these amounts to hire one full-time staff person to promote the adoption of Bree collaborative recommendations and to hold two conferences focused on the sharing of best implementation practices.
Slide 5

23 sets of recommendations + 5 being finalized
Pain (Chronic and Acute) Collaborative care for chronic pain (2018) Low back pain management (2013) Opioid prescribing metrics (2017) Opioid prescribing for postoperative pain (2018) Opioid prescribing in dentistry (2017) Long-term opioid prescribing management
(2019) Behavioral Health
Integrating behavioral health into primary care (2016)
Addiction and substance use disorder screening and intervention (2014)
Suicide care (2018) Treatment for opioid use disorder (2016) Prescribing antipsychotics to children and
adolescents (2016) Risk of Violence to Others (2019)
Oncology Oncology care (2015) Prostate cancer screening (2015)
Slide 6
Procedural (surgical) Bundled payment models and warranties:
Total knee and total hip replacement (2013, re-review 2017)
Lumbar fusion (2014, re-review 2018) Coronary artery bypass surgery (2015)
Bariatric surgery (2016) Hysterectomy (2017) Data collection on appropriate cardiac
surgery (2013) Obstetrics
Obstetric care (2012) Maternity Bundle (2019)
Aging Advance care planning for the end-of-life
(2014) Alzheimer’s disease and other dementias
(2017) Palliative Care (2019) Hospital readmissions (2014) LGBTQ health care (2018) Shared Decision Making (2019)

Technical Assistance Plan
Primary Care Practice Behavioral Health Integration Initiative Pilot Group Target: Primary care practices Goal: Integration of behavioral health into primary care Intensity: High
Behavioral Health Integration Learning Community Target: Primary care practices Goal: Integration of behavioral health into primary care Intensity: Low
Health Plan Engagement Target: Medicaid Managed Care Plans, Commercial Health Plans Goal: Integration of behavioral health into primary care, value-based purchasing Intensity: Medium
Assessment: Delivery Systems and Health Plans Target: Hospitals, primary care practices, behavioral health, health plans Goal: All Bree Collaborative topics Intensity: Low
Value Based Payment Target: Hospitals and ambulatory surgical centers Goal: Use of bundled payment models Intensity: Medium Slide 7
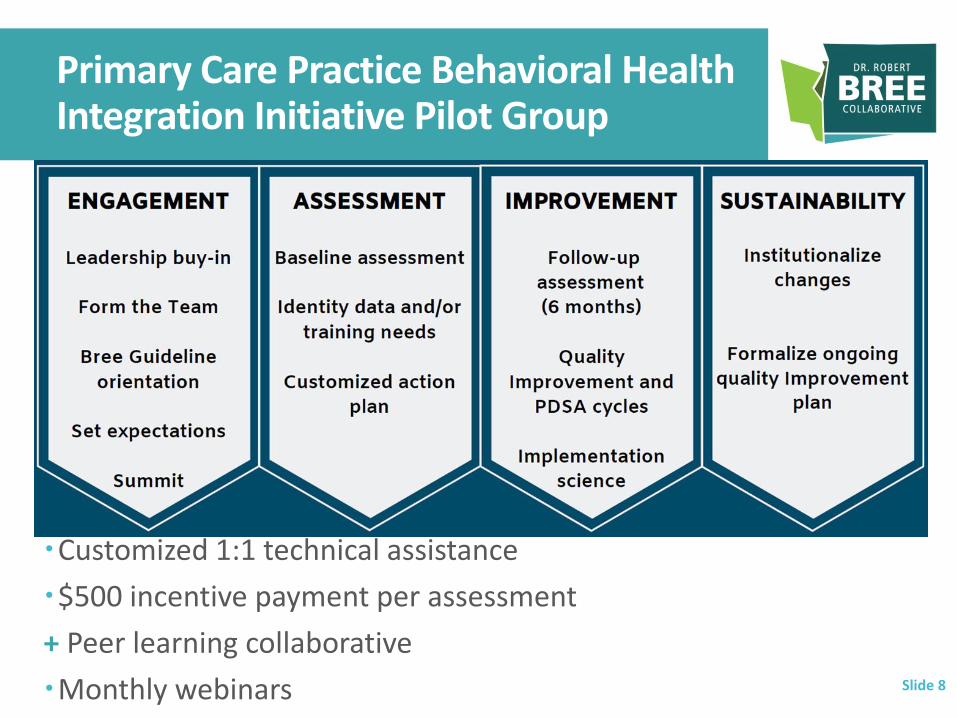
Primary Care Practice Behavioral Health Integration Initiative Pilot Group
Customized 1:1 technical assistance
$500 incentive payment per assessment
+ Peer learning collaborative
Monthly webinars Slide 8

Monthly Webinars + PortalFoster Peer-to-Peer Learning
January 29 – Intro, Welcome, Behavioral Health Integration
February 26 – Suicide Care
March 25 – Screening, Brief Intervention, Referral to Treatment
April 22 – Opioid Use Disorder
Slide 9

Save the Date
Slide 10
Bree Collaborative Implementation Summit
March 17th, 2020
SeaTac Airport Conference Center

2020 Topics
Reproductive HealthChair: Dr. Charissa Fotinos
Primary CareChair: Dr. Judy Zerzan
ChemotherapyChair: Dr. Hugh Straley
Colorectal Chair: Dr. Rick Ludwig
Slide 11

Final Adoption: Shared Decision Making
Emily Transue, MD, MHAAssociate Medical Director,Washington State Health Care Authority
November 20th, 2019 | Bree Collaborative Meeting

Workgroup Members
Chair: Emily Transue, MD, MHA, Associate Medical Director, Washington State Health Care Authority
David Buchholz, MD, Medical Director, Premera
Sharon Gilmore, RN, Risk Consultant, Coverys
Leah Hole-Marshall, JD, General Counsel and Chief Strategist, Washington Health Benefit Exchange
Steve Jacobson MD, MHA, CPC, Associate Medical Director, Care Coordination, The Everett Clinic, a DaVita Medical Group
Dan Kent, MD, Medical Director, United Health Care
Andrew Kartunen, Program Director, Growth and Strategy, Virginia Mason Medical System
Dan Lessler, MD, Physician Executive for Community Engagement and Leadership, Comagine Health
Jessica Martinson, MA, Director of Clinical Education and Professional Development, Washington State Medical Association
Karen Merrikin, JD, Consultant, Washington State Health Care Authority
Randy Moseley, MD, Medical Director, Quality, Confluence Health
Michael Myint, MD, Medical Director, Population Health, Swedish Hospital
Martine Pierre Louis, MPH, Director, Interpreter Services, Harborview Medical Center
Karen Posner, PhD, Research Professor, Laura Cheney Professor in Anesthesia Patient Safety, Department of Anesthesiology & Pain Medicine, University of Washington
Angie Sparks, MD, Family Physician and Medical Director, Clinical Knowledge Development, Kaiser Permanente of Washington
Anita Sulaiman, Patient Advocate Slide 13

Today’s Goal
Review public comments
Review changes to recommendations
Vote on final adoption
Slide 14

Public Comments
Slide 15

Changes Made
Added table comparing patient decision aids and patient education materials
Removed Venn Diagram
Made clear that perception shared decision making is already happening is barrier to use
Ten topic areas: Edited Cancer Screening to include breast, prostate,
colorectal, lung
Added herniated disk
Added steps to address common barriers to implementation for delivery organizations
Slide 16
Focus Areas
A common understanding and shared definition of shared decision making and the benefit of shared decision making.
Ten priority areas as an initial focus for the health care community.
Highly reliable implementation using an existing framework customized to an individual organization.
Documentation, coding, and reimbursement structure to support broad use.
Slide 17
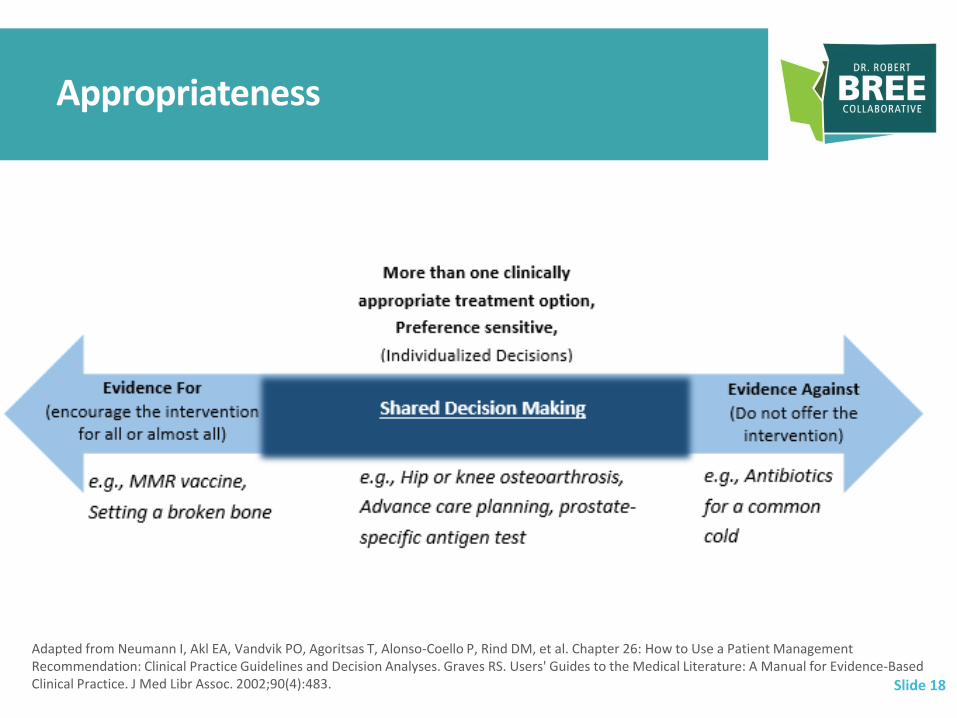
Appropriateness
Slide 18
Adapted from Neumann I, Akl EA, Vandvik PO, Agoritsas T, Alonso-Coello P, Rind DM, et al. Chapter 26: How to Use a Patient Management Recommendation: Clinical Practice Guidelines and Decision Analyses. Graves RS. Users' Guides to the Medical Literature: A Manual for Evidence-Based Clinical Practice. J Med Libr Assoc. 2002;90(4):483.

Workgroup Goal
State-wide movement toward greater use of shared decision making in clinical practice at a care delivery site and organizational level.
Stages of change frameworkPrecontemplationContemplationPreparationActionMaintance
Slide 19

Drivers of Shared Decision Making Implementation
Skills-based Education/Training
Patient Decision Aids
Patient/Family Engagement
Systems-Based
Slide 20

Selected Health Care Services
Surgical/Procedural: Knee and Hip Osteoarthritis (HCA certified)
Spine Surgery (HCA certified)
Abnormal Uterine Bleeding
Trial of Labor After Cesarean Section (HCA certified)
Herniated disk
Advanced Care Planning (HCA certified)
Cancer Screening (breast, prostate, colorectal, lung)
Behavioral health: Depression Treatment
Attention Deficit Hyperactivity Disorder Treatment
Opioid Use Disorder Treatment
Slide 21

Implementation Framework
National Quality Partner’s Playbook: Shared Decision Making in Healthcare = implementation fundamentals with basic, intermediate, advanced steps
Leadership and culture
Patient education and engagement
Healthcare team knowledge and training
Action and implementation
Tracking, monitoring and reporting
Accountability
The Agency for Healthcare Research and Policy (AHRQ) developed the SHARE (Seek, Help, Assess, Reach, and Evaluate) approach
Slide 22

Health Care Delivery Organizations and Systems
Slide 23
Stage of Change Steps
Precontemplation
Review your organization’s mission, vision, and values.
Define how shared decision making can help advance your organizational goals and align with
regional, state-wide, and Federal programs, expectations, and contracting.
Contemplation Define/select a framework with which to implement shared decision making.
Identify clinical champions who will be willing to help educate their peers, and administrative
champion to support necessary operational changes.
Select an appropriate training for your providers and staff about shared decision making.
Preparation Spread awareness about shared decision making broadly within your organization. Use the
definitions and materials within this report.
Work with your clinical champion(s) to educate providers about the value of shared decision
making and how to have a good conversation that uses the patient decision aid or references the
patient decision aid if the aid will be distributed to patients prior to the visit.
Select one of the 10 clinical areas to pilot (e.g., breast cancer screening).
Address common barriers to implementing patient decision aids with staff
Select a patient decision aid or aids to integrate into the care stream. If using a patient decision aid
that has not been certified by the HCA, the workgroup recommends using the IPDAS-based criteria
adapted by the HCA within Appendix G.

Health Care Delivery Organizations and Systems
Slide 24
Stage of Change
Steps
Preparation Define where in the care stream to use the aid (e.g., prior to visit via email).
Clearly identify roles for care team members. Non-clinical staff can have a shared decision making
conversation.
Providing templates for documentation of use of shared decision-making.
Conduct clinic- or system-wide training.
Action Implement your shared decision making pilot.
Implement performance metrics outlined on page 16.
Maintenance Evaluate use of the shared decision making process including feedback on the specific patient
decision aid.
Decide whether to change any components within the pilot if not working.
Spread to other sites or adopt shared decision making within another clinical area.
Review new evidence on a regular basis to update the shared decision making options based on the
most current evidence.

Health Plans and/or Professional Liability Carriers
Reimbursement
Value-based care standards
Metrics
Availability of patient decision aids
Prior authorization requirement
Continuing education
Discounts or other incentives
Documentation templates
Slide 25

Documentation, Coding, Reimbursement
Documented like any other clinical encounter
Some limited existing codes (e.g., G0296 Counseling)
Development of additional coding for added shared decision making reimbursement.
Prior authorization
Included as part of some alternative payment models (e.g., total joint replacement bundles)
Slide 26

Next Steps
Adopt Shared Decision Making Report and Recommendations
Slide 27
Final Adoption: Palliative Care
John Robinson, MD, SMChief Medical Officer, First Choice Health
November 20th, 2019 | Puget Sound Regional Council

Workgroup Members
Slide 29
Chair: John Robinson, MD, SM, Chief Medical Officer, First Choice Health Lydia Bartholomew, MD, Senior Medical Director, Pacific Northwest, Aetna George Birchfield, MD, Inpatient Hospice, EvergreenHealth Raleigh Bowden, MD, Director, Okanogan Palliative Care Team Mary Catlin, MPH, Senior Director, Honoring Choices, Washington State Hospital Association Randy Curtis, MD, MPH, Director, Cambia Palliative Care Center of Excellence, University of Washington Medicine Leslie Emerick, Director of Public Policy, WA State Hospice & Palliative Care Organization Ross Hayes, MD, Palliative Care Program, Bioethics, Rehabilitation, Pediatrician, Seattle Childrens Greg Malone, MA, MDiv, BCC, Palliative Care Services Manager, Swedish Medical Group Kerry Schaefer, MS, Strategic Planner for Employee Health, King County Bruce Smith, MD, Medical Director of Providence Hospice of Seattle, Providence Health and Services Richard Stuart, DSW, Psychologist, Swedish Medical Center - Edmonds Campus Stephen Thielke, MD, Geriatric Psychiatry, University of Washington Cynthia Tomik, LICSW, Manager, Palliative Care, Evergreen Health Gregg Vandekieft, MD, MA, Medical Director for Palliative Care, Providence St. Peter Hospital Hope Wechkin, MD, Medical Director, Hospice and Palliative Care, EvergreenHealth

Today’s Goal
Review public comments
Review changes to recommendations
Vote on final adoption
Slide 30

Public Comments
Slide 31

Changes Made
Added “or similar suitable document” to Physician Orders for Life-Sustaining Treatment (POLST)
Removed “pain” as the example of symptoms needing palliative care
Adding language to communicate within state agencies, with the Legislature, or other stakeholders
Listing services for health plans to include as part of palliative care
Red flags or warning signs
Adding clarity in when to refer
Adding resources available in the community as part of goals of care conversations
Adding more information in the appendix about California Palliative Care legislation and operationalizing
Slide 32
Focus Areas
Defining palliative care using the standard definition developed by the National Consensus Project including appropriateness of primary and specialty palliative care.
Spreading awareness of palliative care.
Clinical best practice provisions of palliative that are: Responsive to local cultural needs
Includes advance care planning
Incorporates goals of care conversations into the medical record and plan of care
Availability of palliative care through revision of benefit structure such as a per member per month (PMPM) benefit. Slide 33

Definitions
Serious illness is a condition that “negatively impacts quality of life and daily function, and/or is burdensome in symptoms, treatments, or caregiver stress… [and] carries a high risk of mortality.”
Source: Kelley AS. Defining "serious illness". J Palliat Med. 2014 Sep;17(9):985.
Source: National Consensus Project for Quality Palliative Care. Clinical Practice Guidelines for Quality Palliative Care, 4th edition. Richmond, VA: National Coalition for Hospice and Palliative Care; 2018. www.nationalcoalitionhpc.org/ncp. Slide 34
Time
“focuses on expert assessment and management of…symptoms, assessment and support of caregiver needs, and coordination of care [attending] to the physical, functional, psychological, practical, and spiritual consequences of a serious illness. It is a person- and family-centered approach to care, providing people living with serious illness relief from the symptoms and stress of an illness.”

The power of metaphor
Weir Slide 35

Primary and Specialty Palliative Care
Primary palliative care Delivered within primary care and relevant sub-specialty care
Meets physical, functional, psychological, practical, and spiritual consequences of a serious illness
Refer patients to specialty palliative care when needs cannot be met
Specialty palliative care Interdisciplinary team
Includes or has access to a care coordination function and is able to meet medical, psychological, and spiritual care needs
Access (e.g., telemedicine) to 24/7 specialty expertise highly recommended
Slide 36
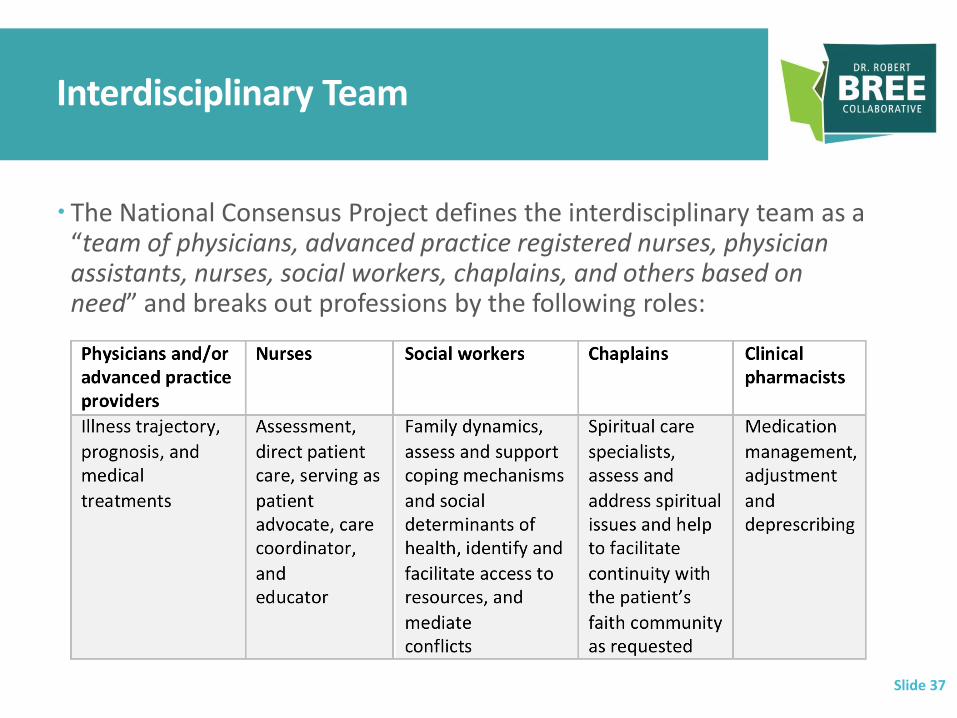
Interdisciplinary Team
The National Consensus Project defines the interdisciplinary team as a “team of physicians, advanced practice registered nurses, physician assistants, nurses, social workers, chaplains, and others based on need” and breaks out professions by the following roles:
Slide 37

Initial Assessment and Ongoing Assessment and Management
Goals of care conversations including around hospitalization
Advance care planning
Cognitive impairment
Functional needs
Symptom management and medical care
Pharmacy management
Caregiver needs
Behavioral health and psychosocial (i.e., depression, anxiety, suicidality, others)
Spiritual care needs
Care Coordination
Urgent Issues Slide 38

Benefit Structure
A per member per month (PMPM) palliative care benefit for seriously ill patients
Open to all ages
Follows a patient across care settings (e.g., if hospitalized)
Does not require the patient to be homebound or to stop curative or disease modifying therapy
Setting the of provision of specialty palliative care services (e.g., hospital) as the accountable entity
Slide 39

Benefit Structure
Identification: Develop an agreed-upon strategy to identify seriously ill patients (e.g., such as with the PACSSI Eligibility and Tiering Criteria outlined in Appendix D).
Interdisciplinary: Require an interdisciplinary approach to care that does not require a physician to lead the interdisciplinary team.
Payment structure: Offer a larger payment for the initial intake visit, a PMPM payment, and a smaller per-in-person visit payment.
Services: Palliative care should include the following services (outlined in more detail on the following pages):
An initial assessment Goals of care conversation(s) Advance care planning Assessment of cognitive impairment Assessment and management of functional needs Assessment and management of symptoms/medical care Pharmacy management Caregiver support, if needed Assessment and management of behavioral health/psychosocial needs related to serious illness Spiritual care needs Other, as needed Ongoing management Define excluded services (e.g., hospitalizations for unrelated diagnoses)
Measure: Measure success using at least one metric related to (1) potentially avoidable complications and (2) patient-specific quality of life. See page 18 for options under each of these categories. Metrics may be tied to gainsharing. Slide 40

Stakeholder Groups
Washington State Health Care Authority and Department of Health
Health Plans
Health Care Purchasers (employers and union trusts)
Patients and Family Members
Specialty Palliative Care Teams
Primary Care Providers and Sub-specialty Providers
Health Systems
Slide 41

Next Steps
Adopt Palliative Care Report and Recommendations
Slide 42
Public Comment: Risk of Violence to Others
Kim Moore, MDAssociate Chief Medical Officer, CHI Franciscan
November 20th, 2019 | Puget Sound Regional Council

Workgroup Members
Slide 44
Chair: Kim Moore, MD, Associate Chief Medical Officer, CHI Franciscan Ann Allen, MSW, Member, National Association of Social Workers, Washington Chapter G. Andrew Benjamin, JD, PhD, ABPP, Clinical Psychologist, Affiliate Professor of Law, University of Washington Jason Fodeman, MD, Labor and Industries Jaclyn Greenberg, JD, LLM, Policy Director, Legal Affairs, Washington State Hospital Association Laura Groshong, LICSW, Clinical Social Work, Private Practice Ian Harrel, MSW, Chief Operating Officer, Behavioral Health Resources Katerina LaMarche, JD, Policy Analyst, Washington State Medical Association Kelli Nomura, MBA, Behavioral Health Administrator, King County Mary Ellen O'Keefe, ARNP, MN, MBA, Clinical Nurse Specialist - Adult Psychiatric/Mental Health Nursing; President Elect, Association of Advanced Psychiatric Nurse Practitioners Jennifer Piel, MD, JD, Psychiatrist, Department of Psychiatry, University of Washington Julie Rickard, PhD, Program Director, American Behavioral Health Systems – Parkside Samantha Slaughter, PsyD, Member, WA State Psychological Association Jeffery Sung, MD, Member, Washington State Psychiatric Association Amanda Ibaraki Stine, MFT, Member, Washington Association for Marriage and Family Therapists Marianne Marlow, MA, LMHC, Member, Washington Mental Health Counseling Association Adrianne Tillery, Harborview Mental Health and Addiction Services (Certified Counselor)

Background Volk v. DeMeerleer187 Wn.2d 241, 386 P.3d 254
This 2016 Washington State Supreme Court decision alters the scope of the ‘duty to warn or protect’.
now clearly applies to clinicians in voluntary inpatient and outpatient settings
persons to ‘warn or protect’ now includes those who are ‘foreseeable’ victims, not ‘reasonably identifiable’ victims subject to an actual threat
Source: www.phyins.com/uploads/file/Volk%20recs-FINAL.PDF
Slide 45

Legal Background
The current legal framework in Washington state makes the implementation of a mental health provider’s duty of care and duty to protect untenable.
In all likelihood, this environment will have negative downstream effects on the community.
However, these negative impacts to access and quality of care can be remedied with changes in the laws to reduce the ambiguity presented by the Volk decision and the conflicting laws as outlined on page 12.
Slide 46

Review Problem Statement, Aim, Purpose
Problem Statement
Patients may be reluctant to engage with health care providers about their violence risk.
Health care providers may be uncertain about how to meet their legal obligations.
Aim
To recommend evidence-based, clinical best practices for patients with risk of violence
Purpose
To recommend evidence-based, clinical best practices for:
assessing risk for violence
identifying risk factors for violence
reconciling the right to confidentiality, least restrictive environment, and the duty to protect
actions to take when there is a risk for violence concern
means for discharging patients based on treatment setting
record-keeping to decrease variation in practice patterns in these areas
Slide 47

Focus Areas
Identification of increased risk for violence
Further assessment of violence risk
Violence risk management
Protection of third parties
Slide 48

Identification of increased risk for violence
Screen all patients over 18 years for the following behavioral health conditions:
Depression
Suicidality
Alcohol misuse and drug use
For youth ages 14-18, use developmentally appropriate screening tools
Other observations that may increase risk for violence (e.g., acute agitation)
Screen for thoughts of doing physical harm to others
Past history of violent acts
Document identification in the record including low risk of violence to others
Slide 49

Further Assessment of Violence Risk
Historical risk and/or triggering factors (e.g., history of criminal acts)
Clinical risk factors (if not already identified previously)
Protective factors that may mitigate risk (e.g., community and family ties)
Other relevant psychiatric symptoms or warning signs at clinician’s discretion (e.g., texting, stalking)
If appropriate, arrange for a second opinion risk assessment
If appropriate for further assessment, use a validated instrument (e.g., Historical Clinical Risk Management-20)
Training
Developmentally appropriate
Document results in the health recordSlide 50
Violence Risk Management
Match level of risk for violence with management plan.
If patient in acute crisis or acutely agitated, first ensure personal safety
Evidence-based treatment plan, if present, including medication, if indicated.
Consultation
Additional management strategies: More frequent visits.
Medication compliance/changes
Lethal means safety.
Involving others
Referral
Hospitalization
Addressing non-adherence
Addressing termination of therapeutic relationship
At each clinical decision point, document actions taken in the health record. Slide 51

Protection of Third Parties
If in an acute crisis, attempt to keep patient in an observed, safe, and appropriate environment
Consider voluntary admission
If needed, contact Designated Crisis Responder (DCR) for assessment for involuntary commitment.
If the provider decides that issuing a warning is needed, current law permits the clinicians to notify law enforcement before notifying potential victim(s). The clinician may follow RCW 70.02.230 as needed.
If needed and feasible, contact potential victim or victims including relatives, or parent or guardian if the potential victim is a minor, is a vulnerable adult, or has been adjudicated incompetent, employers, or household members of the patient, if reasonably identified.
At each decision point, document actions taken in the health record.
Slide 52
Recommendations to Washington State Legislature
While the recommendations included in this document are intended to provide an overview of best practices for clinical care, the recommendations exist in the context of significant legal ambiguities that undermine their implementation. In order to support Washington’s behavioral health professionals in caring for patients with elevated risk for violence and protecting third parties, the workgroup recommends that the legislature address Volk’s discrepancies with current law (RCWs 71.05.120, 70.02.050, and 70.02.230), and take action to create one uniform standard on the duties of mental health professionals to protect third parties from violent acts of patients to supersede Volk and apply regardless of treatment settings (e.g., including inpatient, outpatient, voluntary and involuntary) and to:
Clarify the scope of the duty to protect by specifying: The range of clinicians subject to the duty to protect, Conditions that trigger the duty to protect, Persons to whom the duty to protect is owed, Options for discharging the duty to protect.
Slide 53

Key Takeaway Points
Violent acts that harm others are of social and clinical significance
The majority of patients with mental health conditions do not engage in violent behavior
Substance use disorder more strongly associated with risk of violence, especially when present with a mental illness diagnosis
Clinicians cannot predict impending violent acts with certainty
Patient’s have a right to confidentiality and also to care in the least restrictive environment
Clinicians have a duty to protect the community
Clinicians can identify/assess/manage those at risk of violence
Clinicians cannot possibly warn all those who are ‘foreseeable’ victims, but are not ‘reasonably identifiable’ victims subject to an actual threat
Slide 54

Recommendation
Vote to disseminate for public comment
Slide 55

BREAK
56
Public Comment: Maternity Bundled Payment Model
Carl Olden, MDFamily Physician, Pacific Crest Family Medicine
November 20th, 2019 | Puget Sound Regional Council

Workgroup Members
Slide 58
Chair: Carl Olden, MD, Family Physician, Pacific Crest Family Medicine Andrew Castrodale, MD, Family Physician, Coulee Medical Center Angela Chien, MD, Obstetrics and Gynecology, EvergreenHealth Neva Gerke, LM, President, Midwives Association of Washington Molly Firth, MPH, Patient Advocate Lisa Humes-Schulz, MPA/Lisa Pepperdine, MD, Director of Strategic Initiatives/ Director of Clinical Services, Planned Parenthood of the Great Northwest and Hawaiian Islands Rita Hsu, MD, FACOG, Obstetrics and Gynecology, Confluence Health Ellen Kauffman, MD, Medical Director Emeritus, Obstetrics Clinical Outcomes Assessment Program Caroline Kline, MD, Obstetrics and Gynecology, Overlake Medical Center Dale Reisner, MD, Obstetrics and Gynecology, Swedish Medical Center Janine Reisinger, MPH, Director, Maternal-Infant Health Initiatives, Washington State Hospital Association Mark Schemmel, MD, Obstetrics and Gynecology, Spokane Obstetrics and Gynecology, Providence Health and Services Vivienne Souter, MD, Research Director, Obstetrics Clinical Outcomes Assessment Program Judy Zerzan, MD Chief Medical Officer Washington State Health Care Authority

Overview
Slide 59
Pre
nat
al C
are
270 days prior to delivery
Lab
or
and
Del
iver
y
Facility and Professional services
Po
stp
artu
m C
are
84 days post-delivery
Single Payment Ideal is to move to 365 days post delivery including pediatric care
Structure
Fee-for-service with retrospective reconciliation initially The workgroup recommends moving toward a prospective payment model
Exclude anesthesia, contraception, and genetic testing
Risk adjustment based on patient-specific factors
Including prenatal care, labor and delivery, postpartum services for both facility and professional services
Obstetric care provider or group is the accountable entity
Exclusion criteria: Age: younger than 16, older than 40 Cost below first percentile or higher than ninety-ninth percentile Diagnoses within the episode window or 90 prior to or after episode window as
determined by the payer or purchaser based on high-cost claims. See Appendix D for Exclusion criteria examples. The workgroup does not recommend basing exclusion criteria on behavioral health diagnoses including substance use disorder or drug use and/or body mass index (BMI).
Death within episode windowSlide 60

Care PathwayPrenatal Care
Intake visit as soon as possible after a patient contacts the provider or group with a positive pregnancy test. At a minimum, the intake visit should happen in the first trimester. (e.g., insurance, nutrition, dating ultrasound, behavioral health screenings)
At a minimum, monthly visits up to 28 weeks gestation at minimum
At a minimum, biweekly visits up to 36 weeks gestation at minimum.
Content: Cardiovascular disease Behavioral Health Screening Infectious Disease Screening Gestational Diabetes Screening Vaccination Third trimester education (e.g., breastfeeding, birth spacing, shared decision
making as appropriate) Social Determinants of Health
Slide 61

Care PathwayLabor Management and Delivery
Emphasizing a physiologic birth when safe (e.g., spontaneous onset and progression of labor, vaginal birth of the infant and placenta)
Shared decision making, where appropriate
Endorse standards within the Washington State Hospital Association Labor Management Bundle
2012 Bree Collaborative Obstetric guidelines
Comprehensive, client-centered contraceptive counseling (including LARC)
Slide 62

Care PathwayPostpartum Care
At least two visits with additional visits as needed (e.g., if higher-risk) Three weeks postpartum visit
Additional comprehensive visit prior to 12 weeks postpartum including
Assessment of mood and emotional well-being including screening with a validated tool for depression (e.g., PHQ-9, Edinburgh Postnatal Depression Scale), anxiety (e.g., GAD), suicidality, and tobacco, alcohol, marijuana, and other drug use.
Sexuality including contraception
Infant care and feeding including breastfeeding
Sleep and fatigue
Patient support
Postpartum discharge summary
Connection to primary care Slide 63

Other stakeholder groups
Health Care Purchasers (Employers and Union Trusts) Investigate moving to value-based reimbursement in partnership with other
purchasers such as the Washington State Health Care Authority. High-deductible health plans = moving the deductible above a specified
allowance for the perinatal episode.
Emergency Department and Urgent Care Cardiovascular Disease. Assess all women of childbearing age for recent
pregnancy and last menstrual period. Women may be at higher risk for cardiovascular disease up to five months postpartum and may present with shortness of breath, chest pain, unresolved cough or swelling.
Department of Health Link the gestational parent’s member ID and newborn ID. Resources around social determinants of health
Washington State Health Care Authority Extend Washington State Medicaid eligibility to 12 months (365 days)
postpartum at the same income level as for pregnancy.
Slide 64
Quality Metrics
Reflect clinical priorities, process and outcome, balance w/ unexpected outcomes
Overall cost
PC-O2 Cesarean Section
Chlamydia Screening
Group B Streptococcus Screening
Postpartum Visit Scheduled
Behavioral Health Risk Assessment
PC-O6 Unexpected Complications in Term Newborns
O1: Severe Maternal Morbidity
Slide 65

Recommendation
Vote to disseminate for public comment
Slide 66
Workgroup Update: Opioid Prescribing: Long-Term Opioid Therapy
Gary Franklin, MD, MPHMedical Director, Washington State Department of Labor and Industries
November 20th, 2019 | Bree Collaborative Meeting

Workgroup Members
Co-Chair: Gary Franklin, MD, MPH, Medical Director, Washington State Department of Labor and Industries
Co-Chair: Charissa Fotinos, MD, Deputy Chief Medical Officer, Washington State Health Care Authority
Co-Chair: Andrew Saxon, MD, Director, Center of Excellence in Substance Abuse Treatment and Education (CESATE), VA Puget Sound Health Care System
Rose Bigham and Cyndi Hoenhous, Co-chairs, Patient Advocates Washington Patients in Intractable Pain
Malcolm Butler, MD Chief Medical Officer Columbia Valley Community Health Pamela Stitzlein Davies, MS, ARNP, FAANP Nurse Practitioner Departments of Neurology & Nursing,
University of Washington Jason Fodeman, MD, Washington State Department of Labor and Industries Andrew Friedman, MD Physical Medicine and Rehabilitation Virginia Mason Medical Center Kelly Golob, DC Chiropractor Tumwater Chiropractic Center Dan Kent, MD Chief Medical Officer UnitedHealthcare Kathy Lofy, MD Chief Science Officer Washington State Department of Health Jaymie Mai, PharmD Pharmacy Manager Washington State Department of Labor and Industries Joseph Merrill, MD, MPH Associate Professor of Medicine University of Washington Anne Blake-Nickels Patient Advocate Gregory Rudolph, MD Addiction Medicine Swedish Pain Services Jennifer Davies-Sandler Patient Advocate Mark Stephens President Change Management Consulting Mark Sullivan, MD, PhD Psychiatrist University of Washington David Tauben, MD Chief of Pain Medicine University of Washington Medical Center Gregory Terman MD, PhD Professor Department of Anesthesiology and Pain Medicine and the
Graduate Program in Neurobiology and Behavior, University of Washington John Vassall, MD, FACP Physician Executive for Quality and Safety Comagine Health Mia Wise, DO Medical Director, Collaborative Healthcare Solutions Premera Blue Cross Slide 68

GuidelinesBackground
Help primary care and other providers support patients in managing chronic pain
Follow National Pain Strategy: Patient-centered, accounting for individual preferences, risks, and social
contexts
Comprehensive, meeting biopsychosocial needs
Multimodal and integrated, using evidence-based treatments
Focus on goals of clinically meaningful improvement in function, as well as improved quality of life, and greater patient functional independence rather than on pain relief
Priority = safety and avoidance of serious adverse outcomes
Slide 69

Slide 70

Pain Rules (WAC)
Slide 71

GuidelinesFocus Areas
Patient Engagement and Support
Assessment
Develop a Treatment Plan Maintain and MonitorReduce Dosage
Transition to medication-assisted therapy
Delivery Systems and Health Plans
Slide 72
Patient Engagement
Discuss goals of care
Set expectations – safety while maximizing function
Assess knowledge about pain and medication(s), educate on knowledge gaps
Respect
Engage and educate others, where appropriate
Consistent messaging
Cultural competency Source: Wyse JJ, Ganzini L, Dobscha SK, Krebs EE, Morasco BJ. Setting Expectations, Following Orders, Safety, and Standardization: Clinicians' Strategies to Guide Difficult Conversations About Opioid Prescribing. J Gen Intern Med. 2019 Jul;34(7):1200-1206.Kennedy LC, Binswanger IA, Mueller SR, Levy C, Matlock DD, Calcaterra SL, Koester S, Frank JW. "Those Conversations in My Experience Don't Go Well": A Qualitative Study of Primary Care Provider Experiences Tapering Long-term Opioid Medications. Pain Med. 2018 Nov 1;19(11):2201-2211.Sullivan MD, Turner JA, DiLodovico C, D'Appollonio A, Stephens K, Chan YF. Prescription Opioid Taper Support for Outpatients With Chronic Pain: A Randomized Controlled Trial. J Pain. 2017 Mar;18(3):308-318.
Slide 73

Slide 74

Assessment
Patient history
Observation of the patient’s affect and behavior
Health record
Physical exam
Pain and functional status
Prescription Monitoring Program
Urine drug test
Co-occurring behavioral health conditions (i.e., depression, anxiety, suicidality, post-traumatic stress disorder, adverse childhood experiences, alcohol misuse, substance use)
Evaluate for opioid use disorderSlide 75
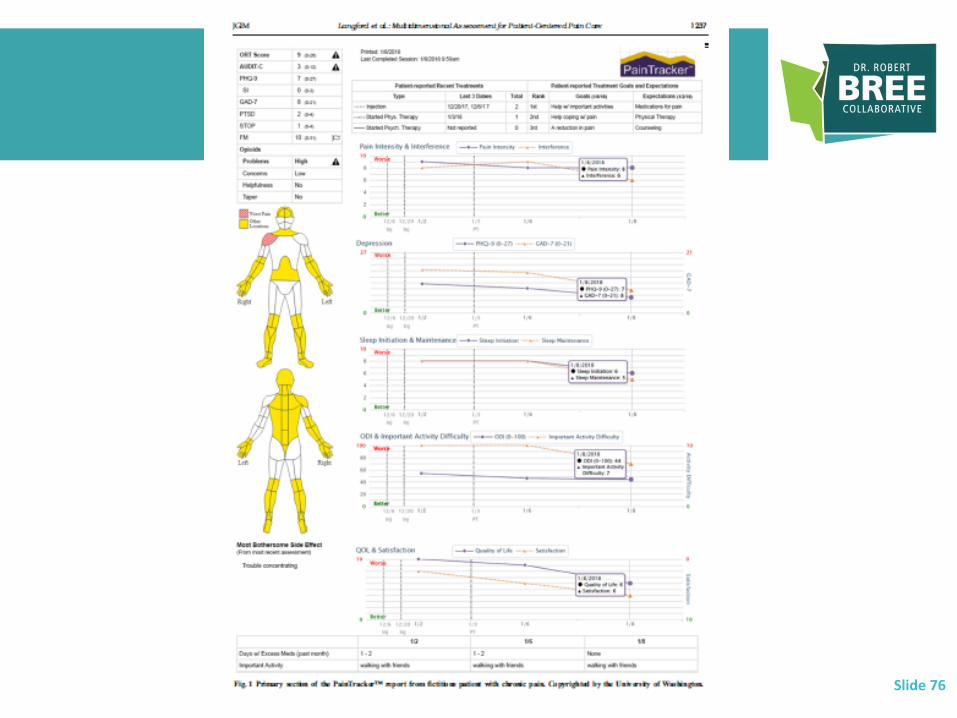
Slide 76

Develop a Treatment Plan
Referencing WAC (e.g., documentation)
Involve behavioral health providers, where possible
Use non-opioid pharmacological pain management
Use non-pharmacological pain management
Risks/benefits Maintain and Monitor
Periodic review as stated in WAC
Written agreement as stated in WAC
Tapering or Discontinuation -> HHS Guidelines
Medication-Assisted Treatment
Slide 77

Slide 78

Retreat:
Wednesday, January 15th, 202012:30 – 4:30
Puget Sound Regional Council5th Floor Board Room1011 Western Avenue, Seattle WA