Breast Augmentation: Choosing the Optimal Incision, Implant...
14
COSMETIC Breast Augmentation: Choosing the Optimal Incision, Implant, and Pocket Plane David A. Hidalgo, M.D. New York, N.Y. Summary: A retrospective study of 220 patients was performed to review surgical design in breast augmentation. Three specific issues were studied: incision site, implant variables, and pocket plane selection. The influence of these three factors on aesthetic results in both primary and secondary cases was the focus of the analysis. No attempt was made to address long-term issues such as capsular contracture or saline implant deflation rates. In 77 primary augmentation pa- tients and 80 unilateral augmentations for symmetry in breast reconstruction, there were the following untoward results: 11 revisions for unilateral malposi- tion, change to a different implant shape, or change to a larger implant size; four deflations of saline implants requiring replacement; and four conversions of saline to silicone gel implants. In 63 secondary cases, there were two hematomas and two infections requiring implant removal and subsequent replacement. Operative technique in breast augmentation is described, as are recommenda- tions for each of the options associated with the three variables studied. (Plast. Reconstr. Surg. 105: 2202, 2000.) T he design of breast augmentation procedures is almost entirely determined by three vari- ables: the selection of incision location, the pocket plane for implant placement (either subpec- toral or completely subglandular), and the appro- priate implant. Implant-related variables include size, shape, shell texture, filler substance, and final implant fill volume in the case of saline implants. There is no incontrovertible evidence that supports the superiority of one combination of choices over another. However, certain anatomic configurations in primary cases as well as certain problems pre- sented in secondary cases are best treated with a specific combination of options that may differ from a usual preferred approach. This study is a retro- spective review that seeks to establish the optimal indications for each of three variable options as they relate to specific types of augmentation problems. PATIENTS AND METHODS A total of 220 patients underwent breast aug- mentation between 1991 and 1998. This included 77 primary augmentations performed for aesthetic pur- poses, 80 unilateral augmentations performed as symmetry procedures in breast reconstruction, and 63 aesthetic augmentation patients who required secondary removal and replacement of breast im- plants. The follow-up period ranged from 1 month to 6 years. A meaningful average follow-up period was difficult to determine because many patients did not return for follow-up after several postoperative visits. Therefore, no attempt was made to determine overall patient satisfaction or the incidence of capsular contracture, topics that are not the focus of this study and have been reported elsewhere previously. 1–5 Operative Technique Preoperative preparation includes the admin- istration of intravenous antibiotics, padding, se- curing the head to stabilize the patient for sitting up later in the procedure, and securing the arms either abducted on armboards (transaxillary ap- proach) or taped across the lap (periareolar or inframammary incision approach). Monitored se- dation anesthesia is typically used. The intercostal nerves are individually blocked with 0.25% bupiv- acaine. Each of the lateral intercostal nerves as- sociated with ribs two through eight is injected at the lower edge of each rib, and also the interspace of ribs two through six approximately 1 cm lateral to the sternocostal junctions. A total of 30 to 40 cc is used. This nerve block is not difficult because these patients are usually thin and the landmarks From the Division of Plastic Surgery at Cornell University Medical College. Received for publication January 5, 1999; revised July 22, 1999. Reprinted and reformatted from the original article published with the May 2000 issue (Plast Reconstr Surg. 2000;105: 2202–2206). Copyright ©2012 by the American Society of Plastic Surgeons DOI: 10.1097/PRS.0b013e318269af42 www.PRSJournal.com 59S
Transcript of Breast Augmentation: Choosing the Optimal Incision, Implant...

COSMETIC
Breast Augmentation: Choosing the OptimalIncision, Implant, and Pocket Plane
David A. Hidalgo, M.D.
New York, N.Y.Summary: A retrospective study of 220 patients was performed to review surgicaldesign in breast augmentation. Three specific issues were studied: incision site,implant variables, and pocket plane selection. The influence of these threefactors on aesthetic results in both primary and secondary cases was the focusof the analysis. No attempt was made to address long-term issues such as capsularcontracture or saline implant deflation rates. In 77 primary augmentation pa-tients and 80 unilateral augmentations for symmetry in breast reconstruction,there were the following untoward results: 11 revisions for unilateral malposi-tion, change to a different implant shape, or change to a larger implant size; fourdeflations of saline implants requiring replacement; and four conversions ofsaline to silicone gel implants. In 63 secondary cases, there were two hematomasand two infections requiring implant removal and subsequent replacement.Operative technique in breast augmentation is described, as are recommenda-tions for each of the options associated with the three variables studied. (Plast.Reconstr. Surg. 105: 2202, 2000.)
The design of breast augmentation proceduresis almost entirely determined by three vari-ables: the selection of incision location, the
pocket plane for implant placement (either subpec-toral or completely subglandular), and the appro-priate implant. Implant-related variables includesize, shape, shell texture, filler substance, and finalimplant fill volume in the case of saline implants.There is no incontrovertible evidence that supportsthe superiority of one combination of choices overanother. However, certain anatomic configurationsin primary cases as well as certain problems pre-sented in secondary cases are best treated with aspecific combination of options that may differ froma usual preferred approach. This study is a retro-spective review that seeks to establish the optimalindications for each of three variable options as theyrelate to specific types of augmentation problems.
PATIENTS AND METHODSA total of 220 patients underwent breast aug-
mentation between 1991 and 1998. This included 77
primary augmentations performed for aesthetic pur-poses, 80 unilateral augmentations performed assymmetry procedures in breast reconstruction, and63 aesthetic augmentation patients who requiredsecondary removal and replacement of breast im-plants. The follow-up period ranged from 1 monthto 6 years. A meaningful average follow-up periodwas difficult to determine because many patients didnot return for follow-up after several postoperativevisits. Therefore, no attempt was made to determineoverall patient satisfaction or the incidence of capsularcontracture, topics that are not the focus of this studyand have been reported elsewhere previously.1–5
Operative TechniquePreoperative preparation includes the admin-
istration of intravenous antibiotics, padding, se-curing the head to stabilize the patient for sittingup later in the procedure, and securing the armseither abducted on armboards (transaxillary ap-proach) or taped across the lap (periareolar orinframammary incision approach). Monitored se-dation anesthesia is typically used. The intercostalnerves are individually blocked with 0.25% bupiv-acaine. Each of the lateral intercostal nerves as-sociated with ribs two through eight is injected atthe lower edge of each rib, and also the interspaceof ribs two through six approximately 1 cm lateralto the sternocostal junctions. A total of 30 to 40 ccis used. This nerve block is not difficult becausethese patients are usually thin and the landmarks
From the Division of Plastic Surgery at Cornell UniversityMedical College.Received for publication January 5, 1999; revised July 22,1999.Reprinted and reformatted from the original article publishedwith the May 2000 issue (Plast Reconstr Surg. 2000;105:2202–2206).Copyright ©2012 by the American Society of Plastic Surgeons
DOI: 10.1097/PRS.0b013e318269af42
www.PRSJournal.com 59S

easily palpable. It contributes significantly to thepatient’s comfort postoperatively. The incision,the inframammary crease, and the soft tissue inthe region of the inferomedial origin of the pec-toralis major muscle are injected with 1% lido-caine with epinephrine.
After the incision is made and the pocket de-veloped, the patient is placed in a sitting position,and a saline sizer is inserted. A sizer is critical toaccurately determine the proper implant size.There is usually a narrow volume range thatachieves the desired aesthetics, and this is estab-lished by adjusting the sizer volume and observingthe effect. Exceeding the range that provides ad-equate augmentation without distortion results ina less natural appearance. Distortion results froma combination of excessive volume for chest andoverall patient proportions, excessive implant di-ameter, and convex upper pole shape (Fig. 1).Selecting the corresponding implant size in thecase of silicone gel implants must be precise be-cause of the fixed size of these devices. Selectingthe most appropriate saline implant size shouldtake into account whether or not filling the im-plant beyond its stated shell size is desired. In verythin individuals, round saline implants can beused with minimal rippling if they are “overfilled”as much as 15 percent higher than the stated im-
plant size (Fig. 2). This is the maximum amountthat will not cause the implant shape to be con-spicuous or its consistency too firm. The implantsize selected should take into account the amountof “overfill” desired so that the final volume ap-proximates closely the sizer-determined volume.Shaped implants become even less “anatomic”with overfill and resemble more a lozenge than a“teardrop.” Therefore, they should be filled be-yond their stated shell size more conservatively ifat all. Final fill volume with implants used forcombined augmentation and mastopexy is lesscritical because these patients typically haveenough native breast tissue to hide the implantwell even if filled to less than the stated implantshell size.
The medial aspect of the pocket is developedas much as desired before the lateral aspect isenlarged. The latter is generally done conserva-tively to prevent lateralization of the implants.Subpectoral implant placement requires partialdetachment of the pectoralis major origin. This isusually limited to the inferomedial aspect of themuscle. Excessive detachment superiorly can con-tribute to symmastia or dimpling of the overlyingskin with muscle contraction.
Placement of the implants usually requireslowering the inframammary crease. The crease
Fig. 1. Implant size (diameter) and fill volume are key determinants of breast appearance. (Left) Anatural result with a flat upper pole was achieved by a modest submuscular augmentation usingsmooth-shell 200 cc round implants filled to 210 cc on both sides. Preexisting breast volume esti-mated at 80 to 100 g. (Right) A distorted and unnatural appearance is seen in this patient who hadapproximately 75 g of breast tissue preoperatively. Implant diameter is excessive and contributesto a tight appearance with a convex upper pole. Textured-shell 360 cc saline implants were usedwith a final fill volume of 390 cc.
Plastic and Reconstructive Surgery • Fall 2012
60S

should always be lowered enough so that the hor-izontal midaxis of the implant is centered on thenipple. It is obvious that the larger the implant di-ameter the more the crease will have to be lowered.Lowering the crease excessively to accommodate anoverly large implant makes inframammary creaseasymmetry or a “double-bubble” deformity more
likely to occur. Therefore, this should be taken intoconsideration in determining the best implant sizeand volume for a particular situation. An inframam-mary crease that is inadvertently lowered too muchduring a transaxillary approach can be correctedimmediately by placing an external bolster suture(s)at the appropriate level while manually displacing
Fig. 2. Transaxillary submuscular breast augmentation in the extremely thin patient.Smooth-shell 250 cc round saline implants were placed with a final fill volume of 288 cc onboth sides. A guideline of 15 percent volume overfill is reliable to provide maximum protec-tion against postoperative rippling while retaining reasonably soft breast consistency. Thispatient subsequently requested an exchange for silicone gel implants, which did not yield asignificantly different result.
Volume 130, Number 5S-3 • Breast Augmentation
61S

the implant superiorly. This type of suture shouldinclude the deep soft tissue of the chest wall and isleft in place for as long as 2 weeks postoperatively.
Antibiotics are placed in the implant but ste-roids are not.6 The implant is rinsed with dilutebetadine before insertion.7 A closed system of fluidadministration is used to fill the implants.
Certain adjunctive procedures are helpful tofurther improve aesthetic results. These includenipple reduction and adjustment of areolar diam-eter. Nipple reduction can be accomplished eitherby excising skin circumferentially as much as 50percent of the nipple height. Simply closing the
resultant defect decreases nipple projection. Nip-ples that are prominent and wide can be reducedby partial vertical excision. Patients must be ad-vised about the possible impact on sensation ofthese techniques, although clinical experiencehas shown little adverse effect. Areolar diametercan be reduced by intra-areolar excision. However,circumareolar scars are an even trade at best forareolar diameter reduction, and this method is notrecommended for routine use. It is best reserved forunilateral application in the rare case where there isa considerable side-to-side diameter discrepancy.Skin excisions that are less than 1 cm wide around
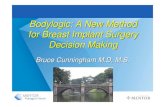
Fig. 3. Circumareolar skin excision with and without mastopexy as an adjunct in breast augmen-tation. (Above) Areolar repositioning was not elected in this patient who preferred mild asymmetryand ptosis to additional scars. Indications for mastopexy in borderline cases should be conserva-tive, as most patients seem indifferent to areolar position asymmetry in the absence of true ptosisof the gland. (Below) Circumareolar skin excision of 5 cm in diameter was designed on the right sideto raise the areolar position. It was combined with excision of 20 g of periareolar breast tissue in thiscase of mild tubular breast formation.
Plastic and Reconstructive Surgery • Fall 2012
62S

the circumference of the areola usually are associ-ated with excellent quality scars. Circumareolar skinexcision, possibly combined with intra-areolar exci-sion, is useful in cases of tubular breast hypomastiawhere there is considerable pseudoherniation ante-riorly with prominence of the areola and associatedgland ptosis. In cases of either circumareolar or in-tra-areolar excision, a pursestring suture of nonab-sorbable material such as 2-0 clear nylon on a Keithneedle (Ethicon) is recommended to stabilize thedecreased areolar diameter.
Position asymmetry of the areolae is commonpreoperatively, and the placement of breast implantsoften magnifies any preexisting discrepancy follow-ing augmentation. The breast implants should al-ways be placed symmetrically, even though the are-olar position may be different on each side. Mostpatients tolerate naturally occurring asymmetrywithout concern so that correction, with its atten-dant scars, should not be advocated unless the de-gree of asymmetry is expected to be considerable(Fig. 3). It is possible to raise the areolar positionslightly with a vertically eccentric skin excision de-sign, although it becomes more challenging to pre-cisely control areolar shape as the perpendiculardiameters of the skin excision design increasinglydiffer. More significant areolar position issues suchas ptosis may require concurrent mastopexy, a pro-cedure beyond the scope of this discussion.
Postoperatively, it has proved useful in cases ofsubmuscular augmentation to have the patientwear an adjustable strap across the upper pole ofthe breasts for as long as 6 weeks (Fig. 4). Thisprevents upward migration of the implants andensures that the lowered inframammary creaseremains at the desired height. This practice is mosthelpful in the case of transaxillary augmentationand should be used with caution when an infra-mammary incision has been used. The strap ten-sion may require adjustment, and the patientshould be seen at appropriate intervals to monitorimplant position and strap tension. Patients arenot instructed to massage the implants.
RESULTSThe most common options selected for primary
augmentation (both aesthetic and reconstructive) inthis study included transaxillary approach, submus-cular pocket plane, and smooth saline implants.Other combinations were far less common and wereselected according to the guidelines described be-low. The most common options selected for second-ary augmentation included periareolar incision, nochange in pocket plane, and placement of texturedsilicone gel implants.
The significant number of secondary cases inthis study support the notion that breast augmen-tation patients frequently pursue revisional sur-gery with another surgeon. Therefore, accuratefollow-up of both primary and secondary cases isdifficult, and the results reported here are likely tounderestimate the true incidence of revisional sur-gery. The primary aesthetic breast augmentationpatient group included seven that required ad-justment of implant position on one side,3 changefrom round to shaped implant,1 or bilateral in-crease in implant size.3 There were four patientswho underwent exchange of implant(s) for pre-mature deflation of saline implants, all occur-ring within 3 years of placement. This includedone patient who had premature bilateral defla-tion of shaped implants with failure occurringat the superior-most aspect of the implant onboth sides. There were two patients augmentedwith saline implants that opted for replacementwith a silicone gel type. There were two primarycongenital asymmetry patients who chose tohave a second procedure years later for furtherimprovement. In the unilateral augmentationgroup for breast reconstruction, there were fourrevisions to further improve symmetry. Two pa-tients in this group also opted for exchange ofsaline implants for a silicone gel type. Therewere two hematomas requiring evacuation in
Fig. 4. Adjustable straps are useful postoperatively to preventupward migration of breast implants. They are indicated primar-ily in patients with submuscular implants placed through an ax-illary incision, although they are helpful in any patient in whomthe inframammary crease requires significant lowering.
Volume 130, Number 5S-3 • Breast Augmentation
63S

the secondary aesthetic group, and both oc-curred in patients where the pocket plane wasconverted from subglandular to subpectoral.Two secondary patients required removal of im-plants for infection with later replacement.
DISCUSSION
Incision SelectionIncision choices in breast augmentation in-
clude axillary, inframammary, periareolar, andmore recently, periumbilical. There are multiplefactors that influence incision selection (Table 1).Each patient presents with certain anatomicvariables that suggest one or more choices assuperior options. It is best not to rely rigidly onone incision type.
Periareolar incisions are the most versatile.They allow central access to the implant pocketand are compatible with either muscle plane andall types of implants. They are the best choicewhen it is necessary to lower the inframammarycrease considerably (Fig. 5). They are a logicalchoice when concurrent mastopexy may be re-quired but is not certain pre-operatively. In thesepatients, a sizer is typically placed and the breastshape previewed. This may prove to obviate theneed for additional incisions that a mastopexywould require, but if not, the periareolar incision
is simply incorporated into the design. A periareo-lar incision is also the best choice for cases oftubular breast hypomastia because it allows cir-cumareolar skin and parenchymal excision shouldthis prove necessary. It is the incision of choice insecondary procedures that require either capsu-lectomy and exchange of old implants or capsu-lorrhaphy to correct implant malposition. The fewcontraindications to a periareolar incision aresmall areolar diameter or a very light areolar colorwith indistinct margins. A variant of the periareo-lar scar method not commonly practiced is a smallincision at the base of the nipple. Although theremay be a scar-concealing advantage to this ap-proach, exposure is quite limited.
Inframammary crease incisions are popularand almost as versatile as periareolar incisions.They are an ideal choice in patients who havesignificant breast volume preoperatively and ex-hibit either postpartum atrophy or just glandularptosis (Fig. 6). These patients usually have a breastbase of appropriate diameter so that the incisionwill not end up displaced from the inframammarycrease following implant placement. In mostcases, the final scar is well concealed in a deepcrease below a slightly ptotic breast. This incisionis usually a secondary choice when the inframam-mary crease is either high or nonexistent. It is alsonot indicated in tubular breast hypomastia unless
Table 1. Incision Options*
Factor Axillary Periareolar Inframammary Periumbilical†
Implant planeSubmuscular � � � �Subglandular � � � �
Implant typeSaline round � � � �Saline shaped � � � �Silicone round/shaped � � � �
Preoperative breast volumeHigh (�200 g) � � � �Low (�200 g) � � � �
Preoperative breast base positionHigh � � � �Low � � � �
Breast shapeTubular � � � �Glandular tosis � � � �Ptosis (grade I–II) � � � �
Areolar characteristicsSmall diameter � � � �Light/indistinct � � � �
Inframammary creaseNone � � � �High � � � �Low � � � �
Secondary procedure � � � �
*(�) indicates applicable; (�) indicates not generally recommended.†Included for completeness but not generally recommended.
Plastic and Reconstructive Surgery • Fall 2012
64S

the areolar deformity is minimal and it provesnecessary to add a skin flap to widen the breastbase at the inframammary crease.8
The inframammary crease incision is not asgood as a periareolar incision in secondary casesrequiring capsulectomy or closing down the su-perior portion of the pocket because it is at theperiphery of the pocket as opposed to its center.In addition, wound closure is more precarious interms of either implant puncture during closure orexposure postoperatively given that the weight of theimplant presses against it and the soft-tissue coveringat the incision may be minimal. It is not unreason-able in some secondary cases where there are pre-existing inframammary incisions and either thickcapsules or severe deformity to consider a periareo-
lar incision to optimize exposure and thereby im-prove control of the procedure. The inframammaryincision is also not the best choice for patients un-dergoing unilateral augmentation as a symmetryprocedure in breast reconstruction. In these cases, itincreases the overall scar burden on the chest andmay compromise lower skin-flap circulation shoulda mastectomy be required on the augmented side inthe future.
The axillary incision is applicable to most casesof hypomastia that do not have more than gradeI ptosis (Fig. 7). Its obvious appeal is that there isno scar on the breast.9–11 This approach does notrequire endoscopy, although there is evidence tosuggest that the procedure is more accurate whenit is used.12 Whereas many patients require reas-
Fig. 5. Periareolar subglandular augmentation. Preoperatively, this patient exhibited grade II pto-sis owing to an abnormally high inframammary crease. A periareolar incision provided centralaccess to the implant pocket, allowing the inframammary crease to be lowered substantially butaccurately. It was not obvious preoperatively which plane would be best. A subglandular plane wasused after a trial submuscularly on one side proved aesthetically inferior. Smooth-shell 300 cc roundsaline implants were placed with a final fill volume of 320 cc on the right and 340 cc on the left. Thepatient’s photosensitive skin is an unrelated issue.
Volume 130, Number 5S-3 • Breast Augmentation
65S

surance that the axillary scar will not be visible andwill be of good quality, this routinely occurs. It isan ideal choice in patients having a low preoper-ative volume and high breast position on the chestwall, those with small diameter areolae, and thosewith no inframammary crease. Like the inframam-mary crease incision option, an axillary incision isan excellent choice for women with high preop-erative breast volume who only require a small
implant primarily to improve the upper breastcontour. This incision is not practical for subg-landular augmentation; fortunately, breast char-acteristics that suggest a subglandular approachusually favor other incision choices. An axillaryincision is more challenging in patients with longchests and low breast position, but this scenariodoes not constitute a contraindication to thischoice. Tubular breast hypomastia is a contrain-
Fig. 6. This patient with low breast position, glandular ptosis, postpartum atrophy, andsignificant preoperative breast volume proved an ideal candidate for subglandular aug-mentation through an inframammary crease incision. Smooth-shell 350 cc round salineimplants were used with a final fill volume of 375 cc on the left and 350 cc on the right.
Plastic and Reconstructive Surgery • Fall 2012
66S

dication for an axillary approach unless the de-formity is truly minimal.
Secondary procedures in breast augmentationare usually a contraindication to an axillary inci-sion approach. A simple exchange of implantsthrough the original axillary incision requires en-doscopy and can be challenging because multiplecapsulotomies are often required.13 A second in-cision, such as a periareolar type, is well toleratedas an alternative by patients because it still con-
stitutes the first scar on the breast. However, en-doscopy is preferred by some for both primary andsecondary transaxillary breast augmentation. Itsproponents claim that the additional time in-volved with use of the endoscope is not significantonce experience is gained, and that implant mal-position problems in primary cases are less fre-quent when an endoscope is used.14
The periumbilical approach has been devel-oped recently with its chief advantage being a
Fig. 7. Transaxillary submuscular breast augmentation without endoscopy. Smooth-shell 275 cc round saline implants were placed with a final fill volume of 300 cc on bothsides. Note that shaped implants are not required to establish a desirable upper polecontour. Most patients seeking breast augmentation are good candidates for this ap-proach.
Volume 130, Number 5S-3 • Breast Augmentation
67S

single inconspicuous scar located at a distancefrom the breasts.15 This method has many disad-vantages, which include poor access to the implantpocket, inability to create a subpectoral pocket,inability to use a silicone gel prosthesis, inability touse a shaped prosthesis, and the need for a secondincision for revision or implant replacement. It isnot applicable to more complex conditions suchas tubular breast hypomastia or other situationsrequiring alteration of nipple-areola complex po-sition or shape. Its true value in breast augmen-tation remains to be established.
Implant SelectionImplant variables include filler type, shape,
surface texture, and volume. Silicone gel implantuse in the United States is restricted to secondaryapplications and very selected primary cases. Thelatter includes patients requiring concurrent mas-topexy or undergoing treatment for a congenitaldeformity. The majority of women who seek pri-mary augmentation are therefore currently notcandidates for silicone gel implants.
Silicone gel implants are commonly used toreplace old silicone gel implants. Most patientswho have had these devices for a long time are lessconcerned about alleged safety issues and are gen-erally not pleased with the consistency of salineimplants nor as accepting of their spontaneousdeflation risk. Silicone gel implants are also usedto convert saline-implant augmentation patientswho have unacceptable results because of theirthin body habitus, which makes the implant shapeand ripples obvious. Silicone implants are avail-able with more “anatomic” shapes, but these arelikely to prove more useful for breast-reconstruc-tion applications.
All implants are available with either smoothor rough shell texture. There are several studiesthat support the claim of decreased capsularcontracture with textured implants.1,7,16 –19 Mostpractitioners prefer this surface type with sili-cone gel implants, but it is believed that ripplesare more common and more extensive in tex-tured saline implants compared with smoothshell types.20 Therefore, smooth shell saline im-plants are usually selected for primary augmen-tation in thin patients, the most common type.Textured saline implants can be used withoutdisadvantage in patients with higher preopera-tive breast volume, such as those undergoingaugmentation with mastopexy. Another goodindication is a small volume augmentation in-tended primarily to fill out a flat or depressed
upper pole in patients with otherwise satisfac-tory breast volume.
Adjustable implants offer the prospect ofchanging implant volume postoperatively.21 Al-though this is an attractive feature, it should notbe necessary in most cases because it is possibleto accurately select the appropriate implant vol-ume with the use of a sizer intraoperatively. Itwould tend to make postoperative care unnec-essarily complex if this option were to be rou-tinely offered to all patients. There is also theneed to remove a subcutaneous remote valvelater.
These devices may be appropriate for the un-usual situation where a wide range of volume looksappropriate and the patient cannot clearly com-municate her goals preoperatively. In this study,only a few patients required an additional proce-dure to change implant size.
Shaped or “anatomic” implants may havemore conceptual superiority to round implantsthan they actually offer in practice. The type thatis applicable to breast augmentation has a ver-tical axis longer than the horizontal axis and hasbeen successfully marketed by the manufacturerto prospective patients as having a natural, “tear-drop” shape. The majority of breast augmenta-tion patients are still best served by conventionalround implants, although shaped implants arevery successful when applied to the quite dif-ferent setting of breast reconstruction. A flatupper pole of the breast can be consistentlyachieved with round implants when the appro-priate size and final fill volume are selected(Figs. 5 through 7). A patient with a long chestand low breast position may constitute one ofthe better indications for these particular de-vices. In most cases, the choice of shaped versusround implant is not a dominant variable in thedesign of the procedure. Selection of a shapedimplant does not guarantee a successful out-come when other important factors are ignored(Fig. 8). Shaped implants should be used withcaution in secondary cases where there is anestablished implant cavity with a retained cap-sule. In these cases, the implants may rotate ontheir axis during the postoperative period andresult in asymmetry requiring further surgery. Itis also not clear whether the stress forces thatultimately result in implant failure are equallydistributed in shaped implants compared withround implants. Bilateral premature failure wasobserved in shaped implants at the top of theirvertical axis in one patient in the study group.
Plastic and Reconstructive Surgery • Fall 2012
68S

Pocket Plane SelectionSubpectoral implant placement refers to par-
tial muscle coverage underneath the pectoralismajor muscle. The implant is subglandular in itslower portion to a variable degree in these cases.Complete submuscular coverage involving mobi-lization of the serratus anterior muscle and ante-rior rectus sheath is useful for tissue expanders inbreast reconstruction but not appropriate for aes-thetic breast augmentation. Placement below themuscle is believed to contribute to a decreasedincidence of capsular contracture.22–24 It is un-equivocally helpful in most patients to obscuresuperior pole implant shape and minimize thepotential for perceptible ripples with saline im-plant use. Previously, with the widespread use ofsilicone gel implants in primary augmentation,subglandular placement was popular because itsimplified the procedure and minimized postop-erative patient discomfort and recovery.
It has also been claimed that subpectoralimplant placement is advantageous for breastcancer monitoring, although the ratio of im-plant volume to breast tissue volume is likely amore important variable.25,26 Large implantswith a small native breast volume stretched in
front impair mammogram interpretation farmore than the difference in effect between sub-glandular and subpectoral placement of an av-erage size implant.
Subpectoral implant placement is indicatedin most cases of primary breast augmentationexcept for patients with normal body habitus(not excessively thin) who present with signifi-cant postpartum atrophy and exhibit loosebreast skin, glandular ptosis, and significant re-sidual breast volume (more than 200 g per side).Subglandular augmentation in these individualsmore effectively restores shape without the riskof visible implant shape. Subpectoral implantplacement in these individuals may fail to cor-rect ptosis completely, which may result in anabnormal double breast contour.
Patients who present for secondary augmen-tation with capsular contracture often have a char-acteristic appearance based on whether their im-plants are subpectoral or subglandular in location.Breast appearance with capsular contracture andsubpectoral implant placement usually has a con-vex upper pole owing to superior displacement ofthe implants. The breast is flat anteriorly and thenative tissue often ptotic (Fig. 9, above). Patients
Fig. 8. This patient presented with previously placed shaped implants (McGhan style 468). (Left)Although subglandular location contributed to the odd appearance, this photograph illustratesthat “anatomic” implants do not guarantee a natural result. Implant size, fill volume, muscle plane,and implant volume together are more important variables than implant shape in most cases.(Right) Postoperative appearance following submuscular placement of textured round silicone gelimplants through a periareolar incision.
Volume 130, Number 5S-3 • Breast Augmentation
69S

Fig 9. Secondary augmentation. (Above, left) Typical appearance of submuscular aug-mentations with capsular contracture. The breasts are full superiorly, and flat and ptoticinferiorly. (Above, right) The appearance is improved following replacement of nine-year-old silicone gel implants with slightly larger textured-shell round saline implants in thesame submuscular pocket following capsulectomy. (Center, left) Typical appearance ofsubglandular implants with capsular contracture. The implants remain low, but there is a
Plastic and Reconstructive Surgery • Fall 2012
70S

with capsular contracture and subglandular im-plant location often maintain implant position butexhibit a sharp shelf-like contour deformity of theupper pole of the breast, which is often quitestriking (Fig. 9, center). In general, subpectoralimplant location influences breast appearance lessthan subglandular location when contracture isonly mild.
Secondary breast augmentation frequently in-cludes the option of changing subglandular im-plants to a subpectoral location. This is generallyadvisable in patients who have been previouslyaugmented with saline implants and present withvisible implant contour with or without ripples(Figs. 8 and 9, below). These individuals are com-monly thin and may also be best served with aconversion to silicone gel implants at the sametime to minimize the possibility of residual defor-mity requiring yet another procedure. Patientswith old silicone gel implants commonly presentwith capsular contracture, distortion, and a historyof original subglandular placement. It is not nec-essary to convert these patients to a submuscularplane in most cases. Plane conversion prolongssurgery, adding only questionable benefit, con-tributes to a more difficult recovery, and is moreprone to postoperative complications such as he-matoma. The procedure is tedious because thesubglandular pocket must be obliterated superi-orly with sutures, and this is added to a procedurethat may already be lengthy because of the needto perform almost a complete capsulectomy.
In summary, a standardized approach tobreast augmentation may be suitable for most pa-tients. However, optimal results will be consis-tently achieved if flexibility is retained in surgicaldesign and if the combination of incision, pocketplane, and implant is customized when one is pre-sented with specific anatomic variants and second-ary problems.
David A. Hidalgo, M.D.655 Park Avenue
New York, N.Y. [email protected]
REFERENCES1. Asplund O, Gylbert L, Jurell G, Ward C. Textured or smooth
implants for submuscular augmentation: A controlled study.Plast Reconstr Surg. 1996;97:1200.
2. Handel N, Wellisch D, Silverstein MJ, Jensen JA, Waisman E.Knowledge, concern, and satisfaction among augmentationmammaplasty patients. Ann Plast Surg. 1993;30:13.
3. Rheingold LM, Yoo RP, Courtiss EH. Experience with 326inflatable breast implants. Plast Reconstr Surg. 1994;93:118.
4. Strom SS, Baldwin BJ, Sigurdson AJ, Schusterman MA. Cos-metic saline breast implants: A survey of satisfaction, breast-feeding experience, cancer screening, and health. Plast Re-constr Surg. 1997;100:1553.
5. Young VL, Nemecek JR, Nemecek, DA. The efficacy of breastaugmentation: Breast size increase, patient satisfaction, andpsychological effects. Plast Reconstr Surg. 1994;94:958.
6. Burkhardt BR, Fried M, Schnur PL, Tofield JJ. Capsules,infection, and intraluminal antibiotics. Plast Reconstr Surg.1981;68:43.
7. Burkhardt BR, Eades E. The effect of biocell texturing andpovidone-iodine irrigation on capsular contracture aroundsaline-inflatable breast implants. Plast Reconstr Surg. 1995;96:1317.
8. Dinner MJ, Dowden RV. The tubular/tuberous breast syn-drome. Ann Plast Surg. 1987;19:414.
9. Hoehler H. Breast augmentation: The axillary approach. Br JPlast Surg. 1973;26:373.
10. Tebbetts JB. Transaxillary subpectoral augmentationmammaplasty: A 9-year experience. Clin Plast Surg. 1988;15:557.
11. Tebbetts JB. Transaxillary subpectoral augmentation mam-maplasty: Long-term follow-up and refinements. Plast Recon-str Surg. 1984;74:636.
12. Price CI, Eaves FF III, Nahai F. Endoscopic transaxillarysubpectoral breast augmentation. Plast Reconstr Surg. 1994;94:612.
13. Howard PS, Oslin BD, Moore JR. Endoscopic transaxillarysubmuscular augmentation mammaplasty with textured sa-line breast implants. Ann Plast Surg. 1996;37:12.
14. Smith JW, Shaw LW, Friedland JA. Endoscopic transaxillarysubpectoral augmentation mammaplasty: A comparativeanalysis of endoscopic versus non-endoscopic transaxillarysubpectoral augmentation mammaplasty using smooth sa-line implants. Plast Surg Forum 1998;21:127.
15. Johnson GW, Christ JE. The endoscopic breast augmenta-tion: The transumbilical insertion of saline-filled breast im-plants. Plast Reconstr Surg. 1993;92:801.
16. Ersek RA. Rate and incidence of capsular contracture: Acomparison of smooth and textured silicone double-lumenbreast prostheses. Plast Reconstr Surg. 1991;87:879.
17. Pollock H. Breast capsular contracture: A retrospective studyof textured versus smooth silicone implants. Plast ReconstrSurg. 1993;91:404.
18. Burkhardt B, Eades E. The effect of Biocell texturing andpovidone-iodine irrigation on capsular contracturearound saline-inflatable breast implants. Plast ReconstrSurg. 1995;96:1317.
19. Coleman DJ, Foo ITH, Sharpe DT. Textured or smoothimplants for breast augmentation? A prospective, controlledtrial. Br J Plast Surg. 1991;44:444.
20. Handel N, Jensen JA, Black Q. The fate of breast implants:A critical analysis of complications and outcomes. Plast Re-constr Surg. 1995;96:1521.
(Fig. 9. Continued) characteristic shelf effect where the implantmeets the chest wall superiorly. (Center, right) The appearance isimproved following replacement of 10-year-old stacked polyure-thane-covered gel implants with a slightly larger size silicone gelimplant placed in the same subglandular plane following capsu-lectomy. (Below, left) Visible subglandular saline implants withrippling. (Below, right) Appearance following conversion to a sub-muscular plane and exchange of saline implants for silicone geltype.
Volume 130, Number 5S-3 • Breast Augmentation
71S

21. Becker H. Breast augmentation using the expander mam-mary prosthesis. Plast Reconstr Surg. 1987;79:192.
22. Biggs TM, Yarish RS. Augmentation mammaplasty: Retr-opectoral versus retromammary implantation. Clin PlastSurg. 1988;15:549.
23. Gylbert L, Jurell G, Asplund O, Olenius M. Results of subglandularbreast augmentation using a new classification method: 18-yearfollow-up. Scand J Plast Reconstr Surg Hand Surg. 1989;23:133.
24. Puckett CL, Croll GH, Reichel CA, Concannon MJ. A critical lookat capsular contracture in subglandular versus subpectoral mam-mary augmentation. Aesthetic Plast Surg. 1987;11:23.
25. Grace GT, Roberts C, Cohen IK. The role of mammographyin detecting breast cancer in augmented breasts. Ann PlastSurg. 1990;25:119.
26. Leibman AJ, Kruse BD. Imaging of breast cancer after augmen-tation mammoplasty. Ann Plast Surg. 1993;30:111.
Plastic and Reconstructive Surgery • Fall 2012
72S