Breast
106
Managing Breast Abnormalities BY PROF/ GOUDA ELLABBAN
-
Upload
scu-hospital -
Category
Health & Medicine
-
view
30 -
download
3
Transcript of Breast

Managing Breast Abnormalities
BYPROF/ GOUDA ELLABBAN

Outline - 1
Clinical presentations of breast disease Nipple discharge Mastalgia Breast mass
diagnostic imaging who to biopsy how to biopsy

Outline – 2
Treatment of breast cancer Local-regional control of breast cancer
Surgery Modified Radical Mastectomy (MRM) Breast Conservation Therapy (BCT) Addressing nodal disease
Axillary Lymph Node Dissection (ALND) Sentinel Lymph Node Biopsy (SLNB)
Radiation therapy Postmastectomy Radiotherapy (PMRT) Whole breast irradiation versus Accelerated Partial Breast
Irradiation (APBI)

Outline - 3
Systemic adjuvant therapy Advances in chemotherapy
Taxanes Dose dense regimens
Evolving paradigms in hormonal manipulation Estrogen receptor inhibition Aromatase inhibitors

Outline - 4
Breast cancer screening Guidelines for screening Risk Factors for breast cancer
Family history Low relative risk High relative risk
BRCA genes Who should be tested
Breast cancer risk reduction Prophylatic surgery Chemoprevention

Clinical Presentation
3 most common breast complaints: Mastalgia NIPPLE DISCHARGE MASS
>50% of patients presenting to surgeon with a breast condition will have benign disease
Marchant, Surg Oncol Clinics of North America, 1998

Caution!
Applying the correct diagnostic and/or therapeutic algorithm is critical Treat patient thoughtfully –
Look for a mass Image area as appropriate
Ultrasound Mammogram
Balance the need for diagnostic workup and avoid unnecessary procedure(s)

Breast Pain (Mastalgia) Almost all women will have experienced varying
degree of breast pain in her lifetime ranging mild discomfort severe pain cyclical
estrogen overstimulation methylxanthines

Mastalgia
Mastalgia is a poor predictor for cancer risk <5% of breast cancer are associated with
pain >95% of patients with some breast pain Beware!
Though the association of breast pain and breast cancer is NOT strong, the fear is very REAL

Management of Mastalgia The most important questions:
Is there a dominant mass? Physical examination for dominant mass
Follow the workup of a breast mass Is there associated nipple discharge?
If there is bloody or serous discharge, follow nipple discharge workup
Does patient have recent breast imaging Mammogram Ultrasound If abnormal, follow workup of a breast mass

Management of Mastalgia If the breast examination and mammograms are
negative: Discontinue caffeinated products Discontinue nicotine use Nonsteroidal anti-inflammatory agents (NSAIDs) Hormonal manipulation
Danazol 6 month trial of 100 to 400mg daily Side effects
Tamoxifen Vitamins
A and E Repeat examination in 4 to 6 months

Nipple Discharge
Less than 5% chance of cancer
Leis, World J Surgery, 1999
Differentiate between high versus low risk by history
Higher risk Lower riskSpontaneous versus provoked
Unilateral versus bilateral
Bloody/serous versus cloudy and/or multicolored
Post- versus pre-menopasual

Nipple Discharge Physical examination
Is there a subareolar mass? Types of imaging
Mammogram Ultrasound
Duct ectasia Ductogram
Intraductal defect

Nipple Discharge
Determine the need for histologic diagnosis based on the following History Examination Imaging
Causes of nipple discharge Most common cause for spontaneous nipple discharge
is intraductal papiloma BUT intraductal (DCIS) and invasive ductal carcinoma
can cause nipple discharge (5%)

Management of a Breast Mass
Questions that need to be addressed Is it dominant? What is the age of patient? How long has it been? Has it change in size? Any associated symptoms?
discharge skin changes pain
What is the relative risk for cancer? previous biopsy family history

Management of a Breast Mass
Determine the type of imaging Diagnostic mammogram
Reserved for older than 30 years of age Pleomorphic microcalcification Architectural distortion
Ultrasound Diagnostic imaging Cystic versus solid NOT a screening test – nonspecific
MRI Dense breast tissue Post radiation therapy
PET scan In house protocol for recurrent disease


Management of a Breast Mass
Determine if histologic confirmation is necessary Cystic lesion
Simple versus complex Is there any intra-cystic defect? Does it need drainage?
Solid lesion Mammographic criteria
BiRads Suspicious ultrasound characteristics
Solid lesion with Low level internal echo Irregular margin Taller than in it is wide


Management of a Breast Mass
2 categories of biopsy Excisional
Removes the whole lesion Incisional
Removes part of the lesion

Excisional Biopsy
Often used for palpable lesion Nonpalpable, mammographically detected lesion
Needle localization Blue dye injection
Benefits Removes lesion completely Reduces risk for sampling error If tumor-free margin is achieved
Lumpectomy with curative intent


Incisional Biopsy
By definition, samples the lesion Fine needle aspiration (FNA)
Cytology Open wedge biopsy Tru-cut or core biopsy
Image guided or by palpation Mammogram
Stereotatic core biopsy (SCB) Mammotomy
Ultrasound

Treatment for Breast Cancer

Breast Cancer Outcome Incidence 211,240 Death 40,410 5 yr survival
1975 75%1986 78%2000 88%
Jemal, et al., CA Cancer J Clin 55(1);10, 2005
Improvement in breast cancer outcome Early detection Multimodal therapy
Locoregional control Systemic adjuvant therapy

Breast Cancer Therapy
Local-regional control Surgery Radiation therapy (XRT)
Systemic control Chemotherapy Hormonal manipulation

Surgical Therapy for Breast Cancer“The Gold Standard”
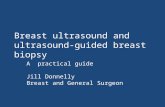
Modified Radical Mastectomy (MRM) Total mastectomy
Removal of all gross breast tissue including the nipple areolar complex
Level I and II axillary node dissection (ALND) Breast Conservation Therapy (BCT)
Excision of cancer with tumor-free margin lumpectomy
ALND XRT

Systemic Therapy Adjuvant therapy based weighing
Risk of recurrence Sequelae of therapy
Chemotherapy Node-positive patients Tumors >1 cm Age/Menopausal status Overall health of patient
Endocrine therapy Receptor status (ER and PR)
Anti-estrogen Aromatase inhibitors (AIs)
Modified Radical Mastectomy



Breast Conservation Therapy Removal of breast cancer
Lumpectomy Quadrantectomy Partial mastectomy Segmentectomy Must achieve tumor-free margins
Axillary node dissection Breast irradiation
4500 to 5000 cGy 5 to 6weeks Whole breast irradiation


What to do with the lymph nodes?

Management of Axillary Lymph Nodes
Infitrating ductal cell carcinoma (IDCA) Invasion of tumor cells beyond the basement
membrane Nodal basin needs evaluation
Gold Standard Complete ALND
Sentinel Node Biopsy (SLNB) Early breast cancer

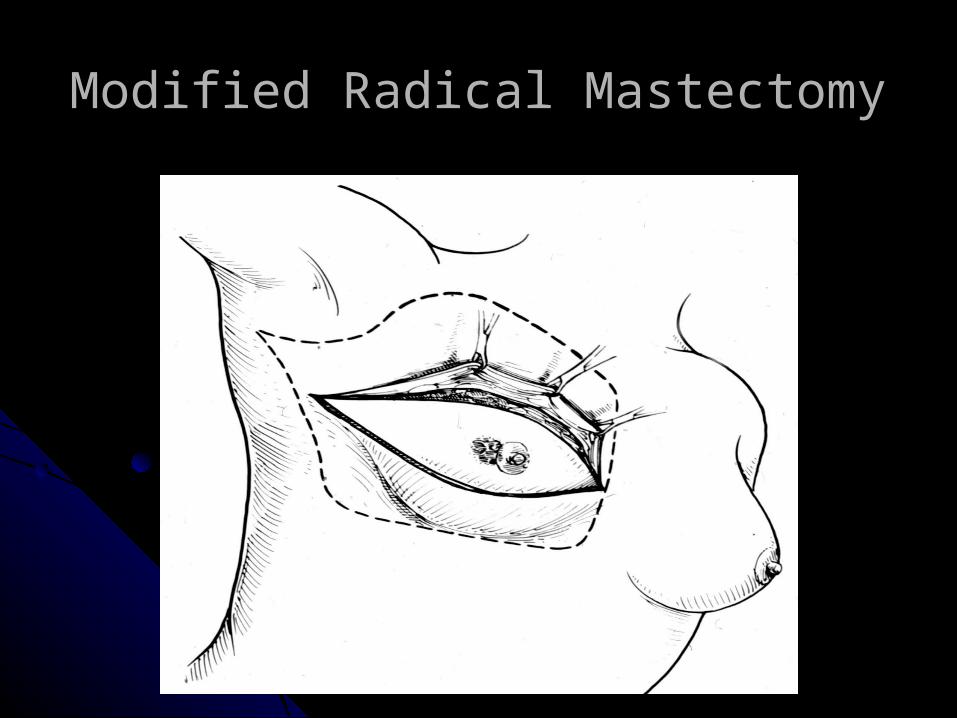
Axillary Node Dissection
Staging: Single best predictor for risk of systemic
disease and cancer recurrence Therapeutic decisions
Systemic therapy Radiation therapy
May improve survival and cuure
Axilla Nodes-Level I, II and III

NSABP B-06 20 Year Update Randomized trial initiated in 1976
3 arms (all patients underwent ALND) Total mastectomy (MRM) Lumpectomy Lumpectomy and XRT (BCT)
Accrued 2,163 patients with tumors < 4 cm Included node- positive and negative patients
Establishes the efficacy and safety for BCT
Fisher, NEJM Oct., 2002


Breast Conservation Versus Mastectomy
For most women, breast conservation therapy is as good as mastectomy
Contraindications remain Multicentric disease Inability to obtain negative margins Breast lesion and breast size Contraindication to radiation therapy Patients’ preference Compliance

Evolving Treatment Paradigms:The Sentinel Node

Sentinel Lymph Node Biopsy (SLNB)
Definition “gate-keeper” or first echelon node to drain a tumor,
i.e. primary breast cancer
Focuses on Identify node-negative patients
avoid unnecessary node dissection Identify node-positive patients
Complete node dissection Systemic therapy XRT

Identifying the Sentinel Node
Injection material Technetium-99m sulfur colloid Isosulfan blue
Site of injection Intra-tumoral Intra-parenchymal Intra-dermal/peri-areolar
Embryological: axilla May miss internal mammary nodes

Blue Sentinel Node

Potential Benefits Risk reduction for lymphedema
Group 1: 117 patients SLNB and node dissection Group 2: 303 patients SLNB without node dissection Lymphedema 17.1% versus 3% (p<0.0001)
Sener, Cancer, 2001
Higher degree of scrutiny of SLN by pathologists Cursory examination of 10 to 25 nodes Extensive evaluation of a few nodes Application of molecular techniques

Potential Risks
Risk of not finding the sentinel node: 5% In clinical trials after training Higher in early part of learning curve
FALSE negative rate (FNS): 5 to 10% Technical error
Injection site Type of contrast used
Learning curve Alternate lymphatic drainage

Risks of False Negative SLN
Implications for the patients Leaving behind nodal disease
Local-regional recurrence Systemic implications
Understaging of disease will lead to under-treatment
Small tumor, node-negative disease Impacts choice of adjuvant
Chemo regimen Postoperative axillary XRT

False Negative SLN
To reduce the number of missed node-positive patients: Select patients with less likelihood of node-
positive disease Practical application based on 1,000 patients
FNR = 5% Applied to a 10% node-positive risk group
You will miss 5 node-positive patients Applied to a 40% node-positive risk group
You will miss 20 node-positive patients

Critical Issues with SLN Biopsy
Technical competence Learning curve Mapping accuracy
Blue dye plus Tc-sulfur colloid Maintain quality control
False negative rate must be 5% or less Validated by performing completion ALND in the initial
experience Surveillance of patients for cancer recurrence

Critical Issues with SLN Biopsy
NO SURVIVAL DATA NSABP trial ACOSOG Z00010 and Z00011
Await cancer cooperative groups results
Importance of Informed Consent

Is SLNB Safe?
Prospective, randomized trial in Milan Over 250 patients in each arm SLNB with completion ALND versus SLNB alone (if
SLNB is negative) In the SLNB followed by ALND
Accuracy = 96.9% False negative rate = 8.8%
SLNB alone group (median follow-up = 46 months) No overt axillary metastasis No difference in rate of cancer events
16.4 per 1,000 per year in ALND 10.1 per 1,000 per year in SLNB
Veronesi, et al., NEJM, 2003.

Take Home Message ALND remains the gold standard Quality control Careful patient selection for SLNB alone
T1 and small T2 lesion Unicentric lesion Avoid patients with excisional breast biopsy > 6 cm Avoid patients treated with neoadjuvant therapy Avoid patients with previous axilla surgery Avoid patients with gross nodal disease
Anderson, JNCCN, 2003.

Evolving Treatment Paradigms: Adjuvant Radiation Therapy
Accelerated Partial Breast Irradiation (APBI)
Postmastectomy radiotherapy (PMRT)

Postoperative XRT after BCT
External Beam Radiation Therapy (EBRT) Whole breast therapy Daily treatment for 5 to 6 weeks Total dosage: 5000 cGy
Compliance issue Non-compliance: 50% Local failure: 50%
Li, Ann Surg, 1999

Accelerated Partial Breast Irradiation (APBI)
Limit the volume of breast to be treated Within 2 cm border of lumpectomy
XRT completed in 4 to 5 days after lumpectomy
Multicatheter interstitial brachytherapy Balloon catheter brachytherapy (MammoSite) 3-D conformal external beam radiotherapy Intraoperative radiotherapy

Brachytherapy

IBRT

3D-Conformal EBRT

Summary of APBI Results
Multicatheter interstitial brachytherapy Longest follow-up (median FU 27 to 91 months) 5 yr local recurrence (LR) rate: 5% (0% to 37%)
Balloon catheter brachytherapy (MammoSite) LR rate: 0% (F/U11 to 29 months) Infection rate 16%
3-D conformal external beam radiotherapy LR rate: 0 to 25%
Arthur, et al., J Clin Oncol 23:1726, 2005.

Clinical Trial – NSABP B39
Partial breast irradiation trial Tumor size < 3 cm Unifocal tumor After lumpectomy, randomized to
External beam radiation (EBRT) Partial breast irradiation (PBI)
MammoSite Intracavitary catheters 3-D conformal EBRT

Take Home Message
The role of APBI is evolving This is NOT the standard of care Must be considered in the context of
Clinical trial Careful patient selection Informed consent

Radiotherapy After Mastectomy Pre-1997: NOT indicated except for
Positive margins High risk for local failure
Locally advance breast cancer Inflammatory breast cancer
Post-1997 Overgaard, et al., NEJM 337:949, 1997.
Danish Breast Cancer Cooperative Group Ragaz, et al., NEJM 337:956, 1997.
British Columbia Postmastectomy radiotherapy became relevant

Postmastectomy Radiotherapy (PMRT)
ASCO Expert Panel Reviewed data from 18 randomized clinical
trials (RCTs) Reduction in risk for local failure (LF)
By two thirds to three quarters, proportionally In practical terms:
Reduction of LF from 8 per 100 patients To 2-3 per 100 patients
Recht, et al., J Clin Oncol19(5):1539, 2001

Controversies with PMRT
Sparked debates regarding routine use of PMRT Complications of XRT include
Lymphedema Brachial plexopathy Radiation pneumonitis Rib fractures Cardiac toxicity Radiation-induced 2nd primaries

ASCO Expert Panel
Specific review of the British Columbia and Danish trials First to report improvement in DFS and OS
Relative reduction in risk for death Danish trial: 29%
British Columbia Trial: 26%

Controversies with PMRT
Limitations of the Danish and BC trials No other trials demonstrating similarly
significant benefits Benefits only apparent after 12 years
of follow-up Number of nodes recovered after
mastectomy were low

Take Home Message
ASCO Guidelines for PMRT Patients with 4 or more positive nodes Patients with T3 or Stage III Disease Insufficient data to PMRT:
Patients with 1 to 3 positive nodes All patients treated with neoadjuvant therapy and
mastectomy Other tumor characteristics
HER2, ER, vascular and lymphatic invasion, etc
Recht, et al., J Clin Oncol19(5):1539, 2001

Advances in Systemic Adjuvant Therapy: Chemotherapy and Endocrine Therapy

Adjuvant Chemotherapy
Treatment of patients at risk for disease dissemination prior to the diagnosis and initiation of therapy of the primary cancer
Goal: Reduce risk for recurrence and death
Only helps those who recur May harm those that do not

After 200+ RCTs - Combination therapy is superior to single
agents 4 to 6 months produced optimal results
Longer treatment with the same regimen did NOT provide incremental gains
Hormone receptor-positive patients benefit from sequential chemotherapy plus endocrine therapy Additive therapeutic effect

What have we learned?
Standard regimens are CMF and CAF Anthracycline (e.g. Adriamycin) containing
regimens are superior to those that lacks it High dose therapy did not improve overall
survival Increased morbidity and mortality
Hamilton, et al., J Clin Oncol 23:1760, 2005.

Taxanes
1st Trial CALGB 9344: AC + placlitaxel(T) 3,121 node-positive patients Median follow-up of 69 months
5 yr DFS: 70% v 65%, p=0.0023 5 yr OS: 80% v 77%, p=0.0064
Henderson, et al., J Clin Oncol 21:976, 2003

Supporting Data
NSABP B28 Trial 3,060 node-positive patients AC X4 + T X4 Relative risk for recurrence reduced by 13%
Mamounas, et al., Proc ASCO 22:4, 2003.
MDACC 94-002 524 patients T X4 + FAC X4 v FAC X8 Relative risk for recurrence reduced by 22%
Buzdar, et al., Clin Cancer Res 8:1073, 2002.

Docetaxel (Taxotere) Trial
BCIRG 001 Trial 1,491 node-positive patients TAC X6 v FAC X6 5 yr outcome
DFS: 75% v 68% OS: 87% v 81%
Increased morbidity Febrile neutropenia 10X control arm Neurotoxicity
Nabholz, et al., Proc ASCO 21:36, 2002

Dose-dense Regimen
Theoretical premise:“Full doses of drug, given at the highest possible frequency, will
produce the highest degree of cell kill”
CALGB 9741 2,005 node-positive patients 2 X 2 factorial design
A T C every 3 weeks A T C every 2 weeks + G-CSF AC T every 3 weeks AC T every 2 weeks + G-CSF

CALGB 9741
Median follow-up of 36 months Dose dense regimen
4 yr DFS: 82% v 75% Significant OS in favor of dose-dense arm Low rate of neutropenic fever and cardiac
toxicity Increased rate of anemia
Citron, et al., J Clin Oncol 21:1431,2003.

Neoadjuvant Chemotherapy
NSABP B-18 pre- versus post-operative adjuvant therapy 1,523 women
operable breast cancer AC X 4 pre v post
No survival benefit

Advantages
Higher rate of breast conservation Convert some “inoperable” breast cancer to potentially
curative surgical candidates Response in real time
Lack of response – change regimen Prognosis can be refined by degree of residual
disease Pathologic clinical response had much higher DFS and
OSWolmark, et al., JNCI 30:96, 2001.

Take Home Message Node-positive breast cancer patients with high
likelihood of a long life span should be offered taxane systemic therapy in addition to anthracycline-based chemotherapy
Dose-dense regimen may play a more significant role in chemotherapy administration in the near future
Neoadjuvant therapy should be considered for late stage disease and/or for larger lesions in women who are to be considered for BCT

Endocrine Therapy
Gold Standard: Tamoxifen (Nolvadex) Anti-estrogen receptor 5 years treatment of ER+/PR+ breast cancer Relative risk reduction of 25%
Node-positive: 10% improvement in 10-yr survival Node-negative: 5% improvement in 10-yr survival
Lower toxicity profile compared to chemotherapy

Aromatase Inhibitors (AIs) Conversion of androgenic substrates to estradiol
Enzyme complex - aromatase Highly expressed in ovarian follicles in premenopausal women
AIs blocks aromatase activity Postmenopausal women:
Residual estrogen production by peripheral conversion Subcutaneous fat, liver, muscle
AIs suppress circulating estrogen by 98+%

AIs and Breast Cancer
Estrogen and receptor positive breast carcinoma Tamoxifen binds estrogen receptors and exerts anti-estrogenic
effect AIs block peripheral estrogen conversion in postmenopausal
women Reduction in estrogen results in cancer growth inhibition
AIs have minimal effect on breast cancer in premenopausal women in clinical trials


Aromasin
Arimidex Femara

AIs in the Adjuvant Setting ATAC Trial
Arimidex, Tamoxifen, Alone or in Combination 9,366 postmenopausal patients After median follow-up of 47 months:
Risk for recurrence Hazard Ratio of patients on AI = 0.86 that of Tamoxifen (p=0.03)
Risk for 2nd primary in contralateral breast Hazard Ratio of patients on AI = 0.56 that of Tamoxifen (p=0.04)
Combination of Arimidex and Tamoxifen did not appear to be superior
No overall survival difference to date

Adverse Effects: AIs v Tamoxifen
Lower incidence Hot flashes Vaginal bleeding and discharge Venous thromboembolism Endometrial cancer
Higher risk for Musculoskeletal symptoms Fractures associated with osteoporosis
ATAC Trialists’ Group Lancet 359:2313, 2002.
Baum, et al., Cancer 98:1802, 2003.

Use of AIs Beyond Year 5
ER+ patients treated with tamoxifen fail between 5 to 15 years after surgery
Tamoxifen therapy beyond 5 yrs NOT useful
Question: Does adding AI to beast cancer patients after 5
years of Tamoxifen therapy help?

MA.17 Trial
5,187 women after 4.5 to 6 yrs of Tamoxifen Randomized to placebo v letrozole (Femera) Median follow-up of 2.4 yrs
Trial terminated DFS: 93% v 87%, p<0.001 HR for recurrence 0.57 (p=0.00008)
Extending endocrine therapy beyond 5 yrs with an AI offers significant DFS benefit
Goss, et al., NEJM 349:1793, 2003.

Clinical Trial – ACoSOG Z1031 Stage II and III breast cancer patients Neoadjuvant hormonal manipulation trial
comparing the 3 aromatase inhibitors Anastrozole Letrozole Exemestane
Estrogen receptor positive Postmenopausal women Endpoints
Response Toxicity profile

Take Home Message In postmenopausal women, AIs appears to be
superior to Tamoxifen Reducing/delaying cancer recurrence Lowering contralateral second primary cancer Slightly better adverse effects profile except for
osteoporosis Should be considered for women having
difficulties with Tamoxifen Should be considered in addition to 5 years of
Tamoxifen

Breast Cancer Screening

Breast Cancer Screening General population guideline
Age 50 and above Breast examination
Annually by healthcare professional Monthly breast self examination
Annual mammogram Age 40 to 49
Guidelines based on risk assessment More controversial
More false positives More procedures Higher risk for interval cancer

Cancer Screening in Young Women
Controversies High false positive rates
3 of 10 women will have a “positive” mammogram Unnecessary procedures and anxiety
Non-invasive cancer (DCIS) No statistically significant difference in breast
cancer mortality 0-10 lives in 10,000 screened from 40 - 49
Canadian National Breast Cancer Screening Study, Can Med Assoc J, 1992
Reserved for high risk women
NIH Consensus Panel
Risk reduction in cancer death by breast cancer screening women over 50
33% risk reduction in death in the screened populationNIH Consensus Statement, 1977
women between 40 and 49 17% risk reduction in death in the screened population
NIH Consensus Statement, 1997

Defining “High Risk” Patients What exactly is the relative risk when there is a
family history of breast cancer? One family member with postmenopausal breast
cancer 2-3 fold relative risk elevation
“high risk” family Multiple 1st degree relatives Pre-menopausal breast cancer Bilateral breast cancer Male breast cancer Ovarian cancer

The BReast CAncer (BRCA) Genes
5 to 10% of breast cancer are hereditary BRCA1 BRCA2
50% to 80% lifetime risk Tumor suppressor genes
Involved in cell cycle control In addition to breast cancer
BRCA1 mutation is associated with 50% risk for ovarian cancer BRCA2 mutation is associated with increased risk for male
breast CA

BRCA Genes
Who should be considered for BRCA testing? 2 first degree relatives One first degree relative
Premenopausal Bilateral
Ovarian cancer Multiple breast cancer, including male breast cancer
Offered with complete genetic/social counseling

Other Risk Factors Personal history of breast cancer
10 to 15% lifetime risk for contralateral breast cancer Previous biopsy with the diagnosis of in situ carcinoma
Lobular Carcinoma In Situ (LCIS) Ductal Carcinoma In Situ (DCIS)
Proliferative breast disease Without atypia With atypia
Estrogen Unopposed stimulation versus prolonged exposure Replacement therapy

Prophylatic Surgery for Breast Cancer
Bilateral mastectomies 639 patients with family history of breast cancer 90% risk reduction
Hartman, NEJM, 1999 Women with BRCA1 or BRCA2 mutations
76 underwent prophylatic mastectomies 63 surveillance only At 3 years follow-up
0 patients with breast cancer in 76 treated with prophylatic mastectomies
8 patients with breast cancer in the surveillance groupMeijers-Heiboer, NEJM, 2001

Prophylatic Surgery for Breast Cancer
Prospective trial of 131 BRCA carriers 69 underwent prophylatic bilateral
oophorectomies 3 developed breast cancer subsequently
62 patients were in the surveillance group 8 developed breast cancer
Median follow-up of 2 years
Kauff, NEJM, 2002

Chemoprevention NSABP BPCT-1
13,388 women randomized to receive tamoxifen versus placebo
At median follow-up of 54 months 49% reduction of invasive breast cancer 50% reduction of non-invasive breast cancer
Caveats No reduction in ER negative carcinomas Overall survival was not a measured outcome
We Don’t Know If The Breast Cancer Reduction Translates into Cancer Death Reduction
Increased risk for endometrial cancer (RR = 4 in age>50) DVT (RR = 1.7) PE (RR=3.0)
Fisher, JNCI, 1999

Summary - 1
Management of the 3 most common clinical presentations for breast disease Nipple discharge Mastalgia Breast mass
diagnostic imaging who to biopsy how to biopsy

Summary – 2
Treatment of breast cancer Local-regional control
Surgery Modified Radical Mastectomy (MRM) versus Breast
Conservation Therapy (BCT) Addressing nodal disease
Axillary Lymph Node Dissection (ALND) Sentinel Lymph Node Biopsy (SLNB)
Radiation therapy Whole breast irradiation versus Accelerated Partial Breast
Irradiation (APBI) Postmastectomy Radiotherapy (PMRT)

Summary - 3
Systemic adjuvant therapy Advances in chemotherapy
Anthracycline-based therapy Taxanes Dose dense regimens
Evolving paradigms in hormonal manipulation Estrogen receptor inhibition
Tamoxifen Aromatase inhibitors
Femara, Aromasin, Arimidex

Outline - 4
Breast cancer screening Guidelines for screening
NIH consensus statement: women over 40 Breast examination
Risk Factors for breast cancer Family history BRCA genes
Who should be tested Breast cancer risk reduction
Surgical prophylaxis Tamoxifen

Questions ????