Breaking Eroom’s Law - Nature Research
2
Early in the last decade, researchers at Sanford Bernstein published ‘Eroom’s Law’— Moore’s Law in reverse — that the all-in cost of R&D on new drugs approved by the US FDA had risen exponentially for 60 years (Nat. Rev. Drug Discov. 11, 191–200; 2012). Among the potential contributing factors underlying the trend, the authors highlighted a progressively higher bar for improvements over existing therapies (the ‘better than the Beatles’ problem) and a progressive lowering of risk tolerance by regulatory agencies (the ‘cautious regulator’ problem). However, as the researchers posited might happen, about the same time Eroom’s Law was published, it was already being broken. Here, we analyse the changes and discuss the underlying factors. Details of the data and analysis are provided in Supplementary Box 1. Breaking the law: how and why Starting around 2010, the trend line changed, with a net result of an additional 0.7 new molecular entity (NME) launches per billion US$ of R&D spending per year by 2018 (P <1.5 × 10 −10 ) (FIG. 1a). This change is seen not just in the raw count but also with the value-weighted count of drugs (P <2.5 × 10 −5 ) (FIG. 1b), which is more pertinent from both in particular, improving decision making. The third factor is changes to the threshold for regulatory approval, perhaps related to shifts in disease areas or regulatory philosophy (reversing the ‘cautious regulator’ problem, at least in some diseases). We explore each of these factors below. Better information. There has been increasing emphasis on the use of human genetic data to understand disease. One proxy variable for our increasing under- standing of human genetic data is the growth of genome-wide association studies (GWASs). Analysis of the percentage of drug approvals for which the target of an NME had GWAS validation at the time of its entry into development, scaled relative to the total number of GWASs available at the time (which has increased substan- tially over the period), indicates an increase since 2012 (FIG. 2a). We do not suggest that GWAS data were used to support all of these approvals, but this trend supports the hypothesis that there has been an increasing focus on targets that have validation from human genetic data. Even small changes in the quality of information can have large effects on R&D an investor and patient perspective, albeit noisier to measure (Drug Discov. Today 22, 1749–1753; 2017). What changed? Our analysis indicates that the proximate cause of the resurgence was the same as the prior decline: changes in success rates that changed the costs asso- ciated with failed NMEs. The data shown in FIG. 1c illustrate the estimated impact on the development costs per NME split between successful and failed molecules for 3 selected years over the past 3 decades. Success rates, particularly in late-stage R&D, declined precipitously during the period of declining R&D productivity, but levelled off and began to increase approximately 5 years ago, driving the turnaround in R&D productivity. This turnaround in the timing and amount of attrition could only be achieved as a result of one or more of three main factors. The first is better information for decisions — that is, better knowledge of disease biology or how to modulate it, leading to new ways to treat diseases for which therapies are already available and/or side-stepping the ‘better than the Beatles’ problem by moving into diseases that lack effective therapies. A second, related factor is better use of that information; Breaking Eroom’s Law Michael S. Ringel, Jack W. Scannell, Mathias Baedeker and Ulrik Schulze Iryna_L/iStock/Getty Images Plus Number of NMEs per billion US$ R&D spending 100 a 10 1.0 0.1 1940 1960 1980 2000 2020 Cost of failure Cost of molecule Δ: By 2018, 0.7 more NMEs per billion US$ R&D spending Eroom’s Law published with data up to 2010 Peak sales (US$ billions) of NMEs per billion US$ R&D spending 10 b 1.0 0.1 1990 2000 2010 2020 Δ: By 2018, $0.3 billion more peak sales per billion US$ R&D spending Eroom’s Law published with data up to 2010 All-in cost of development (US$ billions) per NME 1.5 c 1.0 0.5 0 1990 2004 2013 56% 44% 18% 40% 60% 82% Fig. 1 | Breaking Eroom’s Law. a | Count of new molecular entities (NMEs) per billion US$ R&D spending. b | Aggregate peak sales (US$ billions) of NMEs per billion US$ R&D spending. c | All-in cost of development (US$ billions) per NME. See Supplementary Box 1 for details of the data and analysis. VOLUME 19 | DECEMBER 2020 | 833 FROM THE ANALYST’S COUCH NATURE REVIEWS | DRUG DISCOVERY NEWS & ANALYSIS
Transcript of Breaking Eroom’s Law - Nature Research

Early in the last decade, researchers at Sanford Bernstein published ‘Eroom’s Law’— Moore’s Law in reverse — that the all- in cost of R&D on new drugs approved by the US FDA had risen exponentially for 60 years (Nat. Rev. Drug Discov. 11, 191–200; 2012). Among the potential contributing factors underlying the trend, the authors high lighted a progres sively higher bar for improvements over existing therapies (the ‘better than the Beatles’ problem) and a progressive lowering of risk tolerance by regulatory agencies (the ‘cauti ous regulator’ problem). However, as the researchers posited might happen, about the same time Eroom’s Law was published, it was already being broken. Here, we analyse the changes and discuss the underlying factors. Details of the data and analysis are provided in Supplementary Box 1.
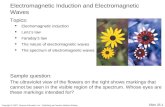
Breaking the law: how and whyStarting around 2010, the trend line changed, with a net result of an additional 0.7 new molecular entity (NME) launches per billion US$ of R&D spending per year by 2018 (P <1.5 × 10−10) (Fig. 1a). This change is seen not just in the raw count but also with the value- weighted count of drugs (P <2.5 × 10−5) (Fig. 1b), which is more pertinent from both
in particular, improving decision making. The third factor is changes to the threshold for regulatory approval, perhaps related to shifts in disease areas or regulatory philosophy (reversing the ‘cautious regulator’ problem, at least in some diseases). We explore each of these factors below.
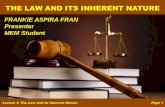
Better information. There has been increasing emphasis on the use of human genetic data to understand disease. One proxy variable for our increasing under-standing of human gene tic data is the growth of genome- wide associa tion studies (GWASs). Analysis of the percent age of drug approvals for which the target of an NME had GWAS validation at the time of its entry into development, scaled relative to the total number of GWASs available at the time (which has increased substan-tially over the period), indicates an increase since 2012 (Fig. 2a). We do not suggest that GWAS data were used to support all of these approvals, but this trend supports the hypothesis that there has been an increasing focus on targets that have validation from human genetic data. Even small changes in the quality of information can have large effects on R&D
an investor and patient perspective, albeit noisier to measure (Drug Discov. Today 22, 1749–1753; 2017).
What changed? Our analysis indicates that the proximate cause of the resurgence was the same as the prior decline: changes in success rates that changed the costs asso-ciated with failed NMEs. The data shown in Fig. 1c illustrate the estimated impact on the development costs per NME split between successful and failed molecules for 3 selected years over the past 3 decades. Success rates, particularly in late- stage R&D, declined precipitously during the period of declining R&D productivity, but levelled off and began to increase approximately 5 years ago, driving the turnaround in R&D productivity.
This turnaround in the timing and amount of attrition could only be achieved as a result of one or more of three main factors. The first is better information for decisions — that is, better knowledge of disease biology or how to modulate it, leading to new ways to treat diseases for which therapies are already available and/or side- stepping the ‘better than the Beatles’ problem by moving into diseases that lack effective therapies. A second, related factor is better use of that information;
Breaking Eroom’s LawMichael S. Ringel, Jack W. Scannell, Mathias Baedeker and Ulrik Schulze Ir
yna_
L/iS
tock
/Get
ty Im
ages
Plu
s
Num
ber o
f NM
Es p
er b
illio
n U
S$ R
&D
spe
ndin
g
100
a
10
1.0
0.11940 1960 1980 2000 2020
Cost of failureCost of molecule
Δ: By 2018, 0.7 more NMEs per billion US$R&D spending
Eroom’s Law published with data up to 2010 Pe
ak s
ales
(US$
bill
ions
) of N
MEs
per
bill
ion
US$
R&
D s
pend
ing
10
b
1.0
0.11990 2000 2010 2020
Δ: By 2018, $0.3 billion more peak sales per billion US$ R&D spending
Eroom’s Law published with data up to 2010
All-
in c
ost o
f dev
elop
men
t (U
S$ b
illio
ns) p
er N
ME
1.5
c
1.0
0.5
01990 2004 2013
56%
44%
18%
40%
60%
82%
Fig. 1 | Breaking Eroom’s Law. a | Count of new molecular entities (NMEs) per billion US$ R&D spending. b | Aggregate peak sales (US$ billions) of NMEs per billion US$ R&D spending. c | All- in cost of development (US$ billions) per NME. See Supplementary Box 1 for details of the data and analysis.
volume 19 | December 2020 | 833
From the AnAlyst’s couch
nAture reviews | Drug DiscovEry
N E W S & A N A LY S I S

productivity (PLoS One 11, e0147215; 2016), and others have previously linked the use of human genetic data to improved success rates in clini cal develop ment (Nat. Rev. Drug Discov. 17, 167–181; 2018). Based on these data as well as our direct impressions from working with multiple biopharma companies, we believe the better informa-tion derived from human genetics has been an important factor in the breaking of Eroom’s Law.
One implication of pursuing targets with human genetic validation is that this could, on average, result in drug approvals covering smaller populations, given that many mala-dies traditionally treated as single diseases based on their clinical presentation often have heterogeneous underlying mechanisms. As shown in Fig. 2b, we identified a statisti-cally significant trend (P < 3 × 10−8) towards approvals covering more focused indications within particular diseases, as assessed by the share of approvals made at International Statistical Classification of Diseases and Related Health Problems version 10 (ICD-10) levels lower than 3.
In addition, many rare diseases are caused by specific genetic variants and there has been substantial progress in identi-fying these genes. This knowledge provides a strong scientific basis for drug develop-ment, and, indeed, there has been a signif-icant (P < 2 × 10−5) shift in the proportion of NMEs that treat rare diseases (Fig. 2c). Furthermore, as rare diseases often lack specific therapies, drugs for rare diseases may circumvent the ‘better than the Beatles’ problem.
This trend towards smaller patient populations is also a plausible explanation for why the count version of Eroom’s Law (Fig. 1a) is more radically broken than the value- adjusted version (Fig. 1b), as these approved NMEs could have smaller sales per approval than those for larger populations.
set too stringently. Another contributor could be a shift in drug development to areas with a different risk–benefit ratio, such as diseases that had previously been under-served, particularly those that lacked specific therapies. Indeed, as already noted, there has been a shift in the proportion of NMEs that treat rare diseases (Fig. 2c). While it is not necessarily the case that the regulatory threshold would be lower for such diseases, FDA leaders have noted that the risk–benefit balance for new drugs is different when there are no existing therapies. There are examples from particularly severe diseases where it appears a lower regulatory thresh-old has been acceptable, such as the approval of eteplirsen for the treatment of Duchenne muscular dystrophy, suggesting that this factor might also be partly responsible for the breaking of Eroom’s Law.
ConclusionsThe data presented in this article support the hypothesis that there has been a turnaround in pharma R&D, and that it can be ascribed at least in part to the availability of better information and improvements in the use of that information. Unfortunately, this is not a prediction that the underlying forces that caused the prior decline, such as the ‘better than the Beatles’ problem, have gone away. We believe they persist and will again take hold once the effects of the recent improvements in understanding of disease biology and decision making wane. Furthermore, there are new pressures on the horizon, such as increasing uncertainty in the future payment for innovation, that have the potential to inhibit R&D productivity. Nevertheless, for the next few years at least, companies that take advantage of better information and decision making could continue to reap the rewards and outperform those that do not.
Michael S. Ringel1 ✉, Jack W. Scannell2, Mathias Baedeker3 and Ulrik Schulze4
1Boston Consulting Group, Boston, MA, USA.2University of Edinburgh, Edinburgh, UK.
3Boston Consulting Group, Munich, Germany.4Boston Consulting Group, Zürich, Switzerland.
✉e- mail: [email protected]
https://doi.org/10.1038/d41573-020-00059-3
AcknowledgementsThe authors thank Q. N. Vuong for analytical support and P. Kirkpatrick for valuable commentary on an earlier draft.
Competing interestsM.S.R., M.B. and U.S. are employees of The Boston Consulting Group (BCG), a management consultancy that works with the world’s leading biopharmaceutical companies. The research for this specific article was funded by BCG’s Health Care practice.
Supplementary informationSupplementary information is available for this paper at https://doi.org/10.1038/d41573-020-00059-3.
Better use of information. Regarding ‘better decision- making processes’, there are two major types of deviation from optimal decision making: irrational and rational.
On the irrational side, several known cognitive biases can be particularly important in drug R&D, including overvaluing optionality, optimism bias and loss aversion, which can set the threshold to terminate failing programmes at too high a level. Rational factors can be relevant wherever there is a difference between the actions that are optimal for an individual within a company and the actions that are optimal for the company, such as the potential for ‘progression- seeking’ behaviour rather than ‘truth- seeking’ behaviour in drug R&D if employees’ personal incentives are disproportionately aligned with the continuation of drug projects (Nat. Rev. Drug Discov. 15, 441–442; 2016).
Our personal experience in direct consultation with the majority of the top 20 pharmaceutical companies is that they are making improvements to their decision- making processes. Some compan ies have also reported improvements in their R&D productivity, attributed in part to improved decision making (Nat. Rev. Drug Discov. 17, 167–181; 2018; Nat. Rev. Drug Discov. 15, 441–442; 2016). So, although the available evidence is limited, it supports the hypothesis that improvements in decision making by at least some companies could have contributed to Eroom’s Law being broken.
Changes to the threshold for approval. The last potential factor is a change in the thresh-old for approval. This could be via a change in the overall risk tolerance of the regula-tory agencies, which we do not consider, although we note that it could be rational if there is better on- market monitoring or if there is evidence that prior thresholds were
Perc
enta
ge
50a b c
40
30
20
10
02010 2012 2014 2016 2018
38
36
34
32
30
28
01990 2000 2010 2020
R2 = 0.78P < 3 x 10–8
R2 = 0.78P < 9 x 10–3
R2 = 0.67P < 2 x 10–5
60
40
20
02000 2005 2010 2015 2020
Fig. 2 | Analysis of factors that could contribute to Eroom’s Law being broken. a | Percentage of new molecular entities (NMEs) with a supporting genome- wide association study (GWAS) at least 5 years before approval, scaled by the number of GWAS available. b | Seven- year rolling average for the percentage of NMEs approved at indications lower than ICD-10 level 3. c | Percentage of NMEs designated as treatments for rare diseases. See Supplementary Box 1 for details of the data and analysis.
834 | December 2020 | volume 19 www.nature.com/nrd
N E W S & A N A LY S I S