Brainstem Stroke Annegret Dahlmann-Noor Consultant in Paediatric Ophthalmology and Strabismus Wales...
44
Brainstem Stroke Annegret Dahlmann-Noor Consultant in Paediatric Ophthalmology and Strabismus Wales and West Vision Conference 26 June2015
-
Upload
gwenda-douglas -
Category
Documents
-
view
228 -
download
3
Transcript of Brainstem Stroke Annegret Dahlmann-Noor Consultant in Paediatric Ophthalmology and Strabismus Wales...
Brainstem StrokeAnnegret Dahlmann-NoorConsultant in Paediatric Ophthalmology and Strabismus
Wales and West Vision Conference
26 June2015
www.moorfields.nhs.uk
BackgroundIncidence:
Each year in England, approximately 110,000 people have a first or recurrent stroke and a further 20,000 people have a transient ischaemic attack
Wales: 11,000 have a first or recurrent stroke per year, of which 6,000 new stroke events
More than 900,000 people in England are living with the effects of stroke, with half of these being dependent on other people for help with everyday activities
Eye movement problems after stroke
Eye movement problems after stroke
www.moorfields.nhs.uk
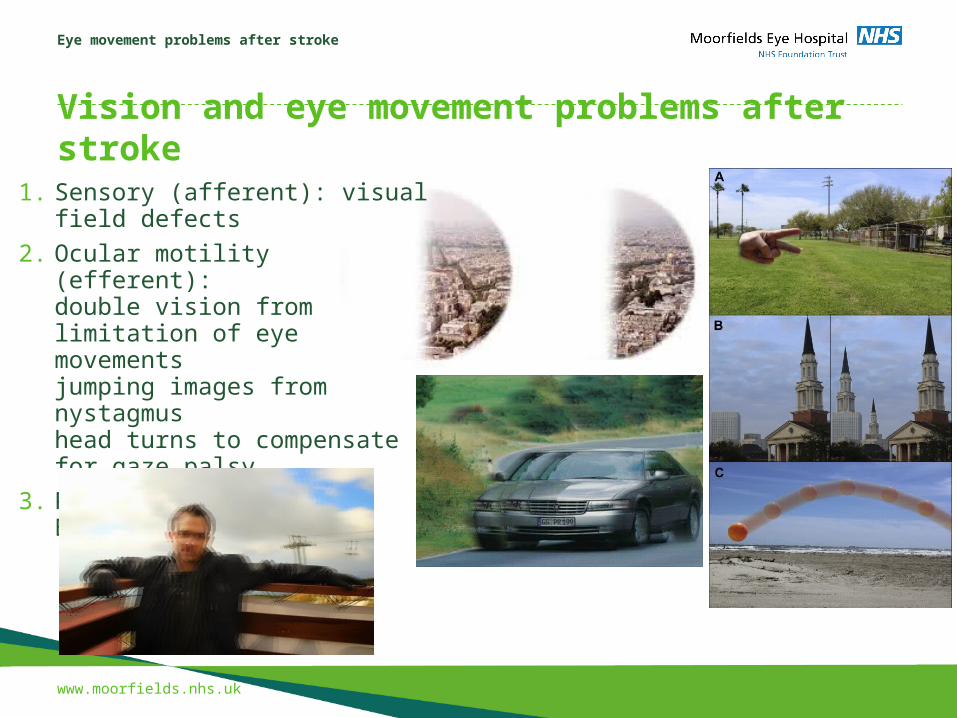
Vision and eye movement problems after stroke1. Sensory (afferent): visual field
defects
2. Ocular motility (efferent):double vision from limitation of eye movementsjumping images from nystagmushead turns to compensate for gaze palsy
3. Processing: Charles Bonnet, palinopsia

Eye movement problems after stroke
www.moorfields.nhs.uk
BackgroundMost strokes are ischaemic (80-85%), some are haemorrhagic
Two main blood supplies to the brain:
1) Carotid
2) Vertebral/basilar arteries
Eye movement problems after stroke
www.moorfields.nhs.uk
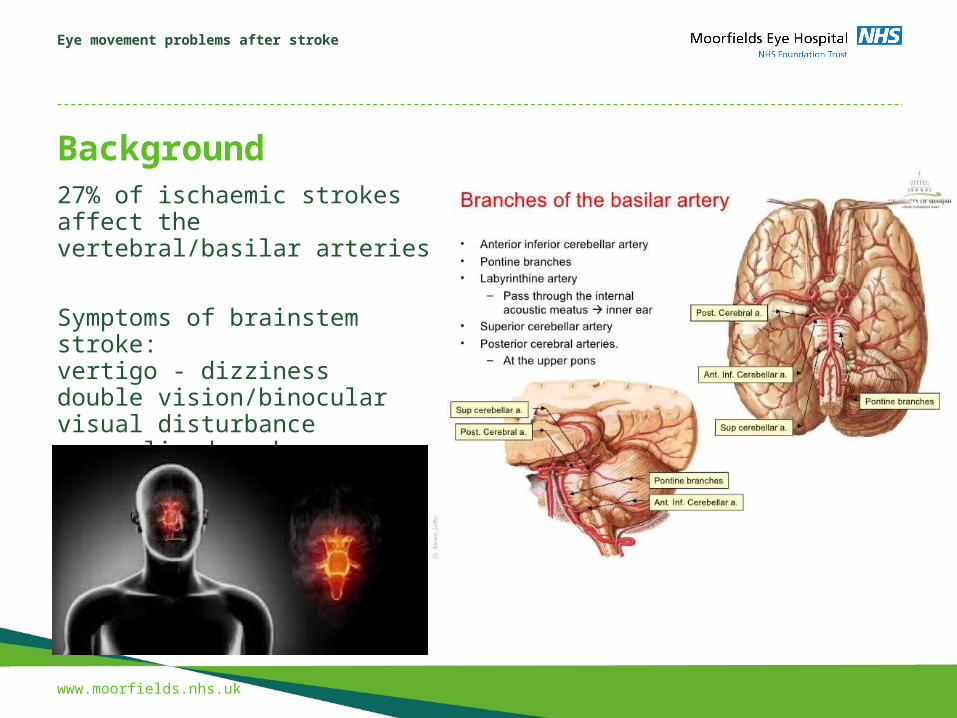
Background27% of ischaemic strokes affect the vertebral/basilar arteries
Symptoms of brainstem stroke: vertigo - dizzinessdouble vision/binocular visual disturbance generalised weakness
Eye movement problems after stroke
www.moorfields.nhs.uk
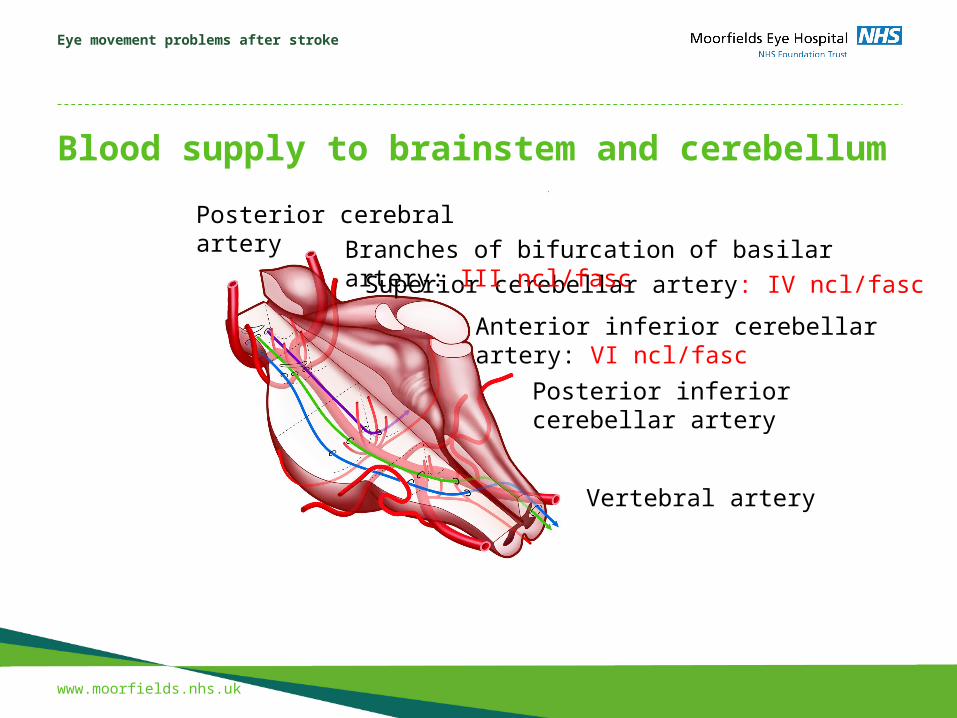
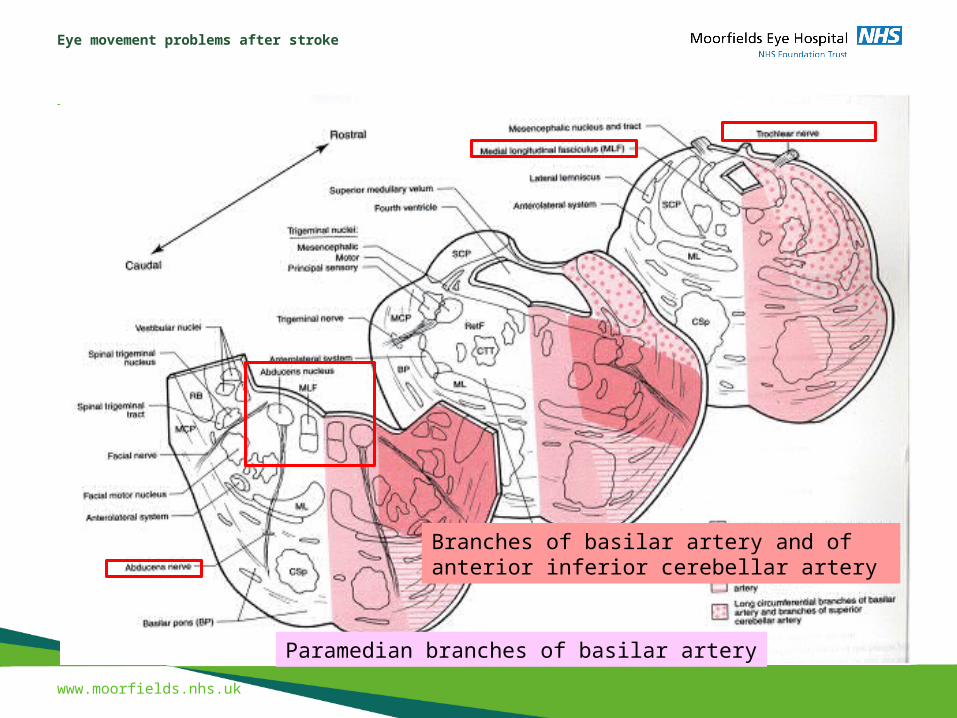
Blood supply to brainstem and cerebellum
Posterior cerebral artery
Superior cerebellar artery: IV ncl/fasc
Anterior inferior cerebellar artery: VI ncl/fasc
Posterior inferior cerebellar artery
Vertebral artery
Branches of bifurcation of basilar artery: III ncl/fasc
Eye movement problems after stroke
www.moorfields.nhs.uk
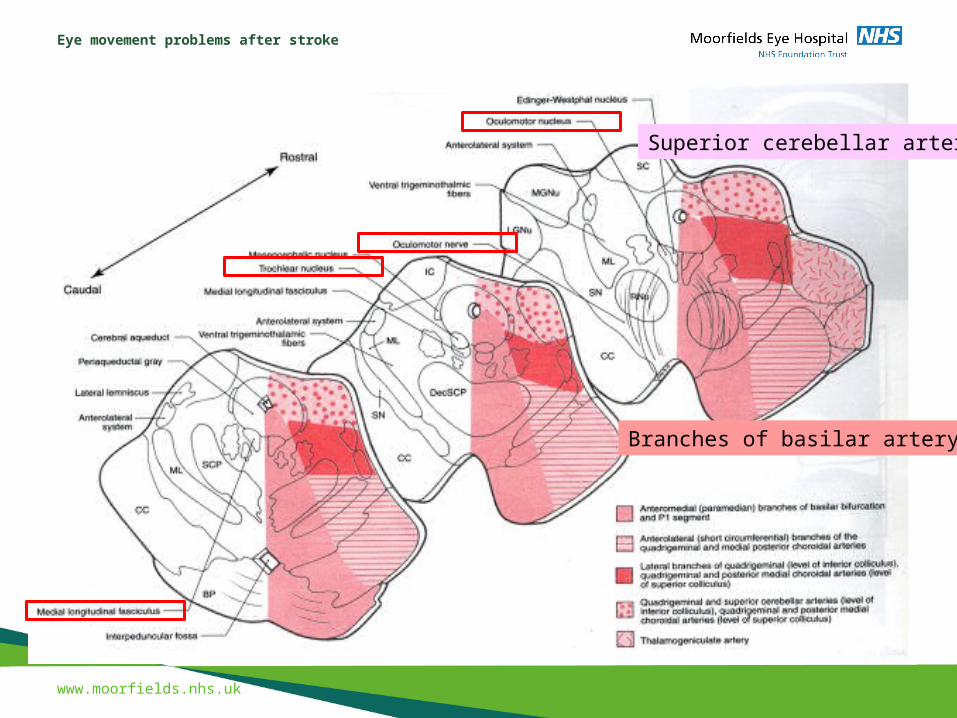
Superior cerebellar artery
Branches of basilar artery
Eye movement problems after stroke
www.moorfields.nhs.uk
Paramedian branches of basilar artery
Branches of basilar artery and of anterior inferior cerebellar artery
Eye movement problems after stroke
www.moorfields.nhs.uk
Eye movements• Smooth pursuit: eyes follow a moving target
• Saccades: gaze rapidly jumps from one fixation point to another
• Vergence eye movements: eyes do not move in parallel, but in relation to each other: convergence: when looking at something close up
• Vestibulo-ocular reflex (VOR): the signal triggering eye movements comes from the balance organ (labyrinth), which keps the image of the visual surroundings stable on the retina during head movements
• Optokinetic reflex: triggered by moving visual targets, consists of smooth pursuit and saccades
• Gaze holding: ability to keep the eyes in an eccentric position
Eye movement problems after stroke
www.moorfields.nhs.uk
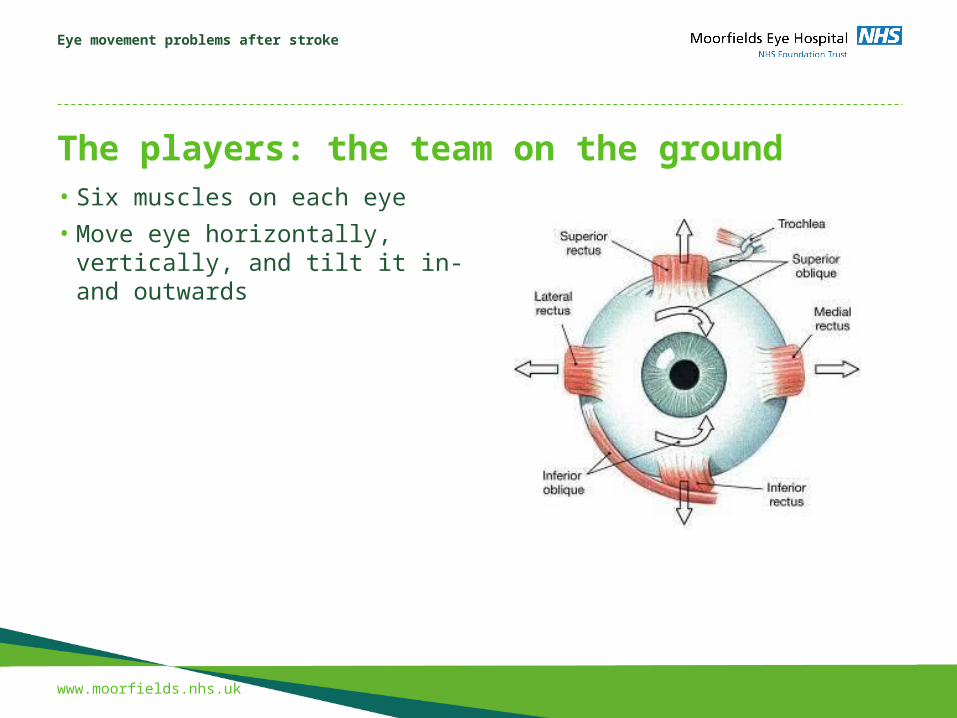
The players: the team on the ground• Six muscles on each eye
• Move eye horizontally, vertically, and tilt it in- and outwards
Eye movement problems after stroke
www.moorfields.nhs.uk
The players: the middle managementVertical eye movements
• Interstitial nucleus of Cajal (INC)
• Rostral interstitial nucleus of the MLF (riMLF)
Horizontal eye movements
• Parapontine reticular formation (PPRF)
• Abducens nucleusThe runner:
Medial longitudinal fasciculus (MLF)

Eye movement problems after stroke
www.moorfields.nhs.uk
The playersVertical eye movements
• Interstitial nucleus of Cajal
• Rostral interstitial nucleus of the MLF
Horizontal eye movements
• Paramedian pontine reticular formation
• Abducens nucleus
Eye movement problems after stroke
www.moorfields.nhs.uk
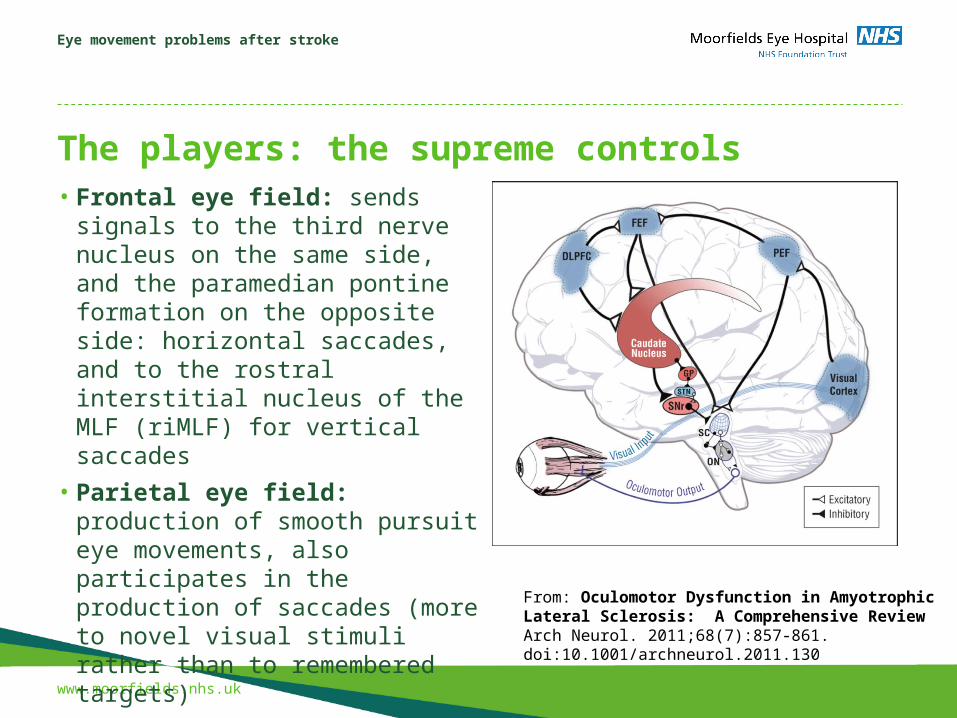
The players: the supreme controls• Frontal eye field: sends signals to the
third nerve nucleus on the same side, and the paramedian pontine formation on the opposite side: horizontal saccades, and to the rostral interstitial nucleus of the MLF (riMLF) for vertical saccades
• Parietal eye field: production of smooth pursuit eye movements, also participates in the production of saccades (more to novel visual stimuli rather than to remembered targets)
• Paramedian pontine reticular formation: excitatory burst neurons that start the “pulse”
From: Oculomotor Dysfunction in Amyotrophic Lateral Sclerosis: A Comprehensive ReviewArch Neurol. 2011;68(7):857-861. doi:10.1001/archneurol.2011.130
Eye movement problems after stroke
www.moorfields.nhs.uk
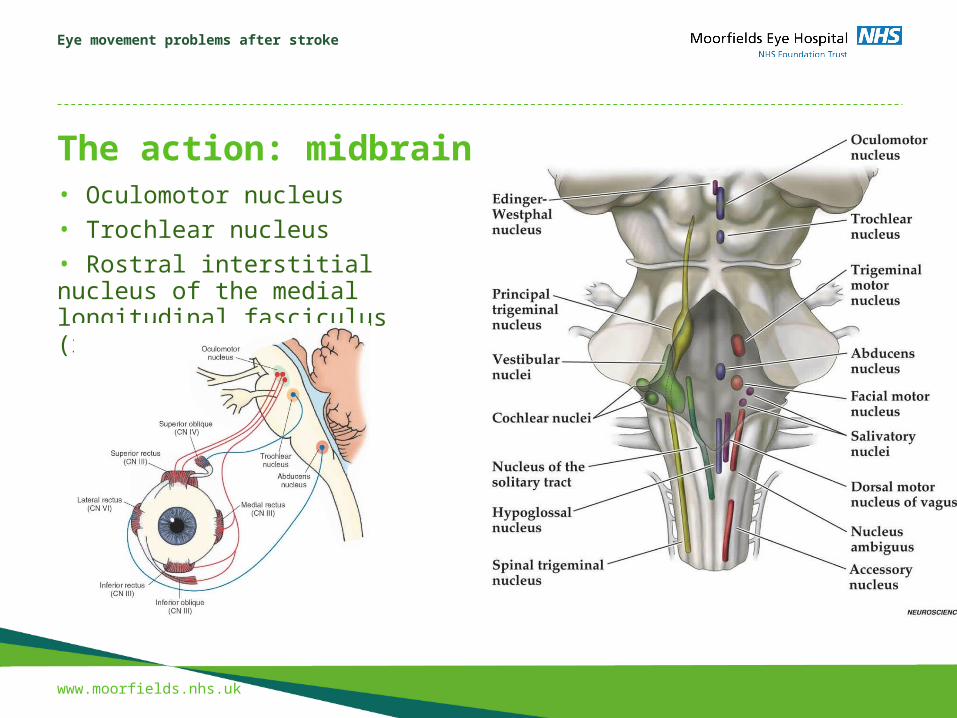
The action: midbrain• Oculomotor nucleus• Trochlear nucleus• Rostral interstitial nucleus of the medial longitudinal fasciculus (riMLF)
Presentation title to go here
www.moorfields.nhs.uk
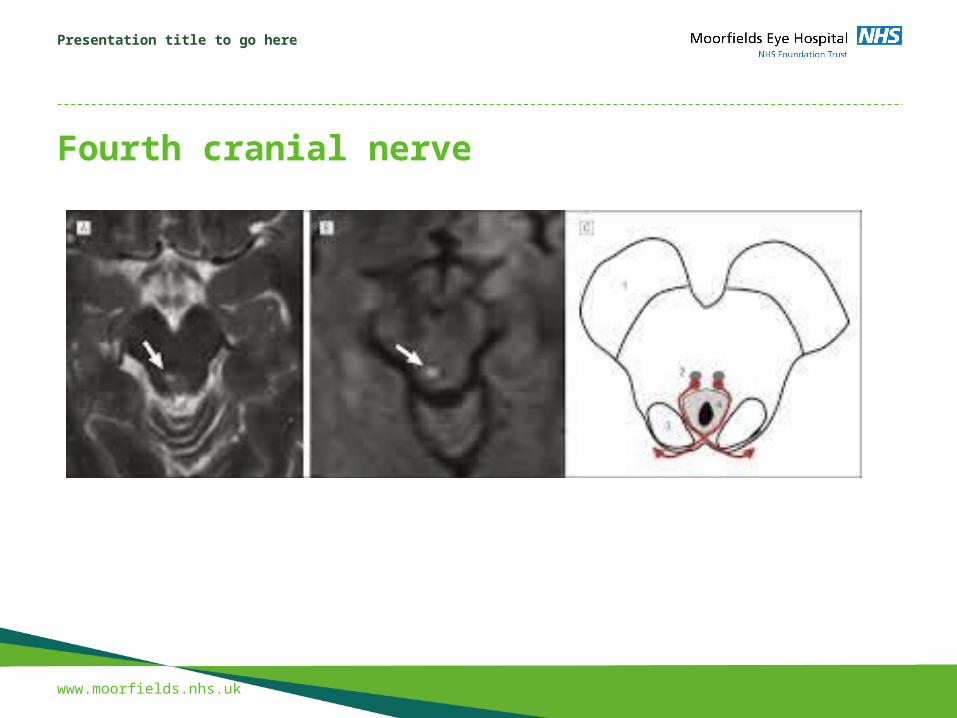
Fourth cranial nerve
Presentation title to go here
www.moorfields.nhs.uk
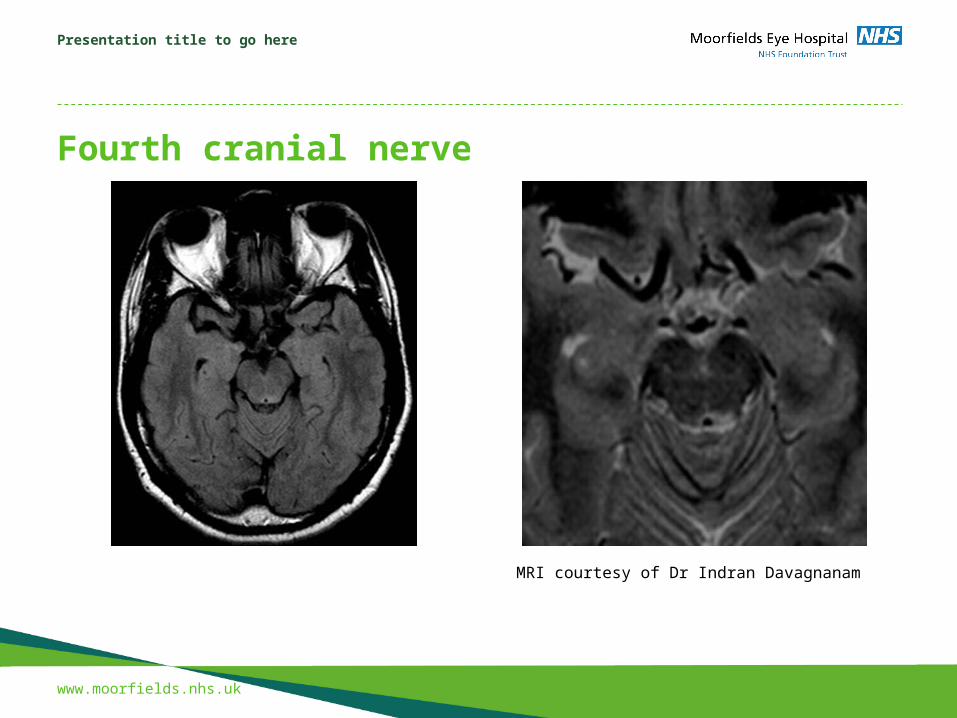
Fourth cranial nerve
MRI courtesy of Dr Indran Davagnanam
Presentation title to go here
www.moorfields.nhs.uk
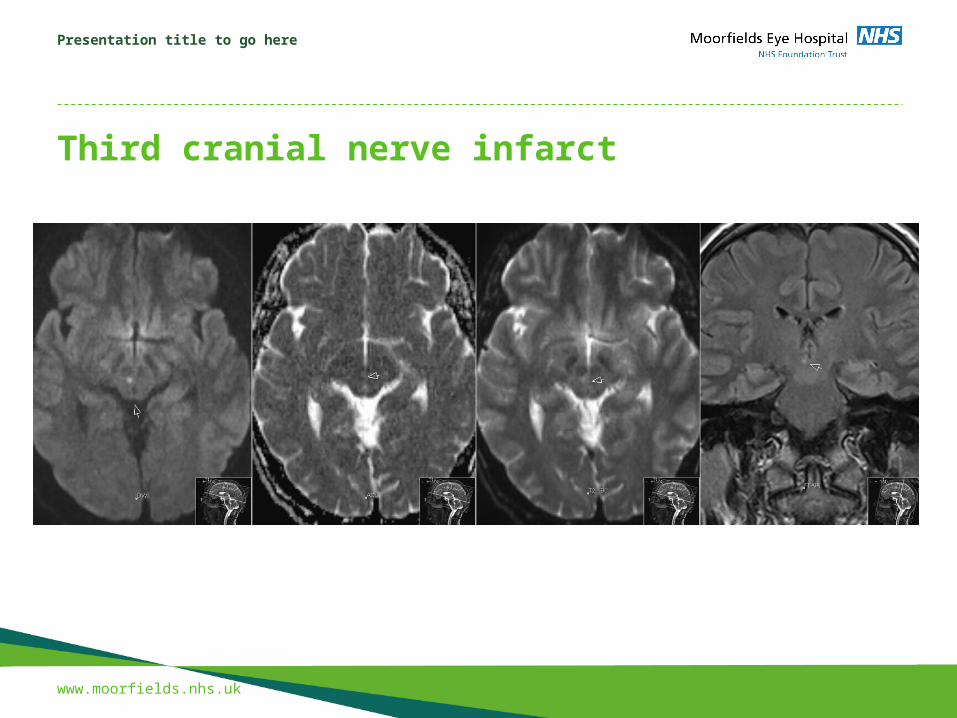
Third cranial nerve infarct

Presentation title to go here
www.moorfields.nhs.uk
Oculomotor nerve paresis• lack of adduction: eye deviated outwards• lack of elevation: eye deviated downwards• lid droop (ptosis)
Eye movement problems after stroke
www.moorfields.nhs.uk
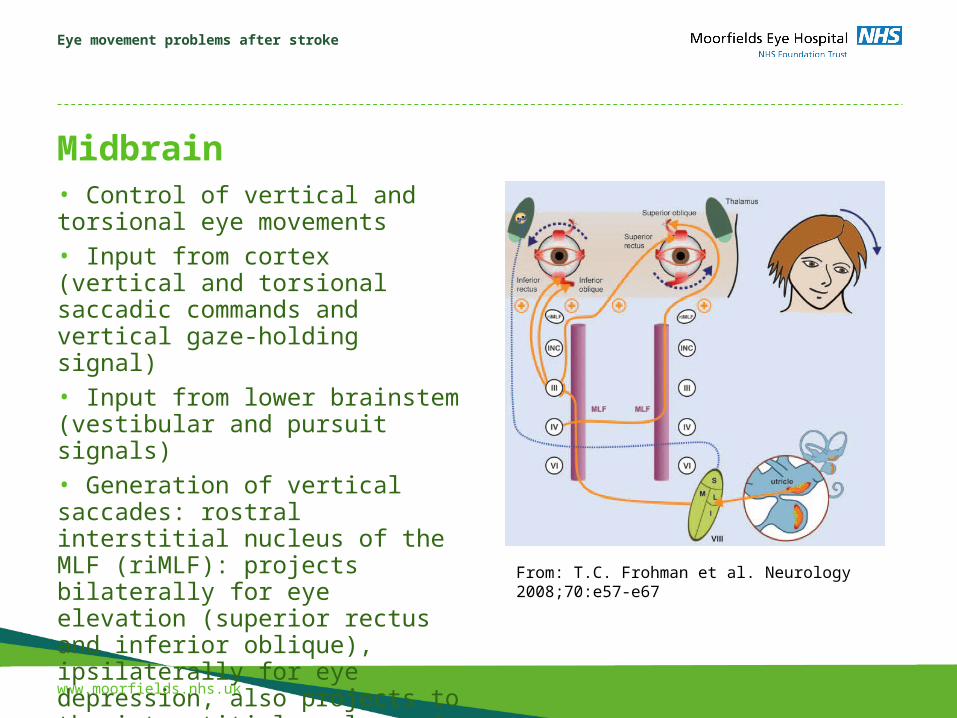
Midbrain• Control of vertical and torsional eye movements• Input from cortex (vertical and torsional saccadic commands and vertical gaze-holding signal)• Input from lower brainstem (vestibular and pursuit signals)• Generation of vertical saccades: rostral interstitial nucleus of the MLF (riMLF): projects bilaterally for eye elevation (superior rectus and inferior oblique), ipsilaterally for eye depression, also projects to the interstitial nucleus of Cajal (INC) From: T.C. Frohman et al. Neurology 2008;70:e57-e67
Eye movement problems after stroke
www.moorfields.nhs.uk
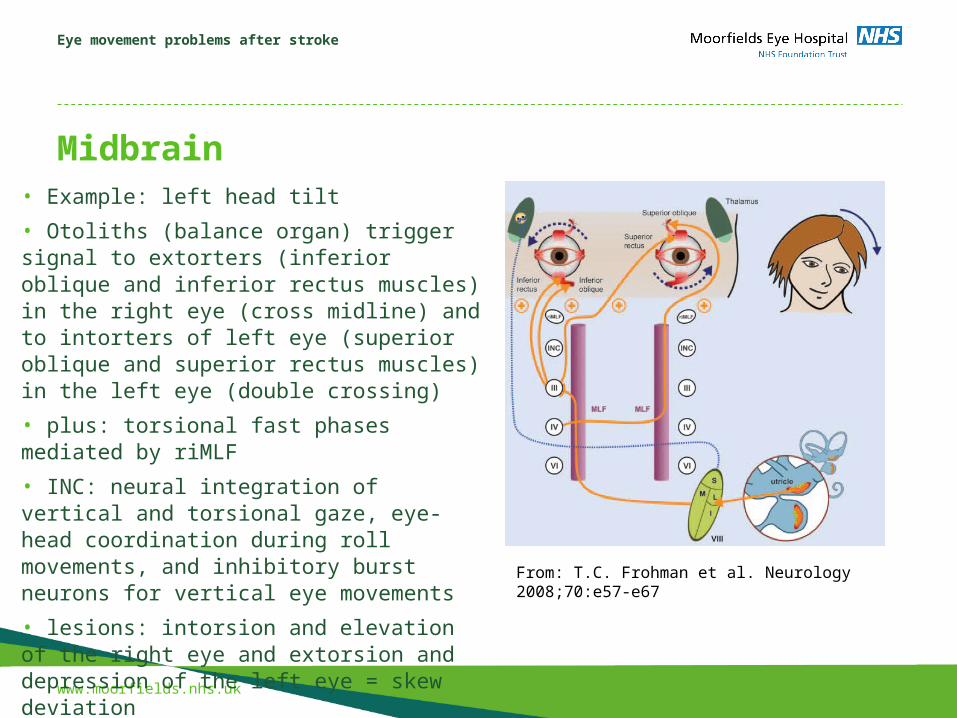
Midbrain• Example: left head tilt
• Otoliths (balance organ) trigger signal to extorters (inferior oblique and inferior rectus muscles) in the right eye (cross midline) and to intorters of left eye (superior oblique and superior rectus muscles) in the left eye (double crossing)
• plus: torsional fast phases mediated by riMLF
• INC: neural integration of vertical and torsional gaze, eye-head coordination during roll movements, and inhibitory burst neurons for vertical eye movements
• lesions: intorsion and elevation of the right eye and extorsion and depression of the left eye = skew deviation From: T.C. Frohman et al. Neurology 2008;70:e57-e67
Eye movement problems after stroke
www.moorfields.nhs.uk
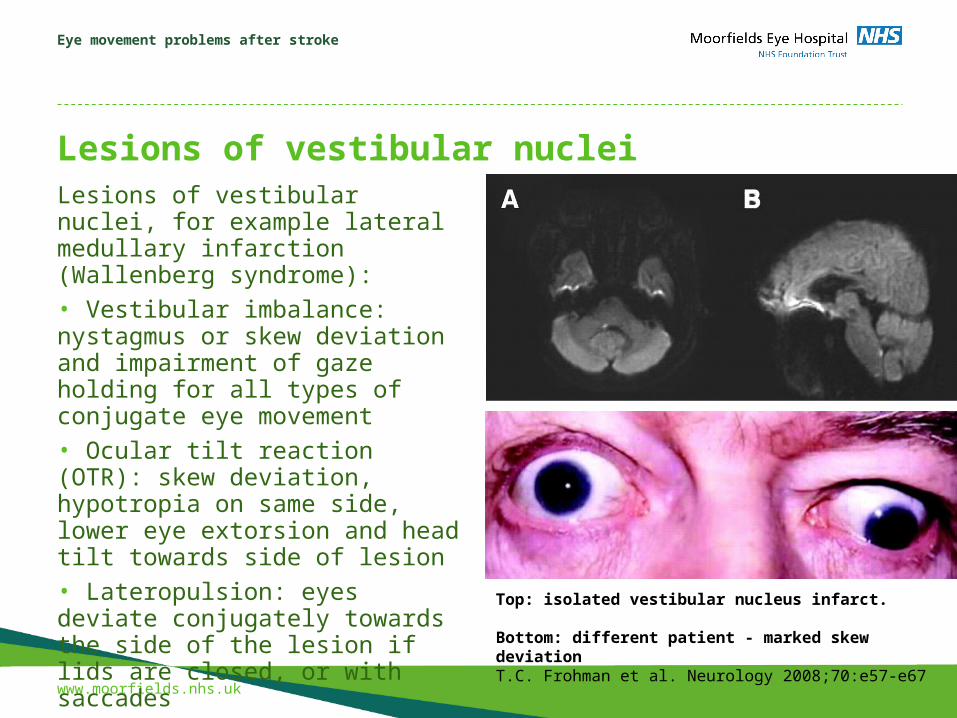
Lesions of vestibular nucleiLesions of vestibular nuclei, for example lateral medullary infarction (Wallenberg syndrome):• Vestibular imbalance: nystagmus or skew deviation and impairment of gaze holding for all types of conjugate eye movement• Ocular tilt reaction (OTR): skew deviation, hypotropia on same side, lower eye extorsion and head tilt towards side of lesion • Lateropulsion: eyes deviate conjugately towards the side of the lesion if lids are closed, or with saccades Top: isolated vestibular nucleus infarct.
Bottom: different patient - marked skew deviationT.C. Frohman et al. Neurology 2008;70:e57-e67
Eye movement problems after stroke
www.moorfields.nhs.uk
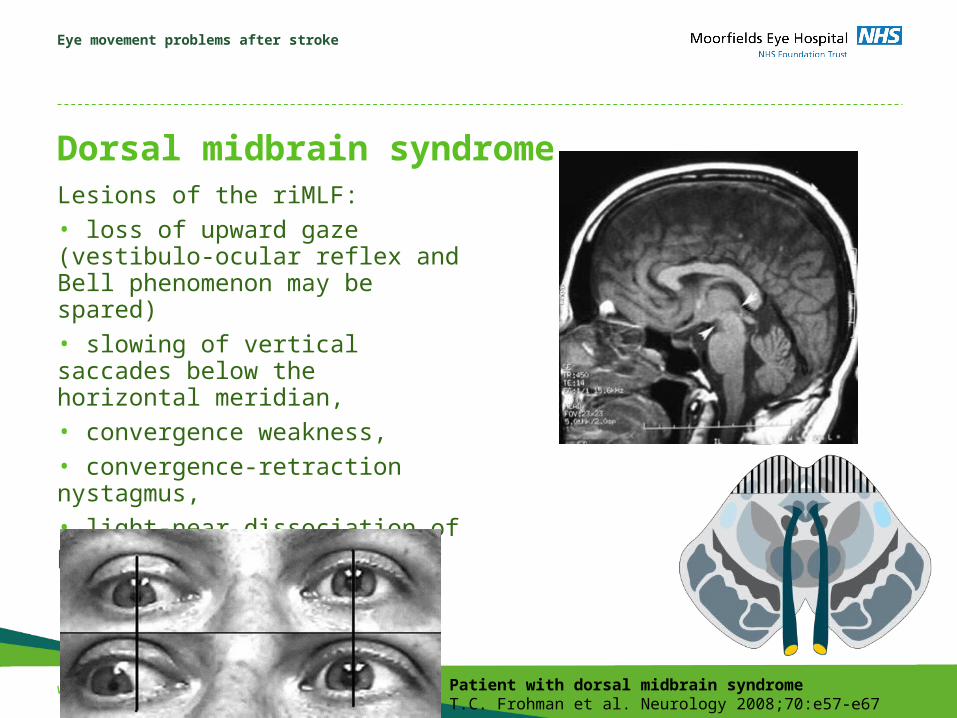
Dorsal midbrain syndromeLesions of the riMLF: • loss of upward gaze (vestibulo-ocular reflex and Bell phenomenon may be spared)• slowing of vertical saccades below the horizontal meridian, • convergence weakness, • convergence-retraction nystagmus, • light-near dissociation of pupils,• lid retraction
Patient with dorsal midbrain syndromeT.C. Frohman et al. Neurology 2008;70:e57-e67
Eye movement problems after stroke
www.moorfields.nhs.uk
Stop and recap• 1. Strokes affecting the basilar artery or its brances can affect eye movements, causing double vision and jumping images• 2. There are different types of eye movements – smooth pursuit, saccades, vergences, and eye movements in response to changes in head or body position• 3. Areas in the cortex trigger saccades (fast eye movements) and pursuits.• 4. Centres in the midbrain forward signals to the cranial nerves which innervate the eye muscles that move the eyes vertically and in torsion.• 5. Lesions in these pathways can cause loss of saccades and vertical eye movements, and a complex change in vertical and torsional eye movements (skey deviation)

Eye movement problems after stroke
www.moorfields.nhs.uk
Now the easy stuff: horizontal eye movements• Abducens nucleus

Eye movement problems after stroke
www.moorfields.nhs.uk
Horizontal eye movements
1. Two types of nerve fibres in the abducens nerve:a) motoneurons to lateral rectus muscle on the same sideb) internuclear neurons, which project up the contralateral medial longitudinal fasciculus to contact medial rectus motoneurons of the oculomotor nucleus
=> Conjugate, horizontal eye movements
. Details of the descending projection involved in the volitional control of horizontal saccadic eye movements. Excitatory pathways are shown in orange and the reciprocal inhibitory pathways are shown in blue. T.C. Frohman et al. Neurology 2008;70:e57-e67

Eye movement problems after stroke
www.moorfields.nhs.uk
Abducens nucleus
1. Inputs: vestibular and optokinetic inputs from vestibular nuclei
2. Saccadic commands originate from burst neurons of the pontine and medullary reticular formation
3. Descending smooth pursuit pathway via cerebellar nuclei to abducens nucleus
.
Projections involved in the activation of the left lateral semicircular canal. This figure illustrates the projections involved during the activation of the left lateral semicircular canal. T.C. Frohman et al. Neurology 2008;70:e57-e67
Eye movement problems after stroke
www.moorfields.nhs.uk
Stop and recap
1. From the abducens nucleus, signals go the lateral rectus muscle on the same side and medial rectus on the opposite side
2. Those signals are triggered by messages from the vestibular nuclei (tilting head), cerebellar nuclei (moving body), burst neurons in the PPRF, and the frontal and parietal eye fields.
Eye movement problems after stroke
www.moorfields.nhs.uk
How things can go wrong in brainstem stroke1. Abducens nucleus lesions
2. Medial longitudinal fasciculus lesions
3. Combined lesions of MLF and abducens nucleus
4. PPRF lesion
Eye movement problems after stroke
www.moorfields.nhs.uk
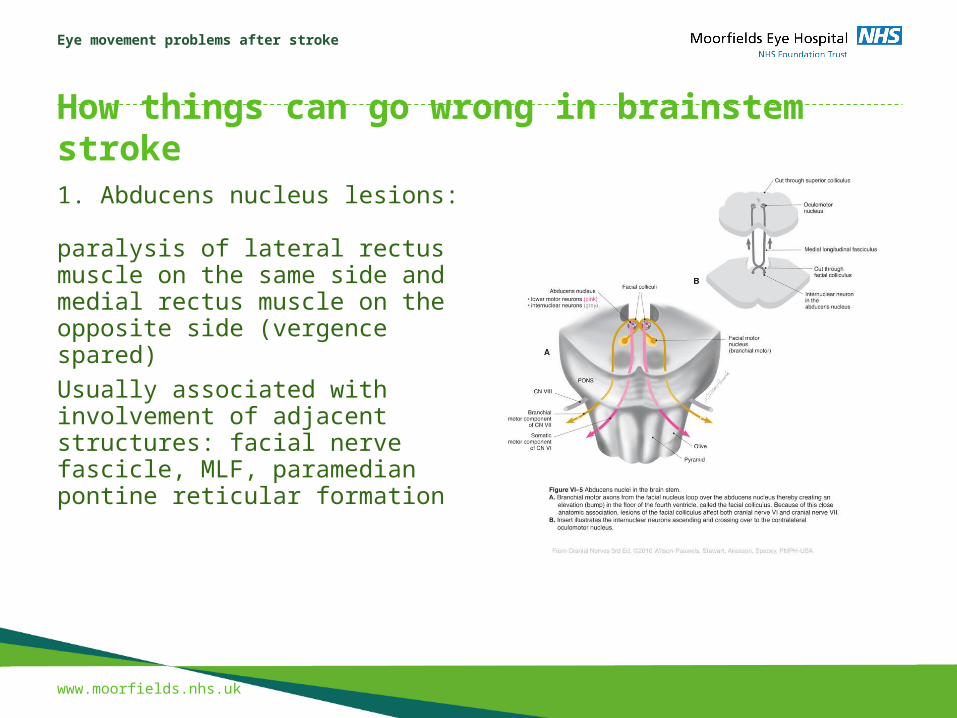
How things can go wrong in brainstem stroke1. Abducens nucleus lesions: paralysis of lateral rectus muscle on the same side and medial rectus muscle on the opposite side (vergence spared)
Usually associated with involvement of adjacent structures: facial nerve fascicle, MLF, paramedian pontine reticular formation
Eye movement problems after stroke
www.moorfields.nhs.uk
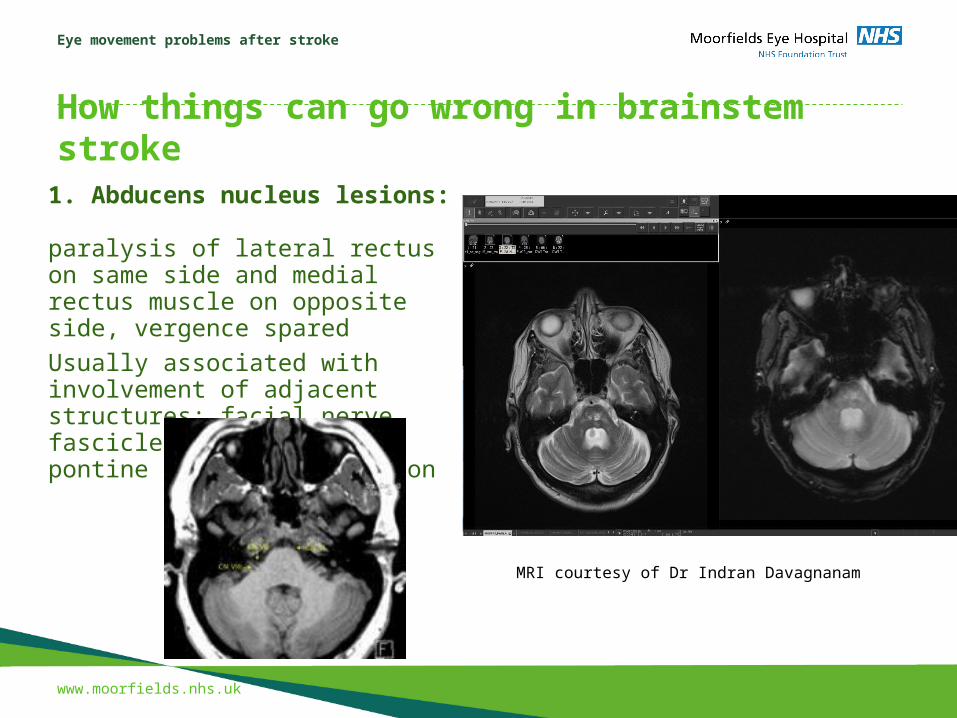
How things can go wrong in brainstem stroke1. Abducens nucleus lesions: paralysis of lateral rectus on same side and medial rectus muscle on opposite side, vergence spared
Usually associated with involvement of adjacent structures: facial nerve fascicle, MLF, paramedian pontine reticular formation
MRI courtesy of Dr Indran Davagnanam
Eye movement problems after stroke
www.moorfields.nhs.uk
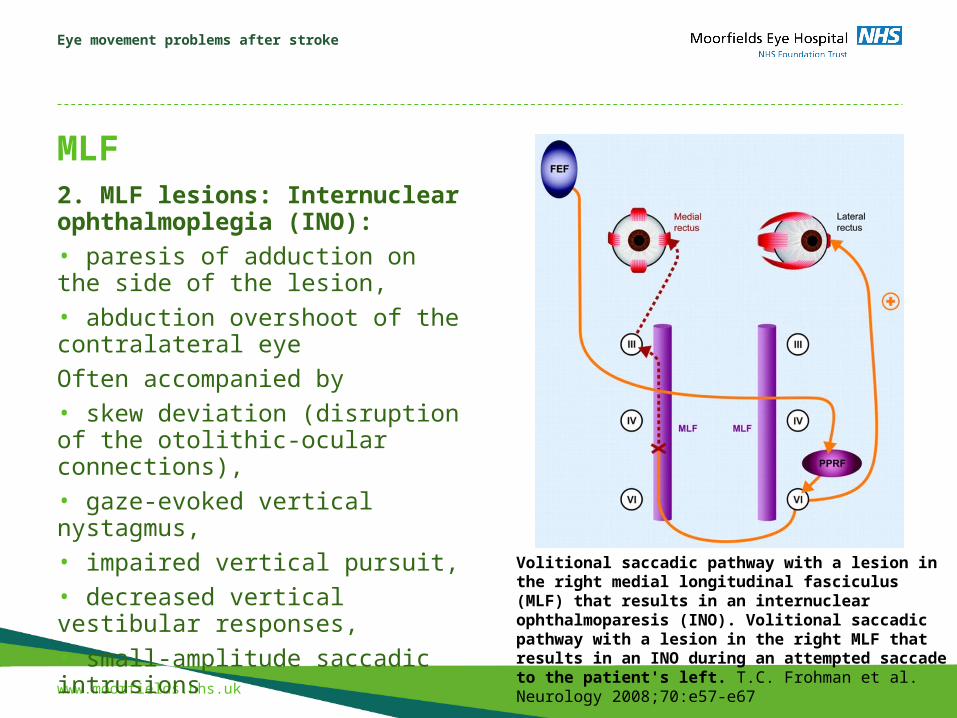
MLF2. MLF lesions: Internuclear ophthalmoplegia (INO): • paresis of adduction on the side of the lesion,• abduction overshoot of the contralateral eye
Often accompanied by • skew deviation (disruption of the otolithic-ocular connections), • gaze-evoked vertical nystagmus,• impaired vertical pursuit, • decreased vertical vestibular responses, • small-amplitude saccadic intrusions
Volitional saccadic pathway with a lesion in the right medial longitudinal fasciculus (MLF) that results in an internuclear ophthalmoparesis (INO). Volitional saccadic pathway with a lesion in the right MLF that results in an INO during an attempted saccade to the patient's left. T.C. Frohman et al. Neurology 2008;70:e57-e67
Eye movement problems after stroke
www.moorfields.nhs.uk
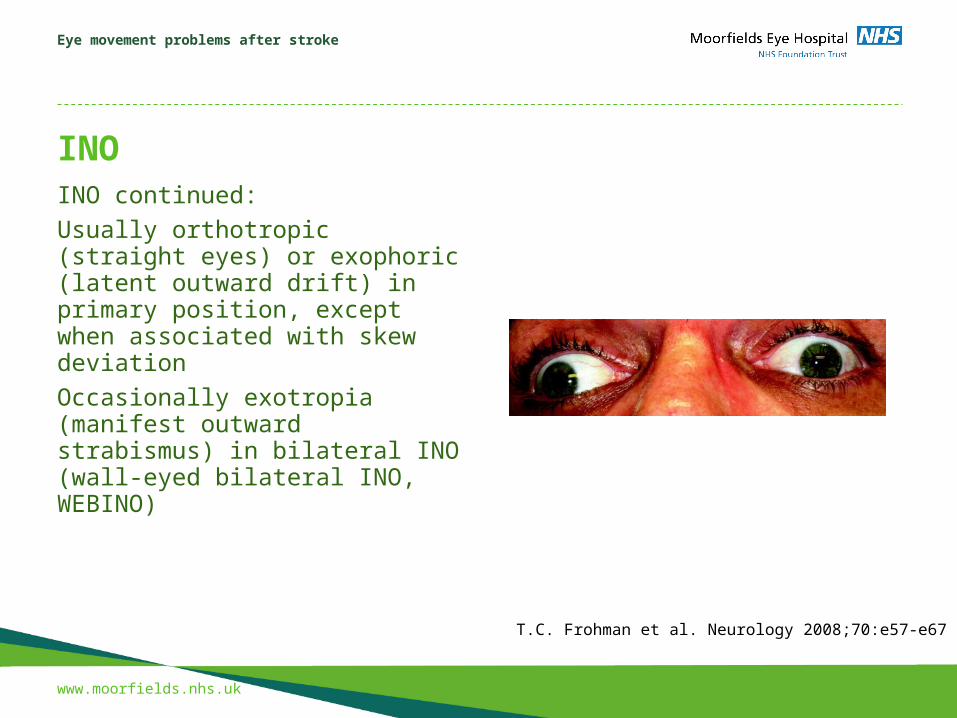
INOINO continued:
Usually orthotropic (straight eyes) or exophoric (latent outward drift) in primary position, except when associated with skew deviation
Occasionally exotropia (manifest outward strabismus) in bilateral INO (wall-eyed bilateral INO, WEBINO)
T.C. Frohman et al. Neurology 2008;70:e57-e67
Eye movement problems after stroke
www.moorfields.nhs.uk
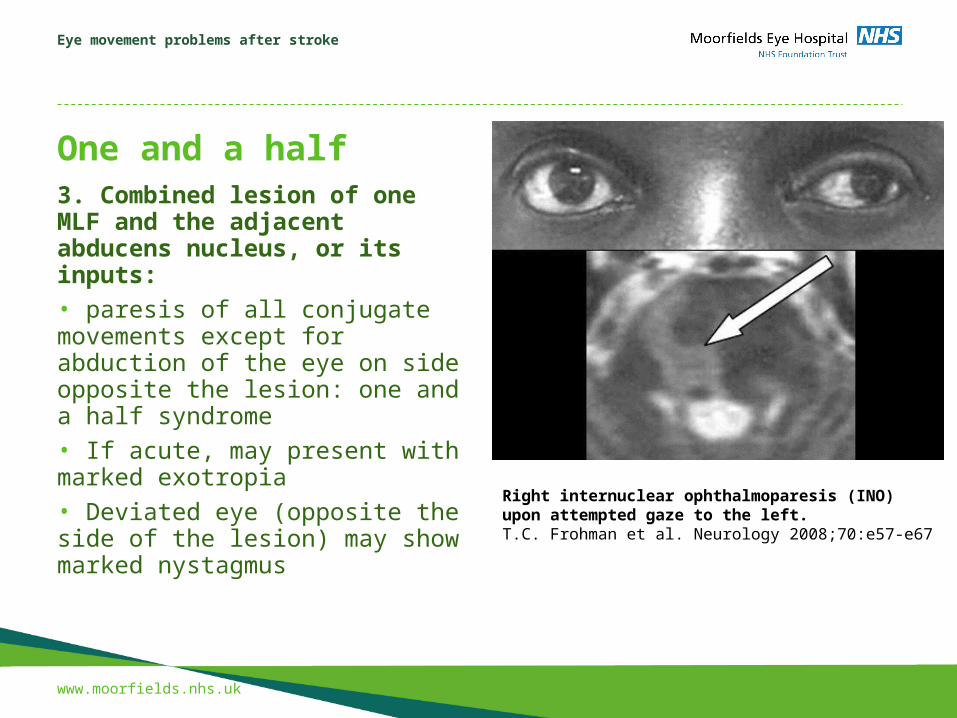
One and a half3. Combined lesion of one MLF and the adjacent abducens nucleus, or its inputs: • paresis of all conjugate movements except for abduction of the eye on side opposite the lesion: one and a half syndrome• If acute, may present with marked exotropia• Deviated eye (opposite the side of the lesion) may show marked nystagmus
Right internuclear ophthalmoparesis (INO) upon attempted gaze to the left. T.C. Frohman et al. Neurology 2008;70:e57-e67
Eye movement problems after stroke
www.moorfields.nhs.uk
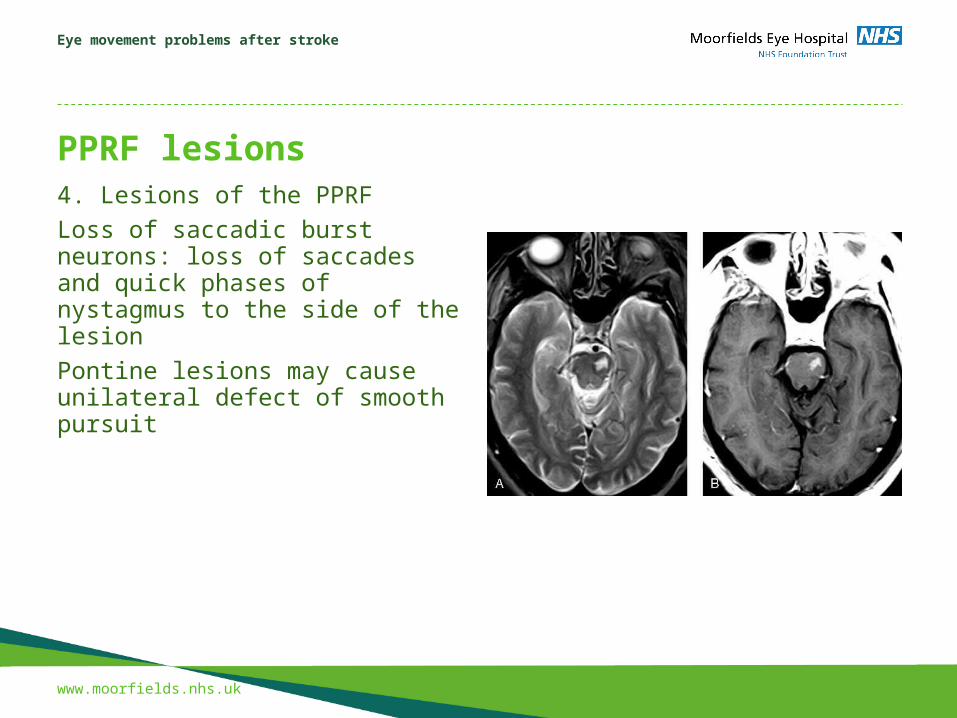
PPRF lesions4. Lesions of the PPRF
Loss of saccadic burst neurons: loss of saccades and quick phases of nystagmus to the side of the lesion
Pontine lesions may cause unilateral defect of smooth pursuit

Eye movement problems after stroke
www.moorfields.nhs.uk
Stop and recap
1. Abducens nucleus lesions: loss of abduction same side, loss of adduction opposite side; often involve PPRF as well, so horizontal gaze palsy
2. Medial longitudinal fasciculus lesions: impaired adduction on the side of the lesion, abduction overshoot of the opposite eye
3. Combined lesions of MLF and abducens nucleus: affects all horizontal eye movements except for abduction on the side opposite the lesion
4. PPRF lesion: loss of saccades to the side of the lesion

Eye movement problems after stroke
www.moorfields.nhs.uk
The last part of the talk: cerebellum and cortex stroke
Eye movement problems after stroke
www.moorfields.nhs.uk
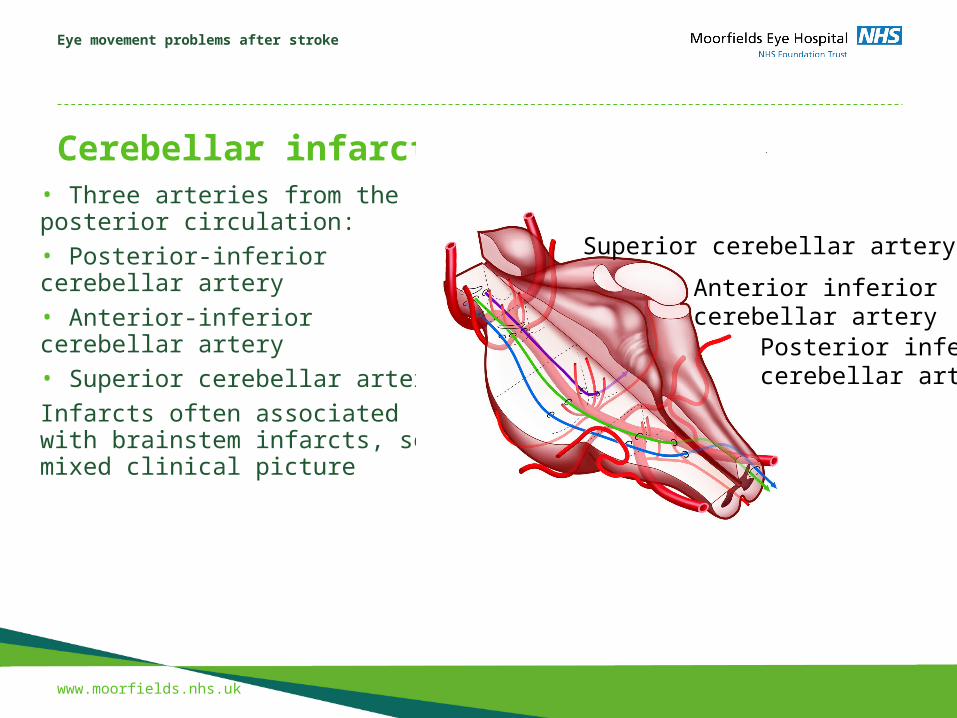
Cerebellar infarct• Three arteries from the posterior circulation:• Posterior-inferior cerebellar artery• Anterior-inferior cerebellar artery• Superior cerebellar artery
Infarcts often associated with brainstem infarcts, so mixed clinical picture
Superior cerebellar artery
Anterior inferior cerebellar artery
Posterior inferiorcerebellar artery
Eye movement problems after stroke
www.moorfields.nhs.uk
Cerebellar infarct
• Posterior-inferior cerebellar artery: acute vertigo and nystagmus, possibly gaze-evoked nystagmus
• Anterior-inferior cerebellar artery:vertigo, vomiting, hearing loss, facial palsy, ipsilateral limb ataxia
• Superior cerebellar artery: ataxia of gait and limbs and vertigo, saccadic contrapulsion (overshooting of contralateral saccades, undershooting of ipsilateral saccades; attempted vertical saccades are oblique)
Eye movement problems after stroke
www.moorfields.nhs.uk
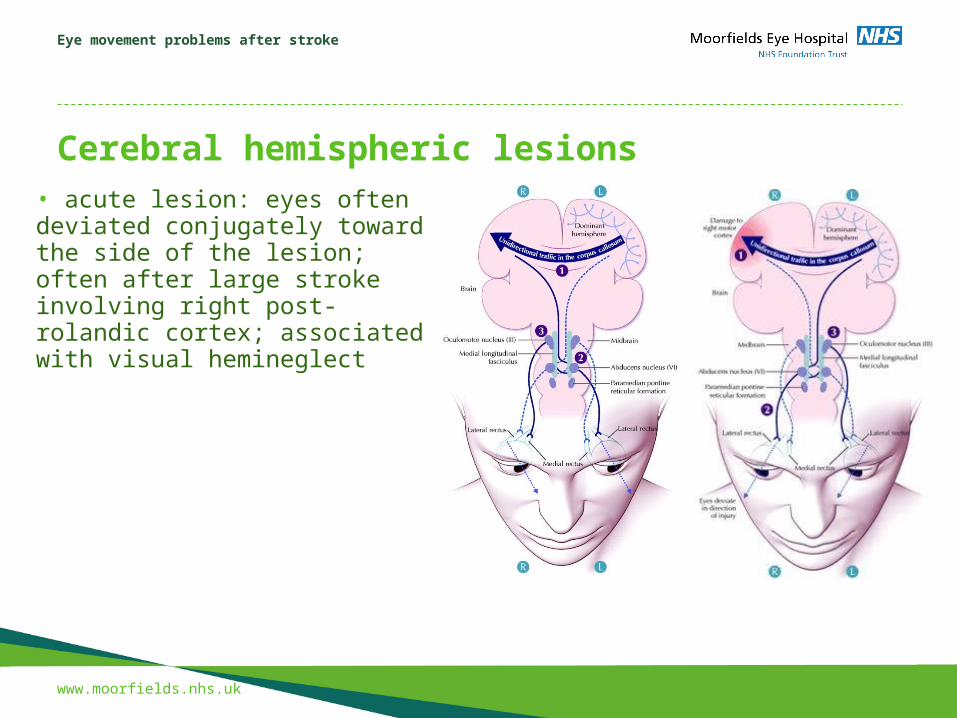
Cerebral hemispheric lesions • acute lesion: eyes often deviated conjugately toward the side of the lesion; often after large stroke involving right post-rolandic cortex; associated with visual hemineglect
Eye movement problems after stroke
www.moorfields.nhs.uk
Cerebral hemispheric lesions • chronic lesion: no resting deviation; persistence of gaze deviation• Small-amplitude nystagmus• Deficit of horizontal pursuit when tracking targets moving towards the side of the lesion (OKN)

Eye movement problems after stroke
www.moorfields.nhs.uk
Bilateral Frontoparietal lesions • Acquired Ocular Motor Apraxia• Loss of voluntary control of eye movements• Preservation of reflex movements, including vestibulo-ocular reflex and quick phases of nystagmus• Can be associated with difficulty in lid opening• Balint syndrome: loss of voluntary eye movements plus disturbance of visual attention
Eye movement problems after stroke
www.moorfields.nhs.uk
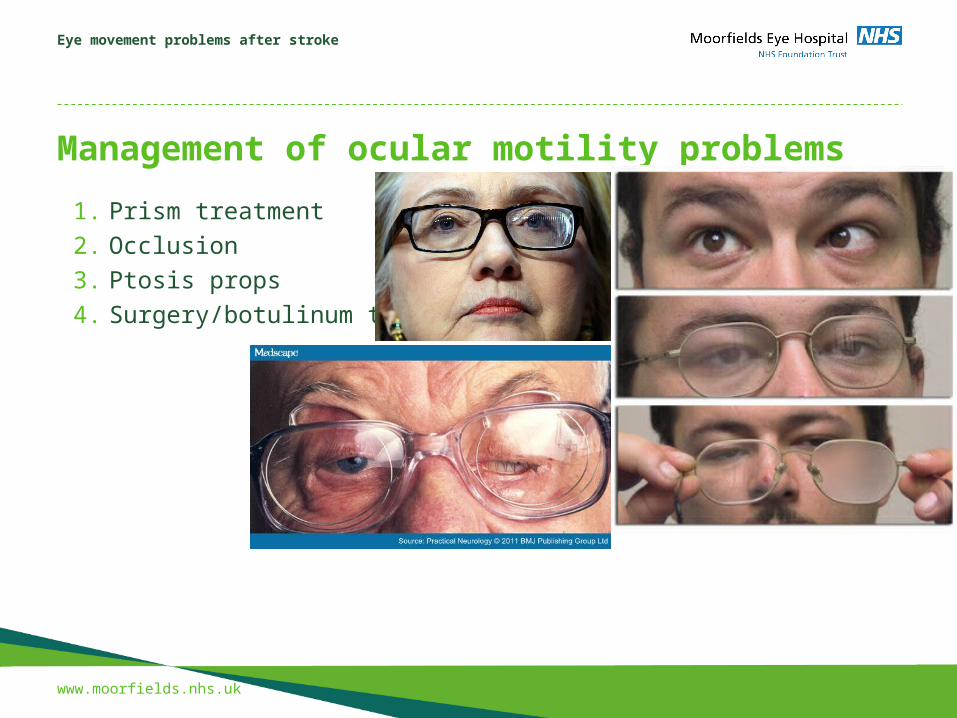
Management of ocular motility problems
1. Prism treatment
2. Occlusion
3. Ptosis props
4. Surgery/botulinum toxin
www.moorfields.nhs.uk
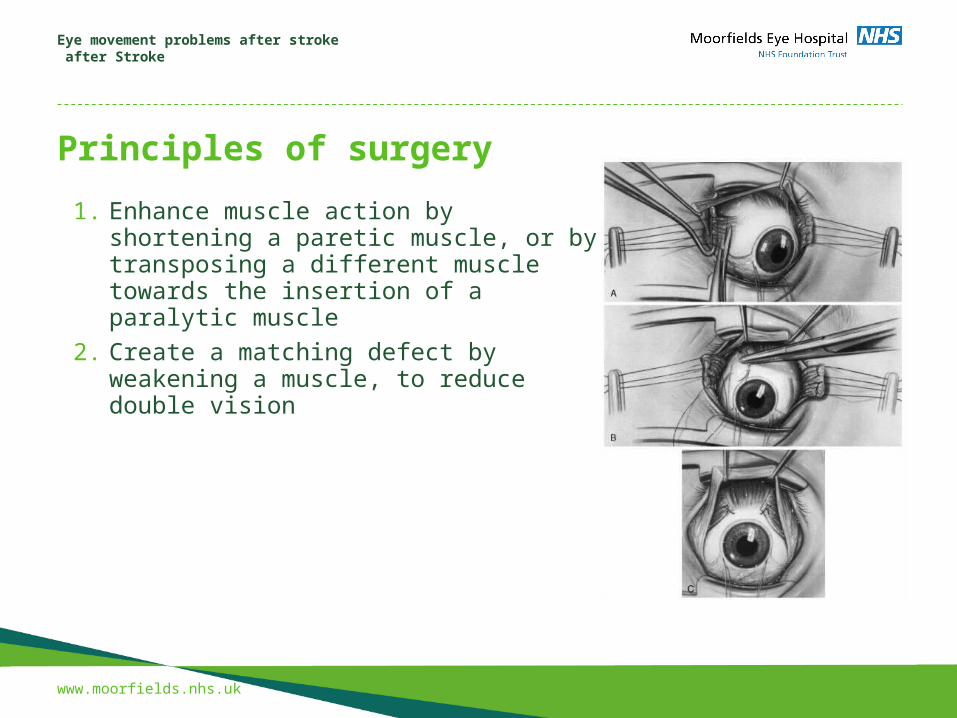
Principles of surgery
Eye movement problems after stroke after Stroke
1. Enhance muscle action by shortening a paretic muscle, or by transposing a different muscle towards the insertion of a paralytic muscle
2. Create a matching defect by weakening a muscle, to reduce double vision
Presentation title to go here
www.moorfields.nhs.uk
Thank you