
Brain ct and mri in icu
33
BRAIN CT AND MRI IN ICU SAMIR EL ANSARY
-
Upload
dr-mohamed-maged-kharabish -
Category
Health & Medicine
-
view
127 -
download
2
Transcript of Brain ct and mri in icu
BRAIN CT AND MRI IN ICU
SAMIR EL ANSARY
A Quick Primer of Brain CT/MRI
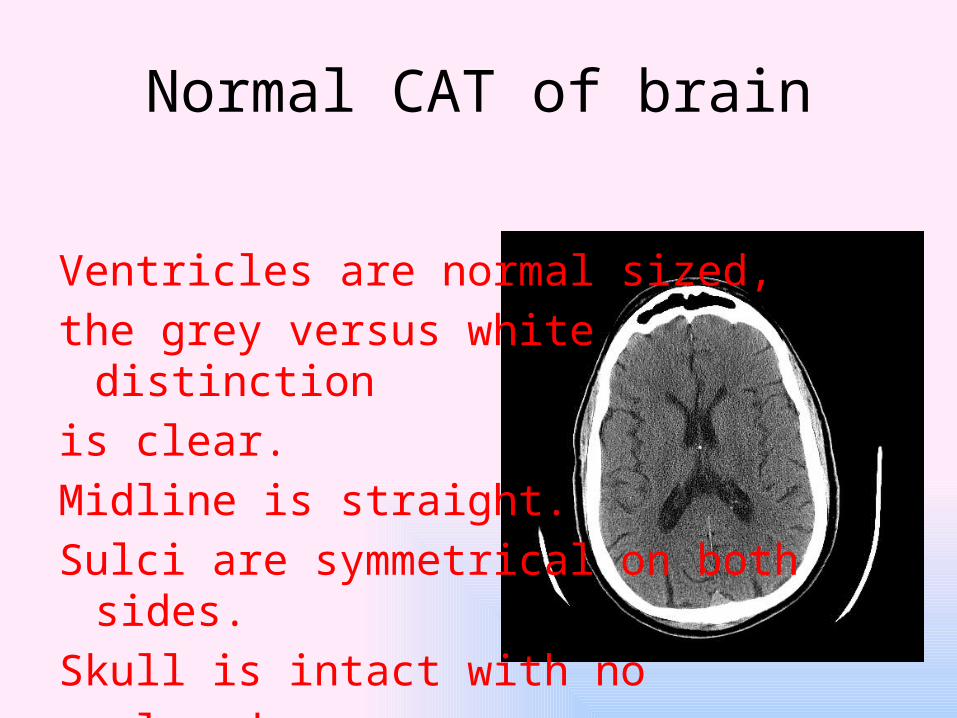
Normal CAT of brain
Ventricles are normal sized, the grey versus white distinctionis clear. Midline is straight. Sulci are symmetrical on both sides.Skull is intact with noscalp edema.
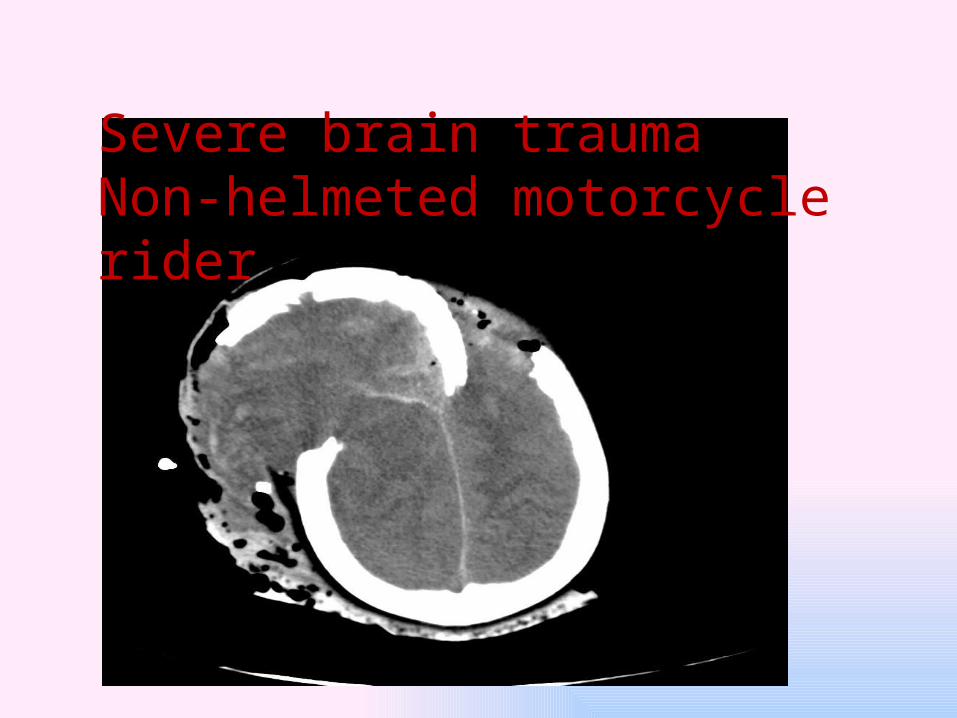
Severe brain traumaNon-helmeted motorcycle rider

CAT of Skull Fracture
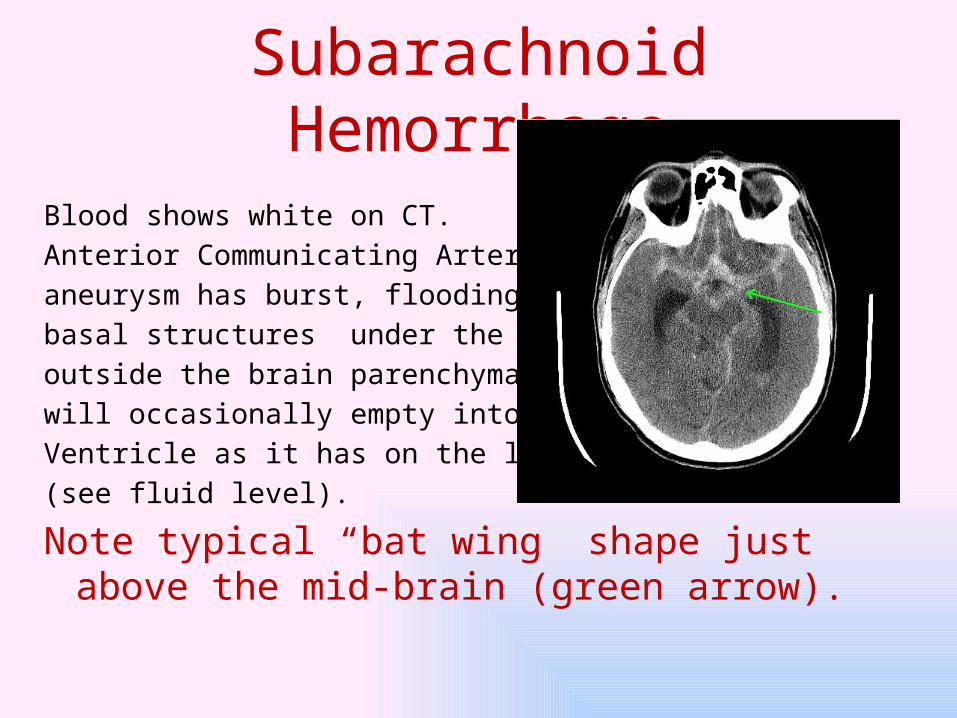
Subarachnoid Hemorrhage
Blood shows white on CT. Anterior Communicating Artery aneurysm has burst, flooding the basal structures under the brain outside the brain parenchyma, but will occasionally empty into a Ventricle as it has on the left here (see fluid level).
Note typical “bat wing” shape just above the mid-brain (green arrow).
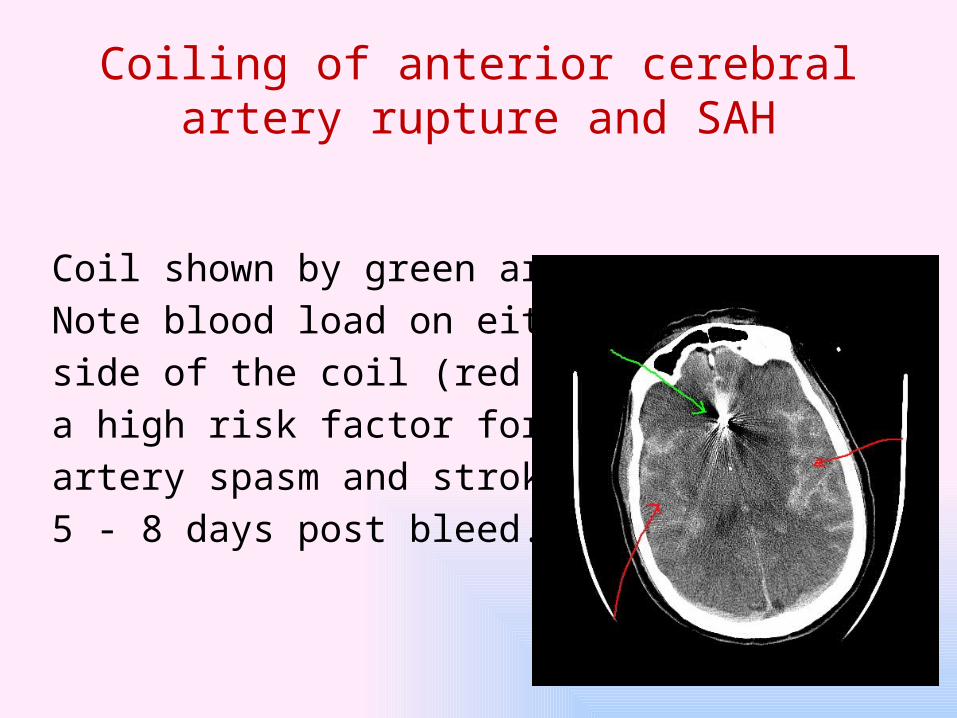
Coiling of anterior cerebral artery rupture and SAH
Coil shown by green arrow. Note blood load on either side of the coil (red arrows) a high risk factor for cerebral artery spasm and stroke 5 - 8 days post bleed.

Severe Subarachnoid Hemorrhage
Severe hemorrhage and probable clotting and obstruction at the 3rd ventricle and /or obstruction at the formena of Luschka and Magendie and 4th ventricle causing hydrocephalus. Poor outcome Likely.
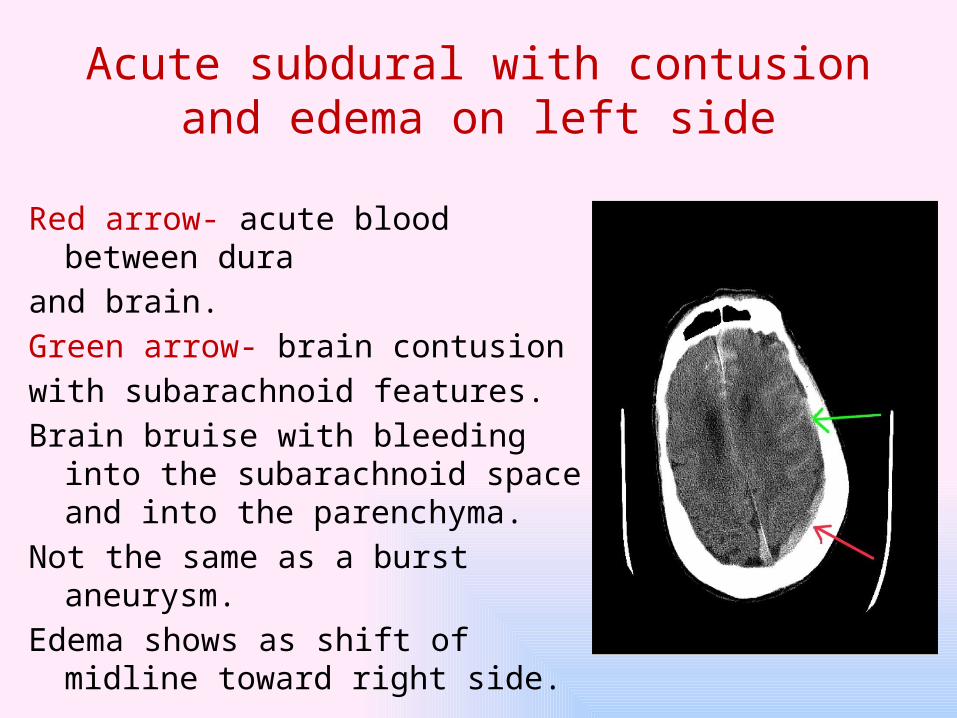
Acute subdural with contusion and edema on left side
Red arrow- acute blood between dura and brain. Green arrow- brain contusion with subarachnoid features. Brain bruise with bleeding into the
subarachnoid space and into the parenchyma.
Not the same as a burst aneurysm. Edema shows as shift of midline toward
right side.
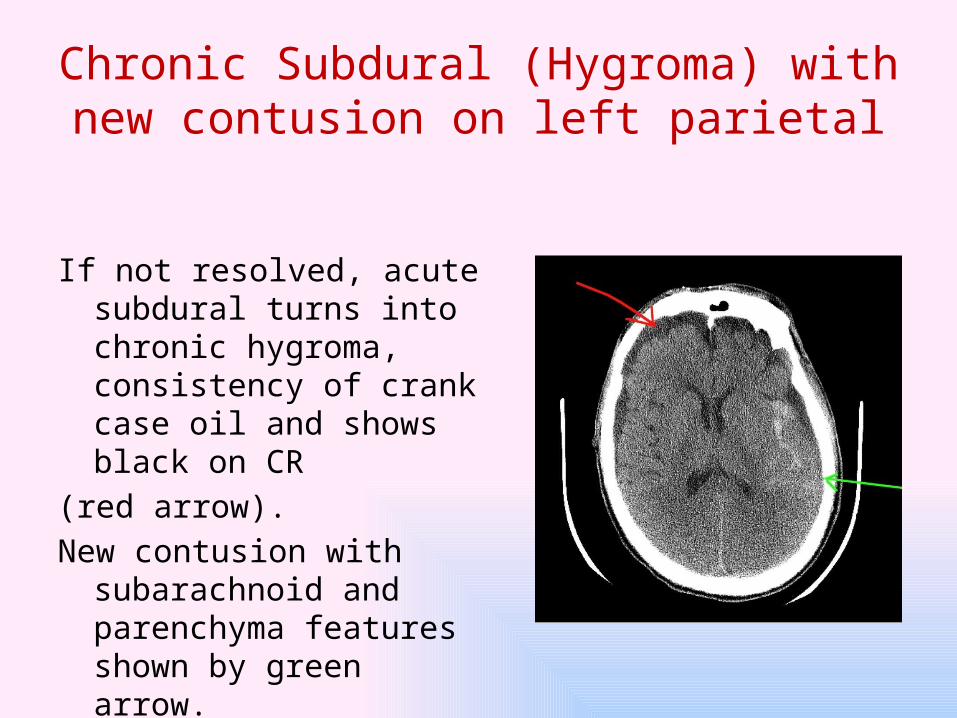
Chronic Subdural (Hygroma) with new contusion on left parietal
If not resolved, acute subdural turns into chronic hygroma, consistency of crank case oil and shows black on CR
(red arrow). New contusion with
subarachnoid and parenchyma features shown by green arrow.

Previous Prefrontal lobotomy as young adult in 50s
Performed by sticking lance shaped knife up into pre-frontal
brain through thin bone over eyeball and swishing back and forth. Very effective in calming agitated patients most of whom assume Hillary Clinton-like smile
permanently
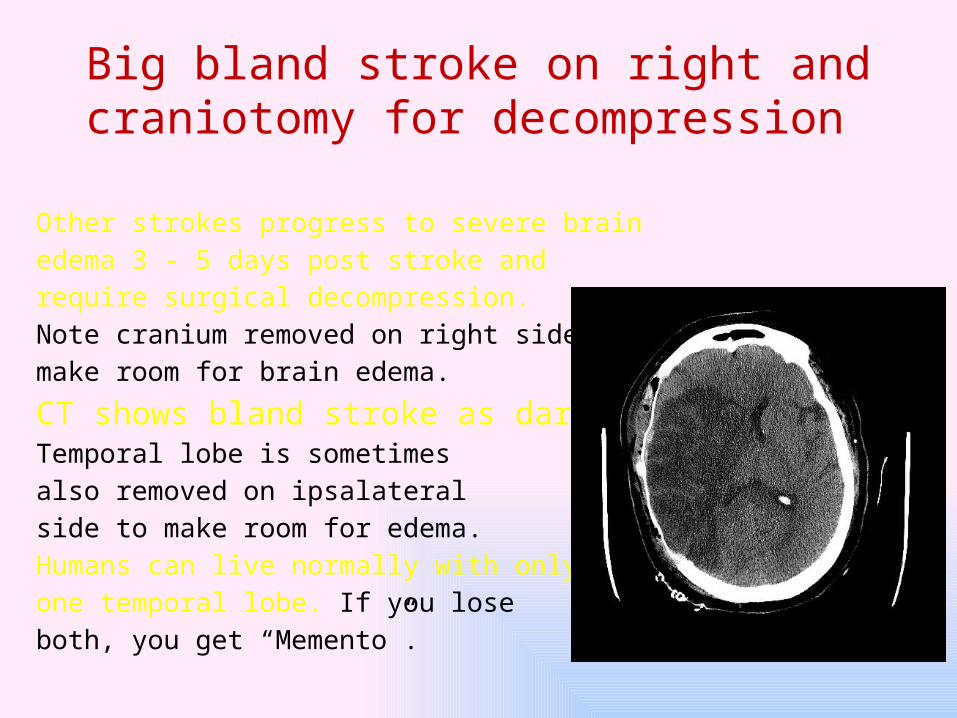
Big bland stroke on right and craniotomy for decompression
Other strokes progress to severe brain edema 3 - 5 days post stroke andrequire surgical decompression. Note cranium removed on right side tomake room for brain edema.
CT shows bland stroke as dark contrast. Temporal lobe is sometimes also removed on ipsalateral side to make room for edema. Humans can live normally with only one temporal lobe. If you loseboth, you get “Memento”.
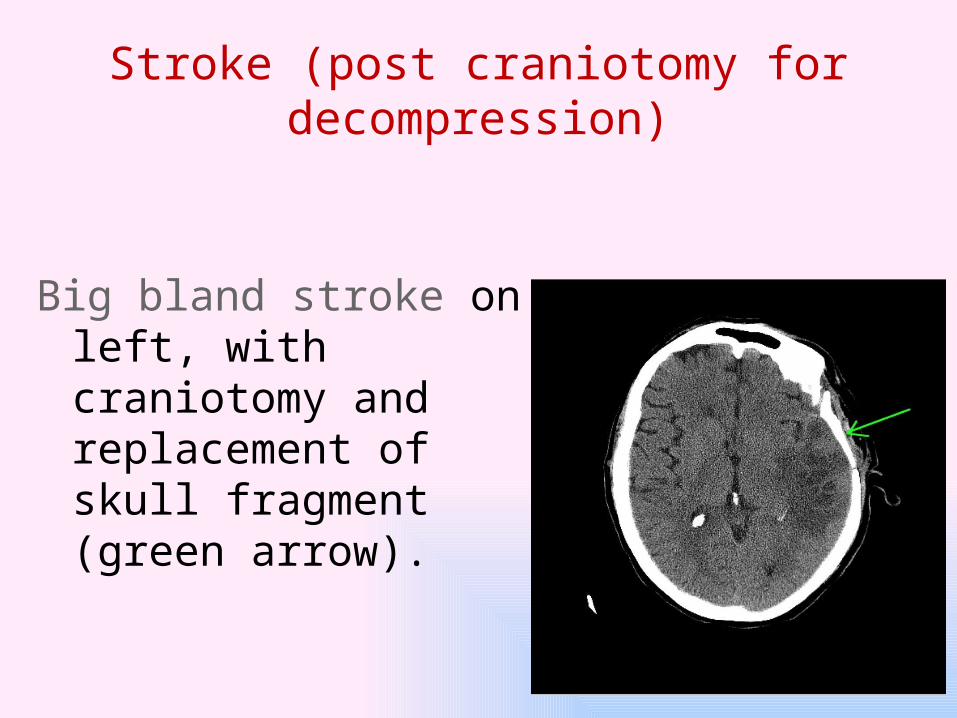
Stroke (post craniotomy for decompression)
Big bland stroke on left, with craniotomy and replacement of skull fragment (green arrow).
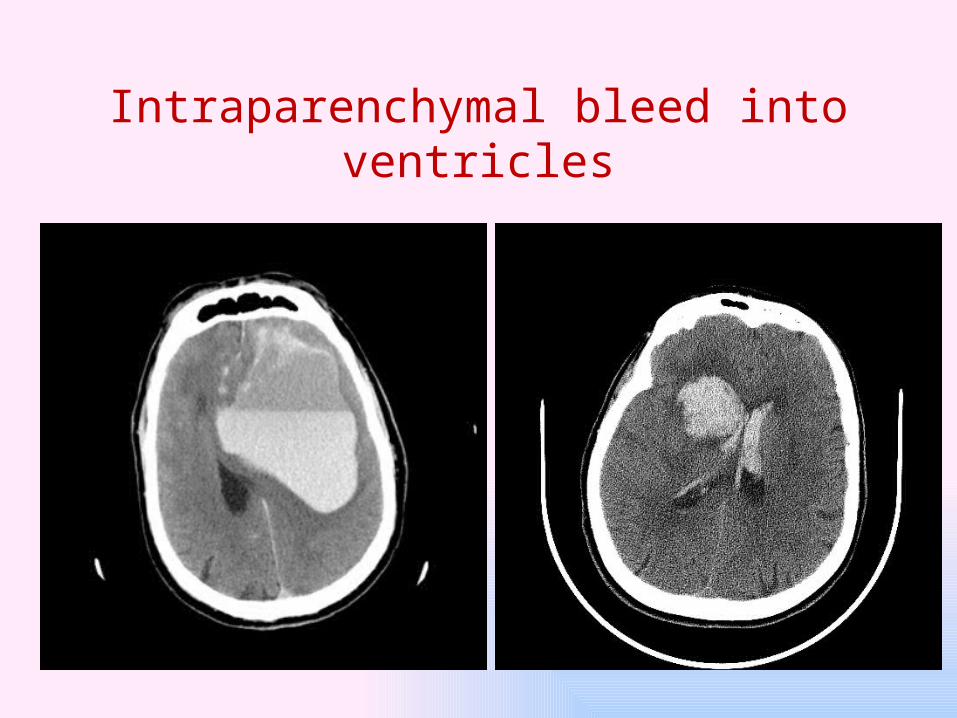
Intraparenchymal bleed into ventricles
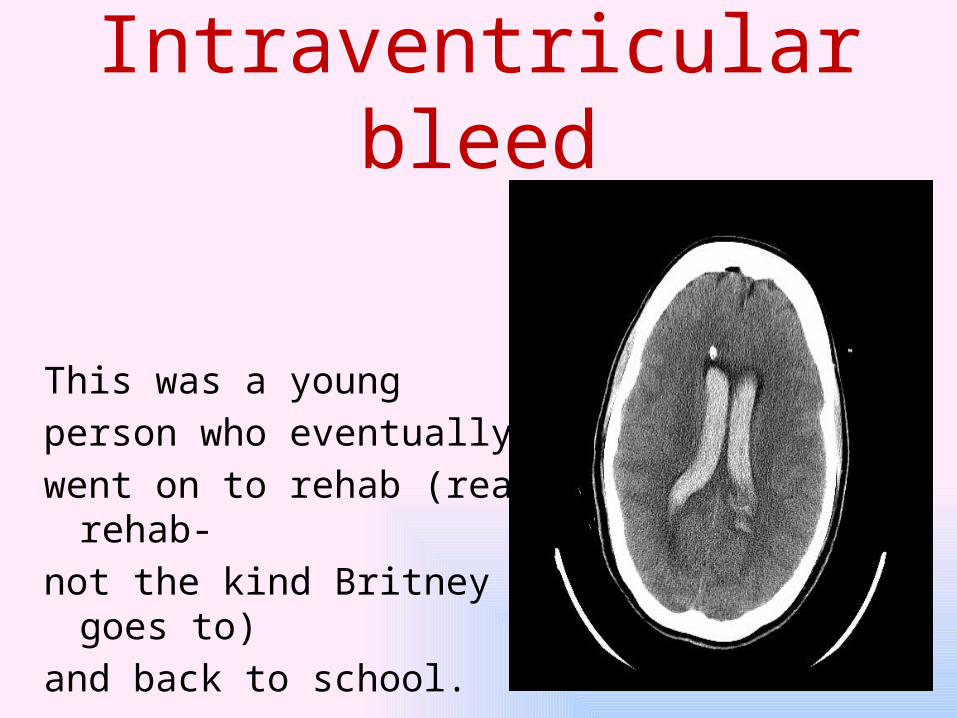
Intraventricular bleed
This was a young person who eventually went on to rehab (real rehab- not the kind Britney goes to) and back to school.

Normal MRI
MRI shows alterations between water and fat content of tissues. Gives a high resolution view of brain,
especially stroke, appearing as white contrast
which sometimes can take as long as 8 hours to show up.
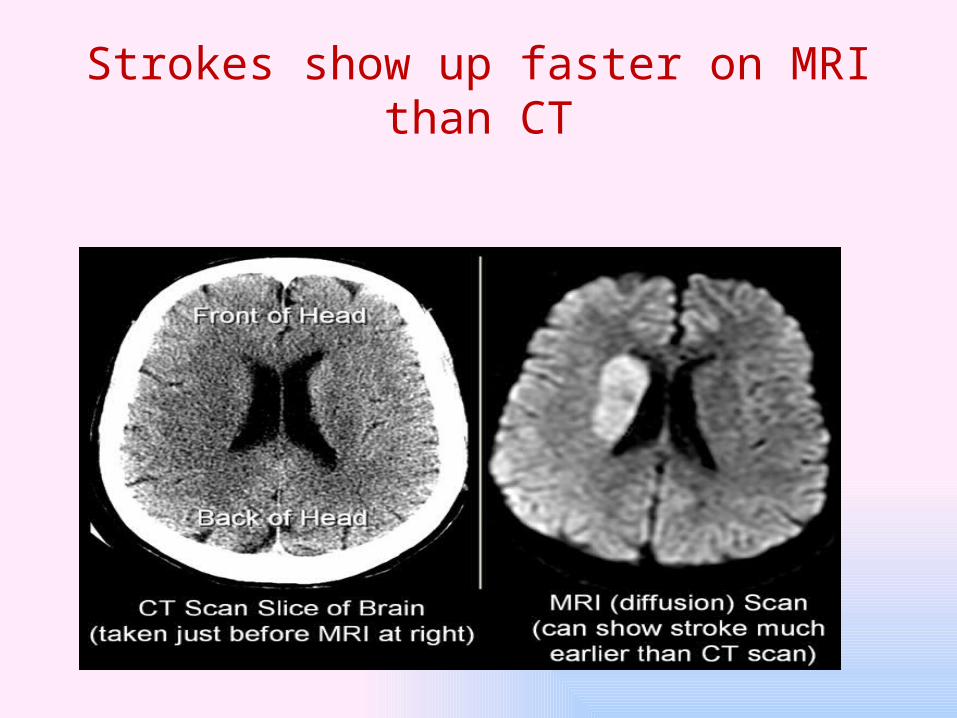
Strokes show up faster on MRI than CT

MRI and CAT views of the same whole R. hemispherical infarct
Some very big strokes settle down and don’t require surgical decompression.
This man opens his eyes to verbal on nasal cannula and follows on the right side 10 days post stroke.
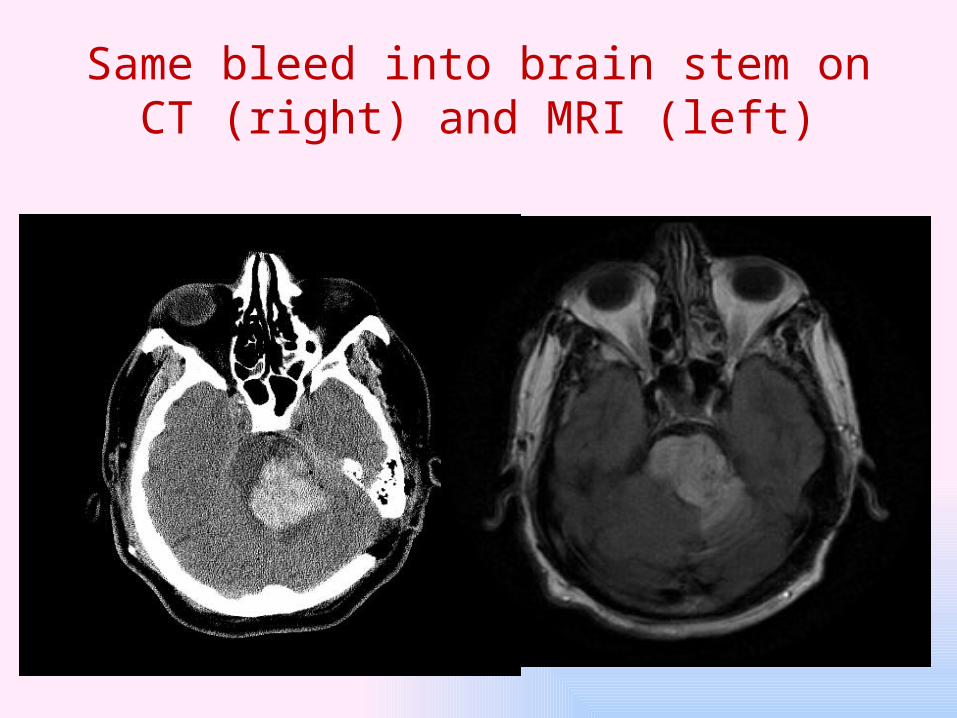
Same bleed into brain stem on CT (right) and MRI (left)
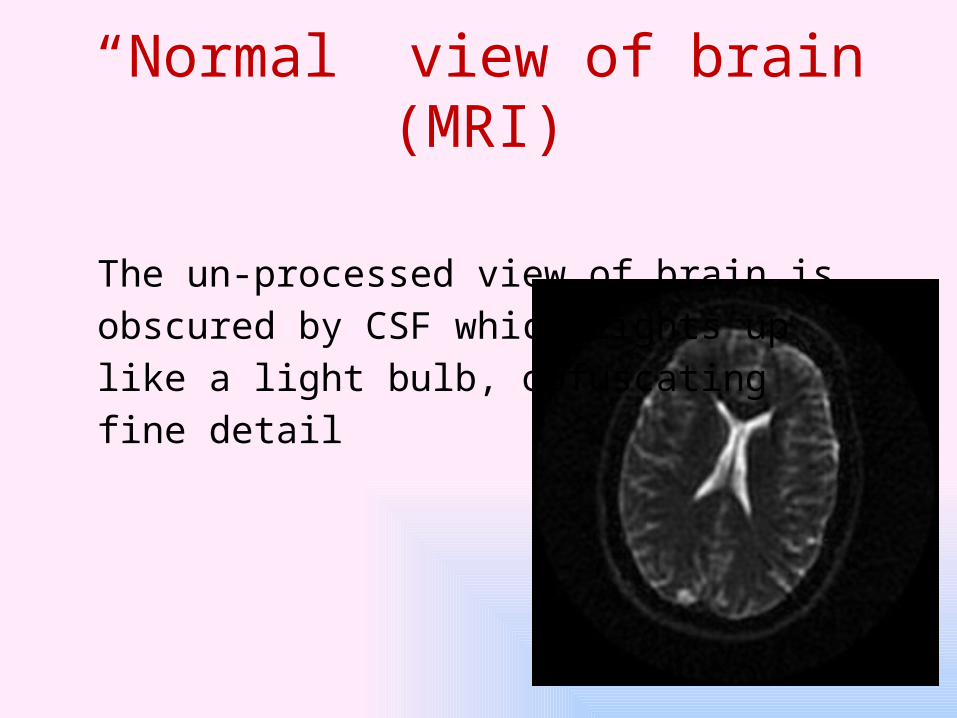
“Normal” view of brain (MRI)
The un-processed view of brain is obscured by CSF which lights up like a light bulb, obfuscating fine detail

T2 FLAIR negates CSF
The T2 FLAIR view negates CSF, allowing a more accurate view of brain structure. However, the T2 shows most pathology in the brain as white and does not differentiate well between ischemia, tissue damage and bleeding.

New stroke on T2 FLAIRNew strokes usually show up as white on T2.
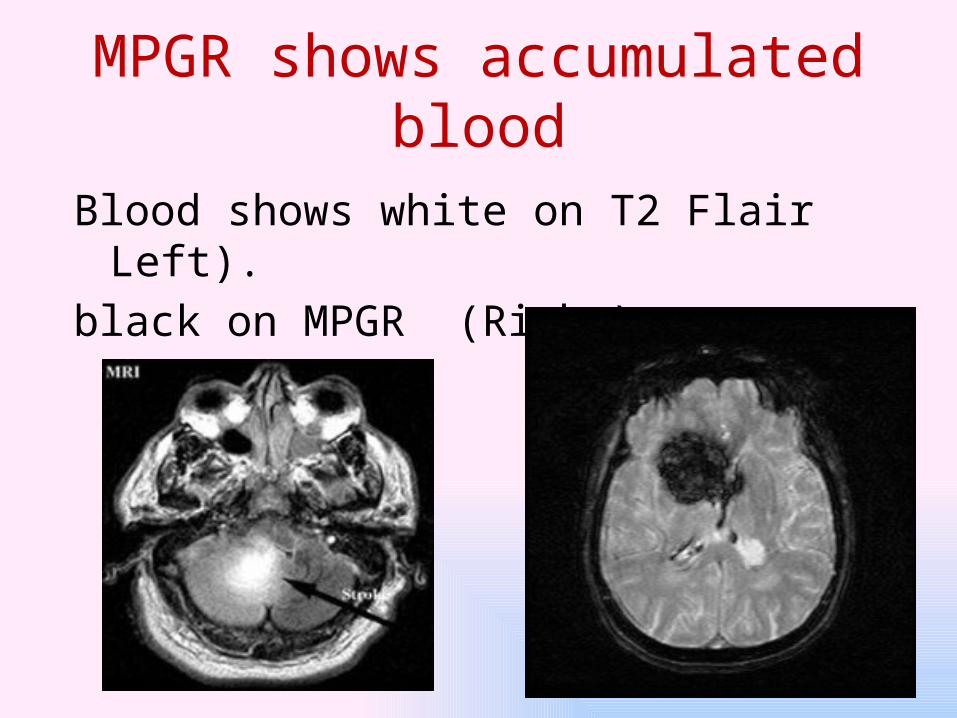
MPGR shows accumulated blood
Blood shows white on T2 Flair Left). black on MPGR (Right),

Old strokeUsually cystify and develop firm borders
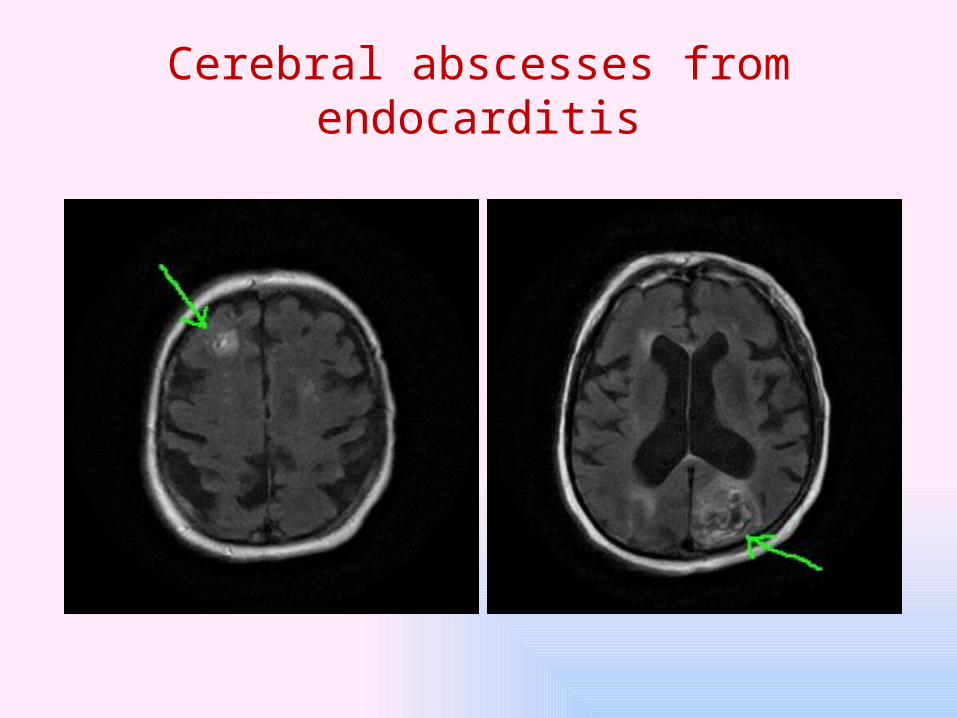
Cerebral abscesses from endocarditis
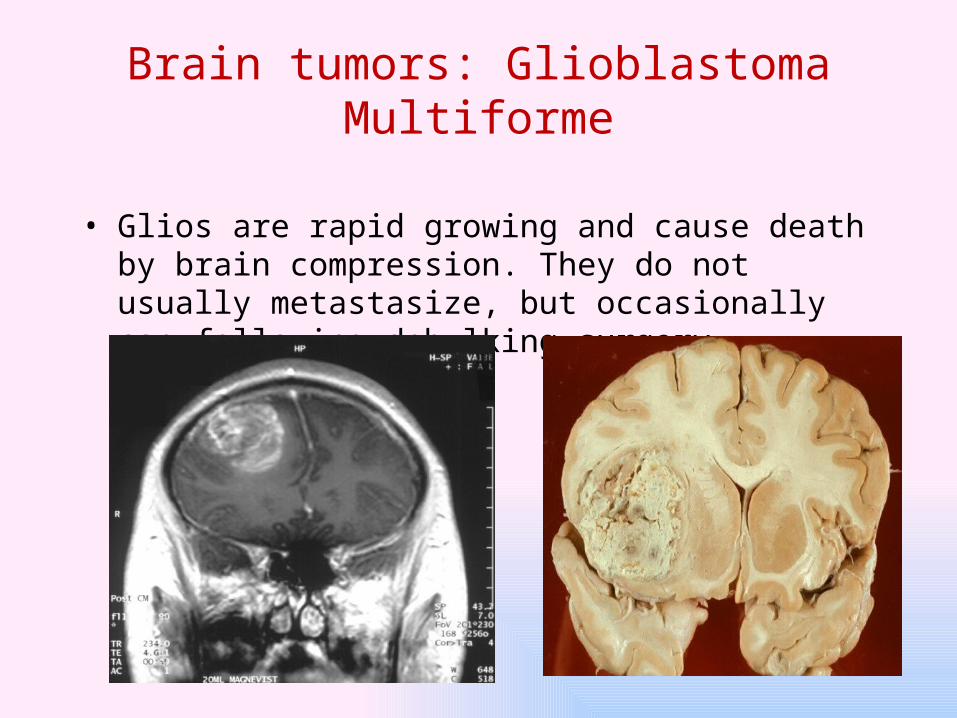
Brain tumors: Glioblastoma Multiforme
• Glios are rapid growing and cause death by brain compression. They do not usually metastasize, but occasionally can following debulking surgery.
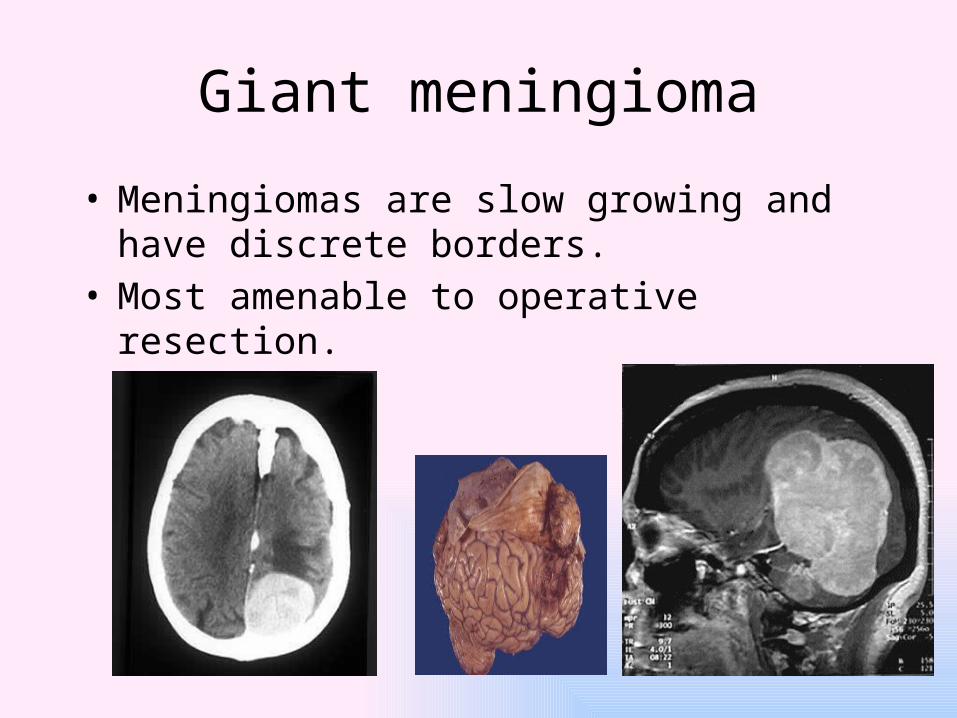
Giant meningioma
• Meningiomas are slow growing and have discrete borders.
• Most amenable to operative resection.
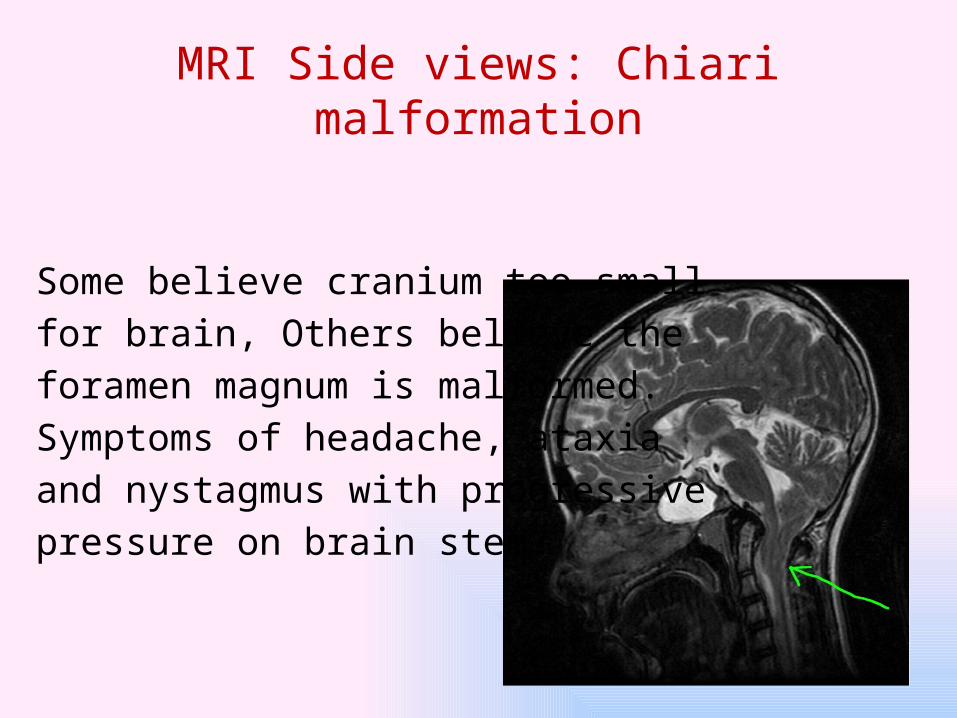
MRI Side views: Chiari malformation
Some believe cranium too small for brain, Others believe the foramen magnum is malformed. Symptoms of headache, ataxia and nystagmus with progressive pressure on brain stem.

Bi-temporal distribution is typical. Thought to occur by re-activation of herpes virus much like “cold sores” except through different nerve distribution
Herpes encephalitis

Hydrocephalus

CT angio of giant unruptured MCA aneurysm
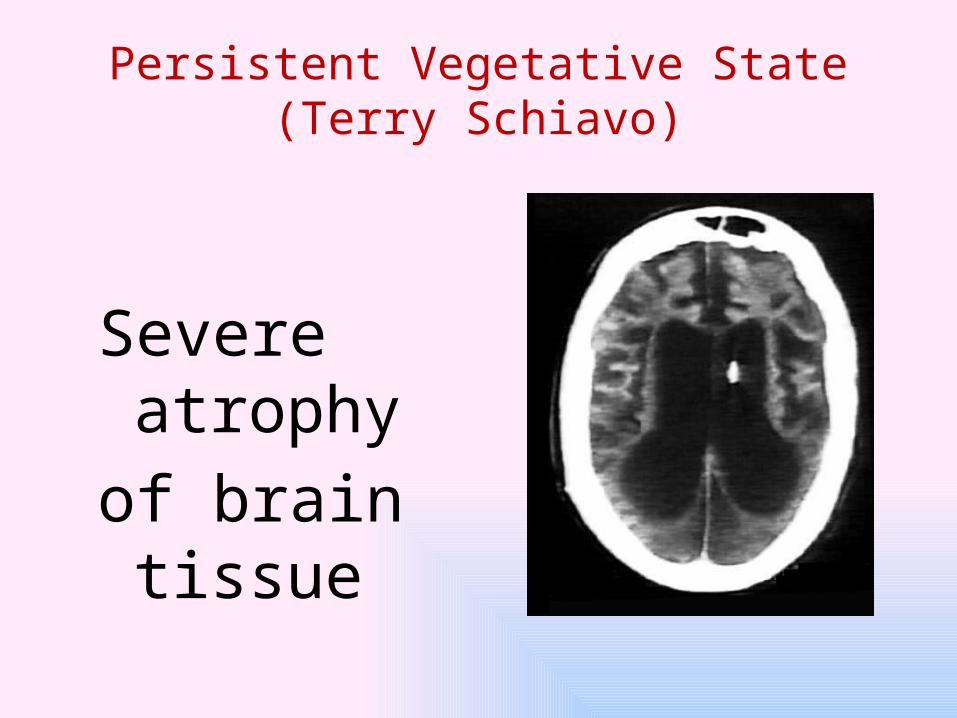
Persistent Vegetative State (Terry Schiavo)
Severe atrophy of brain tissue