BRAIN CHA-NGES IN RUPTURED INTRACRANIAL ANEURYSM · J. clin. Path. (1959), 12, 391. BRAIN CHA-NGES...
9
J. clin. Path. (1959), 12, 391. BRAIN CHA-NGES IN RUPTURED INTRACRANIAL ANEURYSM BY B. E. TOMLINSON From the Department of Pathology, Newcastle General Hospital (RECEIVED FOR PUBLICATION FEBRUARY 19, 1959) Since the papers of Beadles (1907), Fearnsides (1916), and Symonds (1924), there have been numerous publications on the clinical manifesta- tions, prognosis, and treatment of spontaneous subarachnoid haemorrhage. The pathology of the brain has received less attention. Many accounts have been taken from routine necropsy reports and few have included detailed examinations of the brain. Intracerebral bleeding has received most attention, largely since the paper of Richardson and Hyland (1941), but recently ischaemic lesions have been more widely recognized (Robertson, 1949; Wilson, Riggs, and Rupp, 1954; Bebin and Currier, 1957). Robertson (1949) described five instances of ischaemia, and it is noteworthy that three were seen in the 10 cases he observed himself, whereas only two were recorded in more than 80 routine post-mortem reports he reviewed. The greatest incidence of infarction is reported by Wilson et al. (1954), who noted focal ischaemic lesions in 45% of their necropsy material. No account, to my knowledge, however, gives details of the distribution, size, and importance of ischaemic lesions and their relation to other findings in the brain. This paper reports the brain findings in a series of 32 consecutive cases of fatal ruptured intracranial aneurysms. Two further instances have been excluded because surgical intervention made assessment of the pre-operative findings impossible. The ischaemic lesions found are described in detail, as are the instances of localized subarachnoid collections of blood (subarachnoid haematomata) which may well be important in the production of ischaemic lesions and intracerebral haemorrhage. Mention is also made of granular cell degeneration of the cerebellum which is uncommon and probably a terminal event. 20 Method of Investigation At necropsy the brain was examined externally only, and the bleeding aneurysm located where this was possible without disturbing the blood lying in the fissures, or between the lobes. After fixation for one to two months in formol-saline, the basal vessels were removed from the specimen. The brain was then cut into numerous slices and the distribution of blood in the sulci and fissures noted; material for histology was taken from many areas of the cerebral cortex, basal ganglia, brain-stem, and cerebellum. Particular attention was paid to any area suggestive of infarction and sufficient sections were taken to map out the area involved. Haematoxylin and eosin staining was used routinely, but Nissl, Mallory's phosphotungstic-acid- haematoxylin, Holzer, myelin, neurofibrillary, and fat stains were used where needed. Results Multiple aneurysms were found in 14 cases; in one of these, many small aneurysms were present on an angiomatous malformation in the Sylvian fissure. In a further case, a single aneurysm on an anterior cerebral artery was associated with an angioma in the frontal lobe on the same side. Thus, in 15 out of 32 cases (over 46%), multiple possible sources of bleeding existed. This is a higher percentage of multiple aneurysms than usually reported. Robertson (1949) found 5%, Bigelow (1955) 10%, Wilson et al. (1954) 19%, and Richardson and Hyland (1941) 25%. The true figure may not be as high as in this short series, but it will be far higher than is usually reported. Small aneurysms arising on the superior aspect of the circle of Willis will only be detected after the vessels have been dissected off the brain. The ruptured aneurysms were, in all but one instance, situated anteriorly on the circle of Willis or its branches. Commonly, two vessels were copyright. on June 10, 2020 by guest. Protected by http://jcp.bmj.com/ J Clin Pathol: first published as 10.1136/jcp.12.5.391 on 1 September 1959. Downloaded from
Transcript of BRAIN CHA-NGES IN RUPTURED INTRACRANIAL ANEURYSM · J. clin. Path. (1959), 12, 391. BRAIN CHA-NGES...

J. clin. Path. (1959), 12, 391.
BRAIN CHA-NGES IN RUPTURED INTRACRANIALANEURYSM
BY
B. E. TOMLINSON
From the Department of Pathology, Newcastle General Hospital
(RECEIVED FOR PUBLICATION FEBRUARY 19, 1959)
Since the papers of Beadles (1907), Fearnsides(1916), and Symonds (1924), there have beennumerous publications on the clinical manifesta-tions, prognosis, and treatment of spontaneoussubarachnoid haemorrhage. The pathology ofthe brain has received less attention. Manyaccounts have been taken from routine necropsyreports and few have included detailedexaminations of the brain. Intracerebralbleeding has received most attention, largely sincethe paper of Richardson and Hyland (1941), butrecently ischaemic lesions have been more widelyrecognized (Robertson, 1949; Wilson, Riggs,and Rupp, 1954; Bebin and Currier, 1957).Robertson (1949) described five instances ofischaemia, and it is noteworthy that three wereseen in the 10 cases he observed himself, whereasonly two were recorded in more than 80 routinepost-mortem reports he reviewed. The greatestincidence of infarction is reported by Wilsonet al. (1954), who noted focal ischaemic lesions in45% of their necropsy material. No account, tomy knowledge, however, gives details of thedistribution, size, and importance of ischaemiclesions and their relation to other findings in thebrain.
This paper reports the brain findings in a seriesof 32 consecutive cases of fatal rupturedintracranial aneurysms. Two further instanceshave been excluded because surgical interventionmade assessment of the pre-operative findingsimpossible. The ischaemic lesions found aredescribed in detail, as are the instances oflocalized subarachnoid collections of blood(subarachnoid haematomata) which may well beimportant in the production of ischaemic lesionsand intracerebral haemorrhage. Mention is alsomade of granular cell degeneration of thecerebellum which is uncommon and probably aterminal event.
20
Method of InvestigationAt necropsy the brain was examined externally
only, and the bleeding aneurysm located where thiswas possible without disturbing the blood lying in thefissures, or between the lobes. After fixation for oneto two months in formol-saline, the basal vesselswere removed from the specimen. The brain wasthen cut into numerous slices and the distribution ofblood in the sulci and fissures noted; material forhistology was taken from many areas of the cerebralcortex, basal ganglia, brain-stem, and cerebellum.Particular attention was paid to any area suggestiveof infarction and sufficient sections were taken tomap out the area involved.
Haematoxylin and eosin staining was usedroutinely, but Nissl, Mallory's phosphotungstic-acid-haematoxylin, Holzer, myelin, neurofibrillary, andfat stains were used where needed.
ResultsMultiple aneurysms were found in 14 cases; in
one of these, many small aneurysms were presenton an angiomatous malformation in the Sylvianfissure. In a further case, a single aneurysm on ananterior cerebral artery was associated with anangioma in the frontal lobe on the same side.Thus, in 15 out of 32 cases (over 46%), multiplepossible sources of bleeding existed. This is ahigher percentage of multiple aneurysms thanusually reported. Robertson (1949) found 5%,Bigelow (1955) 10%, Wilson et al. (1954) 19%,and Richardson and Hyland (1941) 25%. Thetrue figure may not be as high as in this shortseries, but it will be far higher than is usuallyreported. Small aneurysms arising on thesuperior aspect of the circle of Willis will only bedetected after the vessels have been dissected offthe brain.The ruptured aneurysms were, in all but one
instance, situated anteriorly on the circle of Willisor its branches. Commonly, two vessels were
copyright. on June 10, 2020 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.12.5.391 on 1 Septem
ber 1959. Dow
nloaded from

B. E. TOMLINSON
involved by the aneurysm arising at a bifurcation,a fact of surgical importance and one which mayinfluence the distribution of the ischaemic lesions.Subdural haematomas were seen twice fromruptured internal carotid aneurysms, but onneither occasion were they large enough to be ofpractical importance. Some surface subarachnoidhaemorrhage was visible in All but one case, and,in this, separation of the frontal lobes revealeda massive haemorrhage. In 14 the surfacebleeding was slight, but in 17 it was generalized,and at least 2-3 mm. thick over some portion ofthe brain. In only three of the 32 cases wasmassive generalized subarachnoid bleeding theonly significant finding. The other 29 (90%) hadadditional lesions.
Localized Collections of Blood in SubarachnoidSpace (Subarachnoid Haematomata). - Theimpression that, at most, a little blood clot ismet with in the subarachnoid space (Falconer,1954) is shown to be incorrect by the examinationof brains which have been fixed withoutdisturbance of the sulci or fissures. With orwithout generalized subarachnoid bleeding, sulciclose to the aneurysm are often widened byblood. This may spread in the depth of the sulci
AA. A
I...2
i.".- - I
.i
w..w:: t4
/: :t++~~~
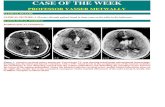
FIG. 1.-A massive collection of blood confined to the Sylvian fissureand depths of neighbouring sulci.
FIG. 2.-Blood in the Sylvian fissure with rupture down a sulcus onthe insular cortex. Infarction surrounding distended neighbour-ing sulcus.
for considerable distances and be from 0.5 to 1.5cm. thick and accompanied by infarction in thesurrounding cortex. Subarachnoid haematomataare particularly liable to collect between thefrontal lobes from ruptured aneurysms on theanterior communicating and anterior cerebralarteries, and in the Sylvian fissures from rupturedmiddle cerebral aneurysms. In these situations,the blood may be confined to the subarachnoidspace, or may rupture into the cerebral tissue,whilst little escapes on to the brain surface.Large haematomata act as space-occupyingmasses, and are not infrequently associated withinfarction.
In this series, large haematomata, totally orpartially confined to the subarachnoid space, werepresent in nine (28%) brains.Three very large collections were seen in the
Sylvian fissure from ruptured middle cerebralaneurysms, one (Fig. 1) being entirely confined tothe fissure and causing death by acting as aspace-occupying lesion. The white matter of thetemporal lobe was markedly oedematous and fociof acute neuronal degeneration were present inthe insular cortex. In the second instance (Fig. 2)a massive clot was present in the Sylvian fissure
392
X
copyright. on June 10, 2020 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.12.5.391 on 1 Septem
ber 1959. Dow
nloaded from

BRAIN CHANGES IN RUPTURED INTRACRANIAL ANEURYSM
and had caused limited intracerebral bleeding bybreaching the deepest limit of an insular sulcus.The blood also greatly widened a neighbouringsulcus. The insular and much of the temporalcortex was infarcted. Again, little surfacebleeding was present. In the third case a massof blood, 6 cm. long and 3 cm. wide, in theSylvian fissure had ruptured into thepostero-superior aspect of the insula, producingintracerebral and some intraventricular bleeding;pantine and peduncular haemorrhages, the resultof the supratentorial mass, were present. Theaneurysm was partly embedded in cerebral tissuebut had not ruptured directly into the brain, thebreach of the insular cortex being far posterior tothe aneurysm. Small areas of acute infarctionwere present in the cortex of the middle andsuperior temporal gyri.
Six large subarachnoid haematomata, wereassociated with ruptured aneurysms on theanterior cerebral or anterior communicatingarteries. From these sites the blood may burrowinto the sulci on the medial and inferiorsurfaces of the frontal lobes, or collect betweenthe frontal lobes. If this occurs the thin rostrumof the corpus callosum may rupture withresulting intraventricular bleeding, as seen inFig. 3. In this patient subarachnoid bleedingwas present long before the intraventricularhaemorrhage, since, three weeks before death, thepatient had recurrent headaches with blood-stainedcerebrospinal fluid, before becoming deeply
FIG. 3.-A massive collection of blood burrowing into sulci on theinferomedial surface of the frontal lobe and causing intraventri-cular haemorrhage by tearing the rostrum of the corpus callosum.
unconscious a few days before death. Further,small areas of infarction of some standing werepresent in the frontal lobes, for new blood vesselformation and astrocytic proliferation hadoccurred and the peripheral parts of the bloodclot itself were being organized.A second case presented almost identical
pathological findings.In the third case a blood clot, 3 cm. across,
separated the frontal lobes, opening up the sulcion the medial surface on the left side, withnumerous narrow tracks of blood into thehemisphere. This, like Robertson's (1949) similarcase, was accompanied by infarction over thedistribution of both anterior cerebral arteries.The fourth case presented a similar blood clotbetween the frontal lobes with necrosis limited tothe frontal lobes in the immediate vicinity of theclot. In the fifth case much blood was present inthe basal cisterns, but the Sylvian fissures andparieto-temporal sulci had been greatly widened,and blood had extended into the olfactory sulcusfrom below, producing what at first sightappeared to be an intracerebral haemorrhage(Fig. 4). The triangular-shaped blood clot was,however, almost completely surrounded by greymatter and was confined to the sulcus except atits posterior limit, where it had slightly extendedinto the brain. Infarction of the insular cortexand putamen was present. The sixth case showedan extension of blood over the superior surface ofthe infarcted and collapsed corpus callosum(Fig. 5), and there was massive bilateralinfarction of anterior cerebral artery distribution.An attempt to clip the aneurysm, five days beforedeath, was not responsible for the findings, for thehistology was that of infarction of several weeks'standing and the diagnosis of frontal lobeinfarction was suggested before operation.Similar cases have been seen by Robertson (1949)and Maloney (1958).
In two other instances the olfactory sulcus hasbeen markedly distended by blood, and clot more.than 1 cm. wide has been seen in the Sylvianfissure also twice. In a further case, from rupture.of an internal carotid aneurysm, blood had,tracked into, and greatly distended, many sulci onthe inferomedial surface of the hemisphere on theside of the aneurysm, with little trace of bleedingover the gyri.
Intracerebral and Intraventricular Haemor.rhage.-Bleeding into the brain occurred in 17 ofthe 32 cases (53%), and in 12 of these massivebleeding reached the ventricles. The route to theventricles was through the rostrum of the corpus
393
4...:.~:.I
copyright. on June 10, 2020 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.12.5.391 on 1 Septem
ber 1959. Dow
nloaded from

B. E. TOMLINSON
FIG. 4.-A massive collection of blood in a greatly widened olfactorysulcus; much blood in Sylvian fissure and depths of neigh-bouring sulci. Infarction of putamen.
callosum in seven, the insular cortex in one, andthe frontal lobe to the anterior horn in four. Inthree cases where the rostrum was torn,haematomata were present in the frontal lobe.Of the five instances of intracerebral haematomatawithout rupture into the ventricles, three wereinto the basal ganglia through the insular cortex,one into the temporal lobe, and one into thefrontal lobe. An important point in relation to
these 17 instances is that in only six was theaneurysm adherent to or embedded in cerebraltissue, and the bleeding into the brain wastherefore not direct.A little blood was present in the ventricles
in a further six instances; in two of these it hadreached the anterior horn of the lateral ventriclevia narrow haemorrhagic tracks through the cere-bral substance, but in four blood had apparentlyreached the ventricles through the foramina ofthe fourth ventricle.The percentage of intracerebral haemorrhage in
this series is somewhat lower than the 60-75 whichis usually recorded, but it would have beenconsiderably higher (68%) if subarachnoid haema-tomata had not been separated from intracerebralbleeding. One must also distinguish massive intra-cerebral bleeding from the linear haemorrhageswhich are common in the neighbourhood of theruptured aneurysm. These latter, histologically,are perivascular and often run at right anglesto the cerebral surface, and when numerous theyare usually accompanied by parenchymatousdegeneration. Their appearances strongly suggestthat they result from blood tracking along theVirchow-Robin spaces into the cerebral tissueitself, forming linear intracerebral haemorrhages.It is clearly possible that coalescence of numeroushaemorrhages produced in this fashion may resultin a large haematoma.
Massive bleeding into the ventricles usuallycauses death in less than six hours (Bebin andCurrier, 1957). Blood cannot escape rapidly fromthe ventricles (Symonds, 1924), and great dilatationcommonly follows intraventricular bleeding. Thefourth ventricle is often dilated to several timesits normal size, with consequent distortion andpressure on pontine, medullary, and cerebellarstructures. Haemorrhages, oedema, and occa-sionally actual infarction in the roof of the fourthventricle result, and, less frequently, lesions inthe medulla and pons. Subependymal haemor-rhages also occur in the lateral ventricles, andless commonly in the peri-aqueductal tissues andanterior hypothalamus. Hypothalamic haemor-rhages and necrosis are common with ruptureof the rostrum, and in this series have been seennine times ; in eight the lesions were in the anteriorhypothalamus. In six instances this hypothalamicdamage was associated with massive intra-ventricular haemorrhage; in the other threeinstances the ruptured aneurysm was twice situatedon the anterior cerebral and once on the internalcarotid artery.
394
copyright. on June 10, 2020 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.12.5.391 on 1 Septem
ber 1959. Dow
nloaded from

BRAIN CHANGES IN RUPTURED INTRACRANIAL ANEURYSM
FIG. 5.-Blood clot lying over infarcted corpus callosum. Infarction of medial surface of anterior half of hemisphere.
Haemorrhages or degeneration, separately, ortogether, in the pons or cerebral peduncles, havebeen seen nine times, and in all but one instance,where infarction in the distribution of theposterior cerebral artery was present, they wereconsidered to be due to increased supratentorialpressure. In four instances they accompaniedmassive intraventricular haemorrhage, in threesubarachnoid bleeding without intracerebralbleeding, and in one massive infarction with greatswelling of a hemisphere.
Cerebral Infarction. -Localized degenerationand gliosis up to 1 cm. in depth is almostinvariable around aneurysms embedded incerebral tissue. This lesion may be asymptomaticand found in people who die from a singlerapidly fatal haemorrhage. In addition,ischaemic lesions, varying from microscopic focito massive infarctions, are very common. In thisseries 25 of the 32 brains examined (78%)showed ischaemic lesions, and in 13 (40%) thesewere massive. The smaller lesions are oftenmultiple, and cortical foci up to 1 cm. across maybe separated by areas of normal brain, and in thefixed specimen appear as pale, irregularly roundareas in the cortex, to which, if numerous, theyimpart a " moth-eaten " appearance. Similar,
scattered foci are infrequently seen in the deepwhite matter, and occasionally, as reported byFalconer (1954), they occur in the depths of thesulci. If the foci are few, they are usually inthe immediate neighbourhood of the rupturedaneurysm. They are particularly common on themedial surface of the hemisphere with rupturedaneurysms on or near the anterior communicatingvessels. Four instances of such lesions have beenseen in this series. In ruptured middle cerebralaneurysms similar foci occur on the insularcortex but also in the parietal or temporal lobewell away from the source of bleeding. Withruptured internal carotid aneurysms ischaemicfoci may occur in the territory of both the middleand anterior cerebral arteries.Of the 13 major infarctions, four involved the
cortical territory of the anterior cerebral artery,on three occasions bilaterally. In two examplesof bilateral infarction, the aneurysm was on theanterior communicating artery; in the third itwas on the internal carotid, and patchy infarctionof middle cerebral artery distribution was alsopresent. In these three cases the cortex andunderlying white matter was to a large extentdestroyed in all sections from the medial surfaceof both hemispheres as far as the occipito-parietal
395
copyright. on June 10, 2020 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.12.5.391 on 1 Septem
ber 1959. Dow
nloaded from

B. E. TOMLINSON
sulcus and of the corpus callosum. In the fourthcase the aneurysm was on the anteriorcommunicating artery and one frontal lobeshowed massive infarction, the other onlyscattered ischaemic foci. In three of the aboveinfarction was limited to the cortical supply ofthe artery, but in one areas of infarction in thehead of the caudate nucleus and anterior limb ofthe internal capsule indicated involvement ofcentral branches. In two of the above fourinstances the infarction was associated withsubarachnoid haematomata, once between theanterior frontal lobes and once over the corpuscallosum. In the other two, massiveintraventricular haemorrhage had occurredthrough rupture of the rostrum, and in one ofthese a large haematoma filled the olfactorysulcus. Since massive intraventricular rupture isprobably rapidly fatal, it is likely in these cases thatconsiderable haemorrhage anterior to the rostrumwas present for some time before its rupture.
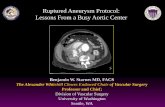
In eight cases there was infarction of a largearea of brain supplied by the middle cerebralartery. In three the aneurysm was on the middlecerebral artery on the same side as the infarctionand in three it was on the internal carotid on thatside. In two it was on the anterior communicatingartery; in one of these a haematoma occupied thefrontal lobe. In both cases the only infarctionwas in the territory of the middle cerebral artery.In three of the eight cases almost all the cortexsupplied by the middle cerebral' artery wasinfarcted, and in two of these the territory of theposterior cerebral artery was also involved(Fig. 6). In the other five cases a considerablearea of cortex supplied by the middle cerebralartery was infarcted; in two the insular was mostseverely involved. A considerable depth of whitematter was involved in these infarctions, usuallyreaching the lateral ventricle; in two instancesfoci of softening throughout the centrum semi-ovale were more obvious to the naked eye thancortical lesions, though the latter were extensivemicroscopically. Foci of infarction were found inthe basal ganglia only once, indicating that thecentral branches of the middle cerebral arteryusually escape involvement. In four of these eightinstances a layer of blood more than 1 cm. thickwas present in the Sylvian fissure. Two of theremaining four had an intracerebral haematoma,one in the frontal lobe, the other in the anteriortemporal lobe.One instance of infarction of the entire
territory of the posterior cerebral artery alone wasseen, this associated with a ruptured aneurysm
I
FIG. 6.-Infarction of middle and posterior cerebral artery territoryfrom rupture of an aneurysm on the middle cerebral artery.
involving the basilar and posterior cerebralarteries. Only moderate bleeding around theruptured aneurysm was present. The twoinstances of posterior cerebral artery infarctionassociated with middle cerebral artery lesionswere probably the result of supratentorialpressure from the bleeding and from swelling ofthe hemisphere from the middle cerebral lesion.Feigin (1955) reported two similar cases.
In most instances the age of the infarction,based on histological appearances, correspondedapproximately to the time of a major clinicalepisode. Two patients dying less than 24 hoursafter a single haemorrhage showed early, massiveinfarction, with patchy coagulative necrosis,numerous haemorrhages and oedema, andshrinkage of neurones in the involved tissue. Asubject dying after three days showed greatoedema of both frontal lobes with disintegrationof the majority of neurones, myelin sheaths, andoligodendroglia. One man living for seven daysshowed great swelling of both frontal lobes withmuch neuronal destruction, increase of cellularity,new blood vessel formation, and well-markedsoftening of the white matter. Patients survivinglonger than this showed progressively more
396
*.ffi.
Al..
copyright. on June 10, 2020 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.12.5.391 on 1 Septem
ber 1959. Dow
nloaded from

BRAIN CHANGES IN RUPTURED INTRACRANIAL ANEURYSM
advanced softening of the white matter withdistinct astrocytic proliferation after threeweeks.Of the 13 instances of major infarction, eight
had only one episode of bleeding, but in the otherfive the course suggested recurrent haemorrhages,and in two of these the histology andsymptomatology suggested that the infarctionoccurred with the second and not the initialhaemorrhage. In a further case there wereinfarctions of obviously different ages, one relatedto the original bleeding six weeks before death,and the other to the final bleeding a few hoursbefore death.There was no evidence, from the clinical
course of the patients in this series, thatinvestigation or operation contributed to thedevelopment of infarction. Apart from the twocases eliminated because of surgery, two othersunderwent major operative procedures. In one,no infarction was present; in the other, frontallobe infarction was correctly diagnosed beforethe operation. Two cases had exploratory burrholes; one had an infarction, but the operationwas performed immediately before death andcould not have produced the ischaemic lesion.
Eighteen cases received no treatment or onlyantibiotics. In this group there were four majorinfarctions. In the treated group five showedclinical evidence of a cerebral lesion which provedto be an infarction, before treatment orinvestigation was begun. Therefore, in ninecases a major ischaemic lesion developedindependently of treatment.Ten of the treated cases were investigated by
angiography without adverse effects. Four caseswith major infarctions received, for the treatmentof decerebrate rigidity or multiple convulsions,medication capable of producing hypotension,and in one of these a severe episode ofhypotension was recorded. Possibly, therefore,the ischaemic lesion in these patients wasinfluenced by medication. There is no way ofdetermining this; all four were gravely ill whentreatment was begun, and possibly already hadischaemic lesions. But, clearly, hypotension ina patient with cerebral ischaemia is likely toincrease the severity of the lesion.
Degeneration of Granular Layer of Cere.belium. - Four instances of degeneration ofthe granular layer of the cerebellum were seen.The histological features in these cases were verysimilar to those described by Leigh and Meyer(1949) in association with visceral carcinomataand hypoglycaemic coma; they also mentioned
its occurrence in a case of subarachnoidhaemorrhage. The lesions varied from necrosisof all the nucleated elements in the granularlayer to patchy severe destruction of the granularlayer in which Golgi type 2 cells were preserved.In one case severe destruction of the granularlayer was present in all sections; the other threeshowed patchy destruction, one in all areasexamined, the other two mainly in the dorso-medial folia. The Bergmann glia appearedunaffected, and the Purkinje cells were notreduced in number though, in one case, someshowed acute chromatolysis. There was noevidence of reaction to the necrotic foci, anddegeneration of myelin and neurofibrils, glialproliferation, or excess of lipoids could not bedemonstrated. No changes were found in thedentate nucleus or the inferior olives.The ruptured aneurysm in three of these cases
was on the internal carotid artery and in thefourth on the anterior communicating artery.The bleeding was massive in three and slight inthe fourth.The lack of reaction to the degeneration
suggests it was a terminal event. All four patientshad an episode of subarachnoid bleeding threeto seven weeks before death, with partial orcomplete recovery. All four died suddenly froma further bleeding at the end of this period ofconvalescence. Three had been in hospital afterthe original bleeding, and no evidence ofcerebellar abnormality was noted.
DiscussionA variety of pathological lesions follows
rupture of an intracranial aneurysm. Withmassive bleeding, death may occur quickly, andlittle be found beyond blood in the subarachnoidspace or brain. In other cases bleeding leads tothe development of subarachnoid or intracerebralhaematomata which, acting as space-occupyinglesions, result in temporal herniation, lesions inthe brain-stem, and occasionally ischaemia of theoccipital and temporal lobes and posteriorthalamus. All these lesions have been seen in thisseries, and massive infarction with brain swellingcan produce them. Ruptured anterior cerebral,anterior communicating, and middle cerebralaneurysms are particularly likely to producehaematomata between the frontal lobes or in theSylvian fissure. From internal carotid aneurysms,blood may track into the Sylvian fissures, andfrom any aneurysm groups of sulci may be
397
copyright. on June 10, 2020 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.12.5.391 on 1 Septem
ber 1959. Dow
nloaded from

B. E. TOMLINSON
opened out by tracking blood. Blood may also
spread down the Virchow-Robin spaces into thebrain, producing perivascular haemorrhageswhich often extend into the white matter. When
the brain is sufficiently stretched by a localizedcollection intracerebral bleeding occurs. Thisprocess is probably more common than therupture directly into the cerebral tissue of an
aneurysm which has become embedded in, or
adherent to, the brain. Adhesions in thesubarachnoid space, resulting from previoushaemorrhage, would further hinder the escape ofblood from sulci or fissures and increase thelikelihood of intracranial rupture; the delicaterostrum of the corpus callosum is especially liableto be torn by a neighbouring haematoma.With rupture of any aneurysm, ischaemic
damage to some portion of the brain is highlylikely and massive infarction is not uncommon.
In this series no instance of a thrombosedmajor artery has been seen. Embolism from theaneurysmal sac is an equally unlikely cause ofthe infarction, for many involve the entireterritory of an artery and the clot would clearlyhave to lodge in the main stem of the arterywhere its detection would be easy. Smallperipheral emboli could account for scatteredinfarctions, but in many hundreds of sectionsexamined an occluded cortical artery has been*seen only once.
Three other possibilities exist to account forischaemic lesions. First, localized collections ofblood could, by stretching or kinking, greatlynarrow the vessels (Johnson, Potter, and Reid,1958). Second, a large mass of blood stretchinga major vessel may tear small branches passingfrom the parent vessel to the brain. This woulddeprive small areas of brain of their blood supplyand provide further sources of bleeding into thesubarachnoid space or brain. Either or both ofthese mechanisms might account for scattered as
well as major infarctions, and could be responsiblefor ischaemic lesions even when no localizedcollections are found at necropsy; stretching ofvessels by a haematoma may lead to irreversibleischaemic damage, but if the blood later escapesinto the generalized subarachnoid space or
ventricles, no local collection will be found atnecropsy.
The third possibility is that spasm maycause the ischaemic lesions. The radiologicalevidence that spasm occurs after subarachnoidhaemorrhage is strong (Ecker and Riemen-schneider, 1951; Norldn and Olivecrona, 1953).In peripheral arteries, stretching is a powerful
stimulus to spasm (Simmons, 1956), but the samecannot be said with certainty of the cerebralvessels. Localized blanching of the cerebralvessels may follow the production of brain swellingfrom intracerebral injection of saline (Wolff,1936), and Byrom (1954) attributed focal spasmduring experimental window insertion tostretching of the affected vessels. In the latter'sexperiments on rats local pressure on arteries didnot result in arterial contraction, though rubbingvessels (Florey, 1925) produced spasm whichvaried with the animal used. The latter alsoobserved spasm on either side of a point ofrupture, though it was insufficient to stopbleeding entirely.
Therefore, three mechanisms exist which mightlead to ischaemic lesions; these are stretching orkinking of vessels, tearing of small vessels, andspasm possibly induced by stretching. Sufficientevidence to incriminate one or more of thesemechanisms is not at present available, but all ofthem might be produced by haematomata, andthese are demonstrable in many instances.When intraventricular bleeding occurs slowly
the blood may, presumably, escape from theventricles sufficiently quickly to prevent theirgross distension. Massive bleeding with greatdilatation of the ventricles is, however, commonand clearly the rate of entry of blood into theventricles is then greater than its speed of exitthrough the foramina. The original bleeding neednot be rapid for this to occur. It is more likelythat rapidly fatal intraventricular haemorrhageresults from rupture of an intracerebral orsubarachnoid haematoma into the ventricularsystem, the haematoma often having collectedslowly. Obstruction to the escape of blood fromthe ventricles can occur from compression of theaqueduct after temporal herniation (Smyth andHenderson, 1938), but no instance of this hasbeen noted in this series.No explanation can be offered for the granule-
cell degeneration of the cerebellum, and it wouldappear to be a terminal phenomenon in the cases
reported here.Patients who survive rupture of an intracranial
aneurysm without sequelae presumably escapemajor infarction and large intracerebral or
subarachnoid haematomas. When recovery iscomplete the bleeding will have been either smallor from a site where blood could freely escapeinto the generalized subarachnoid space. But inWalton's series (1956), only about one third were
so fortunate, and the remainder had residualabnormalities. The cerebral lesions in these cases
398
copyright. on June 10, 2020 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.12.5.391 on 1 Septem
ber 1959. Dow
nloaded from

BRAIN CHANGES IN RUPTURED INTRACRANIAL ANEURYSM
probably only differed in degree from those in thefatal cases. Intracerebral and subarachnoidhaematomas will be largely absorbed with time,and ischaemia of varying degree probablyaccounts for most of the disabilities, though onlya careful study of such cases would settle thispoint.
It may be inappropriate to discuss treatment onthe basis of the findings in these fatal cases, buttwo points stand out. Draining the spinalsubarachnoid space can only be of value whenthe blood has ready access from the bleeding siteto the basal cisterns. When haematomata haveformed, draining the spinal theca will be futileand dangerous. Secondly, some cases havesubarachnoid or intracerebral collections whichrequire immediate surgery. Attempts to dealwith the aneurysm within a few hours ofhaemorrhage have frequently had dire results, butthere is little to be lost in attempting simpledrainage of entrapped collections through burrholes in patients who otherwise appear certain todie. The knowledge that these large collectionsare usually in or between the frontal lobes, or inthe Sylvian fissure or temporal lobes, should makeattempted evacuation a reasonable possibility inpatients otherwise considered hopeless. Thesurgical attack on the actual ruptured vesselcould be considered if improvement followeddirect drainage of the blood.
SummaryThe findings in the brain in 32 fatal cases of
ruptured intracranial aneurysm are reported.Blood tends to collect between the frontal
lobes, in the Sylvian fissure, and in the depths ofsulci, and in these positions may form largehaematomata. These may cause death by actingas space-occupying lesions and may lead to
intracerebral and intraventricular haemorrhage.They are probably of importance in thedevelopment of infarction.
Ischaemic cerebral lesions are very commonand massive infarction was found in 40% in thisseries. Ischaemic lesions probably producemost of the residual disabilities in non-fatalsubarachnoid haemorrhage. The possiblemechanisms of production of ischaemic lesionsare discussed.
I wish to thank my colleagues in the laboratory,particularly Dr. S. M. Bell and Dr. B. J. Smith, fortheir help in collecting this material; my clinicalcolleagues, particularly Mr. L. P. Lassman, forpermission to peruse their records; Dr. A. F. J.Maloney for most valuable comments on thehistological findings; and Mr. A. Hall, Mr. E.Manns, and Miss G. Hunt for technical assistance.
REFERENCESBeadies, C. F. (1907). Brain, 30, 285.Bebin, J., and Currier, R. D. (1957). A.M.A. Arch. intern. Med., go
771.Bigelow, N. H. (1955). A.M.A. Arch. Neurol. Psychiat., 73, 76.Byrom, F. B. (1954). Lancet, 2, 201.Ecker, A., and Riemenschneider, P. A. (1951). J. Neurosurg., 8, 660.Falconer, M. A. (1954). Proc. roy. Soc. Med., 47, 693.Fearnsides, E. G. (1916). Brain, 39, 224.Feigin, I. (1955). A.M.A. Arch. Neurol. Psychiat., 73, 463.Florey, H. (1925). Brain, 48, 43.Johnson, R. J., Potter, J. M., and Reid, R. G. (1958). J. Neurol.
Neurosurg. Psychiat., 21, 68.Leigh, A. D., and Meyer, A. (1949). Ibid., 12, 287.Maloney, A. F. J. (1958). Personal communication.Norlen, G., and Olivecrona, H. (1953). J. Neurosurg., 10, 404.Richardson, J. C., and Hyland, H. H. (1941). Medicine (Baltimore),
20, 1.Robertson, E. G. (1949). Brain, 72, 150.Simmons, E. H. (1956). A.M.A. Arch. Surg., 73, 625.Smyth, G. E., and Henderson, W. R. (1938). J. Neurol. Psychiat.,
n.s., 1, 226.Symonds, C. P. (1924). Quart. J. Med., 18, 93.Walton, J. N. (1956). Subarachnoid Haemorrhage. Livingstone,
Edinburgh and London.Wilson, G., Riggs, H. E., and Rupp, C. (1954). J. Neurosurg., 11, 128.Wolff, H. G. (1936). Physiol. Rev., 16, 545.
399
copyright. on June 10, 2020 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.12.5.391 on 1 Septem
ber 1959. Dow
nloaded from